

Postprandial Glycemic and Insulinemic Response by a Brewer’s Spent Grain Extract-Based Food Supplement in Subjects with Slightly Impaired Glucose Tolerance: A Monocentric, Randomized, Cross-Over, Double-Blind, Placebo-Controlled Clinical Trial
 , ,
, ,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. BSG Extract-Based Food Supplement, and Placebo Used in the Clinical Study
2.2. Chemical Characterization of BSG Extract
2.2.1. Total Dietary Fiber Determination
2.2.2. Glucose, Arabinose, Xylose, Total Β-Glucans, Total Arabinoxylans, and Resistant Starch Determination
2.2.3. Water and Alkali Extractable Arabinoxylans
2.2.4. Total Polyphenol Content and Ferulic Acid Determinations
Simulated In Vitro Oral-Gastric-Duodenal Digestion Process of BSG Extract
Total Polyphenol Content
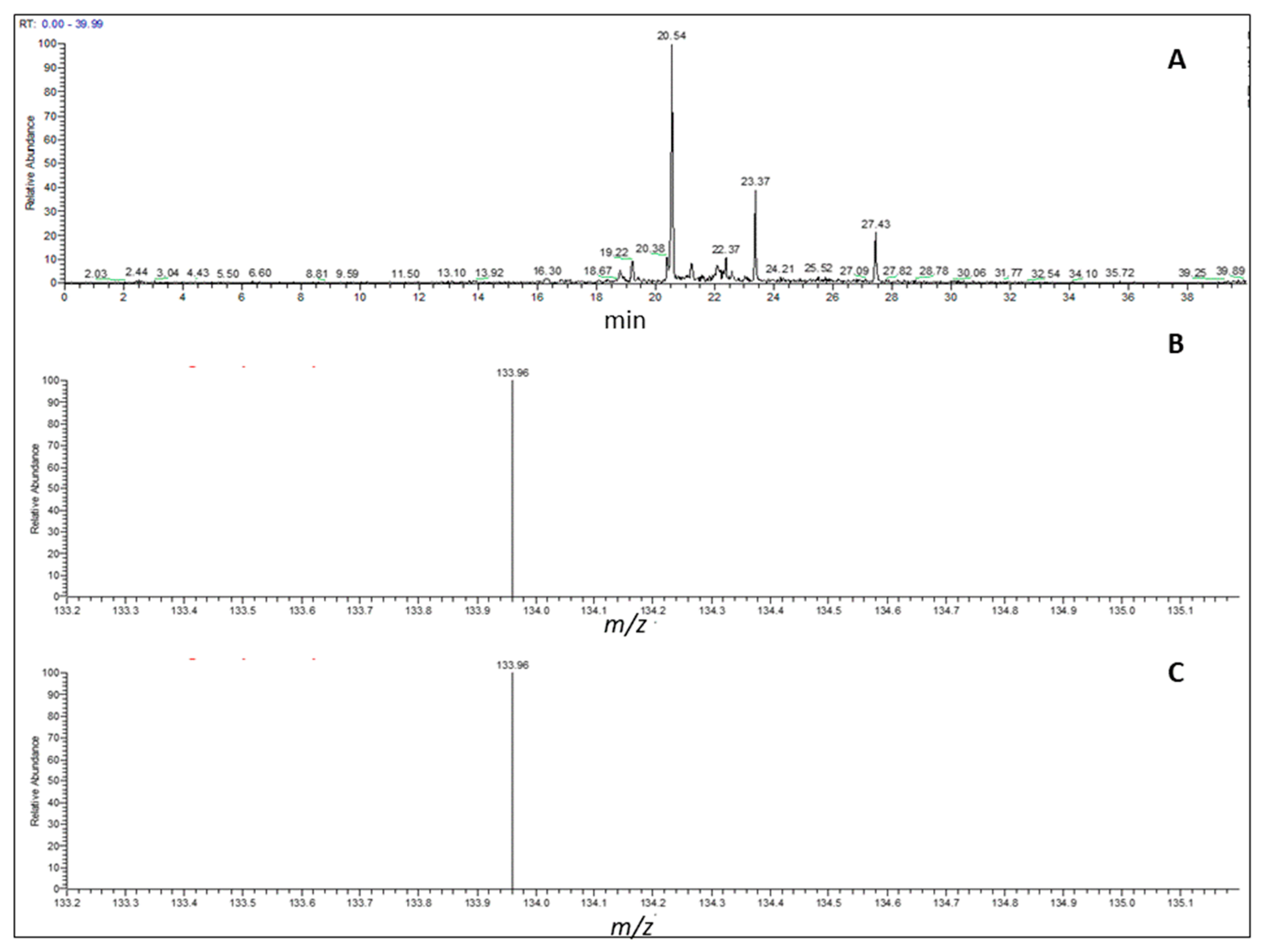
UHPLC-MS Analysis and Quantification of Ferulic Acid after Digestion
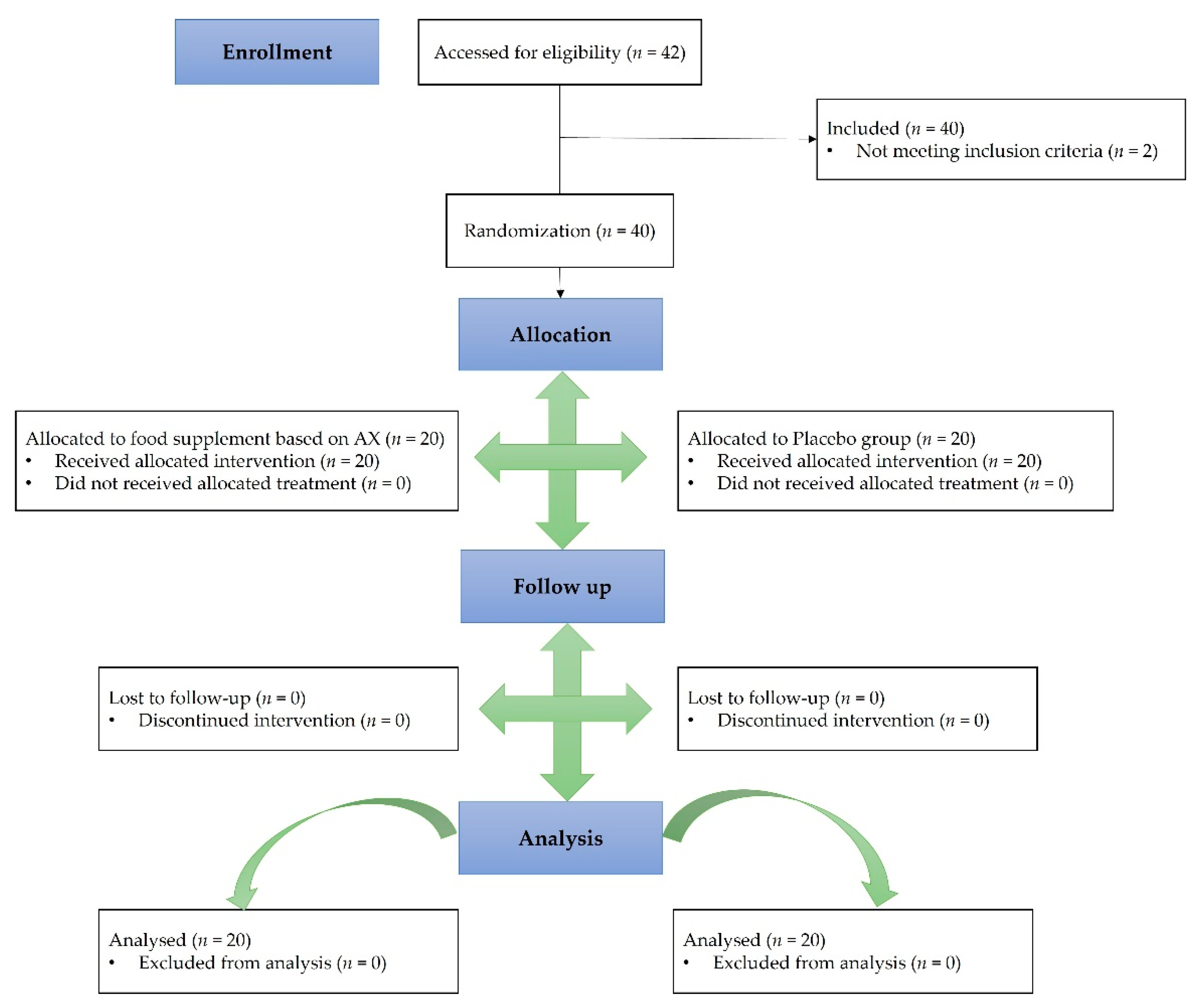
2.3. Clinical Trial Design
2.3.1. Study Population
2.3.2. Outcomes of the Study
2.3.3. Safety
2.4. Statistical Analysis
3. Results
3.1. Chemical Characterization of BSG Extract
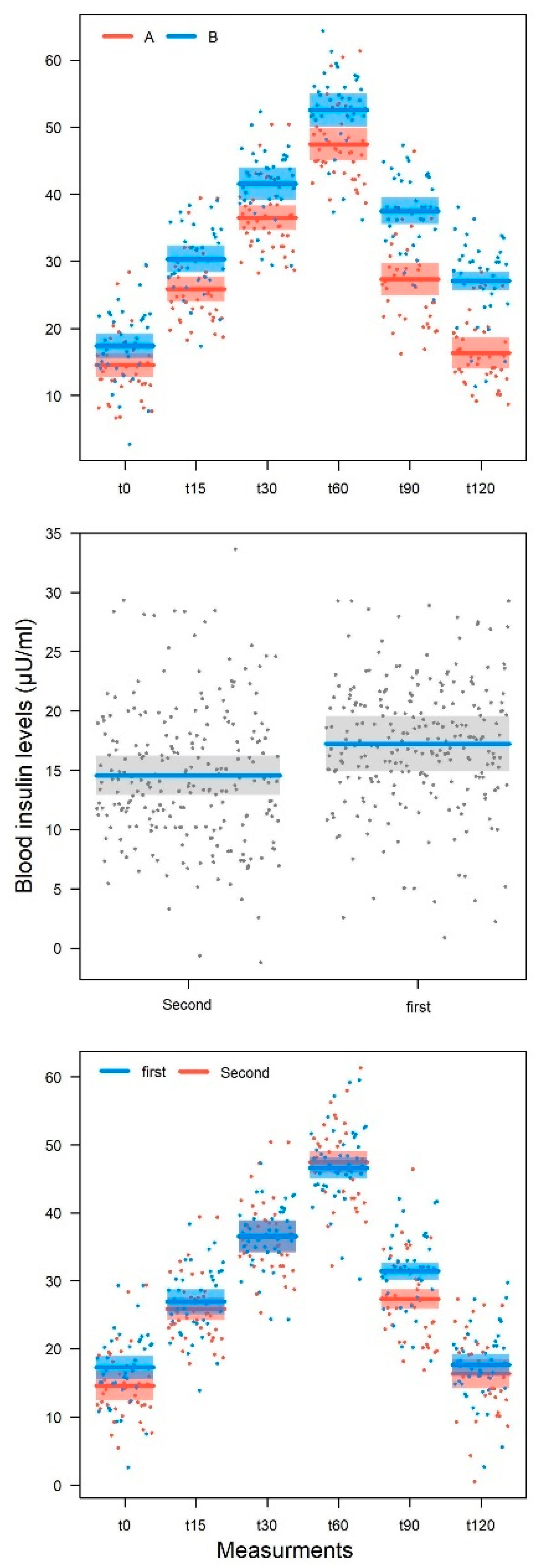
3.2. Clinical Trial
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Filippis, A.; Ullah, H.; Baldi, A.; DaCrema, M.; Esposito, C.; Garzarella, E.U.; Santarcangelo, C.; Tantipongpiradet, A.; Daglia, M. Gastrointestinal Disorders and Metabolic Syndrome: Dysbiosis as a Key Link and Common Bioactive Dietary Components Useful for their Treatment. Int. J. Mol. Sci. 2020, 21, 4929. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.-S.; Byeon, S.; Shin, D.-M. Sources of Dietary Fiber are Differently Associated with Prevalence of Depression. Nutrition 2020, 12, 2813. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Li, S.; Song, X.; Li, Z.; Zhang, D. Exploration of the association between dietary fiber intake and depressive symptoms in adults. Nutrition 2018, 54, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Berding, K.; Carbia, C.; Cryan, J.F. Going with the Grain: Fiber, Cognition, and the Microbiota-Gut-Brain-Axis. Exp. Biol. Med. 2021, 246, 796–811. [Google Scholar] [CrossRef]
- Pascale, A.; Marchesi, N.; Govoni, S.; Coppola, A.; Gazzaruso, C. The role of gut microbiota in obesity, diabetes mellitus, and effect of metformin: New insights into old diseases. Curr. Opin. Pharmacol. 2019, 49, 1–5. [Google Scholar] [CrossRef]
- Chen, Z.; Li, S.; Fu, Y.; Li, C.; Chen, D.; Chen, H. Arabinoxylan structural characteristics, interaction with gut microbiota and potential health functions. J. Funct. Foods 2019, 54, 536–551. [Google Scholar] [CrossRef]
- Zhang, S.; Li, W.; Smith, C.J.; Musa, H. Cereal-Derived Arabinoxylans as Biological Response Modifiers: Extraction, Molecular Features, and Immune-Stimulating Properties. Crit. Rev. Food Sci. Nutr. 2015, 55, 1035–1052. [Google Scholar] [CrossRef]
- Ain, H.B.U.; Saeed, F.; Ahmad, N.; Imran, A.; Niaz, B.; Afzaal, M.; Imran, M.; Tufail, T.; Javed, A. Functional and health-endorsing properties of wheat and barley cell wall’s non-starch polysaccharides. Int. J. Food Prop. 2018, 21, 1463–1480. [Google Scholar] [CrossRef]
- Ndeh, D.; Gilbert, H.J. Biochemistry of complex glycan depolymerisation by the human gut microbiota. FEMS Microbiol. Rev. 2018, 42, 146–164. [Google Scholar] [CrossRef]
- Lynch, K.M.; Strain, C.R.; Johnson, C.; Patangia, D.; Stanton, C.; Koc, F.; Gil-Martinez, J.; O’Riordan, P.; Sahin, A.W.; Ross, R.P.; et al. Extraction and characterisation of arabinoxylan from brewers spent grain and investigation of microbiome modulation potential. Eur. J. Nutr. 2021, 60, 4393–4411. [Google Scholar] [CrossRef]
- Chen, H.; Chen, Z.; Fu, Y.; Liu, J.; Lin, S.; Zhang, Q.; Liu, Y.; Wu, D.; Lin, D.; Han, G.; et al. Structure, Antioxidant, and Hypoglycemic Activities of Arabinoxylans Extracted by Multiple Methods from Triticale. Antioxidants 2019, 8, 584. [Google Scholar] [CrossRef] [PubMed]
- Yuwang, P.; Sulaeva, I.; Hell, J.; Henniges, U.; Böhmdorfer, S.; Rosenau, T.; Chitsomboon, B.; Tongta, S. Phenolic compounds and antioxidant properties of arabinoxylan hydrolysates from defatted rice bran. J. Sci. Food Agric. 2018, 98, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Lu, Z.X.; Walker, K.Z.; Muir, J.G.; Mascara, T.; O’Dea, K. Arabinoxylan fiber, a byproduct of wheat flour processing, reduces the postprandial glucose response in normoglycemic subjects. Am. J. Clin. Nutr. 2000, 71, 1123–1128. [Google Scholar] [CrossRef]
- Lu, Z.X.; Walker, K.Z.; Muir, J.G.; O’Dea, K. Arabinoxylan fibre improves metabolic control in people with Type II diabetes. Eur. J. Clin. Nutr. 2004, 58, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Möhlig, M.; Koebnick, C.; Weickert, M.O.; Lueder, W.; Otto, B.; Steiniger, J.; Twilfert, M.; Meuser, F.; Pfeiffer, A.F.H.; Zunft, H.J. Arabinoxylan-enriched Meal Increases Serum Ghrelin Levels in Healthy Humans. Horm. Metab. Res. 2005, 37, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Venn, B.J.; Green, T.J. Glycemic index and glycemic load: Measurement issues and their effect on diet–disease relationships. Eur. J. Clin. Nutr. 2007, 61, S122–S131. [Google Scholar] [CrossRef] [PubMed]
- Christensen, K.L.; Hedemann, M.S.; Lærke, H.N.; Jørgensen, H.; Mutt, S.J.; Herzig, K.-H.; Knudsen, K.E.B. Concentrated Arabinoxylan but not Concentrated β-Glucan in Wheat Bread Has Similar Effects on Postprandial Insulin as Whole-Grain Rye in Porto-arterial Catheterized Pigs. J. Agric. Food Chem. 2013, 61, 7760–7768. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the Substantiation of Health Claims Related to Arabinoxylan Produced from Wheat Endosperm and Reduction of Post-prandial Glycaemic Responses (ID 830) Pursuant to Article 13 (1) of Regulation (EC) No 1924/2006. EFSA J. 2011, 9, 2205. [Google Scholar] [CrossRef]
- Jackowski, M.; Niedźwiecki, Ł.; Jagiełło, K.; Uchańska, O.; Trusek, A. Brewer’s Spent Grains—Valuable Beer Industry by-Product. Biomolecules 2020, 10, 1669. [Google Scholar] [CrossRef]
- Mitri, S.; Salameh, S.J.; Khelfa, A.; Leonard, E.; Maroun, R.G.; Louka, N.; Koubaa, M. Valorization of Brewers’ Spent Grains: Pretreatments and Fermentation, a Review. Fermentation 2022, 8, 50. [Google Scholar] [CrossRef]
- Buffington, J. The Economic Potential of Brewer’s Spent Grain (BSG) as a Biomass Feedstock. Adv. Chem. Eng. Sci. 2014, 04, 308–318. [Google Scholar] [CrossRef]
- Megazyme Total Dietary Fiber. Available online: https://www.megazyme.com/total-dietary-fiber-assay-kit (accessed on 24 February 2022).
- Bonjoch, N.P.; Tamayo, P.R. Protein content quantification by bradford method. In Handbook of Plant Ecophysiology Techniques; Roger, M.J.R., Ed.; Springer: Dordrecht, Netherlands, 2001; pp. 283–295. [Google Scholar]
- Megazyme D-Xylose. Available online: https://www.megazyme.com/d-xylose-assay-kit (accessed on 1 February 2020).
- Megazyme L-Arabinose & D-Galactose. Available online: https://www.megazyme.com/l-arabinose-d-galactose-assay-kit?sSearch=L-Arabinose%20&%20D-Galactose (accessed on 1 February 2022).
- Buksa, K.; Praznik, W.; Loeppert, R.; Nowotna, A. Characterization of water and alkali extractable arabinoxylan from wheat and rye under standardized conditions. J. Food Sci. Technol. 2016, 53, 1389–1398. [Google Scholar] [CrossRef] [PubMed]
- Minekus, M.; Alminger, M.; Alvito, P.; Ballance, S.; Bohn, T.; Bourlieu, C.; Carrière, F.; Boutrou, R.; Corredig, M.; Dupont, D.; et al. A Standardised Static in Vitro Digestion Method Suitable for Food–an International Consensus. Food Funct 2014, 5, 1113–1124. [Google Scholar] [CrossRef] [PubMed]
- Ullah, H.; Sommella, E.; Santarcangelo, C.; D’Avino, D.; Rossi, A.; Dacrema, M.; Di Minno, A.; Di Matteo, G.; Mannina, L.; Campiglia, P.; et al. Hydroethanolic Extract of Prunus domestica L.: Metabolite Profiling and In Vitro Modulation of Molecular Mechanisms Associated to Cardiometabolic Diseases. Nutrients 2022, 14, 340. [Google Scholar] [CrossRef]
- Bates, D.; Maechler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Soft. 2015, 67, 1–48. [Google Scholar]
- R Core Team, R. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: http://www.r-project.org/index.html (accessed on 3 April 2022).
- Escarpa, A.; González, M. Approach to the content of total extractable phenolic compounds from different food samples by comparison of chromatographic and spectrophotometric methods. Anal. Chim. Acta. 2001, 427, 119–127. [Google Scholar] [CrossRef]
- Calvert, M.; Blazeby, J.; Altman, D.G.; Revicki, D.A.; Moher, D.; Brundage, M.D.; CONSORT PRO Group, F.T. Reporting of Patient-Reported Outcomes in Randomized Trials: The CONSORT PRO Extension. JAMA 2013, 309, 814–822. [Google Scholar] [CrossRef]
- Simental-Mendía, L.E.; Rodríguez-Morán, M.; Guerrero-Romero, F. The Product of Fasting Glucose and Triglycerides as Surrogate for Identifying Insulin Resistance in Apparently Healthy Subjects. Metab. Syndr. Relat. Disord. 2008, 6, 299–304. [Google Scholar] [CrossRef]
- Baez-Duarte, B.G.; Zamora-Ginez, I.; González-Duarte, R.; Torres-Rasgado, E.; Ruiz-Vivanco, G.; Pérez-Fuentes, R. The Multidisciplinary Research Group of Diabetes Celis. Triglyceride/high-density lipoprotein cholesterol (TG/HDL-C) index as a reference criterion of risk for metabolic syndrome (MetS) and low insulin sensitivity in apparently healthy subjects. Gac. Med. Mex. 2017, 153, 152–158. [Google Scholar]
- Heallo, S.R.L. Idrolizzato Di Fibra Vegetale E Suoi Usi Nell’alimentazione Umana Ed Animale. Italian Patent N. 102019000005588, 2 March 2021. [Google Scholar]
- Slavin, J.L. Position of the American Dietetic Association: Health Implications of Dietary Fiber. J. Am. Diet. Assoc. 2008, 108, 1716–1731. [Google Scholar] [CrossRef]
- Birsan, R.I.; Wilde, P.; Waldron, K.W.; Rai, D.K. Recovery of Polyphenols from Brewer’s Spent Grains. Antioxidants 2019, 8, 380. [Google Scholar] [CrossRef] [PubMed]
- Meneses, N.G.T.; Martins, S.; Teixeira, J.A.; Mussatto, S.I. Influence of extraction solvents on the recovery of antioxidant phenolic compounds from brewer’s spent grains. Sep. Purif. Technol. 2013, 108, 152–158. [Google Scholar] [CrossRef]
- Carvalho, D.O.; Guido, L.F. A review on the fate of phenolic compounds during malting and brewing: Technological strategies and beer styles. Food Chem. 2021, 372, 131093. [Google Scholar] [CrossRef]
- Nankar, R.; Prabhakar, P.; Doble, M. Hybrid drug combination: Combination of ferulic acid and metformin as anti-diabetic therapy. Phytomedicine 2017, 37, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Mussatto, S.I.; Dragone, G.; Roberto, I.C. Ferulic and p-coumaric acids extraction by alkaline hydrolysis of brewer’s spent grain. Ind. Crop. Prod. 2007, 25, 231–237. [Google Scholar] [CrossRef]
- Papakonstantinou, E.; Oikonomou, C.; Nychas, G.; Dimitriadis, G.D. Effects of Diet, Lifestyle, Chrononutrition and Alternative Dietary Interventions on Postprandial Glycemia and Insulin Resistance. Nutrients 2022, 14, 823. [Google Scholar] [CrossRef]
- Dimitriadis, G.; Maratou, E.; Kountouri, A.; Board, M.; Lambadiari, V. Regulation of Postabsorptive and Postprandial Glucose Metabolism by Insulin-Dependent and Insulin-Independent Mechanisms: An Integrative Approach. Nutrients 2021, 13, 159. [Google Scholar] [CrossRef]
- Brand-Miller, J.C.; Stockmann, K.; Atkinson, F.; Petocz, P.; Denyer, G. Glycemic index, postprandial glycemia, and the shape of the curve in healthy subjects: Analysis of a database of more than 1000 foods. Am. J. Clin. Nutr. 2009, 89, 97–105. [Google Scholar] [CrossRef]
- Lightowler, H.; Thondre, S.; Holz, A.; Theis, S. Replacement of glycaemic carbohydrates by inulin-type fructans from chicory (oligofructose, inulin) reduces the postprandial blood glucose and insulin response to foods: Report of two double-blind, randomized, controlled trials. Eur. J. Nutr. 2018, 57, 1259–1268. [Google Scholar] [CrossRef]
- Chambers, E.S.; Byrne, C.S.; Morrison, D.J.; Murphy, K.G.; Preston, T.; Tedford, C.; Garcia-Perez, I.; Fountana, S.; Serrano-Contreras, J.I.; Holmes, E.; et al. Dietary supplementation with inulin-propionate ester or inulin improves insulin sensitivity in adults with overweight and obesity with distinct effects on the gut microbiota, plasma metabolome and systemic inflammatory responses: A randomised cross-over trial. Gut 2019, 68, 1430–1438. [Google Scholar] [CrossRef]
- Mauvais-Jarvis, F. Gender differences in glucose homeostasis and diabetes. Physiol. Behav. 2018, 187, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Lartey, A.H.; Li, X.; Li, Z.; Zhang, Q.; Wang, J. Age- and sex-specific profiles of temporal fasting plasma glucose variability in a population undergoing routine health screening. BMC Public Health. 2021, 21, 320. [Google Scholar] [CrossRef] [PubMed]
- Sicree, R.A.; Zimmet, P.Z.; Dunstan, D.W.; Cameron, A.J.; Welborn, T.A.; Shaw, J.E. Differences in height explain gender differences in the response to the oral glucose tolerance test-the AusDiab study. Diabet. Med. 2008, 25, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Dalla Man, C.; Campioni, M.; Basu, A.; Klee, G.; Toffolo, G.; Cobelli, C.; Rizza, R.A. Effects of Age and Sex on Postprandial Glucose Metabolism: Differences in Glucose Turnover, Insulin Secretion, Insulin Action, and Hepatic Insulin Extraction. Diabetes 2006, 55, 2001–2014. [Google Scholar] [CrossRef]
- Umpierrez, G.E.; Pasquel, F.J. Management of Inpatient Hyperglycemia and Diabetes in Older Adults. Diabetes Care 2017, 40, 509–517. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Average Nutritional Values | g/100 g of Product |
|---|---|
| Energy | 1601 kJ–378 kcal |
| Fats | 2.5 g |
| of which saturated fatty acids | 0.5 g |
| Carbohydrates | 74.5 g |
| of which sugars | 3.4 g |
| Dietary fibers | 4.8 g |
| Protein | 12.7 g |
| Salts | 1.3 g |
| Compound | Concentration (g/100 g) 1 |
|---|---|
| Free glucose occurring in BSG extract | 5.53 ± 0.01 |
| Free arabinose occurring in BSG extract | 0.71 ± 0.01 |
| Free xylose occurring in BSG extract | 0.95 ± 0.01 |
| Total AXs occurring in BSG extract | 7.50 ± 0.05 |
| WEAX—water extractable arabinoxylans | 1.23 ± 0.02 |
| AEAX—alkali extractable arabinoxylans | 6.36 ± 0.03 |
| AXs insoluble in ethanol (78%) occurring in total fiber dry residue | 0.45 ± 0.01 |
| AXs soluble in ethanol (78%) 2 | 7.05 ± 0.01 |
| Total β-glucans occurring in BSG extract | 1.92 ± 0.05 |
| β-glucans insoluble in ethanol (78%) occurring in total fiber dry residue | N.D.3 |
| Glucose after 30 min of enzymatic hydrolysis occurring in BSG extract 4 | 30.36 ± 0.01 |
| Glucose after 4 h of enzymatic hydrolysis occurring in BSG extract 5 | 45.00 ± 0.06 |
| Glucose after 4 h of enzymatic hydrolysis occurring in total fiber dry residue | 0.62 ± 0.01 |
| Total dietary fiber | 7.45 ± 0.03 |
| Features | Group 1 (n = 20) | Group 2 (n = 20) |
|---|---|---|
| Age (years) | 53 ± 5 | 57 ± 7 |
| Gender: | ||
| Male | 7 | 8 |
| Female | 13 | 12 |
| Ethnicity: European | 20 | 20 |
| BMI (kg/m2) | 21.82 ± 2.05 − (18.6–24.7) | 21.93 ± 2.32 − (18.5–24.8) |
| TC (mg/dL) | 217.25 ± 17.89 − (180–245) | 220.7 ± 17.71 − (180–246) |
| HDL-C (mg/dL) | 48.55 ± 12.14 − (30–65) | 54.9 ± 9.18 − (33–68) |
| LDL-C (mg/dL) | 112.85 ± 17.78 − (83–153) | 120.25 ± 23.42 − (82–160) |
| Triglyceride (mg/dL) | 131.55 ± 26.49 − (82–167) | 125.6 ± 22.6 − (85–170) |
| Homa index | 3.39 ± 1.32 − (1.21–5.25) | 4.58 ± 1.45 − (1.54–6.81) |
| TyG index | 8.51 ± 0.24 (7.99–8.86) | 8.61 ± 0.21 (8.19–8.99) |
| Variable Treatment | t0 | t1 | t2 | t3 | t4 | t5 | |
|---|---|---|---|---|---|---|---|
| Blood glycemia (mg/dL) | |||||||
| Female | A | 81.6 ± 7.7 | 86.9 ± 7.6 | 92.2 ± 7.8 | 97.5 ± 7.6 | 91.4 ± 7.3 | 83.3 ± 8.3 |
| (70–95) | (75–100) | (80–105) | (85–110) | (80–106) | (72–101) | ||
| B | 81.5 ± 6.5 | 86.7 ± 6.4 | 91.8 ± 6.5 | 97.3 ± 6.6 | 93.2 ± 6.7 | 89.3 ± 6.5 | |
| (70–94) | (76–99) | (81–104) | (87–109) | (82–105) | (79–101) | ||
| Male | A | 86 ± 8.1 | 91.3 ± 7.9 | 96.4 ± 7.8 | 101.4 ± 7.4 | 94.8 ± 8.1 | 88.3 ± 8 |
| (72–95) | (77–100) | (83–106) | (88–110) | (82–105) | (74–96) | ||
| B | 84.3 ± 7.6 | 89.7 ± 7.4 | 95.3 ± 7.1 | 100.5 ± 6.7 | 96.5 ± 6.6 | 93.2 ± 6 | |
| (74–94) | (80–100) | (86–105) | (91–109) | (85–104) | (83–100) | ||
| Blood insulin (µU/mL) | |||||||
| Female | A | 17.3 ± 7.2 | 27.7 ± 7.2 | 37.8 ± 7 | 48.3 ± 7 | 30.5 ± 9.6 | 18.5 ± 7.1 |
| (6–30) | (17–41) | (27–52) | (38–62) | (18–48) | (8–34) | ||
| B | 17.9 ± 8.1 | 30.2 ± 7.5 | 40.6 ± 7.7 | 51.3 ± 8.5 | 38.1 ± 7.7 | 26.8 ± 8.8 | |
| (6–30) | (20–41) | (28–53) | (34–64) | (25–51) | (9–39) | ||
| Male | A | 16.3 ± 6.4 | 26.9 ± 6.2 | 36.9 ± 6.5 | 47.4 ± 6.1 | 30.3 ± 6.8 | 17 ± 5.4 |
| (7–28) | (18–39) | (28–49) | (39–58) | (20–42) | (9–27) | ||
| B | 21.6 ± 6 | 33.7 ± 6.7 | 44.8 ± 6.9 | 55.2 ± 7.9 | 43.2 ± 5.7 | 30.9 ± 5.8 | |
| (10–30) | (21–45) | (32–58) | (43–72) | (33–51) | (20–40) | ||
| Template | F | Df | P |
|---|---|---|---|
| Glycemia | |||
| Measurement | 89.11 | 5, 423 | <0.001 |
| Treatment | 11.01 | 1, 427 | <0.001 |
| Sex | 6.63 | 1, 37 | 0.014 |
| Age | 4.96 | 1, 37 | 0.032 |
| Processing order | 22.83 | 1, 423 | <0.001 |
| Measurement × Treatment | 4.69 | 5, 423 | <0.001 |
| Measurement × Order of treatment | 0.04 | 5, 423 | 0.99 |
| Insulin | |||
| Measurement | 324.06 | 5, 423 | <0.001 |
| Treatment | 138.95 | 1, 428 | <0.001 |
| Sex | 1.36 | 1, 37 | 0.25 |
| Age | 2.58 | 1, 37 | 0.12 |
| Processing order | 6.87 | 1, 423 | 0.0097 |
| Measurement × Treatment | 6.29 | 5, 423 | <0.001 |
| Measurement × Order of treatment | 1.86 | 5, 423 | 0.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ullah, H.; Esposito, C.; Piccinocchi, R.; De Lellis, L.F.; Santarcangelo, C.; Minno, A.D.; Baldi, A.; Buccato, D.G.; Khan, A.; Piccinocchi, G.; et al. Postprandial Glycemic and Insulinemic Response by a Brewer’s Spent Grain Extract-Based Food Supplement in Subjects with Slightly Impaired Glucose Tolerance: A Monocentric, Randomized, Cross-Over, Double-Blind, Placebo-Controlled Clinical Trial. Nutrients 2022, 14, 3916. https://doi.org/10.3390/nu14193916
Ullah H, Esposito C, Piccinocchi R, De Lellis LF, Santarcangelo C, Minno AD, Baldi A, Buccato DG, Khan A, Piccinocchi G, et al. Postprandial Glycemic and Insulinemic Response by a Brewer’s Spent Grain Extract-Based Food Supplement in Subjects with Slightly Impaired Glucose Tolerance: A Monocentric, Randomized, Cross-Over, Double-Blind, Placebo-Controlled Clinical Trial. Nutrients. 2022; 14(19):3916. https://doi.org/10.3390/nu14193916
Chicago/Turabian StyleUllah, Hammad, Cristina Esposito, Roberto Piccinocchi, Lorenza Francesca De Lellis, Cristina Santarcangelo, Alessandro Di Minno, Alessandra Baldi, Daniele Giuseppe Buccato, Ayesha Khan, Gaetano Piccinocchi, and et al. 2022. "Postprandial Glycemic and Insulinemic Response by a Brewer’s Spent Grain Extract-Based Food Supplement in Subjects with Slightly Impaired Glucose Tolerance: A Monocentric, Randomized, Cross-Over, Double-Blind, Placebo-Controlled Clinical Trial" Nutrients 14, no. 19: 3916. https://doi.org/10.3390/nu14193916
APA StyleUllah, H., Esposito, C., Piccinocchi, R., De Lellis, L. F., Santarcangelo, C., Minno, A. D., Baldi, A., Buccato, D. G., Khan, A., Piccinocchi, G., Sacchi, R., & Daglia, M. (2022). Postprandial Glycemic and Insulinemic Response by a Brewer’s Spent Grain Extract-Based Food Supplement in Subjects with Slightly Impaired Glucose Tolerance: A Monocentric, Randomized, Cross-Over, Double-Blind, Placebo-Controlled Clinical Trial. Nutrients, 14(19), 3916. https://doi.org/10.3390/nu14193916