
Evaluation of Ozonized Gel Application for Stain Removal on Dental Composite Resins

 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Specimens’ Preparation
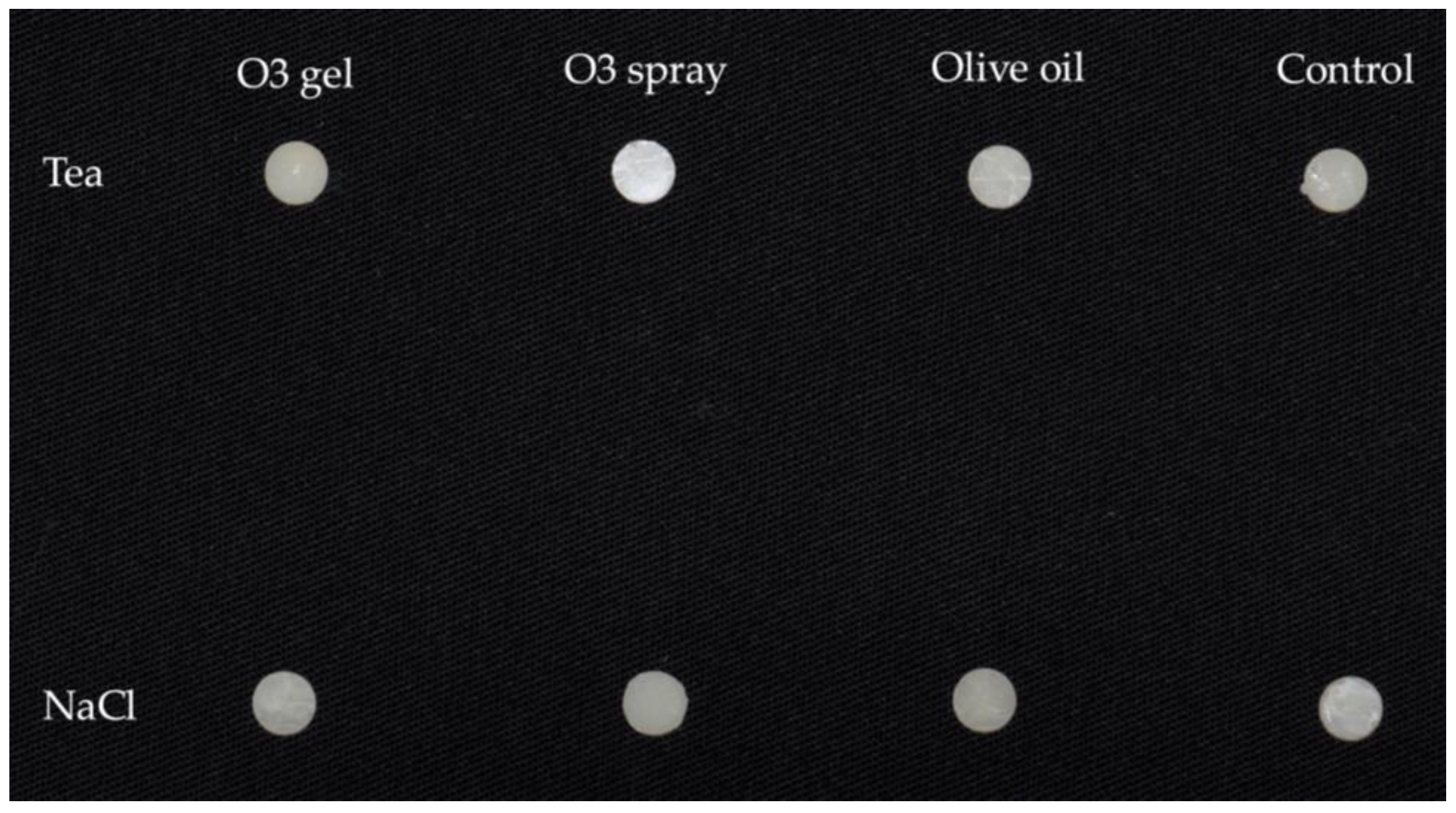
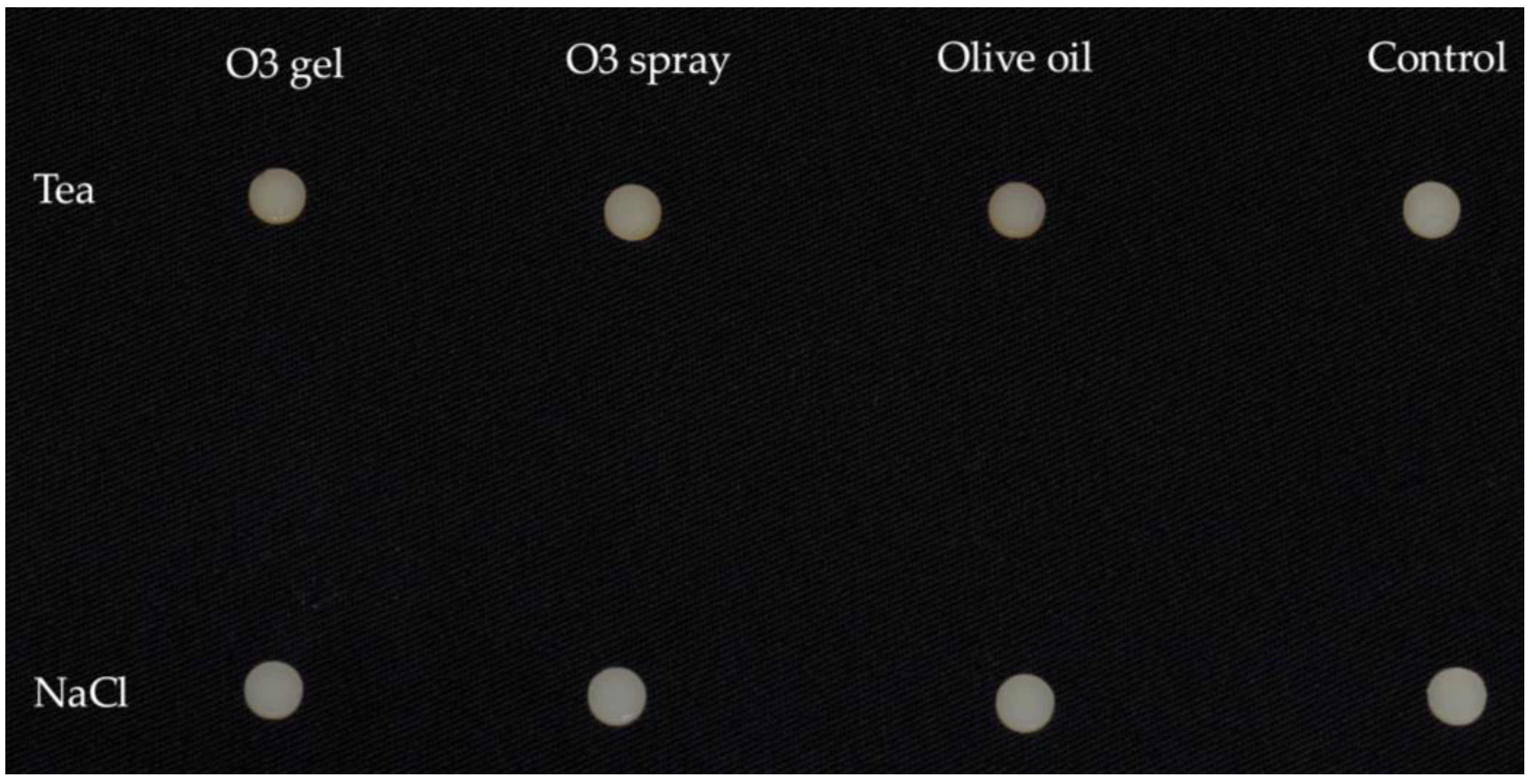
2.2. Experimental Procedure
- -
- Group Tea: Twenty specimens underwent a pigmentation treatment consisting of a 1 h immersion in a 37 °C tea solution assessed with a contact thermometer (PeakTech® Digital Thermometer 5135/5140 Prilf—und Messtechnik, GmbH, Ahrensburg, Germany); the solution was obtained with 10 applications of 10′ each of the teabag (Lipton, Glasgow, Scotland). The time of application was chosen to simulate a weekly consumption of tea.
- -
- Group NaCl: Twenty specimens were immersed in physiological solution (B. Braun, Milan, Italy) for 1 h.
- -
- O3 gel: Two applications of 1 h each of ozonized gel (Gelio3, Bioemmei Srl, 36100 Vicenza, Italy) containing a bio-ozonized olive oil, hydrated silica, and arnica;
- -
- O3 spray: Two applications of 1 h each of ozonized spray (Gelio3 without hydrated silica);
- -
- Olive oil: Two applications of 1 h each of ozonized oil (Gelio3 without hydrated silica and ozone);
- -
- Control: Maintenance in physiological solution for 1 h.
2.3. Colorimetric Evaluation
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Owens, B.M. Replacement and initial placement of tooth colored restorations: A review and discussion. J. Tenn. Dent. Assoc. 1998, 78, 26–29. [Google Scholar]
- Hickel, R.; Heidemann, D.; Staehle, H.J.; Minnig, P.; Wilson, N.H. Direct composite restorations: Extended use in anterior and posterior situations. Clin. Oral. Investig. 2004, 8, 43–44. [Google Scholar] [PubMed]
- Janda, R.; Roulet, J.F.; Kaminsky, M.; Steffin, G.; Latta, M. Color stability of resin matrix restorative materials as a function of the method of light activation. Eur. J. Oral Sci. 2004, 112, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Stober, T.; Gilde, H.; Lenz, P. Color stability of highly filled composite resin materials for facings. Dent. Mater. 2001, 17, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.K.; Lim, B.S.; Rhee, S.H.; Yang, H.C.; Powers, J.M. Color and translucency of A2 shade composite resins after curing, polishing and thermocycling. Oper. Dent. 2005, 30, 436–442. [Google Scholar]
- HashemiKamangar, S.S.; Jafari, S.; Rouhaninasab, M. Effects of curing time and intensity and polishing technique on color stability of bleach-shade composite resins. Dent. Res. J. (Isfahan) 2023, 20, 67. [Google Scholar] [CrossRef]
- Schulze, K.A.; Marshall, S.J.; Gansky, S.A.; Marshall, G.W. Color stability and hardness in dental composites after accelerated aging. Dent. Mater. 2003, 19, 612–619. [Google Scholar] [CrossRef]
- Farah, R.I.; Elwi, H. Spectrophotometric evaluation of color changes of bleach-shade resin-based composites after staining and bleaching. J. Contemp. Dent. Pract. 2014, 15, 587–594. [Google Scholar] [CrossRef]
- de Gee, A.J.; ten Harkel-Hagenaar, E.; Davidson, C.L. Color dye for identification of incompletely cured composite resins. J. Prosthet. Dent. 1984, 52, 626–631. [Google Scholar] [CrossRef]
- Gül, P.; Harorli, O.T.; Akgül, N.; Gündoğdu, M. Effect of different bleaching applications on the surface properties and staining susceptibility of dentalcomposites. J. Wuhan. Univ. Technol. Mater. Sci. Ed. 2016, 31, 677–683. [Google Scholar] [CrossRef]
- Borges, A.B.; Marsilio, A.L.; Pagani, C.; Rodrigues, J.R. Surface roughness of packable composite resins polished with various systems. J. Esthet. Restor. Dent. 2004, 16, 42–47. [Google Scholar] [CrossRef]
- Guler, A.U.; Yilmaz, F.; Kulunk, T.; Guler, E.; Kurt, S. Effects of different drinks on stainability of composite resin provisional restorative materials. J. Prosthet. Dent. 2005, 94, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Bagheri, R.; Burrow, M.F.; Tyas, M. Influence of food simulating solutions and surface finish on susceptibility to staining of aesthetic restorative materials. J. Dent. 2005, 33, 389–398. [Google Scholar] [CrossRef]
- Vidal, M.L.; Pecho, O.E.; Collares, K.; Brandeburski, S.; Bona, A.D. Color Change of Resin-based Composites After In Vitro Bleaching Protocols: A Systematic Review and Meta-analysis. Oper. Dent. 2022, 47, 149–162. [Google Scholar] [CrossRef]
- Barczyk, I.; Masłyk, D.; Walczuk, N.; Kijak, K.; Skomro, P.; Gronwald, H.; Pawlak, M.; Rusińska, A.; Sadowska, N.; Gronwald, B.; et al. Potential Clinical Applications of Ozone Therapy in Dental Specialties—A Literature Review, Supported by Own Observations. Int. J. Environ. Res. Public Health 2023, 20, 2048. [Google Scholar] [CrossRef] [PubMed]
- Moureu, S.; Violleau, F.; Ali Haimoud-Lekhal, D.; Calmon, A. Ozonation of sunflower oils: Impact of experimental conditions on the composition and the antibacterial activity of ozonized oils. Chem. Phys. Lipids 2015, 186, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Scribante, A.; Gallo, S.; Pascadopoli, M.; Soleo, R.; Di Fonso, F.; Politi, L.; Venugopal, A.; Marya, A.; Butera, A. Management of Periodontal Disease with Adjunctive Therapy with Ozone and Photobiomodulation (PBM): A Randomized Clinical Trial. Photonics 2022, 9, 138. [Google Scholar] [CrossRef]
- Sen, S.; Sen, S. Ozone therapy a new vista in dentistry: Integrated review. Med. Gas Res. 2020, 10, 189–192. [Google Scholar] [CrossRef]
- Alsakr, A.; Gufran, K.; Alqahtani, A.S.; Alasqah, M.; Alnufaiy, B.; Alzahrani, H.G.; Alahmari, A.A.; Alhumaidani, F.K.; Alhumaidani, R.K.; Althobiti, M.J. Ozone Therapy as an Adjuvant in the Treatment of Periodontitis. J. Clin. Med. 2023, 12, 7078. [Google Scholar] [CrossRef]
- Scribante, A.; Gallo, S.; Pascadopoli, M.; Frani, M.; Butera, A. Ozonized gels vs chlorhexidine in non-surgical periodontal treatment: A randomized clinical trial. Oral Dis. 2024, 30, 3993–4000. [Google Scholar] [CrossRef]
- Choudhary, A.; Rajasekar, A. Efficacy of Ozonated Olive Oil Gel in the Management of Peri-Implant Mucositis. J. Long. Term. Eff. Med. Implants. 2024, 34, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Santos, G.M.; Pacheco, R.L.; Bussadori, S.K.; Santos, E.M.; Riera, R.; de Oliveira Cruz Latorraca, C.; Mota, P.; Benavent Caldas Bellotto, E.F.; Martimbianco, A.L.C. Effectiveness and Safety of Ozone Therapy in Dental Caries Treatment: Systematic Review and Meta-analysis. J. Evid. Based Dent. Pract. 2020, 20, 101472. [Google Scholar] [CrossRef]
- Makeeva, M.K.; Daurova, F.Y.; Byakova, S.F.; Turkina, A.Y. Treatment of an Endo-Perio Lesion with Ozone Gas in a Patient with Aggressive Periodontitis: A Clinical Case Report and Literature Review. Clin. Cosmet. Investig. Dent. 2020, 12, 447–464. [Google Scholar] [CrossRef] [PubMed]
- Suh, Y.; Shrey, P.; Re, K.; Gandhi, J.; Joshi, G. Clinical utility of ozone therapy in dental and oral medicine. Med. Gas. Res. 2019, 9, 163–167. [Google Scholar]
- Berezow, A.B.; Darveau, R.P. Microbial shift and periodontitis. Periodontology 2000 2011, 55, 36–47. [Google Scholar] [CrossRef]
- El Meligy, O.A.; Elemam, N.M.; Talaat, I.M. Ozone Therapy in Medicine and Dentistry: A Review of the Literature. Dent. J. 2023, 11, 187. [Google Scholar] [CrossRef]
- Abd Elhamid, M.; Mosallam, R. Effect of bleaching versus repolishing on colour and surface topography of stained resin composite. Aust. Dent. J. 2010, 55, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Gallo, S.; Colombo, M.; Poggio, C.; Scribante, A.; Saracino, M.; Beltrami, R. Bleaching Effect of Ozonized Substances on Resin Composite: A New Potentiality for Ozone Therapy in Dentistry. Appl. Sci. 2023, 13, 2149. [Google Scholar] [CrossRef]
- Agnihotry, A.; Gill, K.S.; Singhal, D.; Fedorowicz, Z.; Dash, S.; Pedrazzi, V. A comparison of the bleaching effectiveness of chlorine dioxide and hydrogen peroxide on dental composite. Braz. Dent. J. 2014, 25, 524–527. [Google Scholar] [CrossRef]
- Rode, K.M.; Kawano, Y.; Turbino, M.L. Evaluation of curing light distance on resin composite microhardness and polymerization. Oper. Dent. 2007, 32, 571–578. [Google Scholar] [CrossRef]
- Zorzin, J.; Maier, E.; Harre, S.; Fey, T.; Belli, R.; Lohbauer, U.; Petschelt, A.; Taschner, M. Bulk-fill resin composites: Polymerization properties and extended light curing. Dent. Mater. 2015, 31, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Poggio, C.; Lombardini, M.; Gaviati, S.; Chiesa, M. Evaluation of Vickers hardness and depth of cure of six composite resins photo-activated with different polymerization modes. J. Conserv. Dent. 2012, 15, 237. [Google Scholar] [CrossRef] [PubMed]
- Alrahlah, A.; Silikas, N.; Watts, D.C. Post-cure depth of cure of bulk fill dental resin composites. Dent. Mater. 2014, 30, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.R.; Cui, G.; Rigg, B. The development of the CIE 2000 colour-difference formula: CIEDE2000. Color. Res. Appl. 2001, 26, 340–350. [Google Scholar] [CrossRef]
- Randi, C.J.; Heiderich, C.M.C.; Serrano, R.V.; Morimoto, S.; de Moraes, L.O.C.; Campos, L.; Palma, L.F. Use of Ozone Therapy in Implant Dentistry: A Systematic Review. Oral. Maxillofac. Surg. 2024, 28, 39–49. [Google Scholar] [CrossRef]
- Kumar, A.; Srivastava, A.; Sah, N.; Sah, S.; Nair, V.I.N.; Das, A.; Singh, A.K. Evidence-Based Effectiveness of Ozone Therapy in the Treatment for Oral Lichen Planus—A Systematic Review. Natl. J. Maxillofac. Surg. 2024, 15, 18–22. [Google Scholar] [CrossRef]
- Liu, J.; Huang, Y.; Huang, J.; Yang, W.; Tao, R. Effects of Ozone Therapy as an Adjuvant in the Treatment of Periodontitis: A Systematic Review and Meta-Analysis. BMC Oral Health 2025, 25, 335. [Google Scholar] [CrossRef]
- Colombo, M.; Gallo, S.; Garofoli, A.; Poggio, C.; Arciola, C.R.; Scribante, A. Ozone Gel in Chronic Periodontal Disease: A Randomized Clinical Trial on the Anti-Inflammatory Effects of Ozone Application. Biology 2021, 10, 625. [Google Scholar] [CrossRef]
- Johnston, W.M. Color Measurement in Dentistry. J. Dent. 2009, 37 (Suppl. 1), e2–e6. [Google Scholar] [CrossRef]
- Talic, N.F.; Almudhi, A.A. The effect of dietary pigmentation on the esthetic appearance of clear orthodontic elastomeric modules. J. Orthod. Sci. 2016, 5, 70–73. [Google Scholar]
- Ludovichetti, F.S.; Zerman, N.; Stellini, E.; Zambon, G.; Mazzoleni, S.; Zuccon, A. Dental Bleaching: Patient Perception and Satisfaction. Minerva Dent. Oral Sci. 2024, 73, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Demirkol, D.; Aksu, S.; Çalışkan, S.; Tüloğlu, N. Evaluation of pediatric dentists’ knowledge and approaches to tooth discoloration. J. Clin. Pediatr. Dent. 2024, 48, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Chavez, J.A.; Soto-Barreras, U.; Perez-Aguirre, B.; Nevarez-Rascon, M.; Villegas-Mercado, C.E.; Dominguez-Perez, R.A. Reliability of Dental Shade Selection Methods: Agreement among Spectrophotometer, Intraoral Scanner, and Cross-Polarization Photography. J. Esthet. Restor. Dent. 2025, in press. [CrossRef] [PubMed]
- Joiner, A. Tooth color: Review of the literature. J. Dent. 2004, 32, 3–12. [Google Scholar] [CrossRef]
- O’Brien, W.J. Dental Materials and Their Selection, 3rd ed.; Quint Pub Inc.: Chicago, IL, USA, 2002; p. 28. [Google Scholar]
- International Commission on Illumination. Colorimetry: Official Recommendations of the Interntional Commission on Illumination, 2nd ed.; Bureau Central de la CIE: Vienna, Austria, 1986. [Google Scholar]
- Pereira-Lores, P.; Gancedo-Gancedo, T.; Martín-Biedma, B.; Varela-Aneiros, I.; Dablanca-Blanco, A.B.; Villasenín-Sánchez, C.; Martín-González, J.; Alonso de la Peña, V.; Castelo-Baz, P. Is At-Home Bleaching More Effective on the Upper Arch than the Lower Arch? A Prospective Cohort Study. J. Dent. 2025, 157, 105729. [Google Scholar] [CrossRef]
- Peker, O.; Bolgul, B. Evaluation of surface roughness and color changes of restorative materials used with different polishing procedures in pediatric dentistry. J. Clin. Pediatr. Dent. 2023, 47, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Hashemikamangar, S.S.; Farahani, S.; Khoshgoo, S.; Doroudgar, P. Comparative Efficacy of Four Stain Removal Methods for Bleach-Shade Composite Resins after Immersion in Staining Solutions: An In Vitro Study. Int. J. Dent. 2023, 2023, 8909288. [Google Scholar] [CrossRef]
- Dietrich, L.; de Assis Costa, M.D.M.; Blumenberg, C.; Nascimento, G.G.; Paranhos, L.R.; da Silva, G.R. A meta-analysis of ozone effect on tooth bleaching. Sci. Rep. 2021, 11, 13177. [Google Scholar] [CrossRef]
- Fidan, M.; Çankaya, N. Effect of food-simulating liquids and polishing times on the color stability of microhybrid and nanohybrid resin composites. Discov. Nano. 2025, 20, 43. [Google Scholar] [CrossRef]
- Zupo, R.; Castellana, F.; De Nucci, S.; Dibello, V.; Lozupone, M.; Giannelli, G.; De Pergola, G.; Panza, F.; Sardone, R.; Boeing, H. Beverages Consumption and Oral Health in the Aging Population: A Systematic Review. Front. Nutr. 2021, 8, 762383. [Google Scholar] [CrossRef]
- Alkahtani, R.; Stone, S.; German, M.; Waterhouse, P. A Review on Dental Whitening. J. Dent. 2020, 100, 103423. [Google Scholar] [CrossRef]
- Alqahtani, M.Q. Tooth-Bleaching Procedures and Their Controversial Effects: A Literature Review. Saudi Dent. J. 2014, 26, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, R.R.; Carlos, N.R.; Campos, F.U.; Turssi, C.P.; Vieira Júnior, W.F.; Amaral, F.L.D.; Basting, R.T. Ozone Gas Therapy for Tooth Bleaching Preserves Enamel Microhardness, Roughness, and Surface Micromorphology. Acta Odontol. Latinoam. 2023, 36, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Bin Hassan, S.A. Tooth Sensitivity Following Hydrogen Peroxide Bleaching with and without Ozone: A Randomized Controlled Trial: Tooth Sensitivity Following H2O2 versus H2O2/Ozone Bleaching. Pain. Res. Manag. 2024, 2024, 2695533. [Google Scholar] [CrossRef] [PubMed]
- Erdem, R.Z.; Çellik, Ö. Investigation of the Bleaching Efficiencies of Different Office-Type Bleaching Techniques and the Changes Caused on the Enamel Surface. Lasers Med. Sci. 2023, 38, 211. [Google Scholar] [CrossRef]
- Akl, M.A.; Sim, C.P.C.; Nunn, M.E.; Zeng, L.L.; Hamza, T.A.; Wee, A.G. Validation of Two Clinical Color Measuring Instruments for Use in Dental Research. J. Dent. 2022, 125, 104223. [Google Scholar] [CrossRef]
- Santos, M.; Leandro, F.; Barroso, H.; Delgado, A.H.S.; Proença, L.; Polido, M.; Vasconcelos e Cruz, J. Antibacterial Effect of Ozone on Cariogenic Bacteria and Its Potential Prejudicial Effect on Dentin Bond Strength—An In Vitro Study. Pharmaceutics 2024, 16, 614. [Google Scholar] [CrossRef]
- Pérez Mdel, M.; Ghinea, R.; Rivas, M.J.; Yebra, A.; Ionescu, A.M.; Paravina, R.D.; Herrera, L.J. Development of a customized whiteness index for dentistry based on CIELAB color space. Dent. Mater. 2016, 32, 461–467. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product | Manufacturer | Type | Shade | Composition | ||
|---|---|---|---|---|---|---|
| Matrix | Filler | Initiator | ||||
| G-aenial Anterior | GC International | Composite resin | A3 | Urethane Dimethacrylate (UDMA); (Octahydro-4,7-methano-1H-indenediyl)bis(methylene) bismethacrylate; 2,2-dimethyl-1,3-propanediyl bismethacrylate; esterified Bis-EMA | Pre-polymerized fillers with silica, strontium, lanthanoid fluoride; silica (nano and micro); fluoroaluminosilicate glass; ytterbium trifluoride; silanated silica | Camphorquinone; amine accelerator |
| Product | Material | Composition |
|---|---|---|
| Lipton | Tea | White tea, rosehips, green tea, hibiscus flowers, natural flavor, sweet blackberry leaves, dried black currant fruit pieces, dried blackberry fruit pieced, dried blueberry fruit pieces, dried raspberry fruit pieces, modified corn starch, sunflower lecithin |
| Physiological solution | Physiologic solution | 0.9% NaCl solution |
| Gelio3 | Ozonized gel | Bio-ozonized olive oil (20 mEq O2/kg), Arnica, Hydrated Silica |
| Ozonized spray | Bio-ozonized olive oil spray (20 mEq O2/kg), Arnica | |
| Olive oil | Olive oil |
| Group | Mean | SD | Minimum | Median | Maximum | Significance * |
|---|---|---|---|---|---|---|
| Tea O3 gel | 2.78 | 0.98 | 1.52 | 3.25 | 3.83 | A |
| Tea O3 spray | 2.78 | 1.07 | 1.17 | 2.83 | 3.77 | A |
| Tea Olive oil | 2.93 | 1.38 | 1.88 | 2.49 | 5.32 | A |
| Tea Control | 2.39 | 0.55 | 1.71 | 2.37 | 3.10 | A, B, C |
| NaCl O3 gel | 0.60 | 0.57 | 0.15 | 0.48 | 1.54 | B, C |
| NaCl O3 spray | 0.89 | 0.51 | 0.37 | 0.88 | 1.65 | C |
| NaCl Olive oil | 0.67 | 0.49 | 0.15 | 0.68 | 1.24 | C |
| NaCl Control | 1.23 | 0.72 | 0.23 | 1.15 | 2.07 | A, B, C |
| Group | Mean | SD | Minimum | Median | Maximum | Significance * |
|---|---|---|---|---|---|---|
| Tea O3 gel | 1.60 | 0.54 | 0.78 | 1.81 | 2.12 | A |
| Tea O3 spray | 0.94 | 0.32 | 0.65 | 0.85 | 1.45 | A |
| Tea Olive oil | 1.34 | 0.69 | 0.62 | 1.06 | 2.42 | A |
| Tea Control | 0.37 | 0.23 | 0.17 | 0.26 | 0.67 | A |
| NaCl O3 gel | 1.79 | 1.28 | 0.39 | 1.58 | 3.15 | A |
| NaCl O3 spray | 1.03 | 0.47 | 0.50 | 1.18 | 1.56 | A |
| NaCl Olive oil | 1.10 | 0.73 | 0.19 | 0.96 | 2.21 | A |
| NaCl Control | 0.87 | 0.56 | 0.30 | 0.68 | 1.73 | A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zampetti, P.; Colombo, M.; Pascadopoli, M.; Gallo, S.; Poggio, C.; Tayybia, J.; Scribante, A. Evaluation of Ozonized Gel Application for Stain Removal on Dental Composite Resins. J. Compos. Sci. 2025, 9, 238. https://doi.org/10.3390/jcs9050238
Zampetti P, Colombo M, Pascadopoli M, Gallo S, Poggio C, Tayybia J, Scribante A. Evaluation of Ozonized Gel Application for Stain Removal on Dental Composite Resins. Journal of Composites Science. 2025; 9(5):238. https://doi.org/10.3390/jcs9050238
Chicago/Turabian StyleZampetti, Paolo, Marco Colombo, Maurizio Pascadopoli, Simone Gallo, Claudio Poggio, Jamil Tayybia, and Andrea Scribante. 2025. "Evaluation of Ozonized Gel Application for Stain Removal on Dental Composite Resins" Journal of Composites Science 9, no. 5: 238. https://doi.org/10.3390/jcs9050238
APA StyleZampetti, P., Colombo, M., Pascadopoli, M., Gallo, S., Poggio, C., Tayybia, J., & Scribante, A. (2025). Evaluation of Ozonized Gel Application for Stain Removal on Dental Composite Resins. Journal of Composites Science, 9(5), 238. https://doi.org/10.3390/jcs9050238