
Histological and Histomorphometric Evaluation of RegenerOss®: A Porcine-Derived Bone Substitute for Guided Bone Regeneration

 ,
,  , ,
, ,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Surgical Procedure
2.2. Histological, Histomorphometric, and Statistical Analysis
2.3. Physico-Chemical Characterization of the Biomaterial
3. Results
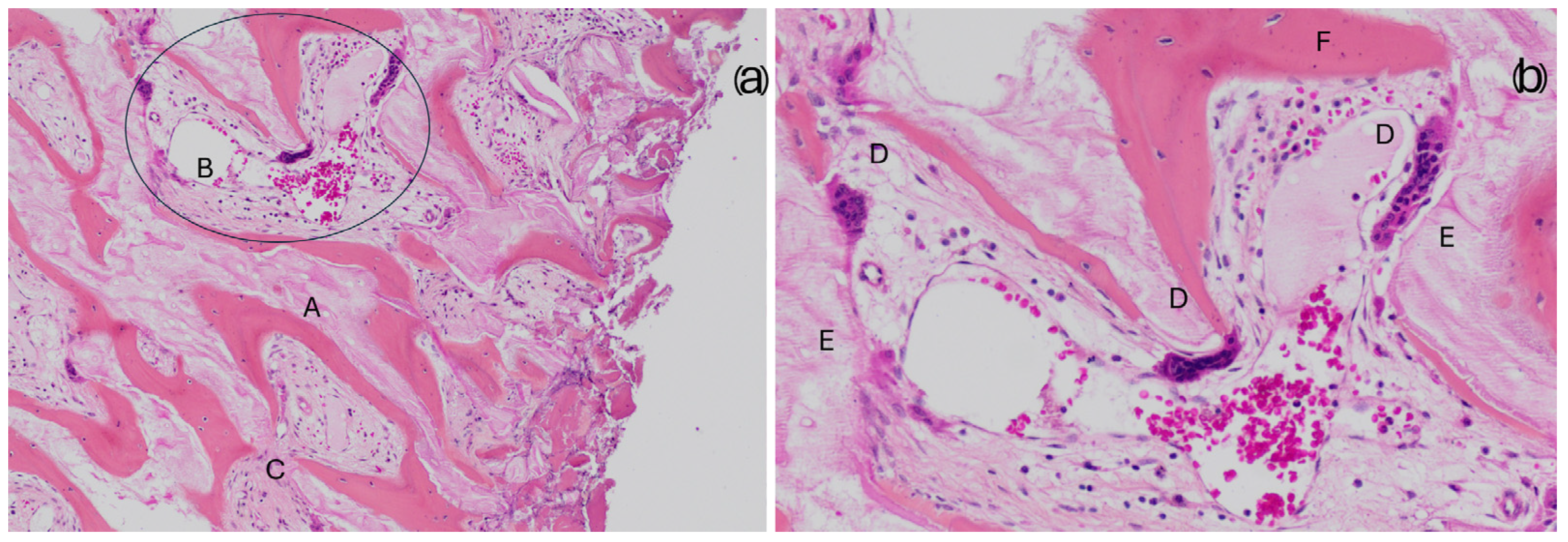
3.1. Qualitative Evaluation of Newly Formed Bone

3.2. Correlation Analysis
- SCORE2 was proposed after it was observed that the INFL variable (inflammatory infiltrates) was not significantly correlated with NFB.
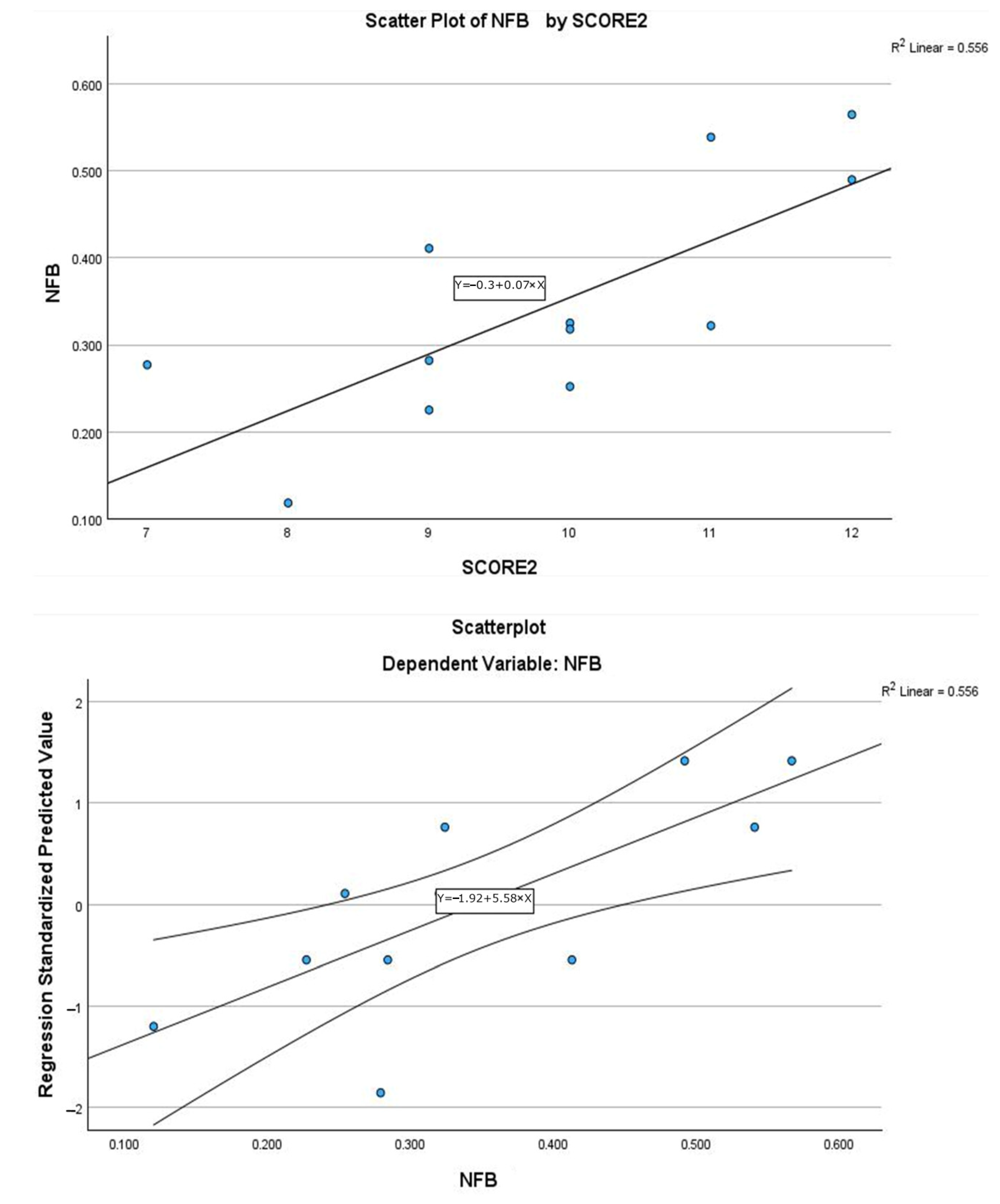
3.3. Linear Regression Models
- Model 1: SCORE as the independent variable.
- Model 2: SCORE2 as the independent variable.
- Insufficient samples: 5 samples with scores < 10, including 3 with 9.
- Sufficient samples: 3 samples with a score of 10.
- Good/excellent samples: 4 samples with a score ≥ 11 (75th percentile) are considered high-quality samples [34].
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tatullo, M.; Zavan, B.; Piattelli, A. Critical overview on regenerative medicine: New insights into the role of stem cells and innovative biomaterials. Int. J. Mol. Sci. 2023, 24, 7936. [Google Scholar] [CrossRef] [PubMed]
- Ntege, E.H.; Sunami, H.; Shimizu, Y. Advances in regenerative therapy: A review of the literature and future directions. Regen. Ther. 2020, 14, 136–153. [Google Scholar] [CrossRef] [PubMed]
- Petrosyan, A.; Martins, P.N.; Solez, K.; Uygun, B.E.; Gorantla, V.S.; Orlando, G. Regenerative medicine applications: An overview of clinical trials. Front. Bioeng. Biotechnol. 2022, 10, 942750. [Google Scholar] [CrossRef] [PubMed]
- Smeets, R.; Matthies, L.; Windisch, P.; Gosau, M.; Jung, R.; Brodala, N.; Stefanini, M.; Kleinheinz, J.; Payer, M.; Henningsen, A.; et al. Horizontal augmentation techniques in the mandible: A systematic review. Int. J. Implant Dent. 2022, 8, 23. [Google Scholar] [CrossRef]
- Al-Nawas, B.; Schiegnitz, E. Augmentation procedures using bone substitute materials or autogenous bone—A systematic review and meta-analysis. Eur. J. Oral Implantol. 2014, 7 (Suppl. 2), S219–S234. [Google Scholar]
- Tumedei, M.; Savadori, P.; Del Fabbro, M. Synthetic blocks for bone regeneration: A systematic review and meta-analysis. Int. J. Mol. Sci. 2019, 20, 4221. [Google Scholar] [CrossRef]
- O’Brien, F.J. Biomaterials & scaffolds for tissue engineering. Mater. Today 2011, 14, 88–95. [Google Scholar] [CrossRef]
- Ciszyński, M.; Dominiak, S.; Dominiak, M.; Gedrange, T.; Hadzik, J. Allogenic Bone Graft in Dentistry: A Review of Current Trends and Developments. Int. J. Mol. Sci. 2023, 24, 16598. [Google Scholar] [CrossRef]
- Schmidt, A.H. Autologous bone graft: Is it still the gold standard? Injury 2021, 52 (Suppl. 2), S18–S22. [Google Scholar] [CrossRef]
- Georgeanu, V.A.; Gingu, O.; Antoniac, I.V.; Manolea, H.O. Current options and future perspectives on bone graft and biomaterials substitutes for bone repair, from clinical needs to advanced biomaterials research. Appl. Sci. 2023, 13, 8471. [Google Scholar] [CrossRef]
- De Long WGJr Einhorn, T.A.; Koval, K.; McKee, M.; Smith, W.; Sanders, R.; Watson, T. Bone grafts and bone graft substitutes in orthopaedic trauma surgery: A critical analysis. J. Bone Jt. Surg. Am. Vol. 2007, 89, 649–658. [Google Scholar] [CrossRef]
- Jing, L.; Su, B. Resorption rates of bone graft materials after crestal maxillary sinus floor elevation and its influencing factors. J. Funct. Biomater. 2024, 15, 133. [Google Scholar] [CrossRef] [PubMed]
- Starch-Jensen, T.; Deluiz, D.; Tinoco, E.M.B. Horizontal Alveolar Ridge Augmentation with Allogeneic Bone Block Graft Compared with Autogenous Bone Block Graft: A Systematic Review. J. Oral Maxillofac. Res. 2020, 11, e1. [Google Scholar] [CrossRef] [PubMed]
- De Azambuja Carvalho, P.; De Oliveria Ciaramicolo, N.; Ferreira, J.O.; Pereira-Filho, V. Clinical and laboratorial outcomes of xenogenic biomaterials: Literature review. Front. Oral Maxillofac. Med. 2021, 5, 8. Available online: https://fomm.amegroups.org/article/view/56185 (accessed on 28 January 2025).
- Santoro, A.; Voto, A.; Fortino, L.; Guida, R.; Laudisio, C.; Cillo, M.; D’Ursi, A.M. Bone Defect Treatment in Regenerative Medicine: Exploring Natural and Synthetic Bone Substitutes. Int. J. Mol. Sci. 2025, 26, 3085. [Google Scholar] [CrossRef]
- Starch-Jensen, T.; Deluiz, D.; Vitenson, J.; Bruun, N.H.; Tinoco, E.M.B. Maxillary Sinus Floor Augmentation with Autogenous Bone Graft Compared with a Composite Grafting Material or Bone Substitute Alone: A Systematic Review and Meta-Analysis Assessing Volumetric Stability of the Grafting Material. J. Oral Maxillofac. Res. 2021, 12, e1. [Google Scholar] [CrossRef]
- Vanka, S.; Kasem, F.A.; Kailani, T.; Wali, O.; Vanka, A. Bone graft substitutes and dental implant stability in immediate implant surgery: A systematic review and meta-analysis. Evid.-Based Dent. 2024, 26, 70. [Google Scholar] [CrossRef]
- Azadi, A.; Hazrati, P.; Tizno, A.; Rezaei, F.; Akbarzadeh Baghban, A.; Tabrizi, R. Bone expansion as a horizontal alveolar ridge augmentation technique: A systematic review and meta-analysis. Oral Maxillofac. Surg. 2025, 29, 32. [Google Scholar] [CrossRef]
- Zhao, R.; Yang, R.; Cooper, P.R.; Khurshid, Z.; Shavandi, A.; Ratnayake, J. Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments. Molecules 2021, 26, 3007. [Google Scholar] [CrossRef]
- Perić Kačarević, Z.; Kavehei, F.; Houshmand, A.; Franke, J.; Smeets, R.; Rimashevskiy, D.; Wenisch, S.; Schnettler, R.; Jung, O.; Barbeck, M. Purification processes of xenogeneic bone substitutes and their impact on tissue reactions and regeneration. Int. J. Artif. Organs 2018, 41, 789–800. [Google Scholar] [CrossRef]
- Akita, K.; Fukuda, N.; Kamada, K.; Kudoh, K.; Kurio, N.; Tsuru, K.; Ishikawa, K.; Miyamoto, Y. Fabrication of porous carbonate apatite granules using microfiber and its histological evaluations in rabbit calvarial bone defects. J. Biomed. Mater. Res. Part A 2020, 108, 709–721. [Google Scholar] [CrossRef] [PubMed]
- Battafarano, G.; Rossi, M.; De Martino, V.; Marampon, F.; Borro, L.; Secinaro, A.; Del Fattore, A. Strategies for bone regeneration: From graft to tissue engineering. Int. J. Mol. Sci. 2021, 22, 1128. [Google Scholar] [CrossRef] [PubMed]
- Hwang, D.; Wang, H.L. Medical contraindications to implant therapy: Part I: Absolute contraindications. Implant Dent. 2006, 15, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Savadori, P.; Dalfino, S.; Piazzoni, M.; Inchingolo, F.; Del Fabbro, M.; Tartaglia, G.M.; Giardino, L. Arduino Automated Microwave Oven for Tissue Decalcification. Bioengineering 2023, 10, 79. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Giardino, L.; Grande, N.M.; Savadori, P.; Fabbro, M.D.; Plotino, G. Clinical and Histological Findings of Post-Treatment Infection in the Presence of Vertical Root Fracture and Apical Periodontitis: Case Reports. Eur. Endod. J. 2019, 4, 45–48. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Giardino, L.; Generali, L.; Del Fabbro, M.; Tartaglia, G.M.; Bidossi, A.; Savadori, P. Detection of bacteria in dental samples using the Periodic acid-Schiff (PAS) histological stain. Micron 2023, 172, 103498. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.; Lowe, D.G. Recognising Panoramas. In Proceedings of the 9th IEEE International Conference on Computer Vision, Nice, France, 13–16 October 2003. [Google Scholar]
- Canullo, L.; Donato, A.; Savadori, P.; Radovanovic, S.; Iacono, R.; Rakic, M. Effect of argon plasma abutment activation on soft tissue healing: RCT with histological assessment. Clin. Implant Dent. Relat. Res. 2024, 26, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Minetti, E.; Palermo, A.; Savadori, P.; Patano, A.; Inchingolo, A.D.; Rapone, B.; Malcangi, G.; Inchingolo, F.; Dipalma, G.; Tartaglia, F.C.; et al. Socket Preservation Using Dentin Mixed with Xenograft Materials: A Pilot Study. Materials 2023, 16, 4945. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Söhling, N.; Von Jan, O.; Janko, M.; Nau, C.; Ritz, U.; Marzi, I.; Henrich, D.; Verboket, R.D. Measuring Bone Healing: Parameters and Scores in Comparison. Bioengineering 2023, 10, 1011. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lucaciu, O.; Gheban, D.; Soriţau, O.; Băciuţ, M.; Câmpian, R.S.; Băciuţ, G. Comparative assessment of bone regeneration by histometry and a histological scoring system/Evaluarea comparativă a regenerării osoase utilizând histometria și un scor de vindecare histologică. Rev. Romana Med. Lab. 2015, 23, 31–45. [Google Scholar] [CrossRef]
- Gerstenfeld, L.C.; Wronski, T.J.; Hollinger, J.O.; Einhorn, T.A. Application of histomorphometric methods to the study of bone repair. J. Bone Miner. Res. 2005, 20, 1715–1722. [Google Scholar] [CrossRef] [PubMed]
- Li, S.-T.; Chen, H.-C.; Yuen, D. Isolation and Characterization of a Porous Carbonate Apatite from Porcine Cancellous Bone. Sci. Technol. Innov. 2014, 1, 13. [Google Scholar]
- Nease, R.F., Jr.; Owens, D.K.; Sox, H.C., Jr. Threshold analysis using diagnostic tests with multiple results. Med. Decis. Making 1989, 9, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Dalfino, S.; Savadori, P.; Piazzoni, M.; Connelly, S.T.; Giannì, A.B.; Del Fabbro, M.; Tartaglia, G.M.; Moroni, L. Regeneration of Critical-Sized Mandibular Defects Using 3D-Printed Composite Scaffolds: A Quantitative Evaluation of New Bone Formation in In Vivo Studies. Adv. Healthc. Mater. 2023, 12, e2300128. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Buccino, F.; Zagra, L.; Savadori, P.; Galluzzo, A.; Colombo, C.; Grossi, G.; Banfi, G.; Vergani, L.M. Mapping local mechanical properties of human healthy and osteoporotic femoral heads. Materialia 2021, 20, 101229. [Google Scholar] [CrossRef]
- Figueiredo, A.; Coimbra, P.; Cabrita, A.; Guerra, F.; Figueiredo, M. Comparison of a xenogeneic and an alloplastic material used in dental implants in terms of physico-chemical characteristics and in vivo inflammatory response. Mater. Sci. Eng. C Mater. Biol. Appl. 2013, 33, 3506–3513. [Google Scholar] [CrossRef]
- Giardino, L.; Bidossi, A.; Del Fabbro, M.; Savadori, P.; Maddalone, M.; Ferrari, L.; Ballal, N.V.; Das, S.; Rao, B.S.S. Antimicrobial activity, toxicity and accumulated hard-tissue debris (AHTD) removal efficacy of several chelating agents. Int. Endod. J. 2020, 53, 1093–1110. [Google Scholar] [CrossRef]
- Ferraz, M.P. Bone Grafts in Dental Medicine: An Overview of Autografts, Allografts and Synthetic Materials. Materials 2023, 16, 4117. [Google Scholar] [CrossRef]
- Krennmair, S.; Postl, L.; Schwarze, U.Y.; Malek, M.; Stimmelmayr, M.; Krennmair, G. Clinical, radiographic, and histological/histomorphometric analysis of maxillary sinus grafting with deproteinized porcine or bovine bone mineral: A randomized clinical trial. Clin. Oral Implants Res. 2023, 34, 1230–1247. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| New Bone Formation | Range/Description | Value | Bone Substitute Residue | Range/Description | Value |
|---|---|---|---|---|---|
| 76–100% | 4 | 1–15% | 4 | ||
| 51–75% | 3 | 16–30% | 3 | ||
| 26–50% | 2 | 31–60% | 2 | ||
| 10–25% | 1 | 61–90% | 1 | ||
| <10% | 0 | 91–100% | 0 | ||
| Bone Structure | Range/Description | value | Inflammation | Range/Description | value |
| Well-defined trabecular bone, presence of multiple dense bone areas (more than 3 secondary osteons in different core areas) | 4 | None | 4 | ||
| Well-defined trabecular bone, presence of dense bone areas (at least 1–2 secondary osteons) | 3 | Very reduced: sporadic foci (1 or 2) | 3 | ||
| Long but thin trabeculae, no dense bone (no presence of secondary osteons) | 2 | Reduced: occasional foci | 2 | ||
| Short and fragmented trabeculae | 1 | Moderate: numerous foci | 1 | ||
| Poorly defined or amorphous tissue | 0 | Extensive | 0 |
| Media | Median | Min | Max | Dev. St. | |
|---|---|---|---|---|---|
| Newly formed bone | 34.4% | 32% | 11.8% | 56.5% | 13.40% |
| Residual material | 6.1% | 4.8% | 0.0% | 19.8% | 6.60% |
| NFB | QTY | RES | QLTY | INFL | SCORE | SCORE2 | ||
|---|---|---|---|---|---|---|---|---|
| NFB | Pearson Correlation | -- | ||||||
| N | 12 | |||||||
| QTY | Pearson Correlation | 0.924 ** | -- | |||||
| Sig. (2-tailed) | <0.001 | |||||||
| N | 12 | 12 | ||||||
| RES | Pearson Correlation | 0.799 ** | 0.682 * | -- | ||||
| Sig. (2-tailed) | 0.002 | 0.015 | ||||||
| N | 12 | 12 | 12 | |||||
| QLTY | Pearson Correlation | 0.650 * | 0.713 ** | 0.37 | -- | |||
| Sig. (2-tailed) | 0.022 | 0.009 | 0.236 | |||||
| N | 12 | 12 | 12 | 12 | ||||
| INFL | Pearson Correlation | 0.087 | 0.064 | −0.012 | −0.308 | -- | ||
| Sig. (2-tailed) | 0.789 | 0.843 | 0.971 | 0.331 | ||||
| N | 12 | 12 | 12 | 12 | 12 | |||
| SCORE | Pearson Correlation | 0.851 ** | 0.861 ** | 0.634 * | 0.600 * | 0.476 | -- | |
| Sig. (2-tailed) | <0.001 | <0.001 | 0.027 | 0.039 | 0.118 | |||
| N | 12 | 12 | 12 | 12 | 12 | 12 | ||
| SCORE2 | Pearson Correlation | 0.899 ** | 0.927 ** | 0.722 ** | 0.884 ** | −0.14 | 0.804 ** | -- |
| Sig. (2-tailed) | <0.001 | <0.001 | 0.008 | <0.001 | 0.665 | 0.002 | ||
| N | 12 | 12 | 12 | 12 | 12 | 12 | 12 | |
| Model | Coefficients | Unstandardized Coefficients | Standardized Coefficients | 95% Confidence Interval for B | ||||
|---|---|---|---|---|---|---|---|---|
| B | Std. Error | β | t | Sig. | Lower | Upper | ||
| Model 1 | (Constant) | −0.367 | 0.141 | −2.61 | 0.026 | −0.68 | −0.054 | |
| SCORE | 0.055 | 0.011 | 0.851 | 5.114 | <0.001 | 0.031 | 0.079 | |
| Model 2 | (Constant) | −0.278 | 0.097 | −2.861 | 0.017 | −0.495 | −0.062 | |
| SCORE2 | 0.065 | 0.01 | 0.899 | 6.5 | <0.001 | 0.043 | 0.088 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savadori, P.; Del Fabbro, M.; Sora, V.M.; Giardino, L.; Generali, L.; Kondic, D.; Santoro, F. Histological and Histomorphometric Evaluation of RegenerOss®: A Porcine-Derived Bone Substitute for Guided Bone Regeneration. J. Compos. Sci. 2025, 9, 245. https://doi.org/10.3390/jcs9050245
Savadori P, Del Fabbro M, Sora VM, Giardino L, Generali L, Kondic D, Santoro F. Histological and Histomorphometric Evaluation of RegenerOss®: A Porcine-Derived Bone Substitute for Guided Bone Regeneration. Journal of Composites Science. 2025; 9(5):245. https://doi.org/10.3390/jcs9050245
Chicago/Turabian StyleSavadori, Paolo, Massimo Del Fabbro, Valerio Massimo Sora, Luciano Giardino, Luigi Generali, Danijel Kondic, and Fausto Santoro. 2025. "Histological and Histomorphometric Evaluation of RegenerOss®: A Porcine-Derived Bone Substitute for Guided Bone Regeneration" Journal of Composites Science 9, no. 5: 245. https://doi.org/10.3390/jcs9050245
APA StyleSavadori, P., Del Fabbro, M., Sora, V. M., Giardino, L., Generali, L., Kondic, D., & Santoro, F. (2025). Histological and Histomorphometric Evaluation of RegenerOss®: A Porcine-Derived Bone Substitute for Guided Bone Regeneration. Journal of Composites Science, 9(5), 245. https://doi.org/10.3390/jcs9050245