Abstract
Levosimendan, a calcium-sensitizing inodilator, has emerged as a promising adjunctive therapy in patients undergoing veno-arterial extracorporeal membrane oxygenation (V-A ECMO). Its pharmacodynamic profile, combining positive inotropy with vasodilation and mitochondrial protective effects, offers a unique therapeutic potential in the context of mechanical circulatory support. Despite growing interest, the clinical impact of Levosimendan in ECMO remains debated, with heterogeneous evidence regarding its efficacy in improving weaning success, reducing vasopressor requirements or mitigating ischemia-reperfusion injury. This narrative review aims to critically appraise the current literature on Levosimendan use in ECMO settings, exploring its mechanistic rationale, pharmacologic behavior under extracorporeal circulation and potential role in various clinical scenarios including post-cardiotomy shock and refractory cardiogenic failure. The limitations of existing studies are critically examined, underscoring the need for high-quality clinical trials to define appropriate patient selection, optimal timing of administration and dosing strategies. This review synthesizes current evidence to determine whether Levosimendan constitutes a true therapeutic asset or remains merely an adjunctive agent in the complex management of ECMO supported patients.
1. Introduction
Veno-arterial extracorporeal membrane oxygenation (V-A ECMO) has become an essential rescue therapy in patients with refractory cardiogenic shock or post-cardiotomy cardiac failure, providing temporary mechanical circulatory support and maintaining systemic perfusion while the underlying myocardial function recovers [1,2]. Despite remarkable technological progress, ECMO remains a bridge rather than a cure: the delicate balance between sufficient perfusion and excessive ventricular afterload, the risk of ischemia-reperfusion injury and the complexity of weaning continue to pose major clinical challenges [1,3,4,5]. Within this context, pharmacological strategies that optimize myocardial performance and protect cellular energetics are of growing interest. Among the available inotropic agents, Levosimendan stands apart for its unique pharmacodynamic profile. By sensitizing troponin C to calcium, it enhances myocardial contractility without increasing intracellular calcium concentration or oxygen consumption. Simultaneously, its opening of ATP-dependent potassium channels in vascular smooth muscle induces vasodilation, while mitochondrial K-ATP (mitoK-ATP) channel activation confers cytoprotective and anti-apoptotic effects [6,7,8]. This triad of inotropy, vasodilation and mitochondrial protection positions Levosimendan as a potentially valuable adjunct in the pharmacologic management of patients supported by V-A ECMO [9]. Beyond hemodynamic modulation, Levosimendan’s ability to improve microvascular flow, reduce oxidative stress and preserve mitochondrial bioenergetics aligns with emerging paradigms in pharmacologic organ protection during extracorporeal support. The interplay between its systemic and myocardial effects could theoretically enhance tissue oxygen delivery and facilitate myocardial recovery, thereby influencing the likelihood of successful ECMO weaning [9,10]. Nevertheless, the pharmacologic behavior of Levosimendan under extracorporeal circulation is complex. The circuit’s components may alter drug kinetics through adsorption and changes in distribution volume, while profound alterations in systemic hemodynamics, organ perfusion and inflammatory activation can modify both efficacy and tolerability [11]. Furthermore, the optimal timing, dosing regimen and patient selection criteria for its use remain uncertain, raising questions about whether Levosimendan represents a genuine paradigm shift in ECMO pharmacotherapy or merely an adjunctive measure in the multifaceted management if advanced cardiac failure.
This narrative review aims to critically examine the mechanistic rationale, pharmacodynamic considerations and potential clinical implications of Levosimendan administration in V-A ECMO-supported patients. A comprehensive search of literature was performed in PubMed and Scopus up to September 2025 using combinations of the following keywords: “Levosimendan”, “veno-arterial ECMO”, “mechanical circulatory support”, “cardiogenic shock”, “ECMO weaning”. Both clinical and experimental studies, as well as relevant reviews and pharmacologic analyses, were included without language restrictions. Emphasis was placed on peer-reviewed articles exploring the pharmacologic rationale, hemodynamic effects and clinical outcomes of Levosimendan in ECMO settings.
2. Relevant Sections
2.1. Pharmacologic Profile of Levosimendan
Levosimendan is a calcium-sensitizing inodilator that exerts its hemodynamic and cytoprotective effects through a triad of mechanisms involving myocardial calcium sensitization, smooth-muscle K-ATP channel activation and mitochondrial modulation [6,7,8]. Structurally, it belongs to pyridazinone-dinitrile class and acts as a prodrug rapidly converted to its active metabolites OR-1855 and OR-1896, the latter characterized by a prolonged half-life that sustains the drug’s pharmacodynamic activity for up to one week after a single infusion [12,13]. At the myocardial level, the Levesimendan binds selectively to cardiac troponin C in a calcium-dependent manner, stabilizing its conformation during systole. This interaction enhances the sensitivity of the contractile apparatus to existing cytosolic calcium without increasing intracellular calcium concentration or myocardial oxygen consumption, thereby augmenting contractility while avoiding the arrhythmogenic and energy-demanding effects typical of catecholaminergic inotropes. This unique mechanism translates into improved systolic performance with preserved diastolic relaxation and reduced risk of myocardial injury [14]. Concurrently, Levosimendan induces vasodilation by opening ATP-sensitive potassium channels (K-ATP) in vascular smooth-muscle cells, leading to hyperpolarization and decreased calcium influx. The result is a balanced reduction in preload and afterload, improved coronary and peripheral perfusion and alleviation of ventricular wall stress [15,16]. In the setting of V-A ECMO, such vasodilatory properties may help mitigate ECMO-related left ventricular distension and facilitate ventricular unloading [17]. Beyond hemodynamic modulation, Levosimendan exhibits a range of non-hemodynamic, cytoprotective effects that have garnered increasing attention. By activating mitochondrial ATP sensitive potassium (mitoK-ATP) channels, it stabilizes mitochondrial membrane potential, limits the opening of the mitochondrial permeability transition pore and attenuates calcium overload during ischemia-reperfusion. These effects translate into reduced oxidative stress, preservation of ATP synthesis and attenuation of apoptotic signaling pathways [10,18,19]. Furthermore, Levosimendan has been shown to modulate inflammatory cascades and endothelial function, potentially improving microvascular perfusion and organ resilience under systemic hypoperfusion [20,21], (Figure 1).
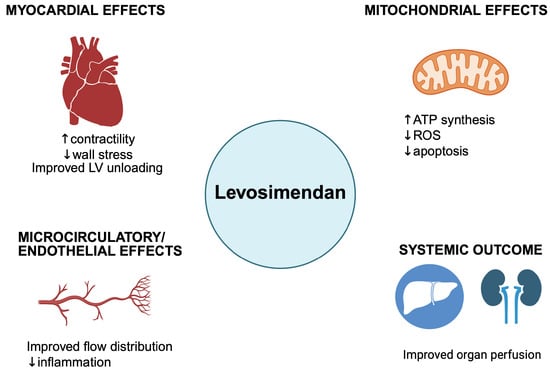
Figure 1.
The multidimensional mechanism of Levosimendan. LV: left ventricle; ROS: reactive oxygen species; ATP: adenosine triphosphate. Up arrow: Increase; down arrow: decrease. Created in BioRender. Pirri, C. (2025) https://BioRender.com/80gjhg6, accessed on 16 October 2025.
Pharmacokinetically, the parent compound displays a short elimination half-life of approximately one hour, but its long-acting metabolite OR-1896 extends hemodynamic effects over several days [21,22]. The drug is extensively protein-bound and metabolized primarily in the liver via conjugation and reduction pathways [13]. Because the intestinal microbiota contributes to the reduction in Levosimendan to OR-1855, and subsequently to OR-1896, conditions affecting splanchnic perfusion or gut microbial activity during ECMO could theoretically influence this metabolic pathway. Although this possibility has not been formally investigated, it represents a physiologically plausible consideration. During ECMO, pharmacokinetics may be substantially altered by circuit absorption, hemodilution and changes in plasma protein binding, which could affect both onset and duration of action [23]. These variables highlight the need for tailored dosing strategies when Levosimendan is administered under ECMO support.
2.2. Pathophysiological Rationale for Levosimendan in ECMO
The implementation of V-A ECMO profoundly alters cardiovascular physiology. While V-A ECMO provides immediate circulatory support and restores systemic oxygen delivery, it simultaneously imposes an abnormal hemodynamic state characterized by increased afterload on the left ventricle, retrograde aortic flow and potential impairment of pulmonary venous drainage. The resulting ventricular distension can aggravate myocardial ischemia, elevate wall stress and trigger secondary pulmonary edema [24,25]. These effects underscore the importance of preserving residual myocardial function and minimizing the deleterious consequences of mechanical circulatory support. Levosimendan may offer distinct advantages in this complex pathophysiological context (Figure 2). Its calcium-sensitizing mechanism enhances contractile efficiency without increasing intracellular calcium or myocardial oxygen demand, an especially valuable feature when oxygen delivery and metabolic reserves are already compromised. By promoting systolic performance while maintaining diastolic relaxation, Levosimendan supports ventricular ejection and may counteract the ECMO-induced rise in left ventricular (LV) afterload. The concurrent reduction in filling pressures and improved compliance further facilitate ventricular unloading, potentially reducing the need for mechanical decompression strategies such as venting or Impella assistance [9,17,26,27]. Moreover, the Levosimendan’s vasodilatory properties extend beyond the systemic circulation. By activating ATP-sensitive potassium channels within the coronary and pulmonary vasculature, it enhances coronary flow and reduces right ventricular afterload, improving biventricular coupling and optimizing overall cardiac performance [28,29,30,31]. This balanced inodilator effect may contribute to smoother transitions during V-A ECMO weaning, when abrupt hemodynamics shifts often expose subclinical ventricular dysfunction. At the cellular level, Levosimendan exerts mitochondrial protective actions that may mitigate ischemia-reperfusion injury, a common challenge both at the initiation and discontinuation of ECMO [18,32]. MitoK-ATP channel activation helps preserve membrane potential, stabilize ATP generation and prevent calcium overload, thereby limiting apoptosis and oxidative stress [32,33]. These effects align with emerging evidence that myocardial recovery during mechanical support is strongly limited to mitochondrial integrity and metabolic resilience. Additionally, Levosimendan’s capacity to modulate endothelial tone and microvascular perfusion could enhance global tissue oxygenation and organ recovery in the systemic inflammatory milieu typical of ECMO patients. By improving the coherence between macro and micro-circulation, it may help counteract the maldistribution of flow and oxygen extraction abnormalities that frequently complicate prolonged extracorporeal support [34,35,36,37].
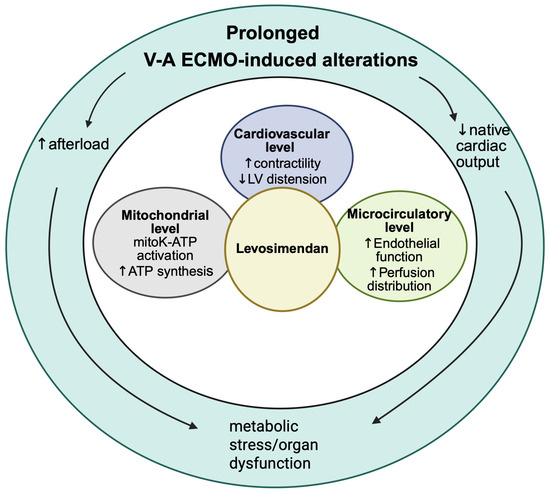
Figure 2.
Integrative model of Levosimendan effects counteracting prolonged V-A ECMO induced pathophysiological alterations. LV: left ventricle; ROS: reactive oxygen species; ATP: adenosine triphosphate; mitoK-ATP: mitochondrial ATP-sensitive potassium channel. Up arrow: Increase; down arrow: decrease. Created in BioRender. Pirri, C. (2025) https://BioRender.com/mcnst7b, accessed on 16 October 2025.
2.3. Clinical Evidence in ECMO Patients
Clinical experience with Levosimendan in patients supported by V-A ECMO has evolved from exploratory case observations to more structured analyses, though the overall level of evidence remains modest [36], (Table 1). Most available data originate from small single center studies, retrospective cohorts and limited prospective investigations, reflecting the inherent difficulty of performing randomized trials in this critically ill population. Nevertheless, these reports provide meaningful insights into the hemodynamic and physiological consequences of Levosimendan use under extracorporeal circulation. Across various settings, Levosimendan administration has been associated with improvements in cardiac index (CI), left ventricular ejection fraction (LVEF), aortic velocity time integral (VTI) and systemic perfusion surrogates, as well as a reduction in catecholamine requirements. When given during or shortly before ECMO weaning, it appears to promote myocardial recovery and facilitate decannulation in selected patients [17,38,39,40,41,42,43,44,45,46]. These effects are mechanistically consistent with its calcium-sensitizing and vasodilatory profile, which enhances contractile efficiency, reduces ventricular loading conditions and improves coronary flow [47]. In post-cardiotomy shock, Levosimendan has been explored as a pharmacologic bridge to myocardial recovery, whereas in refractory cardiogenic shock it has been considered as an adjunct to optimize ventricular performance before transitioning to autonomous circulation or long-term mechanical support [48,49]. Similarly, in patients undergoing V-A ECMO following cardiac arrest (extracorporeal cardiopulmonary resuscitation, eCPR), Levosimendan has been investigated as a means to attenuate post-resuscitation myocardial stunning and improve systemic microcirculatory recovery. In retrospective series, Levosimendan administration early post-return of spontaneous circulation (ROSC) phases has been associated with improved ventricular performance and higher rates of V-A ECMO weaning, although no randomized evidence is yet available [41]. Despite these encouraging hemodynamic observations, the impact of Levosimendan on hard clinical outcomes, such as survival, duration of ECMO support and incidence of multiorgan failure, remains uncertain [43,50,51,52]. Considerable heterogeneity in patient selection, ECMO configurations and concomitant therapies complicates the interpretation of available data. Potential confounders, including the use of mechanical ventricular unloading devices, variations in weaning protocols and differences in timing and dosing regimens, further limit comparability between studies. Consequently, most published evidence should be regarded as hypothesis-generating rather than confirmatory. To date, no large, adequately powered randomized controlled trial has conclusively demonstrated that Levosimendan improves major clinical outcomes in ECMO supported patients. A few early randomized pilot trials in post-cardiotomy populations suggested transient improvements in ventricular function and reduced vasopressor requirements, yet these findings did not translate into significant gains in successful decannulation or survival [52]. Two major multicenter trials currently aim to clarify the clinical value of Levosimendan in this context. The LEVOSIMENDAN to Facilitate Weaning From ECMO trial (NCT04728932) is designed to test whether pre-weaning infusion of Levosimendan increases the rate of successful decannulation compared with placebo, while the WEANILEVO study (NCT 04148674) investigates its impact on myocardial recovery and early survival after ECMO discontinuation. These studies are expected to address critical gaps in knowledge concerning optimal timing, dosing strategies and patient selection. Beyond the V-A ECMO field, several landmark randomized controlled trials have explored Levosimendan in broader populations of critically ill patients, providing context for its variable clinical efficacy. The CHEETAH trial (NCT00994825) evaluated perioperative Levosimendan in cardiac surgery but failed to demonstrate a reduction in mortality or post-operative low-output syndrome [53]. Similarly, the LEVO-CTS study (NCT02025621) in patients undergoing cardiac surgery with LV dysfunction did not confirm a survival advantage, although secondary analyses suggested improved outcomes in high-risk subgroup [54]. Furhermore, the LeoPARDS trial (ISRCTN12776039), conducted in septic shock patients, reported no improvement in organ failure scores or mortality and highlighted potential concerns regarding hypotension in this population [55]. Collectively, these trials indicate that while Levosimendan exerts clear hemodynamic effects, its impact on major clinical endpoints may depend strongly on patient selection, timing of intervention and the underlying pathophysiological substrate, factors that are particularly complex also in the ECMO environment. A recent comprehensive meta-analysis by Zhao et al. [42] has substantially strengthened the evidence base for Levosimendan in ECMO patients. Pooling data from 16 studies encompassing over 2000 individuals, the authors reported a significantly higher likelihood of successful weaning and a reduction in both 30-day and in-hospital mortality. Interestingly, these benefits were accompanied by longer ECMO and ICU durations, possibly reflecting a more controlled and progressive recovery trajectory among treated patients. Although the analysis was limited by its reliance on observational studies and inter-study heterogeneity, it consolidates previous evidence suggesting that Levosimendan may enhance myocardial recovery and short-term outcomes during ECMO support. Until the results of the ongoing ECMO, specific trials become available, Levosimendan should be regarded as a promising yet adjunctive option in extracorporeal pharmacotherapy. Its physiological rationale is strong and its safety profile acceptable, but robust evidence confirming a consistent survival benefit remains elusive. Further well-controlled investigations are required to determine whether Levosimendan can evolve from a supportive agent into a true therapeutic cornerstone in the management of patients receiving mechanical circulatory support.

Table 1.
Summary of clinical evidence on Levosimendan use in V-A ECMO. V-A ECMO: veno-arterial extracorporeal membrane oxygenation; eCPR: extracorporeal cardiopulmonary bypass; ICU: intensive care unit; RCT: randomized controlled trial; LVEF: left ventricular ejection fraction; VTI: velocity time integral.
2.4. Pharmacological and Technical Challenges Under ECMO
The pharmacologic management of patients supported by V-A ECMO poses unique challenges, as the extracorporeal circuit alters drug disposition, interaction and pharmacodynamics [57]. Levosimendan, with its distinctive physiochemical characteristics, high lipophilicity, extensive protein binding (≈97–98%) and formation of long-acting active metabolities, OR-1855 and OR-1896, behaves differently under ECMO compared to conventional critical care settings [23]. A fundamental issue arises from drug sequestration within the ECMO circuit. The synthetic material composing the oxygenator membrane, tubing and connectors can adsorb lipophilic or highly protein-bound molecules, thereby reducing the free circulating fraction and delaying the attainment of therapeutic steady-state concentrations. Levosimendan can adhere to polymethylpentene and polyvinylchloride surfaces, particularly during the first hour of extracorporeal circulation, leading to early underexposure and variable pharmacokinetics. In practice, this may translate into a delayed onset of inodilatory effect following infusion initiation, especially if a loading dose is omitted, a frequent choice in ECMO to avoid hypotension. Another critical aspect is the alteration of drug distribution volume and clearance. ECMO patients often present with systemic inflammation, capillary leak, hypoalbuminemia and hemodilution, all of which contribute to unpredictable pharmacokinetic profiles [5,11,23,58]. The combination of circuit adsorption and altered protein binding can transiently reduce the free active fraction of Levosimendan, whereas accumulation of its long-acting metabolite, OR-1896, may sustain pharmacologic effects long after discontinuation of the infusion. This biphasic dynamic complicates dose titration and makes the assessment of hemodynamic response less immediate than in non-ECMO settings [21,59]. Moreover, the complex interplay between V-A ECMO flow, native cardiac output and vascular tone adds additional layer of variability. Levosimendan exerts systemic vasodilatory effect through K-ATP channel activation, which may lead to reduced afterload and improved ventricular-arterial coupling but can also precipitate hypotension if ECMO flow is not adequately maintained [8,21,60]. Balancing perfusion pressure, oxygen delivery and coronary perfusion becomes particularly challenging in this context, where systemic vascular resistance and circuit flow are mechanically interdependent. From a technical standpoint, monitoring the pharmacodynamic response to Levosimendan in ECMO is also nontrivial. Continuous hemodynamic monitoring, using echocardiography, pulmonary artery catheterization or advanced non-invasive indices such as ventricular elastance and arterial coupling, is therefore essential to interpret drug efficacy and avoid overestimation of its true contractile effect [60,61,62,63].
2.5. Timing and Dosing Strategies
The optimal timing and dosing of Levosimendan administration during V-A ECMO remain subjects of ongoing debate. Current practice varies widely across centers, reflecting both the heterogeneity of clinical indications and the lack of standardized protocols derived from randomized trials. Nevertheless, several physiologic principles and consistent observational findings have begun to outline a rationale framework for its use.
2.5.1. Timing of Administration
Two principal strategies have been described in clinical practice: pre-emptive and pre-weaning administration.
- Pre-emptive (early) administration involves initiating Levosimendan infusion shortly after ECMO cannulation in patients with cardiogenic shock or post-cardiotomy failure, with the aim of promoting myocardial protection and reducing catecholamine dependence during the early stabilization phase. This approach is supported by observational data suggesting improved ventricular recovery and lower mortality when Levosimendan is introduced within the first 24 h of ECMO initiation [39,40].
- Pre-weaning administration, the most commonly adopted approach, consists of initiating Levosimendan 12–24 h before planned ECMO discontinuation. The rational lies in enhancing residual ventricular contractility and facilitating liberation from mechanical support by leveraging both the parent compound’s inotropic action and the prolonged activity of its metabolite OR-1896. Several studies, indicate that pre-weaning infusion correlates with higher rates of successful decannulation and reduced short-term mortality [17,56].
The absence of randomized comparisons precludes definitive recommendations.
2.5.2. Dosing Consideration
Levosimendan dosing during ECMO typically omits the loading bolus to avoid abrupt vasodilation and hypotension. Continuous infusions are generally maintained between 0.1 and 0.2 µcg/kg/min for 24 h, sometimes extended up to 48 h in refractory cases [9,64]. Given the circuit-related sequestration and delayed equilibration, therapeutic onset may be slower than in non-ECMO patients, emphasizing the importance of early initiation when myocardial recovery is anticipated. Pharmacokinetic modeling suggests that despite initial adsorption to the ECMO circuit, steady-state concentrations are achieved after several hours and the long-acting metabolite ensures persistent hemodynamic support up to 7–9 days post-infusion [56,58]. This prolonged effect allows clinicians to harness the benefit of Levosimendan during the critical period of ECMO weaning without continuous drug administration, reducing the risk of cumulative vasodilation and tachyarrhythmia. Individualized titration remains crucial. Dosing adjustments should account for baseline cardiac function, mean arterial pressure, ECMO flow and concurrent vasoactive support. In patients with marginal perfusion pressure, gradual up-titration (starting from 0.05 µcg/kg/min) and vigilant hemodynamic monitoring are recommended to avoid excessive afterload reduction. Conversely, in cases of preserved systemic pressure and high afterload, early full dose infusion may enhance contractile efficiency and expedite myocardial recovery [65].
2.5.3. Safety Profile and Hemodynamic Consideration
Although generally well tolerated, Levosimendan use during V-A ECMO requires careful hemodynamic monitoring due to its potent vasodilatory and inotropic effects, which may interact unpredictably with extracorporeal flow dynamics and concomitant vasoactive therapy. The balance between enhanced contractility and reduced systemic vascular resistance is delicate, particularly in patients with unstable perfusion pressure or right ventricular dysfunction. The principal safety concern is hypotension, resulting from peripheral vasodilation via K-ATP channel activation in vascular smooth muscle. This effect, while beneficial in improving ventricular-arterial coupling and afterload reduction, can transiently decrease mean arterial pressure and compromise systemic or coronary perfusion if ECMO flow is insufficiently adjusted [66]. In this context, omitting the loading bolus and using a gradual continuous infusion (0.05–0.2 µcg/kg/min) are standard preventive strategies [66]. When hypotension occurs, temporary escalation of V-A ECMO blood flow or cautious vasopressor supplementation (typically norepinephrine) is preferred over premature discontinuation of Levosimendan. Arrhythmogenic potential represents another theoretical concern. However, clinical data indicate that Levosimendan does not significantly increase the incidence of supraventricular or ventricular arrhythmias compared to conventional inotropes. Its calcium-sensitizing mechanism enhances myofilament responsiveness without increasing intracellular calcium concentration, thereby minimizing proarrhythmic risk, a clear pharmacologic advantage over catecholamines or phosphodiesterase inhibitors [67]. From a systemic perspective, Levosimendan may improve microcirculatory perfusion and end-organ oxygenation, mitigating ischemia-reperfusion injury during myocardial recovery [68]. Evidence suggests favorable effects on renal and hepatic function, mediated by mitoK-ATP channel activation and enhanced tissue oxygen utilization [69,70,71]. These properties are particularly valuable in prolonged ECMO runs, where microcirculatory dysfunction and organ congestion often contribute to morbidity and delayed recovery. Nonetheless, certain patient subgroups warrant caution [72,73]. In individuals with profound vasoplegia, severe right ventricular failure or concomitant septic shock physiology, the vasodilatory response may predominate over the inotropic benefit, necessitating higher ECMO flows or combined vasopressor therapy to maintain adequate perfusion. Drug-drug interactions under ECMO are relatively limited but clinically relevant. The concurrent use of high-dose catecholamines can mask the true inotropic contribution of Levosimendan, while aggressive vasopressor escalation may counteract its afterload-reducing benefit [36,74]. Conversely, its combination with mechanical unloading devices, such as the intra-aortic balloon pump (IABP) or Impella, could show synergistic hemodynamic effects, improving both forward flow and myocardial energetics [75]. Overall, the safety profile of Levosimendan is favorable, provided that administration is guided by vigilant monitoring and hemodynamic tailoring. Adverse events are usually transient and manageable within the framework of advanced circulatory support. When properly titrated, Levosimendan appears to offer a unique combination of inotropy, vasodilation and cytoprotection, rendering it a valuable pharmacologic adjunct in the complex hemodynamic landscape of V-A ECMO supported patients [66,76,77].
3. Discussion
The role of Levosimendan in patients supported by V-A ECMO continues to stimulate debate at the intersection of pharmacology and mechanical circulatory support. Over the past decade, the perception of this agent gradually shifted from experimental curiosity to a pharmacologic tool with plausible physiologic and clinical value. This change mirrors the broader transformation in ECMO management, from an emergency salvage therapy to a dynamic platform for myocardial recovery and organ preservation. In this evolving context, Levosimendan represents a candidate drug capable of bridging the mechanical and biological dimensions of cardiac support. The consistency of recent meta-analyses, suggest that Levosimendan may improve the probability of successful ECMO weaning and reduce short-term mortality, particularly when administered early or before planned discontinuation of support [38,39,40,41,42,43,44,45,46]. Although causality remains uncertain, the convergence of evidence across heterogeneous patient populations and study design is notable. Beyond its hemodynamic benefits, Levosimendan may facilitate a smoother transition from mechanical to intrinsic circulation by optimizing ventricular-arterial coupling, improving myocardial energetics and enhancing microvascular coherence. This integrated effect, rather than any single pharmacologic action, could explain the more controlled recovery patterns and prolonged ECMO duration observed in treated patients. Nevertheless, several limitations persist. Most studies to date are observational and prone to selection bias, patients receiving Levosimendan are often those judged by clinicians to have recoverable myocardial function, introducing an inherent survival advantage [37,39,41,56]. Differences in ECMO configuration, timing of infusion and the use of unloading devices further obscure interpretation. The drug’s pharmacokinetic variability under extracorporeal circulation adds another layer of complexity, as circuit adsorption and altered protein binding may delay or attenuate its early effects [11,23,59]. These factors underscore the need for standardized administration protocols and for pharmacokinetic-pharmacodynamic modeling specific to ECMO physiology. Importantly, the potential value of Levosimendan may extend beyond contractile enhancement. Its activation of mitoK-ATP channels and modulation of endothelial function point toward a systemic protective effect that could mitigate the organ dysfunction frequently seen during prolonged ECMO runs [18,19,78]. Improved renal and hepatic perfusion, better oxygenation extraction and attenuated inflammatory activation have been all reported, suggesting that the drug acts as a modulator of cellular resilience rather than as mere inotrope [79,80,81,82]. Such properties align with the emerging concept of metabolic support therapy, wherein pharmacologic agents are used to stabilize mitochondrial function and tissue perfusion during mechanical assistance. The challenge ahead lies in translating these physiologic and observational findings into evidence-based practice. The ongoing WEANILEVO (NCT 04148674) and LEVOECMO (NCT04728932) randomized controlled trials will be crucial in defining whether the observed improvements in weaning success and early survival are reproducible under standardized conditions. Should these results confirm a tangible benefit, Levosimendan could evolve from a promising adjunct to central component of ECMO pharmacotherapy. Conversely, if neutral, its role may remain confined to specific clinical niches, such as post-cardiotomy shock or early myocardial stunning. In a broader sense, the discussion surrounding Levosimendan reflects a paradigm shift in the physiology of ECMO management itself. The focus is no longer limited to restoring macrocirculation, but rather to integrating metabolic, microvascular and mitochondrial preservation into patient care. Within this framework, Levosimendan exemplifies a new generation of pharmacologic interventions, designed not merely to sustain life mechanically, but to facilitate genuine physiologic recovery.
4. Conclusions
Building on the current physiologic and observational landscape, Levosimendan has emerged as a pharmacologically coherent adjunct for patients supported by V-A ECMO. Through calcium sensitization, K-ATP channel activation and mitochondrial protection, it offers a unique bridge between mechanical circulatory support and biological recovery. Available evidence, though predominantly observational, suggests improved ventricular performance, a higher likelihood of successful weaning and potential reductions in short-term mortality, particularly when administered early or before planned decannulation. Beyond its hemodynamic effects, Levosimendan may enhance microvascular coherence, metabolic resilience and end-organ protection, features that align with the evolving concept of ECMO as a platform for myocardial and systemic recovery rather than mere circulatory substitution. Nevertheless, heterogeneity in study design, dosing strategies and patient selection, along with the pharmacokinetic complexity introduced by extracorporeal circuits, limits firm conclusion. The ongoing WEANILEVO and LEVOECMO trials are expected to define whether these promising mechanistic and clinical signals translate into reproducible benefits. Until high-quality evidence becomes available, Levosimendan should be regarded as a promising yet adjunctive component within a multimodal ECMO strategy, one that prioritizes myocardial recovery, optimized perfusion and protection of vulnerable organ systems.
Author Contributions
Conceptualization, D.E.T.; methodology, C.P.; software, C.P.; validation, D.E.T. and C.P.; formal analysis, C.P.; investigation, D.E.T.; resources, C.P.; data curation, D.E.T.; writing—original draft preparation, D.E.T.; writing—review and editing, D.E.T.; visualization, C.P.; supervision, C.P.; project administration, D.E.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ECMO | Extracorporeal membrane oxygenation |
| V-A ECMO | Veno-arterial extracorporeal membrane oxygenation |
| LVEF | Left ventricular ejection fraction |
| IABP | Intra-aortic balloon pump |
References
- Koziol, K.J.; Isath, A.; Rao, S.; Gregory, V.; Ohira, S.; Van Diepen, S.; Lorusso, R.; Krittanawong, C. Extracorporeal Membrane Oxygenation (VA-ECMO) in Management of Cardiogenic Shock. J. Clin. Med. 2023, 12, 5576. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guglin, M.; Zucker, M.J.; Bazan, V.M.; Bozkurt, B.; El Banayosy, A.; Estep, J.D.; Gurley, J.; Nelson, K.; Malyala, R.; Panjrath, G.S.; et al. Venoarterial ECMO for Adults: JACC Scientific Expert Panel. J. Am. Coll. Cardiol. 2019, 73, 698–716. [Google Scholar] [CrossRef] [PubMed]
- Tsangaris, A.; Alexy, T.; Kalra, R.; Kosmopoulos, M.; Elliott, A.; Bartos, J.A.; Yannopoulos, D. Overview of Veno-Arterial Extracorporeal Membrane Oxygenation (VA-ECMO) Support for the Management of Cardiogenic Shock. Front. Cardiovasc. Med. 2021, 8, 686558. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Heymer, J.; Hein, A.; Ott, M.; Schilling, T.; Räpple, D. Weaning assessment of veno-arteriovenous (V-AV) extracorporeal membrane oxygenation (ECMO). Intensive Care Med. Exp. 2023, 11, 47. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hatami, S.; Hefler, J.; Freed, D.H. Inflammation and Oxidative Stress in the Context of Extracorporeal Cardiac and Pulmonary Support. Front. Immunol. 2022, 13, 831930. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pollesello, P.; Papp, Z.; Papp, J.G. Calcium sensitizers: What have we learned over the last 25 years? Int. J. Cardiol. 2016, 203, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Milligan, D.J.; Fields, A.M. Levosimendan: Calcium sensitizer and inodilator. Anesthesiol. Clin. 2010, 28, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Burkhoff, D.; Rich, S.; Pollesello, P.; Papp, Z. Levosimendan-induced venodilation is mediated by opening of potassium channels. ESC Heart Fail. 2021, 8, 4454–4464. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ellouze, O.; Soudry Faure, A.; Radhouani, M.; Abou-Arab, O.; Besnier, E.; Moussa, M.; Cransac, A.; Ksiazek, E.; Fischer, M.O.; Mertes, P.M.; et al. Levosimendan in venoarterial ECMO weaning. Rational and design of a randomized double blind multicentre trial. ESC Heart Fail. 2021, 8, 3339–3347. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grossini, E.; Farruggio, S.; Pierelli, D.; Bolzani, V.; Rossi, L.; Pollesello, P.; Monaco, C. Levosimendan Improves Oxidative Balance in Cardiogenic Shock/Low Cardiac Output Patients. J. Clin. Med. 2020, 9, 373. [Google Scholar] [CrossRef]
- Cheng, V.; Abdul-Aziz, M.H.; Roberts, J.A.; Shekar, K. Optimising drug dosing in patients receiving extracorporeal membrane oxygenation. J. Thorac. Dis. 2018, 10 (Suppl. 5), S629–S641. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Erdei, N.; Papp, Z.; Pollesello, P.; Edes, I.; Bagi, Z. The levosimendan metabolite OR-1896 elicits vasodilation by activating the K(ATP) and BK(Ca) channels in rat isolated arterioles. Br. J. Pharmacol. 2006, 148, 696–702. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kipka, H.; Schaflinger, R.; Tomasi, R.; Pogoda, K.; Mannell, H. The Effects of the Levosimendan Metabolites OR-1855 and OR-1896 on Endothelial Pro-Inflammatory Responses. Biomedicines 2023, 11, 918. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Haikala, H.; Nissinen, E.; Etemadzadeh, E.; Levijoki, J.; Lindén, I.B. Troponin C-mediated calcium sensitization induced by levosimendan does not impair relaxation. J. Cardiovasc. Pharmacol. 1995, 25, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Lehtonen, L. Levosimendan: A calcium-sensitizing agent for the treatment of patients with decompensated heart failure. Curr. Heart Fail. Rep. 2004, 1, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Gödény, I.; Pollesello, P.; Edes, I.; Papp, Z.; Bagi, Z. Levosimendan and its metabolite OR-1896 elicit KATP channel-dependent dilation in resistance arteries In Vivo. Pharmacol. Rep. 2013, 65, 1304–1310. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kaddoura, R.; Omar, A.S.; Ibrahim, M.I.M.; Alkhulaifi, A.; Lorusso, R.; Elsherbini, H.; Soliman, O.; Caliskan, K. The Effectiveness of Levosimendan on Veno-Arterial Extracorporeal Membrane Oxygenation Management and Outcome: A Systematic Review and Meta-Analysis. J. Cardiothorac. Vasc. Anesth. 2021, 35, 2483–2495. [Google Scholar] [CrossRef] [PubMed]
- Pollesello, P.; Papp, Z. The cardioprotective effects of levosimendan: Preclinical and clinical evidence. J. Cardiovasc. Pharmacol. 2007, 50, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Das, B.; Sarkar, C. Pharmacological preconditioning by levosimendan is mediated by inducible nitric oxide synthase and mitochondrial KATP channel activation in the in vivo anesthetized rabbit heart model. Vascul. Pharmacol. 2007, 47, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Adam, M.; Meyer, S.; Knors, H.; Klinke, A.; Radunski, U.K.; Rudolph, T.K.; Rudolph, V.; Spin, J.M.; Tsao, P.S.; Costard-Jäckle, A.; et al. Levosimendan displays anti-inflammatory effects and decreases MPO bioavailability in patients with severe heart failure. Sci. Rep. 2015, 5, 9704. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Antila, S.; Sundberg, S.; Lehtonen, L.A. Clinical pharmacology of levosimendan. Clin. Pharmacokinet. 2007, 46, 535–552. [Google Scholar] [CrossRef] [PubMed]
- Cholley, B.; Levy, B.; Fellahi, J.L.; Longrois, D.; Amour, J.; Ouattara, A.; Mebazaa, A. Levosimendan in the light of the results of the recent randomized controlled trials: An expert opinion paper. Crit. Care 2019, 23, 385. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bourgoin, P.; Lecomte, J.; Oualha, M.; Berthomieu, L.; Pereira, T.; Davril, E.; Lamoureux, F.; Joram, N.; Chenouard, A.; Duflot, T. Population Pharmacokinetics of Levosimendan and its Metabolites in Critically Ill Neonates and Children Supported or Not by Extracorporeal Membrane Oxygenation. Clin. Pharmacokinet. 2023, 62, 335–348, Erratum in Clin. Pharmacokinet. 2023, 62, 349. https://doi.org/10.1007/s40262-023-01218-6. [Google Scholar] [CrossRef] [PubMed]
- Ezad, S.M.; Ryan, M.; Donker, D.W.; Pappalardo, F.; Barrett, N.; Camporota, L.; Price, S.; Kapur, N.K.; Perera, D. Unloading the Left Ventricle in Venoarterial ECMO: In Whom, When, and How? Circulation 2023, 147, 1237–1250. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Otake, M.; Morita, H.; Sato, K.; Saku, K. Impact of Venoarterial Extracorporeal Membrane Oxygenation on Hemodynamics and Cardiac Mechanics: Insights From Pressure-Volume Loop Analysis. Int. J. Heart Fail. 2025, 7, 125–138. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Todaka, K.; Wang, J.; Yi, G.H.; Stennett, R.; Knecht, M.; Packer, M.; Burkhoff, D. Effects of levosimendan on myocardial contractility and oxygen consumption. J. Pharmacol. Exp. Ther. 1996, 279, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Michaels, A.D.; McKeown, B.; Kostal, M.; Vakharia, K.T.; Jordan, M.V.; Gerber, I.L.; Foster, E.; Chatterjee, K. Effects of intravenous levosimendan on human coronary vasomotor regulation, left ventricular wall stress, and myocardial oxygen uptake. Circulation 2005, 111, 1504–1509. [Google Scholar] [CrossRef] [PubMed]
- Ikonomidis, I.; Parissis, J.T.; Paraskevaidis, I.; Kourea, K.; Bistola, V.; Lekakis, J.; Filippatos, G.; Kremastinos, D.T. Effects of levosimendan on coronary artery flow and cardiac performance in patients with advanced heart failure. Eur. J. Heart Fail. 2007, 9, 1172–1177. [Google Scholar] [CrossRef] [PubMed]
- Papp, Z.; Édes, I.; Fruhwald, S.; De Hert, S.G.; Salmenperä, M.; Leppikangas, H.; Mebazaa, A.; Landoni, G.; Grossini, E.; Caimmi, P.; et al. Levosimendan: Molecular mechanisms and clinical implications: Consensus of experts on the mechanisms of action of levosimendan. Int. J. Cardiol. 2012, 159, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Rieg, A.D.; Rossaint, R.; Verjans, E.; Maihöfer, N.A.; Uhlig, S.; Martin, C. Levosimendan Relaxes Pulmonary Arteries and Veins in Precision-Cut Lung Slices—The Role of KATP-Channels, cAMP and cGMP. PLoS ONE 2013, 8, e66195. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hu, Y.; Wei, Z.; Zhang, C.; Lu, C.; Zeng, Z. The effect of levosimendan on right ventricular function in patients with heart dysfunction: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 24097. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shi, F.; Bao, H.; Meng, F.; Pang, Y. Levosimendan alleviates myocardial ischemia-reperfusion injury by regulating mitochondrial autophagy through cGAS-STING signaling pathway. J. Clin. Biochem. Nutr. 2025, 77, 74–78. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Aminzadeh, A.; Mehrzadi, S. Cardioprotective effect of levosimendan against homocysteine-induced mitochondrial stress and apoptotic cell death in H9C2. Biochem. Biophys. Res. Commun. 2018, 507, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Volleman, C.; Dubelaar, D.P.C.; Vlaar, A.P.J.; van den Brom, C.E. Exploring the Impact of Extracorporeal Membrane Oxygenation on the Endothelium: A Systematic Review. Int. J. Mol. Sci. 2024, 25, 10680. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yao, Y.; Kang, H.; Cheng, Y.; Su, X.; Wang, B. Inflammatory Progression in Patients Undergoing Extracorporeal Membrane Oxygenation. Curr. Mol. Med. 2024, 24, 844–855. [Google Scholar] [CrossRef] [PubMed]
- Girardis, M.; Bettex, D.; Bojan, M.; Demponeras, C.; Fruhwald, S.; Gál, J.; Groesdonk, H.V.; Guarracino, F.; Guerrero-Orriach, J.L.; Heringlake, M.; et al. Levosimendan in intensive care and emergency medicine: Literature update and expert recommendations for optimal efficacy and safety. J. Anesth. Analg. Crit. Care 2022, 2, 4. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sangalli, F.; Avalli, L.; Laratta, M.; Formica, F.; Maggioni, E.; Caruso, R.; Cristina Costa, M.; Guazzi, M.; Fumagalli, R. Effects of Levosimendan on Endothelial Function and Hemodynamics During Weaning From Veno-Arterial Extracorporeal Life Support. J. Cardiothorac. Vasc. Anesth. 2016, 30, 1449–1453. [Google Scholar] [CrossRef] [PubMed]
- Vally, S.; Ferdynus, C.; Persichini, R.; Bouchet, B.; Braunberger, E.; Lo Pinto, H.; Martinet, O.; Vandroux, D.; Aujoulat, T.; Allyn, J.; et al. Impact of levosimendan on weaning from peripheral venoarterial extracorporeal membrane oxygenation in intensive care unit. Ann. Intensive Care 2019, 9, 24. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen, Y.W.; Lee, W.C.; Wu, P.J.; Fang, H.Y.; Fang, Y.N.; Chen, H.C.; Tong, M.S.; Sung, P.H.; Lee, C.H.; Chung, W.J. Early Levosimendan Administration Improved Weaning Success Rate in Extracorporeal Membrane Oxygenation in Patients With Cardiogenic Shock. Front. Cardiovasc. Med. 2022, 9, 912321. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Distelmaier, K.; Roth, C.; Schrutka, L.; Binder, C.; Steinlechner, B.; Heinz, G.; Lang, I.M.; Maurer, G.; Koinig, H.; Niessner, A.; et al. Beneficial effects of levosimendan on survival in patients undergoing extracorporeal membrane oxygenation after cardiovascular surgery. Br. J. Anaesth. 2016, 117, 52–58. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gaisendrees, C.; Schlachtenberger, G.; Gerfer, S.; Krasivskyi, I.; Djordjevic, I.; Sabashnikov, A.; Kosmopoulos, M.; Jaeger, D.; Luehr, M.; Kuhn, E.; et al. The impact of levosimendan on survival and weaning from ECMO after extracorporeal cardiopulmonary resuscitation. Artif. Organs. 2023, 47, 1351–1360. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.M.; Zhao, G.M.; Zhang, H.; Chen, W.; Zhou, J.X.; Li, H.L. Clinical outcomes of levosimendan administration in veno-arterial extracorporeal membrane oxygenation: A meta-analysis. BMJ Open. 2025, 15, e101995. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guilherme, E.; Jacquet-Lagrèze, M.; Pozzi, M.; Achana, F.; Armoiry, X.; Fellahi, J.L. Can levosimendan reduce ECMO weaning failure in cardiogenic shock?: A cohort study with propensity score analysis. Crit Care 2020, 24, 442, Erratum in Crit Care 2020, 24, 487. https://doi.org/10.1186/s13054-020-03213-w. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Burgos, L.M.; Seoane, L.; Furmento, J.F.; Costabel, J.P.; Diez, M.; Vrancic, M.; Aissaoui, N.; Benzadón, M.N.; Navia, D. Effects of levosimendan on weaning and survival in adult cardiogenic shock patients with veno-arterial extracorporeal membrane oxygenation: Systematic review and meta-analysis. Perfusion 2020, 35, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Zhao, T.; Guo, B.; Li, Y. Short-term effects of levosimendan use for venoarterial extracorporeal membrane oxygenation: A systematic review and meta-analysis. Perfusion 2023, 38, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, L.; Yao, Y.; Li, Y.; Qin, W.; Li, Y.; Xue, W.; Li, P.; Chen, Y.; Chen, X.; et al. Effects of levosimendan on the outcome of veno-arterial extracorporeal membrane oxygenation: A systematic review and meta-analysis. Clin. Res. Cardiol. 2024, 113, 509–521. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.M. Levosimendan, a new calcium-sensitizing inotrope for heart failure. Pharmacotherapy 2004, 24, 1366–1384. [Google Scholar] [CrossRef] [PubMed]
- Friedrichson, B.; Jasny, T.; Nordine, M.; Old, O.; Zacharowski, K.; Kloka, J. 171: Protective effects of Levosimendan in postcardiotomy V-A ECMO patients. Results of 6,456 ECMO runs. ASAIO J. 2023, 69 (Suppl. 3), 17. [Google Scholar] [CrossRef]
- Braun, J.P.; Jasulaitis, D.; Moshirzadeh, M.; Doepfmer, U.R.; Kastrup, M.; von Heymann, C.; Dohmen, P.M.; Konertz, W.; Spies, C. Levosimendan may improve survival in patients requiring mechanical assist devices for post-cardiotomy heart failure. Crit. Care 2006, 10, R17. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Massol, J.; Simon-Tillaux, N.; Tohme, J.; Hariri, G.; Dureau, P.; Duceau, B.; Belin, L.; Hajage, D.; De Rycke, Y.; Charfeddine, A.; et al. Levosimendan in patients undergoing extracorporeal membrane oxygenation after cardiac surgery: An emulated target trial using observational data. Crit. Care 2023, 27, 51. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hau, M.; Fong, K.M.; Au, S.Y. Levosimendan’s effect on venoarterial extracorporeal membrane oxygenation weaning. Int. J. Artif. Organs 2022, 45, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Paulo, N.; Kimmoun, A.; Hajage, D.; Hubert, P.; Levy, D.; Pineton de Chambrun, M.; Chommeloux, J.; Saura, O.; Del Marmol, G.; Moyon, Q.; et al. Does Levosimendan hasten veno-arterial ECMO weaning? A propensity score matching analysis. Ann. Intensive Care. 2025, 15, 48. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mehta, R.H.; Leimberger, J.D.; van Diepen, S.; Meza, J.; Wang, A.; Jankowich, R.; Harrison, R.W.; Hay, D.; Fremes, S.; Duncan, A.; et al. Levosimendan in Patients with Left Ventricular Dysfunction Undergoing Cardiac Surgery. N. Engl. J. Med. 2017, 376, 2032–2042. [Google Scholar] [CrossRef] [PubMed]
- Landoni, G.; Lomivorotov, V.V.; Alvaro, G.; Lobreglio, R.; Pisano, A.; Guarracino, F.; Calabrò, M.G.; Grigoryev, E.V.; Likhvantsev, V.V.; Salgado-Filho, M.F.; et al. Levosimendan for Hemodynamic Support after Cardiac Surgery. N. Engl. J. Med. 2017, 376, 2021–2031. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.C.; Perkins, G.D.; Singer, M.; McAuley, D.F.; Orme, R.M.; Santhakumaran, S.; Mason, A.J.; Cross, M.; Al-Beidh, F.; Best-Lane, J.; et al. Levosimendan for the Prevention of Acute Organ Dysfunction in Sepsis. N. Engl. J. Med. 2016, 375, 1638–1648. [Google Scholar] [CrossRef] [PubMed]
- Affronti, A.; di Bella, I.; Carino, D.; Ragni, T. Levosimendan may improve weaning outcomes in venoarterial ECMO patients. ASAIO J. 2013, 59, 554–557. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.S.; Kooda, K.; Igneri, L.A. A Narrative Review of the Impact of Extracorporeal Membrane Oxygenation on the Pharmacokinetics and Pharmacodynamics of Critical Care Therapies. Ann. Pharmacother. 2023, 57, 706–726. [Google Scholar] [CrossRef] [PubMed]
- Bertin, S.; Haefliger, D.; Perez, M.H.; Guidi, M.; Decosterd, L.A.; Chanez, V.; Di Paolo, E.R.; Buclin, T.; Livio, F. Pharmacokinetics of levosimendan in critically Ill children on extracorporeal membrane oxygenation: A prospective observational study. Front Pediatr. 2025, 13, 1542417. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dzierba, A.L.; Abrams, D.; Brodie, D. Medicating patients during extracorporeal membrane oxygenation: The evidence is building. Crit. Care 2017, 21, 66. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fresiello, L.; Hermens, J.A.J.; Pladet, L.; Meuwese, C.L.; Donker, D.W. The physiology of venoarterial extracorporeal membrane oxygenation—A comprehensive clinical perspective. Perfusion 2024, 39, 5S–12S. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hussey, P.T.; von Mering, G.; Nanda, N.C.; Ahmed, M.I.; Addis, D.R. Echocardiography for extracorporeal membrane oxygenation. Echocardiography 2022, 39, 339–370. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Levy, D.; Schmidt, M.; Hekimian, G.; Combes, A.; Saura, O. Clinical validation of pulmonary artery catheter use for continuous thermodilution cardiac output monitoring in VA-ECMO patients. Intensive Care Med. 2025, 51, 785–787. [Google Scholar] [CrossRef] [PubMed]
- Chirinos, J.A. Ventricular-arterial coupling: Invasive and non-invasive assessment. Artery Res. 2013, 7, 2–14. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Herpain, A.; Bouchez, S.; Girardis, M.; Guarracino, F.; Knotzer, J.; Levy, B.; Liebregts, T.; Pollesello, P.; Ricksten, S.E.; Riha, H.; et al. Use of Levosimendan in Intensive Care Unit Settings: An Opinion Paper. J. Cardiovasc. Pharmacol. 2019, 73, 3–14. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nieminen, M.S.; Akkila, J.; Hasenfuss, G.; Kleber, F.X.; Lehtonen, L.A.; Mitrovic, V.; Nyquist, O.; Remme, W.J. Hemodynamic and neurohumoral effects of continuous infusion of levosimendan in patients with congestive heart failure. J. Am. Coll. Cardiol. 2000, 36, 1903–1912. [Google Scholar] [CrossRef] [PubMed]
- Susilo, H.; Aldian, F.M.; Wungu, C.D.K.; Alsagaff, M.Y.; Sutanto, H.; Multazam, C.E.C.Z. Levosimendan, a Promising Pharmacotherapy in Cardiogenic Shock: A Comprehensive Review. Eur. Cardiol. 2024, 19, e21. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kasikcioglu, H.A.; Cam, N. A review of levosimendan in the treatment of heart failure. Vasc Health Risk Manag. 2006, 2, 389–400. [Google Scholar] [CrossRef] [PubMed] [PubMed Central][Green Version]
- Gagliardi, V.; Ceccherelli, F.; Lovato, A.; Gagliardi, G. The Effects of Levosimendan on Microcirculation and Peripheral Perfusion in Septic Shock: A Pilot Study. Life 2025, 15, 871. [Google Scholar] [CrossRef] [PubMed]
- Brunner, S.N.; Bogert, N.V.; Schnitzbauer, A.A.; Juengel, E.; Moritz, A.; Werner, I.; Kornberger, A.; Beiras-Fernandez, A. Levosimendan protects human hepatocytes from ischemia-reperfusion injury. PLoS ONE 2017, 12, e0187839. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhao, L.; Tian, L.; Wang, S.; Yang, W.; Lu, X.; Zhu, C. Levosimendan in rats decreases acute kidney injury after cardiopulmonary resuscitation by improving mitochondrial dysfunction. Transl. Androl. Urol. 2021, 10, 3010–3020. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tian, L.; Wang, S.; Zhao, L.; Lu, X.; Zhu, C.; Gong, H.; Yang, W. Renoprotective effects of levosimendan on acute kidney injury following cardiac arrest via anti-inflammation, anti-apoptosis, and ERK activation. FEBS Open Bio. 2021, 11, 2236–2244. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Govender, K.; Cabrales, P. Extracorporeal circulation impairs microcirculation perfusion and organ function. J. Appl. Physiol. (1985) 2022, 132, 794–810. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Volleman, C.; Raasveld, S.J.; Jamaludin, F.S.; Vlaar, A.P.J.; van den Brom, C.E. Microcirculatory Perfusion Disturbances During Veno-Arterial Extracorporeal Membrane Oxygenation: A Systematic Review. Microcirculation 2024, 31, e12891. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Xiong, F.; Hou, Y.; Yu, X.; Pan, P. Levosimendan for sepsis-induced myocardial dysfunction: Friend or foe? Front. Cardiovasc. Med. 2025, 11, 1520596. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Turkiewicz, K.; Rola, P.; Kulczycki, J.J.; Włodarczak, S.; Jastrzębski, A.; Pęcherzewski, M.; Furtan, Ł.; Barycki, M.; Doroszko, A.; Włodarczak, A.; et al. High-risk PCI facilitated by levosimendan infusion and Impella CP support in ACS cohort-pilot study. Kardiol. Pol. 2024, 82, 771–773. [Google Scholar] [CrossRef] [PubMed]
- Nieminen, M.S.; Fruhwald, S.; Heunks, L.M.; Suominen, P.K.; Gordon, A.C.; Kivikko, M.; Pollesello, P. Levosimendan: Current data, clinical use and future development. Heart Lung Vessel. 2013, 5, 227–245. [Google Scholar] [PubMed] [PubMed Central]
- Papp, Z.; Agostoni, P.; Alvarez, J.; Bettex, D.; Bouchez, S.; Brito, D.; Černý, V.; Comin-Colet, J.; Crespo-Leiro, M.G.; Delgado, J.F.; et al. Levosimendan Efficacy and Safety: 20 years of SIMDAX in Clinical Use. Card. Fail. Rev. 2020, 6, e19. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bunge, J.J.H.; Mariani, S.; Meuwese, C.; van Bussel, B.C.T.; Di Mauro, M.; Wiedeman, D.; Saeed, D.; Pozzi, M.; Loforte, A.; Boeken, U.; et al. Characteristics and Outcomes of Prolonged Venoarterial Extracorporeal Membrane Oxygenation After Cardiac Surgery: The Post-Cardiotomy Extracorporeal Life Support (PELS-1) Cohort Study. Crit. Care Med. 2024, 52, e490–e502. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tholén, M.; Ricksten, S.E.; Lannemyr, L. Effects of levosimendan on renal blood flow and glomerular filtration in patients with acute kidney injury after cardiac surgery: A double blind, randomized placebo-controlled study. Crit. Care 2021, 25, 207. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, H.; Jiang, L.; Fu, R.; Qin, P.; Zhang, X.; Tian, T.; Feng, G.X.; Yang, Y.M. Impact of levosimendan on efficacy and renal function in acute heart failure according to renal function: A perspective, multi-center, real-world registry. Front. Cardiovasc. Med. 2022, 9, 986039. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grossini, E.; Bellofatto, K.; Farruggio, S.; Sigaudo, L.; Marotta, P.; Raina, G.; De Giuli, V.; Mary, D.; Pollesello, P.; Minisini, R.; et al. Levosimendan inhibits peroxidation in hepatocytes by modulating apoptosis/autophagy interplay. PLoS ONE 2015, 10, e0124742. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Farmakis, D.; Alvarez, J.; Gal, T.B.; Brito, D.; Fedele, F.; Fonseca, C.; Gordon, A.C.; Gotsman, I.; Grossini, E.; Guarracino, F.; et al. Levosimendan beyond inotropy and acute heart failure: Evidence of pleiotropic effects on the heart and other organs: An expert panel position paper. Int. J. Cardiol. 2016, 222, 303–312. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).