Abstract
The authors report on a patient with ischaemic cardiopathy and chronic congestive heart failure treated with a cardiac resynchronisation therapy device with a defibrillator back-up (CRT-D), who experienced two syncopal episodes. The first syncope was associated with an episode of fast ventricular arrhythmia, correctly recognised and cardioverted by the internal defibrillator. The second episode was independent from arrhythmias but was caused by a transient decrease in cerebral flow, due to a subclavian steal syndrome. This case highlights the importance of differential diagnosis in case of syncopal episodes, even in a clinical context, particularly prone to arrhythmias, such as ischaemic cardiopathy.
Case report
A 74-year-old man with ischaemic cardiopathy and an implanted cardiac resynchronisation therapy device with a defibrillator back-up (CRT-D), was admitted to the emergency room after a syncopal episode. Interrogation of the device’s recordings showed an episode of high-rate ventricular tachycardia concomitant to the syncope, which was cardioverted by the defibrillator (Figure 1A). Coronary angiography revealed no progression of coronary artery disease.
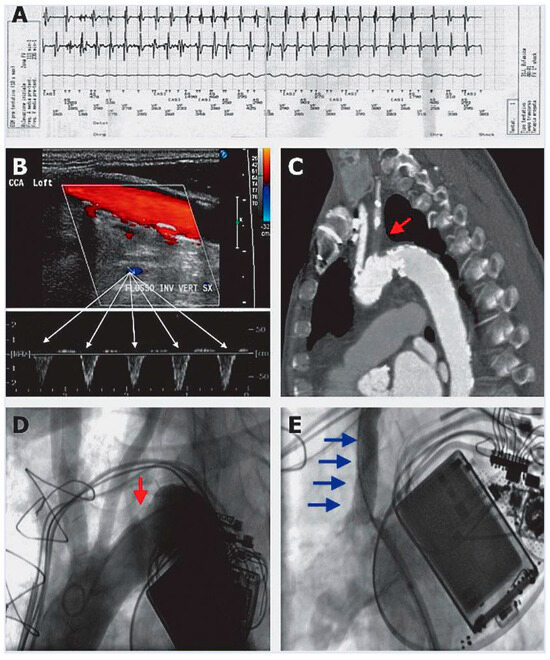
Figure 1.
(A) CRT-D recording of endocavitary electrogram showing ventricular tachycardia concomitant to first syncope. (B) Ultrasonographic evidence of reverse flow in the left vertebral artery. (C) Computed tomography sagittal section showing complete proximal occlusion of the left subclavian artery (red arrow). (D,E) Supraaortic angiography (25° left anterior oblique view) before and after percutaneous recanalisation and stenting of the left subclavian artery.
Two weeks after hospital discharge, the patient experienced a new syncopal episode; however no arrhythmia was detected by the CRT-D. At physical examination, left brachial artery pressure was lower than the right one by about 30 mm Hg. The left radial artery pulse was decreased in amplitude and delayed, compared with the right one. No carotid bruits were audible bilaterally. Supraaortic vessels duplex ultrasonography showed reverse flow in the left vertebral artery (Figure 1B) and a complete proximal occlusion of the left subclavian artery. Computed tomography angiography confirmed the findings of duplex ultrasonography, while showing an additional moderate stenosis of the basilar artery (Figure 1C).
These radiological findings supported the clinical suspicion of a subclavian steal syndrome. Thereafter, the patient underwent a percutaneous recanalisation and stenting of the proximal left subclavian artery (Figure 1D,E).
Discussion
Multiple studies have demonstrated that in high-risk patients with CRT-D, syncope is often linked to ventricular arrhythmias [1]. Nevertheless, it should not be forgotten that arrhythmias are not the only cause of syncope in patients with depressed left ventricular systolic function. Indeed, Middlekauff and co-workers showed that 12% of patients with either ischaemic or non-ischaemic dilated cardiopathy and congestive heart failure had a history of syncope, of which a cardiac origin could be identified in 48% of cases, whereas other causes were found in 52% of cases [2]. Subclavian steal syndrome has a prevalence of 2% in the overall population, and 7% in the in-hospital population [3], and should be considered especially in patients with ischaemic cardiopathy and a differential brachial systolic arterial pressure >15 mm Hg [4]. In fact, it has been clearly demonstrated that subclavian steal syndrome is correlated with current and past smoking history, systolic blood hypertension, low levels of high-density lipoprotein, and peripheral artery disease [3], which are associated with coronary artery disease.
To sum up, this report describes a patient with ischaemic cardiopathy treated with CRT-D who experienced two syncopal episodes, the first one due to arrhythmia and the second one to a subclavian steal syndrome. This report highlights the importance of differential diagnosis of syncope in patients with previous tachyarrhythmias.
Conflicts of Interest
The authors certify that there is no actual or potential conflict of interest in relation to this article.
References
- Menozzi, C.; Brignole, M.; Garcia-Civera, R.; et al. Mechanism of syncope in patients with heart disease and negative electrophysiologic test. Circulation. 2002, 5, 2741–2745. [Google Scholar] [CrossRef] [PubMed]
- Middlekaff, H.R.; Stevenson, W.G.; Stevenson, L.W.; Saxon, L.A. Syncope in advanced heart failure: high risk of sudden death regardless of origin of syncope. J Am Coll Cardiol. 1993, 21, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Shadman, R.; Criqui, M.H.; Bundens, W.P.; et al. Subclavian artery stenosis: prevalence, risk factors, and association with cardiovascular diseases. J Am Coll Cardiol. 2004, 44, 618–623. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Criqui, M.H.; McDermott, M.M.; et al. The vital prognosis of subclavian stenosis. J Am Coll Cardiol. 2007, 49, 1540–1545. [Google Scholar] [CrossRef] [PubMed]

© 2010 by the authors. Attribution-Non-Commercial-NoDerivatives 4.0.