
Ketoanalogue Supplementation in Patients with Non-Dialysis Diabetic Kidney Disease: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Quality Assessment
2.3. Statistical Analyses
3. Results
3.1. Literature Search and Study Characteristics
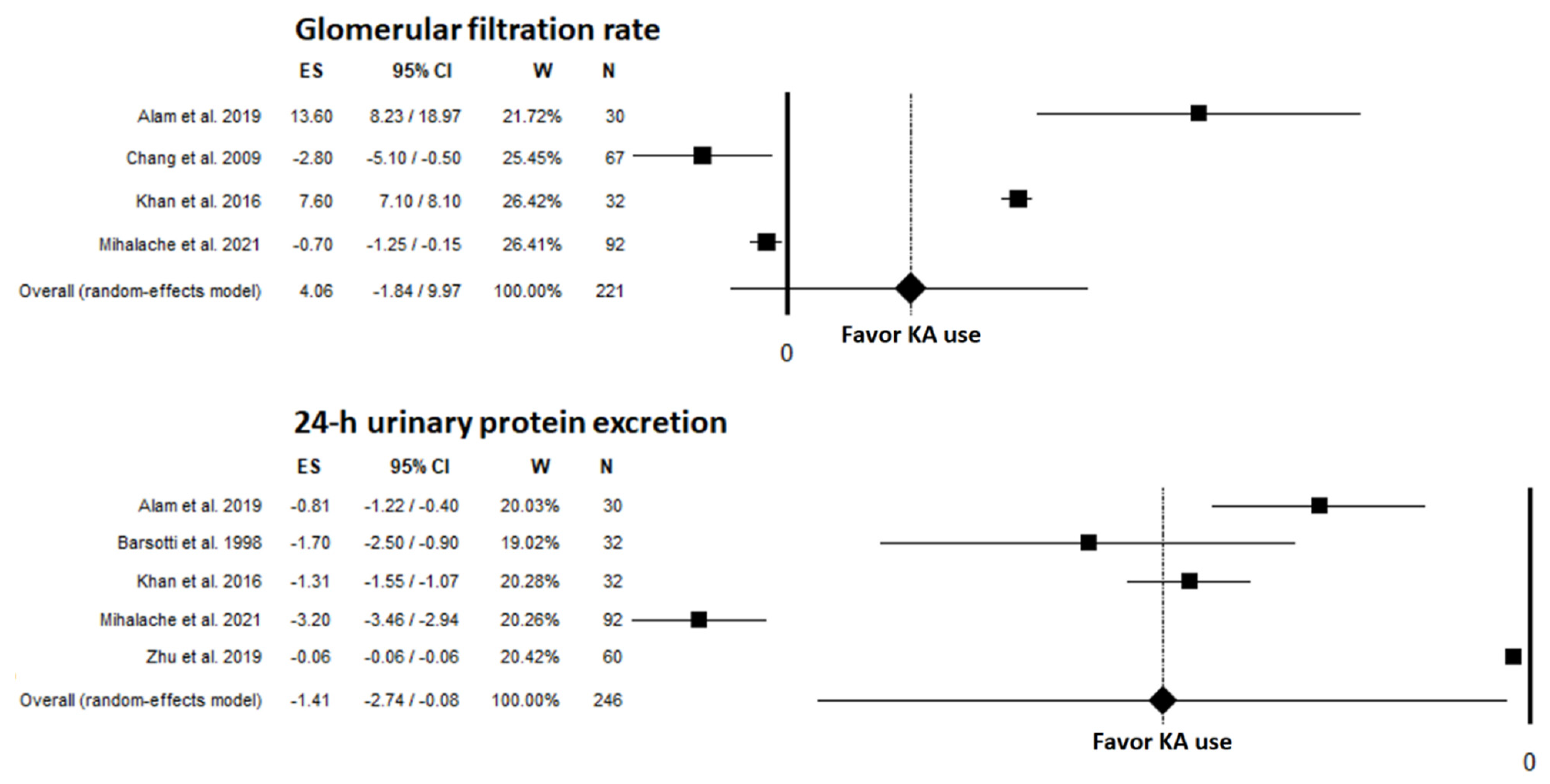
3.2. Renal Outcomes
3.3. Metabolic and Clinical Outcomes
3.4. Nutritional Outcomes
3.5. Safety Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alicic, R.Z.; Rooney, M.T.; Tuttle, K.R. Diabetic kidney disease: Challenges, progress, and possibilities. Clin. J. Am. Soc. Nephrol. 2017, 12, 2032–2045. [Google Scholar] [CrossRef] [PubMed]
- Bellizzi, V.; Calella, P.; Hernández, J.N.; González, V.F.; Lira, S.M.; Torraca, S.; Arronte, R.U.; Cirillo, P.; Minutolo, R.; Cárdenas, R.A.M. Safety and effectiveness of low-protein diet supplemented with ketoacids in diabetic patients with chronic kidney disease. BMC Nephrol. 2018, 19, 110. [Google Scholar] [CrossRef]
- Umanath, K.; Lewis, J.B. Update on Diabetic Nephropathy: Core Curriculum 2018. Am. J. Kidney Dis. 2018, 71, 884–895. [Google Scholar] [CrossRef]
- Bellizzi, V.; Cupisti, A.; Locatelli, F.; Bolasco, P.; Brunori, G.; Cancarini, G.; Caria, S.; De Nicola, L.; Di Iorio, B.R.; Di Micco, L.; et al. Low-protein diets for chronic kidney disease patients: The Italian experience. BMC Nephrol. 2016, 17, 77. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Fouque, D. Nutritional management of chronic kidney disease. N. Engl. J. Med. 2017, 377, 1765–1776. [Google Scholar] [CrossRef] [PubMed]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76 (Suppl. 1), S1–S107. [Google Scholar] [CrossRef] [PubMed]
- Kovesdy, C.P.; Kalantar-Zadeh, K. Back to the future: Restricted protein intake for conservative management of CKD, triple goals of renoprotection, uremia mitigation, and nutritional health. Int. Urol. Nephrol. 2016, 48, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.H.; Kim, D.K.; Park, J.T.; Kang, E.W.; Yoo, T.H.; Kim, B.S.; Choi, K.H.; Lee, H.Y.; Han, D.S.; Shin, S.K. Influence of ketoanalogs supplementation on the progression in chronic kidney disease patients who had training on low-protein diet. Nephrology 2009, 14, 750–757. [Google Scholar] [CrossRef]
- American Diabetes Association. Introduction: Standards of Medical Care in Diabetes—2019. Diabetes Care 2019, 42 (Suppl. 1), S1–S2. [Google Scholar] [CrossRef]
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S.; et al. Nutrition therapy for adults with diabetes or prediabetes: A consensus report. Diabetes Care 2019, 42, 731–754. [Google Scholar] [CrossRef] [PubMed]
- Mitch, W.E.; Walser, M.; Steinman, T.I.; Hill, S.; Zeger, S.; Tungsanga, K. The effect of a keto acid-amino acid supplement to a restricted diet on the progression of chronic renal failure. N. Engl. J. Med. 1984, 311, 623–629. [Google Scholar] [CrossRef]
- Khan, I.A.; Nasiruddin, M.; Haque, S.F.; Khan, R.A. Comparative evaluation of efficacy and safety profile of rhubarb and α-keto analogs of essential amino acids supplementation in patients with diabetic nephropathy. Saudi J. Kidney Dis. Transpl. 2016, 27, 710–716. [Google Scholar] [CrossRef]
- Aparicio, M.; Bellizzi, V.; Chauveau, P.; Cupisti, A.; Ecder, T.; Fouque, D.; Garneata, L.; Lin, S.; Mitch, W.E.; Teplan, V.; et al. Protein-restricted diets plus keto/amino acids--a valid therapeutic approach for chronic kidney disease patients. J. Ren. Nutr. 2012, 22 (Suppl. 2), S1–S21. [Google Scholar] [CrossRef]
- Aparicio, M.; Bellizzi, V.; Chauveau, P.; Cupisti, A.; Ecder, T.; Fouque, D.; Garneata, L.; Lin, S.; Mitch, W.E.; Teplan, V.; et al. Keto acid therapy in predialysis chronic kidney disease patients: Final consensus. J Ren Nutr. 2012, 22 (Suppl. 2), S22–S24. [Google Scholar] [CrossRef]
- Aparicio, M.; Bellizzi, V.; Chauveau, P.; Cupisti, A.; Ecder, T.; Fouque, D.; Garneata, L.; Lin, S.; Mitch, W.; Teplan, V.; et al. Do ketoanalogues still have a role in delaying dialysis initiation in CKD predialysis patients? Semin. Dial. 2013, 26, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Garneata, L.; Mircescu, G. Effect of low-protein diet supplemented with keto acids on progression of chronic kidney disease. J. Ren. Nutr. 2013, 23, 210–213. [Google Scholar] [CrossRef]
- Jiang, Z.; Zhang, X.; Yang, L.; Li, Z.; Qin, W. Effect of restricted protein diet supplemented with keto analogues in chronic kidney disease: A systematic review and meta-analysis. Int. Urol. Nephrol. 2016, 48, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.M.; Ahmadi, S.F.; Kovesdy, C.P.; Kalantar-Zadeh, K. Low-protein diet for conservative management of chronic kidney disease: A systematic review and meta-analysis of controlled trials. J. Cachexia Sarcopenia Muscle 2018, 9, 235–245. [Google Scholar] [CrossRef]
- Bellizzi, V.; Signoriello, S.; Minutolo, R.; Di Iorio, B.; Nazzaro, P.; Garofalo, C.; Calella, P.; Chiodini, P.; De Nicola, L.; Torraca, S.; et al. No additional benefit of prescribing a very low-protein diet in patients with advanced CKD under regular nephrology care: A pragmatic, randomized, controlled trial. Am. J. Clin. Nutr. 2021. online ahead of print. [Google Scholar] [CrossRef]
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Available online: http://www.prisma-statement.org/ (accessed on 28 October 2021).
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P.; The Ottawa Hospital Research Institute. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 19 October 2021).
- National Heart, Lung, and Blood Institute. Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 19 October 2021).
- Alam, M.A.; Nasiruddin, M.; Haque, S.F.; Khan, R.A. Nigella sativa oil as an add-on in the conservative management of diabetic nephropathy: A novel synergistic approach. Asian J. Pharm. Clin. Res. 2019, 12, 230–236. [Google Scholar] [CrossRef]
- Barsotti, G.; Ciardella, F.; Morelli, E.; Cupisti, A.; Mantovanelli, A.; Giovannetti, S. Nutritional treatment of renal failure in type 1 diabetic nephropathy. Clin. Nephrol. 1988, 29, 280–287. [Google Scholar]
- Barsotti, G.; Cupisti, A.; Barsotti, M.; Sposini, S.; Palmieri, D.; Meola, M.; Lenti, C.; Morelli, E. Dietary treatment of diabetic nephropathy with chronic renal failure. Nephrol. Dial. Transplant. 1998, 13 (Suppl. 8), 49–52. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.Y.; Sun, C.Y.; Lee, C.C.; Wu, I.W.; Chen, Y.C.; Lin, Y.H.; Fang, W.C.; Pan, H.C. Ketoanalogue supplements reduce mortality in patients with pre-dialysis advanced diabetic kidney disease: A nationwide population-based study. Clin. Nutr. 2021, 40, 4149–4160. [Google Scholar] [CrossRef] [PubMed]
- Mihalache, A.; Garneata, L.; Mocanu, C.A.; Simionescu, T.P.; Mircescu, G. Low-salt low-protein diet and blood pressure control in patients with advanced diabetic kidney disease and heavy proteinuria. Int. Urol. Nephrol. 2021, 53, 1197–1207. [Google Scholar] [CrossRef]
- Teodoru, I.; Rusu, E.; Radulian, G. A 4 years study in diabetic chronic kidney disease patients on ketoaminoacids treatment in Bucharest. Results after 1-year follow-up. Farmacia 2018, 66, 296–301. [Google Scholar]
- Wang, Y.C.; Juan, S.H.; Chou, C.L.; Hsieh, T.C.; Wu, J.L.; Fang, T.C. Long-term effects of ketoanalogues on mortality and renal outcomes in advanced chronic kidney disease patients receiving a low-protein diet. Nutrients 2020, 12, 2708. [Google Scholar] [CrossRef]
- Zhu, H.; Zhang, L.; Wu, M.; Yang, M.; Yang, R.; Li, T.; Li, J. Study on effects of irbesartan combined with compound α-ketoacid tablets on the levels of tumour necrosis factor-1 (TNF-A), type IV collagen and 25-hydroxyvitamin D3 in patients with diabetic nephropathy. Acta Med. Mediterr. 2019, 35, 2469–2473. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Tobías, A. Assessing the influence of a single study in the meta-analysis estimate. Stata Tech. Bull. 1999, 8, 15–17. [Google Scholar]
- van Houwelingen, H.C.; Arends, L.R.; Stijnen, T. Advanced methods in meta-analysis: Multivariate approach and meta-regression. Stat. Med. 2002, 21, 589–624. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Hahn, D.; Hodson, E.M.; Fouque, D. Low protein diets for non-diabetic adults with chronic kidney disease. Cochrane Database Syst. Rev. 2018, 10, CD001892. [Google Scholar] [CrossRef] [PubMed]
- Garneata, L.; Stancu, A.; Dragomir, D.; Stefan, G.; Mirescu, G. Ketoanalogue-supplemented vegetarian very low-protein diet and CKD progression. J. Am. Soc. Nephrol. 2016, 27, 2164–2176. [Google Scholar] [CrossRef]
- Li, A.; Lee, H.Y.; Lin, Y.C. The effect of ketoanalogues on chronic kidney disease deterioration: A meta-analysis. Nutrients 2019, 11, 957. [Google Scholar] [CrossRef]
- Li, Q.; Wen, F.; Wang, Y.; Li, S.; Lin, S.; Qi, C.; Chen, Z.; Qiu, X.; Zhang, Y.; Zhang, S.; et al. Diabetic kidney disease benefits from intensive low-protein diet: Updated systematic review and meta-analysis. Diabetes Ther. 2021, 12, 21–36. [Google Scholar] [CrossRef] [PubMed]
- Klahr, S.; Levey, A.S.; Beck, G.J.; Caggiula, A.W.; Hunsicker, L.; Kusek, J.W.; Striker, G. The effects of dietary protein restriction and blood-pressure control on the progression of chronic renal disease. Modification of Diet in Renal Disease Study Group. N. Engl. J. Med. 1994, 330, 877–884. [Google Scholar] [CrossRef] [PubMed]
- Bellizzi, V.; Di lorio, B.R.; De Nicola, L.; ERIKA Study Group. Very low protein diet supplemented with ketoanalogs improves blood pressure control in chronic kidney disease. Kidney Int. 2007, 71, 245–251. [Google Scholar] [CrossRef]
- Rigalleau, V.; Blanchetier, V.; Combe, C.; Guillot, C.; Deleris, G.; Aubertin, J.; Aparicio, M.; Gin, H. A low-protein diet improves insulin sensitivity of endogenous glucose production in predialytic uremic patients. Am. J. Clin. Nutr. 1997, 65, 1512–1516. [Google Scholar] [CrossRef]
- Gougeon, R.; Pencharz, P.B.; Sigal, R.J. Effect of glycemic control on the kinetics of whole-body protein metabolism in obese subjects with non-insulin-dependent diabetes mellitus during iso- and hypoenergetic feeding. Am. J. Clin. Nutr. 1997, 65, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Kopple, J.D.; Levey, A.S.; Greene, T.; Chumlea, W.C.; Gassman, J.J.; Hollinger, D.L.; Maroni, B.J.; Merrill, D.; Scherch, L.K.; Schulman, G.; et al. Effect of dietary protein restriction on nutritional status in the Modification of Diet in Renal Disease Study. Kidney Int. 1997, 52, 778–791. [Google Scholar] [CrossRef] [PubMed]
- Bellizzi, V.; Chiodini, P.; Cupisti, A.; Viola, B.F.; Pezzotta, M.; De Nicola, L.; Minutolo, R.; Barsotti, G.; Piccoli, G.B.; Di Iorio, B. Very low-protein diet plus ketoacids in chronic kidney disease and risk of death during end-stage renal disease: A historical cohort controlled study. Nephrol. Dial. Transplant. 2015, 30, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Cianciaruso, B.; Capuano, A.; D’amaro, E.; Ferrara, N.; Nastasi, A.; Conte, G.; Bellizzi, V.; Andreucci, V.E. Dietary compliance to a low protein and phosphate diet in patients with chronic renal failure. Kidney Int. 1989, 36 (Suppl. 27), S173–S176. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Search Terms |
|---|---|
| Population | Advanced kidney disease, advanced renal disease, chronic kidney disease, chronic kidney failure, chronic renal disease, chronic renal failure, chronic renal insufficiency, diabetes, diabetes mellitus, diabetic, diabetic kidney disease, diabetic nephropathy, pre-dialysis kidney disease, renal failure, renal insufficiency data |
| Intervention | Ketoacid, ketoacids, keto acid, keto acids, ketoacid supplements, ketoanalog, ketoanalogs, keto-analog, keto-analogs, ketoanalogue, ketoanalogues, keto-analogue, keto-analogues, KA, EAA |
| Author Study Design | CKD Stage | Intervention Group | Control Group | Comparison (Control vs Patients) | Follow-Up (Months) | Quality Rating 1 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Disease, Patients (n) | Protein Intake (g/kg/day) | KA Pills | Disease, Patients (n) | Protein Intake (g/kg/day) | KA Pills | |||||
| Alam, 2019 RCT [23] | 3/4 | DKD, 32 | NR | Ketolog®, 3 × 600 mg/day + oil | DKD, 30 | NR | Ketolog®, 3 × 600 mg/day | KA vs KA + oil 2 | 3 | 6 |
| Barsotti, 1988 Pre-post [24] | NR | Diabetic nephropathy, 8 | VLPD/LPD (0.25–0.6) | EAA/KA 144 mg/kg/day | --- | Free diet | None | No KA/diet vs. KA + LPD/VLPD | >12 | 5 |
| Barsotti, 1998 Pre-post [25] | NR | Diabetic nephropathy, 32 | VLDP/LPD (0.3/0.7) 3 | Alfa Kappa®, 1 Tab/6 kg/day | --- | Free diet | None | No KA/diet vs. KA + LPD/VLPD | >60 | 5 |
| Bellizzi, 2018 Prospective observational [2] | 3–5 | DKD, 81 DKD, 29 | LPD (0.5–0.6) | Ketosteril®, 1 Tab/5–7 kg/day | CKD, 116 CKD, 35 | LPD (0.5–0.6) | Ketosteril®, 1 Tab/5–7 kg/day | CKD vs. DKD | 6 & 36 | 8 |
| Chang, 2009 Retrospective pre-post [8] | 3–5 | DKD, 67 | LPD (≤0.6) | Ketosteril®, 12 Tab/day | --- CKD, 53 | LPD (≤0.6) | NoneKetosteril®, 12 Tab/day | LPD vs. LPD + KA CKD vs. DKD | 6 | 6 |
| Chen, 2021 Retrospective cohort [26] | 5 | DKD, KA users 4 1001 | NR | NR | DKD, KA non-users 14,781 | NR | None | KA non-users vs. KA users | 60 | --- |
| Khan, 2016 RCT [12] | 3/4 | DKD, 32 | NR | α-KA, 3 × 600 mg/day | DKD, 32 (placebo) DKD, 32 (rhubarb) | NR | None | Placebo vs. rhubarb capsules vs. KA 5 | 3 | 6 |
| Mihalache, 2021 Pre-post(subgroup analysis) [27] | 4/5 | DKD, 92 | LPD (0.6) 6 | Ketosteril®, 1 Tab/10 kg/day | --- | LPD (0.6) | None | LPD vs. LPD + KA | 12 | 7 |
| Teodoru, 2018 Prospective cohort (subgroup analysis) [28] | 4 | DKD, KA compliant 11 | VLPD (0.3) | NR | DKD, KA noncompliant 9 | LPD > 0.6 at least once | NR | KA noncompliant vs. KA compliant | 12 | --- |
| Wang, 2020 Retrospective cohort [29] | 5 | DKD, KA user 67 | LPD (0.6) | Ketosteril® max. 6 Tab/day | DKD, KA non-user 107 CKD, KA non-user 58 CKD, KA user 98 | LPD (0.6) | None None max. 6 Tab/day | KA non-user vs. KA user in DKD, and compared to CKD | up to 108 7 | --- |
| Zhu, 2019 RCT [30] | NR | Diabetic nephropathy, 60 | LPD advised | Crodi®, 3 × 4 Tab ea. 0.63 g/day | Diabetic nephropathy, 60 | LPD advised | None | Irbesartan vs. irbesartan+ KA 8 | 3 | 6 |
| Parameter | Study | Outcome |
|---|---|---|
| GFR/estimated GFR | Alam et al., 2019 (RCT) [23] | Mean ± SD baseline vs week 12 (mL/min/1.73 m2): α-KA (control): 21.36 ± 6.66 vs 34.96 ± 17.17 1 α-KA + N. sativa oil: 22.37 ± 6.85 vs 41.84 ± 17.92 1,2 |
| Chang et al., 2009 (pre-post study) [8] | Mean ± SD pre vs post intervention (mL/min/1.73 m2): 3 Diabetics: 28.9 ± 10.2 vs. 26.1 ± 8.9 Mean ± SD change LPD v. LPD + KA (mL/min/1.73 m2/year): Diabetic: −12.3 ± 11.3 vs −4.0 ± 11.3 4 Nondiabetic: −8.8 ± 8.7 vs −3.6 ± 6.4 4 Independent predictors of attenuated decline with LPD + KA: Diabetes (HR 3.50; 95% CI 1.42, 8.62; p = 0.006) Elevated serum albumin (HR 3.13; 95% CI 1.30, 7.54; p = 0.011) | |
| Khan et al., 2016 (RCT) [12] | Mean ± SD baseline vs. 12 w (mL/min/1.73 m2): Placebo: 28.3 ± 1.53 vs. 32.4 ± 1.51 4 Rhubarb: 28.4 ± 1.51 vs. 35.6 ± 1.46 1,5 α-KA: 29.8 ± 1.48 vs. 37.4 ± 1.43 1,6 | |
| Mihalache et al., 2021 (pre-post study) [27] | Median (95% CI) pre vs. post intervention (mL/min/1.73 m2): 11.7 (11.2, 12.2) vs. 11.0 (10.3, 11.5) Median (95% CI) change pre to post intervention (mL/min/1.73 m2): −0.9 (−1.6, −0.1); p = 0.02 | |
| Teodoru et al., 2018 (cohort study) [28] | Median (IQR) annual decline compliant (n = 11) vs. noncompliant 7 (n = 9) patients (mL/min/1.73 m2/year): From initial diagnosis of stage 4 CKD: 1.4 (2.02) vs. 4.1 (5.2); p = 0.006 From study baseline: 3.75 (7.4) vs. 4.1 (5.6); p = 0.37 | |
| Serum creatinine | Khan et al., 2016 (RCT) [12] | Mean ± SD baseline vs. week 12 (mg/dL): Placebo: 3.43 ± 1.14 vs 2.33 ± 0.87 1 Rhubarb: 3.06 ± 1.38 vs. 1.82 ± 0.84 1,5 α-KA: 3.68 ± 1.20 vs. 1.83 ± 0.70 1,6 |
| Alam et al., 2019 (RCT) [23] | Mean ± SD baseline vs. week 12 (mg/dL): α-KA: 2.91 ± 0.74 vs. 2.07 ± 0.77 1 α-KA + N. sativa oil: 2.85 ± 0.69 vs. 1.79 ± 0.67 1,2 | |
| Creatinine clearance | Barsotti et al., 1988 (pre-post study) [24] | Mean ± SD change pre vs. post intervention (mL/min/mo): −1.38 ± 0.27 vs. −0.03 ± 0.37 1 |
| Barsotti et al., 1998 (pre-post study) [25] | Mean ± SD change pre vs. post intervention (mL/min/mo): −0.9 ± 0.62 vs. −0.22 ± 0.21 1 | |
| Urinary protein excretion | Alam et al., 2019 (RCT) [23] | Mean ± SD baseline vs. week 12 (g/day in 24-h urine): α-KA (control): 2.79 ± 1.19 vs. 1.98 ± 1.10 1 α-KA + N. sativa oil: 2.68 ± 0.89 vs. 1.57 ± 0.84 1,6 |
| Barsotti et al., 1998 (pre-post study) [25] | Mean ± SD pre vs. post intervention (g/day): 4.2 ± 2.6 vs. 2.5 ± 1.8 4 | |
| Khan et al., 2016 (RCT) [12] | Mean ± SD baseline vs. week 12 (g/day in 24-h urine): Placebo: 2.43 ± 1.24 vs. 1.43 ± 0.97 4 Rhubarb: 2.38 ± 1.52 vs. 1.22 ± 0.78 1 α-KA: 2.34 ± 0.78 vs. 1.03 ± 0.54 1,5 | |
| Mihalache et al., 2021 (pre-post study) [27] | Median (95% CI) change pre vs. post intervention (g/g creatininuria): −3.4 (−3.8, −3.1) 1 | |
| Urinary protein excretion | Zhu et al., 2019 (RCT) [30] | Mean ± SD baseline vs. week 12 (mg/day in 24-h urine): Irbesartan: 189.17 ± 12.67 vs. 150.46 ± 10.34 8 Irbesartan + α-KA: 190.32 ± 10.57 vs. 129.67 ± 8.24 5,8 |
| Mean ± SD baseline vs. week 12 (µg UAER/min in 24-h urine): Irbesartan: 102.28 ± 10.19 vs. 76.43 ± 8.57 8 Irbesartan + α-KA: 104.46 ± 8.37 vs. 60.87 ± 6.68 5,8 | ||
| Mean ± SD baseline vs. week 12 (g ALB/Cr per L in 24-h urine): Irbesartan: 178–47 ± 10.84 vs. 139.55 ± 10.46 8 Irbesartan + α-KA: 175.17 ± 11.47 vs. 110.64 ± 12.29 5,8 |
| Parameter | Study | Outcome |
|---|---|---|
| Serum urea | Alam et al., 2019 (RCT) [23] | Mean ± SD baseline vs. week 12 (mg/dL): α-KA (control): 84.47 ± 26.11 vs. 63.86 ± 23.33 1 α-KA + N. sativa oil: 82.85 ± 15.96 vs. 53.93 ± 14.35 1,2 |
| Barsotti et al., 1988 (pre-post study) [24] | Mean ± SD pre vs. post intervention (mg/dL): 112.7 ± 57.7 vs. 51.7 ± 22.5 1 | |
| Bellizzi et al., 2018 (observational study) [2] | Mean ± SD baseline vs. 6 months (mg/dL): Diabetic: 131 ± 58 3 vs. 105 ± 49 3,4 Nondiabetic: 115 ± 52 vs 88 ± 36 4 Mean ± SD baseline vs. final (duration 38 ± 13 mos, n = 64) (mg/dL): Diabetic: 130 ± 64 3 vs. 108 ± 51 3 Nondiabetic: 98 ± 48 vs. 90 ± 52 | |
| Chang et al., 2009 (pre-post study) [8] | Mean ± SD pre vs. post intervention (mg/dL): 5 Diabetic: 47.8 ± 12.4 vs. 48.5 ± 13.2 | |
| Khan et al., 2016 (RCT) [12] | Mean ± SD baseline vs. week 12 (mg/dL): Placebo: 97.3 ± 26.0 vs 59.5 ± 14.5 6 Rhubarb: 99.0 ± 22.6 vs. 52.7 ± 16.3 1 α-KA: 96.6 ± 21.4 vs. 46.3 ± 12.2 1,7 | |
| Serum/blood glucose | Alam et al., 2019 (RCT) [23] | Mean ± SD baseline vs. week 12 (mg/dL)—fasting: α-KA: 98.76 ± 10.97 vs. 92.20 ± 9.76 1 α-KA + N. sativa oil: 102.53 ± 21.26 vs. 94.25 ± 17.98 1 Mean ± SD baseline vs. week 12 (mg/dL)—postprandial: α-KA: 124.09 ± 14.02 vs. 116.93 ± 10.77 1 α-KA + N. sativa oil: 132.84 ± 30.08 vs. 122.12 ± 24.66 1 |
| Barsotti et al., 1988 (pre-post study) [24] | Mean ± SD pre vs. post intervention (mg/dL)—fasting: 154.6 ± 46.4 vs. 116.1 ± 10.9; p = NS | |
| Barsotti et al., 1998 (pre-post study) [25] | Mean ± SD pre vs. post intervention (mg/dL)—fasting: 174 ± 58 vs. 121 ± 20 4 | |
| Bellizzi et al., 2018 (observational study) [2] | Mean ± SD baseline vs. 6 months (mg/dL)—fasting: Diabetic: 126 ± 52 3 vs. 103 ± 29 3,4 Nondiabetic: 97 ± 18 vs. 97 ± 25 Mean ± SD baseline vs. final (duration 38 ± 13 mos, n = 64) (mg/dL): Diabetic: 114 ± 55 vs. 104 ± 18 3 Nondiabetic: 99 ± 16 vs. 94 ± 15 | |
| Chang et al., 2009 (pre-post study) [8] | Mean ± SD pre vs. post intervention (mg/dL)—fasting: 5 Diabetics: 180.5 ± 12.5 vs. 168.5 ± 11.8 | |
| Khan et al., 2016 (RCT) [12] | Mean ± SD baseline vs. week 12 (mg/dL)—fasting: Placebo: 140 ± 15.9 vs. 113 ± 14.3 1 Rhubarb: 142 ± 15.6 vs. 108 ± 14.0 1,8 α-KA: 141 ± 14.31 vs. 105 ± 9.5 1,7 Mean ± SD baseline vs. week 12 (mg/dL)—postprandial: Placebo: 195 ± 31.2 vs. 167 ± 24.3 1 Rhubarb: 192 ± 32.1 vs. 157 ± 16.6 1,8 α-KA: 191 ± 35.2 vs. 153 ± 13.9 1,7 | |
| Zhu et al., 2019 (RCT) [30] | Mean ± SD baseline vs. week 12 (mg/dL 9)—fasting: Irbesartan: 153.2 ± 18.0 vs. 135.1 ± 18.0 4 Irbesartan + α-KA: 153.2 ± 21.6 vs. 117.1 ± 18.0 4,8 | |
| Glycosylated hemoglobin | Mihalache et al., 2021 (pre-post study) [27] | Median (95% CI) pre vs. post intervention (%): 8.5 (8.4, 8.7) vs. 8.1 (7.8, 8.3) Median (95% CI) change pre to post intervention (%): −0.5 (−0.3, −0.8) 1 |
| Zhu et al., 2019 (RCT) [30] | Mean ± SD baseline vs. week 12 (%): Irbesartan: 8.41 ± 0.61 vs. 8.20 ± 0.52 4 Irbesartan + α-KA: 8.39 ± 0.53 vs. 7.76 ± 0.45 4,8 | |
| Insulin requirement | Barsotti et al., 1988 (pre-post study) [24] | Mean ± SD pre vs. post intervention (IU/day): 51.4 ± 11.5 vs. 38.5 ± 3.0 1 |
| Barsotti et al., 1998 (pre-post study) [25] | Mean ± SD pre vs. post intervention (IU/day): 49 ± 21 vs. 28 ± 10 6 | |
| Blood pressure | Alam et al., 2019 (RCT) [23] | Mean ± SD baseline vs. week 12 (mmHg)—SBP: α-KA: 126.23 ± 8.32 vs. 122.82 ± 6.68 4 α-KA + N. sativa oil: 132.5 ± 11.72 vs 130.62 ± 7.39 Mean ± SD baseline vs. week 12 (mmHg)—SBP: α-KA: 82.88 ± 6.88 vs. 80.26 ± 4.28 α-KA + N. sativa oil: 84.32 ± 11.66 vs. 82.46 ± 6.64 |
| Bellizzi et al., 2018 (observational study) [2] | Mean ± SD baseline vs. month 6 (mmHg)—SBP: Diabetic: 137 ± 20 3 vs. 130 ± 21 Nondiabetic: 127 ± 15 vs 129 ± 16 Mean ± SD baseline vs. month 6 (mmHg)—DBP: Diabetic: 78 ± 18 vs. 76 ± 8 Nondiabetic: 76 ± 8 vs. 76 ± 10 | |
| Chang et al., 2009 (pre-post study) [8] | Mean ± SD pre vs. post intervention (mmHg)—SBP: 5 Diabetics: 135.8 ± 10.2 vs. 128.5 ± 8.9 Mean ± SD pre vs. post intervention (mmHg)—DBP: 5 Diabetics: 72.5 ± 8.5 vs. 83.6 ± 8.2 | |
| Khan et al., 2016 (RCT) [12] | Mean ± SD baseline vs. week 12 (mmHg)—SBP: Placebo: 151.3 ± 18.6 vs. 136 ± 16.2 6 Rhubarb: 151.0 ± 21.6 vs. 132 ± 8.89 6 α-KA: 153.8 ± 22.9 vs. 129 ± 9.53 1,8 Mean ± SD baseline vs. week 12 (mmHg)—DBP: Placebo: 88.2 ± 10.4 vs. 85.98 ± 9.65 Rhubarb: 88.6 ± 11.4 vs. 84.63 ± 9.21 6 α-KA: 89.0 ± 12.4 vs. 83.7 ± 10.0 1,8 | |
| Mihalache et al., 2021 (pre-post study) [27] | Median (95% CI) pre vs post intervention (mmHg): SBP: 125 (120, 140) vs. 120 (110, 130) DBP: 80 (75, 80) vs. 65 (60, 65) Median (95% CI) change pre to post intervention (mmHg): SBP: −5 (−15, 0): p = 0.08 DBP: −15 (−20, −10); p < 0.001 | |
| Zhu et al., 2019 (RCT) [30] | Mean ± SD baseline vs. week 12 (mg/dL)—SBP: Irbesartan: 142.98 ± 10.01 vs. 132.56 ± 8.94 4 Irbesartan + α-KA: 144.17 ± 10.32 vs. 130.38 ± 8.76 4 Mean ± SD baseline vs. week 12 (mg/dL)—DBP: Irbesartan: 88.06 ± 7.96 vs. 72.48 ± 6.34 4 Irbesartan + α-KA: 87.43 ± 8.01 vs. 70.37 ± 6.78 4 | |
| Blood pressure | Barsotti, 1998 (pre-post study) [25] | No significant changes. |
| Hemoglobin | Alam et al., 2019 (RCT) [23] | Mean ± SD baseline vs. week 12 (g/dL): α-KA: 8.27 ± 1.34 vs. 9.39 ± 1.17 1 α-KA + N. sativa oil: 8.95 ± 1.51 vs. 10.34 ± 1.18 1,2 |
| Chang et al., 2009 (pre-post study) [8] | Mean ± SD pre vs. post intervention (g/dL): 5 Diabetics: 10.5 ± 0.68 vs. 10.2 ± 0.98 | |
| Bellizzi et al., 2018 (observational study) [2] | Mean ± SD baseline vs. month 6 (g/dL): Diabetic: 12.0 ± 1.7 vs. 11.7 ± 1.5 Nondiabetic: 12.2 ± 2.2 vs. 12.3 ± 1.7 | |
| Khan et al., 2016 (RCT) [12] | Mean ± SD baseline vs. week 12 (g/dL): Placebo: 8.81 ± 1.88 vs. 9.91 ± 1.58 1 Rhubarb: 8.97 ± 2.03 vs. 10.0 ± 1.68 1 α-KA: 8.94 ± 1.13 vs. 10.3 ± 0.89 1,8 | |
| Calcium | Bellizzi et al., 2018 (observational study) [2] | Mean ± SD baseline vs. month 6 (mg/dL): Diabetic: 9.1 ± 0.8 vs. 9.1 ± 0.6 Nondiabetic: 9.3 ± 1.5 vs. 9.3 ± 0.6 |
| Teodoru, 2018 (cohort study) [28] | Median (IQR) change compliant (n = 11) vs. noncompliant 10 (n = 9) patients (mg/dL): from baseline to 12 months: −0.36 (0.61) vs. 0.07 (0.56); p = 0.1 | |
| Phosphate | Bellizzi et al., 2018 (observational study) [2] | Mean ± SD baseline vs. month 6 (mg/dL): Diabetic: 4.5 ± 1.3 vs. 4.1 ± 1.2 3,11 Nondiabetic: 4.3 ± 1.0 vs. 3.7 ± 0.8 4 |
| Mean ± SD baseline vs. year 2 (mg/dL): Diabetic: 4.3 ± 0.8 3 vs. 3.8 ± 0.5 4 Nondiabetic: 3.8 ± 0.8 vs. 3.6 ± 0.7 | ||
| Potassium | Bellizzi et al., 2018 (observational study) [2] | Mean ± SD baseline vs. month 6 (mEq/dL): Diabetic: 5.0 ± 0.8 vs. 4.7 ± 0.6 Nondiabetic: 4.8 ± 0.7 vs. 4.7 ± 0.6 |
| Parameter | Study | Outcome |
|---|---|---|
| Serum albumin | Barsotti et al., 1998 (pre-post study) [25] | Mean ± SD pre vs. post intervention (g/dL): 3.7 ± 0.4 vs. 3.8 ± 0.3; p = NS |
| Bellizzi et al., 2018 (observational study) [2] | Mean ± SD baseline vs. 6 months (g/dL): Diabetic: 3.7 ± 0.6 1 vs. 3.8 ± 0.4 Nondiabetic: 4.0 ± 0.6 vs 4.0 ± 0.4 | |
| Chang et al., 2009 (pre-post study) [8] | Mean ± SD pre vs. post intervention (g/dL): 2 Diabetic: 3.2 ± 0.6 vs. 3.4 ± 0.7 | |
| Body weight | Barsotti et al., 1988 (pre-post study) [24] | Mean ± SD pre vs. post intervention (kg): 69.1 ± 9.9 vs. 64.8 ± 8.5; p = NS |
| Barsotti et al., 1998 (pre-post study) [25] | Mean ± SD pre vs. post intervention (kg): 68.7 ± 10.1 vs. 67.8 ± 8.1; p = NS | |
| Body weight | Bellizzi et al., 2018 (observational study) [2] | Mean ± SD baseline vs. 6 months (kg): 2 Diabetic: 68.5 ± 14.0 vs. 65.2 ± 12.3 3 Nondiabetic: 66.0 ± 15.0 vs 63.9 ± 15.1 3 |
| Chang et al., 2009 (pre-post study) [8] | Mean ± SD pre vs. post intervention (kg): 2 Diabetic: 64.5 ± 6.8 vs. 65.2 ± 8.5 | |
| Teodoru, 2018 (cohort study) [28] | Median (IQR) change compliant (n = 11) vs. noncompliant 4 (n = 9) patients (kg): from baseline to 12 months: 1.75 (4.5) vs. 1.5 (7); p = 0.44 | |
| Cholesterol | Bellizzi et al., 2018 (observational study) [2] | Mean ± SD baseline vs. 6 months (mg/dL): Diabetic: 186 ± 50 vs. 165 ± 37 3 Nondiabetic: 177 ± 57 vs 166 ± 39 |
| Triglycerides | Bellizzi et al., 2018 (observational study) [2] | Mean ± SD baseline vs. 6 months (mg/dL): Diabetic: 183 ± 86 vs. 167 ± 83 Nondiabetic: 171 ± 88 vs 165 ± 78 |
| Teodoru, 2018 (cohort study) [28] | Median (IQR) change compliant (n = 11) vs. noncompliant 4 (n = 9) patients (mg/dL): from baseline to 12 months: 13.59 (45.34) vs. 73.79 (135.68); p = 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellizzi, V.; Garofalo, C.; Ferrara, C.; Calella, P. Ketoanalogue Supplementation in Patients with Non-Dialysis Diabetic Kidney Disease: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 441. https://doi.org/10.3390/nu14030441
Bellizzi V, Garofalo C, Ferrara C, Calella P. Ketoanalogue Supplementation in Patients with Non-Dialysis Diabetic Kidney Disease: A Systematic Review and Meta-Analysis. Nutrients. 2022; 14(3):441. https://doi.org/10.3390/nu14030441
Chicago/Turabian StyleBellizzi, Vincenzo, Carlo Garofalo, Carmela Ferrara, and Patrizia Calella. 2022. "Ketoanalogue Supplementation in Patients with Non-Dialysis Diabetic Kidney Disease: A Systematic Review and Meta-Analysis" Nutrients 14, no. 3: 441. https://doi.org/10.3390/nu14030441
APA StyleBellizzi, V., Garofalo, C., Ferrara, C., & Calella, P. (2022). Ketoanalogue Supplementation in Patients with Non-Dialysis Diabetic Kidney Disease: A Systematic Review and Meta-Analysis. Nutrients, 14(3), 441. https://doi.org/10.3390/nu14030441