
Influence of a Nutrigenetic Intervention on Self-Efficacy, Emotions, and Rewarding Behaviors in Unhealthy Eating among Mexicans: An Exploratory Pilot Study

 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
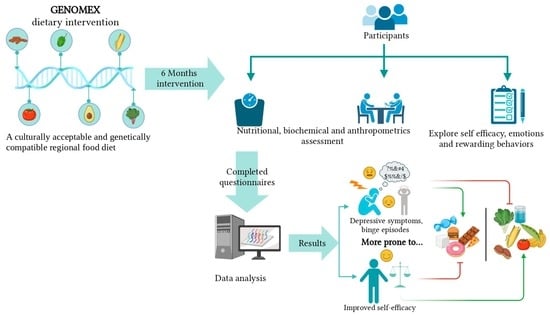
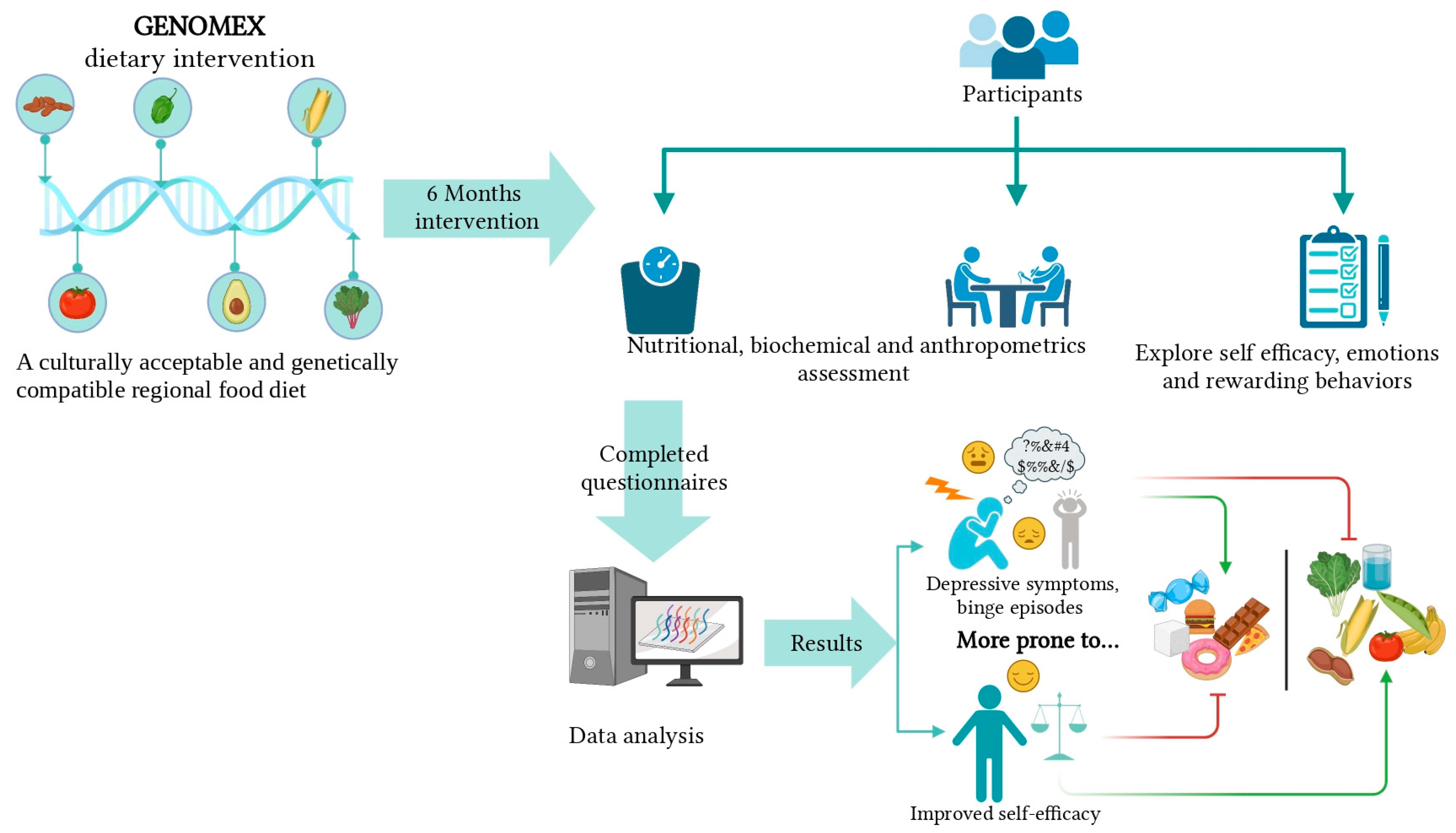
2.1. Study Design
2.2. Participants
2.3. Body Composition Assessment
2.4. Dietary Assessment
2.5. Depression Severity Assessment
2.6. Rewarding Food Behaviors
2.7. Mood and Food Behavior
2.8. Data Analysis
3. Results
3.1. Demographic and Anthropometric Characteristics
3.2. Dietary Characteristics
3.3. Symptoms of Depression
3.4. Reward-Based Eating Drive Scale
3.5. Mood and Food Behavior
3.6. Changes in Food Decisions and Self-Efficacy during the Dietary Intervention
3.7. Risk of Unhealthy Food Consumption with a Low Level of Self-Efficacy and the Presence of Binge Episodes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- OECD Obesity Update 2017. Available online: https://www.oecd.org/els/health-systems/Obesity-Update-2017.pdf (accessed on 10 August 2021).
- Hernández-Ávila, M. Encuesta Nacional de Salud y Nutrición de Medio Camino 2016: Resultados Ponderados. Available online: https://www.gob.mx/cms/uploads/attachment/file/209093/ENSANUT.pdf (accessed on 11 August 2021).
- Furst, T.; Connors, M.; Bisogni, C.A.; Sobal, J.; Falk, L.W. Food Choice: A Conceptual Model of the Process. Appetite 1996, 26, 247–266. [Google Scholar] [CrossRef] [Green Version]
- Roman, S.; Ojeda-Granados, C.; Panduro, A. Genética y Evolución de La Alimentación de La Población En México. Rev. Endo-Crinol. Nutr. 2013, 21, 42–51. [Google Scholar]
- Barquera, S.; Hernández-Barrera, L.; Tolentino, M.L.; Espinosa, J.; Ng, S.W.; Rivera, J.A.; Popkin, B.M. Energy Intake from Beverages Is Increasing among Mexican Adolescents and Adults. J. Nutr. 2008, 138, 2454–2461. [Google Scholar] [CrossRef] [PubMed]
- Gan, W.Y.; Mohamad, N.; Law, L.S. Factors Associated with Binge Eating Behavior among Malaysian Adolescents. Nutrients 2018, 10, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, J.-Y.; Kim, K.-H.; Woo, H.-Y.; Shin, D.-W.; Shin, Y.-C.; Oh, K.-S.; Shin, E.-H.; Lim, S.-W. Binge eating is associated with trait anxiety in Korean adolescent girls: A cross sectional study. BMC Womens Health 2017, 17, 8. [Google Scholar] [CrossRef] [Green Version]
- Macht, M. Characteristics of Eating in Anger, Fear, Sadness and Joy. Appetite 1999, 33, 129–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharifirad, G.; Azadbakht, L.; Feizi, A.; Hozori, M.; Mohebi, S. Predicting of perceived self efficacy in the amount of macronutrients intake in women with metabolic syndrome—2012. J. Educ. Health Promot. 2014, 3, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ha, S.A.; Lee, S.Y.; Kim, K.A.; Seo, J.S.; Sohn, C.M.; Park, H.R.; Kim, K.W. Eating habits, physical activity, nutrition knowledge, and self-efficacy by obesity status in upper-grade elementary school students. Nutr. Res. Pract. 2016, 10, 597–605. [Google Scholar] [CrossRef] [Green Version]
- Gacek, M. Association between self-efficacy and dietary behaviours of American football players in the Polish Clubs in the light of dietary recommendations for athletes. Rocz. Państwowego Zakładu Hig. 2015, 66, 361–366. [Google Scholar]
- Glasofer, D.R.; Haaga, D.A.; Ba, L.H.; Field, S.E.; Kozlosky, M.; Reynolds, J.; Yanovski, J.; Tanofsky-Kraff, M. Self-efficacy beliefs and eating behavior in adolescent girls at-risk for excess weight gain and binge eating disorder. Int. J. Eat. Disord. 2013, 46, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Kushida, O.; Iriyama, Y.; Murayama, N.; Saito, T.; Yoshita, K. Associations of self-efficacy, social support, and knowledge with fruit and vegetable consumption in Japanese workers. Asia Pac. J. Clin. Nutr. 2017, 26, 725–730. [Google Scholar]
- Nastaskin, R.S.; Fiocco, A.J. A survey of diet self-efficacy and food intake in students with high and low perceived stress. Nutr. J. 2015, 14, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robles, B.; Smith, L.V.; Ponce, M.; Piron, J.; Kuo, T. The Influence of Gender and Self-Efficacy on Healthy Eating in a Low-Income Urban Population Affected by Structural Changes to the Food Environment. J. Obes. 2014, 2014, 908391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, P.J.; Hardman, C.A. Food reward. What it is and how to measure it. Appetite 2015, 90, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epel, E.S.; Tomiyama, A.J.; Mason, A.E.; Laraia, B.A.; Hartman, W.; Ready, K.; Acree, M.; Adam, T.C.; Jeor, S.S.; Kessler, D. The Reward-Based Eating Drive Scale: A Self-Report Index of Reward-Based Eating. PLoS ONE 2014, 9, e101350. [Google Scholar] [CrossRef] [Green Version]
- Ojeda-Granados, C.; Panduro, A.; Rivera-Iñiguez, I.; Sepúlveda-Villegas, M.; Roman, S. A Regionalized Genome-Based Mexican Diet Improves Anthropometric and Metabolic Parameters in Subjects at Risk for Obesity-Related Chronic Diseases. Nutrients 2020, 12, 645. [Google Scholar] [CrossRef] [Green Version]
- Ojeda-Granados, C.; Panduro, A.; Gonzalez-Aldaco, K.; Sepulveda-Villegas, M.; Rivera-Iñiguez, I.; Roman, S. Tailoring Nutritional Advice for Mexicans Based on Prevalence Profiles of Diet-Related Adaptive Gene Polymorphisms. J. Pers. Med. 2017, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Panduro, A.; Rivera-Iñiguez, I.; Sepulveda-Villegas, M.; Roman, S. Genes, emotions and gut microbiota: The next frontier for the gastroenterologist. World J. Gastroenterol. 2017, 23, 3030–3042. [Google Scholar] [CrossRef]
- Garaulet, M. Chapter 22—The Mediterranean Diet and Obesity from a Nutrigenetic and Epigenetics Perspective. In The Medi-Terranean Diet; Preedy, V.R., Watson, R.R., Eds.; Academic Press: San Diego, CA, USA, 2015; pp. 237–247. ISBN 978-0-12-407849-9. [Google Scholar]
- Ojeda-Granados, C.; Roman, S. Mediterranean diet or genome-based nutrition diets in Latin America’s clinical practice guidelines for managing chronic liver diseases? Ann. Hepatol. 2021, 20, 100291. [Google Scholar] [CrossRef]
- Konttinen, H. Emotional eating and obesity in adults: The role of depression, sleep and genes. Proc. Nutr. Soc. 2020, 79, 283–289. [Google Scholar] [CrossRef]
- Patel, K.; Schlundt, D. Impact of moods and social context on eating behavior. Appetite 2001, 36, 111–118. [Google Scholar] [CrossRef]
- Collins, R.; Stafford, L.D. Feeling happy and thinking about food. Counteractive effects of mood and memory on food consumption. Appetite 2015, 84, 107–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO) Obesity and Overweight. 2017. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 30 August 2021).
- Familiar, I.; Ortiz-Panozo, E.; Hall, B.; Vieitez, I.; Romieu, I.; Lopez-Ridaura, R.; Lajous, M. Factor structure of the Spanish version of the Patient Health Questionnaire-9 in Mexican women. Int. J. Methods Psychiatr. Res. 2015, 24, 74–82. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Stuckey, H.L. Three types of interviews: Qualitative research methods in social health. J. Soc. Health Diabetes 2013, 1, 056–059. [Google Scholar] [CrossRef] [Green Version]
- Sanderson, S.C.; Diefenbach, M.A.; Streicher, S.A.; Jabs, E.W.; Smirnoff, M.; Horowitz, C.R.; Zinberg, R.; Clesca, C.; Richardson, L.D. Genetic and Lifestyle Causal Beliefs about Obesity and Associated Diseases among Ethnically Diverse Patients: A Structured Interview Study. Public Health Genom. 2013, 16, 83–93. [Google Scholar] [CrossRef] [Green Version]
- Doucerain, M.; Fellows, L.K. Eating Right: Linking Food-Related Decision-Making Concepts from Neuroscience, Psychology, and Education. Mind Brain Educ. 2012, 6, 206–219. [Google Scholar] [CrossRef]
- Gase, L.N.; Glenn, B.; Kuo, T. Self-Efficacy as a Mediator of the Relationship Between the Perceived Food Environment and Healthy Eating in a Low Income Population in Los Angeles County. J. Immigr. Minor. Health 2016, 18, 345–352. [Google Scholar] [CrossRef]
- Van Strien, T.; Cebolla, A.; Etchemendy, E.; Gutiérrez-Maldonado, J.; Ferrer-García, M.; Botella, C.; Baños, R. Emotional eating and food intake after sadness and joy. Appetite 2013, 66, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Goldschmidt, A.B.; Wall, M.M.; Choo, T.-H.J.; Bruening, M.; Eisenberg, M.E.; Neumark-Sztainer, D. Examining associations between adolescent binge eating and binge eating in parents and friends. Int. J. Eat. Disord. 2013, 47, 325–328. [Google Scholar] [CrossRef] [Green Version]
- Leung, S.L.; Barber, J.A.; Burger, A.; Barnes, R.D. Factors associated with healthy and unhealthy workplace eating behaviours in individuals with overweight/obesity with and without binge eating disorder. Obes. Sci. Pract. 2018, 4, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Romero-Hidalgo, S.; Molina, T.V.; González-Barrios, J.A.; Canizales-Quinteros, S.; Arellano, M.E.R.; Yañez-Velazco, L.B.; Bernal-Alcantara, D.A.; Villa, A.R.; Antuna-Puente, B.; Acuña-Alonzo, V.; et al. Carbohydrate Intake Modulates the Effect of the ABCA1-R230C Variant on HDL Cholesterol Concentrations in Premenopausal Women. J. Nutr. 2011, 142, 278–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sepulveda-Villegas, M.; Roman, S.; Rivera-Iñiguez, I.; Ojeda-Granados, C.; Gonzalez-Aldaco, K.; Torres-Reyes, L.A.; Jose-Abrego, A.; Panduro, A. High prevalence of nonalcoholic steatohepatitis and abnormal liver stiffness in a young and obese Mexican population. PLoS ONE 2019, 14, e0208926. [Google Scholar] [CrossRef]
- Campos-Perez, W.; Gonzalez-Becerra, K.; Ramos-Lopez, O.; Silva-Gomez, J.A.; Barron-Cabrera, E.; Roman, S.; Panduro, A.; Martinez-Lopez, E. Same Dietary but Different Physical Activity Pattern in Normal-Weight and Overweight Mexican Subjects. J. Food Nutr. Res. 2016, 4, 729–735. [Google Scholar] [CrossRef]
- Gutiérrez-Pliego, L.E.; Camarillo-Romero, E.D.S.; Montenegro-Morales, L.P.; Garduño-García, J.D.J. Dietary patterns associated with body mass index (BMI) and lifestyle in Mexican adolescents. BMC Public Health 2016, 16, 850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francis, H.M.; Stevenson, R.; Chambers, J.R.; Gupta, D.; Newey, B.; Lim, C.K. A brief diet intervention can reduce symptoms of depression in young adults—A randomised controlled trial. PLoS ONE 2019, 14, e0222768. [Google Scholar] [CrossRef]
- Fuller, N.R.; Burns, J.; Sainsbury, A.; Horsfield, S.; da Luz, F.; Zhang, S.; Denyer, G.; Markovic, T.P.; Caterson, I.D. Examining the association between depression and obesity during a weight management programme. Clin. Obes. 2017, 7, 354–359. [Google Scholar] [CrossRef]
- Dalton, M.; Blundell, J.; Finlayson, G. Effect of BMI and Binge Eating on Food Reward and Energy Intake: Further Evidence for a Binge Eating Subtype of Obesity. Obes. Facts 2013, 6, 348–359. [Google Scholar] [CrossRef]
- Moreno-Padilla, M.; Fernández-Serrano, M.J.; Del Paso, G.A.R. Risky decision-making after exposure to a food-choice task in excess weight adolescents: Relationships with reward-related impulsivity and hunger. PLoS ONE 2018, 13, e0202994. [Google Scholar] [CrossRef] [PubMed]
- Yeomans, M.R.; Brace, A. Cued to Act on Impulse: More Impulsive Choice and Risky Decision Making by Women Susceptible to Overeating after Exposure to Food Stimuli. PLoS ONE 2015, 10, e0137626. [Google Scholar] [CrossRef] [Green Version]
- Berg, K.C.; Cao, L.; Crosby, R.D.; Engel, S.G.; Peterson, C.B.; Crow, S.J.; Le Grange, D.; Mitchell, J.E.; Lavender, J.M.; Durkin, N.; et al. Negative affect and binge eating: Reconciling differences between two analytic approaches in ecological momentary assessment research. Int. J. Eat. Disord. 2017, 50, 1222–1230. [Google Scholar] [CrossRef]
- Kukk, K.; Akkermann, K. Fluctuations in negative emotions predict binge eating both in women and men: An experience sampling study. Eat. Disord. 2016, 25, 1–15. [Google Scholar] [CrossRef]
- DiFeliceantonio, A.; Coppin, G.; Rigoux, L.; Thanarajah, S.E.; Dagher, A.; Tittgemeyer, M.; Small, D.M. Supra-Additive Effects of Combining Fat and Carbohydrate on Food Reward. Cell Metab. 2018, 28, 33–44.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, M.-W.; Tan, A.; Ling, J.; Wegener, D.T.; Robbins, L.B. Mediators of intervention effects on dietary fat intake in low-income overweight or obese women with young children. Appetite 2020, 151, 104700. [Google Scholar] [CrossRef] [PubMed]
- Nassim, G.; Redmond, M.; Ofei-Dodoo, S.; Benton, M.; Lu, K. Nutrition Self-Efficacy and Dietary Patterns among Older African American Women in Kansas. Kans. J. Med. 2020, 13, 209–213. [Google Scholar] [CrossRef]
- Prestwich, A.; Kellar, I.; Parker, R.; Macrae, S.; Learmonth, M.; Sykes, B.; Taylor, N.; Castle, H. How can self-efficacy be increased? Meta-analysis of dietary interventions. Health Psychol. Rev. 2013, 8, 270–285. [Google Scholar] [CrossRef]
- Horning, M.L.; Hill, T.; Martin, C.L.; Hassan, A.; Petrovskis, A.; Bohen, L. The East Side Table Make-at-Home Meal-Kit Program is feasible and acceptable: A pilot study. Appetite 2021, 160, 105087. [Google Scholar] [CrossRef]
- Fernández-Medina, I.M.; Ruíz-Fernández, M.D.; Hernández-Padilla, J.M.; Granero-Molina, J.; Fernández-Sola, C.; Jiménez-Lasserrotte, M.D.M.; Lirola, M.-J.; Cortés-Rodríguez, A.E.; López-Rodríguez, M.M. Adherence to the Mediterranean Diet and Self-efficacy as Mediators in the Mediation of Sleep Quality and Grades in Nursing Students. Nutrients 2020, 12, 3265. [Google Scholar] [CrossRef]
- Luszczynska, A.; Tryburcy, M.; Schwarzer, R. Improving fruit and vegetable consumption: A self-efficacy intervention compared with a combined self-efficacy and planning intervention. Health Educ. Res. 2006, 22, 630–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandura, A. Health Promotion by Social Cognitive Means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.O.; Velicer, W.F. The Transtheoretical Model of Health Behavior Change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Topics | Questions (Q) | Probes | References |
|---|---|---|---|
| Frequency of unhealthy food decision making | Q1. When deciding what to eat every day, are you aware of how often you make unhealthy food choices? Rarely, Frequently, or Always? | Describe examples of those times (food shopping, food preparation, snaking, travels) | [31] |
| Perceived self-efficacy | Q2. How confident do you feel about following a healthy diet? Low, Moderate, or High? | Explain that self-efficacy means how confident is a person to perform a behavior (following a healthy diet) | [13,14,15,32] |
| Mood and food intake | Q3. Does your mood influence your food intake? | Discuss if the participant considers being an emotional eater | [8,33] |
| Q4. In what way your mood influences your food intake? | Discuss if mood makes participant eat more, eat less, or not eat | ||
| Binge episodes | Q5. Have you experienced a binge episode? | Explain that the episode characterizes by eating large quantities of food rapidly to the point of discomfort and without control | [6,7,34,35] |
| Q6. What triggers the binge episode? Q7. What flavor induces you to binge eat? | Describe and discuss with participant instances that could trigger binge episodes and ask for the most frequent |
| Variable | Normal Weight | Overweight | Obesity |
|---|---|---|---|
| Subjects n (%) | 5 (17.85) | 11 (39.29) | 12 (42.86) |
| Age (years) | 51 ± 4.24 | 43.64 ± 11.87 | 39.58 ± 13.07 |
| Weight (kg) | 60.12 ± 6.83 | 70.38 ± 5.81 | 90.93 ± 16.6 |
| BMI (kg/m2) | 23.72 ± 0.48 | 26.90 ± 1.20 | 34.37 ± 4.15 |
| Body fat (%) | 31.02 ± 1.82 | 31.15 ± 5.23 | 40.08 ± 4.51 |
| Variable | Normal Weight (n = 5) | Overweight (n = 11) | Obese (n = 12) | p |
|---|---|---|---|---|
| Energy (kcal/day) | 2047.80 ± 637.16 | 2053.20 ± 720.10 | 2510.97 ± 770.93 | 0.034 a |
| Proteins (%) | 21.60 ± 7.50 | 16.90 ± 4.94 | 17.53 ± 4.55 | 0.152 a |
| Total fat (%) | 32.20 ± 4.91 | 33.10 ± 8.36 | 31.41 ± 8.15 | 0.755 b |
| Carbohydrates (%) | 49.40 ± 10.64 | 52.45 ± 10.52 | 52.71 ± 7.81 | 0.744 b |
| Sugars servings | 1.33 ± 1.22 | 4.95 ± 4.26 | 6.66 ± 4.80 | 0.010 a,* |
| Meats servings | 8.53 ± 6.34 | 7.17 ± 5.75 | 9.28 ± 4.96 | 0.377 a |
| Refined grains servings | 7.71 ± 2.47 | 7.42 ± 2.41 | 11.37 ± 3.99 | <0.001 a,** |
| Oils servings | 2.10 ± 1.59 | 3.83 ± 2.80 | 5.18 ± 4.09 | 0.132 a |
| Milk servings | 1.14 ± 0.86 | 0.93 ± 0.81 | 0.75 ± 1.17 | 0.663 a |
| Fruits servings | 3.80 ± 2.96 | 2.94 ± 2.06 | 2.41 ± 1.96 | 0.321 a |
| Vegetables servings | 3.43 ± 3.51 | 2.97 ± 2.05 | 3.34 ± 2.56 | 0.850 a |
| Legumes servings | 0.56 ± 0.95 | 0.30 ± 0.41 | 0.77 ± 1.04 | 0.258 b |
| Variable | Baseline (n = 28) | 3 Months (n = 28) | 6 Months (n = 28) | p |
|---|---|---|---|---|
| Energy (kcal/day) | 2238.74 ± 712.97 | 1498.13 ± 418.59 * | 1748.58 ± 639.93 ** | 0.002 |
| Proteins (%) | 17.74 ± 4.06 | 19.96 ± 5.17 | 23.90 ± 27.41 | 0.182 |
| Total fat (%) | 31.06 ± 7.95 | 28.21 ± 9.16 | 36.70 ± 26.50 | 0.192 |
| Carbohydrates (%) | 53.64 ± 8.98 | 54.63 ± 10.57 | 50.93 ± 9.31 | 0.160 a |
| Sugars servings | 5.12 ± 4.38 | 1.52 ± 2.02 * | 1.63 ± 1.90 ** | <0.001 |
| Meats servings | 7.78 ± 4.40 | 5.74 ± 3.20 | 7.00 ± 2.77 | 0.377 |
| Refined grains servings | 9.28 ± 3.85 | 6.57 ± 2.74 * | 7.48 ± 8.27 | 0.003 |
| Oils servings | 4.31 ± 3.88 | 2.62 ± 1.95 | 3.45 ± 4.37 | 0.437 |
| Milk servings | 1.03 ± 1.18 | 0.30 ± 0.60 * | 0.18 ± 0.39 ** | <0.001 |
| Fruits servings | 3.16 ± 2.02 | 2.60 ± 1.94 | 3.43 ± 2.06 | 0.527 |
| Vegetables servings | 3.04 ± 2.61 | 5.05 ± 3.37 * | 5.95 ± 3.56 ** | <0.001 |
| Legumes servings | 0.63 ± 0.98 | 0.68 ± 1.17 * | 0.75 ± 0.93 ** | <0.001 a |
| Severity of Depression Symptoms | Baseline n (%) | 3 Months n (%) | 6 Months n (%) | Change (%) | pa |
|---|---|---|---|---|---|
| Minimal | 13 (46.4) | 12 (42.9) | 15 (53.5) | 15.3 | 0.285 |
| Mild | 11 (39.3) | 11 (39.3) | 10 (35.7) | −9.2 | 0.402 |
| Moderate | 3 (10.7) | 5 (17.8) | 2 (7.14) | −33.3 | 0.352 |
| Moderately severe | 1 (3.6) | 0 | 1 (3.5) | −2.7 | 0.495 |
| Reward Scale | Baseline (n = 28) | 3 Months (n = 28) | 6 Months (n = 28) | p |
|---|---|---|---|---|
| Score | 1.26 ± 0.81 | 0.94 ± 0.62 | 1.05 ± 0.069 | 0.368 a |
| Low Self-Efficacy Level a | ||
| Characteristic | OR, 95% CI | p |
| High consumption of fats | 10.89, 1.91–62.15 | 0.005 |
| High consumption of saturated fats | 1.257, 1.001–1.577 | 0.049 |
| Low consumption of vegetables | 1.671, 1.191–2.345 | 0.003 |
| Low consumption of fiber | 1.093, 1.015–1.178 | 0.019 |
| Binge-Eating Episodes b | ||
| Characteristic | OR, 95% CI | p |
| High consumption of fats (servings) | 1.221, 1.053–1.416 | 0.008 |
| High consumption of refined grains (servings) | 1.134, 1.051–1.223 | 0.001 |
| High consumption of meats (servings) | 1.160, 1.058–1.272 | 0.002 |
| High consumption of sugars (servings) | 1.192, 1.053–1.349 | 0.006 |
| High consumption of sugars (gr) | 1.023, 1.009–1.038 | 0.002 |
| High energy consumption (kcal) | 1.000, 1.000–1.001 | 0.002 |
| High consumption of carbohydrates (%) | 1.022, 1.008–1.035 | 0.001 |
| High consumption of fats (%) | 1.038, 1.015–1.062 | 0.001 |
| High consumption of saturated fats (%) | 1.135, 1.049–1.228 | 0.002 |
| High consumption of proteins (%) | 1.066, 1.024–1.109 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivera-Iñiguez, I.; Panduro, A.; Villaseñor-Bayardo, S.J.; Sepulveda-Villegas, M.; Ojeda-Granados, C.; Roman, S. Influence of a Nutrigenetic Intervention on Self-Efficacy, Emotions, and Rewarding Behaviors in Unhealthy Eating among Mexicans: An Exploratory Pilot Study. Nutrients 2022, 14, 213. https://doi.org/10.3390/nu14010213
Rivera-Iñiguez I, Panduro A, Villaseñor-Bayardo SJ, Sepulveda-Villegas M, Ojeda-Granados C, Roman S. Influence of a Nutrigenetic Intervention on Self-Efficacy, Emotions, and Rewarding Behaviors in Unhealthy Eating among Mexicans: An Exploratory Pilot Study. Nutrients. 2022; 14(1):213. https://doi.org/10.3390/nu14010213
Chicago/Turabian StyleRivera-Iñiguez, Ingrid, Arturo Panduro, Sergio Javier Villaseñor-Bayardo, Maricruz Sepulveda-Villegas, Claudia Ojeda-Granados, and Sonia Roman. 2022. "Influence of a Nutrigenetic Intervention on Self-Efficacy, Emotions, and Rewarding Behaviors in Unhealthy Eating among Mexicans: An Exploratory Pilot Study" Nutrients 14, no. 1: 213. https://doi.org/10.3390/nu14010213
APA StyleRivera-Iñiguez, I., Panduro, A., Villaseñor-Bayardo, S. J., Sepulveda-Villegas, M., Ojeda-Granados, C., & Roman, S. (2022). Influence of a Nutrigenetic Intervention on Self-Efficacy, Emotions, and Rewarding Behaviors in Unhealthy Eating among Mexicans: An Exploratory Pilot Study. Nutrients, 14(1), 213. https://doi.org/10.3390/nu14010213