Definition
Primary chondroprogenitors obtained from standardized cell sources (e.g., FE002 clinical grade cell sources) may be cultured in vitro and may be cytotherapeutically applied in allogeneic musculoskeletal regenerative medicine. Multicentric translational research on FE002 human primary chondroprogenitors under the Swiss progenitor cell transplantation program has notably validated their robustness and high versatility for therapeutic formulation in clinically compatible prototypes, as well as a good safety profile in diverse in vivo preclinical models. Therein, stringently controlled primary cell source establishment and extensive cell manufacturing optimization have technically confirmed the adequation of FE002 primary chondroprogenitors with standard industrial biotechnology workflows for consistent diploid cell biobanking under GMP. Laboratory characterization studies and extensive qualification work on FE002 progenitor cell sources have elucidated the key and critical attributes of the cellular materials of interest for potential and diversified human cytotherapeutic uses. Multiple formulation studies (i.e., hydrogel-based standardized transplants, polymeric-scaffold-based tissue engineering products) have shown the high versatility of FE002 primary chondroprogenitors, for the obtention of functional allogeneic cytotherapeutics. Multiple in vivo preclinical studies (e.g., rodent models, GLP goat model) have robustly documented the safety of FE002 primary chondroprogenitors following implantation. Clinically, FE002 primary chondroprogenitors may potentially be used in various forms for volumetric tissue replacement (e.g., treatment of large chondral/osteochondral defects of the knee) or for the local management of chondral affections and pathologies (i.e., injection use in mild to moderate osteoarthritis cases). Overall, standardized FE002 primary chondroprogenitors as investigated under the Swiss progenitor cell transplantation program were shown to constitute tangible contenders in novel human musculoskeletal regenerative medicine approaches, for versatile and safe allogeneic clinical cytotherapeutic management.
1. Introduction
Musculoskeletal diseases in general and chondral/osteochondral affections, in particular, are highly incident in aging patient populations [1,2,3,4]. While conservative orthopedic best practices enable the successful clinical management of critical cases of cartilage injury or degeneration (e.g., prosthetic replacement), effective regenerative medicine interventions and solutions are necessary in the cases of moderate to severe affections [3,5,6,7,8]. Therefore, many natural and artificial biomaterials or bioengineered constructs have been successfully clinically applied for chondropathies and cartilage tissue defects, with extensive available hindsight (i.e., intervention safety, quality, efficacy) [5,9,10,11,12,13,14,15,16,17,18]. Parallelly, important translational efforts, deployed over the past 40 years, have led to the implementation of diverse clinical protocols for several generations of autologous chondrocyte implantation (ACI) [1,4,8,19,20,21,22,23,24,25,26,27,28]. While initial and successful approaches to ACI may have relied on the use of cultured cells or minimally manipulated chondrocyte suspensions, current commercially available clinical approaches to cartilage regenerative medicine often comprise the use of a matrix/scaffold component (i.e., combination products, e.g., cells in a hyaluronan-based hydrogel scaffold or bilayer collagen constructs) [1,10,11,28,29,30,31,32,33,34,35,36,37].
Vast arrays of potential cell sources (e.g., various stem and progenitor cells, somatic cells, platelets, etc.) and processing methods (e.g., preparation of cell suspensions, spheroids) have been investigated for the high-quality cytotherapeutic management of chondropathies and chondral/osteochondral defects [7,11,38,39,40,41,42]. Recently, multiple genetically modified cell lines, designed for enhanced chondrogenic function, have been studied and clinically proposed for cartilage tissue engineering [6,43,44,45]. From a technical standpoint, the scientific knowledge of the in vitro behavior and functional evolution (i.e., transiently reduced chondrogenesis potential in monolayer cellular expansion) of cultured chondrocytes has rapidly increased [5,8,14,31,46,47,48,49,50,51,52,53,54,55]. For therapeutic cell manufacturing purposes, numerous studies have enabled and have validated (i.e., from technical, quality, and functional standpoints) the substitution of fetal bovine serum (FBS) by human platelet lysates (HPL) as cellular growth medium supplements [28,56,57,58,59,60,61,62,63]. Notwithstanding, despite enormous progress in the biotechnological and bioengineering approaches to cell-based combination products for cartilage repair and regeneration, important regulatory and clinical bottlenecks have recently been documented [28,40,64,65,66,67,68,69,70]. Indeed, specific quality-oriented and process-based approaches to cell therapy manufacturing have become the norm (e.g., application of cGMPs for cellular active substances and finished cell-based product manufacture) [28]. Importantly from the clinical standpoint, the cartilage lesion localization, the surgical approach, and the patient follow-up management plan have been identified as critical factors for consistently attaining long-term clinical success with cytotherapies for cartilage tissue affections [14,65,69].
Human primary chondroprogenitors (e.g., FE002 clinical grade cell sources) have been extensively investigated under the Swiss progenitor cell transplantation program as a potential cytotherapeutic solution for the optimal homologous allogeneic management of diverse cartilage tissue disorders [38,71,72]. Human FE002 primary chondroprogenitors are cultured diploid cells, inherently pre-terminally differentiated, which display monomodal and stable phenotypes in vitro [38,72]. Homogeneous and robust cryopreserved cell banks and cell lots of FE002 primary chondroprogenitors may be exploited as highly sustainable tools and material sources for allogeneic musculoskeletal cytotherapeutic applications under modern restrictive quality requirements [71,72]. Importantly, human FE002 primary chondroprogenitors are highly biocompatible with diverse biomaterials, possess an inherent immune privilege, and present no known tumorigenic behaviors [38,72].
Such standardized biological materials are biotechnologically manufactured and are formulated following best practices in pharmaceutical sciences and cell-based bioengineering, with the central therapeutic objectives of rapidly and optimally restoring chondral tissular structures and functions [72]. Overall, the FE002 primary chondroprogenitors investigated under the Swiss progenitor cell transplantation program were shown to present high robustness and versatility in an array of potential therapeutic uses (e.g., fresh or off-the-freezer cell therapies) in human musculoskeletal regenerative medicine [71,72]. A succinct overview of the currently published body of knowledge (i.e., scientific peer-reviewed elements) on FE002 primary chondroprogenitors is presented in Table 1.

Table 1.
Summary of the published peer-reviewed reports describing the collaborative and multicentric translational work (i.e., characterization, qualification, validation) on FE002 primary chondroprogenitors under the Swiss progenitor cell transplantation program. This constantly evolving body of knowledge has established FE002 primary chondroprogenitors as standardized and versatile cytotherapeutic contenders for human musculoskeletal regenerative medicine, for repair promotion and/or regeneration support in chondral/osteochondral affections. CAM, chorioallantoic membrane model; GLP, good laboratory practices; HA, hyaluronic acid.
Notably, multiple in vivo preclinical studies (e.g., in rodent and goat models) have robustly documented the safety of FE002 primary chondroprogenitors following implantation, which may therefore be safely considered for investigational human cytotherapeutic use (i.e., international first-in-man clinical trials) [72,76,77,79]. From a clinical indication standpoint, such cellular materials and combinations thereof may potentially be used for volumetric tissue replacement (e.g., treatment of extensive chondral/osteochondral defects of the knee) or the local management of mild to moderate chondral affections and pathologies (i.e., injectable hydrogels in osteoarthritis patients) [72]. Overall, the aggregated multicentric translational work on FE002 primary progenitor cell sources, performed over the past decade in Switzerland, has confirmed their high versatility and safety for application as cellular active ingredients within the development of novel cytotherapeutic products and standardized transplants for human use (Table 1) [38,72,76,77,78,79,80].
2. Primary Chondroprogenitors for Novel Allogeneic Tissue Engineering Applications: High International Focus & Published Translational Studies
Primary chondroprogenitors initially derived from prenatal tissues are often mentioned by researchers investigating potentially optimal therapeutic primary cell sources for allogeneic cartilage tissue engineering [3,14,38,76]. In addition to the high robustness and stability of these non-modified biological materials (i.e., “extensively manipulated” by cellular expansion, but without gene editing), the reported maintenance of chondrogenic functional potential by such cultured cells is critical for tissue engineering product function/efficacy [38,72]. Furthermore, the immune privilege of such primary progenitor cell sources procures tangible advantages in an allogeneic or xenogeneic therapeutic setting, for avoiding rejection by an immunocompetent host/recipient [71,72].
The scope of the present entry was set on the FE002 primary chondroprogenitors studied under the Swiss progenitor cell transplantation program, as all the considered cellular materials were derived from the same initial organ donation (i.e., FE002 donation, Table 1) [71,72]. However, important parallel preclinical work by international research groups has also focused on similar processes or uses of (i.e., primary or transformed) prenatal cartilage-derived progenitor cells and is noteworthy. Translational work on such primary cells has notably been undertaken by Korean- and US-based groups, reaching advanced preclinical model levels [81,82,83,84,85,86,87,88,89,90]. Specifically, the applicability and functionality of clinically compatible bioengineered prototypes containing primary chondroprogenitors were shown in vivo [81,83,84]. Therein, similar conclusions were drawn (i.e., as compared to the various Swiss groups) about the vast potential of the considered biological materials for high-quality allogeneic tissue engineering and alternative clinical applications in human orthopedic medicine [81,82,83,87].
Furthermore, a most notable and unique landmark in cell and gene therapies for cartilage tissue engineering is the historical case of Invossa (Tonogenchoncel-L, TissueGene-C, Kolon TissueGene, Rockville, MD, USA), a first-in-class orthopedic cell and gene therapy product [45]. Initially studied at preclinical levels over the 2000–2010 decade, this preparation comprises a mixture of cell populations [91,92,93,94]. Indeed, Invossa is reported to contain allogeneic non-transformed cells (i.e., chondrocytes from human polydactyly tissue) and retrovirally transduced human chondrocytes expressing TGF-β1 for enhanced functionality [95]. However, of particular interest, Invossa was instead reported to contain HEK-293 cells (i.e., immortalized cell line, derived from human embryonic kidney tissue) [45,96]. Therefore, instead of the transduced chondrocytes as initially described for Invossa, it was HEK-293 cells expressing TGF-β1 that were mixed with the allogeneic chondrocytes. Despite thunderous clinical trial interruptions following this gross mislabeling or cellular cross-contamination event, the clinical safety of the intervention (i.e., absence of adverse event occurrence, meeting of efficacy endpoints) was documented and enabled promoters to obtain regulatory approvals to continue the investigative human clinical work in the USA [45,96]. Of utmost importance, the fact that several clinical stages were successively and successfully passed by Invossa over the 2010–2020 decade and its ongoing investigational use (i.e., multi-centric clinical trials) in the USA create a strong and undeniable precedent for the direct use of prenatal tissue-derived cytotherapeutics (e.g., HEK-293 cells) in human regenerative medicine [6,97,98]. Specifically, while several technical elements and deviations remain to be clarified in the case of Invossa (i.e., potential cross-contaminations by HEK-293 stocks during therapeutic cell manufacturing), the specified orthopedic clinical endpoints were reported to have been met [45].
3. Starting Biological Material Procurement & Clinical-Grade FE002 Primary Chondroprogenitor Cell Source Establishment Methodology
Modern quality, safety, and traceability requirements around the processing of cytotherapeutic materials for human investigational regenerative medicine use are currently stringent and necessitate extensive methodological planning and documentation [99]. Therein, good manufacturing practices (GMP) must be employed notably for combined advanced therapy medicinal products (cATMP), which encompass most bioengineered cartilage tissue grafts requiring cell culture steps (i.e., substantial manipulation of the cells) [72]. Furthermore, close consideration of the locally applicable legal and ethical framework is necessary for biological starting material (i.e., cartilage tissue) procurement and for subsequent clinical grade progenitor cell source establishment [71,99]. In particular, up-to-date legal and ethical guidelines must constitute the basis of the methodological devising of starting material procurement and bioprocessing for clinical cytotechnologies and cytotherapeutics [71]. These elements are key in view of demonstrating to national regulators and health authorities that specific primary progenitor cell sources are fit for human investigational clinical use. Therefore, the considered examples of FE002 primary progenitor cell sources were established in Switzerland under a validated progenitor cell transplantation program, with standardized whole-cell bioprocessing and cell banking in view of eventual clinical and commercial use (Figure 1) [71].
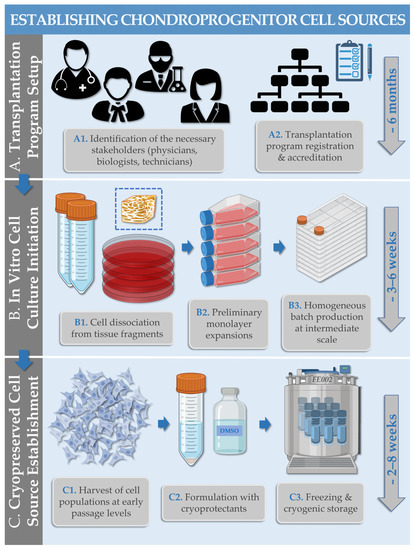
Figure 1.
Schematic and illustrated methodological workflow describing the establishment of FE002 primary progenitor cell sources under the Swiss progenitor cell transplantation program. (A1,A2) Appropriate roles and responsibility attribution within the operational team (i.e., for starting material procurement) is critical for the methodological soundness and accreditation of the cell transplantation program. (B1–B3) Following rapid initial cellular isolation from starting materials, serial in vitro cellular expansions are performed during the adherent cell culture initiation phase. (C1–C3) The obtained cellular materials are harvested after the monolayer expansion and are appropriately processed for cryopreservation in a cell bank system. Approximative timelines for individual phase execution are presented in blue font. DMSO, dimethyl sulfoxide.
Importantly, the robustness of primary progenitor cell biobanking and subsequent biotechnological cell manufacturing processes is a key technical parameter for obtaining homogeneous, high-quality, and consistent cellular harvests [71,72]. This enables to sustainably exploit defined progenitor cell sources and to perform extensive qualification/validation work on the manufacturing process and the obtained material lots, contrasting with autologous cell sources (i.e., usually highly limited in material availability) used in ACI [28,72]. Ultimately, these elements are useful and necessary for demonstrating the technological soundness and the preclinical quality of the retained allogeneic cytotherapeutic approach.
4. Optimized & Standardized FE002 Primary Chondroprogenitor Cell Banking & Biotechnological Manufacturing Processes
As previously mentioned for primary progenitor cell source establishment, the use of robust processes is essential for maintaining both the high quality and the sustainability of the considered biological source [72]. Therefore, process optimization studies and standardization work are critical early elements of industrial manufacturing process development and validation, enabling the specification of key and critical process parameters (KPP, CPP) or attributes [28]. Starting with seeding cell lots (i.e., usually parental cell bank (PCB) materials), all of the in vitro manufacturing activities are carried out according to conservative best practices of primary diploid cell culture (e.g., serial multi-tiered cell banking and cryopreserved vial lot manufacture, Figure 2) in grade A GMP manufacturing environments [72].
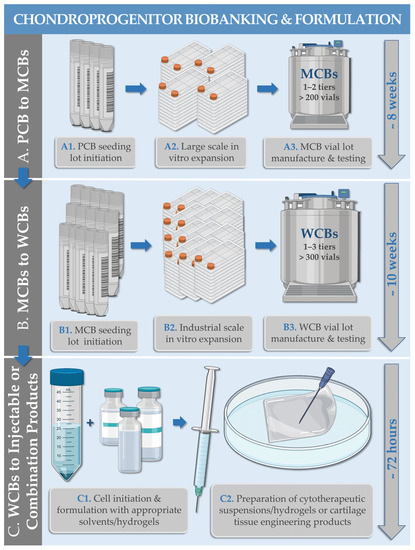
Figure 2.
Schematic and illustrated methodological workflow describing the multi-tiered cell banking and some of the combined cytotherapeutic uses of primary chondroprogenitors (e.g., FE002 primary progenitor cell sources). (A1–A3) Parental cell bank (PCB) cellular materials (i.e., cells at early in vitro passage levels) are used to generate master cell bank (MCB) materials (i.e., cells at intermediate in vitro passage levels). (B1–B3) MCB cellular materials are used to generate working cell bank (WCB) materials (i.e., cells at in vitro passage levels appropriate for clinical use). (C1,C2) WCB cellular materials may eventually be used for off-the-freezer reconstitution of injectable combination products (e.g., cell suspensions in autologous serum-based solutions or hyaluronan-based hydrogels) or for seeding of bioengineered cartilage grafts (e.g., use of Chondro-Gide collagen scaffolds). Within GMP-compliant multi-tiered biobanking systems, the various cell bank tiers are characterized by the in vitro cell passage level or by the in vitro cell population doubling level of the corresponding cellular population, in the sequential order of increasing levels along the progenitor cell manufacturing workflow. Approximative timelines for individual phase execution are presented in blue font. GMP, good manufacturing practices; MCB, master cell bank; PCB, parental cell bank; WCB, working cell bank.
Due to the documented high cellular robustness and overall in vitro stability of the studied FE002 chondroprogenitors, consistent technical specifications (e.g., cell seeding and harvest densities, culture medium exchange intervals, total cell culture periods) may be used for the successive adherent cellular expansion rounds of manufacturing campaigns (Table 1, Figure 3) [72].
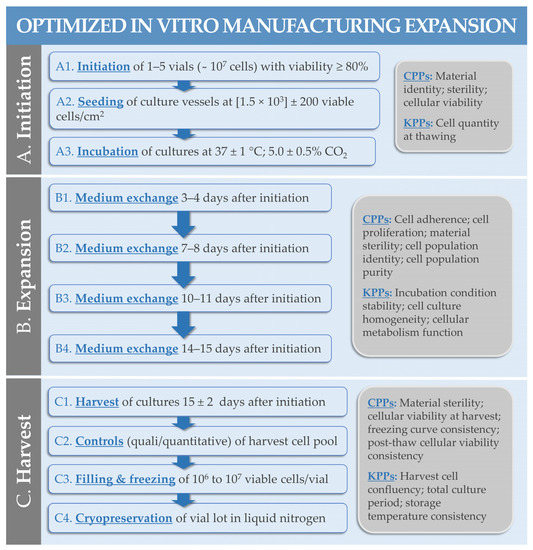
Figure 3.
Schematic methodological workflow describing an entire optimized in vitro expansion process for primary chondroprogenitors under the Swiss progenitor cell transplantation program (e.g., FE002 primary progenitor cell sources). A single cellular expansion phase is used within the defined cell banking workflow to sequentially and incrementally generate cell lots of superior passage levels. Consistent technical specifications (e.g., cell seeding densities, harvest cell confluency levels) are used for the in vitro cellular expansions throughout the entire progenitor cell biobanking workflow. All contact-process consumables (e.g., cell culture vessels), materials, and reagents (e.g., culture medium nutritive supplement, cell dissociation reagent, cell cryopreservation solution) are qualified/validated before production and all equipment or techniques are validated. (A1–A3) Initiation of the seeding cellular materials is performed by retrieval, controlled thawing and assessment, and distribution of the cells in the retained cell culture system. (B1–B4) The cellular expansion phase comprises incubation (i.e., 37 °C; 5% CO2) of the cell cultures and periodic cell culture medium exchange procedures. The nutritive component of the cell proliferation medium is classically 10% v/v FBS. (C1–C4) Endpoint enzymatic harvest of the expanded cell population is performed and enables the constitution of a new cell bank lot, following conditioning for storage and controlled-rate freezing of the bulk cellular suspension. Possible CPPs and KPPs are specified for individual process phases. CPP, critical process parameter; FBS, fetal bovine serum; KPP, key process parameter.
Once the progenitor cell lot manufacturing activities are performed (i.e., including GMP-specific in-process controls, IPC), appropriate safety and quality-oriented post-process controls (PPC, i.e., characterization or qualification assays, release testing) are performed on the cryopreserved vial lots [28,71]. FE002 progenitor cellular materials for human therapeutic use are usually manufactured in a GMP cell bank system, where biosafety testing schemes are adapted from Ph. Eur. general chapter 5.2.3 and ICH Q5A (Table 2) [100,101].
Table 2.
Generic testing requirements for clinical grade FE002 progenitor cytotherapeutic materials (i.e., primary diploid cell type) within a GMP multi-tiered cell bank system, adapted from Ph. Eur. general chapter 5.2.3. The implementation of specific tests and assays at specific stages/tiers of the cell banking process is designed and performed by the manufacturer, based on specific and appropriate risk analyses. EOPCB, end-of-production cell bank; GMP, good manufacturing practices; MCB, master cell bank; PCB, parental cell bank; WCB, working cell bank.
Despite the existence of minimal standards and basic requirements, each cytotherapeutic product manufacturing process is different (i.e., “the process is the product”) and must be considered from an overall quality and safety point-of-view [99]. Therefore, both the frequency and the extent of the necessary testing are based on justified risk analyses performed by the manufacturer (Table 2). From a technical standpoint, the use of defined-composition cell proliferation media or cell cryopreservation media is in accordance with modern guidelines, yet the highest attention must be paid to benchmarking and stringent qualification/validation of such elements against conservative standards (e.g., FBS, DMSO-based cryoprotectant solutions) as concerns stability and functional parameters (i.e., ICH Q5E, Q11) [72]. Finally, preclinical research and early process validation steps should be undertaken with manufacturing scalability and GMP-transposition objectives in mind, to rationalize the fixed costs of product/protocol development [71].
5. FE002 Primary Chondroprogenitor In Vitro Characterization & Qualification Data: Robust Fibroblastic Cells with Conserved Chondrogenic Functions
Multicentric characterization and qualification studies, collaboratively performed in Switzerland on FE002 primary chondroprogenitors, have been enabled to gather substantial data in view of their further translational use and clinical applications (Table 1). Notably, complementary research groups from two Universities and two federal polytechnical schools (i.e., Lausanne and Zurich, respectively) have locally contributed to enhancing the multifaceted body of knowledge existing around such potential cytotherapeutic materials (Table 1, Figure 4).
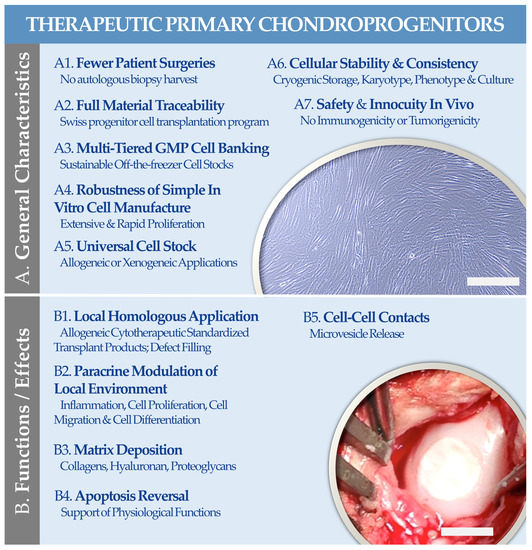
Figure 4.
An illustrated summary of the (A1–A7) general characteristics and of the (B1–B5) possible functions or effects of FE002 primary chondroprogenitors for therapeutic use in allogeneic orthopedic regenerative medicine. (A) The illustration represents contrast phase microscopic records of adherent FE002 chondroprogenitors at the end of the in vitro proliferation phase. Scale bar = 100 µm. (B) The illustration represents a bioengineered cartilage graft, consisting of FE002 primary chondroprogenitors seeded on a bilayer collagen scaffold (Chondro-Gide, Geistlich Pharma, Wolhusen, Switzerland), following implantation in the knee joint in a GLP goat model of chondral defect. Scale bar = 7.5 mm. GLP, good laboratory practices; GMP, good manufacturing practices. Modified and adapted from [72].
Overall, the reported scientific and technical body of knowledge around the considered FE002 primary chondroprogenitors was found to be in line with alternative literature reports as concerns the applicability of such cellular materials in therapeutic cartilage bioengineering [72,81,83,84]. Specifically, the accumulated data has underscored that such biological materials were well-adapted for the standardized manufacturing of novel allogeneic cytotherapies for human clinical use (Table 1) [72]. Therein, high versatility in the formulation options for the cellular active substance of interest was confirmed, as detailed hereafter.
6. Therapeutic Formulation Options for FE002 Primary Chondroprogenitors: High Versatility in Potential Cell-Assisted Orthopedic Applications
The multicentric formulation studies performed in Switzerland using FE002 primary chondroprogenitors for orthopedic standardized transplant products have further been enabled to gather complementary data of high translational relevance [72]. In particular, it was underscored that several formulation options (e.g., based on gels or solid scaffolds) are adequate for the clinical delivery of FE002 primary chondroprogenitors in a viable and functional form (Table 3).
Table 3.
Descriptive listing of the various cell-based product formulation options investigated for primary FE002 chondroprogenitors, as studied under the Swiss progenitor cell transplantation program. The reported diversity in formulation options and technological approaches has confirmed the versatility of the considered biologicals for clinically compatible cytotherapeutics. ACAN, aggrecan; COL, collagen; CRIS, compression released-induced suction; EGDMA, ethylene glycol dimethacrylate; GAG, glycosaminoglycan; GelNB, gelatin norbornene; GLP, good laboratory practices; HA, hyaluronic acid; HEMA, 2-hydroxyethyl methacrylate; Hep, heparin; PEGdiSH, poly(ethylene glycol)dithiol; TG, transglutaminase; TGF-β1, transforming growth factor β1; TRPV4, transient receptor potential channels 4.
Notably, several in vitro studies have been enabled to gain better comprehension and knowledge about the mechanobiology of the considered FE002 primary progenitor cells and about the influence of formulation and environmental parameters on cellular function/potency (Table 3) [72,73,74,75,76,77,78,79]. Furthermore, several translational studies have been enabled to verify combination product safety and function in vivo in diverse complex settings [72,76,79,80]. Overall, the available reports have underscored the versatility of the considered FE002 primary chondroprogenitors for cytotherapeutic product formulation, with effective resistance to various physical and chemical stresses in multiple experimental environments (Table 3). Based on existing clinical practices of ACI, two formulation types may tangibly be further considered for the clinical investigational use of allogeneic FE002 primary chondroprogenitors, namely an injectable hydrogel carrying the cellular payload (e.g., cellular suspension, cell spheroids), or a three-dimensional tissue-engineered chondral graft (e.g., cell culture and chondrogenic induction on a bilayer collagen scaffold) [72,79,80]. Therefore, depending on the therapeutic indication or the severity of the orthopedic affection, the diversified cytotherapeutic approach may be modulated regarding product formulation and delivery to fit clinical needs (Figure 4).
7. FE002 Primary Chondroprogenitor Preclinical Safety Evidence: Consistency of Product Innocuity in Various Animal Models
In complement to the in vitro characterization/qualification data available for the considered FE002 primary chondroprogenitors, several in vivo studies were performed and may be aggregated to robustly confirm the safety parameters of the cytotherapeutic materials, in view of their further translational and clinical uses (Table 4).
Table 4.
Summarized descriptive listing of the various in vivo models used to study the considered FE002 primary chondroprogenitors and the related cytotherapeutic product prototypes under the Swiss progenitor cell transplantation program. CAM, chorioallantoic membrane model; CRP, C-reactive protein; ECM, extracellular matrix; GLP, good laboratory practices; IL, interleukin; SAA, serum amyloid A protein; SAP, serum amyloid P component; TNF, tumor necrosis factor.
Importantly, the absence of toxicity, immunogenicity, or tumorigenicity of the considered FE002 primary chondroprogenitors was demonstrated within the retained in vivo experimental setups, among which a large animal GLP study (Table 4) [72]. The aggregation of the available and published in vivo safety-related evidence has enabled a positive assessment of the applicability of FE002 primary chondroprogenitors for further translational investigation and pilot human clinical trials [72].
8. Regulatory-Oriented Considerations for Allogeneic Tissue Engineering Products Containing Viable FE002 Primary Chondroprogenitors
Clinical cytotherapeutic applications of bioengineered cartilage grafts containing viable primary chondroprogenitors are regulated by legal dispositions on standardized transplant products (TrSt) in Switzerland [72]. Due to burdensome regulatory constraints (i.e., frequent framework and guideline shifts, high direct costs) for novel product development, limited numbers of sponsors have been investigating and commercializing orthopedic TrSt or cATMP protocols/products for cartilage (e.g., Spherox, CO.DON, Leipzig, Germany) in recent years [64,68]. Notably, examples of authorization expiration for commercialized protocols or products (e.g., MACI in the EU, Genzyme Europe, Amsterdam, The Netherlands) have been documented [103]. Furthermore, some products have been withdrawn by the manufacturer (e.g., ChondroCelect, TiGenix NV, Leuven, Belgium), despite obtained and valid market authorizations [103,104]. These examples tangibly illustrate the difficulty of integration of such innovative cell-based therapeutic approaches in current healthcare systems (i.e., for a variety of reasons, e.g., lack of efficacy, unfavorable cost–benefit ratios, extensive manufacturing delays), despite sizeable clinical need and demand [103]. In addition, several technical and logistical elements (i.e., cryogenic storage and cold chains) and clinical bottlenecks (e.g., low rates of therapeutic cell engraftment) must be considered early on during cytotherapeutic product development phases [72,105].
Notwithstanding, the current state-of-the-art as regards the human cytotherapeutic use of allogeneic FE002 primary chondroprogenitors for cartilage tissue engineering is at the crossroad of large animal models and first-in-man investigational use [72]. Critical aspects of priority interest to regulators and health authorities in view of authorizing a corresponding phase I clinical trial pertain mainly to the quality of manufacturing processes and the demonstration of product safety [70,71,72]. As concerns the quality of a specified product/protocol, recent harmonization in requirements for GMP manufacturing activities has led to technical updates and the current availability of several contract manufacturers across Europe [99]. With regard to the safety of a novel cytotherapeutic combination product containing allogeneic FE002 primary chondroprogenitors, the use of a registered medical device as a cell scaffold (e.g., Chondro–Gide) may alleviate part of the regulatory scrutiny, as compared to the development of a proprietary matrix/scaffold [72]. As concerns the safety of the cellular active substance itself, the combination of in vivo studies and GMP qualification/release testing results appears significant to form an appropriate preclinical assessment.
Importantly, clinical workflow parameters of allogeneic cytotherapies and cartilage tissue engineering products present significant potential advantages over ACI in its various generations (e.g., reduced operative burdens, no autologous biopsy harvest, no manufacturing-related delays) (Figure 4). Therefore, building on the large available clinical hindsight in ACI (e.g., 5-year follow-up with quantitative endpoints/outcomes), appropriate efficacy targets may be specified for novel allogeneic orthopedic approaches [106,107,108,109,110,111,112,113,114]. However, as regards the preclinical efficacy evaluation of novel cell or gene-based orthopedic products, high methodological inhomogeneity has been documented and no consensus is currently available [70]. In detail, very few GLP animal studies were reportedly performed (i.e., within market approval procedures) for FDA-authorized cell and gene therapy products [70]. Furthermore, as many patient-reported scored outcomes are used in orthopedics, the need for in vivo preclinical efficacy data has been recently directly challenged, for the rationalization of animal experimentation and resources [70]. Therefore, based on the growing preclinical data on allogeneic orthopedic cell therapies (e.g., based on FE002 chondroprogenitors) and specific historical cases of documented clinical evidence (e.g., Invossa) of therapeutic success, a transition from autologous to allogeneic cell-based approaches is currently well underway [72].
9. Conclusions and Prospects
Based on the extensive clinical hindsight available for autologous cell therapies in orthopedics and the growing preclinical experience around allogeneic applications, high interest is currently set on the translational development of novel products and protocols for optimized cartilage repair/regeneration. The compilation of the published body of knowledge around FE002 primary chondroprogenitors has confirmed the high versatility of such robust biological materials within translational approaches of chondropathy therapeutic management. Multicentric preclinical research under the Swiss progenitor cell transplantation program has notably demonstrated that such standardized biologicals could be safely and consistently used in various orthopedic product formulations for allogeneic bioengineering approaches. These elements were further confirmed by international literature reports on the similar potential therapeutic uses of chondroprogenitors or derivatives. Clinically, standardized transplants containing FE002 primary chondroprogenitors may potentially be applied in cases of volumetric tissue replacement (e.g., extensive chondral/osteochondral defects of the knee) or localized chondral affections and pathologies (e.g., mild to moderate osteoarthritis). Overall, the use of safe and standardized cell sources, such as FE002 primary chondroprogenitors, and appropriate quality-oriented manufacturing and clinical approaches constitute a tangible working basis for the further translational development of allogeneic orthopedic cytotherapies.
Author Contributions
Conceptualization, A.L., A.J., C.S., N.H.-B. and L.A.A.; methodology, A.L., A.J., C.S., V.P., P.A.-S., R.M., N.H.-B. and L.A.A.; software, A.L.; validation, A.L., A.J., C.P., C.S., V.P., P.A.-S., W.R., R.M., N.H.-B. and L.A.A.; formal analysis, A.L., A.J., C.S., P.A.-S., N.H.-B. and L.A.A.; investigation, A.L., A.J., C.P., C.S., V.P., P.A.-S., W.R., R.M., N.H.-B. and L.A.A.; resources, A.L. and L.A.A.; data curation, A.L.; writing—original draft preparation, A.L. and L.A.A.; writing—review and editing, A.L., A.J., C.P., C.S., V.P., P.A.-S., W.R., R.M., N.H.-B. and L.A.A.; visualization, A.L. and L.A.A.; supervision, W.R., N.H.-B. and L.A.A.; project administration, A.L. and L.A.A.; funding acquisition, L.A.A. Author A.L. participated in this work within the scope of an industrial Ph.D. thesis at the Faculty of Biology and Medicine (FBM) of the University of Lausanne (UNIL, Lausanne, Switzerland) under the co-supervision of authors N.H.-B. and W.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors are grateful to the S.A.N.T.E and Sandoz Foundations for their unconditional support of the Swiss progenitor cell transplantation program. The authors are grateful and thankful for the shared time and close collaboration with the Pharmaceutical Technology group at the Institute of Pharmaceutical Sciences of Western Switzerland (University of Geneva, Geneva, Switzerland), the Tissue Engineering and Biofabrication laboratory at the ETH Zurich (Zurich, Switzerland), the Laboratory of Biomechanical Orthopedics at the EPFL (Lausanne, Switzerland), and the Musculoskeletal Research Unit at the UZH (Zurich, Switzerland). Artwork templates for the figures of the present study were partly created with www.biorender.com, accessed 15 February 2023.
Conflicts of Interest
Authors A.L., A.J. and C.P. were employed by LAM Biotechnologies SA during the preparation and redaction of this work. The funders had no role in the study’s design; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. The remaining authors declare no conflicts of interest.
Abbreviations
| ACAN | aggrecan |
| ACI | autologous chondrocyte implantation |
| ATMP | advanced therapy medicinal product |
| CAM | chorioallantoic membrane model |
| cATMP | combined advanced therapy medicinal product |
| Col | collagen |
| CPP | critical process parameter |
| CRIS | compression released-induced suction |
| CRP | C reactive protein |
| DMSO | dimethyl sulfoxide |
| ECM | extracellular matrix |
| EGDMA | ethylene glycol dimethacrylate |
| EOPCB | end of production cell bank |
| EU | European Union |
| FBS | fetal bovine serum |
| FDA | US Food and Drug Administration |
| GAG | glycosaminoglycan |
| GelB | gelatin norbornene |
| GLP | good laboratory practices |
| GMP | good manufacturing practices |
| HA | hyaluronic acid |
| HEMA | 2-hydroxyethyl methacrylate |
| Hep | heparin |
| KPP | key process parameter |
| IL | interleukin |
| IPC | in-process control |
| MCB | master cell bank |
| PCB | parental cell bank |
| PEGdiSH | poly(ethylene glycol)dithiol |
| Ph. Eur. | European pharmacopoeia |
| PPC | post-process control |
| SAA | serum amyloid A protein |
| SAP | serum amyloid P component |
| TG | transglutaminase |
| TGF | transforming growth factor |
| TNF | tumor necrosis factor |
| TRPV4 | transient receptor potential channels 4 |
| TrSt | standardized transplant product |
| USA | United States of America |
| WCB | working cell bank |
References
- Brittberg, M.; Lindahl, A.; Nilsson, A.; Ohlsson, C.; Isaksson, O.; Peterson, L. Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N. Engl. J. Med. 1994, 331, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Bedi, A.; Feeley, B.T.; Williams, R.J. Management of articular cartilage defects of the knee. J. Bone Jt. Surg. Am. 2010, 92, 994–1009. [Google Scholar] [CrossRef] [PubMed]
- Urlic, I.; Ivkovic, A. Cell sources for cartilage repair-biological and clinical perspective. Cells 2021, 10, 2496. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.; Laurent, A.; Applegate, L.A.; Philippe, V. Grands défects chondraux et ostéochondraux du genou: Traitement par greffe chondrocytaire autologue. Rev. Med. Suisse 2022, 18, 2384–2390. [Google Scholar] [CrossRef] [PubMed]
- Makris, E.A.; Gomoll, A.H.; Malizos, K.N.; Hu, J.C.; Athanasiou, K.A. Repair and tissue engineering techniques for articular cartilage. Nat. Rev. Rheumatol. 2015, 11, 21–34. [Google Scholar] [CrossRef]
- Cherian, J.J.; Parvizi, J.; Bramlet, D.; Lee, K.H.; Romness, D.W.; Mont, M.A. Preliminary results of a phase II randomized study to determine the efficacy and safety of genetically engineered allogeneic human chondrocytes expressing TGF-B1 in patients with grade 3 chronic degenerative joint disease of the knee. Osteoarthr. Cartil. 2015, 23, 2109–2118. [Google Scholar] [CrossRef]
- Teo, A.Q.A.; Wong, K.L.; Shen, L.; Lim, J.Y.; Wei, S.T.; Lee, H.; Hui, J.H.P. Equivalent 10-year outcomes after implantation of autologous bone marrow-derived mesenchymal stem cells versus autologous chondrocyte implantation for chondral defects of the knee. Am. J. Sport. Med. 2019, 47, 2881–2887. [Google Scholar] [CrossRef]
- Asnaghi, M.A.; Power, L.; Barbero, A.; Haug, M.; Köppl, R.; Wendt, D.; Martin, I. Biomarker signatures of quality for engineering nasal chondrocyte-derived cartilage. Front. Bioeng. Biotechnol. 2020, 8, 283. [Google Scholar] [CrossRef]
- Ehlers, E.M.; Fuss, M.; Rohwedel, J.; Russlies, M.; Kühnel, W.; Behrens, P. Development of a biocomposite to fill out articular cartilage lesions. Light, scanning and transmission electron microscopy of sheep chondrocytes cultured on a collagen I/III sponge. Ann. Anat. 1999, 181, 513–518. [Google Scholar] [CrossRef]
- Marcacci, M.; Berruto, M.; Brocchetta, D.; Delcogliano, A.; Ghinelli, D.; Gobbi, A.; Kon, E.; Pederzini, L.; Rosa, D.; Sacchetti, G.L.; et al. Articular cartilage engineering with Hyalograft C: 3-year clinical results. Clin. Orthop. Rel. Res. 2005, 435, 96–105. [Google Scholar] [CrossRef]
- Dhollander, A.A.; Verdonk, P.C.; Lambrecht, S.; Verdonk, R.; Elewaut, D.; Verbruggen, G.; Almqvist, K.F. Midterm results of the treatment of cartilage defects in the knee using alginate beads containing human mature allogenic chondrocytes. Am. J. Sport. Med. 2012, 40, 75–82. [Google Scholar] [CrossRef]
- Marlovits, S.; Aldrian, S.; Wondrasch, B.; Zak, L.; Albrecht, C.; Welsch, G.; Trattnig, S. Clinical and radiological outcomes 5 years after matrix-induced autologous chondrocyte implantation in patients with symptomatic, traumatic chondral defects. Am. J. Sport. Med. 2012, 40, 2273–2280. [Google Scholar] [CrossRef]
- Brix, M.O.; Stelzeneder, D.; Chiari, C.; Koller, U.; Nehrer, S.; Dorotka, R.; Windhager, R.; Domayer, S.E. Treatment of full-thickness chondral defects with Hyalograft C in the knee: Long-term results. Am. J. Sport. Med. 2014, 42, 1426–1432. [Google Scholar] [CrossRef]
- Kon, E.; Roffi, A.; Filardo, G.; Tesei, G.; Marcacci, M. Scaffold-based cartilage treatments: With or without cells? A systematic review of preclinical and clinical evidence. Arthroscopy 2015, 31, 767–775. [Google Scholar] [CrossRef]
- Brittberg, M.; Gomoll, A.H.; Canseco, J.A.; Far, J.; Lind, M.; Hui, J. Cartilage repair in the degenerative ageing knee. Acta Orthop. 2016, 87, 26–38. [Google Scholar] [CrossRef]
- Kon, E.; Filardo, G.; Brittberg, M.; Busacca, M.; Condello, V.; Engebretsen, L.; Marlovits, S.; Niemeyer, P.; Platzer, P.; Posthumus, M.; et al. A multilayer biomaterial for osteochondral regeneration shows superiority vs. microfractures for the treatment of osteochondral lesions in a multicentre randomized trial at 2 years. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 2704–2715. [Google Scholar] [CrossRef]
- Binder, H.; Hoffman, L.; Zak, L.; Tiefenboeck, T.; Aldrian, S.; Albrecht, C. Clinical evaluation after matrix-associated autologous chondrocyte transplantation: A comparison of four different graft types. Bone Jt. Res. 2021, 10, 370–379. [Google Scholar] [CrossRef]
- Porcello, A.; Laurent, A.; Hirt-Burri, N.; Abdel-Sayed, P.; de Buys Roessingh, A.; Raffoul, W.; Jordan, O.; Allémann, E.; Applegate, L.A. Hyaluronan-based hydrogels as functional vectors for standardized therapeutics in tissue engineering and regenerative medicine. In Nanopharmaceuticals in Regenerative Medicine; CRC Press: Boca Raton, FL, USA, 2022. [Google Scholar] [CrossRef]
- Peterson, L.; Minas, T.; Brittberg, M.; Nilsson, A.; Sjögren-Jansson, E.; Lindahl, A. Two- to 9-year outcome after autologous chondrocyte transplantation of the knee. Clin. Orthop. Rel. Res. 2000, 374, 212–234. [Google Scholar] [CrossRef]
- Harris, J.D.; Siston, R.A.; Pan, X.; Flanigan, D.C. Autologous chondrocyte implantation: A systematic review. J. Bone Jt. Surg. 2010, 92, 2220–2233. [Google Scholar] [CrossRef]
- Peterson, L.; Vasiliadis, H.S.; Brittberg, M.; Lindahl, A. Autologous chondrocyte implantation: A long-term follow-up. Am. J. Sport. Med. 2010, 38, 1117–1124. [Google Scholar] [CrossRef]
- Bentley, G.; Biant, L.C.; Vijayan, S.; Macmull, S.; Skinner, J.A.; Carrington, R.W. Minimum ten-year results of a prospective randomised study of autologous chondrocyte implantation versus mosaicplasty for symptomatic articular cartilage lesions of the knee. J. Bone Jt. Surg. 2012, 94, 504–509. [Google Scholar] [CrossRef] [PubMed]
- Biant, L.C.; Bentley, G.; Vijayan, S.; Skinner, J.A.; Carrington, R.W. Long-term results of autologous chondrocyte implantation in the knee for chronic chondral and osteochondral defects. Am. J. Sport. Med. 2014, 42, 2178–2183. [Google Scholar] [CrossRef] [PubMed]
- Nawaz, S.Z.; Bentley, G.; Briggs, T.W.; Carrington, R.W.; Skinner, J.A.; Gallagher, K.R.; Dhinsa, B.S. Autologous chondrocyte implantation in the knee: Mid-term to long-term results. J. Bone Jt. Surg. 2014, 96, 824–830. [Google Scholar] [CrossRef] [PubMed]
- Oussedik, S.; Tsitskaris, K.; Parker, D. Treatment of articular cartilage lesions of the knee by microfracture or autologous chondrocyte implantation: A systematic review. Arthroscopy 2015, 31, 732–744. [Google Scholar] [CrossRef]
- Mumme, M.; Barbero, A.; Miot, S.; Wixmerten, A.; Feliciano, S.; Wolf, F.; Asnaghi, A.M.; Baumhoer, D.; Bieri, O.; Kretzcchmar, M.; et al. Nasal chondrocyte-based engineered autologous cartilage tissue for repair of articular cartilage defects: An observational first-in-human trial. Lancet 2016, 388, 1985–1994. [Google Scholar] [CrossRef]
- Davies, R.L.; Kuiper, N.J. Regenerative medicine: A review of the evolution of autologous chondrocyte implantation (ACI) therapy. Bioengineering 2019, 6, 22. [Google Scholar] [CrossRef]
- Philippe, V.; Laurent, A.; Hirt-Burri, N.; Abdel-Sayed, P.; Scaletta, C.; Schneebeli, V.; Michetti, M.; Brunet, J.-F.; Applegate, L.A.; Martin, R. Retrospective analysis of autologous chondrocyte-based cytotherapy production for clinical use: GMP process-based manufacturing optimization in a Swiss university hospital. Cells 2022, 11, 1016. [Google Scholar] [CrossRef]
- Abelow, S.P.; Guillen, P.; Ramos, T. Arthroscopic technique for matrix-induced autologous chondrocyte implantation for the treatment of large chondral defects in the knee and ankle. Op. Tech. Orthop. 2006, 16, 257–261. [Google Scholar] [CrossRef]
- Brittberg, M. Cell carriers as the next generation of cell therapy for cartilage repair: A review of the matrix-induced autologous chondrocyte implantation procedure. Am. J. Sport. Med. 2010, 38, 1259–1271. [Google Scholar] [CrossRef]
- Albrecht, C.; Tichy, B.; Nürnberger, S.; Hosiner, S.; Zak, L.; Aldrian, S.; Marlovits, S. Gene expression and cell differentiation in matrix-associated chondrocyte transplantation grafts: A comparative study. Osteoarthr. Cart. 2011, 19, 1219–1227. [Google Scholar] [CrossRef]
- Flohé, S.; Betsch, M.; Ruße, K.; Wild, M.; Windolf, J.; Schulz, M. Comparison of two different matrix-based autologous chondrocyte transplantation systems: 1 year follow-up results. Eur. J. Trauma Emerg. Surg. 2011, 37, 397–403. [Google Scholar] [CrossRef]
- Cortese, F.; McNicholas, M.; Janes, G.; Gillogly, S.; Abelow, S.P.; Gigante, A.; Coletti, N. Arthroscopic delivery of matrix-induced autologous chondrocyte implant: International experience and technique recommendations. Cartilage 2012, 3, 156–164. [Google Scholar] [CrossRef]
- Crawford, D.C.; DeBerardino, T.M.; Williams, R.J., 3rd. NeoCart, an autologous cartilage tissue implant, compared with microfracture for treatment of distal femoral cartilage lesions: An FDA phase-II prospective, randomized clinical trial after two years. J. Bone Jt. Surg. 2012, 94, 979–989. [Google Scholar] [CrossRef]
- Vijayan, S.; Bartlett, W.; Bentley, G.; Carrington, R.W.; Skinner, J.A.; Pollock, R.C.; Alorjani, M.; Briggs, T.W. Autologous chondrocyte implantation for osteochondral lesions in the knee using a bilayer collagen membrane and bone graft: A two- to eight-year follow-up study. J. Bone Jt. Surg. 2012, 94, 488–492. [Google Scholar] [CrossRef]
- McCarthy, H.S.; Roberts, S. A histological comparison of the repair tissue formed when using either Chondrogide(®) or periosteum during autologous chondrocyte implantation. Osteoarthr. Cart. 2013, 21, 2048–2057. [Google Scholar] [CrossRef]
- Li, X.; Li, S.; Qian, J.; Chen, Y.; Zhou, Y.; Fu, P. Early efficacy of type I collagen-based matrix-assisted autologous chondrocyte transplantation for the treatment of articular cartilage lesions. Front. Bioeng. Biotechnol. 2021, 9, 760179. [Google Scholar] [CrossRef]
- Darwiche, S.E.; Scaletta, C.; Raffoul, W.; Pioletti, D.P.; Applegate, L.A. Epiphyseal chondroprogenitors provide a stable cell source for cartilage cell therapy. Cell Med. 2012, 4, 23–32. [Google Scholar] [CrossRef]
- Pelttari, K.; Pippenger, B.; Mumme, M.; Feliciano, S.; Scotti, C.; Mainil-Varlet, P.; Procino, A.; von Rechenberg, B.; Schwamborn, T.; Jakob, M.; et al. Adult human neural crest-derived cells for articular cartilage repair. Sci. Transl. Med. 2014, 6, 251ra119. [Google Scholar] [CrossRef]
- Huang, B.J.; Hu, J.C.; Athanasiou, K.A. Cell-based tissue engineering strategies used in the clinical repair of articular cartilage. Biomaterials 2016, 98, 1–22. [Google Scholar] [CrossRef]
- Mortazavi, F.; Shafaei, H.; Soleimani Rad, J.; Rushangar, L.; Montaceri, A.; Jamshidi, M. High quality of infant chondrocytes in comparison with adult chondrocytes for cartilage tissue engineering. World J. Plast. Surg. 2017, 6, 183–189. [Google Scholar]
- Hoburg, A.; Niemeyer, P.; Laute, V.; Zinser, W.; Becher, C.; Kolombe, T.; Fay, J.; Pietsch, S.; Kuźma, T.; Widuchowski, W.; et al. Sustained superiority in KOOS subscores after matrix-associated chondrocyte implantation using spheroids compared to microfracture. Knee Surg. Sport. Traumatol. Arthrosc. 2023, 31, 2482–2493. [Google Scholar] [CrossRef] [PubMed]
- Ha, C.-W.; Noh, M.J.; Choi, K.B.; Lee, K.H. Initial phase I safety of retrovirally transduced human chondrocytes expressing transforming growth factor-beta-1 in degenerative arthritis patients. Cytotherapy 2012, 14, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Tritschler, H.; Fischer, K.; Seissler, J.; Fiedler, J.; Halbgebauer, R.; Huber-Lang, M.; Schnieke, A.; Brenner, R.E. New insights into xenotransplantation for cartilage repair: Porcine multi-genetically modified chondrocytes as a promising cell source. Cells 2021, 10, 2152. [Google Scholar] [CrossRef]
- Evans, C.H.; Ghivizzani, S.C.; Robbins, P.D. Orthopaedic gene therapy: Twenty-five years on. JBJS Rev. 2021, 9, e20. [Google Scholar] [CrossRef] [PubMed]
- Manning, W.K.; Bonner, W.M., Jr. Isolation and culture of chondrocytes from human adult articular cartilage. Arthritis Rheum. 1967, 10, 235–239. [Google Scholar] [CrossRef]
- Tallheden, T.; Karlsson, C.; Brunner, A.; Van Der Lee, J.; Hagg, R.; Tommasini, R.; Lindahl, A. Gene expression during redifferentiation of human articular chondrocytes. Osteoarthr. Cart. 2004, 12, 525–535. [Google Scholar] [CrossRef]
- Kang, S.W.; Yoo, S.P.; Kim, B.S. Effect of chondrocyte passage number on histological aspects of tissue-engineered cartilage. Bio-Med. Mat. Eng. 2007, 17, 269–276. [Google Scholar] [PubMed]
- Martinez, I.; Elvenes, J.; Olsen, R.; Bertheussen, K.; Johansen, O. Redifferentiation of in vitro expanded adult articular chondrocytes by combining the hanging-drop cultivation method with hypoxic environment. Cell Transplant. 2008, 17, 987–996. [Google Scholar] [CrossRef]
- Lin, Z.; Fitzgerald, J.B.; Xu, J.; Willers, C.; Wood, D.; Grodzinsky, A.J.; Zheng, M.H. Gene expression profiles of human chondrocytes during passaged monolayer cultivation. J. Orthop. Res. 2008, 26, 1230–1237. [Google Scholar] [CrossRef]
- Enochson, L.; Brittberg, M.; Lindahl, A. Optimization of a chondrogenic medium through the use of factorial design of experiments. BioRes Open Access 2012, 1, 306–313. [Google Scholar] [CrossRef]
- Oseni, A.O.; Butler, P.E.; Seifalian, A.M. Optimization of chondrocyte isolation and characterization for large-scale cartilage tissue engineering. J. Surg. Res. 2013, 181, 41–48. [Google Scholar] [CrossRef]
- Chijimatsu, R.; Kobayashi, M.; Ebina, K.; Iwahashi, T.; Okuno, Y.; Hirao, M.; Fukuhara, A.; Nakamura, N.; Yoshikawa, H. Impact of dexamethasone concentration on cartilage tissue formation from human synovial derived stem cells in vitro. Cytotechnology 2018, 70, 819–829. [Google Scholar] [CrossRef]
- Kisiday, J.D. Expansion of chondrocytes for cartilage tissue engineering: A review of chondrocyte dedifferentiation and redifferentiation as a function of growth in expansion culture. Regen. Med. Front. 2020, 2, e200002. [Google Scholar] [CrossRef]
- Chen, Y.; Yu, Y.; Wen, Y.; Chen, J.; Lin, J.; Sheng, Z.; Zhou, W.; Sun, H.; An, C.; Chen, J.; et al. A high-resolution route map reveals distinct stages of chondrocyte dedifferentiation for cartilage regeneration. Bone Res. 2022, 10, 38. [Google Scholar] [CrossRef]
- Mandl, E.W.; van der Veen, S.W.; Verhaar, J.A.; van Osch, G.J. Serum-free medium supplemented with high-concentration FGF2 for cell expansion culture of human ear chondrocytes promotes redifferentiation capacity. Tissue Eng. 2002, 8, 573–580. [Google Scholar] [CrossRef]
- Gaissmaier, C.; Fritz, J.; Krackhardt, T.; Flesch, I.; Aicher, W.K.; Ashammakhi, N. Effect of human platelet supernatant on proliferation and matrix synthesis of human articular chondrocytes in monolayer and three-dimensional alginate cultures. Biomaterials 2005, 26, 1953–1960. [Google Scholar] [CrossRef]
- Hildner, F.; Eder, M.J.; Hofer, K.; Aberl, J.; Redl, H.; van Griensven, M.; Gabriel, C.; Peterbauer-Scherb, A. Human platelet lysate successfully promotes proliferation and subsequent chondrogenic differentiation of adipose-derived stem cells: A comparison with articular chondrocytes. J. Tissue Eng. Regen. Med. 2015, 9, 808–818. [Google Scholar] [CrossRef]
- Sykes, J.G.; Kuiper, J.H.; Richardson, J.B.; Roberts, S.; Wright, K.T.; Kuiper, N.J. Impact of human platelet lysate on the expansion and chondrogenic capacity of cultured human chondrocytes for cartilage cell therapy. Eur. Cell Mater. 2018, 35, 255–267. [Google Scholar] [CrossRef]
- Rikkers, M.; Levato, R.; Malda, J.; Vonk, L.A. Importance of timing of platelet lysate-supplementation in expanding or redifferentiating human chondrocytes for chondrogenesis. Front. Bioeng. Biotechnol. 2020, 8, 804. [Google Scholar] [CrossRef]
- Philippe, V.; Laurent, A.; Abdel-Sayed, P.; Hirt-Burri, N.; Applegate, L.A.; Martin, R. Human platelet lysate as an alternative to autologous serum for human chondrocyte clinical use. Cartilage 2021, 13, 509S–518S. [Google Scholar] [CrossRef]
- Kachroo, U.; Zachariah, S.M.; Thambaiah, A.; Tabasum, A.; Livingston, A.; Rebekah, G.; Srivastava, A.; Vinod, E. Comparison of human platelet lysate versus fetal bovine serum for expansion of human articular cartilage-derived chondroprogenitors. Cartilage 2021, 13, 107S–116S. [Google Scholar] [CrossRef]
- Liau, L.L.; Hassan, M.N.F.b.; Tang, Y.L.; Ng, M.H.; Law, J.X. Feasibility of human platelet lysate as an alternative to fetal bovine serum for in vitro expansion of chondrocytes. Int. J. Mol. Sci. 2021, 22, 1269. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.C.; Bertram, T.A.; Tawil, B.; Hellman, K.B. Hurdles in tissue engineering/regenerative medicine product commercialization: A survey of North American academia and industry. Tissue Eng. Part A 2011, 17, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.D.; Siston, R.A.; Brophy, R.H.; Lattermann, C.; Carey, J.L.; Flanigan, D.C. Failures, re-operations, and complications after autologous chondrocyte implantation--A systematic review. Osteoarthr. Cart. 2011, 19, 779–791. [Google Scholar] [CrossRef] [PubMed]
- Pearce, K.F.; Hildebrandt, M.; Greinix, H.; Scheding, S.; Koehl, U.; Worel, N.; Apperley, J.; Edinger, M.; Hauser, A.; Mischak-Weissinger, E.; et al. Regulation of advanced therapy medicinal products in Europe and the role of academia. Cytotherapy 2014, 16, 289–297. [Google Scholar] [CrossRef]
- Ikawa, T.; Yano, K.; Watanabe, N.; Masamune, K.; Yamato, M. Non-clinical assessment design of autologous chondrocyte implantation products. Regen. Ther. 2015, 1, 98–108. [Google Scholar] [CrossRef]
- Ramezankhani, R.; Torabi, S.; Minaei, N.; Madani, H.; Rezaeiani, S.; Hassani, S.N.; Gee, A.P.; Dominici, M.; Silva, D.N.; Baharvand, H.; et al. Two decades of global progress in authorized advanced therapy medicinal products: An emerging revolution in therapeutic strategies. Front. Cell Develop. Biol. 2020, 8, 547653. [Google Scholar] [CrossRef]
- Niethammer, T.R.; Gallik, D.; Chevalier, Y.; Holzgruber, M.; Baur-Melnyk, A.; Müller, P.E.; Pietschmann, M.F. Effect of the defect localization and size on the success of third-generation autologous chondrocyte implantation in the knee joint. Internat. Orthop. 2021, 45, 1483–1491. [Google Scholar] [CrossRef]
- Nordberg, R.C.; Otarola, G.A.; Wang, D.; Hu, J.C.; Athanasiou, K.A. Navigating regulatory pathways for translation of biologic cartilage repair products. Sci. Transl. Med. 2022, 14, eabp8163. [Google Scholar] [CrossRef]
- Laurent, A.; Hirt-Burri, N.; Scaletta, C.; Michetti, M.; de Buys Roessingh, A.S.; Raffoul, W.; Applegate, L.A. Holistic approach of Swiss fetal progenitor cell banking: Optimizing safe and sustainable substrates for regenerative medicine and biotechnology. Front. Bioeng. Biotechnol. 2020, 8, 557758. [Google Scholar] [CrossRef]
- Laurent, A.; Abdel-Sayed, P.; Ducrot, A.; Hirt-Burri, N.; Scaletta, C.; Jaccoud, S.; Nuss, K.; de Buys Roessingh, A.S.; Raffoul, W.; Pioletti, D.P.; et al. Development of standardized fetal progenitor cell therapy for cartilage regenerative medicine: Industrial transposition and preliminary safety in xenogeneic transplantation. Biomolecules 2021, 11, 250. [Google Scholar] [CrossRef]
- Abdel-Sayed, P.; Darwiche, S.E.; Kettenberger, U.; Pioletti, D.P. The role of energy dissipation of polymeric scaffolds in the mechanobiological modulation of chondrogenic expression. Biomaterials 2014, 35, 1890–1897. [Google Scholar] [CrossRef]
- Nasrollahzadeh, N.; Applegate, L.A.; Pioletti, D.P. Development of an effective cell seeding technique: Simulation, implementation, and analysis of contributing factors. Tissue Eng. Part C 2017, 23, 485–496. [Google Scholar] [CrossRef]
- Nasrollahzadeh, N.; Karami, P.; Wang, J.; Bagheri, L.; Guo, Y.; Abdel-Sayed, P.; Laurent-Applegate, L.; Pioletti, D.P. Temperature evolution following joint loading promotes chondrogenesis by synergistic cues via calcium signaling. eLife 2022, 11, e72068. [Google Scholar] [CrossRef]
- Studer, D.; Cavalli, E.; Formica, F.A.; Kuhn, G.A.; Salzmann, G.; Mumme, M.; Steinwachs, M.R.; Applegate, L.A.; Maniura-Weber, K.; Zenobi-Wong, M. Human chondroprogenitors in alginate-collagen hybrid scaffolds produce stable cartilage in vivo. J. Tissue Eng. Regen. Med. 2017, 11, 3014–3026. [Google Scholar] [CrossRef]
- Cavalli, E.; Fisch, P.; Formica, F.A.; Gareus, R.; Linder, T.; Applegate, L.A.; Zenobi-Wong, M. A comparative study of cartilage engineered constructs in immunocompromised, humanized and immunocompetent mice. J. Immunol. Regen. Med. 2018, 2, 36–46. [Google Scholar] [CrossRef]
- Levinson, C.; Lee, M.; Applegate, L.A.; Zenobi-Wong, M. An injectable heparin-conjugated hyaluronan scaffold for local delivery of transforming growth factor β1 promotes successful chondrogenesis. Acta Biomater. 2019, 99, 168–180. [Google Scholar] [CrossRef]
- Li, F.; Levinson, C.; Truong, V.X.; Laurent-Applegate, L.A.; Maniura-Weber, K.; Thissen, H.; Forsythe, J.F.; Zenobi-Wong, M.; Frith, J.E. Microencapsulation improves chondrogenesis in vitro and cartilaginous matrix stability in vivo compared to bulk encapsulation. Biomater. Sci. 2020, 8, 1711–1725. [Google Scholar] [CrossRef]
- Tosoratti, E.; Fisch, P.; Taylor, S.; Laurent-Applegate, L.A.; Zenobi-Wong, M. 3D-printed reinforcement scaffolds with targeted biodegradation properties for the tissue engineering of articular cartilage. Adv. Healthc. Mat. 2021, 10, e2101094. [Google Scholar] [CrossRef]
- Lee, S.J.; Oh, H.J.; Truong, M.D.; Lee, K.B.; Kim, J.; Kim, Y.J.; Park, S.R.; Min, B.H. Therapeutic possibility of human fetal cartilage-derived progenitor cells in rat arthritis model. Tissue Eng. Regen. Med. 2015, 12, 147–154. [Google Scholar] [CrossRef]
- Choi, W.H.; Kim, H.R.; Lee, S.J.; Jeong, N.; Park, S.R.; Choi, B.H.; Min, B.H. Fetal cartilage-derived cells have stem cell properties and are a highly potent cell source for cartilage regeneration. Cell Transplant. 2016, 25, 449–461. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Kim, J.; Park, S.R.; Park, D.Y.; Kim, Y.J.; Choi, B.H.; Min, B.H. Comparison of fetal cartilage-derived progenitor cells isolated at different developmental stages in a rat model. Dev. Growth Diff. 2016, 58, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Ribitsch, I.; Mayer, R.L.; Egerbacher, M.; Gabner, S.; Kańduła, M.M.; Rosser, J.; Haltmayer, E.; Auer, U.; Gültekin, S.; Huber, J.; et al. Fetal articular cartilage regeneration versus adult fibrocartilaginous repair: Secretome proteomics unravels molecular mechanisms in an ovine model. Dis. Mod. Mech. 2018, 11, dmm033092. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.R.; Kim, J.; Park, S.R.; Min, B.H.; Choi, B.H. Characterization of human fetal cartilage progenitor cells during long-term expansion in a xeno-free medium. Tissue Eng. Regen. Med. 2018, 15, 649–659. [Google Scholar] [CrossRef]
- Dasargyri, A.; Reichmann, E.; Moehrlen, U. Bio-engineering of fetal cartilage for in utero spina bifida repair. Ped. Surg. Int. 2020, 36, 25–31. [Google Scholar] [CrossRef]
- Park, D.Y.; Min, B.H.; Park, S.R.; Oh, H.J.; Truong, M.D.; Kim, M.; Choi, J.Y.; Park, I.S.; Choi, B.H. Engineered cartilage utilizing fetal cartilage-derived progenitor cells for cartilage repair. Sci. Rep. 2020, 10, 5722. [Google Scholar] [CrossRef]
- Park, I.S.; Kim, B.K.; Truong, M.D.; Yang, H.S.; Park, S.H.; Park, H.S.; Choi, B.H.; Won, B.H.; Min, B.H. Corneal repair with adhesive cell sheets of fetal cartilage-derived stem cells. Tissue Eng. Regen. Med. 2021, 18, 187–198. [Google Scholar] [CrossRef]
- Rikkers, M.; Korpershoek, J.V.; Levato, R.; Malda, J.; Vonk, L.A. The clinical potential of articular cartilage-derived progenitor cells: A systematic review. NPJ Regen. Med. 2022, 7, 2. [Google Scholar] [CrossRef]
- Kim, J.; Tran, A.N.; Lee, J.Y.; Park, S.H.; Park, S.R.; Min, B.H.; Choi, B.H. Human fetal cartilage-derived progenitor cells exhibit anti-inflammatory effect on IL-1β-mediated osteoarthritis phenotypes in vitro. Tissue Eng. Regen. Med. 2022, 19, 1237–1250. [Google Scholar] [CrossRef]
- Lee, K.H.; Song, S.U.; Hwang, T.S.; Yi, Y.; Oh, I.S.; Lee, J.Y.; Choi, K.B.; Choi, M.S.; Kim, S.J. Regeneration of hyaline cartilage by cell-mediated gene therapy using transforming growth factor beta 1-producing fibroblasts. Hum. Gene Ther. 2001, 12, 1805–1813. [Google Scholar] [CrossRef]
- Song, S.U.; Cha, Y.D.; Han, J.U.; Oh, I.S.; Choi, K.B.; Yi, Y.; Hyun, J.P.; Lee, H.Y.; Chi, G.F.; Lim, C.L.; et al. Hyaline cartilage regeneration using mixed human chondrocytes and transforming growth factor-beta1- producing chondrocytes. Tissue Eng. 2005, 11, 1516–1526. [Google Scholar] [CrossRef]
- Yi, Y.; Choi, K.B.; Lim, C.L.; Hyun, J.P.; Lee, H.Y.; Lee, K.B.; Yun, L.; Ayverdi, A.; Hwang, S.; Yip, V.; et al. Irradiated human chondrocytes expressing bone morphogenetic protein 2 promote healing of osteoporotic bone fracture in rats. Tissue Eng. Part A 2009, 15, 2853–2863. [Google Scholar] [CrossRef]
- Noh, M.J.; Copeland, R.O.; Yi, Y.; Choi, K.B.; Meschter, C.; Hwang, S.; Lim, C.L.; Yip, V.; Hyun, J.P.; Lee, H.Y.; et al. Pre-clinical studies of retrovirally transduced human chondrocytes expressing transforming growth factor-beta-1 (TG-C). Cytotherapy 2010, 12, 384–393. [Google Scholar] [CrossRef]
- Lee, B. INVOSSA, a first-in-class of cell and gene therapy for osteoarthritis treatment: The phase III trial. Osteoarthr. Cart. 2018, 26, S43–S44. [Google Scholar] [CrossRef]
- Evans, C.H. The vicissitudes of gene therapy. Bone Jt. Res. 2019, 8, 469–471. [Google Scholar] [CrossRef]
- Evans, C.H.; Ghivizzani, S.C.; Robbins, P.D. Getting arthritis gene therapy into the clinic. Nat. Rev. Rheumatol. 2011, 7, 244–249. [Google Scholar] [CrossRef]
- Kim, M.K.; Ha, C.W.; In, Y.; Cho, S.D.; Choi, E.S.; Ha, J.K.; Lee, J.H.; Yoo, J.D.; Bin, S.I.; Choi, C.H.; et al. A multicenter, double-blind, phase III clinical trial to evaluate the efficacy and safety of a cell and gene therapy in knee osteoarthritis patients. Hum. Gene Ther. 2018, 29, 48–59. [Google Scholar] [CrossRef]
- European Directorate for the Quality of Medicines & Healthcare. European Committee (Partial Agreement) on organ transplantation (CD-P-TO). In Guide to the Quality and Safety of Tissues and Cells for Human Application, 4th ed.; EDQM: Strasbourg, France, 2019; ISBN 978-92-871-8945-5. [Google Scholar]
- European Medicines Agency. ICH Topic Q 5 A (R1) Quality of Biotechnological Products: Viral Safety Evaluation of Biotechnology Products Derived from Cell Lines of Human or Animal Origin; CPMP/ICH/295/95; EMEA: London, UK, 1997. [Google Scholar]
- European Directorate for the Quality of Medicines & Healthcare. General Chapter 5.2.3. Cell substrates for the production of vaccines for human use. In European Pharmacopoeia 11.0; EDQM: Strasbourg, France, 2023. [Google Scholar]
- Broguiere, N.; Cavalli, E.; Salzmann, G.M.; Applegate, L.A.; Zenobi-Wong, M. Factor XIII cross-linked hyaluronan hydrogels for cartilage tissue engineering. ACS Biomat. Sci. Eng. 2016, 2, 2176–2184. [Google Scholar] [CrossRef]
- European Medicines Agency. EPAR Summary for the Public–MACI Matrix Applied Characterised Autologous Cultured Chondrocytes; EMA/282918/2013; EMEA: London, UK, 2013. [Google Scholar]
- Vonk, L.A.; Roël, G.; Hernigou, J.; Kaps, C.; Hernigou, P. Role of matrix-associated autologous chondrocyte implantation with spheroids in the treatment of large chondral defects in the knee: A systematic review. Int. J. Mol. Sci. 2021, 22, 7149. [Google Scholar] [CrossRef]
- Cottle, C.; Porter, A.P.; Lipat, A.; Turner-Lyles, C.; Nguyen, J.; Moll, G.; Chinnadurai, R. Impact of cryopreservation and freeze-thawing on therapeutic properties of mesenchymal stromal/stem cells and other common cellular therapeutics. Curr. Stem Cell Rep. 2022, 8, 72–92. [Google Scholar] [CrossRef]
- Ferruzzi, A.; Buda, R.; Faldini, C.; Vannini, F.; Di Caprio, F.; Luciani, D.; Giannini, S. Autologous chondrocyte implantation in the knee joint: Open compared with arthroscopic technique. Comparison at a minimum follow-up of five years. J. Bone Jt. Surg. 2008, 90, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Brun, P.; Dickinson, S.C.; Zavan, B.; Cortivo, R.; Hollander, A.P.; Abatangelo, G. Characteristics of repair tissue in second-look and third-look biopsies from patients treated with engineered cartilage: Relationship to symptomatology and time after implantation. Arthritis Res. Ther. 2008, 10, R132. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, A.; Kon, E.; Berruto, M.; Filardo, G.; Delcogliano, M.; Boldrini, L.; Bathan, L.; Marcacci, M. Patellofemoral full-thickness chondral defects treated with second-generation autologous chondrocyte implantation: Results at 5 years’ follow-up. Am. J. Sport. Med. 2009, 37, 1083–1092. [Google Scholar] [CrossRef] [PubMed]
- Kon, E.; Di Martino, A.; Filardo, G.; Tetta, C.; Busacca, M.; Iacono, F.; Delcogliano, M.; Albisinni, U.; Marcacci, M. Second-generation autologous chondrocyte transplantation: MRI findings and clinical correlations at a minimum 5-year follow-up. Eur. J. Radiol. 2011, 79, 382–388. [Google Scholar] [CrossRef]
- Aldrian, S.; Zak, L.; Wondrasch, B.; Albrecht, C.; Stelzeneder, B.; Binder, H.; Kovar, F.; Trattnig, S.; Marlovits, S. Clinical and radiological long-term outcomes after matrix-induced autologous chondrocyte transplantation: A prospective follow-up at a minimum of 10 years. Am. J. Sport. Med. 2014, 42, 2680–2688. [Google Scholar] [CrossRef]
- Wondrasch, B.; Risberg, M.A.; Zak, L.; Marlovits, S.; Aldrian, S. Effect of accelerated weightbearing after matrix-associated autologous chondrocyte implantation on the femoral condyle: A prospective, randomized controlled study presenting MRI-based and clinical outcomes after 5 years. Am. J. Sport. Med. 2015, 43, 146–153. [Google Scholar] [CrossRef]
- Ebert, J.R.; Fallon, M.; Wood, D.J.; Janes, G.C. A prospective clinical and radiological evaluation at 5 years after arthroscopic matrix-induced autologous chondrocyte implantation. Am. J. Sport. Med. 2017, 45, 59–69. [Google Scholar] [CrossRef]
- Brittberg, M.; Recker, D.; Ilgenfritz, J.; Saris, D.B.F.; SUMMIT Extension Study Group. Matrix-applied characterized autologous cultured chondrocytes versus microfracture: Five-year follow-up of a prospective randomized trial. Am. J. Sport. Med. 2018, 46, 1343–1351. [Google Scholar] [CrossRef]
- Ibarra, C.; Villalobos, E.; Madrazo-Ibarra, A.; Velasquillo, C.; Martinez-Lopez, V.; Izaguirre, A.; Olivos-Meza, A.; Cortes-Gonzalez, S.; Perez-Jimenez, F.J.; Vargas-Ramirez, A.; et al. Arthroscopic matrix-assisted autologous chondrocyte transplantation versus microfracture: A 6-year follow-up of a prospective randomized trial. Am. J. Sport. Med. 2021, 49, 2165–2176. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).