
The Impact of the COVID-19 Lockdown on Sugar-Sweetened Beverage Consumption in Children in Saudi Arabia: A Mixed-Methods Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
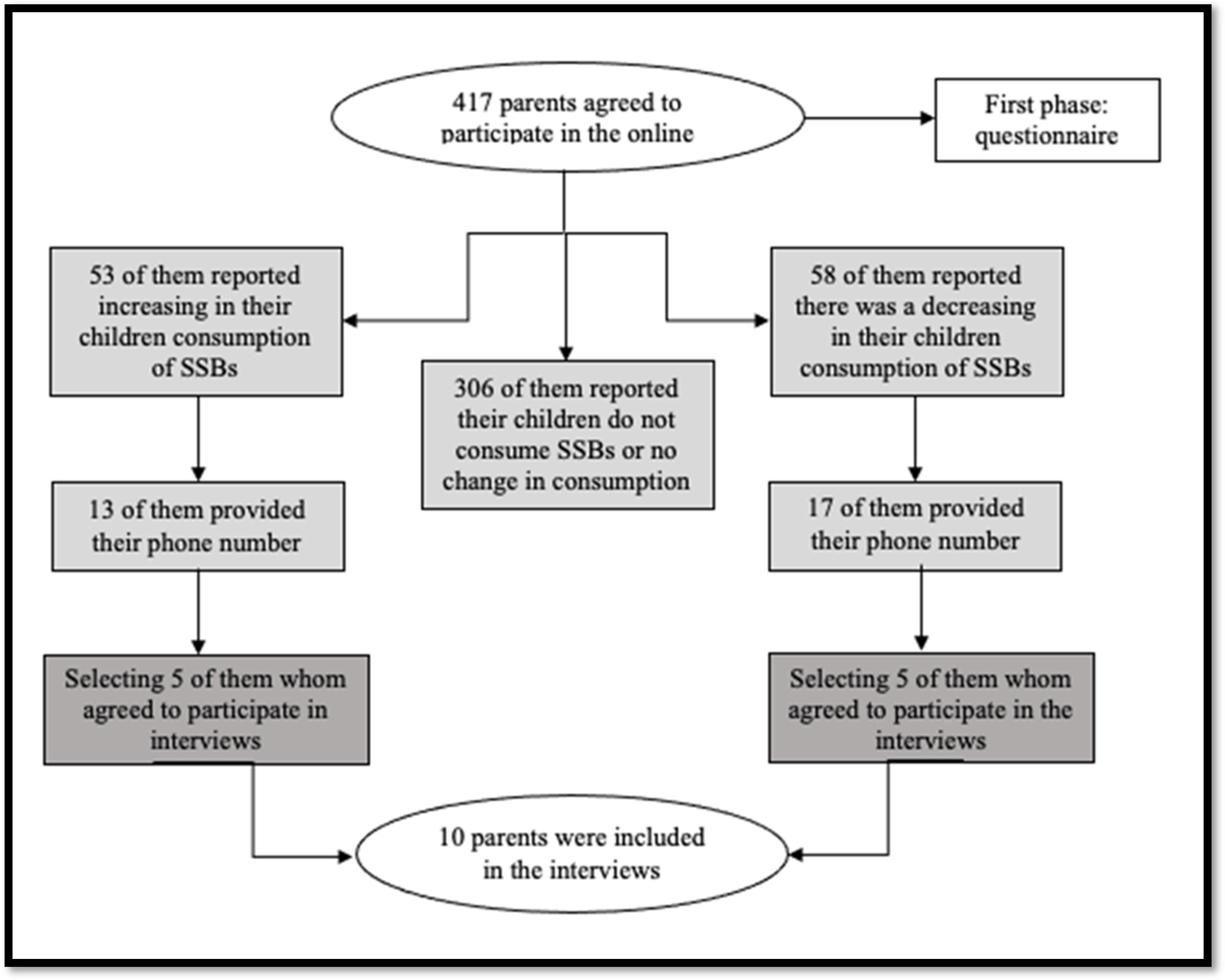
2.2. Sample Size and Sampling Technique
2.3. First Phase: Questionnaire
2.4. Second Phase: Interviews
2.5. Data Analysis
3. Results
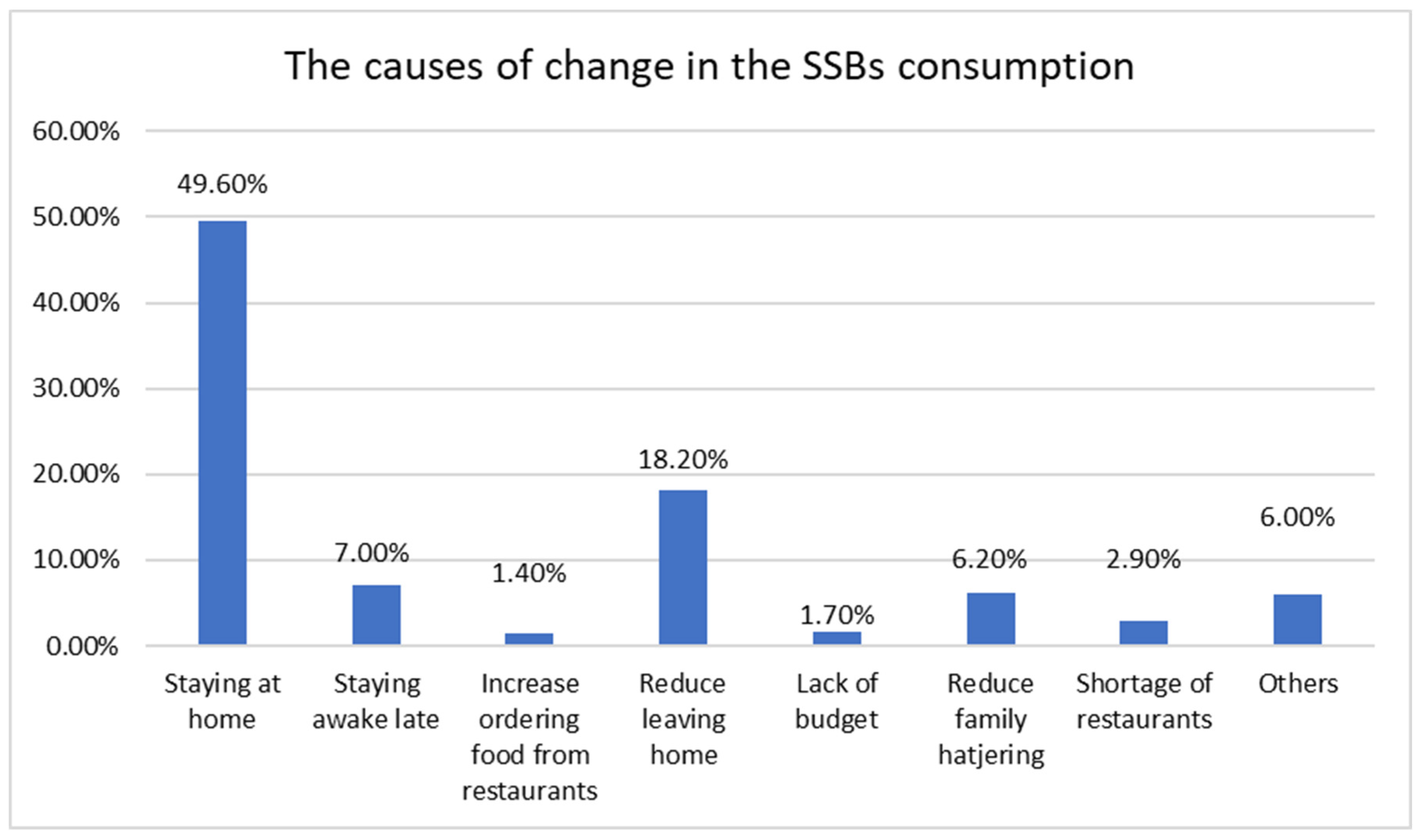
3.1. Results of the First Phase (Questionnaire)
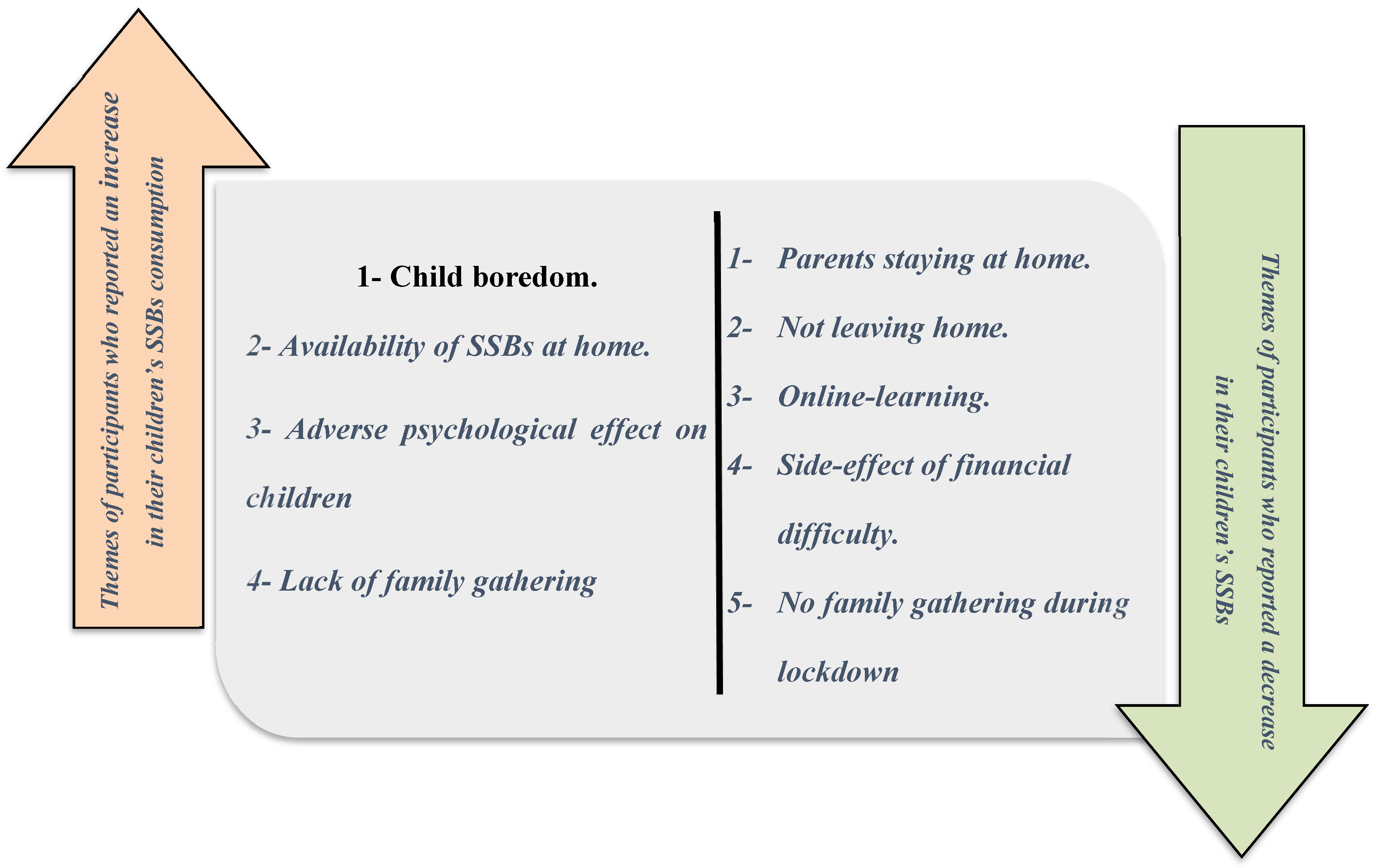
3.2. Results of the Second Phase (Interview)
- Child boredom
- 2.
- Availability of SSBs at home
- 3.
- Adverse psychological effect on children
- 4.
- Lack of family gathering
- 5.
- Parents staying at home.
- 6.
- Not leaving home.
- 7.
- Online-learning.
- 8.
- Side-effect of financial difficulty.
- 9.
- No family gathering during lockdown.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- 1-
- What is the nationality of the child?
- 2-
- What is the relationship with the child?
- 3-
- How old are you?
- 4-
- What is the marital status?
- 5-
- What is the mother’s level of education?
- 6-
- What is the father’s level of education?
- 7-
- Number of Children?
- 8-
- What is the monthly family income?
- 9-
- What is the age of your child
- 10-
- How much does a child weight in Kg?
- 11-
- How tall is the child in Cm?
- 12-
- Who does the child live with?
- 13-
- Have you ever taken your child to the Dentist?
- Yes
- No
- I do not know
- I did not remember
- 14-
- Has the child complained of any dental pain during the past year?
- The child did not complain of toothache
- Yes, once
- Yes, Twice
- Yes, three times
- Yes, more than three times
- I do not know
- I did not remember
- 15-
- When one of your children complains of toothache, do you:
- Give the child a sedative
- Give the child some antibiotics
- Go to the Dentist
- Go to the Pharmacist
- Seek other medical care
- Use herbal medicine
- You ask the child about the tooth that hurts until you take it out
- Family consulting
- Do nothing, and often get better on their own
- None of my children have ever complained of toothache before
- 16-
- Did your child’s consumption of soft drinks changed during the lockdown?
- 17-
- Did your child’s consumption of Juices changed during the lockdown?
- 18-
- Did your child’s consumption of Milk with flavors changed during the lockdown?
- 19-
- If there is a change in the consumption of the child during the lockdown (whether its increases or decreases), please choose the reason (more than on potion can be selected):
- Stay at home
- Stay up late
- Increase ordering food from restaurants
- Reduce leaving home
- Lack of budget
- Reduce family gathering
- Shortage or restaurants
- Other
- 20-
- If the answer in the previous question was due to other reason, please clarify them?
- 21-
- Does taxation affect your child’s consumption of SSBs?
- Yes
- No
Appendix B
- Tell me about yourself?
- How old are you?
- Are you married?
- Tell me about your education? and what is your academic major? and what is the last degree certificate you obtained?
- Are you working? What is your occupation (job)? How many hours do you spend on your work?
- How many kids do you have?
- Who is taken care of your children during your working hours? Is this changed during a lockdown?
- Tell me about the place you are currently live in?
- Are you live with your family in a big house or a small one?
- Is it the same building that your family lived in?
- Do you have a regular family gathering that has a certain place and time?
- Tell me about your work during the lockdown, was it online or not?
- What is your child’s age?
- Tell me about your child’s oral health?
- What about tooth brushing? Prompts (regular, before bedtime)
- How many times did your brush his\her teeth?
- What about dental visits? Prompts (regular, fluoride)
- What are the reasons for a child’s dental visit usually?
- Tell me about your child dietary habit? Who made the decision of what to buy or eat and cook?
- What do you think about your child diet? healthy diet or not? and tell me about the snacks and meals?
- What is the content of meals and snacks?
- Let us now speak about sugar sweetened beverages (SSBs)? And when your child consuming these drinks? prompts (weekday or weakened, with meals or between meals, at home or with family gathering).
- What about food shopping? and who is responsible for the grocery for home, is it you or the father? Do you take him with you? You let him pick what he wants?
- Tell me about buying SSBs? Is it the child picking from the grocery shelf or it is your choice? Do you buy one piece or cartoon?
- What is the favorite choices drinks of your child during shopping? and who is made the decision, is it yours or your child?
- Tell me more about availability of SSBs consumption on the home?
- Are SSBs usually available at home for the child? Is it a child’s choice?
- Does anyone in your family like to drink SSBs (his brother, his father)? Is he sharing the drink with others or father?
- What is the frequency of consuming SSBs? Is it daily, or at weekend? is it only on occasion and gathering?
- During the lockdown period: (total and partial lockdown hours)
- Was SSBs always available at home?
- What do you think more consumption of SSBS or less during the lockdown? And why?
- What about sharing the drink with others or father during the lockdown?
- How much time he is consumed the SSBs? Is it daily, or at weekend? is it only on occasion and gathering?
- Why do think about the change in the consumption during lockdown? Prompts (decrease, increases, family gathering- normal shopping- financial reasons- treats during lockdown)
- Has the consumption of SSBs changed? Why does SSB’s consumption of your child increase or decrease during a lockdown?
- What is the main reason for this change?
- What do you think about absence of parties and family gatherings during lockdown?
- What about family gatherings? Tell me more about this.
- What do you think about restriction of the accessibility to markets and shopping centers?
- What do you think about financial problems during the lockdown? Prompts (some families were affected financially during the lockdown)
Appendix C

{kind=link}
{kind=link}
{kind=link}
| Variable | Increased SSB | Decreased SSB | Child Not Consuming | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| AOR | 95% CI | p Value | AOR | 95% CI | p Value | AOR | 95% CI | p Value | ||
| History of pain in last year | 1.13 | 0.88–1.46 | 0.32 | 1.50 | 1.18–1.92 | 0.001 * | 0.82 | 0.67–1.01 | 0.07 | |
| Mother education | Less than secondary | 1.99 | 0.21–18.5 | 0.54 | 0.43 | 0.27–7.03 | 0.56 | 1.73 | 0.30–9.82 | 0.53 |
| Higher than secondary | 1.81 | 0.48–6.85 | 0.37 | 1.66 | 0.42–6.41 | 0.46 | 1.82 | 0.77–4.28 | 0.16 | |
| Higher education | 1.00 | 1.00 | 1.00 | |||||||
| Father education | Less than secondary | 1.38 | 0.27–6.96 | 0.69 | 1.28 | 1.27–7.09 | 0.69 | 0.31 | 0.08–1.08 | 0.06 |
| Higher than secondary | 1.15 | 0.34–3.84 | 0.81 | 1.07 | 0.31–3.66 | 0.90 | 0.56 | 0.25–1.24 | 0.15 | |
| Higher education | 1.00 | 1.00 | 1.00 | |||||||
| Child visit to the dentist | Yes | 1.27 | 0.58–2.77 | 0.53 | 1.11 | 0.51–2.4 | 0.77 | 1.21 | 0.69–2.13 | 0.49 |
| No | 1.00 | 1.00 | 1.00 | |||||||
| Marital status | Married | 0.38 | 0.10–1.45 | 0.15 | 0.39 | 0.10–1.50 | 0.17 | 0.62 | 0.21–1.84 | 0.39 |
| Single/Divorced | 1.00 | 1.00 | 1.00 | |||||||
| The child lives | One parent | 6.42 | 0.00–6.89 | 0.99 | 0.95 | 0.53–17.12 | 0.97 | 1.67 | 0.22–12.37 | 0.61 |
| Both parents | 2.46 | 0.47–12.83 | 0.28 | 1.6 | 0.37–7.15 | 0.50 | 2.17 | 0.75–6.28 | 0.15 | |
| Others | 1.00 | 1.00 | 1.00 | |||||||
| Monthly income | Low income | 0.79 | 0.27–2.11 | 0.67 | 0.73 | 0.25–2.08 | 0.55 | 1.73 | 0.79–3.79 | 0.17 |
| Moderate | 0.85 | 0.37–1.95 | 0.70 | 0.86 | 0.38–1.97 | 0.73 | 1.05 | 0.57–1.93 | 0.87 | |
| High | 1.00 | 1.00 | 1.00 | |||||||
References
- Nicklaus, S. Development of food variety in children. Appetite 2009, 52, 253–255. [Google Scholar] [CrossRef] [PubMed]
- Alsubaie, A.S.R. Consumption and correlates of sweet foods, carbonated beverages, and energy drinks among primary school children in Saudi Arabia. Saudi Med. J. 2017, 38, 1045. [Google Scholar] [CrossRef]
- Larsen, J.K.; Hermans, R.C.; Sleddens, E.F.; Engels, R.C.; Fisher, J.O.; Kremers, S.P. How parental dietary behavior and food parenting practices affect children’s dietary behavior. Interacting sources of influence? Appetite 2015, 89, 246–257. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Statistics 2015; World Health Organization: Geneva, Switzerland, 2015.
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015.
- Pyne, V.; Macdonald, I.A. Update on carbohydrates and health: The relevance of the Scientific Advisory Committee on Nutrition report for children. Arch. Dis. Child. 2016, 101, 876–880. [Google Scholar] [CrossRef]
- Wang, Y.C.; Bleich, S.N.; Gortmaker, S.L. Increasing caloric contribution from sugar-sweetened beverages and 100% fruit juices among US children and adolescents, 1988–2004. Pediatrics 2008, 121, e1604–e1614. [Google Scholar] [CrossRef]
- Jevdjevic, M.; Trescher, A.-L.; Rovers, M.; Listl, S. The caries-related cost and effects of a tax on sugar-sweetened beverages. Public Health 2019, 169, 125–132. [Google Scholar] [CrossRef]
- Sánchez-Pimienta, T.G.; Batis, C.; Lutter, C.K.; Rivera, J.A. Sugar-sweetened beverages are the main sources of added sugar intake in the Mexican population. J. Nutr. 2016, 146, 1888S–1896S. [Google Scholar] [CrossRef]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.-P.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes: A meta-analysis. Diabetes Care 2010, 33, 2477–2483. [Google Scholar] [CrossRef]
- Moynihan, P.; Kelly, S. Effect on caries of restricting sugars intake: Systematic review to inform WHO guidelines. J. Dent. Res. 2014, 93, 8–18. [Google Scholar] [CrossRef]
- Hong, J.; Whelton, H.; Douglas, G.; Kang, J. Consumption frequency of added sugars and UK children’s dental caries. Community Dent. Oral Epidemiol. 2018, 46, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Chi, D.L.; Scott, J.M. Added sugar and dental caries in children: A scientific update and future steps. Dent. Clin. 2019, 63, 17–33. [Google Scholar]
- Manal, A.-M.; AlKattan, H.; ALBukhari, L.; El Meligy, O. Assessment of Dental Decay in a Group of Children in Jeddah, Kingdom of Saudi Arabia. Int. J. Clin. Pediatr. Dent. 2019, 12, 423. [Google Scholar]
- Alsukait, R.; Bleich, S.; Wilde, P.; Singh, G.; Folta, S. Sugary drink excise tax policy process and implementation: Case study from Saudi Arabia. Food Policy 2020, 90, 101789. [Google Scholar] [CrossRef]
- Megally, R.; Al-Jawaldeh, A. Impact of sin taxes on consumption volumes of sweetened beverages and soft drinks in Saudi Arabia. F1000Research 2020, 9, 1117. [Google Scholar] [CrossRef]
- Alhabdan, Y.A.; Albeshr, A.G.; Yenugadhati, N.; Jradi, H. Prevalence of dental caries and associated factors among primary school children: A population-based cross-sectional study in Riyadh, Saudi Arabia. Environ. Health Prev. Med. 2018, 23, 60. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary choices and habits during COVID-19 lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 lockdown on lifestyle behaviors in children with obesity living in Verona, Italy: A longitudinal study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef]
- Adair, P.; Pine, C.; Burnside, G.; Nicoll, A.; Gillett, A.; Anwar, S.; Broukal, Z.; Chestnutt, I.; Declerck, D.; Feng, X. Familial and cultural perceptions and beliefs of oral hygiene and dietary practices among ethnically and socio-economically diverse groups. J. Dent. Res. 2003, 82, B66. [Google Scholar]
- Kang, H. Sample size determination and power analysis using the G* Power software. J. Educ. Eval. Health Prof. 2021, 18, 1149215. [Google Scholar] [CrossRef]
- Peters, J.; Parletta, N.; Lynch, J.; Campbell, K. A comparison of parental views of their pre-school children’s ‘healthy’versus ‘unhealthy’diets. A qualitative study. Appetite 2014, 76, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Centralstat. Family Income Based on the Central Statistics and Information Website of Saudi Arabia 2013. Available online: http://www.cdsi.gov.sa/english/ (accessed on 4 April 2020).
- Snuggs, S.; McGregor, S. Food & meal decision making in lockdown: How and who has Covid-19 affected? Food Qual. Prefer. 2021, 89, 104145. [Google Scholar] [PubMed]
- Bennett, G.; Young, E.; Butler, I.; Coe, S. The impact of lockdown during the COVID-19 outbreak on dietary habits in various population groups: A scoping review. Front. Nutr. 2021, 8, 626432. [Google Scholar] [CrossRef]
- Poudel, P.B.; Poudel, M.R.; Gautam, A.; Phuyal, S.; Tiwari, C.K.; Bashyal, N.; Bashyal, S. COVID-19 and its global impact on food and agriculture. J. Biol. Today’s World 2020, 9, 221–225. [Google Scholar]
- Battram, D.S.; Piché, L.; Beynon, C.; Kurtz, J.; He, M. Sugar-sweetened beverages: Children’s perceptions, factors of influence, and suggestions for reducing intake. J. Nutr. Educ. Behav. 2016, 48, 27–34.e21. [Google Scholar] [CrossRef] [PubMed]
- Boyland, E.J.; Halford, J.C. Television advertising and branding. Effects on eating behaviour and food preferences in children. Appetite 2013, 62, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Philippe, K.; Chabanet, C.; Issanchou, S.; Monnery-Patris, S. Child eating behaviors, parental feeding practices and food shopping motivations during the COVID-19 lockdown in France:(How) did they change? Appetite 2021, 161, 105132. [Google Scholar] [CrossRef]
- Alshehri, L.M.; Al Agha, A.E. Impact of Covid-19 Lockdown on the Unhealthy Dietary Habits and Physical Activity of Children and Adolescents Living in the Kingdom of Saudi Arabia. Ann. Med. Health Sci. Res. 2021, 11, 26–31. [Google Scholar]
- Pujia, R.; Ferro, Y.; Maurotti, S.; Khoory, J.; Gazzaruso, C.; Pujia, A.; Montalcini, T.; Mazza, E. The Effects of COVID-19 on the Eating Habits of Children and Adolescents in Italy: A Pilot Survey Study. Nutrients 2021, 13, 2641. [Google Scholar] [CrossRef]
- Alhareky, M.; Bedi, S.; AlMulhim, A.; El Tantawi, M.; Farooqi, F.A.; AlHumaid, J. Impact of Sugar Tax on Sugar-sweetened Beverage Consumption among Saudi Schoolchildren. Oral Health Prev. Dent. 2021, 19, 189–194. [Google Scholar]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors influencing children’s eating behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [PubMed]
- Alsubaie, A.S.R. Oral health-related behaviors and dental pain among children in Saudi Arabia. J. Int. Oral Health 2019, 11, 1. [Google Scholar] [CrossRef]
- Adachi-Mejia, A.; Longacre, M.; Skatrud-Mickelson, M.; Li, Z.; Purvis, L.; Titus, L.; Beach, M.; Dalton, M. Variation in access to sugar-sweetened beverages in vending machines across rural, town and urban high schools. Public Health 2013, 127, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Łuszczki, E.; Bartosiewicz, A.; Pezdan-Śliż, I.; Kuchciak, M.; Jagielski, P.; Oleksy, Ł.; Stolarczyk, A.; Dereń, K. Children’s Eating Habits, Physical Activity, Sleep, and Media Usage before and during COVID-19 Pandemic in Poland. Nutrients 2021, 13, 2447. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, D.; Shrivastava, P. Interview as a Method for Qualitative Research; Southern Cross University and the Southern Cross Institute of Action Research in Lismore; SCIAR: Bar Beach, Australia, 2002. [Google Scholar]
- O’Connor, C.; Joffe, H. Intercoder reliability in qualitative research: Debates and practical guidelines. Int. J. Qual. Methods 2020, 19, 1609406919899220. [Google Scholar] [CrossRef]
- Booth, A.; Hannes, K.; Harden, A.; Noyes, J.; Harris, J. COREQ (Consolidated Criteria for Reporting Qualitative Studies). 2014. Available online: https://onlinelibrary.wiley.com/doi/10.1002/9781118715598.ch21 (accessed on 4 April 2020).
- Etikan, I.; Musa, S.A.; Alkassim, R.S. Comparison of convenience sampling and purposive sampling. Am. J. Theor. Appl. Stat. 2016, 5, 1–4. [Google Scholar] [CrossRef]



| Socio-Demographic Variable | Number (n = 417) | Percentage (100%) |
|---|---|---|
| Child nationality | ||
| Saudi | 373 | 89.4 |
| Non-Saudi | 44 | 10.6 |
| Participant | ||
| Mother | 348 | 83.4 |
| Father | 30 | 7.2 |
| Other | 39 | 9.4 |
| Marital status | ||
| Married | 381 | 91.4 |
| Single/Divorced | 36 | 8.6 |
| Mother’s Level of Education | ||
| Less than Secondary | 14 | 3.4 |
| Secondary/University | 344 | 82.4 |
| Higher education | 59 | 20.6 |
| Father’s Level of Education | ||
| Less than Secondary | 31 | 7.4 |
| Secondary/University | 300 | 71.9 |
| Higher education | 86 | 17.7 |
| Number of Children | ||
| One | 32 | 7.7 |
| Two | 100 | 24 |
| Three | 101 | 24.2 |
| Four or more | 184 | 44.1 |
| Monthly Family Income | ||
| High > 1000 SR | 224 | 53.7 |
| Moderate 7000–10000 SR | 117 | 28.1 |
| Low < 7000 SR | 76 | 18.2 |
| Age of participant parent | ||
| <20 | 19 | 4.6 |
| 20–30 | 90 | 21.6 |
| 31–40 | 195 | 46.7 |
| >40 | 113 | 27.1 |
| Child Lives with | ||
| One parent | 26 | 6.2 |
| Both parents | 385 | 92.3 |
| Others | 6 | 1.4 |
| SSBs Type | Increase | Decrease | Child does not Consume SSBs/no Change | Total N = 417 | |||
|---|---|---|---|---|---|---|---|
| Frequency | % | Frequency | % | Frequency | % | Total% | |
| Soft Drinks | 53 | 12.7 | 58 | 13.9 | 306 | 73.4 | 100 |
| Fruit Juice | 87 | 20.8 | 115 | 27.6 | 215 | 51.6 | 100 |
| Flavored Milk | 63 | 15.1 | 93 | 22.3 | 261 | 62.6 | 100 |
| Socio-Demographic Variable N = 417 | Increase | Decrease | Child does not Consume SSBs/no Change | p-Value * | |||
|---|---|---|---|---|---|---|---|
| Frequency | % | Frequency | % | Frequency | % | ||
| Mother’s Education Level | 0.56 $ | ||||||
| Less than Secondary | 7 | 1.67 | 1 | 0.23 | 6 | 1.43 | |
| Secondary/University | 179 | 42.92 | 52 | 12.47 | 113 | 27.09 | |
| Higher education | 34 | 8.15 | 5 | 1.19 | 20 | 4.79 | |
| Father’s education level | |||||||
| Less than Secondary | 11 | 2.63 | 6 | 1.43 | 14 | 3.35 | 0.10 |
| Secondary/University | 153 | 36.69 | 45 | 10.79 | 102 | 24.46 | |
| Higher education | 56 | 13.42 | 7 | 1.67 | 23 | 5.51 | |
| Parents marital status | |||||||
| Married | 200 | 47.96 | 52 | 12.47 | 128 | 30.69 | 0.66 |
| Single/Divorced | 20 | 4.79 | 6 | 1.43 | 11 | 2.63 | |
| Family average monthly income | |||||||
| High >1000 SR | 44 | 10.55 | 10 | 2.39 | 22 | 5.27 | 0.96 |
| Moderate 7000–10000 SR | 59 | 14.14 | 18 | 4.31 | 40 | 9.59 | |
| Low < 7000 SR | 117 | 28.05 | 30 | 7.19 | 77 | 18.46 | |
| Child lives with whom | |||||||
| One parent | 5 | 1.19 | 1 | 0.23 | 2 | 0.47 | 0.76 $ |
| Both parents | 206 | 49.40 | 54 | 12.94 | 128 | 30.69 | |
| Others | 9 | 2.15 | 3 | 0.71 | 9 | 2.15 | |
| Visiting the dentist last year | |||||||
| Yes | 144 | 34.53 | 41 | 9.83 | 90 | 21.58 | 0.78 |
| No | 76 | 18.22 | 17 | 4.07 | 49 | 11.75 | |
| Variable | Increased SSBs (n = 53) $ | Decreased SSBs (n = 58) $ | |||
|---|---|---|---|---|---|
| AOR | p Value | AOR | p Value | ||
| Mother’s level of education | Less than secondary | 0.49 | 0.55 | 1.24 | 0.88 |
| Secondary/University | 0.54 | 0.36 | 0.69 | 0.58 | |
| Higher education | 1.00 | 1.00 | |||
| Father’s level of education | Less than secondary | 0.62 | 0.58 | 0.51 | 0.46 |
| Secondary/University | 0.81 | 0.73 | 0.65 | 0.48 | |
| Higher education | 1.00 | ||||
| Parents marital status | Married | 2.48 | 0.21 | 2.1 | 0.31 |
| Single/Divorced | 1.00 | 1.00 | |||
| Family average monthly income | Low income | 1.11 | 0.85 | 1.04 | 0.93 |
| Moderate | 1.14 | 0.78 | 1.08 | 0.85 | |
| High | 1.00 | 1.00 | |||
| Child lives with whom | One parent | 0.62 | 0.99 | 0.74 | 0.85 |
| Both parents | 0.47 | 0.39 | 0.50 | 0.38 | |
| Others | 1.00 | 1.00 | |||
| Visiting the dentist last year | Yes | 0.72 | 0.44 | 0.78 | 0.54 |
| No | 1.00 | 1.00 | |||
| History of pain in the last year | 0.81 | 0.14 | 0.64 | 0.001 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baghlaf, K.; Bormah, D.; Hakami, A.; Bagher, S.M. The Impact of the COVID-19 Lockdown on Sugar-Sweetened Beverage Consumption in Children in Saudi Arabia: A Mixed-Methods Study. Nutrients 2022, 14, 4972. https://doi.org/10.3390/nu14234972
Baghlaf K, Bormah D, Hakami A, Bagher SM. The Impact of the COVID-19 Lockdown on Sugar-Sweetened Beverage Consumption in Children in Saudi Arabia: A Mixed-Methods Study. Nutrients. 2022; 14(23):4972. https://doi.org/10.3390/nu14234972
Chicago/Turabian StyleBaghlaf, Khlood, Dania Bormah, Anwar Hakami, and Sara M. Bagher. 2022. "The Impact of the COVID-19 Lockdown on Sugar-Sweetened Beverage Consumption in Children in Saudi Arabia: A Mixed-Methods Study" Nutrients 14, no. 23: 4972. https://doi.org/10.3390/nu14234972
APA StyleBaghlaf, K., Bormah, D., Hakami, A., & Bagher, S. M. (2022). The Impact of the COVID-19 Lockdown on Sugar-Sweetened Beverage Consumption in Children in Saudi Arabia: A Mixed-Methods Study. Nutrients, 14(23), 4972. https://doi.org/10.3390/nu14234972