A Review of Rehabilitation Benefits of Exercise Training Combined with Nutrition Supplement for Improving Protein Synthesis and Skeletal Muscle Strength in Patients with Cerebral Stroke

Abstract
1. Introduction
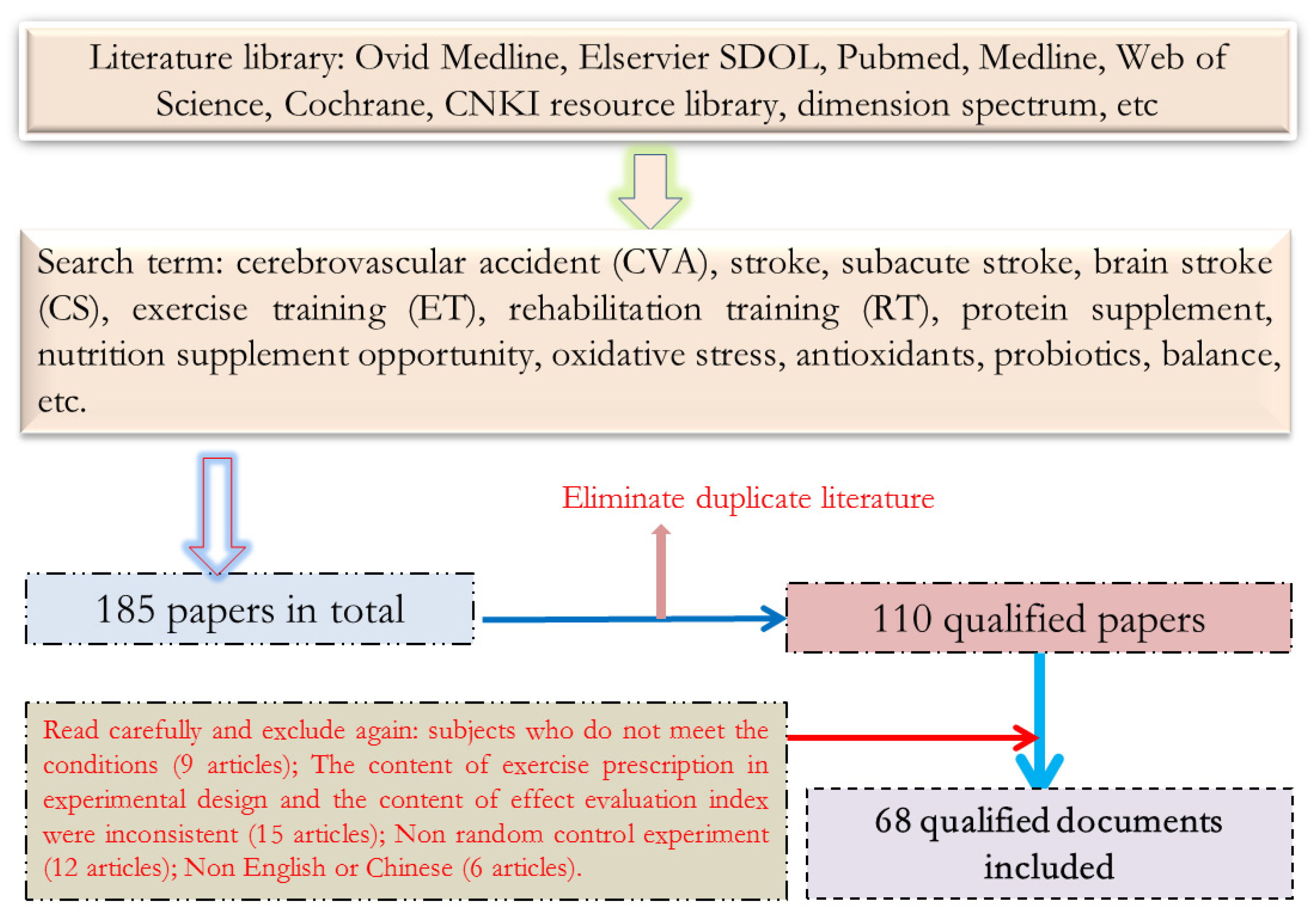
2. Data and Methods
2.1. Data Sources
2.2. Literature Shortlist Criteria
2.3. Literature Exclusion Criteria
2.4. Evaluation of Data Intake Quality
3. Results
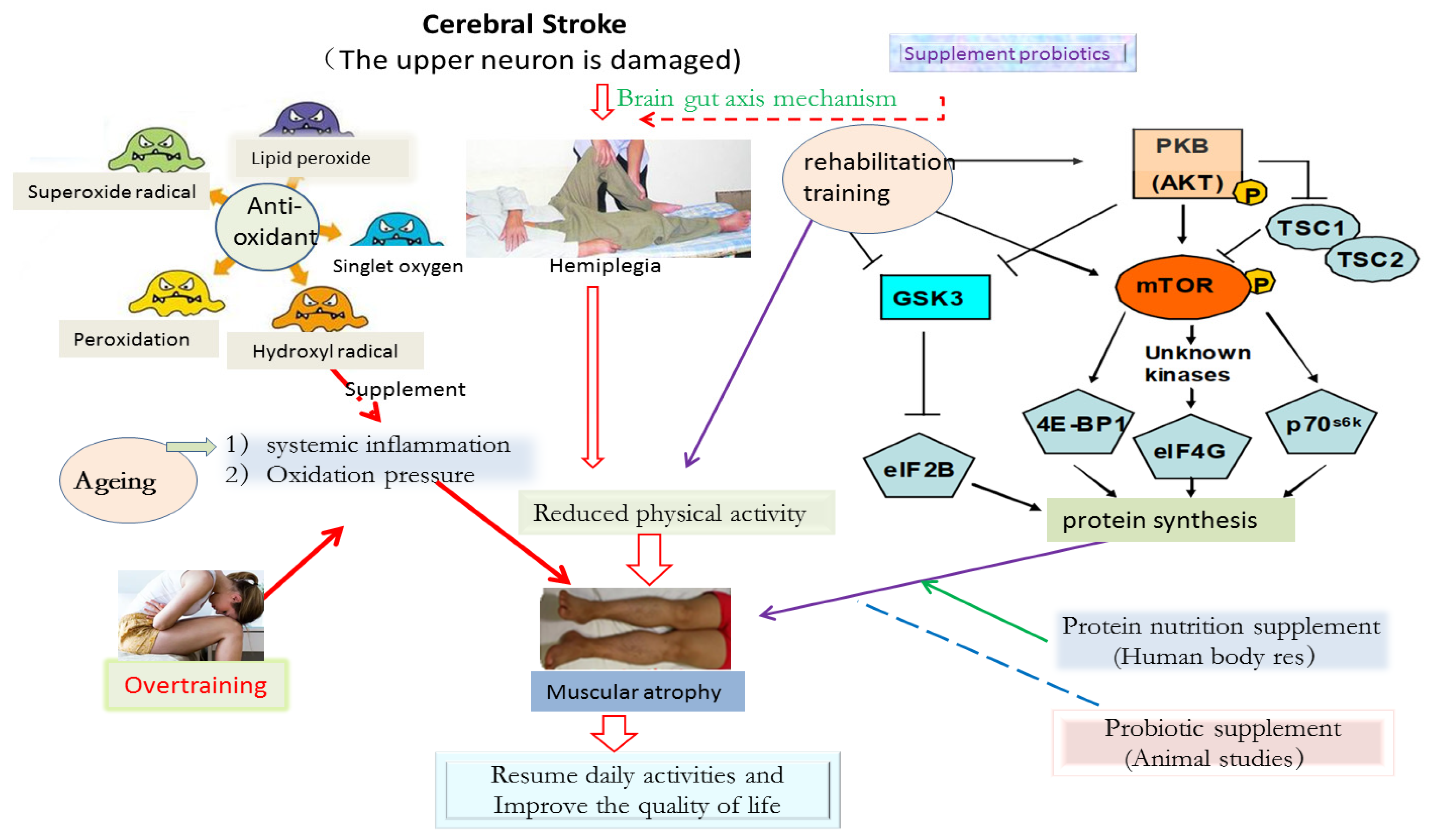
3.1. Possible Mechanism of Exercise Training Combined with Nutrition Supplement to Promote Muscle Growth (or Recovery) in Patients with CVA
3.1.1. mTOR Protein and Its Mechanism of Action
3.1.2. Exercise Training and Activation of mTOR Protein
3.1.3. The Physiological Mechanism of Nutritional Supplement, Amino Acid Circulation and Muscle Growth
3.2. Analysis of the Positive Effect of Exercise Training Combined with Nutritional Supplement on the Rehabilitation of CVA Patients
3.2.1. Rehabilitation Effect of “Carbohydrate and Protein Nutrition” Supplement on CVA Patients
3.2.2. Rehabilitation Effect of “Amino Acid and Protein Nutrition” Supplement on CVA Patients
3.2.3. Rehabilitation Effect of “Probiotics or Natural Antioxidants” on CVA Patients
3.3. Analysis of Negative Effect of Exercise Training Combined with Nutrition Supplement on CVA Patients’ Rehabilitation
4. Conclusions
5. Problems and Prospects
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Aghamiri, S.H.; Assarzadegan, F.; Ghaffari, M.; Khorasani, N.M.; Lima, B.S.; Sepehrirad, A.; Azimi, B.; Delkash, P. Recurrent middle cerebral artery stroke caused by arterial thoracic outlet syndrome and coagulopathy. Radiol. Case Rep. 2022, 17, 1665–1669. [Google Scholar] [CrossRef] [PubMed]
- Ma, L. How to reduce the mortality of stroke in China. Chin. J. Clin. Neurosurg. 2022, 27, 425–426. [Google Scholar] [CrossRef]
- Jiang, G.; Li, W.; Wang, D.; Shen, C.; Ji, Y.; Zheng, W. Epidemiological transition and distribution of stroke incidence in Tianjin, China, 1988–2010. Public Health 2016, 131, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Xiquan, H. Study on the mechanism of exercise training promoting neural plasticity after stroke. J. Sun Yat Sen Univ. Med. Sci. Ed. 2021, 42, 481–486. [Google Scholar] [CrossRef]
- Jiayue, H.; Qionan, C.; Yuqi, G.; Yihong, L. Effect of protein supplementation on rehabilitation of patients with chronic stroke physicotherapeutics. Formos. J. Phys. Ther. 2017, 42, 163. [Google Scholar] [CrossRef]
- Padilla, C.M.; Foucault, A.; Grimaud, O.; Nowak, E.; Timsit, S. Gender difference of geographic distribution of the stroke incidence affected by socioeconomic, clinical and urban–rural factors: An ecological study based on data from the Brest stroke registry in France. BMC Public Health 2021, 21, 39. [Google Scholar] [CrossRef]
- Pandian, J.; Singh, G.; Kaur, P.; Bansal, R.; Paul, B.; Singla, M.; Singh, S.; Samuel, C.; Litoria, P. Incidence, short-term outcome, and spatial distribution of stroke patients in Ludhiana, India. Neurology 2016, 86, 425–433. [Google Scholar] [CrossRef]
- Foley, N.C.; Martin, R.E.; Salter, K.L.; Teasell, R.W. A review of the relationship between dysphagia and malnutrition following stroke. J Rehabil. Med. 2009, 41, 707–713. [Google Scholar] [CrossRef]
- Schalk, B.W.M.; Penninx, B.W.J.H.; Bouter, L.M.; Visser, M. Serum albumin and muscle strength: A longitudinal study in older men and women. J. Am. Geriatr. Soc. 2005, 53, 1331–1338. [Google Scholar] [CrossRef]
- Okon, M.; Blum, B.; Nathaniel, T.I. Risk factors and ambulatory outcome in ischemic stroke patients with pre-stroke depression. J. Vasc. Nurs. 2021, 39, 91–99. [Google Scholar] [CrossRef]
- VanDerwerker, C.J.; Ross, R.E.; Stimpson, K.H.; Embry, A.E.; Aaron, S.E.; Cence, B.; George, M.S.; Gregory, C.M. Combining therapeutic approaches: rTMS and aerobic exercise in post-stroke depression: A case series. Top. Stroke Rehabil. 2018, 25, 61–67. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Uchida, K.; Jeong, S.; Yamaga, M. Effects of nutritional supplements on muscle mass and activities of daily living in elderly rehabilitation patients with decreased muscle mass: A randomized controlled trial. J. Nutr. Health Aging 2016, 20, 185–191. [Google Scholar] [CrossRef]
- Rabadi, M.H.; Coar, P.L.; Lukin, M.; Lesser, M.; Blass, J.P. Intensive nutritional supplements can improve outcomes in stroke rehabilitation. Neurology 2008, 71, 1856–1861. [Google Scholar] [CrossRef]
- Rasmussen, B.B.; Tipton, K.D.; Miller, S.L.; Wolf, S.E.; Wolfe, R.R. An oral essential amino acid-carbohydrate supplement enhances muscle protein anabolism after resistance exercise. J. Appl. Physiol. 2000, 88, 386–392. [Google Scholar] [CrossRef]
- Zielinska, N.E.; Cichon, N.; Saluk-Bijak, J.; Bijak, M.; Miller, E. Nutritional Supplements and Neuroprotective Diets and Their Potential Clinical Significance in Post-Stroke Rehabilitation. Nutrients 2021, 13, 2704. [Google Scholar] [CrossRef]
- Leyva, D.R.; Zahradka, P.; Ramjiawan, B.; Guzman, R.; Aliani, M.; Pierce, G.N. The effect of dietary flaxseed on improving symptoms of cardiovascular disease in patients with peripheral artery disease Rationale and design of the FLAX-PAD randomized controlled trial. Contemp. Clin. Trials 2011, 32, 724–730. [Google Scholar] [CrossRef]
- Goetz, M.E.; Judd, S.E.; Safford, M.M.; Hartman, T.J.; McClellan, W.M.; Vaccarino, V. Dietary flavonoid intake and incident coronary heart disease: The Reasons for Geographic and Racial Differences in Stroke (REGARDS) study. Am. J. Clin. Nutr. 2016, 104, 1236–1244. [Google Scholar] [CrossRef]
- Moreland, J.D.; Goldsmith, C.H.; Huijbregts, M.P.; Anderson, R.E.; Prentice, D.M.; Brunton, K.B.; O’Brien, M.A.; Torresin, W.D. Progressive resistance strengthening exercises after stroke: A single-blind randomized controlled trial. Arch. Phys. Med. Rehabil. 2003, 84, 1433–1440. [Google Scholar] [CrossRef]
- Cramp, M.C.; Greenwood, R.J.; Gill, M.; Rothwell, J.C.; Scott, O.M. Low intensity strength training for ambulatory stroke patients. Disabil. Rehabil. 2006, 28, 883–889. [Google Scholar] [CrossRef]
- Flansbjer, U.B.; Miller, M.; Downham, D.; Lexell, J. Progressive resistance training after stroke: Effects on muscle strength, muscle tone, gait performance and perceived participation. J. Rehabil. Med. 2008, 40, 42–48. [Google Scholar] [CrossRef]
- Twist, C.; Eston, R.G. The effect of exercise-induced muscle damage on perceived exertion and cycling endurance performance. Eur. J. Appl. Physiol. 2009, 105, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Murton, A.J.; Greenhaff, P.L. Physiological control of muscle mass in humans during resistance exercise, disuse and rehabilitation. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.B.; Kim, J.H.; Young, L.; Clark, J.M.; Park, Y. Epigallocatechin gallate (EGCG) alters body fat and lean mass through sex-dependent metabolic mechanisms in Drosophila melanogaster. Int. J. Food Sci. Nutr. 2019, 70, 959–969. [Google Scholar] [CrossRef]
- Perry, R.A.J.; Brown, L.A.; Lee, D.E.; Brown, J.L.; Baum, J.; Greene, N.P.; Washington, T.A. The Akt/mTOR pathway: Data comparing young and aged mice with leucine supplementation at the onset of skeletal muscle regeneration. Data Brief 2016, 8, 1426–1432. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.-C.; Lin, J.-C.; Bernard, J.R.; Liao, Y.-H. Green tea extract supplementation does not hamper endurance-training adaptation but improves antioxidant capacity in sedentary men. Appl. Physiol. Nutr. Metab. 2015, 40, 990–996. [Google Scholar] [CrossRef]
- Li, Y.; Fu, Q.; Wu, W.; Kong, Y. Effect of scalp acupuncture interactive MOTOMED intelligent exercise training on limb motor function and serum NGF BDNF level in stroke patients with hemiplegia. Hebei Med. Sci. 2020, 2, 222–226. [Google Scholar] [CrossRef]
- Lane, M.T.; Herda, T.J.; Fry, A.C.; Cooper, M.A.; Andre, M.J.; Gallagher, P.M. Endocrine responses and acute mTOR pathway phosphorylation to resistance exercise with leucine and whey. Biol. Sport 2017, 34, 197–203. [Google Scholar] [CrossRef]
- Hasegawa, N.; Fujie, S.; Horii, N.; Miyamoto-Mikami, E.; Tsuji, K.; Uchida, M.; Hamaoka, T.; Tabata, I.; Iemitsu, M. Effects of Different Exercise Modes on Arterial Stiffness and Nitric Oxide Synthesis. Med. Sci. Sport. Exerc. 2018, 50, 1177–1185. [Google Scholar] [CrossRef]
- Kido, K.; Ato, S.; Yokokawa, T.; Sato, K.; Fujita, S. Resistance training recovers attenuated APPL1 expression and improves insulin-induced Akt signal activation in skeletal muscle of type 2 diabetic rats. Am. Physiol. Endocrinol. Metab. 2018, 314, E564–E571. [Google Scholar] [CrossRef]
- Bauer, P.; Zeissler, S.; Walscheid, R.; Frech, T.; Hillebrecht, A. Acute effects of high-intensity exercise on hematological and iron metabolic parameters in elite male and female dragon boating athletes. Physician Sport. Med. 2018, 46, 335–341. [Google Scholar] [CrossRef]
- Williamson, D.L.; Kubica, N.; Kimball, S.R.; Jefferson, L.S. Exercise-induced alterations in extracellular signal-regulated kinase 1/2 and mammalian target of rapamycin (mTOR) signalling to regulatory mechanisms of mRNA translation in mouse muscle. J. Physiol. 2006, 573, 497–510. [Google Scholar] [CrossRef]
- Smeuninx, B.; Elhassan, Y.S.; Manolopoulos, K.N.; Sapey, E.; Rushton, A.B.; Edwards, S.J.; Morgan, P.T.; Philp, A.; Brook, M.S.; Gharahdaghi, N. The effect of short-term exercise prehabilitation on skeletal muscle protein synthesis and atrophy during bed rest in older men. J. Cachexia Sarcopenia Muscle 2020, 12, 52–69. [Google Scholar] [CrossRef]
- Li, Z.Y.; Yu, S.K.; Li, J.P.; Li, Y.Z. Effect of differentarterial occlusion pressure and intermittent mode on KAATSU-loaded deep-squat exercise on the characteristics of thigh muscle activation. Chin. J. Appl. Physiol. 2021, 37, 300–304. [Google Scholar] [CrossRef]
- Howard, G.; Cushman, M.; Moy, C.S.; Oparil, S.; Muntner, P.; Lackland, D.T.; Manly, J.J.; Flaherty, M.L.; Judd, S.E.; Wadley, V.G. Association of Clinical and Social Factors with Excess Hypertension Risk in Black Compared With White US Adults. J. Am. Med. Assoc. 2018, 320, 1338–1348. [Google Scholar] [CrossRef]
- Koopman, R.; Wagenmakers, A.J.M.; Manders, R.J.F.; Zorenc, A.H.G.; Senden, J.M.G.; Gorselink, M.; Keizer, H.A.; van Loon, L.J.C. Combined ingestion of protein and free leucine with carbohydrate increases postexercise muscle protein synthesis in vivo in male subjects. Am. J. Physiol. Endocrinol. Metab. 2005, 288, 645–653. [Google Scholar] [CrossRef]
- Li, L.; Shuxiu, W. Effect of comprehensive rehabilitation training combined with acid stimulation on swallowing function and nutritional status in patients with dysphagia after stroke. Mod. Med. 2014, 42, 895–898. [Google Scholar] [CrossRef]
- Oyanagi, K.; Kitai, T.; Yoshimura, Y.; Yokoi, Y.; Ohara, N.; Kohara, N.; Sakai, N.; Honda, A.; Onishi, H.; Iwata, K. Effect of early intensive rehabilitation on the clinical outcomes of patients with acute stroke. Geriatr. Gerontol. Int. 2021, 21, 623–628. [Google Scholar] [CrossRef]
- Kadekawa, K.; Majima, T.; Kawamorita, N.; Okada, H.; Yoshizawa, T.; Mori, K.; Tyagi, P.; Sugaya, K.; Yoshimura, N. Effects of an alpha1A/D-adrenoceptor antagonist, naftopidil, and a phosphodiesterase type 5 inhibitor, tadalafil, on urinary bladder remodeling in rats with spinal cord injury. Neurourol. Urodyn. 2017, 36, 1488–1495. [Google Scholar] [CrossRef]
- Rial, D.; Puighermanal, E.; Chazalon, M.; Valjent, E.; Schiffmann, S.N.; d’Exaerde, A.D. Mammalian Target of Rapamycin-RhoA Signaling Impairments in Direct Striatal Projection Neurons Induce Altered Behaviors and Striatal Physiology in Mice. Biol. Psychiatry 2020, 88, 945–954. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhang, B.; Li, Z.; Hu, Y.; Zhou, Y.; Fan, J. The effect of MOTOMED intelligent exercise training combined with intensive walking training on the rehabilitation of lower limb function of hemiplegic patients after stroke. Clin. Res. China 2019, 32, 976–978. [Google Scholar] [CrossRef]
- Wu, J.; Zhao, F.F.; Tian, F.; Ma, F.; Guan, T. miR-34 Promotes Autophagy and Apoptosis of Spinal Chondrocytes by Mammalian Target of Rapamycin/ Phosphatidylinositol-3-Kinase/Protein Kinase B Signaling. J. Biomater. Tissue Eng. 2020, 10, 1877–1883. [Google Scholar] [CrossRef]
- Li, S.K.Y.; Wan, M.M.P.; Siu, F.P.L.; Chung, S.S.; Pang, M.Y.C. Relationship Between Nutritional Factors and Hip Bone Density in Individuals with Chronic Stroke. Calcif. Tissue Int. 2017, 101, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Atherton, P.; Smith, K.; Rennie, M.J. Human muscle protein synthesis and breakdown during and after exercise. J. Appl. Physiol. 2009, 106, 2026–2039. [Google Scholar] [CrossRef] [PubMed]
- Pataky, M.W.; Van Acker, S.L.; Dhingra, R.; Freeburg, M.M.; Arias, E.B.; Oki, K.; Wang, H.Y.; Treebak, J.T.; Cartee, G.D. Fiber type-specific effects of acute exercise on insulin-stimulated AS160 phosphorylation in insulin-resistant rat skeletal muscle. Am. J. Physiol. Endocrinol. Metab. 2019, 317, E984–E998. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, J.M.; Fry, C.S.; Drummond, M.J.; Gundermann, D.M.; Walker, D.K.; Glynn, E.L.; Timmerman, K.L.; Dhanani, S.; Volpi, E.; Rasmussen, B.B. Mammalian Target of Rapamycin Complex 1 Activation Is Required for the Stimulation of Human Skeletal Muscle Protein Synthesis by Essential Amino Acids. J. Nutr. 2011, 141, 856–862. [Google Scholar] [CrossRef]
- Volpi, E.; Kobayashi, H.; Sheffield-Moore, M.; Mittendorfer, B.; Wolfe, R.R. Essential amino acids are primarily responsible for the amino acid stimulation of muscle protein anabolism in healthy elderly adults. Am. J. Clin. Nutr. 2003, 78, 250–258. [Google Scholar] [CrossRef]
- Candow, D.G.; Burke, N.C.; Smith-Palmer, T.; Burke, D.G. Effect of whey and soy protein supplementation combined with resistance training in young adults. Int. J. Sport Nutr. Exerc. Metab. 2006, 16, 233–244. [Google Scholar] [CrossRef]
- Houston, D.K.; Nicklas, B.J.; Ding, J.Z.; Harris, T.B.; Tylavsky, F.A.; Newman, A.B.; Lee, J.S.; Sahyoun, N.R.; Visser, M.; Kritchevsky, S.B. Dietary protein intake is associated with lean mass change in older, community-dwelling adults: The health, aging, and body composition (health ABC) study. Am. J. Clin. Nutr. 2008, 87, 150–155. [Google Scholar] [CrossRef]
- Yin, H.D.; Cui, C.; Han, S.S.; Chen, Y.Q.; Zhao, J.; He, H.R.; Li, D.Y.; Zhu, Q. Fibromodulin Modulates Chicken Skeletal Muscle Development via the Transforming Growth Factor-Beta Signaling Pathway. Animals 2020, 10, 1477. [Google Scholar] [CrossRef]
- Geranton, S.M.; Jimenez-Diaz, L.; Torsney, C.; Tochiki, K.K.; Stuart, S.A.; Leith, J.L.; Lumb, B.M.; Hunt, S.P. A Rapamycin-Sensitive Signaling Pathway Is Essential for the Full Expression of Persistent Pain States. J. Neurosci. 2009, 29, 15017–15027. [Google Scholar] [CrossRef]
- Bolster, D.R.; Vary, T.C.; Kimball, S.R.; Jefferson, L.S. Leucine regulates translation initiation in rat skeletal muscle via enhanced eIF4G phosphorylation. J. Nutr. 2004, 134, 1704–1710. [Google Scholar] [CrossRef]
- Crozier, S.J.; Kimball, S.R.; Emmert, S.W.; Anthony, J.C.; Jefferson, L.S. Oral leucine administration stimulates protein synthesis in rat skeletal muscle. J. Nutr. 2005, 135, 376–382. [Google Scholar] [CrossRef]
- Nishimura, Y.; Jensen, M.; Bulow, J.; Thomsen, T.T.; Arimitsu, T.; van Hall, G.; Fujita, S.; Holm, L. Coingestion of cluster dextrin carbohydrate does not increase exogenous protein-derived amino acid release or myofibrillar protein synthesis following a whole-body resistance exercise in moderately trained younger males: A double-blinded randomized controlled crossover trial. Eur. J. Nutr. 2022, 61, 2475–2491. [Google Scholar] [CrossRef]
- Markova, M.; Hornemann, S.; Sucher, S.; Wegner, K.; Pivovarova, O.; Rudovich, N.; Thomann, R.; Schneeweiss, R.; Rohn, S.; Pfeiffer, A.F.H. Rate of appearance of amino acids after a meal regulates insulin and glucagon secretion in patients with type 2 diabetes: A randomized clinical trial. Am. J. Clin. Nutr. 2018, 108, 279–291. [Google Scholar] [CrossRef]
- Abdulla, H.; Smith, K.; Atherton, P.J.; Idris, I. Role of insulin in the regulation of human skeletal muscle protein synthesis and breakdown: A systematic review and meta-analysis. Diabetologia 2016, 59, 44–55. [Google Scholar] [CrossRef]
- Scherbakov, N.; Ebner, N.; Sandek, A.; Meisel, A.; Haeusler, K.G.; von Haehling, S.; Anker, S.D.; Dirnagl, U.; Joebges, M.; Doehner, W. Influence of essential amino acids on muscle mass and muscle strength in patients with cerebral stroke during early rehabilitation: Protocol and rationale of a randomized clinical trial (AMINO-Stroke Study). BMC Neurol. 2016, 16, 10. [Google Scholar] [CrossRef]
- Rundqvist, H.C.; Esbjornsson, M.; Rooyackers, O.; Osterlund, T.; Moberg, M.; Apro, W.; Blomstrand, E.; Jansson, E. Influence of nutrient ingestion on amino acid transporters and protein synthesis in human skeletal muscle after sprint exercise. J. Appl. Physiol. 2017, 123, 1501–1515. [Google Scholar] [CrossRef]
- Takeuchi, I.; Yoshimura, Y.; Shimazu, S.; Jeong, S.; Yamaga, M.; Koga, H. Effects of branched-chain amino acids and vitamin D supplementation on physical function, muscle mass and strength, and nutritional status in sarcopenic older adults undergoing hospital-based rehabilitation: A multicenter randomized controlled trial. Geriatr. Gerontol. Int. 2019, 19, 12–17. [Google Scholar] [CrossRef]
- Carlsson, M.; Littbrand, H.; Gustafson, Y.; Lundin-Olsson, L.; Lindelof, N.; Rosendahl, E.; Haglin, L. Effects of high-intensity exercise and protein supplement on muscle mass in ADL dependent older people with and without malnutrition: A randomized controlled trial. J. Nutr. Health Aging 2011, 15, 554–560. [Google Scholar] [CrossRef]
- Esmarck, B.; Andersen, J.L.; Olsen, S.; Richter, E.A.; Mizuno, M.; Kjaer, M. Timing of postexercise protein intake is important for muscle hypertrophy with resistance training in elderly humans. J. Physiol. 2001, 535, 301–311. [Google Scholar] [CrossRef]
- Dreyer, H.C.; Drummond, M.J.; Glynn, E.L.; Fujita, S.; Chinkes, D.L.; Volpi, E.; Rasmussen, B.B. Resistance exercise increases human skeletal muscle AS160/TBC1D4 phosphorylation in association with enhanced leg glucose uptake during postexercise recovery. J. Appl. Physiol. 2008, 105, 1967–1974. [Google Scholar] [CrossRef] [PubMed]
- Sheikholeslami-Vatani, D.; Ahmadi, S. Effect of Oral Branched-Chain Amino Acid Supplementation Prior to Resistance Exercise on Metabolic Hormones, Plasma Amino Acids, and Serum Indices of Muscle Damage in the Recovery Period. Top. Clin. Nutr. 2016, 31, 346–354. [Google Scholar] [CrossRef]
- Carroll, K.M.; Bazyler, C.D.; Bernards, J.R.; Taber, C.B.; Stuart, C.A.; DeWeese, B.H.; Sato, K.; Stone, M.H. Skeletal Muscle Fiber Adaptations Following Resistance Training Using Repetition Maximums or Relative Intensity. Sports 2019, 7, 169. [Google Scholar] [CrossRef] [PubMed]
- Rustad, P.I.; Sailer, M.; Cumming, K.T.; Jeppesen, P.B.; Kolnes, K.J.; Sollie, O.; Franch, J.; Ivy, J.L.; Daniel, H.; Jensen, J. Intake of protein plus carbohydrate during the first two hours after exhaustive cycling improves performance the following day. PLoS ONE 2016, 11, e0153229. [Google Scholar] [CrossRef] [PubMed]
- Serra, M.C.; Monica, C. The Importance of Assessing Nutritional Status to Ensure Optimal Recovery during the Chronic Phase of Stroke. Stroke Res. Treat. 2018, 2018, 1297846. [Google Scholar] [CrossRef]
- de Aguilar-Nascimento, J.; Prado Silveira, B.R.; Dock-Nascimento, D.B. Early enteral nutrition with whey protein or casein in elderly patients with acute ischemic stroke: A double-blind randomized trial. Nutrition 2011, 27, 440–444. [Google Scholar] [CrossRef]
- Phillips, S.; Tang, J.E.; Moore, D.R. The role of milk and soy-based protein in support of muscle protein synthesis and muscle protein accretion in young and elderly persons. J. Am. Coll. Nutr. 2009, 28, 343–354. [Google Scholar] [CrossRef]
- Tang, J.E.; Moore, D.R.; Kujbida, G.W.; Tarnopolsky, M.A.; Phillips, S.M. Ingestion of whey hydrolysate, casein, or soy protein isolate: Effects on mixed muscle protein synthesis at rest and following resistance exercise in young men. J. Appl. Physiol. 2009, 107, 987–992. [Google Scholar] [CrossRef]
- Noble, E.E.; Hsu, T.M.; Kanoski, S.E. Gut to brain dysbiosis: Mechanisms linking western diet consumption, the microbiome, and cognitive impairment. Front. Behav. Neurosci. 2017, 11, 9. [Google Scholar] [CrossRef]
- Westfall, S.; Lomis, N.; Kahouli, I.; Dia, S.Y.; Singh, S.P.; Prakash, S. Microbiome, probiotics and neurodegenerative diseases: Deciphering the gut brain axis. Cell. Mol. Life Sci. 2017, 74, 3769–3787. [Google Scholar] [CrossRef]
- Bel-Rhlid, R.; Durga, J.; Kunz, T.; Schmitt, J.A.J. Probiotic and Polyphenol against Neurodegeneration. U.S. Patent 15/713935, 25 September 2017. [Google Scholar]
- Chen, Y.M.; Wei, L.; Chiu, Y.S.; Hsu, Y.J.; Tsai, T.Y.; Wang, M.F.; Huang, C.C. Lactobacillus plantarum TWK10 supplementation improves exercise performance and increases muscle mass in mice. Nutrients 2016, 8, 205. [Google Scholar] [CrossRef]
- Sanchez-Moreno, C.; Dashe, J.F.; Thaler, D.; Folstein, M.F.; Martin, A. Decreased levels of plasma vitamin C and increased concentrations of inflammatory and oxidative stress markers after stroke. Stroke 2004, 35, 163–168. [Google Scholar] [CrossRef]
- Nabavi, S.F.; Dean, O.M.; Turner, A.; Sureda, A.; Daglia, M.; Nabavi, S.M. Oxidative stress and post-stroke depression: Possible therapeutic role of polyphenols? Curr. Med. Chem. 2015, 22, 343–351. [Google Scholar] [CrossRef]
- Sinha, K.; Chaudhary, G.; Gupta, Y.K. Protective effect of resveratrol against oxidative stress in middle cerebral artery occlusion model of stroke in rats. Life Sci. 2002, 71, 655–665. [Google Scholar] [CrossRef]
- Samavat, H.; Wu, A.H.; Ursin, G.; Torkelson, C.J.; Wang, R.W.; Yu, M.C.; Yee, D.; Kurzer, M.S.; Yuan, J.M. Green Tea Catechin Extract Supplementation Does Not Influence Circulating Sex Hormones and Insulin-Like Growth Factor Axis Proteins in a Randomized Controlled Trial of Postmenopausal Women at High Risk of Breast Cancer. J. Nutr. 2019, 149, 619–627. [Google Scholar] [CrossRef]
- Jones, P.S.; Pomeroy, V.M.; Wang, J.; Schlaug, G.; Marrapu, S.T.; Geva, S.; Rowe, P.J.; Chandler, E.; Kerr, A.; Baron, J.C. Does Stroke Location Predict Walk Speed Response to Gait Rehabilitation? Hum. Brain Mapp. 2016, 37, 689–703. [Google Scholar] [CrossRef]
- Baker, B.A.; Hollander, M.S.; Mercer, R.R.; Kashon, M.L.; Cutlip, R.G. Adaptive stretch-shortening contractions: Diminished regenerative capacity with aging. Appl. Physiol. Nutr. Metab. 2008, 33, 1181–1191. [Google Scholar] [CrossRef]
- Zhang, J.C.; Xu, H.; Yuan, Y.; Chen, J.Y.; Zhang, Y.J.; Lin, Y.; Yuan, S.Y. Delayed treatment with green tea polyphenol EGCG promotes neurogenesis after ischemic stroke in adult mice. Mol. Neurobiol. 2017, 54, 3652–3664. [Google Scholar] [CrossRef]
- Cutlip, R.G.; Baker, B.A.; Geronilla, K.B.; Mercer, R.R.; Kashon, M.L.; Miller, G.R.; Murlasits, Z.; Alway, S.E. Chronic exposure to stretch-shortening contractions results in skeletal muscle adaptation in young rats and maladaptation in old rats. Appl. Physiol. Nutr. Metab. 2006, 31, 573–587. [Google Scholar] [CrossRef]
- Rader, E.P.; Baker, B.A. Inflammaging and the age-specific responsiveness to stretch-shortening contractions. Exerc. Sport Sci. Rev. 2017, 45, 195–200. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author/Year | Test Group (Number) | Sports Training Program | Effectiveness Evaluation | Research Results |
|---|---|---|---|---|
| Moreland et al., (2003) [18] | n = 133 Chronic stroke patients | EG: Resistance training, 10 times/group, 5 groups, 3 times/week, 2 months in total; CG: Traditional treatment. | Lower limb muscle strength, walking for 2 min | lower limb muscle strength ↑ (EG > CG); LLFDI (EG ↔ CG); 2 MW (EG ↔ CG); |
| Cramp et al., (2006) [19] | n = 10 Chronic stroke patients | Self controlled experiment. Resistance: weight, elastic band and body weight; Mode: 5 groups of exercises on the hips and knees of both feet; Intensity: 20% 1 RM first, 50% 1 RM later, 10 times, three groups; Frequency: 2 times/week, 6 months in total. | Lower limb muscle strength; Isometric torque | lower limb muscle strength ↑ Knee extensor muscle strength ↑ Knee flexor muscle strength ↔ |
| Flansbjer et al., (2008) [20] | n = 24 Chronic stroke patients | EG: The training instrument is set to 80% of the maximum strength; CG: General daily activities. 90 min/course of treatment, 2 times/week, 10 weeks in total. | Muscle strength and muscle tension; TUG, 6 MW, SIS | ↑ Strength in PRE (PRE > CG) ↓ Muscle tone in PRE and CG ↑ Strength in PRE ↑ 3 measures in PRE and ↑ TUG and 6MW in PRE ↑ SIS (EG > CG) |
| Twist & Eston (2009) [21] | n = 15 Chronic stroke patients | EG: pull the elastic band on the upper limb, and make 4 TRTs in different directions respectively; Reach for objects 200 times, 45 min/time, 3 times/week, 4 weeks in total. | Trunk and Arm Motion: AROM, WMFT, FMA | ↑ Elbow extension in both groups ↑ Hand path straighten in TRT ↓ Trunk movement and ↑ AROM and FMA in both groups; WMFT:(EG ↔ CG) |
| Murton & Greenhaff (2010) [22] | n = 42 Chronic stroke patients | EG: 70% 1 RM with both feet, repeat 8~10 times as a group, and do three rounds; CG: ROM and soft exercise, 3 times/week, 12 weeks in total. | Lower limb muscle strength; 6 MW, step climbing and station arrival; LLFDI, GDS and SIP | ↑ EG lower limb muscle strength; ↑ Two groups of 6 MW and walking speed; ↑ CGLLFDI; ↑ Two groups of GDS; SIP (EG ↔ CG). |
| Kim et al., (2013) [23] | n = 36 Chronic stroke patients | Ankle muscle strength training group VS Lacing group VS CG. First, use 30% of the force to do plantar flexion for 20 times, and then use bare hands to give pressure to do isometric contraction of back flexion. The resistance movement of the ankle joint on the affected side of EG gradually increased by 40–80%. 4 times/week, 6 weeks. | Gait and balance function detection; 6 MW. | The swing amplitude of body pressure center in the three groups increased significantly. Physical function: the experimental group had positive effects on the toe off movement during walking |
| Lee et al., (2016) [24] | n = 36 Chronic stroke patients | Randomized controlled trial. EG: Air lock. Hip, knee and ankle flexion is performed on both lower limbs on the machine. First do 25% 1RM, four times, then do 70% 1 RM, 8–10 times, three groups; 5 times/week, 6 weeks in total. | Gait and balance function detection; 6 MW; BBS; Stand up and walk test | The balance ability of EG and CG increased significantly. EG’s left and right displacement before and after the body's center of gravity, BBS and the results of timed stand walk test were significantly improved |
| Kuo et al., (2015) [25] | n = 40 Chronic stroke patients | EG: Resistance exercise increased muscle strength FT, and repeated functional action control group; CG: Traditional treatment. Frequency and time: 1 h/day, 5 days/week, lasting for 4–6 weeks. | Isometric torque, MotorFMA, FTHUE, and FIM | ↑ Isometric torque, motor FMA and FTHUE (EG > CG, EG > CG). Follow up: ↑ Palmar pinch (PRE > CG, FT > CG), AROM (EG ↔ CG). |
| Yingying et al., (2016) [26] | n = 48 Chronic stroke patients | EG: Gradually increase the number of repetitions of six tasks, and CG does not intervene; 30 min/day, 3 days/week, 4 weeks in total. | Lower limb muscle strength; Gait performance, 6MW; Steptest; TUG. | ↑ Strength in all muscles in EG; ↑ Gait velocity, 6 MW, and TUG in EG; ↓ Step test in CG + Relationship between muscle strength and function. |
| Lane et al., (2017) [27] | n = 7 Chronic stroke patients | EG: 70% of 1RM was performed on both feet, 8~10 times per group, 3 groups, 2 times per week, a total of 12 weeks | Muscle strength, MAS, BBS; TUG and step registration time; GDS | ↑ Muscle strength, MAS, BBS; ↓ Time required for sitting to the station; No difference in GDS |
| Hasegawa et al., (2018) [28] | n = 48 Chronic stroke patients | EG: Gradually increase the number of repetitions of six tasks; CG: no intervention, 30 min/day, 3 days/week, 4 weeks in total. | Lower limb muscle strength; Walking ability; 6 MW, TUG | ↑ EG lower limb muscle strength; ↑ EG walking speed, 6 MW, TUG |
| Kido et al., (2018) [29] | n = 92 Chronic stroke patients | EG: ROM, muscle strength strengthening, balance, upper limb endurance and functional training; 90 min/time, 3 times/week, 14 weeks in total; CG: No motion. | Grasping power, FMA, WMF, BBS; 10-Meter and 6-MinuteWalk. | ↑ Grip strength, BBS, WMFT in both; ↑ Gait velocity in both. However, EG in each assessment is more improved than CG. |
| Bauer, et al., (2018) [30] | n = 42 Chronic stroke patients | EG: do 70% of 1 RM with both feet, 8~10 times/group, 3 groups/time; CG: ROM and soft exercise, 3 times/week, 6 week in total | Lower limb muscle strength; 6 MW; Stair climb and Chair rise; LLFDI; GDS and SIP. | ↑ Strength in most muscles in EG ↑ 6 MW and gait velocity in both ↑ LLFDI in PRT ↑ GDS and no SIP in bot |
| Williamson et al., (2018) [31] | n = 12 Chronic stroke patients | EG: pull the elastic band on the upper limb, and perform 4 different movements TRT respectively; Reach for objects, 150–180 times/30 min, 3 times/week, 4 weeks in total. | Arm motion track, Trunk and ArmMotion, RMA, MAS | ↑ Elbow extension in EG ↑ Hand path straighten in TRT ↑ Trunk movement in EG ↑ RMA in low level TRT (No difference for the MAS) |
| VanDerwerker et al., (2018) [11] | n = 24 Chronic stroke patients | EG: the machine is set at 80% of the maximum force; CG: general daily activities, 90 min course of treatment, 2 times/week, 10 weeks in total | Muscle strength, muscle tension, TUG, 6 MW | ↑ EG Muscle strength > CG; ↓ Two groups of muscle tension. Follow up: ↑EG Muscle strength; EG: ↑ TUG, 6 MW; ↑ EG: SIS > CG |
| Smeuninx, et al., (2020) [32] | n = 170 Chronic stroke patients | EG: 13 week rehabilitation physical therapy exercise training resistance training, 10 times/group, 4 groups, 3 times/week, 8 Weeks in total; CG: Traditional treatment. | Action capability indicator; Travel speed; Falls | ↑ Action capability indicators (EG > CG); ↑ Travel speed (EG > CG); |
| Xiquan (2021) [4] | n = 28 Chronic stroke patients | EG: weight bearing and standing balance training, 10~15 RM each time; 3 times/week, 4 weeks in total; CG: Physical therapy; 50 min/time, 5 times/week, 4 weeks in total | Muscle strength, maximum weight bearing, MAS, walking speed, PGIC | ↑ EG: maximum weight bearing > CG ↑ EG: Muscle strength lower limb ↑ EG: Walking speed >CG ↑ EG: PGIC > CG |
| Li, et al., (2021) [33] | n = 20 Chronic stroke patients | EG: 15 min warm up, 30 min 10 RM, 45 min/time, 3 times/week, 6 weeks in total; CG: Passive ROM traction, 3 times/week, 6 weeks. | Muscle trength; Walking and stair walking speed; SF-36 | ↑ Strength in both (PRE > CG); ↑ Walking speed in both group; SF-36 (EG ↔ CG). |
| Author/Year | Test Group (Number) | Sports Training Program | Nutrition/Protein Supplement | Key Findings |
|---|---|---|---|---|
| Rabadi et al., (2008) [13] | n = 116 Patients with acute stroke | Hospitalized rehabilitation treatment for acute strok | Nutrition supplement: 3 times/day, 5 g protein/time. | ↑ 2 min and 6 min walking performance; ↑ Independent functional pointer (FIM); ↑ FIM motor subscore |
| Scherbakov et al., (2016) [56] | n = 110 Patients with acute stroke | Rehabilitation treatment for acute stroke patients during hospitalization (<8weeks after onset) | Essential amino acid supplement (4 g essential amino acid); 3 times/day for 8 weeks | Nutritional supplement strategy could significantly improve the muscle atrophy of CVA patients. |
| Rundqvist et al., (2017) [57] | n = 31 Patients with acute stroke | Curling rehabilitation therapy exercise for patients with acute stroke | Nasogastric tube enteral nutrition formula containing casein; Nasogastric tube enteral nutrition formula containing whey protein | Nasogastric tube enteral nutrition formula containing whey protein can more effectively reduce systemic inflammatory reaction and increase antioxidant capacity in elderly patients with acute stroke |
| Takeuchi et al., (2019) [58] | n = 42 Patients with acute stroke | Progressive resistance movement, balance movement; 60 min/time, 3 times/week, 9 months in total. | Supplemented twice a day (at 10:00 and 16:00 respectively): 15 g protein, 25 g carbohydrate, 4.4 g fat (200 kcal in total). | After 3 months, muscle strength ↑ 57%; Simple exercise intervention did not cause difference in lower limb muscle strength; Protein supplement and exercise intervention did not cause FFM difference |
| Carlsson et al., (2011) [59] | n = 177 Patients with acute stroke | High intensity exercise for 3 months; Urgent supplement after exercise | EG: protein supplement 7.4 g, carbohydrate 15.7 g, fat 0.43 g; CG: placebo supplement, containing 0.2 g protein and 10.8 g carbohydrate | There was no difference in muscle mass and body weight; The muscle mass and body weight of EG were negatively affected after 6 months; Inadequate nutrition supplement compensates the energy required for high-intensity exercise. |
| Jiayue, et al., (2017) [5] | n = 12 Patients with acute stroke | Divide into two groups of six; 12 week resistance movement | Group 1: 0.8 g protein/person/day/1KG body weight; The second group: 1.6 g/person/day/1KG body weight. | Resistance exercise significantly increased the energy intake required to maintain weight by 15%, and reduced body fat by 2.2%; Protein intake does not make a difference |
| Esmarck et al., (2001) [60] | n = 13 Patients with acute stroke | Progressive resistance movement; 3 times/week, 12 weeks in total | Nutrition supplement: 10g protein, 7g carbohydrate and 3.3g lipid of milk and beans; In group P1, the intake time was immediately after exercise; P2 group: ingested 2 h after exercise | Cross sectional area of quadriceps femoris in P1 after exercise increased by 6.77%, and the average muscle fiber range increased by 24.01% |
| Zielinska, et al., (2021) [15] | n = 100 Patients with acute stroke | High intensity progressive resistance exercise, 3 times/week, 10 weeks in total | 240 mL of soybean protein was supplemented every night, including 60% carbohydrate, 23% fat and 17% protein. | Exercise group: lower limb muscle strength improved by 113%; Walking speed increased by 11.8%; Step climbing force improved by 28.4%; CG: walking speed decreased by 1%; Nutritional supplements did not result in any significant differences in major outcomes. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, S.; Liu, H.; Yang, L.; Wang, K.; Chen, N.; Zhang, T.; Luo, J. A Review of Rehabilitation Benefits of Exercise Training Combined with Nutrition Supplement for Improving Protein Synthesis and Skeletal Muscle Strength in Patients with Cerebral Stroke. Nutrients 2022, 14, 4995. https://doi.org/10.3390/nu14234995
Liu S, Liu H, Yang L, Wang K, Chen N, Zhang T, Luo J. A Review of Rehabilitation Benefits of Exercise Training Combined with Nutrition Supplement for Improving Protein Synthesis and Skeletal Muscle Strength in Patients with Cerebral Stroke. Nutrients. 2022; 14(23):4995. https://doi.org/10.3390/nu14234995
Chicago/Turabian StyleLiu, Shiqi, Hengxu Liu, Li Yang, Kun Wang, Nuo Chen, Tingran Zhang, and Jiong Luo. 2022. "A Review of Rehabilitation Benefits of Exercise Training Combined with Nutrition Supplement for Improving Protein Synthesis and Skeletal Muscle Strength in Patients with Cerebral Stroke" Nutrients 14, no. 23: 4995. https://doi.org/10.3390/nu14234995
APA StyleLiu, S., Liu, H., Yang, L., Wang, K., Chen, N., Zhang, T., & Luo, J. (2022). A Review of Rehabilitation Benefits of Exercise Training Combined with Nutrition Supplement for Improving Protein Synthesis and Skeletal Muscle Strength in Patients with Cerebral Stroke. Nutrients, 14(23), 4995. https://doi.org/10.3390/nu14234995