



Effects of Branched-Chain Amino Acids on Skeletal Muscle, Glycemic Control, and Neuropsychological Performance in Elderly Persons with Type 2 Diabetes Mellitus: An Exploratory Randomized Controlled Trial

 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Intervention
2.3. Outcomes
2.4. Sample Size
2.5. Randomization
2.6. Physical Measurements
2.7. Dietary Habits and Physical Activity
2.8. Laboratory Analyses
2.9. Serum Metabolite Analyses
2.10. Statistical Analysis
3. Results
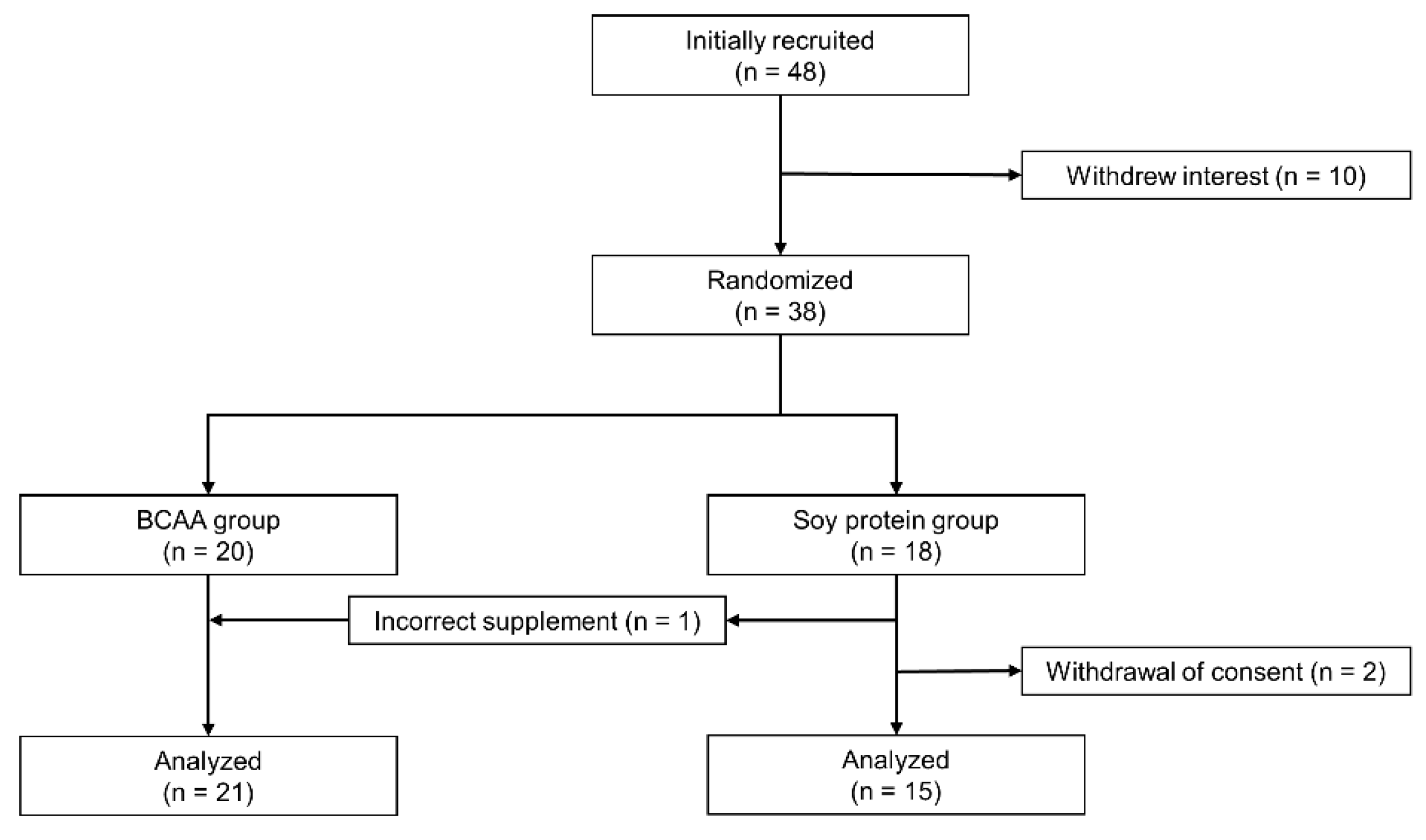
3.1. Recruitment and Baseline Characteristics of Participants
3.2. Dietary Intake and Daily Activities during the Intervention
3.3. Changes in Body Composition, Muscle Strength, and Glucose and Lipid Parameters during the Intervention
3.4. Changes in Renal Function, Neuropsychological Performance, and Amino Acids and Kynurenine Levels during the Intervention
3.5. Changes in Serum Concentrations of Insulin-like Growth Factor 1, Follistatin, and Brain-Derived Neurotropic Factor during the Intervention
3.6. Adverse Events
4. Discussion
4.1. Relationship between Amino Acids Supplementation and Skeletal Muscle Mass and Strength
4.2. Relationship between Amino Acid Supplementation and Glucose and Lipid Metabolism
4.3. Relationship between BCAA Supplementation and Neuropsychological Performance
4.4. Protein Supplementation and Renal Function
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- Mayhew, A.J.; Amog, K.; Phillips, S.; Parise, G.; McNicholas, P.D.; de Souza, R.J.; Thabane, L.; Raina, P. The prevalence of sarcopenia in community-dwelling older adults, an exploration of differences between studies and within definitions: A systematic review and meta-analyses. Age Ageing 2018, 48, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Nomura, T.; Ishiguro, T.; Ohira, M.; Oka, H.; Ikeda, Y. Isometric knee extension force in Japanese type 2 diabetic patients without apparent diabetic polyneuropathy: Data from the Multicenter Survey of the Isometric Lower Extremity Strength in Type 2 Diabetes study. SAGE Open Med. 2019, 7, 2050312118823412. [Google Scholar] [CrossRef] [PubMed]
- Park, S.W.; Goodpaster, B.H.; Strotmeyer, E.S.; Kuller, L.H.; Broudeau, R.; Kammerer, C.; de Rekeneire, N.; Harris, T.B.; Schwartz, A.V.; Tylavsky, F.A.; et al. Accelerated Loss of Skeletal Muscle Strength in Older Adults with Type 2 Diabetes. Diabetes Care 2007, 30, 1507–1512. [Google Scholar] [CrossRef]
- Anagnostis, P.; Gkekas, N.; Achilla, C.; Pananastasiou, G.; Taouxidou, P.; Mitsiou, M.; Kenanidis, E.; Potoupnis, M.; Tsiridis, E.; Goulis, D.G. Type 2 Diabetes Mellitus is Associated with Increased Risk of Sarcopenia: A Systematic Review and Meta-analysis. Calcif. Tissue Res. 2020, 107, 453–463. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Kuroda, A.; Yoshida, S.; Yasuda, T.; Umayahara, Y.; Shimizu, S.; Ryomoto, K.; Yoshiuchi, K.; Yamamoto, T.; Matsuoka, T.; et al. High prevalence and clinical impact of dynapenia and sarcopenia in Japanese patients with type 1 and type 2 diabetes: Findings from the Impact of Diabetes Mellitus on Dynapenia study. J. Diabetes Investig. 2020, 12, 1050–1059. [Google Scholar] [CrossRef] [PubMed]
- Schaap, L.A.; van Schoor, N.M.; Lips, P.; Visser, M. Associations of Sarcopenia Definitions, and Their Components, with the Incidence of Recurrent Falling and Fractures: The Longitudinal Aging Study Amsterdam. J. Gerontol. Ser. A 2018, 73, 1199–1204. [Google Scholar] [CrossRef]
- Beretta, M.V.; Filho, F.F.D.; Freiberg, R.E.; Feldman, J.V.; Nery, C.; Rodrigues, T.C. Sarcopenia and Type 2 diabetes mellitus as predictors of 2-year mortality after hospital discharge in a cohort of hospitalized older adults. Diabetes Res. Clin. Pract. 2020, 159, 107969. [Google Scholar] [CrossRef]
- Nakanishi, S.; Iwamoto, M.; Shinohara, H.; Iwamoto, H.; Kaneto, H. Impact of sarcopenia on glycemic control and atherosclerosis in Japanese patients with type 2 diabetes: Cross-sectional study using outpatient clinical data. Geriatr. Gerontol. Int. 2020, 20, 1196–1201. [Google Scholar] [CrossRef]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People: A Position Paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef]
- Tieland, M.; Berg, K.J.B.-V.D.; Van Loon, L.J.C.; De Groot, L.C.P.G.M. Dietary Protein Intake in Dutch Elderly People: A Focus on Protein Sources. Nutrients 2015, 7, 9697–9706. [Google Scholar] [CrossRef] [PubMed]
- Kamada, C.; Yoshimura, H.; Okumura, R.; Takahashi, K.; Iimuro, S.; Ohashi, Y.; Araki, A.; Umegaki, H.; Sakurai, T.; Yoshimura, Y.; et al. Optimal energy distribution of carbohydrate intake for Japanese elderly patients with type 2 diabetes: The Japanese Elderly Intervention Trial. Geriatr. Gerontol. Int. 2012, 12 (Suppl. 1), 41–49. [Google Scholar] [CrossRef] [PubMed]
- Villani, A.; Barrett, M.; McClure, R.; Wright, H. Protein intake is not associated with functional biomarkers of physical frailty: A cross-sectional analysis of community-dwelling older adults with type 2 diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2020, 31, 827–833. [Google Scholar] [CrossRef] [PubMed]
- Buse, M.G.; Reid, S.S. Leucine. A possible regulator of protein turnover in muscle. J. Clin. Investig. 1975, 56, 1250–1261. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.H.; Saddler, N.I.; Devries, M.C.; McGlory, C.; Baker, S.K.; Phillips, S.M. Leucine supplementation enhances integrative myofibrillar protein synthesis in free-living older men consuming lower- and higher-protein diets: A parallel-group crossover study. Am. J. Clin. Nutr. 2016, 104, 1594–1606. [Google Scholar] [CrossRef]
- Xu, Z.-R.; Tan, Z.-J.; Zhang, Q.; Gui, Q.-F.; Yang, Y.-M. The effectiveness of leucine on muscle protein synthesis, lean body mass and leg lean mass accretion in older people: A systematic review and meta-analysis. Br. J. Nutr. 2015, 113, 25–34. [Google Scholar] [CrossRef]
- Bai, G.-H.; Tsai, M.-C.; Tsai, H.-W.; Chang, C.-C.; Hou, W.-H. Effects of branched-chain amino acid-rich supplementation on EWGSOP2 criteria for sarcopenia in older adults: A systematic review and meta-analysis. J. Nutr. 2021, 61, 637–651. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Nagai, Y.; Kawanabe, S.; Hishida, Y.; Hiraki, K.; Sone, M.; Tanaka, Y. Effects of resistance training using elastic bands on muscle strength with or without a leucine supplement for 48 weeks in elderly patients with type 2 diabetes. Endocr. J. 2021, 68, 291–298. [Google Scholar] [CrossRef]
- Memelink, R.G.; Pasman, W.J.; Bongers, A.; Tump, A.; Van Ginkel, A.; Tromp, W.; Wopereis, S.; Verlaan, S.; Bosch, J.D.V.-V.D.; Weijs, P.J.M. Effect of an Enriched Protein Drink on Muscle Mass and Glycemic Control during Combined Lifestyle Intervention in Older Adults with Obesity and Type 2 Diabetes: A Double-Blind RCT. Nutrients 2020, 13, 64. [Google Scholar] [CrossRef]
- Leenders, M.; Verdijk, L.B.; van der Hoeven, L.; van Kranenburg, J.; Hartgens, F.; Wodzig, W.K.W.H.; Saris, W.H.M.; van Loon, L.J.C. Prolonged Leucine Supplementation Does Not Augment Muscle Mass or Affect Glycemic Control in Elderly Type 2 Diabetic Men. J. Nutr. 2011, 141, 1070–1076. [Google Scholar] [CrossRef]
- Cirillo, M.; Lombardi, C.; Chiricone, D.; De Santo, N.G.; Zanchetti, A.; Bilancio, G. Protein intake and kidney function in the middle-age population: Contrast between cross-sectional and longitudinal data. Nephrol. Dial. Transplant. 2014, 29, 1733–1740. [Google Scholar] [CrossRef] [PubMed]
- Hostetter, T.H.; Meyer, T.W.; Rennke, H.G.; Brenner, B.M.; Noddin, W.T.T.A.O.J.; Sandstrom, D. Chronic effects of dietary protein in the rat with intact and reduced renal mass. Kidney Int. 1986, 30, 509–517. [Google Scholar] [CrossRef]
- Lynch, C.J.; Adams, S.H. Branched-chain amino acids in metabolic signalling and insulin resistance. Nat. Rev. Endocrinol. 2014, 10, 723–736. [Google Scholar] [CrossRef]
- Badoud, F.; Lam, K.P.; DiBattista, A.; Perreault, M.; Zulyniak, M.A.; Cattrysse, B.; Stephenson, S.; Britz-McKibbin, P.; Mutch, D.M. Serum and adipose tissue amino acid homeostasis in the metabolically healthy obese. J. Proteome Res. 2014, 13, 3455–3466. [Google Scholar] [CrossRef]
- Li, X.; Wang, X.; Liu, R.; Ma, Y.; Guo, H.; Hao, L.; Yao, P.; Liu, L.; Sun, X.; He, K.; et al. Chronic leucine supplementation increases body weight and insulin sensitivity in rats on high-fat diet likely by promoting insulin signaling in insulin-target tissues. Mol. Nutr. Food Res. 2013, 57, 1067–1079. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, T.; Nagao, Y.; Matsuoka, H.; Ide, T.; Sata, M. Branched-chain amino acid-enriched supplementation improves insulin resistance in patients with chronic liver disease. Int. J. Mol. Med. 2008, 22, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Fernstrom, J.D. Branched-Chain Amino Acids and Brain Function. J. Nutr. 2005, 135, 1539S–1546S. [Google Scholar] [CrossRef] [PubMed]
- Han, Q.; Robinson, H.; Cai, T.; Tagle, D.A.; Li, J. Biochemical and Structural Properties of Mouse Kynurenine Aminotransferase III. Mol. Cell. Biol. 2009, 29, 784–793. [Google Scholar] [CrossRef]
- Cervenka, I.; Agudelo, L.Z.; Ruas, J.L. Kynurenines: Tryptophan’s metabolites in exercise, inflammation, and mental health. Science 2017, 357, eaaf9794. [Google Scholar] [CrossRef]
- Negm, A.M.; Lee, J.; Hamidian, R.; Jones, C.A.; Khadaroo, R.G. Management of Sarcopenia: A Network Meta-Analysis of Randomized Controlled Trials. J. Am. Med. Dir. Assoc. 2022, 23, 707–714. [Google Scholar] [CrossRef]
- Draznin, B.; Aroda, V.R.; Bakris, G.; Benson, G.; Brown, F.M.; Freeman, R.; Green, J.; Huang, E.; Isaacs, D.; Kahan, S.; et al. 5. Facilitating Behavior Change and Well-being to Improve Health Outcomes: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S60–S82. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Education, Culture, Sports, Science and Technology (MEXT), Japan. Standard Tables of Food Composition in Japan—2020—(Eighth Revised Version). Available online: https://fooddb.mext.go.jp/details/details.pl?ITEM_NO=4_04057_7&MODE=3 (accessed on 19 June 2022).
- Rieu, I.; Balage, M.; Sornet, C.; Giraudet, C.; Pujos, E.; Grizard, J.; Mosoni, L.; Dardevet, D. Leucine supplementation improves muscle protein synthesis in elderly men independently of hyperaminoacidaemia. J. Physiol. 2006, 575, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.K.; Suzuki, T.; Saito, K.; Yoshida, H.; Kobayashi, H.; Kato, H.; Katayama, M. Effects of Exercise and Amino Acid Supplementation on Body Composition and Physical Function in Community-Dwelling Elderly Japanese Sarcopenic Women: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2011, 60, 16–23. [Google Scholar] [CrossRef]
- Kobayashi, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Comparison of relative validity of food group intakes estimated by comprehensive and brief-type self-administered diet history questionnaires against 16 d dietary records in Japanese adults. Public Health Nutr. 2011, 14, 1200–1211. [Google Scholar] [CrossRef] [PubMed]
- Mâsse, L.C.; Fuemmeler, B.F.; Anderson, C.B.; Matthews, C.E.; Trost, S.G.; Catellier, D.J.; Treuth, M. Accelerometer data reduction: A comparison of four reduction algorithms on select outcome variables. Med. Sci. Sports Exerc. 2005, 37, S544–S554. [Google Scholar] [CrossRef]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Maroni, B.J.; Steinman, T.I.; Mitch, W.E. A method for estimating nitrogen intake of patients with chronic renal failure. Kidney Int. 1985, 27, 58–65. [Google Scholar] [CrossRef]
- Nishi, H.; Yamanaka, D.; Masuda, M.; Goda, Y.; Ito, K.; Hakuno, F.; Takahashi, S.I. Alteration of serum amino acid profiles by dietary adenine supplementation inhibits fatty liver development in rats. Sci. Rep. 2020, 10, 22110. [Google Scholar] [CrossRef]
- Hanach, N.I.; McCullough, F.; Avery, A. The Impact of Dairy Protein Intake on Muscle Mass, Muscle Strength, and Physical Performance in Middle-Aged to Older Adults with or without Existing Sarcopenia: A Systematic Review and Meta-Analysis. Adv. Nutr. 2019, 10, 59–69. [Google Scholar] [CrossRef]
- Tieland, M.; Franssen, R.; Dullemeijer, C.; van Dronkelaar, C.; Kim, H.K.; Ispoglou, T.; Zhu, K.; Prince, R.L.; van Loon, L.J.; De Groot, L.C.P.G.M. The impact of dietary protein or amino acid supplementation on muscle mass and strength in elderly people: Individual participant data and meta-analysis of RCT’s. J. Nutr. Health Aging 2017, 21, 994–1001. [Google Scholar] [CrossRef]
- Nunes, E.A.; Colenso-Semple, L.; McKellar, S.R.; Yau, T.; Ali, M.U.; Fitzpatrick-Lewis, D.; Sherifali, D.; Gaudichon, C.; Tomé, D.; Atherton, P.J.; et al. Systematic review and meta-analysis of protein intake to support muscle mass and function in healthy adults. J. Cachex- Sarcopenia Muscle 2022, 13, 795–810. [Google Scholar] [CrossRef] [PubMed]
- Moberg, M.; Apró, W.; Ekblom, B.; van Hall, G.; Holmberg, H.-C.; Blomstrand, E. Activation of mTORC1 by leucine is potentiated by branched-chain amino acids and even more so by essential amino acids following resistance exercise. Am. J. Physiol. Physiol. 2016, 310, C874–C884. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, D.; Kim, C. Resistance Training for Glycemic Control, Muscular Strength, and Lean Body Mass in Old Type 2 Diabetic Patients: A Meta-Analysis. Diabetes Ther. 2017, 8, 459–473. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Sato, Y.; Obeng, K.A.; Yoshizawa, F. Acute oral administration of L-leucine upregulates slow-fiber- and mitochondria-related genes in skeletal muscle of rats. Nutr. Res. 2018, 57, 36–44. [Google Scholar] [CrossRef]
- Xiang, L.; Huang, Z.; Chen, X.; Jia, G.; Liu, G.; Zhao, H. Leucine regulates porcine muscle fiber type transformation via adiponectin signaling pathway. Anim. Biotechnol. 2022, 33, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, W.O.; Ponette, J.; Horwath, O.; Rydenstam, T.; Söderlund, K.; Ekblom, B.; Azzolini, M.; Ruas, J.L.; Blomstrand, E. Changes in plasma concentration of kynurenine following intake of branched-chain amino acids are not caused by alterations in muscle kynurenine metabolism. Am. J. Physiol. Cell Physiol. 2022, 322, C49–C62. [Google Scholar] [CrossRef] [PubMed]
- Backx, E.M.; Horstman, A.M.; Marzuca-Nassr, G.N.; van Kranenburg, J.; Smeets, J.S.; Fuchs, C.J.; Janssen, A.A.; De Groot, L.C.; Snijders, T.; Verdijk, L.B.; et al. Leucine Supplementation Does Not Attenuate Skeletal Muscle Loss during Leg Immobilization in Healthy, Young Men. Nutrients 2018, 10, 635. [Google Scholar] [CrossRef] [PubMed]
- Viña, J.; Gomez-Cabrera, M.C.; Borras, C.; Froio, T.; Sanchis-Gomar, F.; Martinez-Bello, V.; Pallardo, F.V. Mitochondrial biogenesis in exercise and in ageing. Adv. Drug Deliv. Rev. 2009, 61, 1369–1374. [Google Scholar] [CrossRef]
- Parraca, J.A.; Adsuar, J.C.; Domínguez-Muñoz, F.J.; Barrios-Fernandez, S.; Tomas-Carus, P. Test-Retest Reliability of Isokinetic Strength Measurements in Lower Limbs in Elderly. Biology 2022, 11, 802. [Google Scholar] [CrossRef]
- Lynch, G.S.; Cuffe, S.A.; Plant, D.R.; Gregorevic, P. IGF-I treatment improves the functional properties of fast- and slow-twitch skeletal muscles from dystrophic mice. Neuromuscul. Disord. 2001, 11, 260–268. [Google Scholar] [CrossRef]
- Barbé, C.; Bray, F.; Gueugneau, M.; Devassine, S.; Lause, P.; Tokarski, C.; Rolando, C.; Thissen, J.-P. Comparative Proteomic and Transcriptomic Analysis of Follistatin-Induced Skeletal Muscle Hypertrophy. J. Proteome Res. 2017, 16, 3477–3490. [Google Scholar] [CrossRef] [PubMed]
- Delezie, J.; Weihrauch, M.; Maier, G.; Tejero, R.; Ham, D.J.; Gill, J.F.; Karrer-Cardel, B.; Rüegg, M.A.; Tabares, L.; Handschin, C. BDNF is a mediator of glycolytic fiber-type specification in mouse skeletal muscle. Proc. Natl. Acad. Sci. USA 2019, 116, 16111–16120. [Google Scholar] [CrossRef] [PubMed]
- Krebs, M.; Krssak, M.; Bernroider, E.; Anderwald, C.; Brehm, A.; Meyerspeer, M.; Nowotny, P.; Roth, E.; Waldhäusl, W.; Roden, M. Mechanism of Amino Acid-Induced Skeletal Muscle Insulin Resistance in Humans. Diabetes 2002, 51, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.I.; Yoshino, J.; Stromsdorfer, K.L.; Klein, S.J.; Magkos, F.; Reeds, D.N.; Klein, S.; Mittendorfer, B. Protein Ingestion Induces Muscle Insulin Resistance Independent of Leucine-Mediated mTOR Activation. Diabetes 2014, 64, 1555–1563. [Google Scholar] [CrossRef] [PubMed]
- Amirani, E.; Milajerdi, A.; Reiner, Ž.; Mirzaei, H.; Mansournia, M.A.; Asemi, Z. Effects of whey protein on glycemic control and serum lipoproteins in patients with metabolic syndrome and related conditions: A systematic review and meta-analysis of randomized controlled clinical trials. Lipids Health Dis. 2020, 19, 209. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; DeFronzo, R.A. Insulin sensitivity indices obtained from oral glucose tolerance testing: Comparison with the euglycemic insulin clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- Paquin, J.; Lagacé, J.-C.; Brochu, M.; Dionne, I.J. Exercising for Insulin Sensitivity—Is There a Mechanistic Relationship with Quantitative Changes in Skeletal Muscle Mass? Front. Physiol. 2021, 12, 656909. [Google Scholar] [CrossRef]
- Singh, B.P.; Vij, S.; Hati, S. Functional significance of bioactive peptides derived from soybean. Peptides 2014, 54, 171–179. [Google Scholar] [CrossRef]
- Baranyi, A.; Amouzadeh-Ghadikolai, O.; Von Lewinski, D.; Rothenhäusler, H.-B.; Theokas, S.; Robier, C.; Mangge, H.; Reicht, G.; Hlade, P.; Meinitzer, A. Branched-Chain Amino Acids as New Biomarkers of Major Depression—A Novel Neurobiology of Mood Disorder. PLoS ONE 2016, 11, e0160542. [Google Scholar] [CrossRef]
- Koochakpoor, G.; Salari-Moghaddam, A.; Keshteli, A.H.; Afshar, H.; Esmaillzadeh, A.; Adibi, P. Dietary intake of branched-chain amino acids in relation to depression, anxiety and psychological distress. Nutr. J. 2021, 20, 11. [Google Scholar] [CrossRef]
- Walker, A.K.; Wing, E.E.; Banks, W.A.; Dantzer, R. Leucine competes with kynurenine for blood-to-brain transport and prevents lipopolysaccharide-induced depression-like behavior in mice. Mol. Psychiatry 2019, 24, 1523–1532. [Google Scholar] [CrossRef] [PubMed]
- Hunt, C.; e Cordeiro, T.M.; Suchting, R.; de Dios, C.; Leal, V.A.C.; Soares, J.C.; Dantzer, R.; Teixeira, A.L.; Selvaraj, S. Effect of immune activation on the kynurenine pathway and depression symptoms—A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2020, 118, 514–523. [Google Scholar] [CrossRef]
- Sublette, M.E.; Galfalvy, H.C.; Fuchs, D.; Lapidus, M.; Grunebaum, M.F.; Oquendo, M.A.; Mann, J.J.; Postolache, T.T. Plasma kynurenine levels are elevated in suicide attempters with major depressive disorder. Brain. Behav. Immun. 2011, 25, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Boado, R.J.; Li, J.Y.; Nagaya, M.; Zhang, C.; Pardridge, W.M. Selective expression of the large neutral amino acid transporter at the blood–brain barrier. Proc. Natl. Acad. Sci. USA 1999, 96, 12079–12084. [Google Scholar] [CrossRef] [PubMed]
- Holecek, M. Relation between glutamine, branched-chain amino acids, and protein metabolism. Nutrition 2002, 18, 130–133. [Google Scholar] [CrossRef]
- Godfrey, K.E.M.; Gardner, A.C.; Kwon, S.; Chea, W.; Muthukumaraswamy, S.D. Differences in excitatory and inhibitory neurotransmitter levels between depressed patients and healthy controls: A systematic review and meta-analysis. J. Psychiatr. Res. 2018, 105, 33–44. [Google Scholar] [CrossRef]
- Baek, J.H.; Vignesh, A.; Son, H.; Lee, D.H.; Roh, G.S.; Kang, S.S.; Cho, G.J.; Choi, W.S.; Kim, H.J. Glutamine Supplementation Ameliorates Chronic Stress-induced Reductions in Glutamate and Glutamine Transporters in the Mouse Prefrontal Cortex. Exp. Neurobiol. 2019, 28, 270–278. [Google Scholar] [CrossRef]
- Yan, B.; Su, X.; Xu, B.; Qiao, X.; Wang, L. Effect of diet protein restriction on progression of chronic kidney disease: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0206134. [Google Scholar] [CrossRef]
- de Boer, I.H.; Caramori, M.L.; Chan, J.C.; Heerspink, H.J.; Hurst, C.; Khunti, K.; Liew, A.; Michos, E.D.; Navaneethan, S.D.; Olowu, W.A.; et al. KDIGO 2020 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int. 2020, 98, S1–S115. [Google Scholar] [CrossRef] [PubMed]
- Knight, E.L.; Stampfer, M.J.; Hankinson, S.E.; Spiegelman, D.; Curhan, G.C. The impact of protein intake on renal function decline in women with normal renal function or mild renal insufficiency. Ann. Intern. Med. 2003, 138, 460–467. [Google Scholar] [CrossRef]
- Bernier-Jean, A.; Prince, R.L.; Lewis, J.R.; Craig, J.C.; Hodgson, J.M.; Lim, W.H.; Teixeira-Pinto, A.; Wong, G. Dietary plant and animal protein intake and decline in estimated glomerular filtration rate among elderly women: A 10-year longitudinal cohort study. Nephrol. Dial. Transplant. 2020, 36, 1640–1647. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, D.; Shimada, H.; Park, H.; Anan, Y.; Ito, T.; Harada, A.; Suzuki, T. Development of an equation for estimating appendicular skeletal muscle mass in Japanese older adults using bioelectrical impedance analysis. Geriatr Gerontol Int 2014, 14, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Dehghan, M.; Merchant, A.T. Is bioelectrical impedance accurate for use in large epidemiological studies? Nutr. J. 2008, 7, 26. [Google Scholar] [CrossRef] [PubMed]
- Androutsos, O.; Gerasimidis, K.; Karanikolou, A.; Reilly, J.J.; Edwards, C.A. Impact of eating and drinking on body composition measurements by bioelectrical impedance. J. Hum. Nutr. Diet. 2015, 28, 165–171. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| BCAA | Soy Protein | p | |
|---|---|---|---|
| n | 21 | 15 | |
| Age (years) | 73 ± 4 | 73 ± 4 | 0.883 |
| Female (%) | 38 | 33 | 1.000 |
| Duration of diabetes (years) * | 21 (16–24) | 19 (14–29) | 0.431 |
| Current smoking (%) | 5 | 7 | 1.000 |
| Alcohol consumption (g/day) | 0 (0–10) | 0 (0–0) | 0.526 |
| Total energy (kcal/day) | 2017 ± 488 | 1804 ± 545 | 0.226 |
| Protein intake (g/kg/day) * | 1.0 (0.8–1.3) | 1.0 (0.9–1.4) | 0.228 |
| Body mass index (kg/m2) * | 24.3 (22.5–26.0) | 23.1 (20.9–24.6) | 0.132 |
| Skeletal muscle mass (kg) | 24.8 ± 5.4 | 23.4 ± 4.6 | 0.437 |
| Skeletal muscle index (kg/m2) | 7.0 ± 1.2 | 6.6 ± 0.9 | 0.259 |
| Lean body mass (kg) * | 45.9 (36.0–55.0) | 44.1 (36.7–50.4) | 0.520 |
| Body fat percentage (%) | 28.4 ± 8.0 | 25.9 ± 6.4 | 0.339 |
| Grip strength (kg) | 32 ± 10 | 31 ± 8 | 0.882 |
| Knee extension strength (Nm/kg) | 140 ± 40 | 146 ± 50 | 0.694 |
| Knee extension endurance (J) | 844 ± 287 | 762 ± 286 | 0.404 |
| MMSE (points) | 28 (27–30) | 29 (27–30) | 0.590 |
| QIDS (points) | 6 (3–8) | 4 (2–6) | 0.191 |
| SAS (points) | 11 (4–16) | 13 (4–15) | 0.751 |
| Fasting plasma glucose (mmol/L) | 7.6 ± 1.5 | 8.1 ± 1.2 | 0.324 |
| Fasting serum insulin (pmol/L) * | 29 (17–40) | 20 (13–40) | 0.463 |
| HOMA-IR | 1.4 (1.0–2.0) | 1.2 (0.7–2.3) | 0.590 |
| HbA1c (mmol/mol) | 56 ± 7 | 53 ± 3 | 0.190 |
| Total cholesterol (mmol/L) | 4.4 ± 0.8 | 4.7 ± 0.5 | 0.353 |
| LDL-C (mmol/L) | 2.4 ± 0.7 | 2.6 ± 0.4 | 0.293 |
| HDL-C (mmol/L) | 1.5 ± 0.4 | 1.6 ± 0.4 | 0.532 |
| Triglycerides (mmol/L) | 1.1 ± 0.5 | 1.0 ± 0.4 | 0.459 |
| eGFR (mL/min/1.73 m2) | 69 ± 16 | 66 ± 16 | 0.524 |
| Urinary albumin excretion (mg/day) | 23 (5–94) | 13 (6–51) | 0.547 |
| Diabetic Complications | |||
| Neuropathy (%) | 24 | 13 | 0.674 |
| Retinopathy (%) | 57 | 60 | 1.000 |
| Nephropathy (%) | 38 | 33 | 1.000 |
| Cardiovascular disease (%) | 24 | 33 | 0.709 |
| Antidiabetic drugs | |||
| Metformin (%) | 52 | 67 | 0.501 |
| Sulfonylureas (%) | 29 | 13 | 0.424 |
| Glinides (%) | 0 | 33 | 0.008 |
| Thiazolidines (%) | 5 | 7 | 1.000 |
| SGLT2 inhibitors (%) | 38 | 13 | 0.142 |
| DPP-4 inhibitors (%) | 62 | 73 | 0.721 |
| GLP-1 receptor agonists (%) | 14 | 7 | 0.626 |
| α-glucosidase inhibitors (%) | 24 | 27 | 1.000 |
| Group | Baseline | 8 Weeks | 16 Weeks | 24 Weeks | p for Time | p for Groups | p for Group × Time | |
|---|---|---|---|---|---|---|---|---|
| Total energy (kcal/day) | B | 2017 ± 488 | 1890 ± 555 | 1897 ± 463 | 1997 ± 645 | 0.623 | 0.112 | 0.958 |
| S | 1804 ± 545 | 1670 ± 556 | 1599 ± 499 | 1712 ± 533 | 0.476 | |||
| Protein intake (g/kg/day) * | B | 1.0 (0.8–1.3) | 1.0 (0.8–1.4) | 1.1 (0.8–1.3) | 1.0 (0.8–1.3) | 0.943 | 0.123 | 0.931 |
| S | 1.0 (0.9–1.4) | 1.2 (1.0–1.6) | 1.2 (1.0–1.4) | 1.1 (1.0–1.3) | 0.744 | |||
| Daily activity (kcal/day) | B | 654 ± 161 | 633 ± 142 | 643 ± 137 | 613 ± 130 | 0.282 | 0.430 | 0.027 |
| S | 605 ± 189 | 590 ± 186 | 595 ± 191 | 636 ± 219 | 0.128 |
| Group | Baseline | 8 Weeks | 16 Weeks | 24 Weeks | p for Time | Changes between Baseline and 24 Weeks | p for Groups | |
|---|---|---|---|---|---|---|---|---|
| Body mass index (kg/m2) * | B | 24.3 (22.5–26.0) | 24.1 (22.4–26.0) | 23.7 (22.4–25.7) | 24.0 (22.4–24.8) | 0.396 | −0.2 (−0.3–0.2) | 0.222 |
| S | 23.1 (20.9–24.6) | 23.2 (21.0–24.6) | 23.2 (20.8–24.6) | 22.9 (20.6–24.6) | 0.116 | 0.1 (−0.1–0.2) | ||
| Skeletal muscle mass (kg) | B | 24.8 ± 5.4 | 24.7 ± 5.5 | 24.8 ± 5.6 | 24.3 ± 5.2 | 0.940 | −0.1 ± 0.8 | 0.693 |
| S | 23.4 ± 4.6 | 23.7 ± 4.6 | 23.5 ± 4.5 | 23.4 ± 4.5 | 0.444 | 0.0 ± 0.5 | ||
| Knee extension strength (Nm/kg) | B | 140 ± 40 | — | — | 148 ± 40 | 0.086 | 10 ± 24 | 0.781 |
| S | 146 ± 50 | — | — | 159 ± 41 | 0.023 | 12 ± 19 | ||
| Knee extension endurance (J) | B | 844 ± 287 | — | — | 780 ± 263 | 0.036 | −44 ± 90 | 0.526 |
| S | 762 ± 286 | — | — | 744 ± 205 | 0.645 | −18 ± 149 | ||
| Grip strength (kg) | B | 32 ± 10 | — | — | 33 ± 11 | 0.044 | 2 ± 3 | 0.213 |
| S | 31 ± 8 | — | — | 32 ± 9 | 0.486 | 0 ± 2 | ||
| HbA1c (mmol/L) | B | 56 ± 7 | 55 ± 6 | 56 ± 6 | 55 ± 5 | 0.711 | −1 ± 4 | 0.140 |
| S | 53 ± 3 | 55 ± 5 | 55 ± 7 | 55 ± 8 | 0.386 | 2 ± 6 | ||
| Fasting plasma glucose (mmol/L) | B | 7.6 ± 1.5 | 7.7 ± 1.7 | 7.6 ± 1.2 | 7.8 ± 1.1 | 0.864 | 0.1 ± 0.7 | 0.780 |
| S | 8.1 ± 1.2 | 8.9 ± 2.4 | 7.9 ± 1.1 | 8.1 ± 1.2 | 0.156 | 0.0 ± 1.0 | ||
| Fasting serum insulin (pmol/L) * | B | 29 (17–40) | 29 (15–41) | 28 (19–41) | 26 (16–33) | 0.711 | 0 (−8–6) | 0.182 |
| S | 20 (13–40) | 20 (14–38) | 30 (17–34) | 20 (10–28) | 0.315 | −1 (−11–2) | ||
| HOMA-IR * | B | 1.4 (1.0–2.0) | 1.4 (0.9–2.5) | 1.6 (0.9–2.3) | 1.5 (0.9–1.9) | 0.762 | 0.0 (−0.3–0.4) | 0.153 |
| S | 1.2 (0.7–2.3) | 1.2 (0.8–2.3) | 1.5 (0.8–2.1) | 1.3 (0.6–1.6) | 0.320 | −0.1 (−0.7–0.2) | ||
| Total cholesterol (mmol/L) | B | 4.4 ± 0.8 | 4.4 ± 0.9 | 4.5 ± 0.9 | 4.5 ± 0.8 | 0.648 | 0.0 ± 0.3 | 0.145 |
| S | 4.7 ± 0.5 | 4.6 ± 0.6 | 4.5 ± 0.6 | 4.5 ± 0.4 | 0.268 | −0.2 ± 0.3 | ||
| LDL-C (mmol/L) | B | 2.4 ± 0.7 | 2.3 ± 0.7 | 2.4 ± 0.7 | 2.5 ± 0.7 | 0.481 | 0.0 ± 0.3 | 0.037 |
| S | 2.6 ± 0.4 | 2.5 ± 0.5 | 2.5 ± 0.5 | 2.4 ± 0.4 § | 0.044 | −0.2 ± 0.3 | ||
| HDL-C (mmol/L) | B | 1.5 ± 0.4 | 1.4 ± 0.5 | 1.4 ± 0.4 | 1.5 ± 0.4 | 0.602 | 0.0 ± 0.1 | 0.565 |
| S | 1.6 ± 0.4 | 1.5 ± 0.4 | 1.5 ± 0.4 | 1.5 ± 0.4 | 0.177 | 0.0 ± 0.2 | ||
| Triglycerides (mmol/L) | B | 1.1 ± 0.5 | 1.1 ± 0.5 | 1.1 ± 0.5 | 1.0 ± 0.5 | 0.372 | −0.1 ± 0.3 | 0.801 |
| S | 1.0 ± 0.4 | 1.0 ± 0.3 | 1.0 ± 0.3 | 0.9 ± 0.4 | 0.934 | 0.0 ± 0.4 |
| Group | Baseline | 24 Weeks | p for Time | Changes | p for Groups | |
|---|---|---|---|---|---|---|
| eGFR (mL/min/1.73 m2) | B | 69 ± 16 | 71 ± 14 | 0.469 | 0 ± 6 | 0.241 |
| S | 66 ± 16 | 68 ± 17 | 0.602 | 2 ± 7 | ||
| Urinary albumin excretion (mg/day) * | B | 23 (5–94) | 11 (4–52) | 0.258 | −3 (−23–1) | 0.047 |
| S | 13 (6–51) | 12 (4–53) | 0.386 | −1 (−2–23) | ||
| MMSE (points) | B | 28 (27–30) | 29 (26–30) | 0.667 | 0 (−1–1) | 0.086 |
| S | 29 (27–30) | 30 (28–30) | 0.055 | 1 (0–1) | ||
| QIDS (points) | B | 6 (3–8) | 4 (2–7) | 0.019 | −2 (−4–1) | 0.400 |
| S | 4 (2–6) | 3 (2–4) | 0.149 | −1 (−3–1) | ||
| SAS (points) | B | 11 (4–16) | 10 (4–16) | 0.599 | −1 (−3–2) | 0.298 |
| S | 13 (4–15) | 12 (8–16) | 0.461 | 1 (−2–4) | ||
| Total amino acids (μmol/L) | B | 3004 ± 261 | 3149 ± 198 | 0.010 | 145 ± 226 | 0.382 |
| S | 2884 ± 267 | 2960 ± 202 | 0.232 | 76 ± 235 | ||
| Branched-chain amino acids (μmol/L) | B | 407 ± 75 | 446 ± 68 | 0.015 | 39 ± 66 | 0.381 |
| S | 391 ± 62 | 412 ± 76 | 0.186 | 21 ± 57 | ||
| Essential amino acids (μmol/L) | B | 840 ± 111 | 891 ± 87 | 0.034 | 51 ± 99 | 0.629 |
| S | 812 ± 91 | 847 ± 99 | 0.175 | 35 ± 94 | ||
| Non-essential amino acids (μmol/L) | B | 2154 ± 189 | 2250 ± 155 | 0.021 | 96 ± 171 | 0.348 |
| S | 2063 ± 200 | 2104 ± 127 | 0.365 | 41 ± 169 | ||
| Large neutral amino acids (μmol/L) | B | 783 ± 105 | 836 ± 82 | 0.025 | 53 ± 97 | 0.527 |
| S | 764 ± 84 | 796 ± 96 | 0.170 | 33 ± 87 | ||
| Leucine (μmol/L) | B | 124 ± 26 | 135 ± 23 | 0.014 | 12 ± 19 | 0.224 |
| S | 121 ± 23 | 125 ± 24 | 0.601 | 3 ± 22 | ||
| Isoleucine (μmol/L) | B | 74 ± 15 | 78 ± 16 | 0.184 | 4 ± 13 | 0.650 |
| S | 71 ± 14 | 77 ± 18 | 0.075 | 6 ± 12 | ||
| Valine (μmol/L) | B | 209 ± 36 | 233 ± 32 | 0.012 | 24 ± 38 | 0.303 |
| S | 198 ± 28 | 210 ± 36 | 0.109 | 12 ± 26 | ||
| Tryptophan (μmol/L) | B | 50 ± 8 | 55 ± 9 | 0.004 | 5 ± 6 | 0.254 |
| S | 50 ± 10 | 52 ± 7 | 0.329 | 2 ± 7 | ||
| Lysine (μmol/L) * | B | 115 (106–126) | 121 (109–129) | 0.198 | 2 (−7–12) | 0.854 |
| S | 107 (93–120) | 112 (101–124) | 0.225 | 6 (−7–22) | ||
| Methionine (μmol/L) | B | 25 ± 4 | 27 ± 4 | 0.080 | 2 ± 4 | 0.393 |
| S | 23 ± 3 | 24 ± 4 | 0.696 | 0 ± 5 | ||
| Phenylalanine (μmol/L) | B | 58 ± 10 | 61 ± 9 | 0.054 | 3 ± 7 | 0.499 |
| S | 55 ± 10 | 56 ± 10 | 0.622 | 1 ± 10 | ||
| Threonine (μmol/L) * | B | 127 (119–139) | 122 (113–135) | 0.594 | −2 (−18–10) | 0.366 |
| S | 130 (116–148) | 142 (118–154) | 0.264 | 6 (−10–17) | ||
| Histidine (μmol/L) | B | 53 ± 9 | 53 ± 7 | 0.919 | 0 ± 7 | 0.485 |
| S | 51 ± 7 | 52 ± 7 | 0.435 | 2 ± 7 | ||
| Tyrosine (μmol/L) | B | 61 ± 10 | 66 ± 13 | 0.028 | 5 ± 9 | 0.297 |
| S | 60 ± 9 | 62 ± 9 | 0.340 | 2 ± 7 | ||
| Aspartic acid (μmol/L) | B | 37 ± 7 | 38 ± 7 | 0.645 | 1 ± 10 | 0.757 |
| S | 36 ± 5 | 36 ± 7 | 0.979 | 0 ± 8 | ||
| Asparagine (μmol/L) | B | 73 ± 7 | 77 ± 9 | 0.042 | 4 ± 8 | 0.766 |
| S | 71 ± 8 | 74 ± 9 | 0.212 | 3 ± 9 | ||
| Serine (μmol/L) | B | 195 ± 35 | 203 ± 35 | 0.183 | 7 ± 23 | 0.457 |
| S | 191 ± 21 | 192 ± 19 | 0.864 | 1 ± 24 | ||
| Glutamic acid (μmol/L) | B | 53 ± 14 | 54 ± 11 | 0.723 | 1 ± 15 | 0.225 |
| S | 53 ± 15 | 47 ± 17 | 0.217 | −5 ± 16 | ||
| Glutamine (μmol/L) | B | 1062 ± 110 | 1115 ± 98 | 0.022 | 53 ± 95 | 0.534 |
| S | 986 ± 122 | 1018 ± 86 | 0.250 | 32 ± 104 | ||
| Proline (μmol/L) * | B | 82 (73–93) | 87 (78–105) | 0.144 | 2 (−7–11) | 0.068 |
| S | 88 (75–104) | 78 (74–93) | 0.126 | −4 (−13–4) | ||
| Glycine (μmol/L) | B | 209 ± 28 | 207 ± 29 | 0.761 | −2 ± 29 | 0.398 |
| S | 203 ± 33 | 209 ± 33 | 0.384 | 6 ± 26 | ||
| Alanine (μmol/L) | B | 300 ± 47 | 317 ± 43 | 0.085 | 17 ± 42 | 0.249 |
| S | 295 ± 62 | 297 ± 67 | 0.766 | 2 ± 29 | ||
| Arginine (μmol/L) | B | 78 ± 16 | 82 ± 18 | 0.141 | 4 ± 13 | 0.832 |
| S | 79 ± 18 | 82 ± 16 | 0.267 | 3 ± 12 | ||
| Cystine (μmol/L) * | B | 9 (6–11) | 6 (4–9) | 0.137 | −3 (−6–2) | 0.772 |
| S | 8 (4–12) | 7 (5–12) | 0.872 | 3 (−4–7) | ||
| Kynurenine (μmol/L) | B | 4.4 ± 0.9 | 4.5 ± 0.8 | 0.925 | 0.0 ± 1.0 | 0.521 |
| S | 4.2 ± 0.9 | 4.4 ± 0.9 | 0.256 | 0.2 ± 0.7 | ||
| Kynurenic acid (μmol/L) * | B | 0.04 (0.03–0.04) | 0.03 (0.03–0.04) | 0.449 | 0.00 (−0.01–0.01) | 0.218 |
| S | 0.04 (0.03–0.05) | 0.04 (0.03–0.06) | 0.587 | 0.01 (−0.01–0.01) | ||
| Tryptophan to large neutral amino acid ratio * | B | 0.06 (0.06–0.07) | 0.07 (0.06–0.07) | 0.313 | 0.00 (0.00–0.01) | 0.641 |
| S | 0.07 (0.06–0.07) | 0.07 (0.06–0.07) | 0.955 | 0.00 (0.00–0.00) | ||
| Tryptophan to branched-chain amino acids ratio * | B | 0.12 (0.11–0.14) | 0.13 (0.11–0.14) | 0.823 | 0.00 (−0.01–0.01) | 0.783 |
| S | 0.13 (0.12–0.15) | 0.12 (0.12–0.15) | 0.865 | 0.00 (0.01–0.01) | ||
| Kynurenine to tryptophan ratio * | B | 0.09 (0.07–0.10) | 0.08 (0.07–0.09) | 0.117 | 0.00 (−0.02–0.01) | 0.156 |
| S | 0.08 (0.07–0.09) | 0.08 (0.07–0.09) | 0.955 | 0.00 (−0.01–0.01) |
| Group | Baseline | 24 Weeks | p for Time | Changes | p for Groups | |
|---|---|---|---|---|---|---|
| IGF-1 (mg/mL) | B | 102 ± 32 | 99 ± 32 | 0.292 | −3 ± 13 | 0.316 |
| S | 101 ± 40 | 105 ± 33 | 0.589 | 4 ± 28 | ||
| Follistatin (pg/mL) * | B | 1312 (711–1807) | 1419 (868–1857) | 0.675 | 68 (−316–319) | 0.611 |
| S | 1091 (889–2106) | 1232 (907–2225) | 0.595 | −38 (−149–366) | ||
| BDNF (pg/mL) | B | 23,667 ± 4452 | 23,011 ± 5020 | 0.511 | −655 ± 4376 | 0.439 |
| S | 22,130 ± 4919 | 20,093 ± 6210 | 0.214 | −2037 ± 6068 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsuda, T.; Suzuki, H.; Sugano, Y.; Suzuki, Y.; Yamanaka, D.; Araki, R.; Yahagi, N.; Sekiya, M.; Kawakami, Y.; Osaki, Y.; et al. Effects of Branched-Chain Amino Acids on Skeletal Muscle, Glycemic Control, and Neuropsychological Performance in Elderly Persons with Type 2 Diabetes Mellitus: An Exploratory Randomized Controlled Trial. Nutrients 2022, 14, 3917. https://doi.org/10.3390/nu14193917
Matsuda T, Suzuki H, Sugano Y, Suzuki Y, Yamanaka D, Araki R, Yahagi N, Sekiya M, Kawakami Y, Osaki Y, et al. Effects of Branched-Chain Amino Acids on Skeletal Muscle, Glycemic Control, and Neuropsychological Performance in Elderly Persons with Type 2 Diabetes Mellitus: An Exploratory Randomized Controlled Trial. Nutrients. 2022; 14(19):3917. https://doi.org/10.3390/nu14193917
Chicago/Turabian StyleMatsuda, Takaaki, Hiroaki Suzuki, Yoko Sugano, Yasuhiro Suzuki, Daisuke Yamanaka, Risa Araki, Naoya Yahagi, Motohiro Sekiya, Yasushi Kawakami, Yoshinori Osaki, and et al. 2022. "Effects of Branched-Chain Amino Acids on Skeletal Muscle, Glycemic Control, and Neuropsychological Performance in Elderly Persons with Type 2 Diabetes Mellitus: An Exploratory Randomized Controlled Trial" Nutrients 14, no. 19: 3917. https://doi.org/10.3390/nu14193917
APA StyleMatsuda, T., Suzuki, H., Sugano, Y., Suzuki, Y., Yamanaka, D., Araki, R., Yahagi, N., Sekiya, M., Kawakami, Y., Osaki, Y., Iwasaki, H., Hashimoto, K., Takahashi, S.-I., Hada, Y., & Shimano, H. (2022). Effects of Branched-Chain Amino Acids on Skeletal Muscle, Glycemic Control, and Neuropsychological Performance in Elderly Persons with Type 2 Diabetes Mellitus: An Exploratory Randomized Controlled Trial. Nutrients, 14(19), 3917. https://doi.org/10.3390/nu14193917