Abstract
Graduate Medical Education trainees’ wellness has become an important topic in academic medicine. The Accreditation Council for Graduate Medical Education (ACGME) requires oversight, education, and resources, understanding that medical training happens within a complex environment. Patients, personal and psychosocial issues, overlays, administrative demands, and intense oversight at various levels add additional elements of complexity and stress. The demographics of medicine are changing, with a greater proportion of women, minorities, and international medical graduates entering training with different needs and greater expectations. GME trainees constitute a population with unique needs that demand an adaptable and broad approach toward wellbeing and training success. The University of Texas Health San Antonio (UTHSA) created the Wellness Home, a comprehensive and adaptable model inspired by those used in primary care, where support is offered to trainees and training programs. It addresses issues beyond mental health management by including interventions such as coaching, access to medical services, or financial literacy. We present here a detailed description of the program and a rationale for developing this holistic approach in other institutions. Case studies are used to illustrate the complex needs of trainees and the innovative approaches used in their support. Usage data is presented as additional evidence that this model is increasingly and successfully being used.
1. Introduction
The foundations of medicine are changing beneath our feet, with the COVID-19 pandemic and newer austerity measures further exacerbating this shifting landscape. Medical student preparation for the increasingly complex and high-acuity Graduate Medical Education (GME) environment has been impacted by cultural shifts as well, including virtual learning, isolation, and limited overnight call. Robust psycho-social support for these incoming residents is essential.
In 1967, the American Academy of Pediatrics (AAP) introduced the Medical Home concept to help coordinate the care of children with chronic health conditions. As defined by the Patient-Centered Primary Care Collaborative (PCPCC), the Medical Home is “a model or philosophy of primary care that is patient-centered, comprehensive, team-based, coordinated, accessible, and focused on quality and safety.” [1] The terms “compassionate, and culturally effective care,” were added later. This is a strategic approach to delivering high-quality, cost-effective primary healthcare. It employs a patient-centered, culturally appropriate, and team-based method to comprehensively coordinate patient care throughout the entire health system.
This model is empirically linked to meaningful benefits, including enhanced chronic disease management, greater patient and provider satisfaction, substantial cost savings, superior quality of care, and increased rates of preventive services [2,3,4].
We know that a significant number of medical trainees will experience health-deteriorating stress, burnout, and a variety of mental health concerns. In addition, they routinely face obstacles accessing behavioral health services, medical or dental care, and other wellness-enhancing services [5,6,7,8,9,10,11]. Administrative burden, proficiency with electronic health records, and other responsibilities vie for the limited time, energy, and attention that trainees need to learn the essential knowledge and procedural skills of their specialty [12,13]. The University of Texas Health at San Antonio (UTHSA) Office of Graduate Medical Education (OGME) wellness team adopted this novel approach to support the unique and wide-ranging needs of this population based on the Medical Home.
2. Approach
Inspired by the Medical Home model, the Wellness Team created a comprehensive mental health and wellness management model known as the Wellness Home. Similarly to the Medical Home, the Wellness Home is based on a philosophy that is trainee-centered, comprehensive, and team-based. In addition, it must be flexible and innovative in addressing changing needs and requirements. Another essential component is having the Wellness Home staffed by team members with a broad range of competencies, which include mentoring, coaching, and counseling. A full description of these competencies is beyond the scope of this work and will be addressed in a separate manuscript. Within the Wellness Home, we use the ENACT framework, which encourages residents to seek support for their mental wellbeing. It was created by one of the authors (VP) and developed within the UTHSA Wellness Home. It stands for Engagement, Nudging, Acknowledging, Commitment, and Translating. Trainees are engaged by the team through outreach and educational activities, group sessions, direct counseling and coaching, then nudged towards action. Residents acknowledge that they need support and commit to a plan. Finally, residents must translate these intentions into action through their values, emotional buy-in, and commitment. The ENACT framework is derived from several theories. The basic tenet is the theory of nudging popularized by behavioral economist Richard Thaler [14,15]. Other incorporated frameworks include the Salutogenesis coaching model, an adult learning model, and Victor Frankl’s existential therapy [16,17,18]. ENACT supports residents/fellows by providing assistance, resources, coaching, or therapy in their institution’s convenient local setting.
3. Initiatives
Within the Wellness Home, we divided the initiatives put forward based on desired outcomes driven by the needs of our trainees and the most effective ways to fulfill them: building awareness and interventions.
3.1. Building Awareness
Awareness of the Wellness Home programs and resources is critical for helping trainees engage in them. The Wellness Team presents these programs during orientation, offering time for questions and answers.
Lectures and workshops: Specialty programs request lectures and workshops that comply with the ACGME Common Program Requirements: Section VI.C.1.d. These may include management of stress, dealing with burnout, sleep hygiene, distress in peers, or team dynamics.
Website: Our innovative website offers information about our services and contact methods. Residents can access the Interactive Screening Program (ISP) or email the wellness team directly from the form on the website. https://uthscsa.edu/medicine/education/gme/wellness (accessed on 28 August 2025).
Podcast: In collaboration with the UTHSA Communication and Marketing, we produce the “Ripples: Physician Wellbeing” podcast with experts covering a diverse number of topics related to residents’ wellbeing. The podcast is available on the most common streaming services and has completed 4 total seasons. Since its insertion on YouTube, viewership has increased by over 600%. It now accounts for over 20% of the social media engagement for the Long School of Medicine, including all formats and platforms.
The Wellness Mosaic: The Mosaic is a purposeful compilation of wellness best practices shared with each of our GME programs’ leadership. The Mosaic presents eight domains in which wellness interventions can be most effective.
3.2. Interventions
The Behavioral Health Providers (BHPs) use a variety of interventions to support residents and fellows, including the following:
Individual and Group Therapy/Coaching: Culturally competent behavioral health treatment is offered to individuals or groups. The intervention approaches have existential and humanistic philosophic underpinnings but may also include Dialectical Behavioral Therapy (DBT), Cognitive Behavioral Therapy (CBT), the Coaching Model, and other approaches as considered appropriate. Figure 1 shows the rapid growth of the coaching and counseling programs in terms of direct counseling hours.
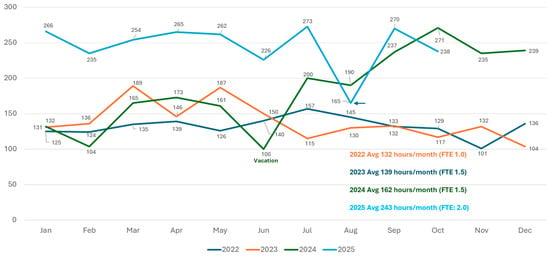
Figure 1.
Counseling/coaching direct hours per month from 2022 to 2025, year to date, noting available Full Time Equivalents (FTEs).
Connecting with Resources: The direct and comprehensive engagement with our residents allows the team to identify a broad array of resident needs and, when necessary, connect trainees to resources in the community, address immigration status concerns, assist with finding childcare, or even help individuals locate places of worship. This may also include referrals to other medical and psychological health providers, including Psychiatry, OB/GYN, or dental care, both at the institution or within the community. We have partnered with our primary care clinics, psychiatric health clinics, and dental school to offer priority appointments to our trainees. Circle of Care meetings with all PGY-1 residents provide an excellent platform for this.
Crisis Management: Although the Wellness Home is not a crisis intervention center and does not bear the responsibilities of such, Wellness Team members are often available last minute, after hours, or on weekends in response to a crisis. This may include helping a Program Director (PD) determine if there is a need to receive a resident’s immediate help, call campus police for safety checks, or provide transport for emergent psychiatric care. Residents can also call the Employee Assistance Program (EAP) for 24/7 crisis support. Figure 2 demonstrates the significant increase in residents presenting in crisis over the past 5 years.
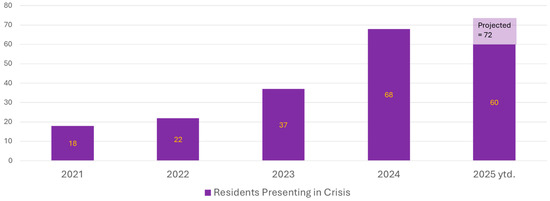
Figure 2.
Resident presentations in crisis from 2021 to 2025, year to date.
3.3. Innovative Programs Within Our Wellness Home
3.3.1. Transition Programs
The transition to residency could be among the most stressful times for a resident. The Wellness Team created a robust two-part program to support residents’ transition from day one through the first four months of training, since transition concerns continue beyond the one-month “transition period”.
Transition to Residency Risk Index (TRRI): The TRRI is a two-category, nine-item instrument created at the UTHSA to assess the risk of a difficult transition. It takes less than 10 min to complete. Category 1 addresses risk issues associated with the match process, including matching into a lower-ranked program or leaving one’s support network [19,20]. Category 2 relates to trainees’ personal stressors and health history that are known risk factors for anxiety, depression, adjustment disorders, suicidality, and other issues [21,22,23,24]. Residents score themselves and provide the PD or Program Coordinator (PC) with the result slip containing only their name and risk level. Programs are advised to intervene when residents score at the moderate or high-risk level. Interventions include increased program leadership check-ins, assignment of a mentor, community-building events, or referral to our BHPs. This questionnaire is an open-source tool [25,26,27,28,29] and has been well-received when presented in national forums. Over a five-year period, over 41% of all residents scored moderate or high-risk, with 11% scoring themselves as high-risk. See Figure 3.
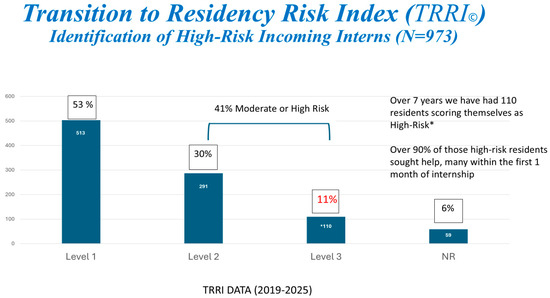
Figure 3.
Transition to Residency Risk Index (TRRI) identification of high-risk (in red) incoming interns * from 2019−2025 (N = 973).
Circle of Care (CofC): The CofC program was designed to engage with each intern in the first year of residency. The Wellness Team coordinates with departmental Wellness Chiefs in signing up each of their interns to meet with a BHP for 20–30-min slots during didactic sessions. This program follows an opt-out model where residents can decline the meeting if desired. Opt-out models have been shown to increase usage and help-seeking behaviors in residency mental health services [30,31]. This meeting does not constitute a counseling session, just a check-in to provide introductions and resources. We seek to ensure a smoother transition from medical school to residency by addressing primary care, psychiatry, or dental referrals, or connecting residents to places of worship, ethnic grocery stores, financial guidance, immigration assistance, or daycare and pet-related resources. It is also an opportunity to assess the interns’ strengths and challenges starting residency. Forty-seven percent of residents in our program required additional services after their CofC visit.
3.3.2. Longitudinal Screening and Assessment for All Resident Levels
Interactive Screening Program (ISP): The ISP is a program managed by the American Foundation for Suicide Prevention (AFSP) that allows users to assess their wellbeing by answering an anonymous and voluntary questionnaire online. The questionnaire focuses on depression, anxiety, burnout, suicidal ideation, substance abuse, and eating disorders. The responses are uploaded automatically to our BHPs, who respond within 24–48 h depending on distress level. It enables online anonymous counseling through a dialog function directly connecting our BHP and our trainees. Thanks to its anonymity, ISP dialogs have been used to support residents in dangerous situations, such as domestic violence, in which family members may be monitoring their methods of communication. To our knowledge, our program is the first to identify and describe this use for the ISP. Since the Fall of 2018, we have had a 14% completion rate for the ISP, slightly higher than the national average of 10% [32,33].
Domain Pulse Checks (DPCs): Residents and fellows at any PGY level are encouraged to explore our wellness presentations and take the DPC assessment, an 8-domain instrument based on the Substance Abuse and Mental Health Services Administration’s (SAMHSA) model and adapted to the needs of residents [34]. It enables trainees to identify life domains in balance and those that are unbalanced or neglected. Typically, this program is introduced as a didactic presentation to all the residents in a GME program. Residents can then individually sign up for a 30 min coaching session with a BHP on dates/times set by the program. In our early experience, more than 70% of those who engage in the DPCs feel more comfortable seeking support or therapy.
Struggling Learner Program: The Wellness Home also supports a Struggling Learner Program (SLP) headed by the Assistant Dean for Wellness (JC) to work with individuals referred by BHPs, their program leadership or following an academic action, i.e., academic status change or probation, in which participating in the SLP is a component of a trainee’s remediation plan [35,36]. Our BHPs routinely refer residents to the SLP for performance issues related to their medical training. The SLP has addressed Title VII, Discrimination, Title IX, Sexual Harassment, attending-peer or peer-peer conflict, resident misconduct, and even underlying medical conditions.
Worst-Case Scenario Protocol: Our worst-case scenario protocol was adapted from a similar protocol created by Luyba Konopasek, M.D., when she was the Designated Institutional Official (DIO) at New York Presbyterian Hospital. This protocol establishes a process to be activated in the event of a missing resident, resident death by suicide, or due to traumatic conditions. The Wellness Home serves a critical role as a guiding member of the response team while working with the resident’s home program, the Dean’s Office, Media Relations, UT Police, and the San Antonio Police Department as needed.
4. Case Studies—Putting It All Together
This series of case studies helps provide some detail to the complexity of issues the Wellness Home model seeks to address and the way we provide assistance. They are all deidentified but based on actual situations with our GME trainees. They demonstrate that a comprehensive wellness program within the OGME is not strictly a 9–5 job focused on typical mental health concerns such as anxiety, depression, or burnout.
- Ahmed is an intern from a Middle Eastern country in the Surgery program. He constantly worries about his people skills and cultural norms. He feels that if he makes a mistake or a patient complains, he might be deported. He has not been able to attend a mosque, and that has caused him extreme guilt. Issue: Cultural competency, international trainee issues, and case management. Approach: BHP connected Ahmed with a mosque in the area, other Middle Eastern residents, and the Office of International Students. Subsequent meetings to discuss local cultural norms and awareness, and people skills.
- Melony is a neurology resident, a wife, and a daughter. Her parents live with her. She finds it hard to spend time with her parents and spouse and take care of her patients. Her spouse has grown frustrated at their lack of privacy. Issue: Relationship issues, working hours, and societal norms for women. Approach: BHP helped Melony identify and develop healthy personal and professional boundaries that reflect her values and improve communication with her spouse.
- Sushma is a 34-year-old radiology resident, and her partner has given her an ultimatum about wanting to have a family. She feels she cannot manage pregnancy at this point in her training. Even with the help of insurance, they cannot afford the cost of freezing her eggs. She is also worried about the side effects of the medications. She heard the Ripples podcast on fertility and decided to reach out to us. Issue: Marital stress, pregnancy, fertility, and egg retrieval consultation resources. Approach: Process fears about “time running out”, connect with a fertility specialist to discuss realistic options and timelines, and have honest conversations with her partner to create a common goal that was not detrimental to her professional development.
- Alex is a PGY-3 anesthesia resident. He lives on his own and has never worried about a budget before because he lived at home during school. Recently, he spent USD 3000 on bouldering gear and USD 2500 on repairs to his car. Now he is struggling to pay for rent and food, and worries about repaying over USD 200,000 in student loans. Issue: Lack of insight and financial literacy, stress. Approach: He realized most of his stress was due to his financial situation. The BHP offered him stress-management strategies and referred him to financial literacy and consultative services for loan repayment and budgeting.
- Caroline is a critical care fellow, and she wants to seek therapy for trauma that she faced as a teenager. She makes an appointment, but needs to change it due to a last-minute call switch. She attended counseling before, but was “dismissed” for missing three appointments. Issue: Trauma, need for consultative flexibility, and potential for frequent rescheduling of appointments. Approach: Flexibility and understanding when it comes to scheduling. We prefer to meet a resident for a short session or reschedule, rather than dismiss residents, only to have them encounter this problem in the community.
5. Conclusions
Residents and fellows constitute a unique population with unique needs that demand an adaptable and flexible approach to promote their wellbeing, mental health, and success in their personal and professional lives. Programs and institutions also benefit from putting into practice programs and interventions that promote broader system-based wellness programs, which are critical in allowing us to live life to its highest potential [37,38,39]. At the UTHSA, we developed a comprehensive and integrated model, the Wellness Home, to support our trainees and promote wellbeing and health. It allows us to assess incoming and established residents, be preventive, and intervene at various degrees as needed. It also encompasses collaboration with leadership, faculty, and other services in our institution (e.g., psychiatry or dental clinics) to offer holistic support. Data from surveys and direct observation suggest the model is successful. Wellness Home also points to a series of qualities and competencies desired in those who are in charge of offering such support. Through this article, we share our experiences and the knowledge we have obtained in the hopes that other institutions can use it as a guide or foundation to develop strong wellness resources for their trainees.
Author Contributions
Conceptualization, methodology, investigation, writing—original draft preparation, V.P., A.D., and J.A.C.; writing—review and editing, V.P., A.D., J.A.C., and W.S.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study because the data do not involve specific humans. It is mostly based on administrative data recorded by the authors.
Informed Consent Statement
Participant consent was waived due to voluntary participation in any of our programs, and the complete anonymity and/or deidentification of the data (including identifiers and details in case studies). It is mostly based on administrative data recorded by the authors.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to privacy, legal, and ethical reasons.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BHP | Behavioral Health Provider |
| GME | Graduate Medical Education |
| UTHSA | University of Texas Health San Antonio |
| ACGME | Accreditation Council for Graduate Medical Education |
References
- Primary Care Collaborative. Available online: https://www.pcpcc.org/about/medical-home (accessed on 12 November 2023).
- Mills, J.; Hall, A.; Tanner, R.; Harman, J.; Wood, D.L.; Lorbeer, C. The comparative impact of different patient-centered medical home domains on satisfaction among individuals living with type II diabetes. Patient Exp. J. 2015, 2, 132–141. [Google Scholar] [CrossRef]
- Bitton, A.; Schwartz, G.; Stewart, E.E.; Henderson, D.E.; Keohane, C.A.; Bates, D.W.; Schiff, G.D. Off the Hamster Wheel? Qualitative Evaluation of a Payment-Linked Patient Centered Medical Home (PCMH) Pilot. Milbank Q. 2012, 90, 484–515. [Google Scholar] [CrossRef] [PubMed]
- Phillips, R.L.; Bronnikov, S.; Petterson, S.; Cifuentes, M.; Teevan, B.; Dodoo, M.; Pace, W.D.; West, D.R. Case Study of a Primary Care-Based Accountable Care Systems Approach to Medical Home Transformation. J. Ambul. Care Manag. 2011, 34, 67–77. [Google Scholar] [CrossRef] [PubMed][Green Version]
- American Academy of Pediatrics, Committee on Pediatric Workforce. Culturally effective pediatric care: Education and training issues. Pediatrics 1999, 103, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Ridout, K.K.; Ridout, S.J.; Guille, C.; Mata, D.A.; Akil, H.; Sen, S. Physician-Training Stress and Accelerated Cellular Aging. Biol. Psychiatry 2019, 86, 725–730. [Google Scholar] [CrossRef]
- Rangel, E.L.; Castillo-Angeles, M.; Kisat, M.; Kamine, T.H.; Askari, R. Lack of Routine Healthcare among Resident Physicians in New England. J. Am. Coll. Surg. 2020, 230, 885–892. [Google Scholar] [CrossRef]
- Cedfeldt, A.S.; Bower, E.A.; Grady-Weliky, T.A.; Flores, C.; Girard, D.E.; Choi, D. A Comparison Between Physicians and Demographically Similar Peers in Accessing Personal Health Care. Acad. Med. 2012, 87, 327–331. [Google Scholar] [CrossRef]
- Jun, T.W.; Liebert, C.A.; Esquivel, M.; Cox, J.A.; Trockel, M.; Katznelson, L. A protected time policy to improve dental health among resident physicians. J. Am. Dent. Assoc. 2019, 150, 362–368.e6. [Google Scholar] [CrossRef]
- Zottola, C.A.; Katz, A.; Leung, T.M.; Gulersen, M. Reproductive Health among Female Resident Physicians. Fertil. Steril. 2020, 114, e174–e175. [Google Scholar] [CrossRef]
- Rosen, I.M.; Christie, J.D.; Bellini, L.M.; Asch, D.A. Health and health care among housestaff in four U.S. internal medicine residency programs. J. Gen. Intern. Med. 2000, 15, 116–121. [Google Scholar] [CrossRef]
- Campbell, S.; Delva, D. Physician do not heal thyself. Survey of personal health practices among medical residents. Can. Fam. Physician 2003, 49, 1121–1127. [Google Scholar] [PubMed]
- Sakata, K.K.; Stephenson, L.S.; Mulanax, A.; Bierman, J.; Mcgrath, K.; Scholl, G.; McDougal, A.; Bearden, D.T.; Mohan, V.; Gold, J.A. Professional and interprofessional differences in electronic health records use and recognition of safety issues in critically ill patient. J. Interprof. Care 2016, 30, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Thaler, R.H.; Sunstein, C. Nudge: Improving Decisions About Health, Wealth, and Happiness; Yale University Press: New Haven, CT, USA, 2008. [Google Scholar]
- Thaler, R.H.; Sunstein, C.R.; Balz, J.P. The Behavioral Foundations of Public Policy; Shafir, E., Ed.; Princeton University Press: Princeton, NJ, USA, 2014; pp. 245–257. [Google Scholar]
- Berfield, K. How does the adult surgeon learn? Thorac. Surg. Clin. 2019, 29, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Gray, D.; Burls, A.; Kogan, M. Salutogenisis and coaching: Testing a proof of concept to develop a model for practitioners. Int. J. Evid. Based Coach. Mentor. 2014, 12, 41–58. [Google Scholar]
- Bushkin, H.; van Niekerk, R.; Stroud, L. Searching for Meaning in Chaos: Viktor Frankl’s Story. Eur. J. Psychol. 2021, 17, 233–242. [Google Scholar] [CrossRef]
- Leigh-Hunt, N.; Bagguley, D.; Bash, K.; Turner, V.; Turnbull, S.; Valtorta, N.; Caan, W. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health 2017, 152, 157–171. [Google Scholar] [CrossRef]
- Dyrbye, L.N.; Burke, S.E.; Hardeman, R.R.; Herrin, J.; Wittlin, N.M.; Yeazel, M.; Dovidio, J.F.; Cunningham, B.; White, R.O.; Phelan, S.M.; et al. Notice of Retraction and Replacement. Association of Clinical Specialty with Symptoms of Burnout and Career Choice Regret Among US Resident Physicians. JAMA 2019, 321, 1220–1221. Available online: https://jamanetwork.com/journals/jama/article-abstract/2728929 (accessed on 28 August 2025).
- Steele, I.H.; Thrower, N.; Noroian, P.; Saleh, F.M. Understanding suicide across the lifespan: A United States perspective of suicide risk factors, assessment & management. J. Forensic Sci. 2018, 63, 162–171. [Google Scholar]
- Miloyan, B.; Bienvenu, O.J.; Brilot, B.; Eaton, W.W. Adverse life events and the onset of anxiety disorders. Psychiatry Res. 2018, 259, 488–492. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Goebert, D. Depressive symptoms in medical students and residents, a multischool study. Acad. Med. 2009, 84, 236–241. [Google Scholar] [CrossRef]
- Available online: https://dl.acgme.org/learn/course/sponsoring-institution-idea-exchange/well-being/the-transition-to-residency-risk-index-trri?client=acgme-hub (accessed on 28 August 2025).
- Courand, J.; Dyurich, A. Transition to Residency Risk Index. Available online: https://www.uthscsa.edu/sites/default/files/2018/trri_format_2_transition_to_residency.pdf (accessed on 28 August 2025).
- Slavin, S.; Yaghmour, N.A.; Courand, J. Support for Mental Health and Well-Being in the Transition to Residency. J. Grad. Med. Educ. 2024, 16, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Slavin, S.; Courand, J. Navigating Transitions: Dr. Jon Courand on Resident Well-Being and the Transition to Residency Risk Index. ACGME Well-being Podcasts. Available online: https://dl.acgme.org/courses/navigating-transitions-dr-jon-courand-on-resident-well-being-and-the-transition-to-residency-risk-index (accessed on 28 August 2025).
- Courand, J.; Prasad, V.; Jones, W. Supporting Wellbeing and Mental Health during the Transition to Residency and Fellowship. In Proceedings of the 2024 ACGME Annual Educational Conference, Orlando, FL, USA, 7–9 March 2024. [Google Scholar]
- Guldner, G.; Siegel, J.T.; Broadbent, C.; Ayutyanont, N.; Streletz, D.; Popa, A.; Fuller, J.; Sisemore, T. Use of an opt-out vs opt-in strategy increases use of residency mental health services. J. Grad. Med. Educ. 2024, 16, 195–201. [Google Scholar] [CrossRef]
- Kevern, T.; Davies, D.R.; Stiel, K.; Raaum, S. Impact of opt-out therapy appointments on resident physicians’ mental health, well-being, stigma, and willingness to engage. J. Grad. Med. Educ. 2023, 15, 734–737. [Google Scholar] [CrossRef]
- Mortali, M.; Moutier, C. Facilitating Help-Seeking Behavior Among Medical Trainees and Physicians Unsing the Interactive Screening Program. J. Med. Regul. 2018, 104, 27–36. [Google Scholar]
- American Foundation for Suicide Prevention. 14 September 2023. Available online: https://afsp.org/story/encouraging-help-seeking-with-anonymous-mental-health-support (accessed on 7 November 2023).
- Substance Abuse and Mental Health Services Administration (SAMHSA). Creating a Healthier Life: Step by Step Guide to Wellness. April 2016. Available online: https://library.samhsa.gov/sites/default/files/sma16-4958.pdf (accessed on 28 August 2025).
- Warburton, K.; Goren, E.; Dine, J. Comprehensive Assessment of Struggling Learners Referred to a Graduate Medical Education Remediation Program. J. Grad. Med. Educ. 2017, 9, 763–767. [Google Scholar] [CrossRef] [PubMed]
- Guerrasio, J. Remediation of the Struggling Medical Learner; Association for Hospital Medical Education: Irwin, PA, USA, 2013. [Google Scholar]
- Sperry, L.; Sperry, J. Core Competencies in Counseling and Psychotherapy: Becoming a Highly Competent and Effective Therapist, 2nd ed.; Routledge: New York, NY, USA, 2023. [Google Scholar]
- Brashear, C.A.; Thomas, N. Core competencies for combatting crisis: Fusing ethics, cultural competence, and cognitive flexibility in counseling. Couns. Psychol. Q. 2022, 35, 215–229. [Google Scholar] [CrossRef]
- National Wellness Institute. NWI’s Six Dimensions of Wellness: What Is Wellness? Available online: https://nationalwellness.org/resources/six-dimensions-of-wellness/ (accessed on 11 November 2023).



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Academic Society for International Medical Education. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).