The Effect of Whey and Soy Protein Isolates on Cognitive Function in Older Australians with Low Vitamin B12: A Randomised Controlled Crossover Trial


Abstract
1. Introduction
2. Materials and Methods
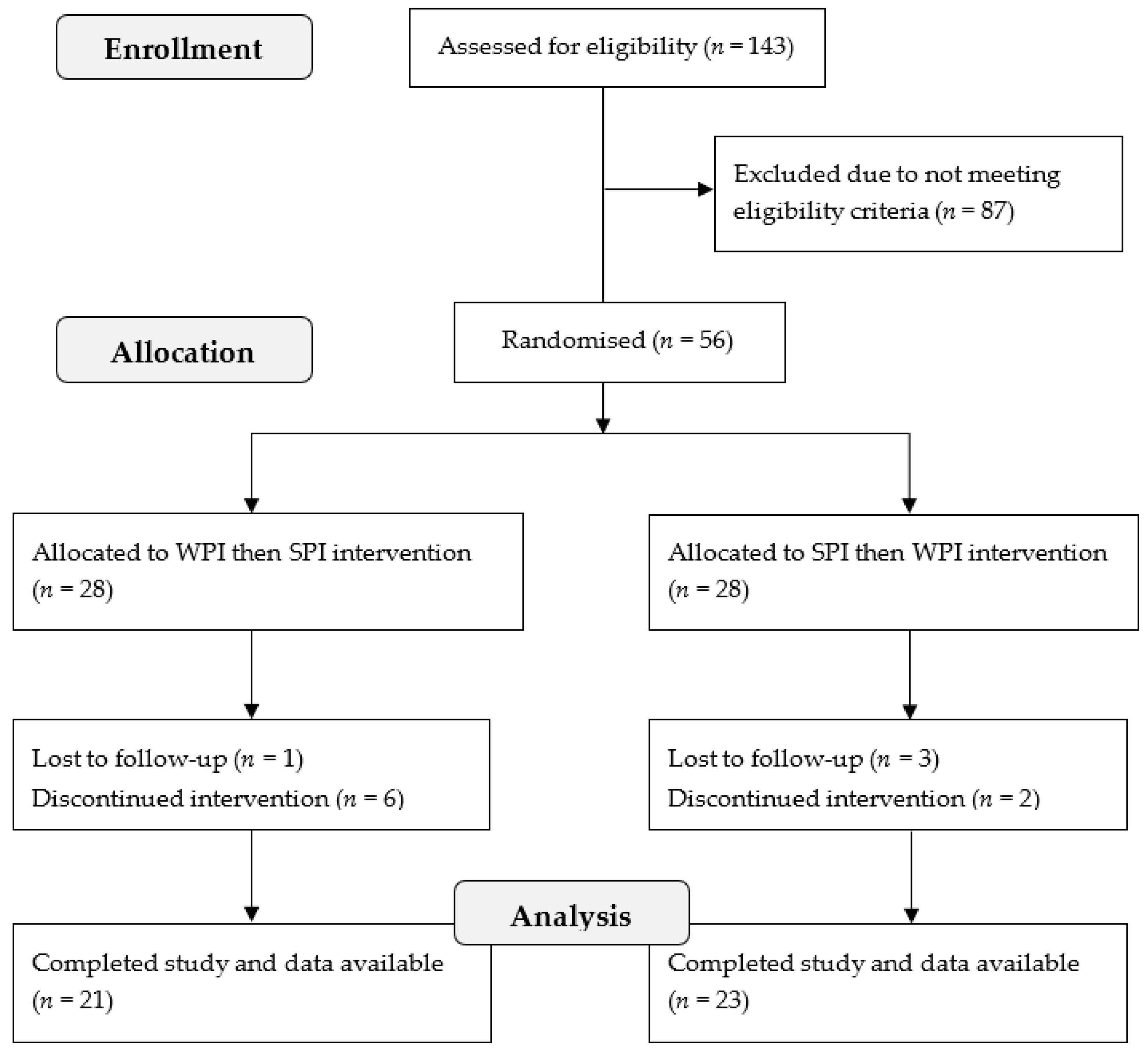
2.1. Screening and Recruitment of Participants
2.2. Intervention Design
2.3. Nutritional Profile of WPI and SPI
2.4. Biochemical Outcome Measures
2.5. Tests of Cognitive Function
2.5.1. Immediate Word Memory
2.5.2. Processing Speed
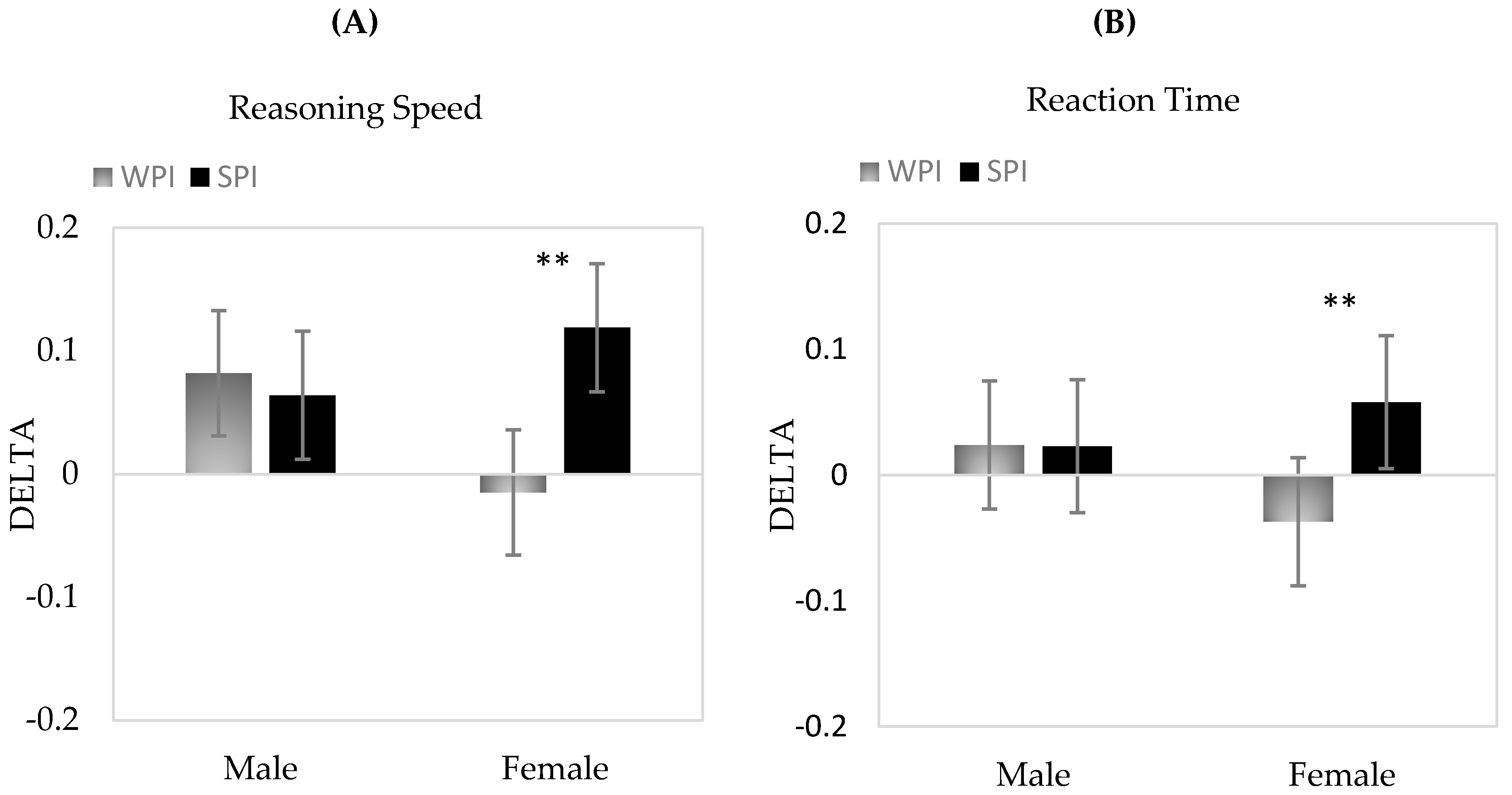
2.5.3. Reaction Time/Attention
2.5.4. Verbal Working Memory
2.5.5. Numerical Working Memory
2.5.6. Delayed Word Memory
2.5.7. Reasoning Speed
2.6. Sample Size, Data Processing and Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Williams, K.N.; Kemper, S. Interventions to Reduce Cognitive Decline in Aging. J. Psychosoc. Nurs. Ment. Health Serv. 2010, 48, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Salthouse, T.A. What and when of cognitive aging. Curr. Dir. Psychol. Sci. 2004, 13, 140–144. [Google Scholar] [CrossRef]
- Ogawa, S. Nutritional management of older adults with cognitive decline and dementia. Geriatr. Gerontol. Int. 2014, 14 (Suppl. 2), 17–22. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C. Nutritional determinants of cognitive aging and dementia. Proc. Nutr. Soc. 2012, 71, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Solfrizzi, V.; Panza, F.; Frisardi, V.; Seripa, D.; Logroscino, G.; Imbimbo, B.P.; Pilotto, A. Diet and Alzheimer’s disease risk factors or prevention: The current evidence. Expert Rev. Neurother. 2011, 11, 677–708. [Google Scholar] [CrossRef] [PubMed]
- Duthie, S.J.; Whalley, L.J.; Collins, A.R.; Leaper, S.; Berger, K.; Deary, I.J. Homocysteine, B vitamin status, and cognitive function in the elderly. Am. J. Clin. Nutr. 2002, 75, 908–913. [Google Scholar] [CrossRef]
- Riggs, K.M.; Spiro, A., 3rd; Tucker, K.; Rush, D. Relations of vitamin B-12, vitamin B-6, folate, and homocysteine to cognitive performance in the Normative Aging Study. Am. J. Clin. Nutr. 1996, 63, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Jensen, E.; Dehlin, O.; Erfurth, E.M.; Hagberg, B.; Samuelsson, G.; Svensson, T.; Hultberg, B. Plasma homocysteine in 80-year-olds: Relationships to medical, psychological and social variables. Arch. Gerontol. Geriatr. 1998, 26, 215–226. [Google Scholar] [CrossRef]
- Refsum, H.; Nurk, E.; Smith, A.D.; Ueland, P.M.; Gjesdal, C.G.; Bjelland, I.; Tverdal, A.; Tell, G.S.; Nygard, O.; Vollset, S.E. The Hordaland Homocysteine Study: A community-based study of homocysteine, its determinants, and associations with disease. J. Nutr. 2006, 136, 1731S–1740S. [Google Scholar] [CrossRef]
- Camfield, D.A.; Owen, L.; Scholey, A.B.; Pipingas, A.; Stough, C. Dairy constituents and neurocognitive health in ageing. Br. J. Nutr. 2011, 106, 159–174. [Google Scholar] [CrossRef]
- McCracken, C.; Hudson, P.; Ellis, R.; McCaddon, A.; Medical Research Council Cognitive Function and Ageing Study. Methylmalonic acid and cognitive function in the Medical Research Council Cognitive Function and Ageing Study. Am. J. Clin. Nutr. 2006, 84, 1406–1411. [Google Scholar] [PubMed]
- Vogel, T.; Dali-Youcef, N.; Kaltenbach, G.; Andrès, E. Homocysteine, vitamin B12, folate and cognitive functions: A systematic and critical review of the literature. Int. J. Clin. Pract. 2009, 63, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Flood, V.M.; Smith, W.T.; Webb, K.L.; Rochtchina, E.; Anderson, V.E.; Mitchell, P. Prevalence of low serum folate and vitamin B12 in an older Australian population. Aust. N. Z. J. Public Health 2006, 30, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Mirkazemi, C.; Peterson, G.M.; Tenni, P.C.; Jackson, S.L. Vitamin B12 deficiency in Australian residential aged care facilities. J. Nutr. Health Aging 2012, 16, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Van Asselt, D.Z.; de Groot, L.C.; van Staveren, W.A.; Blom, H.J.; Wevers, R.A.; Biemond, I.; Hoefnagels, W.H. Role of cobalamin intake and atrophic gastritis in mild cobalamin deficiency in older Dutch subjects. Am. J. Clin. Nutr. 1998, 68, 328–334. [Google Scholar] [CrossRef]
- Lindenbaum, J.; Rosenberg, I.H.; Wilson, P.W.; Stabler, S.P.; Allen, R.H. Prevalence of cobalamin deficiency in the Framingham elderly population. Am. J. Clin. Nutr. 1994, 60, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Green, T.J.; Venn, B.J.; Skeaff, C.M.; Williams, S.M. Serum vitamin B12 concentrations and atrophic gastritis in older New Zealanders. Eur. J. Clin. Nutr. 2005, 59, 205–210. [Google Scholar] [CrossRef]
- Clarke, R.; Grimley Evans, J.; Schneede, J.; Nexo, E.; Bates, C.; Fletcher, A.; Prentice, A.; Johnston, C.; Ueland, P.M.; Refsum, H.; et al. Vitamin B12 and folate deficiency in later life. Age Ageing 2004, 33, 34–41. [Google Scholar] [CrossRef]
- O’Leary, F.; Allman-Farinelli, M.; Samman, S. Vitamin B(1)(2) status, cognitive decline and dementia: A systematic review of prospective cohort studies. Br. J. Nutr. 2012, 108, 1948–1961. [Google Scholar] [CrossRef]
- Clarke, R.; Birks, J.; Nexo, E.; Ueland, P.M.; Schneede, J.; Scott, J.; Molloy, A.; Evans, J.G. Low vitamin B-12 status and risk of cognitive decline in older adults. Am. J. Clin. Nutr. 2007, 86, 1384–1391. [Google Scholar] [CrossRef]
- Tangney, C.C.; Tang, Y.; Evans, D.A.; Morris, M.C. Biochemical indicators of vitamin B12 and folate insufficiency and cognitive decline. Neurology 2009, 72, 361–367. [Google Scholar] [CrossRef]
- Hooshmand, B.; Solomon, A.; Kareholt, I.; Leiviska, J.; Rusanen, M.; Ahtiluoto, S.; Winblad, B.; Laatikainen, T.; Soininen, H.; Kivipelto, M. Homocysteine and holotranscobalamin and the risk of Alzheimer disease: A longitudinal study. Neurology 2010, 75, 1408–1414. [Google Scholar] [CrossRef]
- Kivipelto, M.; Annerbo, S.; Hultdin, J.; Bäckman, L.; Viitanen, M.; Fratiglioni, L.; Lökk, J. Homocysteine and holo-transcobalamin and the risk of dementia and Alzheimers disease: A prospective study. Eur. J. Neurol. 2009, 16, 808–813. [Google Scholar] [CrossRef]
- Clarke, R.; Sherliker, P.; Hin, H.; Nexo, E.; Hvas, A.M.; Schneede, J.; Birks, J.; Ueland, P.M.; Emmens, K.; Scott, J.M.; et al. Detection of vitamin B12 deficiency in older people by measuring vitamin B12 or the active fraction of vitamin B12, holotranscobalamin. Clin. Chem. 2007, 53, 963–970. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.W.; Garrod, M.G.; Rockwood, A.L.; Kushnir, M.M.; Allen, L.H.; Haan, M.N.; Green, R. Measurement of total vitamin B12 and holotranscobalamin, singly and in combination, in screening for metabolic vitamin B12 deficiency. Clin. Chem. 2006, 52, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Hin, H.; Clarke, R.; Sherliker, P.; Atoyebi, W.; Emmens, K.; Birks, J.; Schneede, J.; Ueland, P.M.; Nexo, E.; Scott, J.; et al. Clinical relevance of low serum vitamin B12 concentrations in older people: The Banbury B12 study. Age Ageing 2006, 35, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Vogiatzoglou, A.; Refsum, H.; Johnston, C.; Smith, S.M.; Bradley, K.M.; de Jager, C.; Budge, M.M.; Smith, A.D. Vitamin B12 status and rate of brain volume loss in community-dwelling elderly. Neurology 2008, 71, 826–832. [Google Scholar] [CrossRef]
- Tangney, C.C.; Aggarwal, N.T.; Li, H.; Wilson, R.S.; Decarli, C.; Evans, D.A.; Morris, M.C. Vitamin B12, cognition, and brain MRI measures: A cross-sectional examination. Neurology 2011, 77, 1276–1282. [Google Scholar] [CrossRef]
- Levitt, M.; Wilt, T.; Shaukat, A. Clinical implications of lactose malabsorption versus lactose intolerance. J. Clin. Gastroenterol. 2013, 47, 471–480. [Google Scholar] [CrossRef]
- Markus, C.R.; Olivier, B.; de Haan, E.H. Whey protein rich in alpha-lactalbumin increases the ratio of plasma tryptophan to the sum of the other large neutral amino acids and improves cognitive performance in stress-vulnerable subjects. Am. J. Clin. Nutr. 2002, 75, 1051–1056. [Google Scholar] [CrossRef]
- Dhillon, V.S.; Zabaras, D.; Almond, T.; Cavuoto, P.; James-Martin, G.; Fenech, M. Whey protein isolate improves vitamin B12 and folate status in elderly Australians with subclinical deficiency of vitamin B12. Mol. Nutr. Food Res. 2017, 61, 1600915. [Google Scholar] [CrossRef] [PubMed]
- Inquisit 4 Computer Software, Millisecond Software: Seattle, WA, USA, 2015.
- Wilson, M. Mrc Psycholinguistic Database—Machine-Usable Dictionary, Version 2.00. Behav. Res. Meththods Instrum. Comput. 1988, 20, 6–10. [Google Scholar] [CrossRef]
- Zajac, I.T.; Burns, N.R.; Nettelbeck, T. Do Purpose-Designed Auditory Tasks Measure General Speediness? Int. J. Intell. Sci. 2012, 2, 23–31. [Google Scholar] [CrossRef]
- Ekstrom, R.B.; French, J.W.; Harman, H.H.; Derman, D. Kit of Factor-Referenced Cognitive Tests; Educational Testing Service: Princeton, NJ, USA, 1976. [Google Scholar]
- Scholey, A.; Ossoukhova, A.; Owen, L.; Ibarra, A.; Pipingas, A.; He, K.; Roller, M.; Stough, C. Effects of American ginseng (Panax quinquefolius) on neurocognitive function: An acute, randomised, double-blind, placebo-controlled, crossover study. Psychopharmacology 2010, 212, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.R. Reaction time and psycyometric g. In A Model for Intelligence; Eysenck, H.J., Ed.; Springer: Berlin, Germany, 1982; pp. 93–132. [Google Scholar]
- Diascro, M.N.; Brody, N. Odd-Man-out and Intelligence. Intelligence 1994, 19, 79–92. [Google Scholar] [CrossRef]
- Danthiir, V.; Wilhelm, O.; Schulze, R.; Roberts, R.D. Factor structure and validity of paper-and-pencil measures of mental speed: Evidence for a higher-order model? Intelligence 2005, 33, 491–514. [Google Scholar] [CrossRef]
- Kritz-Silverstein, D.; Von Muhlen, D.; Barrett-Connor, E.; Mathias, B. Isoflavones and cognitive function in older women: The SOy and Postmenopausal Health in AGing (SOPHIA) Study. Menopause 2003, 10, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.-F.; Chen, J.-J.; Zhou, X.-Y.; Ren, Y.-F.; Huang, W.; Zhou, J.-J.; Xie, P. Do soy isoflavones improve cognitive function in postmenopausal women? A meta-analysis. Menopause 2015, 22, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.D.; Smith, S.M.; de Jager, C.A.; Whitbread, P.; Johnston, C.; Agacinski, G.; Oulhaj, A.; Bradley, K.M.; Jacoby, R.; Refsum, H. Homocysteine-Lowering by B Vitamins Slows the Rate of Accelerated Brain Atrophy in Mild Cognitive Impairment: A Randomized Controlled Trial. PLoS ONE 2010, 5, e12244. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.; Elashoff, D.; Di, L.; Teng, E.; Melchor, S.; Kim, J.; Lu, P.-H. Age-associated memory impairment increases risk of conversion to MCI and dementia. Alzheimer’s Dement. 2012, 8, P544. [Google Scholar] [CrossRef]
- Yantcheva, B.; Golley, S.; Topping, D.; Mohr, P. Food avoidance in an Australian adult population sample: The case of dairy products. Public Health Nutr. 2016, 19, 1616–1623. [Google Scholar] [CrossRef] [PubMed]
- Jargin, S.V. Soy and phytoestrogens: Possible side effects. Germ. Med. Sci. 2014, 12. [Google Scholar] [CrossRef]
- Chuchu, N.; Patel, B.; Sebastian, B.; Exley, C. The aluminium content of infant formulas remains too high. BMC Pediatr. 2013, 13, 162. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Treatment Order | |
|---|---|---|
| SPI then WPI (n = 23) | WPI then SPI (n = 21) | |
| % Female (n) | 43% (10) | 52% (11) |
| Mean Age in years (SD) | 61.8 (1.94) | 61.1 (1.78) |
| Mean Body Mass Index (SD) | 26.8 (0.76) | 26.41 (0.88) |
| Composition | Type | Amount in WPI | Amount in SPI |
|---|---|---|---|
| Protein (%) | Total proteins | 93.1 (%) Dry basis | 91.0% Dry basis |
| β-Lactoglobulin | 45% | - | |
| α-Lactabumin | 15% | - | |
| GMP (glycomacropeptide) | 16% | - | |
| Minor components | 3–5% | - | |
| Immunoglobulins | 4% | - | |
| Bovine serum albumin | 1% | - | |
| Lactoferrin | 0.1% | - | |
| Fat (%) | Total fats | 1% | 2.5% |
| Saturated fats | - | 0.8% | |
| Polyunsaturated | - | 1.6% | |
| Monounsaturated | - | 0.6% | |
| Trans fatty acids | - | 0.5% | |
| Carbohydrate (%) | Total carbohydrates | 1.2% | 1% |
| Lactose | 1.2% | - | |
| Sucrose | - | <1% | |
| Vitamins (per 100 g) | Pantothenic acid | <1.0 mg | - |
| Riboflavin (B2) | 0.32 mg | - | |
| B6 | 0.22 mg | 0.1 mg | |
| Thiamine (B1) | 0.12 mg | - | |
| α-Tocopherol | <0.1 mg | - | |
| Niacin (B3) | <0.01 mg | - | |
| Folacin | 458 µg | - | |
| B12 | 6.0 µg | 0.0 µg | |
| Minerals (per 100 g) | Potassium | 1005 mg | 1300 mg |
| Calcium | 307 mg | - | |
| Phosphorus | 210 mg | - | |
| Sodium | 188 mg | 800 mg | |
| Chloride | 11 mg | - | |
| Polyphenols | Isoflavones | - | 10–30 mg |
| Cognitive Domain | Treatment | Baseline | Endpoint | Change | |||
|---|---|---|---|---|---|---|---|
| Mean | ± SE | Mean | ± SE | Mean | ± SE | ||
| Processing Speed | WPI | 0.36 | 0.01 | 0.37 | 0.01 | 0.01 | 0.00 |
| SPI | 0.37 | 0.01 | 0.37 | 0.01 | 0.00 | 0.00 | |
| Reasoning Speed | WPI | 0.83 | 0.04 | 0.86 | 0.04 | 0.04 | 0.02 |
| SPI | 0.79 | 0.04 | 0.88 | 0.04 | 0.09 | 0.02 | |
| Reaction Time/Attention | WPI | 1.67 | 0.05 | 1.67 | 0.05 | −0.01 | 0.02 |
| SPI | 1.66 | 0.05 | 1.70 | 0.05 | 0.04 | 0.02 | |
| Numeric Working Memory | WPI | 1.14 | 0.04 | 1.22 | 0.04 | 0.07 | 0.03 |
| SPI | 1.18 | 0.05 | 1.22 | 0.04 | 0.04 | 0.02 | |
| Verbal Working Memory | WPI | 0.83 | 0.03 | 0.88 | 0.03 | 0.05 | 0.02 |
| SPI | 0.85 | 0.04 | 0.91 | 0.03 | 0.06 | 0.02 | |
| Immediate Word Memory | WPI | 0.91 | 0.04 | 0.91 | 0.04 | 0.00 | 0.03 |
| SPI | 0.93 | 0.03 | 0.89 | 0.04 | −0.03 | 0.03 | |
| Delayed Word Memory | WPI | 0.82 | 0.04 | 0.81 | 0.04 | −0.02 | 0.03 |
| SPI | 0.78 | 0.04 | 0.81 | 0.04 | 0.03 | 0.03 | |
| SPI | WPI | p-Value a | |||
|---|---|---|---|---|---|
| Baseline | % Change | Baseline | % Change | ||
| Serum B12 (pmol/L) | 261.7 ± 8.45 | ↓ −9.47 | 260.2 ± 10.59 | ↓ −4.05 | 0.14 |
| Active B12 (pmol/L) | 70.16 ± 3.97 | ↓ −2.21 | 68.7 ± 4.13 | ↑ +19.08 | <0.001 |
| MMA (mol/L) | 0.26 ± 0.021 | ↑ +12.24 | 0.26 ± 0.022 | ↓ −3.96 | 0.09 |
| tHcy (mol/L) | 11.98 ± 0.53 | ↑ +3.09 | 11.89 ± 0.55 | ↓ −1.78 | 0.14 |
| Serum folate (nmol/L) | 34.78 ± 0.26 | ↓ −1.05 | 34.45 ± 1.79 | ↑ +12.92 | <0.01 |
| Δ Serum B12 | Δ Active B12 | Δ MMA | Δ tHcy | Δ Serum Folate | ||
|---|---|---|---|---|---|---|
| Δ Processing Speed | WPI | 0.09 | 0.29 * | −0.03 | −0.33 * | 0.22 |
| SPI | 0.24 | 0.06 | −0.01 | 0.17 | 0.12 | |
| Δ Reasoning Speed | WPI | −0.03 | 0.01 | −0.11 | 0.21 | −0.10 |
| SPI | 0.22 | 0.18 | −0.01 | −0.49 ** | 0.09 | |
| Δ Numeric Working Memory | WPI | 0.00 | 0.00 | 0.18 | −0.31 * | 0.03 |
| SPI | 0.07 | 0.11 | −0.11 | 0.03 | −0.04 | |
| Δ Verbal Working Memory | WPI | 0.01 | 0.10 | 0.04 | −0.24 | −0.10 |
| SPI | −0.20 | −0.05 | 0.21 | 0.23 | 0.05 | |
| Δ Reaction Time/Attention | WPI | 0.03 | 0.13 | −0.08 | −0.20 | 0.25 * |
| SPI | −0.09 | −0.03 | −0.03 | −0.06 | −0.16 | |
| Δ Immediate Word Memory | WPI | 0.11 | 0.07 | −0.11 | −0.23 | 0.15 |
| SPI | 0.15 | 0.18 | −0.02 | 0.24 | −0.14 | |
| Δ Delayed Word Memory | WPI | 0.03 | −0.02 | 0.03 | −0.06 | 0.39 ** |
| SPI | 0.03 | 0.05 | −0.15 | −0.03 | 0.12 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zajac, I.T.; Herreen, D.; Bastiaans, K.; Dhillon, V.S.; Fenech, M. The Effect of Whey and Soy Protein Isolates on Cognitive Function in Older Australians with Low Vitamin B12: A Randomised Controlled Crossover Trial. Nutrients 2019, 11, 19. https://doi.org/10.3390/nu11010019
Zajac IT, Herreen D, Bastiaans K, Dhillon VS, Fenech M. The Effect of Whey and Soy Protein Isolates on Cognitive Function in Older Australians with Low Vitamin B12: A Randomised Controlled Crossover Trial. Nutrients. 2019; 11(1):19. https://doi.org/10.3390/nu11010019
Chicago/Turabian StyleZajac, Ian T., Danielle Herreen, Kathryn Bastiaans, Varinderpal S. Dhillon, and Michael Fenech. 2019. "The Effect of Whey and Soy Protein Isolates on Cognitive Function in Older Australians with Low Vitamin B12: A Randomised Controlled Crossover Trial" Nutrients 11, no. 1: 19. https://doi.org/10.3390/nu11010019
APA StyleZajac, I. T., Herreen, D., Bastiaans, K., Dhillon, V. S., & Fenech, M. (2019). The Effect of Whey and Soy Protein Isolates on Cognitive Function in Older Australians with Low Vitamin B12: A Randomised Controlled Crossover Trial. Nutrients, 11(1), 19. https://doi.org/10.3390/nu11010019