
Dietary Intake of Polyphenols or Polyunsaturated Fatty Acids and Its Relationship with Metabolic and Inflammatory State in Patients with Type 2 Diabetes Mellitus

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galicia-Garcia, U.; Benito-Vicente, A.; Jebari, S.; Larrea-Sebal, A.; Siddiqi, H.; Uribe, K.B.; Ostolaza, H.; Martin, C. Pathophysiology of Type 2 Diabetes Mellitus. Int. J. Mol. Sci. 2020, 21, 6275. [Google Scholar] [CrossRef] [PubMed]
- Faselis, C.; Katsimardou, A.; Imprialos, K.; Deligkaris, P.; Kallistratos, M.; Dimitriadis, K. Microvascular Complications of Type 2 Diabetes Mellitus. Curr. Vasc. Pharmacol. 2020, 18, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Viigimaa, M.; Sachinidis, A.; Toumpourleka, M.; Koutsampasopoulos, K.; Alliksoo, S.; Titma, T. Macrovascular Complications of Type 2 Diabetes Mellitus. Curr. Vasc. Pharmacol. 2020, 18, 110–116. [Google Scholar] [CrossRef]
- Eizirik, D.L.; Pasquali, L.; Cnop, M. Pancreatic beta-cells in type 1 and type 2 diabetes mellitus: Different pathways to failure. Nat. Rev. Endocrinol. 2020, 16, 349–362. [Google Scholar] [CrossRef] [PubMed]
- Meigs, J.B. The Genetic Epidemiology of Type 2 Diabetes: Opportunities for Health Translation. Curr. Diab. Rep. 2019, 19, 62. [Google Scholar] [CrossRef] [PubMed]
- Berbudi, A.; Rahmadika, N.; Tjahjadi, A.I.; Ruslami, R. Type 2 Diabetes and its Impact on the Immune System. Curr. Diabetes Rev. 2020, 16, 442–449. [Google Scholar] [CrossRef]
- Daryabor, G.; Atashzar, M.R.; Kabelitz, D.; Meri, S.; Kalantar, K. The Effects of Type 2 Diabetes Mellitus on Organ Metabolism and the Immune System. Front. Immunol. 2020, 11, 1582. [Google Scholar] [CrossRef]
- Donath, M.Y.; Dinarello, C.A.; Mandrup-Poulsen, T. Targeting innate immune mediators in type 1 and type 2 diabetes. Nat. Rev. Immunol. 2019, 19, 734–746. [Google Scholar] [CrossRef]
- Association, A.D. Facilitating behavior change and well-being to improve health outcomes: Standards of medical care in diabetes—2021. Diabetes Care 2021, 44, S53–S72. [Google Scholar] [CrossRef]
- Childs, C.E.; Calder, P.C.; Miles, E.A. Diet and Immune Function. Nutrients 2019, 11, 1933. [Google Scholar] [CrossRef] [Green Version]
- Christ, A.; Lauterbach, M.; Latz, E. Western Diet and the Immune System: An Inflammatory Connection. Immunity 2019, 51, 794–811. [Google Scholar] [CrossRef] [PubMed]
- Chester, B.; Babu, J.R.; Greene, M.W.; Geetha, T. The effects of popular diets on type 2 diabetes management. Diabetes Metab. Res. Rev. 2019, 35, e3188. [Google Scholar] [CrossRef] [PubMed]
- Leri, M.; Scuto, M.; Ontario, M.L.; Calabrese, V.; Calabrese, E.J.; Bucciantini, M.; Stefani, M. Healthy Effects of Plant Polyphenols: Molecular Mechanisms. Int. J. Mol. Sci. 2020, 21, 1250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahidi, F.; Ambigaipalan, P. Omega-3 Polyunsaturated Fatty Acids and Their Health Benefits. Annu. Rev. Food Sci. Technol. 2018, 9, 345–381. [Google Scholar] [CrossRef]
- Di Lorenzo, C.; Colombo, F.; Biella, S.; Stockley, C.; Restani, P. Polyphenols and Human Health: The Role of Bioavailability. Nutrients 2021, 13, 273. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Luo, Q.; Nie, R.; Yang, X.; Tang, Z.; Chen, H. Potential implications of polyphenols on aging considering oxidative stress, inflammation, autophagy, and gut microbiota. Crit. Rev. Food Sci. Nutr. 2021, 61, 2175–2193. [Google Scholar] [CrossRef]
- Yahfoufi, N.; Alsadi, N.; Jambi, M.; Matar, C. The immunomodulatory and anti-inflammatory role of polyphenols. Nutrients 2018, 10, 1618. [Google Scholar] [CrossRef] [Green Version]
- Selvakumar, P.; Badgeley, A.; Murphy, P.; Anwar, H.; Sharma, U.; Lawrence, K.; Lakshmikuttyamma, A. Flavonoids and other polyphenols act as epigenetic modifiers in breast cancer. Nutrients 2020, 12, 761. [Google Scholar] [CrossRef] [Green Version]
- Cueva, C.; Gil-Sánchez, I.; Ayuda-Durán, B.; González-Manzano, S.; González-Paramás, A.M.; Santos-Buelga, C.; Bartolomé, B.; Moreno-Arribas, M. An integrated view of the effects of wine polyphenols and their relevant metabolites on gut and host health. Molecules 2017, 22, 99. [Google Scholar] [CrossRef]
- Quiñones, M.; Miguel, M.; Aleixandre, A. The polyphenols, naturally occurring compounds with beneficial effects on cardiovascular disease. Nutr. Hosp. 2012, 27, 76–89. [Google Scholar]
- Santos-Buelga, C.; González-Paramás, A.M.; Oludemi, T.; Ayuda-Durán, B.; González-Manzano, S. Plant phenolics as functional food ingredients. Adv. Food Nutr. Res. 2019, 90, 183–257. [Google Scholar] [PubMed]
- Saini, R.K.; Keum, Y.-S. Omega-3 and omega-6 polyunsaturated fatty acids: Dietary sources, metabolism, and significance—A review. Life Sci. 2018, 203, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Czumaj, A.; Śledziński, T. Biological role of unsaturated fatty acid desaturases in health and disease. Nutrients 2020, 12, 356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harayama, T.; Shimizu, T. Roles of polyunsaturated fatty acids, from mediators to membranes. J. Lipid Res. 2020, 61, 1150–1160. [Google Scholar] [CrossRef]
- Román, G.; Jackson, R.; Gadhia, R.; Román, A.; Reis, J. Mediterranean diet: The role of long-chain ω-3 fatty acids in fish; polyphenols in fruits, vegetables, cereals, coffee, tea, cacao and wine; probiotics and vitamins in prevention of stroke, age-related cognitive decline, and Alzheimer disease. Rev. Neurol. 2019, 175, 724–741. [Google Scholar] [CrossRef] [PubMed]
- Gorzynik-Debicka, M.; Przychodzen, P.; Cappello, F.; Kuban-Jankowska, A.; Marino Gammazza, A.; Knap, N.; Wozniak, M.; Gorska-Ponikowska, M. Potential Health Benefits of Olive Oil and Plant Polyphenols. Int. J. Mol. Sci. 2018, 19, 686. [Google Scholar] [CrossRef] [Green Version]
- Gutierrez, S.; Svahn, S.L.; Johansson, M.E. Effects of Omega-3 Fatty Acids on Immune Cells. Int J Mol Sci 2019, 20, 5028. [Google Scholar] [CrossRef] [Green Version]
- Gasparyan, A.Y.; Ayvazyan, L.; Mukanova, U.; Yessirkepov, M.; Kitas, G.D. The platelet-to-lymphocyte ratio as an inflammatory marker in rheumatic diseases. Ann. Lab. Med. 2019, 39, 345–357. [Google Scholar] [CrossRef] [Green Version]
- Korniluk, A.; Koper-Lenkiewicz, O.M.; Kaminska, J.; Kemona, H.; Dymicka-Piekarska, V. Mean Platelet Volume (MPV): New Perspectives for an Old Marker in the Course and Prognosis of Inflammatory Conditions. Mediat. Inflamm. 2019, 2019, 9213074. [Google Scholar] [CrossRef]
- Semple, J.W.; Italiano, J.E.; Freedman, J. Platelets and the immune continuum. Nat. Rev. Immunol. 2011, 11, 264–274. [Google Scholar] [CrossRef]
- Chen, X.; Shao, M.; Zhang, T.; Zhang, W.; Meng, Y.; Zhang, H.; Hai, H.; Li, G. Prognostic value of the combination of GRACE risk score and mean platelet volume to lymphocyte count ratio in patients with ST-segment elevation myocardial infarction after percutaneous coronary intervention. Exp. Ther. Med. 2020, 19, 3664–3674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kocak, M.Z.; Aktas, G.; Erkus, E.; Duman, T.T.; Atak, B.M.; Savli, H. Mean platelet volume to lymphocyte ratio as a novel marker for diabetic nephropathy. J. Coll. Physicians Surg. Pak. 2018, 28, 844–847. [Google Scholar] [CrossRef] [PubMed]
- Onalan, E.; Gozel, N.; Donder, E. Can hematological parameters in type 2 diabetes predict microvascular complication development? Pak. J. Med. Sci. 2019, 35, 1511. [Google Scholar] [CrossRef] [Green Version]
- Abdallah, A.I.; Abdelaziz, A.A.; El-Sayed, E.-S.E.-M.; Emran, T.M. Study of neutrophil lymphocyte ratio (NLR) and platelet lymphocyte ratio (PLR) as a predictor inflammatory marker for diabetic nephropathy in type 2 diabetic patients. Egypt. J. Hosp. Med. 2018, 72, 4800–4807. [Google Scholar] [CrossRef]
- Wang, J.-R.; Chen, Z.; Yang, K.; Yang, H.-J.; Tao, W.-Y.; Li, Y.-P.; Jiang, Z.-J.; Bai, C.-F.; Yin, Y.-C.; Duan, J.-M. Association between neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and diabetic retinopathy among diabetic patients without a related family history. Diabetol. Metab. Syndr. 2020, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Care, D. Outcomes: Standards of Medical Care in Diabetesd2021. Diabetes Care 2021, 44, S53. [Google Scholar]
- Garcia-Molina, L.; Lewis-Mikhael, A.-M.; Riquelme-Gallego, B.; Cano-Ibáñez, N.; Oliveras-Lopez, M.-J.; Bueno-Cavanillas, A. Improving type 2 diabetes mellitus glycaemic control through lifestyle modification implementing diet intervention: A systematic review and meta-analysis. Eur. J. Nutr. 2020, 59, 1313–1328. [Google Scholar] [CrossRef]
- Huang, X.-L.; Pan, J.-H.; Chen, D.; Chen, J.; Chen, F.; Hu, T.-T. Efficacy of lifestyle interventions in patients with type 2 diabetes: A systematic review and meta-analysis. Eur. J. Intern. Med. 2016, 27, 37–47. [Google Scholar] [CrossRef]
- Schlesinger, S.; Neuenschwander, M.; Ballon, A.; Nothlings, U.; Barbaresko, J. Adherence to healthy lifestyles and incidence of diabetes and mortality among individuals with diabetes: A systematic review and meta-analysis of prospective studies. J. Epidemiol. Community Health 2020, 74, 481–487. [Google Scholar] [CrossRef]
- Raparelli, V.; Romiti, G.F.; Spugnardi, V.; Borgi, M.; Cangemi, R.; Basili, S.; Proietti, M.; The Eva Collaborative, G. Gender-Related Determinants of Adherence to the Mediterranean Diet in Adults with Ischemic Heart Disease. Nutrients 2020, 12, 759. [Google Scholar] [CrossRef] [Green Version]
- Esposito, K.; Maiorino, M.I.; Petrizzo, M.; Bellastella, G.; Giugliano, D. The effects of a Mediterranean diet on the need for diabetes drugs and remission of newly diagnosed type 2 diabetes: Follow-up of a randomized trial. Diabetes Care 2014, 37, 1824–1830. [Google Scholar] [CrossRef] [Green Version]
- Grosso, G.; Stepaniak, U.; Micek, A.; Kozela, M.; Stefler, D.; Bobak, M.; Pajak, A. Dietary polyphenol intake and risk of type 2 diabetes in the Polish arm of the Health, Alcohol and Psychosocial factors in Eastern Europe (HAPIEE) study. Br. J. Nutr. 2017, 118, 60–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grosso, G.; Stepaniak, U.; Micek, A.; Stefler, D.; Bobak, M.; Pająk, A. Dietary polyphenols are inversely associated with metabolic syndrome in Polish adults of the HAPIEE study. Eur. J. Nutr. 2017, 56, 1409–1420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, A.; Betts, N.M.; Leyva, M.J.; Fu, D.; Aston, C.E.; Lyons, T.J. Acute cocoa supplementation increases postprandial HDL cholesterol and insulin in obese adults with type 2 diabetes after consumption of a high-fat breakfast. J. Nutr. 2015, 145, 2325–2332. [Google Scholar] [CrossRef] [PubMed]
- Blostein-Fujii, A.; DiSilvestro, R.A.; Frid, D.; Katz, C. Short term citrus flavonoid supplementation of type II diabetic women: No effect on lipoprotein oxidation tendencies. Free. Radic. Res. 1999, 30, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Braxas, H.; Rafraf, M.; Hasanabad, S.K.; Jafarabadi, M.A. Effectiveness of genistein supplementation on metabolic factors and antioxidant status in postmenopausal women with type 2 diabetes mellitus. Can. J. Diabetes 2019, 43, 490–497. [Google Scholar] [CrossRef]
- Curtis, P.J.; Sampson, M.; Potter, J.; Dhatariya, K.; Kroon, P.A.; Cassidy, A. Chronic ingestion of flavan-3-ols and isoflavones improves insulin sensitivity and lipoprotein status and attenuates estimated 10-year CVD risk in medicated postmenopausal women with type 2 diabetes: A 1-year, double-blind, randomized, controlled trial. Diabetes Care 2012, 35, 226–232. [Google Scholar] [CrossRef] [Green Version]
- Dicks, L.; Kirch, N.; Gronwald, D.; Wernken, K.; Zimmermann, B.F.; Helfrich, H.-P.; Ellinger, S. Regular intake of a usual serving size of flavanol-rich cocoa powder does not affect cardiometabolic parameters in stably treated patients with type 2 diabetes and hypertension—A double-blinded, randomized, placebo-controlled trial. Nutrients 2018, 10, 1435. [Google Scholar] [CrossRef] [Green Version]
- Ebrahimpour-Koujan, S.; Gargari, B.P.; Mobasseri, M.; Valizadeh, H.; Asghari-Jafarabadi, M. Lower glycemic indices and lipid profile among type 2 diabetes mellitus patients who received novel dose of Silybum marianum (L.) Gaertn.(silymarin) extract supplement: A Triple-blinded randomized controlled clinical trial. Phytomedicine 2018, 44, 39–44. [Google Scholar] [CrossRef]
- Liu, X.; Zhou, H.-J.; Rohdewald, P. French maritime pine bark extract Pycnogenol dose-dependently lowers glucose in type 2 diabetic patients. Diabetes Care 2004, 27, 839. [Google Scholar] [CrossRef] [Green Version]
- Palma-Duran, S.A.; Vlassopoulos, A.; Lean, M.; Govan, L.; Combet, E. Nutritional intervention and impact of polyphenol on glycohemoglobin (HbA1c) in non-diabetic and type 2 diabetic subjects: Systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2017, 57, 975–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raimundo, A.F.; Félix, F.; Andrade, R.; García-Conesa, M.-T.; González-Sarrías, A.; Gilsa-Lopes, J.; Raimundo, A.; Ribeiro, R.; Rodriguez-Mateos, A.; Santos, C.N. Combined effect of interventions with pure or enriched mixtures of (poly) phenols and anti-diabetic medication in type 2 diabetes management: A meta-analysis of randomized controlled human trials. Eur. J. Nutr. 2020, 59, 1329–1343. [Google Scholar] [CrossRef] [PubMed]
- Valensi, P.; Behar, A.; De Champvallins, M.; Attalah, M.; Boulakia, F.; Attali, J.R. Effects of a purified micronized flavonoid fraction on capillary filtration in diabetic patients. Diabet. Med. 1996, 13, 882–888. [Google Scholar] [CrossRef]
- Voroneanu, L.; Nistor, I.; Dumea, R.; Apetrii, M.; Covic, A. Silymarin in type 2 diabetes mellitus: A systematic review and meta-analysis of randomized controlled trials. J. Diabetes Res. 2016, 2016, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitale, M.; Vaccaro, O.; Masulli, M.; Bonora, E.; Del Prato, S.; Giorda, C.B.; Nicolucci, A.; Squatrito, S.; Auciello, S.; Babini, A.C. Polyphenol intake and cardiovascular risk factors in a population with type 2 diabetes: The TOSCA. IT study. Clin. Nutr. 2017, 36, 1686–1692. [Google Scholar] [CrossRef]
- Faghihzadeh, F.; Adibi, P.; Rafiei, R.; Hekmatdoost, A. Resveratrol supplementation improves inflammatory biomarkers in patients with nonalcoholic fatty liver disease. Nutr. Res. 2014, 34, 837–843. [Google Scholar] [CrossRef]
- Lockyer, S.; Rowland, I.; Spencer, J.P.E.; Yaqoob, P.; Stonehouse, W. Impact of phenolic-rich olive leaf extract on blood pressure, plasma lipids and inflammatory markers: A randomised controlled trial. Eur. J. Nutr. 2017, 56, 1421–1432. [Google Scholar] [CrossRef] [Green Version]
- Rangel-Huerta, O.D.; Aguilera, C.M.; Martin, M.V.; Soto, M.J.; Rico, M.C.; Vallejo, F.; Tomas-Barberan, F.; Perez-de-la-Cruz, A.J.; Gil, A.; Mesa, M.D. Normal or high polyphenol concentration in orange juice affects antioxidant activity, blood pressure, and body weight in obese or overweight adults. J. Nutr. 2015, 145, 1808–1816. [Google Scholar] [CrossRef] [Green Version]
- Al-Aubaidy, H.A.; Dayan, A.; Deseo, M.A.; Itsiopoulos, C.; Jamil, D.; Hadi, N.R.; Thomas, C.J. Twelve-Week Mediterranean Diet Intervention Increases Citrus Bioflavonoid Levels and Reduces Inflammation in People with Type 2 Diabetes Mellitus. Nutrients 2021, 13, 1133. [Google Scholar] [CrossRef]
- Asadi, A.; Shidfar, F.; Safari, M.; Hosseini, A.F.; Fallah Huseini, H.; Heidari, I.; Rajab, A. Efficacy of Melissa officinalis L.(lemon balm) extract on glycemic control and cardiovascular risk factors in individuals with type 2 diabetes: A randomized, double-blind, clinical trial. Phytother. Res. 2019, 33, 651–659. [Google Scholar] [CrossRef]
- Davis, D.W.; Tallent, R.; Navalta, J.W.; Salazar, A.; Lyons, T.J.; Basu, A. Effects of acute cocoa supplementation on postprandial apolipoproteins, lipoprotein subclasses, and inflammatory biomarkers in adults with type 2 diabetes after a high-fat meal. Nutrients 2020, 12, 1902. [Google Scholar] [CrossRef] [PubMed]
- Homayouni, F.; Haidari, F.; Hedayati, M.; Zakerkish, M.; Ahmadi, K. Blood pressure lowering and anti-inflammatory effects of hesperidin in type 2 diabetes; a randomized double-blind controlled clinical trial. Phytother. Res. 2018, 32, 1073–1079. [Google Scholar] [CrossRef] [PubMed]
- Kar, P.; Laight, D.; Rooprai, H.; Shaw, K.; Cummings, M. Effects of grape seed extract in Type 2 diabetic subjects at high cardiovascular risk: A double blind randomized placebo controlled trial examining metabolic markers, vascular tone, inflammation, oxidative stress and insulin sensitivity. Diabet. Med. 2009, 26, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Pastor, R.F.; Repetto, M.G.; Lairion, F.; Lazarowski, A.; Merelli, A.; Manfredi Carabetti, Z.; Pastor, I.; Pastor, E.; Iermoli, L.V.; Bavasso, C.A. Supplementation with Resveratrol, Piperine and Alpha-Tocopherol Decreases Chronic Inflammation in a Cluster of Older Adults with Metabolic Syndrome. Nutrients 2020, 12, 3149. [Google Scholar] [CrossRef]
- Chen, M.; Zhu, Y.; Wang, J.; Wang, G.; Wu, Y. The Predictive Value of Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio Levels of Diabetic Peripheral Neuropathy. J. Pain Res. 2021, 14, 2049. [Google Scholar] [CrossRef]
- Liu, N.; Sheng, J.; Pan, T.; Wang, Y. Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio are Associated with Lower Extremity Vascular Lesions in Chinese Patients with Type 2 Diabetes. Clin. Lab. 2019, 65, 65. [Google Scholar] [CrossRef]
- Mineoka, Y.; Ishii, M.; Hashimoto, Y.; Yamashita, A.; Nakamura, N.; Fukui, M. Platelet to lymphocyte ratio correlates with diabetic foot risk and foot ulcer in patients with type 2 diabetes. Endocr. J. 2019, 66, 905–913. [Google Scholar] [CrossRef] [Green Version]
- Liese, A.D.; Ma, X.; Ma, X.; Mittleman, M.A.; The, N.S.; Standiford, D.A.; Lawrence, J.M.; Pihoker, C.; Marcovina, S.M.; Mayer-Davis, E.J. Dietary quality and markers of inflammation: No association in youth with type 1 diabetes. J. Diabetes Its Complicat. 2018, 32, 179–184. [Google Scholar] [CrossRef]
- Bjermo, H.; Iggman, D.; Kullberg, J.; Dahlman, I.; Johansson, L.; Persson, L.; Berglund, J.; Pulkki, K.; Basu, S.; Uusitupa, M. Effects of n-6 PUFAs compared with SFAs on liver fat, lipoproteins, and inflammation in abdominal obesity: A randomized controlled trial. Am. J. Clin. Nutr. 2012, 95, 1003–1012. [Google Scholar] [CrossRef] [Green Version]
- Natto, Z.S.; Yaghmoor, W.; Alshaeri, H.K.; Van Dyke, T.E. Omega-3 fatty acids effects on inflammatory biomarkers and lipid profiles among diabetic and cardiovascular disease patients: A systematic review and meta-analysis. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Wei, Y.; Meng, Y.; Li, N.; Wang, Q.; Chen, L. The effects of low-ratio n-6/n-3 PUFA on biomarkers of inflammation: A systematic review and meta-analysis. Food Funct. 2021, 12, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Heilbronn, L.K.; Noakes, M.; Clifton, P.M. Effect of energy restriction, weight loss, and diet composition on plasma lipids and glucose in patients with type 2 diabetes. Diabetes Care 1999, 22, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Johns, I.; Frost, G.; Dornhorst, A. Increasing the proportion of plasma MUFA, as a result of dietary intervention, is associated with a modest improvement in insulin sensitivity. J. Nutr. Sci. 2020, 9, e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Männistö, S.; Kontto, J.; Kataja-Tuomola, M.; Albanes, D.; Virtamo, J. High processed meat consumption is a risk factor of type 2 diabetes in the Alpha-Tocopherol, Beta-Carotene Cancer Prevention study. Br. J. Nutr. 2010, 103, 1817–1822. [Google Scholar] [CrossRef]
- Murphy, A.M.; Smith, C.E.; Murphy, L.M.; Follis, J.L.; Tanaka, T.; Richardson, K.; Noordam, R.; Lemaitre, R.N.; Kähönen, M.; Dupuis, J. Potential Interplay between Dietary Saturated Fats and Genetic Variants of the NLRP3 Inflammasome to Modulate Insulin Resistance and Diabetes Risk: Insights from a Meta-Analysis of 19 005 Individuals. Mol. Nutr. Food Res. 2019, 63, 1900226. [Google Scholar] [CrossRef] [Green Version]
- Miller, M.; Sorkin, J.D.; Mastella, L.; Sutherland, A.; Rhyne, J.; Donnelly, P.; Simpson, K.; Goldberg, A.P. Poly is more effective than monounsaturated fat for dietary management in the metabolic syndrome: The muffin study. J. Clin. Lipidol. 2016, 10, 996–1003. [Google Scholar] [CrossRef] [Green Version]
- Brown, T.J.; Brainard, J.; Song, F.; Wang, X.; Abdelhamid, A.; Hooper, L. Omega-3, omega-6, and total dietary polyunsaturated fat for prevention and treatment of type 2 diabetes mellitus: Systematic review and meta-analysis of randomised controlled trials. BMJ 2019, 366, l4697. [Google Scholar] [CrossRef] [Green Version]
- Golzari, M.H.; Javanbakht, M.H.; Ghaedi, E.; Mohammadi, H.; Djalali, M. Effect of Eicosapentaenoic acid (EPA) supplementation on cardiovascular markers in patients with type 2 diabetes mellitus: A randomized, double-blind, placebo-controlled trial. Diabetes Metab. Syndr. Clin. Res. Rev. 2018, 12, 411–415. [Google Scholar] [CrossRef]
- Fuller, N.R.; Caterson, I.D.; Sainsbury, A.; Denyer, G.; Fong, M.; Gerofi, J.; Baqleh, K.; Williams, K.H.; Lau, N.S.; Markovic, T.P. The effect of a high-egg diet on cardiovascular risk factors in people with type 2 diabetes: The Diabetes and Egg (DIABEGG) study—A 3-mo randomized controlled trial. Am. J. Clin. Nutr. 2015, 101, 705–713. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Demographic Variables | Polyphenol Intake | Omega 3 Intake | ||
|---|---|---|---|---|
| low (n = 64) | high (n = 65) | low (n = 64) | high (n = 65) | |
| gender: female n (%) male n (%) | 36 (56) 28 (44) | 44(68) 21 (32) | 39 (61) 25 (39) | 41 (63) 24 (37) |
| physical activity: low n (%) medium n (%) high n (%) | 39 (61) 20 (31) 5 (8) | 40 (62) 19 (29) 6 (9) | 41 (64) 15 (23) 8 (13) | 38 (58) 24 (37) 3 (5) |
| duration of diabetes (years] | 5 (0; 8) | 3 (0; 10) | 5 (0; 9) | 3 (0;9) |
| following of diabetic diet n (%) | 47 (73) | 47 (72) | 45 (70) | 49 (75) |
| familial diabetes n (%) | 25 (39) | 35 (54) | 24 (37) | 30 (46) |
| Polyphenol Intake | PUFAs Omega 3 Intake | |||
|---|---|---|---|---|
| low | high | low | high | |
| polyphenols (mg/day) | 958 (503; 1410) | 2076 (1845; 2672) | 1410 (585; 1878) | 1817 (1424; 2449) * |
| flavonoids (mg/day) | 406 (179; 694) | 1101 (946; 1301) * | 773 (285; 1021) | 936 (595; 1220) * |
| flavan-3-ols (mg/day) | 225 (64; 390) | 648 (524; 783) * | 442 (102; 622) | 432 (270; 670) |
| phenolic acids (mg/day) | 235 (132; 353) | 452 (285; 704) * | 244 (147; 357) | 413 (280; 745) * |
| stilbenes (mg/day) | 0.1 (0.02; 0.52) | 0.54 (0.07; 1.05) * | 0.08 (0.02; 0.62) | 0.41 (0.09; 0.80) * |
| lignans (mg/day) | 11.9 (6.9; 23.5) | 23.9 (15.4; 44.7) * | 9.7 (6.5; 21.4) | 25.9 (16.4; 46.2) * |
| SFAs (g/day) | 24.0 (13.7; 30.4) | 28.2 (22.3; 38.3) * | 20.8 (12.9; 28.9) | 29.4 (24.3; 40.3) * |
| MUFAs (g/day) | 33.5 (17.9; 45.7) | 38.3 (22.4; 52.1) | 22.4 (16.9; 36.4) | 44.4 (36.4; 61.4) * |
| PUFAs (g/day) | 14.1 (7.9; 23.9) | 18.4 (10.6; 27.4) | 9.3 (5.9; 14.2) | 24.5 (18.6; 31.9) * |
| PUFAs omega 3 (g/day) | 1.87 (1.18; 3.42) | 2.98 (1.90; 4.74) * | 1.37 (1.03; 1.87) | 3.94 (3.08; 6.51) |
| PUFAs omega 6 (g/day) | 11.5 (6.6; 17.7) | 14.8 (8.9; 21.3) | 7.6 (4.4; 12.3) | 18.9 (14.3; 23.7) * |
| EPA + DHA (g/day) | 0.29 (0.17; 0.65) | 0.37 (0.23; 0.83) | 0.23 (0.11; 0.35) | 0.65 (0.29; 1.32) * |
| cholesterol (mg/day) | 221 (127; 313) | 310 (207; 468) * | 196 (126; 311) | 311 (248; 440) * |
| Polyphenols | PUFAs Omega 3 | |||
|---|---|---|---|---|
| low | high | low | high | |
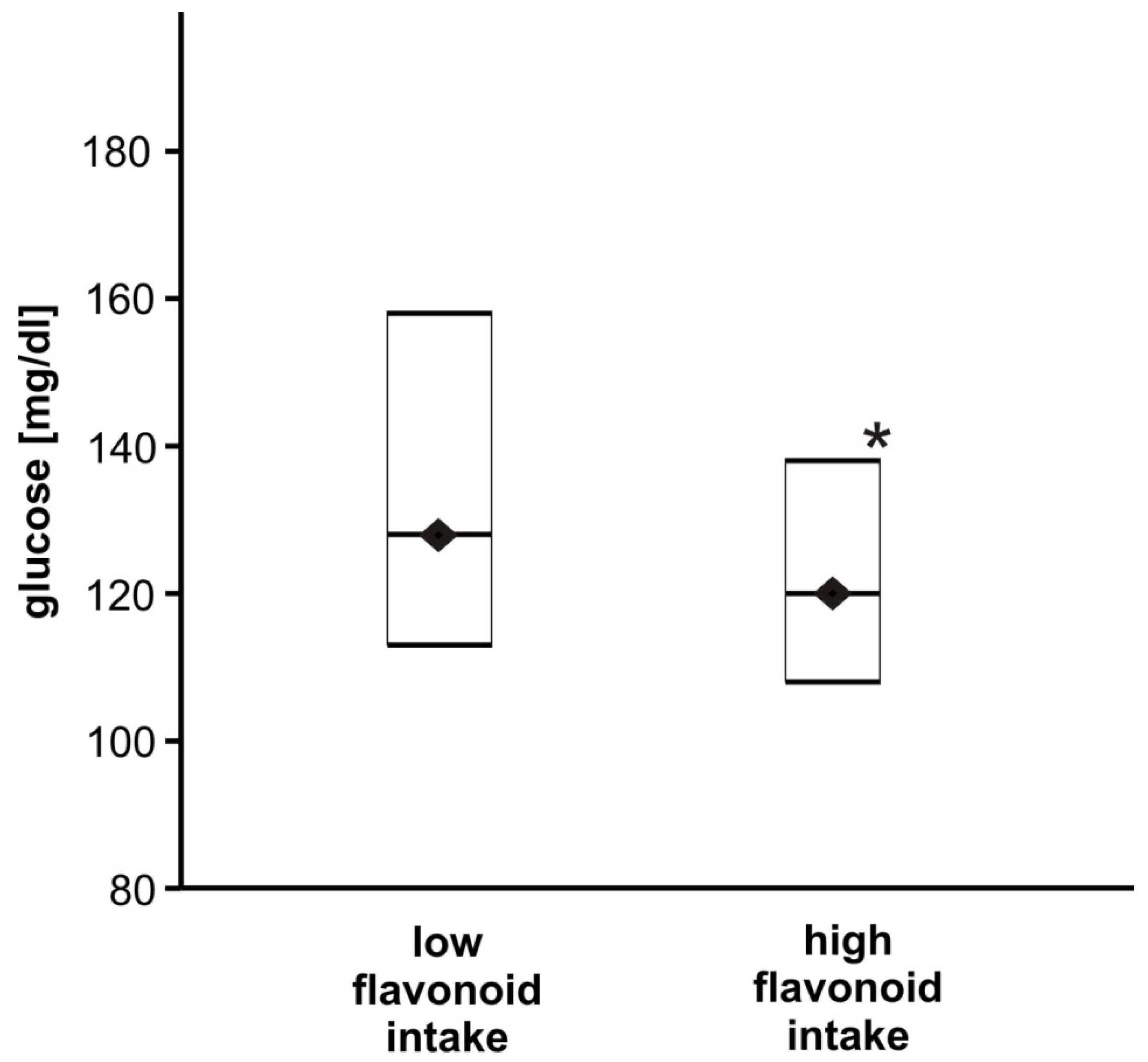
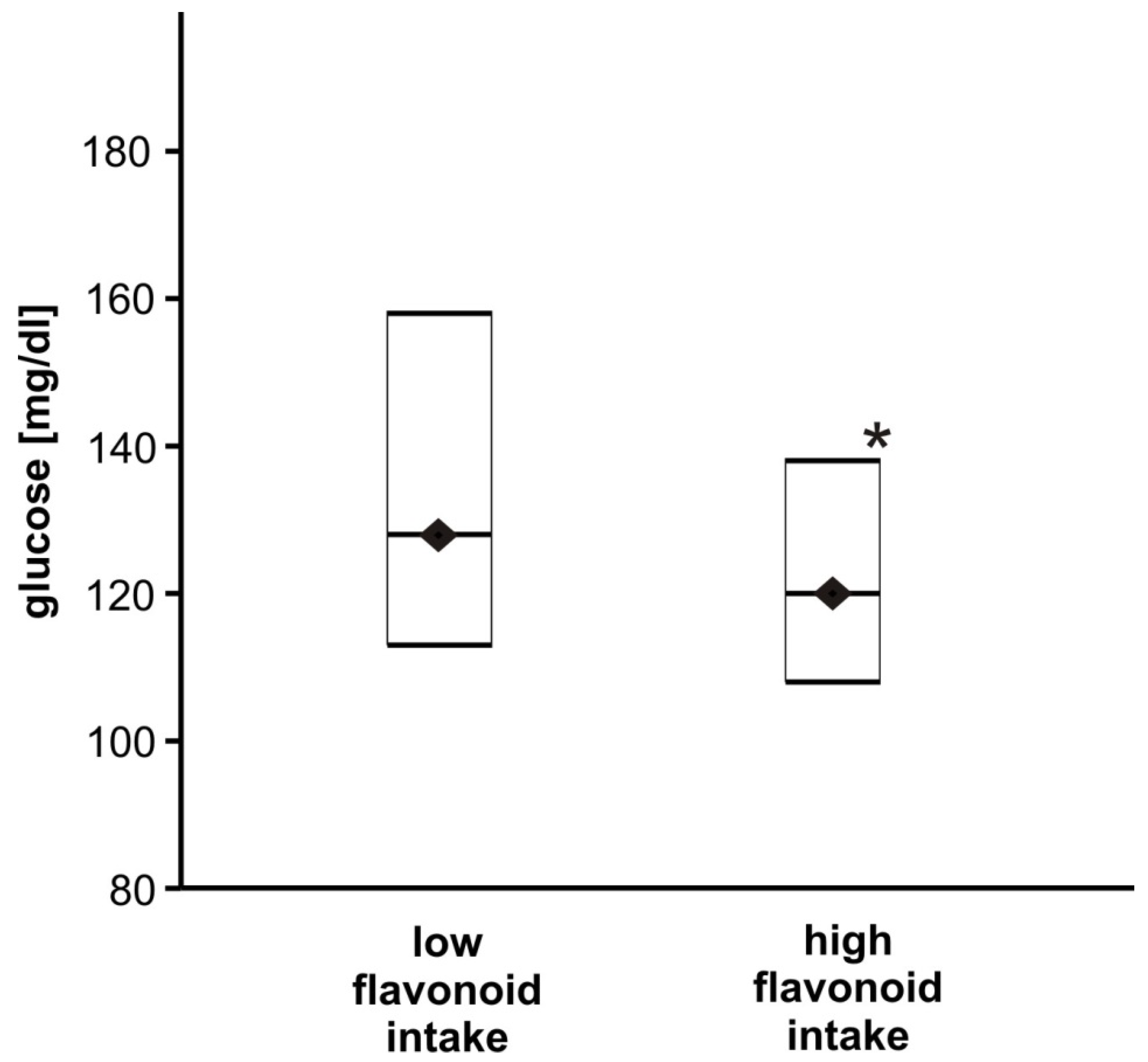
| FG (mg/dL) | 127 (113; 155) | 119 (108; 138) | 122 (112; 157) | 121 (108; 138) |
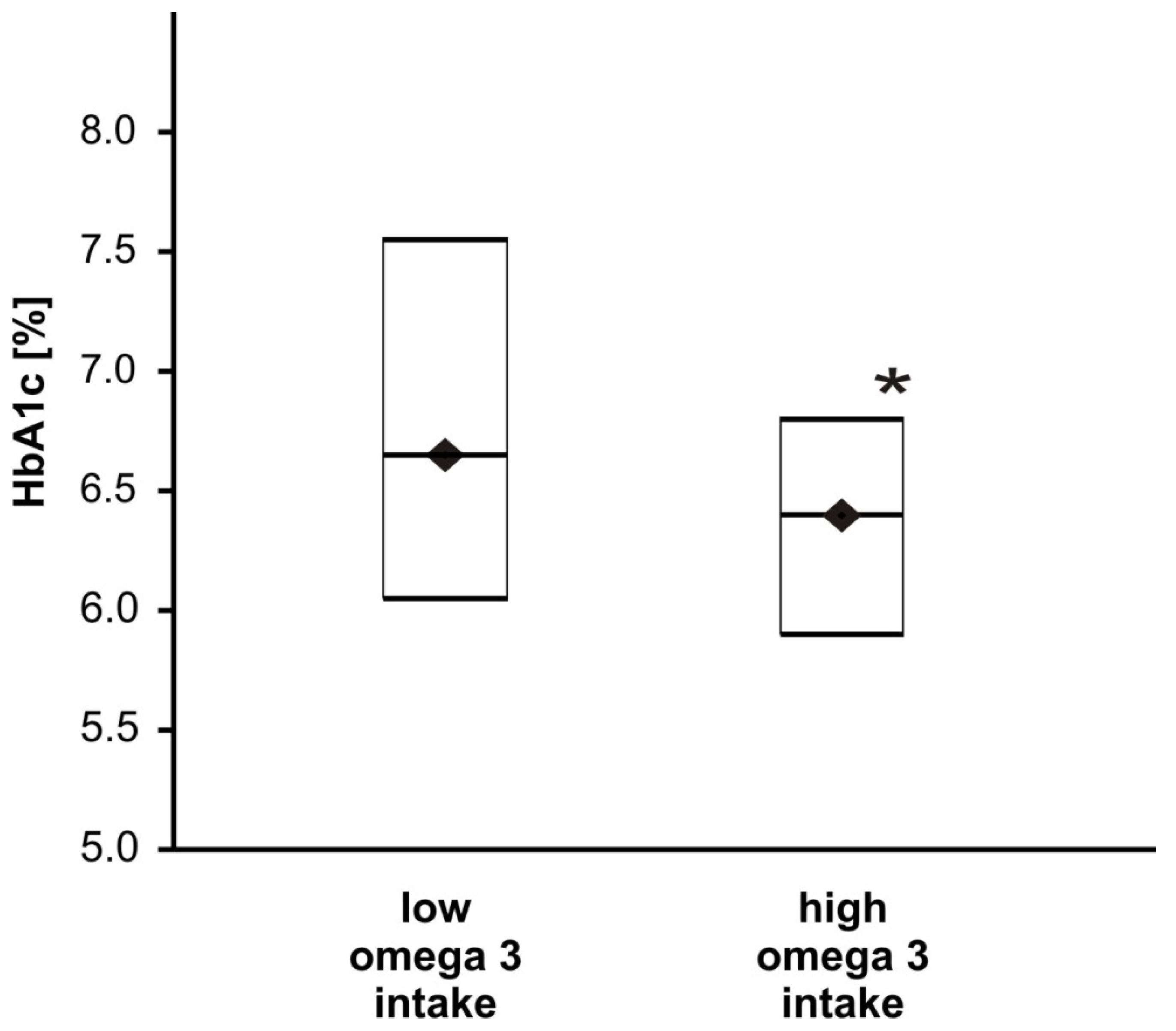
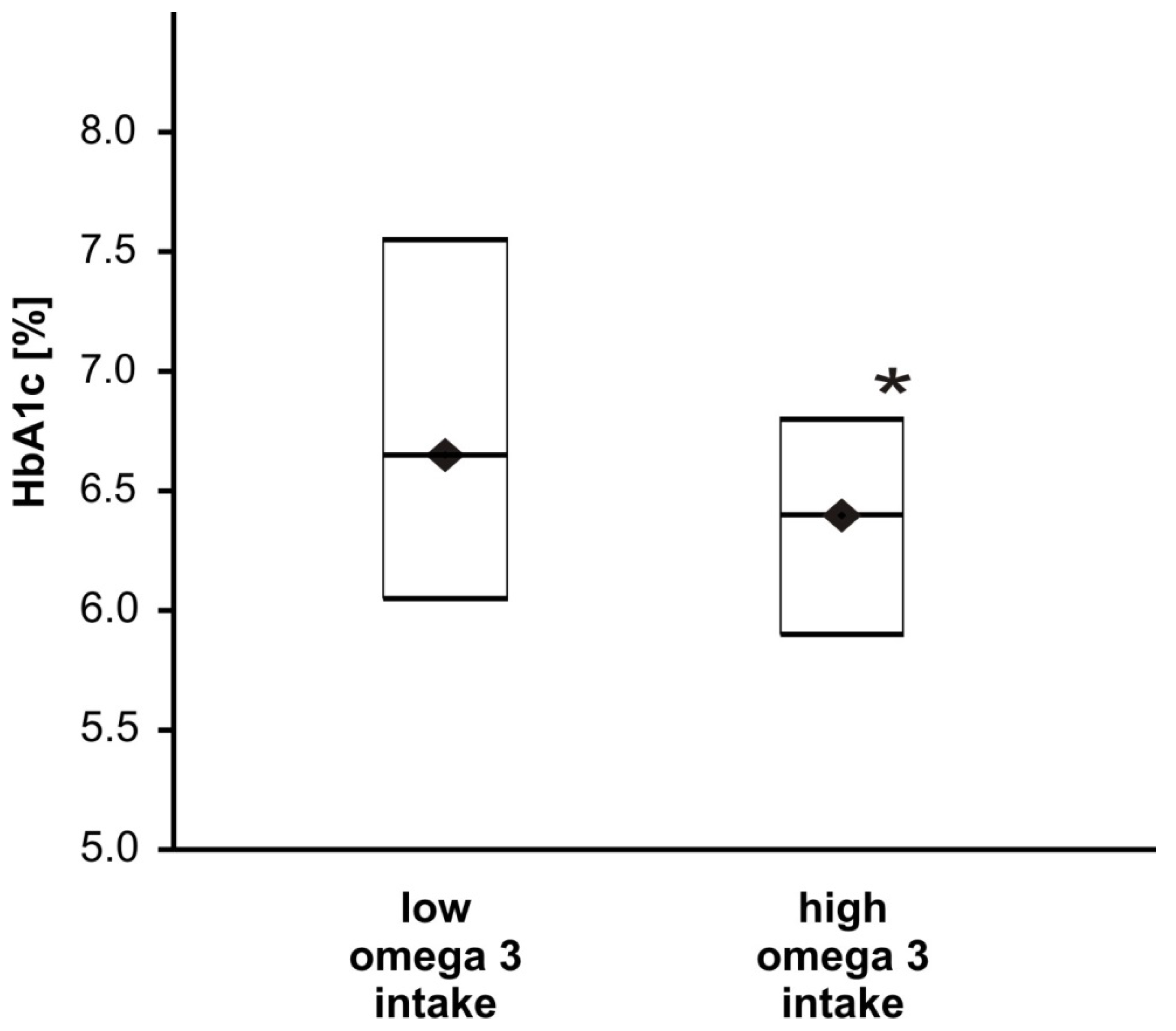
| HbA1c (%) | 6.5 (5.9; 7.3) | 6.4 (6.0; 6.9) | 6.6 (6.0; 7.5) | 6.4 (5.9; 6.8) * |
| TCH (mg/dL) | 180 (144; 207) | 185 (149; 213) | 185 (152; 216) | 177 (145; 201) |
| LDL-TCH (mg/dL) | 100 (73; 132) | 103 (79; 124) | 101 (75; 125) | 102 (76; 131) |
| HDL-CH (mg/dL) | 47 (41; 55) | 49 (40; 61) | 49 (40; 55) | 49 (40; 61) |
| TG (mg/dL) | 141 (104; 201) | 138 (103; 178) | 138 (108; 199) | 139 (101; 174) |
| PLR | 114 (91; 139) | 106 (85; 142) | 107 (82; 131) | 119 (89; 142) |
| NLR | 2.2 (1.6; 2.8) | 2.2 (1.6; 2.9) | 2.2 (1.5; 2.9) | 2.2 (1.6; 2.9) |
| MPVLR | 5.0 (4.1; 6.2) | 4.6 (4.0; 5.9) | 5.2 (4.0; 6.0) | 4.8 (4.1; 6.3) |
| BMI (kg/m2) | 31.2 (28.3; 35.2) | 34.0 (27.1; 38.1) | 33.0 (28.1; 35.9) | 32.0 (28.2; 36.9) |
| waist circumference (cm) | 108 (102; 115) | 111 (101; 119) | 110 (101; 118) | 108 (102; 117) |
| WHR | 0.96 (0.91; 1.01) | 0.97 (0.92; 1.02) | 0.97 (0.91; 1.02) | 0.96 (0.92;1.02) |
| HbA1c | Glycaemia | |
|---|---|---|
| Total polyphenols | −0.045993 | −0.139093 |
| Flavonoids | −0.078909 | −0.143564 |
| Flawan-3-ols | −0.010229 | −0.110597 |
| Phenolic acids | −0.075401 | −0.105316 |
| Stilbenes | −0.149940 | −0.108842 |
| Lignans | −0.076959 | −0.054942 |
| MUFAs | −0.065301 | 0.016014 |
| Total PUFAs | −0.082863 | −0.075725 |
| PUFAs omega 3 | −0.130564 | −0.111073 |
| PUFAs omega 6 | −0.075280 | −0.070239 |
| EPA + DHA | −0.188344 * | −0.245573 * |
| Omega 6/3 proportion | 0.121846 | 0.138595 |
| Cholesterol | −0.024314 | 0.068974 |
| Beta | SE | p | |
|---|---|---|---|
| HbA1c (%) Model 1 Model 2 Model 3 Model 4 | 0.000580 0.000569 0.000466 0.000586 | 0.000254 0.000026 0.000241 0.000257 | 0.024 * 0.028 * 0.055 0.024 * |
| FG (mg/mL) Model 1 Model 2 Model 3 Model 4 | −0.000038 −0.000039 −0.000026 −0.000041 | 0.000032 0.000032 0.000031 0.000032 | 0.243 0.224 0.399 0.205 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosmalski, M.; Pękala-Wojciechowska, A.; Sut, A.; Pietras, T.; Luzak, B. Dietary Intake of Polyphenols or Polyunsaturated Fatty Acids and Its Relationship with Metabolic and Inflammatory State in Patients with Type 2 Diabetes Mellitus. Nutrients 2022, 14, 1083. https://doi.org/10.3390/nu14051083
Kosmalski M, Pękala-Wojciechowska A, Sut A, Pietras T, Luzak B. Dietary Intake of Polyphenols or Polyunsaturated Fatty Acids and Its Relationship with Metabolic and Inflammatory State in Patients with Type 2 Diabetes Mellitus. Nutrients. 2022; 14(5):1083. https://doi.org/10.3390/nu14051083
Chicago/Turabian StyleKosmalski, Marcin, Anna Pękala-Wojciechowska, Agnieszka Sut, Tadeusz Pietras, and Bogusława Luzak. 2022. "Dietary Intake of Polyphenols or Polyunsaturated Fatty Acids and Its Relationship with Metabolic and Inflammatory State in Patients with Type 2 Diabetes Mellitus" Nutrients 14, no. 5: 1083. https://doi.org/10.3390/nu14051083
APA StyleKosmalski, M., Pękala-Wojciechowska, A., Sut, A., Pietras, T., & Luzak, B. (2022). Dietary Intake of Polyphenols or Polyunsaturated Fatty Acids and Its Relationship with Metabolic and Inflammatory State in Patients with Type 2 Diabetes Mellitus. Nutrients, 14(5), 1083. https://doi.org/10.3390/nu14051083