Abstract
Background/Objectives: The presence of postmortem pink teeth is a phenomenon occasionally observed during forensic autopsies. This phenomenon has been typically associated with deaths involving drowning, asphyxiation, trauma, or electrocution. However, the recent literature suggests that it is nonspecific. Despite being recognized in forensic literature for decades, its pathophysiology, prevalence, and forensic relevance remain controversial. The existing evidence is scattered and primarily based on case reports, narrative reviews, or isolated observations. This scoping review aims to systematically map the available scientific evidence on the phenomenon of postmortem pink teeth and its potential role in determining the cause of death within the context of forensic medicine. Methods: This review was conducted following the Joanna Briggs Institute (JBI) methodology for scoping reviews and reported according to the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) guidelines. Results: A comprehensive search was carried out across multiple databases to identify studies addressing the occurrence, mechanisms, and forensic interpretation of pink teeth in postmortem examinations. After application of the inclusion and exclusion criteria, the search allowed for the selection of 12 publications (case reports and observational studies). Conclusions: Collected data from the selected studies allowed us to conclude that PTP is a nonspecific taphonomic artifact, lacking diagnostic value in determining the cause of death. Mapping the current evidence on pink teeth contributed to a better understanding of this phenomenon and its lack of forensic significance, promoting more informed decision-making in postmortem assessments.
1. Introduction
Forensic dentistry is a specialised field of dentistry that plays a vital role in identifying victims and analysing circumstances of death, especially when other methods of identification are inadequate or impossible [1]. Due to their resistance to decomposition and capacity to endure extreme conditions, such as high temperatures and the effects of decomposing agents, teeth have become a dependable source of forensic evidence [2,3]. This resilience makes teeth among the most crucial structures used in homicide investigations, mass disasters, and other scenarios requiring human identification. Forensic dentistry encompasses various areas, including the comparison of dental records, analysis of bite marks, and assessment of dental conditions to estimate the postmortem (PM) interval, among others [1,4].
Within this area, one of the most intriguing and least understood phenomena is the pink tooth phenomenon,” a pink colouration that appears in the dentine of PM teeth.
The pink tooth phenomenon refers to a postmortem discolouration of the tooth crown or root, in which the dental hard tissues acquire a pink-to-reddish hue. Clinically, it appears as a diffuse or localized pink coloration visible through enamel or dentin. Histologically, this change results from the diffusion of haemoglobin breakdown products from decomposing pulp tissues into the dentinal tubules, often facilitated by increased intrapulpal pressure during early stages of decomposition. This phenomenon was first described by Beeley and Harvey [5], who observed that some human teeth had a characteristic pink hue, visible mainly in the anterior teeth. Since then, several studies, such as those by Brøndum and Simonsen [6] and Van Wyk [7], have tried to understand the causes and mechanisms underlying this colouration. The presence of pink teeth has been linked to different causes of death, such as asphyxia, drowning, and head trauma. It is generally understood as a sign that there was some pathological change inside the PM dental pulp.
This phenomenon occurs mainly in conditions where there is increased intrapulpal pressure or when internal bleeding occurs. The most widely accepted histological explanation for the phenomenon is that haemoglobin, or other blood components, infiltrates the PM dentinal tubules, resulting in the pink colouration observed. Studies such as those by Ortmann and DuChesne [8] and Franco et al. [3] suggest that the presence of this phenomenon may be related to cadaveric decomposition and the deterioration of blood cells in the circulatory system, but there is also evidence that factors such as cause of death may influence its occurrence. Thus, although the “pink tooth” is a rare phenomenon, a historical hypothesis suggests that this phenomenon might be of considerable value in forensic medicine [9], as it can provide clues about the cause of death and the time elapsed since death. In cases of death by asphyxiation, drowning, or trauma, for example, observation of the phenomenon can help establish the cause or confirm the suspected cause of death. However, despite its potential diagnostic value, forensic literature still debates the specificity of the phenomenon and its relationship with the cause of death, since not all corpses in similar circumstances present this alteration [10,11]. Furthermore, although pink teeth may be indicative of decomposition, their presence cannot always be considered conclusive evidence of a specific cause of death, raising questions about their practical applicability in forensic investigations [10].
A recent narrative review by Braga et al. [12] on the forensic significance of postmortem pink teeth confirms the long-standing view in the literature that the phenomenon is primarily caused by the infiltration of haemoglobin into the dentinal tubules. The authors corroborate that environmental factors, particularly humidity and the decomposition stage, play a more significant role in the appearance of pink teeth than the specific cause of death. This aligns with the fragmented and often anecdotal evidence mentioned in our protocol, where a definitive link to the cause of death remains elusive. However, the work of Braga et al., being a narrative review, differs methodologically from our proposed scoping review, which will employ a systematic, reproducible, and comprehensive search strategy to map the entirety of available evidence, including grey literature, as per the JBI and PRISMA-ScR guidelines. While the conclusions of Braga et al. reinforce the current understanding, they also highlight the existing knowledge gaps and the lack of consensus, thereby underscoring the necessity for a systematic scoping review to clarify the true forensic value of this phenomenon.
A scoping review was chosen because the aim is to map the breadth and characteristics of existing evidence, rather than assess the quality or effectiveness of interventions. This approach is suitable for emerging, conceptually diverse, or fragmented fields, as it accommodates a wide range of study designs and sources. It provides the flexibility and comprehensive overview needed to address exploratory research questions—something a fully systematic quantitative review, which requires comparable studies for synthesis, cannot offer. Thus, the goal of this scoping review is to map the occurrence, histological mechanisms, and environmental determinants of the pink teeth phenomenon in the context of autopsies and forensic investigations.
2. Materials and Methods
For the development of this scoping review, a research protocol was developed in accordance with the Joanna Briggs Institute (JBI) model [13,14,15], which emphasize the relevance and coverage of sources rather than prescribing a minimum number of databases. This led to the formulation of the following question: what evidence describes the occurrence and mechanisms of pink teeth, and in what conditions can they have limited, context-dependent forensic relevance? Thus, the PCC acronym used was: population (P), humans; concept (C), tooth discolouration; and context (C), postmortem changes.
The methodology applied was based on a search of scientific articles without time restrictions. The databases used in this study were PubMed, ScienceDirect, and Medline (via BVS). The databases chosen constitute the primary and most authoritative repositories for the topic under investigation, ensuring broad access to peer-reviewed studies central to this field. In addition, the search strategy was strengthened through secondary search techniques recommended by JBI, including reference list screening and citation tracking, which further mitigated the risk of missing pertinent literature not indexed in the selected databases. Taken together, this approach provides a comprehensive and methodologically robust search strategy appropriate to the scope and aims of the scoping review. The MeSH terms applied were (humans AND (tooth discolouration)) AND Postmortem Changes). The search using the keyword “tooth discolouration” was used to broaden the search and enable to find more articles without narrowing the scope of the search, even though our focus was on pink teeth. The articles were selected using Rayyan after being retrieved from the above databases. The software developer is Rayyan Systems Inc. of Cambridge, MA, USA. For the final review, the items identified in the reports prepared for the guidance of systematic reviews and meta-analysis extensions (PRISMA-ScR) [16] were used, and the PRISMA checklist (Table S1) was followed. The protocol for this scoping review was registered with the OSF (https://osf.io/8qw2b/, accessed on the 23 September 2025). No deviations from the established protocol were required.
2.1. Inclusion and Exclusion Criteria
All articles directly addressing the phenomenon of “pink tooth” in the context of forensic dentistry were included in this review. The selection considered studies in humans, published in English, Portuguese, Spanish, or French, with no restrictions on time or type of publication. No filters were applied regarding the methodological design of the studies, provided that the content was relevant to the objective of this review.
On the other hand, articles that did not address the proposed topic were excluded. Experimental studies conducted on animal models and publications that mentioned “pink teeth” but did so in a superficial manner or without relevance to forensic practice were also excluded.
2.2. Search Strategy
Selection of articles was performed according to Peer Review of Electronic Search Strategies (PRESS) [17].
A preliminary search was conducted on 13 January 2025 in the selected databases to identify the keywords and index terms used in publications related to the topic. This allowed the development of the search strategy for each database presented in Table 1.

Table 1.
Strategy of the bibliographic research carried out.
After completing the bibliographic search and publications selection, the reference lists of all included articles were reviewed to identify potential additional articles for inclusion. After the search, the identified articles were imported into the EndNote program. The results of the electronic search were exported to Rayyan® [18], and duplicates were removed. The selection of articles was done manually. Rayyan® was used as a support tool and only to gather all the articles found in the different databases described above and identify duplicates.
2.3. Articles Selection, Analysis, and Presentation of Data
The preliminary selection was carried out by two independent reviewers, who began by analysing the title/abstract of the articles and then the full text. After this analysis, 5% of the total articles were used to obtain at least 85% consensus among the reviewers. In the next stage of the research, 2% of the full-text articles were used to obtain the same level of agreement.
Once the necessary consensus was reached, the full selection process proceeded. The same two reviewers independently assessed all titles and abstracts based on the predefined inclusion criteria. The full texts of potentially relevant studies were then retrieved according to JBI guidelines. Any discrepancies between the two reviewers were resolved through discussion with a third reviewer. The article selection process is illustrated using the PRISMA 2020 flowchart (Figure 1).
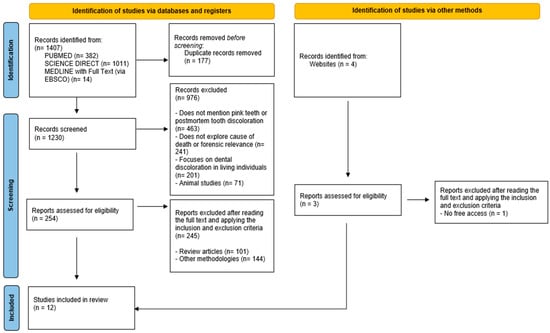
Figure 1.
Flowchart of the article selection process adapted from the PRISMA 2000 flow diagram [16].
After reading the full articles included in this review, data were extracted according to the objectives and research questions of this review, including the following relevant information: title, author(s), year of publication, type of study, objective(s), and results, as included in Lopes Cardoso et al. [19].
In the first phase, filters were applied to the search, resulting in a total of 1407 articles. Of these, 177 duplicates were identified and eliminated. The 1230 articles obtained were initially screened only by reading the title and abstract, which led to the exclusion of 976, for the reasons shown in Figure 1.
A total of 254 articles were selected for full reading, 245 of which were eliminated, and 9 publications were selected. In addition, 4 articles were identified through a citation search, 1 of which was rejected because it was not freely accessible. At the end of this selection process, 12 articles were found and included in this scoping review (Figure 1).
3. Results
A careful content analysis was carried out, which was subsequently systematised according to the following axes: study objective, methodology, and results.
During the analysis of the forensic cases studied, the phenomenon known as postmortem pink tooth (PTP) was observed in multiple corpses of different ages, sexes, and causes of death. The pink discolouration was identified in both deciduous and permanent teeth, involving anterior and posterior teeth in the maxilla and mandible. In 18 cases (13 women and five men), the presence of pink discolouration on the teeth was documented. In some of these cases, the colouring also extended to the nails, suggesting a possible systemic pattern associated with decomposition. This colouring was particularly evident in corpses found in humid and warm environments, conditions that favour putrefaction and the formation of compounds related to autolysis [2].
An increased incidence of PTP has been reported in younger individuals [2], possibly due to the greater permeability of the root canals, facilitating the penetration of haemoglobin-derived pigments. Haemoglobin and its derivatives are believed to be primarily responsible for the pigmentation observed, forming unstable complexes within the tooth structure. Histological analyses revealed significant changes in the dental pulp, including vascular congestion, the presence of haematic pigments, cell disintegration, fibrosis and progressive calcification, and decreased vascularisation [7]. Pink discolouration was observed more frequently in situations involving blood accumulation in the cephalic region, such as inverted PM position or submersion in water [6]. In some cases, particularly in victims of asphyxia, a relationship has been suggested between the pink colouration of the pulp chambers and increased intracranial pressure, which could have caused intrapulpal microhaemorrhages [20]. However, not all cases of asphyxia present PTP [11]. Among 21 victims of asphyxia, only one case presented pink discolouration in the teeth, which reinforces the non-specific nature of this phenomenon [11]. The included studies suggest that, although PTP may be present in cases of death by asphyxia, head trauma, firearm injuries, hypothermia, and poisoning, its presence cannot be considered conclusive for any particular cause of death.
Furthermore, it has been confirmed that discolouration occurs after death and should be distinguished from other dental changes or signs of trauma during life [20]. Histological analysis suggests that PTP may be a PM manifestation associated with biochemical decomposition processes [1].
The classic article by Beeley and Harvey [5] was one of the first to describe in detail the occurrence of pink-coloured teeth in corpses, relating the phenomenon to blood infiltration into the dentinal tubules, especially in cases of violent death or prolonged submersion. The objective was then to elucidate the biochemical and histological origin of this pink colouration by attempting to differentiate between physical and internal causes. Teeth from several corpses in various states of decomposition were analysed. It was noted that the pink colouring was attributed to the presence of haemoglobin-derived pigments that had diffused from the pulp to the dentinal tubules PM, meaning that these pigments were not only found in the pulp canal. It can be said that humidity favours the phenomenon. The possible presence of carboxyhaemoglobin was also detected, suggesting that the colouring could be associated with the amount of carbon dioxide present in the blood. The phenomenon is more common in bodies in an advanced state of decomposition, especially when the environment is humid and anaerobic, which facilitates haemolysis and the release of haemoglobin. Anterior teeth, such as upper incisors and canines, showed a higher frequency of discolouration, possibly due to their structure and pulp irrigation. This hypothesis was later reinforced by Borrman et al. [21], who associated the phenomenon with haemolysis and advanced decomposition, pointing to the frequent presence of root dentine discolouration, especially in anterior teeth. A study involving 62 cases was conducted, documenting the presence or absence of pink teeth. Aspects such as cause of death, putrefaction, type of teeth, location of remains, and environmental conditions were compared. As in Beeley and Harvey [5], it was observed that this phenomenon occurred largely in upper anterior teeth and in bodies with a high state of decomposition located in humid or submerged environments. The presence of pink teeth was more common between 5 and 10 days PM, depending on environmental conditions.
Van Wyk [7] observed pink colouring not only in the anterior teeth, but also in the lower teeth. The colouring was more intense in the cervical region and in the root dentine, where the structure is more porous and closer to the pulp. This researcher found that the translucency of dentine favours the visualisation of pink colouring when properly illuminated, with the phenomenon being more frequent in bodies subjected to early putrefaction, especially in humid and warm environments, which accelerates the decomposition of soft tissues. The pink colouration was then attributed to the infiltration of haemoglobin and degradation products into the dentinal tubules. The dental pulp showed signs of autolysis.
Ortmann and DuChesne [8] also observed pink anterior teeth in a partially mummified body, as well as nails with the same colouration. The authors raised hypotheses such as the accumulation of porphyrins, haemoglobin degradation products, or chemical changes associated with decomposition.
Campobasso et al. [2] analysed the occurrence of PTP in bodies submerged in cold water with low oxygen content and moderate currents. In this study, pink teeth were also found in the upper incisors, varying in colour intensity and location, being more common in cervical and root dentine. The seawater temperature probably favoured slow putrefaction, allowing for a longer diffusion time of haematic pigments, facilitating this environment of internal pressure and anoxia and the extravasation of haemoglobin from the dental pulp.
The study by Soriano et al. [20] involved an adult cadaver in which pink discolouration was observed on the upper teeth. This discolouration occurred uniformly on both central and adjacent incisors. The analysis suggested that, upon death, the biochemical processes and the action of microorganisms that develop in the body may have directly influenced the teeth.
Charan Gowda et al. [4] described two clinical cases in which the teeth had a pink PM colouration. Both corpses were male, in an advanced state of decomposition, and had colouration on the upper incisors. The pink substance was observed in the inner layer of the dentine. Histology indicated that the colour change was caused by the presence of haemoglobin or derivatives that had infiltrated the dentine. The odontoblastic cells showed signs of degeneration, and there was infiltration of decomposition fluids into the dentinal tubules. The study indicated that this phenomenon is associated with autolysis and putrefaction.
Mittal et al. [1] included two cases, one involving an elderly woman who presented pink discolouration on her anterior teeth and the other involving a young man who presented discolouration on his posterior teeth, such as molars. What was observed was more pronounced discolouration on the anterior teeth. What was possible to ascertain was the possible cause: haemoglobin.
The study by Carrasco et al. [10] investigated the histological changes in dental pulp. In the teeth of bodies that had an PM interval of less than 24 h, the dental pulp was still relatively intact. However, as the PM interval increased, progressive necrosis of pulp cells was observed, with loss of cell integrity and changes in collagen fibres. Regarding inflammation and infiltration of inflammatory cells, the study observed that in bodies with a PM interval between 24 and 48 h, an infiltration of inflammatory cells (mainly leukocytes) was identified, especially in the more peripheral regions of the dental pulp. The presence of lymphocytes and macrophages indicated a moderate inflammatory response. With regard to dental calcification, in bodies with PM interval greater than 48 h, the formation of reparative dentine was observed in the pulp region, a natural defence process of the tooth to protect itself from infections. This phenomenon indicates an attempt at organic defence against cell death and bacterial action. Finally, regarding cell death and fibrous tissue formation, Carrasco et al. [10] documented that for corpses more than 5 days after death, the dental pulp was completely necrotic, replaced by fibrous tissue or a cavity filled with decomposition substances. This process was more evident in the teeth of bodies that had undergone advanced decomposition.
Franco et al. [3] identified the phenomenon of pink teeth in corpses with various causes of death, which supports the non-specificity of the aetiology. It was not possible to relate the colouration to hanging, drowning, or cranial haemorrhage. This study observed that this phenomenon occurs in the early-to-intermediate stages of decomposition and is related to autolysis and putrefaction of the dental pulp.
Brites et al. [11] conducted a retrospective study of 21 autopsied cases among children and adults. In this study, various forms of asphyxiation were found, such as drowning, manual strangulation, and hanging. A single case of PTP was confirmed in a 26-year-old male victim of hanging. Thus, this study concluded that PTP is highly non-specific, occurring occasionally, and therefore not reliable for differentiating causes of death by asphyxia.
Finally, Minegishi et al. [9] reviewed 324 autopsies on unidentified corpses. In 68 cases (21%), the PTP phenomenon was observed, with no significant difference between men and women. Furthermore, the location where the corpses were found did not influence the phenomenon. A greater tendency for pink teeth was observed in victims under the age of 60, with the anterior teeth being the most affected. No significant association was observed between pink teeth and the cause of death, leading to the conclusion that this phenomenon is non-specific.
Table 2 summarises the results observed in each of the selected articles.
Table 2.
Essential data taken from the selected publications.
4. Discussion
The phenomenon of pink teeth, PTP, a PM chromatic alteration that has intrigued the forensic community for decades, is at the heart of this research. Its elucidation is fundamental not only for understanding the taphonomic processes that affect human remains, but also for the correct interpretation of findings in a medico-legal context, where the distinction between antemortem pathophysiological phenomena and PM artifacts is imperative. The present scoping review aimed to map the scientific literature, integrating the results of multiple studies to unravel the biochemical and histological bases of PTP; investigate the environmental and anatomical factors that modulate its expression; and, crucially, assess its validity as an indicator of cause of death.
Since its detailed description in the article by Beeley and Harvey [5], the origin of PTP appearance has been deeply discussed. The central hypothesis, consistently reinforced over fifty years of research [1,4,7], attributes the pink colouration to the infiltration of haemoglobin-derived pigments into the dentinal tubules. The process begins with the cessation of PM blood circulation, leading to anoxia and subsequent autolysis of the dental pulp, a richly vascularised tissue. The lysis of erythrocytes (haemolysis) releases haemoglobin into the pulp chamber. Under favourable conditions, this molecule and its degradation products diffuse centrifugally from the pulp into the microstructural network of the dentine.
Beeley and Harvey [5] were pioneers in observing that these pigments were not confined to the pulp canal but permeated the dentine structure, a finding corroborated by subsequent histological analyses. Charan Gowda et al. [4], for example, described the presence of the pink substance in the inner layer of dentine in two cases of advanced decomposition cadavers, associating it with the degeneration of odontoblastic cells and the infiltration of decomposition fluids into the tubules. This observation is fundamental, as dentinal tubules, microscopic channels that extend from the pulp to the enamel–dentine and cemento–dentine junctions, function as passive diffusion pathways for haematic pigments after the loss of cell vitality.
The study by Carrasco et al. [10] provides a detailed chronology of the histological changes that create the substrate for PTP. At a PM interval of less than 24 h, the pulp maintains relative integrity. However, between 24 and 48 h, an inflammatory response begins, with leukocyte infiltration, followed, at PM intervals greater than 48 h, by processes of progressive necrosis and attempts at organic defence, such as the formation of reparative dentine. In more advanced stages (PM interval > 5 days), the pulp is completely necrotic and is often replaced by fibrous tissue or a mass of decomposition substances. It is in this scenario of tissue disintegration and loss of cellular integrity that the diffusion of haematic pigments into the porous dentine is maximised. Autolysis and subsequent putrefaction, driven by microbial action, as suggested by Soriano et al. [20], are therefore essential prerequisites for the manifestation of the phenomenon.
At the biochemical level, research by Beeley and Harvey [5] raised the hypothesis of the presence of carboxyhaemoglobin, suggesting a potential correlation between the colouration and the concentration of carbon dioxide in the blood at the time of death. This hypothesis, although interesting, lacks confirmation through further studies and remains in the realm of speculation. Similarly, Ortmann and DuChesne [8], observing similar colouration on the nails of a partially mummified body, proposed as the cause the accumulation of porphyrins, which are components of the haem group of haemoglobin. Both hypotheses emphasise that the exact identity of the chromophore may vary, involving not only intact haemoglobin but also its various metabolites generated during the decomposition process.
The manifestation of PTP is not universal, its occurrence being modulated by a complex interaction of extrinsic and intrinsic factors. The literature is unanimous in pointing to moisture as a prominent catalyst. Beeley and Harvey [5] were the first to note the strong association with prolonged submersion, an observation corroborated by almost all subsequent studies. Borrman et al. [21], Van Wyk [7], and Campobasso et al. [2] reinforced that humid, anaerobic, or submerged environments facilitate haemolysis and putrefaction, creating ideal conditions for the release and diffusion of haemoglobin. Moisture not only accelerates the decomposition of soft tissues, including pulp, but also keeps the dentinal structure permeable to pigment infiltration.
Temperature also plays a crucial role. Van Wyk [7] pointed out that warm, humid environments accelerate early putrefaction and, consequently, the onset of PTP. Conversely, the study by Campobasso et al. [2] on bodies submerged in cold water suggests that low temperatures, by promoting slower putrefaction, may paradoxically favour the phenomenon by allowing a longer period for the diffusion of haematic pigments before complete tissue disintegration. Additionally, these authors proposed that external water pressure and internal anoxia could facilitate the extravasation of haemoglobin from the pulp, a mechanism particularly relevant in cases of drowning.
The PM interval is another important variable. The study involving 62 cases [20] identified the most common window for PTP onset as being between 5 and 10 days PM, aligning with the early-to-intermediate stages of decomposition described by Franco et al. [3]. This period also aligns with the histological timeline of Carrasco et al. [10] that indicates complete pulp necrosis after 5 days. However, this timeframe is highly flexible and influenced by the environmental conditions mentioned earlier. Anatomically, there is a noticeable tendency for PTP to occur more often in anterior teeth, particularly upper incisors and canines [1,2,4,5,9,20]. Several hypotheses have been proposed to explain this pattern. Beeley and Harvey [5] suggested it might be due to the stronger structure and better pulp irrigation in these single-rooted teeth. Van Wyk [7] and Campobasso et al. [2] added that the increased porosity of dentine in the cervical and root areas, which are closer to the pulp chamber and may have thinner or no enamel, further explains this trend. The increased translucency of dentine in these zones, as Van Wyk [7] observed, also aids in visualising underlying staining. While the predilection for anterior teeth is evident, it is not exclusive. Van Wyk [7] reported the phenomenon in lower teeth, and Mittal et al. [1] documented a case in molars; however, the staining was more intense in the anterior teeth of the same individual. Age appears to play a role as well, with Minegishi et al. [9] noting a higher incidence among victims under 60 years old. The reason remains unclear, but it may be related to age-related changes in tooth structure, such as dentinal sclerosis.
The most critical issue surrounding PTP is undoubtedly its usefulness as a marker of the cause of death. The initial association made by Beeley and Harvey [5] between the phenomenon and violent deaths, such as drowning, strangulation, or intracranial haemorrhages, led to the hypothesis that antemortem cephalic vascular congestion could predispose to pulp haemorrhage and, consequently, to PTP. If confirmed, this hypothesis would give the finding significant diagnostic value in forensic medicine.
However, the overwhelming majority of evidence accumulated in the following decades not only failed to corroborate this specificity, but actively refuted it. More recent and methodologically robust studies have demonstrated that PTP is a nonspecific taphonomic phenomenon. Franco et al. [3] identified pink teeth in corpses with a wide variety of causes of death, failing to establish any statistical correlation with hanging, drowning, or cranial haemorrhage. Their conclusion was unequivocal: PTP is related to the processes of autolysis and putrefaction of the dental pulp, and not to the aetiology of death.
The retrospective study by Brites et al. [11] is particularly enlightening. When analysing 21 cases of death by asphyxiation (including drowning, strangulation, and hanging), the authors found only a single case of PTP in a male victim of hanging. The rarity of the finding in a cohort of cases where, according to the original hypothesis, it should be prevalent, led them to conclude that PTP is highly nonspecific and is not a reliable indicator for differentiating causes of death by asphyxia.
The comprehensive analysis conducted by Minegishi et al. [9] on 324 autopsies of unidentified corpses settled this issue conclusively. Although they observed PTP in 21% of cases, they found no significant association between the presence of pink teeth and the cause of death. Its occurrence was not influenced by the sex of the victim or the location where the corpse was found.
Therefore, the current scientific consensus differs substantially from the original hypothesis. PTP should be interpreted not as a pathognomonic sign of a specific cause of death, but rather as a PM artifact. Its presence informs the forensic investigator about the conditions of decomposition (namely, a humid environment), the state of degradation of the corpse, and the probable PM interval, but not about the circumstances that led to the individual’s death. It is imperative to recognise the limitations inherent in this analysis, which is based on a review of the existing literature. Firstly, the conclusions are intrinsically dependent on the methodological quality, rigour, and potential biases of the primary studies cited here. The heterogeneity between studies is considerable, ranging from single case reports to retrospective studies with samples of varying sizes. This diversity of study designs and sample sizes makes direct comparison and quantitative synthesis of results difficult.
Secondly, most studies are observational and retrospective in nature. Consequently, many of the environmental variables crucial to PTP development, such as exact temperature, humidity level, pH of the medium, and local microbiota, are not controlled or, in many cases, are insufficiently documented. This lack of control prevents the isolation of the effect of each variable, making it difficult to formulate a robust predictive model. Additionally, the possibility of publication bias cannot be ruled out, whereby studies reporting the presence of PTP (a positive finding) may be more likely to be published than those documenting its absence in similar circumstances. Such bias could lead to an overestimation of the prevalence of the phenomenon in the literature.
Finally, some ambiguity remains at the biochemical level. Although haemoglobin is accepted as the primary source of colouration, the exact chemical identity of the pigment(s) in dentine (e.g., definitive confirmation of carboxyhaemoglobin or porphyrins) remains speculative, as most studies have not used advanced analytical techniques for their characterisation.
Other limitations of this study are related to the methodology of scoping reviews. In fact, although this review followed the JBI guidelines and the PRISMA-ScR checklist, it still has some limitations, such as not having critically assessed the methodological quality of the included studies, making it impossible to consider the risk of bias and the reliability of the evidence. Furthermore, the number of chosen databases and the language restriction search, without a systematic search of grey literature or regional databases, may have led to publication bias and excluded important publications. The variety of study types selected (case studies, case series, and observational studies) also compromises the quantitative analysis, making it difficult to generalise the results found. Finally, the failure to consult experts in the process of selecting and interpreting the data collected may have limited the scope and practical applicability of the results.
The limitations identified open the way for several avenues of future research, which could deepen and refine knowledge about PTP:
- -
- Controlled experimental research: Conduct in vitro studies on extracted teeth to systematically isolate variables (e.g., temperature, humidity, pH, and oxygen) and quantify their effects on the formation, intensity, and timing of PTP.
- -
- Advanced biochemical characterisation: Use techniques such as HPLC, mass spectrometry, and Raman spectroscopy to definitively identify and quantify dentinal chromophores, resolving current uncertainty about pigment composition.
- -
- Prospective forensic data collection: Implement standardised, prospective studies in forensic settings to collect robust data on PTP occurrence, alongside cause of death, PMI, and environmental factors, strengthening statistical validity.
- -
- Age-related mechanisms: Investigate why PTP appears more frequently in younger individuals through comparative histological and biochemical analyses focusing on dentine structure and pulp characteristics.
- -
- Longitudinal and temporal analysis: Monitor PTP over time (e.g., in taphonomic facilities) to understand its onset, progression, and disappearance during decomposition.
A primary function of a scoping review is to identify knowledge gaps, and this study was no exception. The mapping made several areas in need of in-depth primary research evident, namely biochemical gap, experimental gap, gap in prospective data, and gap in age-related factors, as mentioned previously.
5. Conclusions
This study, conducted as a scoping review, covering various publications, from case reports to retrospective studies, allowed for the delineation of the current state of knowledge and the identification of gaps that will justify future research.
The mapping of the literature revealed a widespread consensus regarding the aetiology of PTP. Evidence from multiple histological and observational studies unequivocally points to a postmortem process initiated by autolysis and haemolysis of the dental pulp, resulting in the diffusion of haemoglobin and its derivatives into the dentinal tubules.
The analysis of collected data revealed that environmental and anatomical factors are consistently recognised as key modulators of the phenomenon. Humidity and submersion stand out as the most significant catalysts, a finding that is evident in nearly all of the documented literature. Similarly, evidence was found supporting an anatomical predisposition of anterior teeth, although the precise basis for this tendency (pulpal irrigation and dentinal porosity) remains a topic of theoretical debate.
One of the central findings of this review was the identification of a clear evolutionary trajectory in scientific thought regarding the forensic relevance of PTP. The mapping revealed that the early literature suggested a strong association with specific causes of death, such as asphyxia. However, the current body of literature, particularly large-scale retrospective studies, largely agrees on describing PTP as a nonspecific taphonomic artifact, lacking diagnostic value in determining the cause of death. In this way, PTP cannot be considered related to the cause of death. Its role, as supported by the available evidence, is mainly as an indicator of decomposition conditions.
The results of this review confirm that the initially set objectives were met: the existing literature was thoroughly mapped, offering a clear overview of the origin and development of knowledge on PTP. The cause of the phenomenon, commonly understood as a taphonomic process resulting from pulpal autolysis and haemolysis, and the factors that influence its expression are still not fully understood.
Concerning its validity as a forensic marker, recent evidence has challenged the initial diagnostic hypothesis, clarifying that PTP should not be used to determine the cause of death. Practically, this review emphasises the importance of caution when interpreting PTP in medico-legal contexts. So far, its presence should be seen as indicative of specific decomposition conditions, especially humidity and a prolonged postmortem interval, but not as a definitive indicator of cause of death. This distinction is vital to prevent misinterpretations and to maintain forensic objectivity. In this way, PTP should be routinely documented during dental examination, with detailed recording of its presence, distribution, and intensity as part of the overall postmortem findings. However, it must not be used in isolation to infer cause of death, postmortem interval, or specific environmental conditions, as it is a nonspecific phenomenon influenced by multiple variables and can lead to misleading conclusions. Any interpretive value should be considered only within a broader, multidisciplinary forensic context. Instead, it should always be evaluated alongside other autopsy findings, circumstantial evidence, and complementary analytical data to ensure accurate and defensible interpretations.
Based on the identified gaps, namely the absence of controlled experimental studies, the ongoing biochemical ambiguity, the lack of prospective data, and the limited exploration of age-related factors, it is recommended that laboratory investigations with standardised protocols be developed and implemented in forensic institutions. Pursuing these lines of research will contribute to a more comprehensive and detailed understanding of this fascinating postmortem artifact, consolidating the scientific basis for its interpretation in forensic contexts.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/forensicsci6020032/s1, Table S1. PRISMA 2020 checklist.
Author Contributions
Conceptualization, I.L.C., M.T.M., M.S., and M.I.G.; validation: I.L.C., M.T.M., and M.I.G.; literature search, I.L.C., M.T.M., M.S., and M.I.G.; writing—initial draft preparation, I.L.C., M.T.M., M.S., and M.I.G.; writing—editing, I.L.C., M.T.M., and M.I.G.; writing—final text revision, I.L.C., M.T.M., M.S., and M.I.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to (specify the reason for the restriction).
Acknowledgments
The authors wish to thank Fernando Pessoa University.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Mittal, S.; Mahajan, A.; Mittal, S. Pink teeth and the dead: A review with reports of two cases. J. Forensic Dent. Sci. 2016, 8, 112–115. [Google Scholar] [CrossRef]
- Campobasso, C.P.; Dell’Erba, A.S.; Di Vella, G. Pink teeth in a series of bodies recovered from a single shipwreck. J. Forensic Sci. 2006, 51, 636–638. [Google Scholar] [CrossRef] [PubMed]
- Franco, A.; Mendes, S.D.; Picoli, F.F.; Rodrigues, L.G.; Silva, R.F. Forensic thanatology and the pink tooth phenomenon: From the lack of relation with the cause of death to a potential evidence of cadaveric decomposition in dental autopsies—Case series. Forensic Sci. Int. 2018, 291, e8–e12. [Google Scholar] [CrossRef]
- Charan Gowda, B.K.; Nagarajappa, D.; Gopal, M.; Mehta, D.S. Histological appearance of postmortem pink teeth: Report of two cases. J. Forensic Dent. Sci. 2015, 7, 70–72. [Google Scholar] [CrossRef] [PubMed]
- Beeley, J.A.; Harvey, W. Pink teeth appearing as a post-mortem phenomenon. J. Forensic Sci. Soc. 1973, 13, 297–305. [Google Scholar] [CrossRef]
- Brøndum, L.; Simonsen, J. Postmortem red coloration of teeth. A retrospective investigation of 26 cases. Forensic Sci. Int. 1987, 34, 129–135. [Google Scholar] [CrossRef]
- Van Wyk, C.W. Pink teeth of the dead: 1. A clinical and histological description. J. Forensic Odontostomatol. 1987, 5, 41–50. [Google Scholar]
- Ortmann, C.; DuChesne, A. A partially mummified corpse with pink teeth and pink nails. Int. J. Legal Med. 1998, 111, 154–156. [Google Scholar] [CrossRef]
- Minegishi, T.; Furukawa, H.; Takayama, Y.; Sakurada, K. Sixty-eight cases of postmortem pink teeth observed in dental autopsies of unidentified cadavers. Forensic Sci. Int. 2022, 332, 111205. [Google Scholar] [CrossRef]
- Carrasco, P.; Lucena, J.; Andrade, C.; Martín-de-las-Heras, S. Histological transformations of the dental pulp as possible indicator of post-mortem interval: A pilot study. Forensic Sci. Int. 2017, 279, 159–165. [Google Scholar] [CrossRef]
- Brites, A.N.; Rezende Machado, A.L.; Franco, A.; Alves da Silva, R.H. Revisiting autopsies of death by mechanical asphyxia in the search for post-mortem pink teeth. J. Forensic Odontostomatol. 2020, 38, 34–38. [Google Scholar] [PubMed]
- Braga, S.; Caldas, I.M.; Dinis-Oliveira, R.J. Forensic significance of postmortem pink teeth: A narrative review. Arch. Oral. Biol. 2025, 169, 106092. [Google Scholar] [CrossRef]
- Pearson, A.; Wiechula, R.; Court, A.; Lockwood, C. The JBI model of evidence-based healthcare. Int. J. Evid. Based Healthc. 2005, 3, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Pearson, A.; Jordan, Z.; Munn, Z. Translational science and evidence-based healthcare: A clarification and reconceptualization of how knowledge is generated and used in healthcare. Nurs. Res. Pract. 2012, 2012, 792519. [Google Scholar] [CrossRef] [PubMed]
- Jordan, Z.; Lockwood, C.; Munn, Z.; Aromataris, E. The updated Joanna Briggs Institute model for evidence-based healthcare. Int. J. Evid. Based Healthc. 2019, 17, 58–71. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Lopes Cardoso, I.; Sá, M.; Chiadmi, Y.; Moreira, M.T.; Guimarães, M.I. Mapping the Importance of Pink Teeth in Forensic Medicine for Determining Cause of Death: Protocol of a Scoping Review. Arab J. Forensic Sci. Forensic Med. 2025, 7, 147–156. [Google Scholar] [CrossRef]
- Soriano, H.P.; Ramos, E.T.; de León, A.T. The post-mortem pink teeth phenomenon: A case report. J. Philipp. Dent. Assoc. 2009, 61, 38–41. [Google Scholar]
- Borrman, H.; Du Chesne, A.; Brinkmann, B. Medico-legal aspects of postmortem pink teeth. Int. J. Legal Med. 1994, 106, 225–231. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.