Abstract
Pediatric food allergies are an escalating public health concern, with nut allergies representing a primary cause of persistent hypersensitivity and anaphylaxis. New data suggests that pediatric populations with multiple nut allergies (MNA) may be at higher anaphylaxis risk than their counterparts with single nut allergies. Despite this, there is an absence of literature posing multiple nut allergies against singular nut allergy cases. The majority of the research in this topic is directed towards singular nut allergy, without any differentiation between children with one versus multiple sensitivities. Epidemiological evidence indicates that multiple nut allergies are associated with lifelong sensitization, high cross-reactivity potential and increased risk and severity of reactions. Compounding clinical risk factors reinforce the already high risk associated with MNA and indicate that these children require careful monitoring and individual management. Diagnostic tools, including component-resolved diagnostics and oral food challenges, enable differentiation between true multi-nut sensitization and cross-reactivity, guiding targeted interventions. Management strategies must therefore be multifaceted, encompassing selective allergen avoidance, emergency preparedness with epinephrine auto-injectors, asthma control, nutritional support, and psychosocial care. Recognizing MNA as a distinct, high-risk phenotype highlights the necessity of precision-based, biomarker-driven clinical approaches to optimize safety, reduce morbidity, and improve quality of life for affected pediatric populations.
1. Introduction
Food allergies, particularly among children, have become a growing public health concern. Over the past few decades, the occurrence of pediatric food allergies has increased, with studies suggesting 4% of children in developed countries have this aversion [1,2]. This increase in food sensitivity is particularly concerning as it is associated with not only acute allergic reactions but also carries a lasting impact and reduces quality of life. In more severe cases, food allergies can even lead to potentially life-threatening complications through triggering anaphylaxis. These more severe complications are rare but warrant particular emphasis as it requires immediate medical intervention [3,4]. These challenges highlight the need for a comprehensive understanding of pediatric food allergies, particularly the aspects which pertain to an increased risk of more severe reactions.
Among the array of food allergies, peanuts and tree nuts have gained notable significance due to their high potential in causing severe allergic reactions. A substantial portion of emergency department visits and hospitalizations are due to nut allergies, owing to their role as one of the leading causes of food-induced anaphylaxis. Nut allergies are also typically persistent into adulthood, unlike other food allergies such as milk or egg allergies [5]. This persistence, combined with the ubiquity of nuts in processed foods, baked goods, and similar confectionery, creates a lifestyle burden for children and their families. While singular nut allergies are well reviewed in the literature, there is a noticeable gap in knowledge of multiple nut allergies. MNA is characterized by IgE-mediated sensitization and reproducible clinical allergic responses to two or more immunologically distinct tree nuts or peanuts, reflecting independent sensitization events rather than cross-reactivity to homologous proteins. New studies suggest that the most commonly reported allergens listed in individuals with multiple allergies were tree nuts (54%) and peanuts (51%) [1]. This increase arises from a multitude of factors, one of which being structural homology between various nut types. The structural similarities among allergenic proteins in nuts are conserved, allowing for cross-reactivity [6]. Multiple nut allergies also introduce more difficulty in avoidance, allowing unique opportunities for exposure.
Despite this, there is an absence of literature posing multiple nut allergies against singular nut allergy. The majority of research and focus on this topic is directed towards singular nut allergy, and groups peanut allergies and tree nut allergies together without any differentiation between children with one versus multiple sensitivities. The lack of research on this topic limits our understanding of children with multiple nut allergies and prevents adequate handling of these groups. There is still speculation as to whether multiple sensitizations confer an additional synergistic risk for anaphylaxis, the clinical implications that this would carry, and whether current guidelines appropriately address this seemingly high-risk group [7]. These implications extend beyond clinical management into broader public health considerations. Emergency planning for potential anaphylactic reactions, follow-up with allergists, and nutritional counseling are more often required for children with multiple nut allergies [8,9].
Given the increasing trend of food allergies in children, this narrative review intends to highlight potential increased risks imposed by multiple nut allergies, with a particular emphasis on its associated risk of anaphylaxis. We will discuss the epidemiology of nut allergies while examining the global burden of food allergies in pediatric populations, the underlying immunopathophysiology of nut allergy, anaphylaxis risk in multiple nut allergies, as well as diagnostic and management approaches.
2. Epidemiology
The rising prevalence of food allergies worldwide combined with the disproportionate contribution of nuts to severe allergic reactions and anaphylaxis, has become an increasingly important focus on pediatric research. The more severe complications associated with peanut allergy have led it to being traditionally more researched and published in the literature. Tree nut allergies, such as cashew, walnut, almond, hazelnut, pistachio, and pecan, additionally play a significant role in childhood morbidity alongside peanut allergies. This combination creates a synergistic effect of multiple nut allergies coalescing into an array of immune complications [10]. In order to accurately assess the risk of anaphylaxis in children, it is essential to understand the difference in prevalence between peanut and tree nut allergies, the frequency of co-sensitization and clinical reactivity occurring together, and if these allergies improve or remain over a duration of time.
Peanut allergy is consistently reported to have the highest rate of occurrence in children, affecting 1–2% of the pediatric population in multiple population-based studies, primarily in Western countries [11]. On the contrary, tree nut allergies as a group are less common. Many studies with varying study methods, geographic region, and age of cohort have concluded that tree nut allergies occur at a rate of 0.5–1.3% [12]. Tree nut allergies uncommonly occur alone, 23–68% of the pediatric population diagnosed with peanut allergy has an additional reaction to at least one tree nut [13]. Up to 12% of children with tree nut allergy exhibit reactions to multiple nuts, highlighting MNA as a distinct and clinically important subgroup [14]. However, there is a lack of research comparing tree nut allergies to other nuts outside the commonly indexed allergens. The observed overlap, where 23–68% of children with peanut allergy and 12% of those with tree nut allergy react to additional nuts, demonstrates that MNA represents a notable proportion of pediatric nut allergies and underscores the need to consider these children separately from those with single nut allergies.
The complexities of the epidemiology of nut allergies arise when geographic and ethnic varieties are considered. In the United States, 1.4% of individuals reported either a peanut or tree nut allergy [15]. Although several studies based exclusively in Europe report a higher rate of nut allergies, namely hazelnut sensitizations in the north and central regions and walnut sensitizations in Mediterranean countries. These correlations are most likely linked with dietary profiles and pollen sensitization. For example, in Northern Europe, hazelnut allergy is mainly driven by birch pollen sensitization [16]. Similarly, 41 of 100 patients derived from a multicultural pediatric allergy clinic in Leicester (UK) with a clinical history suggestive of cashew nut allergy were from an Asian background, possibly owing to dietary practices [17]. Likewise, the pattern holds true for Middle Eastern cohorts reporting a two-fold difference in pistachio allergy prevalence in pistachio cultivating areas (0.65%) compared to non-cultivating areas (0.3%) [18]. Such regional contrasts suggest that patterns of co-sensitization contributing to MNA may differ geographically, influenced by dietary habits, pollen exposure, and population-specific risk factors, further complicating the epidemiology of multiple nut allergies. In countries with diverse ethnicities, such as the United States, African American and Asian American populations typically experience a 0.5–1.5% higher rate of peanut or tree nut sensitization compared to White children [19]. Although, socioeconomic status and healthcare access may play a role in these differences.
The incidence of multiple nut allergies also vary geographically. In pediatric populations of the U.S. and Canada, 20–30% of patients with peanut allergy also react to at least one tree nut, including cashew, walnut, pistachio, hazelnut, and pecan [20]. This pattern is consistent for other regions too, like Australia, where the rate is 27% [21]. However, there is limited research regarding multiple nut allergies in the United Kingdom, signaling the absence of information regarding this topic. Moreover, in North America, children tend to exhibit co-sensitization to multiple tree nuts even in the absence of a peanut allergy less frequently than those in Europe. In China, despite the limited accessible data, recent studies have suggested MNA becoming a more prevalent cause of childhood anaphylaxis showing a positive trend in peanut and tree nut allergies [22].
The recurring pattern and history of nut allergies highlights the epidemiological impact of MNA. The majority of children that exhibit peanut allergy tend to live with it throughout adulthood. However, the minority, 21.5%, tend to develop long-term tolerance [23]. Tree nut allergies similarly persist, despite much less robust longitudinal data. Evidence has shown that children suffer from long-term tree nut allergy with just a 10% incidence rate of self-resolution [12]. In children on long-term tree-nut elimination diets, 68% had a negative mixed-nut challenge and 21% had only mild symptoms, showing that managing presumed multiple nut allergies remains complex and burdensome [24]. Long-term follow-up studies reveal that achieving tolerance to all implicated nuts is rare and that children with MNA remain with a lifelong risk of accidental exposure and anaphylaxis.
Clinically, the persistence of MNA influences the risk of anaphylaxis across the population. Peanuts and tree nuts have been proven to have the highest association with food-induced anaphylaxis in pediatric populations ranging from 0.4- to 6.8-year-olds, accounting for 49% of in-hospital registries [25]. The breadth of allergens and the increased chances of cross-contamination in foods poses a much greater threat for children with MNA. The extended duration of nut allergies, as opposed to other allergies, plays a role in the increased risk of severe cases due to the typical risk-taking behavior and reduced adherence to avoidance strategies that is observed in the ages past childhood [26].
Reported rates of peanut allergy, as observed in Figure 1, range from as high as 4.81% in Lebanon and 4% in Saudi Arabia to as low as 0.17% in Israel and 0.2% in Japan [27,28,29,30]. Intermediate prevalence rates have been observed in Australia (3%), Taiwan (3.4%), Sweden (3.2%), and the United States (2.6%) [31,32], while lower rates are seen in Singapore (0.3%, 0.64%) [33], Korea (0.22%), Mexico (0.29%), and Canada (0.8%) [34,35,36]. In contrast, tree nut allergies generally show lower prevalence across most regions, with values ranging from 4.1% in Saudi Arabia and 3% in Australia [14] to less than 1% in countries such as the United States (1.1%), Canada (0.6%), the United Kingdom (0.5%), and the Philippines (0.33%) [14,26,33,36]. Notably, several Asian populations, including Singapore (0.3%) and Israel (0.15%), report some of the lowest tree nut allergy rates globally [29,30,31,32,33,34]. These findings highlight substantial geographic variability in both peanut and tree nut allergy prevalence, likely reflecting differences in genetic, environmental, and dietary factors.
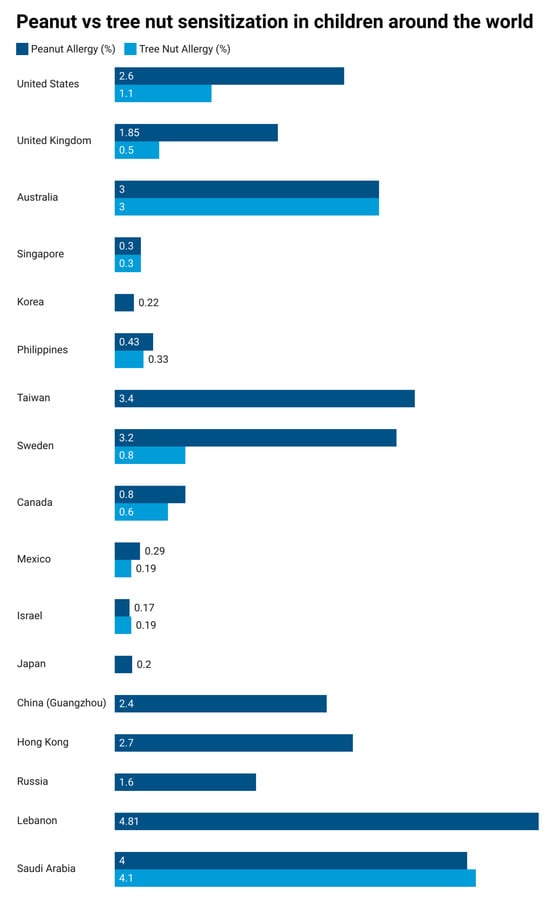
Figure 1.
A comparison of peanut and tree nut sensitizations in children from different countries [27,28,29,30,31,32,33,34].
To summarize, the epidemiology of MNA reflects a high baseline rate of peanut and tree nut co-sensitization, strong geographic and ethnic variability influenced by genetic predisposition, as well as environmental exposures. The majority of children affected with MNA do not develop tolerance, highlighting the implications associated with this issue. This epidemiological profile highlights the necessity of further research in this topic. It is necessary to understand methods of early detection, accurate diagnosis, and personalized strategies to reduce risk in these pediatric populations.
3. Immunopathophysiology
In atopically or genetically predisposed children, the child’s immune system is already primed for an immediate hypersensitivity response upon any form of subsequent exposure to allergens [37]. In the context of multiple nut allergies, this can occur as a result of ingestion of pathogenic protein consumption or as a result of homologous pathogenic protein consumption from various nut genera. This can occur sequentially or simultaneously and possibly amplify the immune system’s response, increasing risk of severe complications such as anaphylaxis [38].
Cross-reactivity between structurally related tree nuts is a significant contributor to MNA. Phylogenetically related nuts, such as pecan and walnut or cashew and pistachio, share homologous protein epitopes that can promote IgE binding, similar to cross-reactive patterns observed in other foods such as cow and goat milk or legumes [39]. Molecular studies demonstrate that when allergenic proteins share more than 50–60% sequence similarity, this is often enough to cause clinically significant cross-sensitization [40]. For example, the 7S vicilin and 11S legumin families can facilitate cross-linking of IgE on effector cells, due to their repetitive surface epitopes. Similarly, the 2S albumin family of storage proteins enable cross-linking through conserved cysteine residues and disulfide bonds that maintain epitope conformation [41,42]. Cross-reactivity has clinical relevance, contributing to observed patterns of co-sensitization in children, though it represents one mechanism among several underlying MNA rather than a feature unique to nuts [43,44].
The risk of sensitization to multiple nuts is highly modified by genetic and atopic predisposition. A familial history of atopic disorders, including atopic dermatitis, asthma, and allergic rhinitis can exhibit skewed responses favoring Th2 dominance, IgE production and mast cell hyperactivity [45,46]. The likelihood of sensitization is also increased by polymorphisms in genes regulating epithelial barrier function, such as filaggrin (FLG). These polymorphisms can compromise the integrity of cutaneous and mucosal surfaces, which facilitate epicutaneous and gastrointestinal allergen exposure [47]. Similarly, genetic and immunologic variations influence Th2-skewed responses, promoting the development of IgE populations targeting distinct nut allergenic proteins such as 2S albumins, 7S vicilins, and 11S legumins, which underlie the co-sensitization observed in MNA [48]. Children with two or more immediate family members with an allergic disease have an approximately 1.8-fold increased risk of food allergy, which may include MNA, suggesting that familial factors could contribute to the development of MNA [49]. Impaired functionality in regulatory T cells, which typically suppress aberrant Th2 cells, is often reduced in children with nut sensitizations [50]. Additionally, mast cells and basophils in these individuals express lower activation thresholds and enhanced receptor expression, predisposing them to more severe reactions [51].
Finally, molecular allergen profiling and epitope specificity have both gained traction in the understanding of the immunopathophysiology of nut allergies. High-resolution epitope mapping of peanut and walnut allergens in individuals allergic to both nuts identified shared IgE-binding regions, suggesting molecular cross-reactivity between these allergens [52]. Although limited to peanut and walnut allergens, these findings suggest that children with MNA recognize a wider repertoire of epitopes across multiple nuts, which may underlie their enhanced clinical reactivity. The integration of component-resolved diagnostics (CRD) into clinical practice has allowed for clarification as to whether sensitization is due to genuine co-allergy, or just cross-reactivity between homologous proteins; in fact, in studies of hazelnut-sensitized children, measurement of IgE to Cor a 9 and Cor a 14 showed potential in improving specificity in identifying clinically tolerant children among those sensitized to hazelnut [53]. Future research leveraging CRD, immunogenomics, and proteomics holds promise for elucidating novel biomarkers that may be predictive of multiple nut allergies and possibly predict increased anaphylaxis risk in affected children.
Clinical cross-reactivity between different nuts in children was assessed to understand the risk of multiple nut allergies. Table 1 summarizes reported cross-reactivity percentages, representing the proportion of children allergic to the index nut who also reacted to the cross-reactive nut. Cashew and pistachio exhibited the highest cross-reactivity (100%), whereas cross-reactivity among other tree nuts was generally lower, ranging from 0.6% to 21.8% [40,54,55].

Table 1.
Summary of clinically confirmed nut-to-nut cross-reactivity in children [40,54,55].
4. Anaphylaxis Risk
Anaphylaxis is the most severe complication of food allergy, and its occurrence in children with multiple nut allergies is particularly concerning. Comparative studies indicate that children with multiple nut allergies often experience more frequent and more severe systemic reactions than their counterparts with single nut allergies. In a recent pediatric cohort, 81% of nut-allergic patients had multiple nut allergies with 36% of IgE-mediated reactions involving anaphylaxis, and persistence of multiple nut allergies was significantly associated with increased anaphylaxis risk [56]. This, combined with the rise in multiple nut allergies incidence [7], indicates a cause for concern among affected individuals. While both groups are subject to potentially life-threatening outcomes, the clinical trajectory of multiple nut allergies is characterized by higher rates of emergency interventions. Cross-reactivity makes this risk exponentially larger as sensitization to one nut may predispose individuals to a reaction from others, even in the absence of direct exposure to the specific allergen [38]. Consequently, multiple nut allergies does not represent an extension of single nut allergy, but should instead be viewed as a distinct clinical entity with a disproportionately elevated risk of anaphylaxis.
Along with the distinction between a singular nut allergy and multiple nut allergies, clinical studies have identified several other factors that predict the likelihood of severe anaphylactic events in children. In a pediatric cohort undergoing OFCs, the presence of asthma and coexisting multi-food allergy significantly increased the likelihood of challenge failure, suggesting that in children with multiple food allergies (potentially including multiple nut allergies) asthma may exacerbate the risk of adverse reactions [57]. Children with food allergies are two to four times more likely to have asthma than those without food allergies, and asthma is reported in approximately 75 percent of fatal food-related anaphylaxis cases, suggesting that in individuals with nut allergy, coexisting asthma may increase the risk of severe systemic reactions [58].
Another key predictor is elevated allergen-specific IgE titers. Children with MNA often exhibit elevated IgE titers across multiple nuts, which is quantitatively higher than in single nut allergy. In children prone to allergic events, sensitization to multiple allergens is common, and coexisting asthma further increases the risk of severe systemic reactions. In reported fatal or near-fatal food-related allergic reactions, approximately 75% of patients had asthma, highlighting the heightened vulnerability of these children [59]. Children with high-titer IgE responses to major peanut components often have lower reaction thresholds and more severe reactions. With studies showing that combining Ara h 2-specific IgE and a basophil activation marker yielded 92% sensitivity and 82% specificity for predicting severe reactions to peanut [60].
In MNA, wheal sizes across multiple nuts are generally larger than in children with single nut allergy, reflecting broader IgE sensitization to key storage proteins and LTPs, and correlating with higher clinical severity during oral food challenges. Evidence suggests that children with multiple large skin prick test (SPT) responses are more likely to experience severe reactions during oral food challenges. This highlights the cumulative effect of multi-allergen sensitization on clinical risk [56].
However, the strongest predictor of anaphylaxis risk is still a history of prior reactions. In a cohort of children who had previously experienced anaphylaxis, 23.1 percent experienced recurrent reactions to the same allergen [61]. Clinicians can combine a patient’s history of prior anaphylaxis with IgE levels and SPT wheal size to guide dietary management. In children with MNA, prior anaphylactic reactions are particularly concerning as not only are they more susceptible to recurrent attacks, but due to cross-reactivity between nut genera, they are also much more likely to trigger a severe systemic response.
This recognition has direct implications for both risk stratification and management. Avoidance strategies also lead to various emotional, social, educational, and career challenges, ranging from minor inconveniences to significant disruptions [9]. Instead, risk assessment must integrate clinical history with serological and functional biomarkers to generate precision-based profiles of anaphylaxis risk, as emerging tools such as basophil activation tests and bead-based epitope assays offer improved predictive value over IgE alone [62]. Emerging biologic agents, including Omalizumab and Ligelizumab, show promise in targeting IgE and facilitating desensitization. In clinical practice, these agents may be considered for children with MNA who have high-risk profiles, repeated reactions, or limited success with avoidance strategies. These therapeutic approaches may provide disease-modifying options for this subset [63]. Collectively, an integrated biomarker-driven approach offers the most promising avenue for reducing morbidity and mortality in MNA-associated anaphylaxis.
5. Diagnostics and Management
Children with MNA present with a unique clinical challenge regarding diagnostic and management methods as sensitization patterns often overlap. These populations also live with an increased risk of severe reactions and dietary restrictions which can be psychosocially cumbersome [64]. Evaluation typically starts with a thorough clinical history and assessment of reported symptom patterns [65,66]. It is essential to distinguish true IgE-mediated allergy from non-allergic food intolerance or incidental sensitization through precise documentation of the type, timing, and consistency of reactions after nut exposure [67]. The likelihood of a clinically relevant allergen can be determined through acknowledgment of the location of the symptoms or factors such as the amount of allergen ingested and the time to symptom onset [68]. It is crucial to assess a detailed clinical history since it may provide insight on the severity of prior reactions, which is important for risk stratification, particularly in children with MNA who face greater anaphylaxis risk [69].
Skin prick testing is commonly used as an initial test, despite its limited diagnostic accuracy in the context of MNA [70]. False-positive results often occur due to cross-reactivity between related tree nuts, such as cashew and pistachio, which share the vicilin Jug n 2, or between peanuts and Brazil nuts via 2S albumins such as Ara h 2 and Ber e 1, reflecting the high sensitivity but limited specificity of skin prick testing in multiple nut allergies [71,72]. This issue often results in overdiagnosis and unnecessary dietary restrictions. Additionally, children with multiple positive SPT results may tolerate some of the nuts tested, creating diagnostic uncertainty that can be clarified by component-resolved diagnostics, which can identify IgE responses to major storage proteins [73]. Serum allergen-specific IgE (sIgE) is frequently measured to complement SPT, though interpretation can be similarly challenging in MNA [74]. Elevated sIgE corresponds to sensitization and increased likelihood of clinical allergy. In addition, sIgE testing can produce positive results to several nuts even if the child is clinically reactive to only one or two. Thus, this method must be interpreted alongside clinical history [75].
Component-resolved diagnostics is increasingly recognized as a more refined method for differentiating primary sensitization from cross-reactivity. The identification and differentiation of child sensitization is made possible by CRD’s role in testing IgE responses to specific allergenic proteins [53]. These differences are especially relevant for regions with high pollen cross-reactivity, such as hazelnut allergy related to birch pollen. CRD is significantly effective in categorizing which nuts pose true anaphylaxis risk to those that will only produce mild symptoms, improving dietary advice and reducing unnecessary restrictions [76]. Even with progress in diagnostic methods, the gold standard for confirming nut allergy is the oral food challenge (OFC). OFC achieves direct determination of which nuts a sensitized child can tolerate and the clinical reactivity of it [77]. However, OFCs impose consequent risk to children with suspected MNA who have reactivity against multiple allergens. Furthermore, this method is limited because of their resource-intensive nature, requiring close supervision, emergency preparedness, and long duration of monitoring [78,79].
A combination of approaches is necessary to prevent reactions, ensure emergency readiness, and support nutrition and psychosocial well-being in the management of children with MNA. An overly restrictive complete nut avoidance diet is traditionally advised, particularly in children who have broad positive sensitization tests but limited true clinical reactivity [80]. To preserve dietary variety while avoiding exposure to high-risk allergens a selective nut diet approach based on cautious testing is implicated alongside OFC in some cases [81].
Emergency preparedness is vital for children with MNA, since accidental exposure and severe reactions can occur. Epinephrine auto-injectors are mandatorily prescribed to caregivers, teachers, and appropriately aged children trained for correct usage [82]. Written action plans outlining the steps necessary for events of accidental ingestion, recognition of early anaphylaxis symptoms, prompt epinephrine administration, and contacts of emergency services are often accompanied with prescriptions [83]. The complex management of several potential allergens aid for proper dietary counseling. The education of families on careful label reading, possible cross-contamination risks in shared manufacturing facilities, and safe substitution strategies is a necessity [84]. Also, unnecessary restrictions must be emphasized by the clinicians to avoid possible nutrition impairment and food-related anxiety [85]. It is recommended to refer these patients to a registered dietitian to ensure adequate intake of macro and micronutrients including protein, fats, vitamins, and minerals, whilst simultaneously excluding several nuts from their diets [86].
The development of therapies may expand management options beyond simple avoidance. The desensitization and reduction in accidental anaphylaxis cases has been shown to occur when oral immunotherapy (OIT) is executed for peanut allergy. Current studies are planning to extend OIT protocols to tree nuts as well [87]. In recent data, OIT has been indicated to confer cross-desensitization between walnut or cashew to related nuts, though safety and long-term effects remain unexamined [88]. Multi-allergen immunotherapy is a broader approach, aiming to desensitize children to multiple nuts simultaneously. However, the safety of this approach needs to be studied, since risks of adverse reactions during therapy occur as a result of exposure to multiple allergens [89]. The confirmation whether multi-allergen OIT can become a standard part of MNA management is critical and can be achieved through careful dose escalation protocols, patient selection, and close monitoring [90].
Approaches to diagnosing and managing MNA in children must balance safety, accuracy, and life quality. The advancements of CRD and OFCs give rise to refined diagnosis and reduction in unnecessary restrictions, while selective nut introduction and complete emergency preparedness can lower risk without heavy dietary burdens. Immunotherapies offer hope for disease modification in the future, though their correlations with multi-allergen cases are actively being studied. Together, these diagnostic approaches highlight an evolving paradigm that prioritizes individualized care for children with MNA.
6. Conclusions
Multiple nut allergies form a unique and clinically significant group among pediatric populations with food allergy, carrying elevated risk of anaphylaxis and long-term health challenges. The complex diagnosis and management arises from the interplay of genetic predisposition, structural protein homology, and cross-reactive immune responses, further amplifying the risk of sensitization. Compared to children with single nut allergies, children with MNA often experience increased psychosocial stress, dietary risks, and a higher rate of severe systemic reactions occurring. Emerging diagnostic tools and the advancement of targeted therapies contribute to the widespread use of precision-focused and individualized strategies that limit dietary avoidance, reshaping the clinical approach for these children. Nevertheless, critical gaps remain in epidemiological data and long-term results, emphasizing the need for further research. Addressing these gaps is crucial to better assessing risk, optimizing treatment strategies, and ultimately improving the quality of life for children and families affected by MNA.
Author Contributions
Conceptualization, A.T.D.J. and K.A.C.; methodology, K.A.C., A.O. and D.S.; software, A.O. and A.T.D.J.; validation, K.A.C., A.O. and D.S.; formal analysis, K.A.C., A.T.D.J. and D.S.; investigation, A.T.D.J. and A.O.; resources, K.A.C. and A.O.; data curation, A.O. and A.T.D.J.; writing—original draft preparation, A.T.D.J., K.A.C. and D.S.; writing—review and editing, A.T.D.J. and A.O.; visualization, A.O. and K.A.C.; supervision, D.S.; project administration, A.T.D.J. and K.A.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MNA | Multiple nut allergies |
| SNA | Single nut allergy |
| OIT | Oral immunotherapy |
| OFC | Oral food challenge |
| CRD | Component-Resolved Diagnostics |
| sIgE | Serum allergen-specific IgE |
| SPT | Skin prick test |
| IgE | Immunoglobulin E |
| Th2 | T Helper 2 Cell |
| LTP | Lipid Transfer Proteins |
| FLG | Filaggrin |
References
- Yaytokgil, Ş.B.; Çelik, İ.K.; Emeksiz, Z.Ş.; Karaatmaca, B.; Giniş, T.; Aydın, S.A.; Toyran, M.; Mısırlıoğlu, E.D.; Civelek, E. Differences between multi-triggered and single-triggered food anaphylaxis in children: A real life study. Turk. J. Pediatr. 2025, 67, 317–326. [Google Scholar] [CrossRef]
- Elghoudi, A.; Narchi, H. Food allergy in children—The current status and the way forward. World J. Clin. Pediatr. 2022, 11, 253–269. [Google Scholar] [CrossRef] [PubMed]
- Flaks-Manov, N.; Goldshtein, I.; Yanover, C.; Lachover-Roth, I. Mental health risks in children with food allergies: A population-based comparison of food allergies with other chronic conditions. Eur. J. Pediatr. 2025, 184, 483. [Google Scholar] [CrossRef] [PubMed]
- Harries, M. Food Allergy Induced Anaphylaxis: An Overview. Pediatr. Ann. 2025, 54, e47–49. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, J.A.; Gupta, R.S.; Knibb, R.C.; Haselkorn, T.; Tilles, S.; Mack, D.P.; Pouessel, G. The global burden of illness of peanut allergy: A comprehensive literature review. Allergy 2021, 76, 1367–1384. [Google Scholar] [CrossRef]
- Smeekens, J.M.; Bagley, K.; Kulis, M. Tree nut allergies: Allergen homology, cross-reactivity, and implications for therapy. Clin. Exp. Allergy 2018, 48, 762–772. [Google Scholar] [CrossRef]
- Brough, H.A.; Caubet, J.-C.; Mazon, A.; Haddad, D.; Bergmann, M.M.; Wassenberg, J.; Panetta, V.; Gourgey, R.; Radulovic, S.; Nieto, M.; et al. Defining challenge-proven coexistent nut and sesame seed allergy: A prospective multicenter European study. J. Allergy Clin. Immunol. 2020, 145, 1231–1239. [Google Scholar] [CrossRef]
- Kachru, R. Psychosocial issues and quality of life associated with food allergy. J. Food Allergy 2020, 2, 95–98. [Google Scholar] [CrossRef]
- Oehrlein, E.; Schoch, S.C.; Escontrías, O.A.; Carver, M.; Eftekhari, S.; Marvel, J.; Pashos, C.L.; Pistiner, M.; Rutta, R.; Voss, J.; et al. US food allergy patients’ experiences, priorities, and needs: A qualitative study. J. Allergy Clin. Immunol. Glob. 2025, 4, 100482. [Google Scholar] [CrossRef]
- Wong, G.W.-K. Food allergies around the world. Front. Nutr. 2024, 11, 1373110. [Google Scholar] [CrossRef]
- Muraro, A.; Sublett, J.W.; Haselkorn, T.; Nilsson, C.; Casale, T.B. Incidence of anaphylaxis and accidental peanut exposure: A systematic review. Clin. Transl. Allergy 2021, 11, e12064. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, T.; Sicherer, S. Current perspectives on tree nut allergy: A review. J. Asthma Allergy 2018, 11, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Abrams, E.M.; Sicherer, S.H. Tree nut introduction in a peanut-allergic child: To eat, to screen, or to avoid? Pediatr. Allergy Immunol. 2022, 33, e13669. [Google Scholar] [CrossRef] [PubMed]
- Chudoba, A.; Żebrowska, A.; Sybilski, A.J. Tree Nut Allergy in Children—What Do We Know?—A Review. Nutrients 2024, 16, 3978. [Google Scholar] [CrossRef]
- Sicherer, S.H.; Muñoz-Furlong, A.; Godbold, J.H.; Sampson, H.A. US prevalence of self-reported peanut, tree nut, and sesame allergy: 11-year follow-up. J. Allergy Clin. Immunol. 2010, 125, 1322–1326. [Google Scholar] [CrossRef]
- Datema, M.R.; Zuidmeer-Jongejan, L.; Asero, R.; Barreales, L.; Belohlavkova, S.; De Blay, F.; Bures, P.; Clausen, M.; Dubakiene, R.; Gislason, D.; et al. Hazelnut allergy across Europe dissected molecularly: A EuroPrevall outpatient clinic survey. J. Allergy Clin. Immunol. 2015, 136, 382–391. [Google Scholar] [CrossRef]
- van der Valk, J.P.M.; Dubois, A.E.J.; Gerth van Wijk, R.; Wichers, H.J.; de Jong, N.W. Systematic review on cashew nut allergy. Allergy 2014, 69, 692–698. [Google Scholar] [CrossRef]
- Noorbakhsh, R.; Mortazavi, S.A.; Sankian, M.; Shahidi, F.; Tehrani, M.; Azad, F.J.; Behmanesh, F.; Varasteh, A. Pistachio allergy-prevalence and in vitro cross-reactivity with other nuts. Allergol. Int. 2011, 60, 425–432. [Google Scholar] [CrossRef]
- Warren, C.; Turner, P.J.; Chinthrajah, R.S.; Gupta, R. Advancing food allergy through epidemiology: Understanding and addressing disparities in food allergy management and outcomes. J. Allergy Clin. Immunol. Pract. 2021, 9, 110–118. [Google Scholar] [CrossRef]
- Lange, L.; Klimek, L.; Beyer, K.; Blümchen, K.; Novak, N.; Hamelmann, E.; Bauer, A.; Merk, H.; Rabe, U.; Jung, K.; et al. White paper on peanut allergy—Part 1: Epidemiology, burden of disease, health economic aspects. Allergo J. Int. 2021, 30, 261–269. [Google Scholar] [CrossRef]
- McWilliam, V.; Peters, R.; Tang, M.L.K.; Dharmage, S.; Ponsonby, A.-L.; Gurrin, L.; Perrett, K.; Koplin, J.; Allen, K.J.; Dwyer, T.; et al. Patterns of tree nut sensitization and allergy in the first 6 years of life in a population-based cohort. J. Allergy Clin. Immunol. 2019, 143, 644–650.e5. [Google Scholar] [CrossRef]
- Leung, A.S.; Jie, S.; Gu, Y.; Wong, G.W. Food Allergy in Children in China. Clin. Exp. Allergy 2025, 55, 634–647. [Google Scholar] [CrossRef] [PubMed]
- Skolnick, H.S.; Conover-Walker, M.K.; Koerner, C.B.; Sampson, H.A.; Burks, W.; Wood, R.A. The natural history of peanut allergy. J. Allergy Clin. Immunol. 2001, 107, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Van Erp, F.C.; Knulst, A.C.; Kok, I.L.; van Velzen, M.F.; van der Ent, C.K.; Meijer, Y. Usefulness of open mixed nut challenges to exclude tree nut allergy in children. Clin. Transl. Allergy 2015, 5, 19. [Google Scholar] [CrossRef] [PubMed]
- Herbert, L.J.; Dahlquist, L.M. Perceived history of anaphylaxis and parental overprotection, autonomy, anxiety, and depression in food allergic young adults. J. Clin. Psychol. Med. Settings 2008, 15, 261–269. [Google Scholar] [CrossRef]
- Venkataraman, D.; Erlewyn-Lajeunesse, M.; Kurukulaaratchy, R.J.; Potter, S.; Roberts, G.; Matthews, S.; Arshad, S.H. Prevalence and longitudinal trends of food allergy during childhood and adolescence: Results of the Isle of Wight Birth Cohort study. Clin. Exp. Allergy 2018, 48, 394–402. [Google Scholar] [CrossRef]
- Sakakini, J.; Irani, C.; Bikai, R.; Sahyoun, G.; Hallit, S.; Salameh, P.; Dano, D. Prevalence of Food Allergy among Schoolchildren in Lebanon. Int. Arch. Allergy Immunol. 2022, 183, 611–616. [Google Scholar] [CrossRef]
- Alibrahim, I.; AlSulami, M.; Alotaibi, T.; Alotaibi, R.; Bahareth, E.; Abulreish, I.; Alsuruji, S.; Khojah, I.; Goronfolah, L.; Rayes, H.; et al. Prevalence of Parent-Reported Food Allergies Among Children in Saudi Arabia. Nutrients 2024, 16, 2693. [Google Scholar] [CrossRef]
- Du Toit, G.; Katz, Y.; Sasieni, P.; Mesher, D.; Maleki, S.J.; Fisher, H.R.; Fox, A.T.; Turcanu, V.; Amir, T.; Zadik-Mnuhin, G.; et al. Early consumption of peanuts in infancy is associated with a low prevalence of peanut allergy. J. Allergy Clin. Immunol. 2008, 122, 984–991. [Google Scholar] [CrossRef]
- Kojima, R.; Shinohara, R.; Kushima, M.; Yui, H.; Otawa, S.; Horiuchi, S.; Miyake, K.; Yokomichi, H.; Akiyama, Y.; Ooka, T.; et al. Infantile Peanut Introduction and Peanut Allergy in Regions with a Low Prevalence of Peanut Allergy: The Japan Environment and Children’s Study (JECS). J. Epidemiol. 2024, 34, 324–330. [Google Scholar] [CrossRef]
- Prescott, S.L.; Pawankar, R.; Allen, K.J.; E Campbell, D.; Sinn, J.K.; Fiocchi, A.; Ebisawa, M.; A Sampson, H.; Beyer, K.; Lee, B.-W. A global survey of changing patterns of food allergy burden in children. World Allergy Organ. J. 2013, 6, 21. [Google Scholar] [CrossRef] [PubMed]
- Soriano, V.X.; Peters, R.L.; Moreno-Betancur, M.; Ponsonby, A.L.; Gell, G.; Odoi, A.; Perrett, K.P.; Tang, M.L.K.; Gurrin, L.C.; Allen, K.J.; et al. Association Between Earlier Introduction of Peanut and Prevalence of Peanut Allergy in Infants in Australia. JAMA 2022, 328, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Shek, L.P.; Cabrera-Morales, E.A.; Soh, S.E.; Gerez, I.; Ng, P.Z.; Yi, F.C.; Ma, S.; Lee, B.W. A population-based questionnaire survey on the prevalence of peanut, tree nut, and shellfish allergy in 2 Asian populations. J. Allergy Clin. Immunol. 2010, 126, 324–331, 331.e1–7. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.P.; Saffari, S.E.; Loh, W.; Goh, S.H.; Goh, A.; Chiang, W.C.; Chong, K.W. A 5-year retrospective review of children with peanut allergy in the largest paediatric hospital in Singapore. Asia Pac. Allergy 2020, 10, e6. [Google Scholar] [CrossRef]
- Ontiveros, N.; Valdez-Meza, E.E.; Vergara-Jiménez, M.J.; Canizalez-Román, A.; Borzutzky, A.; Cabrera-Chávez, F. Parent-reported prevalence of food allergy in Mexican schoolchildren: A population-based study. Allergol. Immunopathol. 2016, 44, 563–570. [Google Scholar] [CrossRef]
- Singer, A.G.; Kosowan, L.; Soller, L.; Chan, E.S.; Nankissoor, N.N.; Phung, R.R.; Abrams, E.M. Prevalence of Physician-Reported Food Allergy in Canadian Children. J. Allergy Clin. Immunol. Pract. 2021, 9, 193–199. [Google Scholar] [CrossRef]
- Galli, S.J.; Tsai, M. IgE and mast cells in allergic disease. Nat. Med. 2012, 18, 693–704. [Google Scholar] [CrossRef]
- Lomas, J.M.; Järvinen, K.M. Managing nut-induced anaphylaxis: Challenges and solutions. J. Asthma Allergy 2015, 8, 115–123. [Google Scholar] [CrossRef]
- Kamath, S.D.; Bublin, M.; Kitamura, K.; Matsui, T.; Ito, K.; Lopata, A.L. Cross-reactive epitopes and their role in food allergy. J. Allergy Clin. Immunol. 2023, 151, 1178–1190. [Google Scholar] [CrossRef]
- Juel-Berg, N.; Larsen, L.F.; Küchen, N.; Norgil, I.; Hansen, K.S.; Poulsen, L.K. Patterns of Clinical Reactivity in a Danish Cohort of Tree Nut Allergic Children, Adolescents, and Young Adults. Front. Allergy 2022, 3, 824660. [Google Scholar] [CrossRef]
- Moreno, F.J.; Clemente, A. 2S Albumin Storage Proteins: What Makes them Food Allergens? Open Biochem. J. 2008, 2, 16–28. [Google Scholar] [CrossRef] [PubMed]
- Kabasser, S.; Pratap, K.; Kamath, S.; Taki, A.C.; Dang, T.; Koplin, J.; Perrett, K.; Hummel, K.; Radauer, C.; Breiteneder, H.; et al. Identification of vicilin, legumin and antimicrobial peptide 2a as macadamia nut allergens. Food Chem. 2022, 370, 131028. [Google Scholar] [CrossRef] [PubMed]
- Dreskin, S.C.; Koppelman, S.J.; Andorf, S.; Nadeau, K.C.; Kalra, A.; Braun, W.; Negi, S.S.; Chen, X.; Schein, C.H. The importance of the 2S albumins for allergenicity and cross-reactivity of peanuts, tree nuts, and sesame seeds. J. Allergy Clin. Immunol. 2021, 147, 1154–1163. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Lopez, J.C.; Zafra, A.; Palanco, L.; Florido, J.F.; Alché Jde, D. Identification and Assessment of the Potential Allergenicity of 7S Vicilins in Olive (Olea europaea L.) Seeds. Biomed. Res. Int. 2016, 2016, 4946872. [Google Scholar] [CrossRef]
- Lu, Y.; Sun, L.; Li, C.; Wang, X.; Li, W.; Zhao, T.; Huang, L.; Wang, Z. Comparative mass spectrometry analysis of N-glycans from the glycoproteins of eight allergy-inducing plants. Food Chem. 2022, 384, 132440. [Google Scholar] [CrossRef]
- Vaseghi-Shanjani, M.; Samra, S.; Yousefi, P.; Biggs, C.M.; Turvey, S.E. Primary atopic disorders: Inborn errors of immunity causing severe allergic disease. Curr. Opin. Immunol. 2025, 94, 102538. [Google Scholar] [CrossRef]
- Dębińska, A.; Sozańska, B. Epicutaneous Sensitization and Food Allergy: Preventive Strategies Targeting Skin Barrier Repair—Facts and Challenges. Nutrients 2023, 15, 1070. [Google Scholar] [CrossRef]
- Ashley, S.E.; Tan, H.T.; Peters, R.; Allen, K.J.; Vuillermin, P.; Dharmage, S.C.; Tang, M.L.K.; Koplin, J.; Lowe, A.; Ponsonby, A.L.; et al. Genetic variation at the Th2 immune gene IL13 is associated with IgE-mediated paediatric food allergy. Clin. Exp. Allergy 2017, 47, 1032–1037. [Google Scholar] [CrossRef]
- Koplin, J.J.; Allen, K.J.; Gurrin, L.C.; Peters, R.L.; Lowe, A.J.; Tan, H.-T.T.; Dharmage, S.C. The Impact of Family History of Allergy on Risk of Food Allergy: A Population-Based Study of Infants. Int. J. Env. Res. Public. Health 2013, 10, 5364–5377. [Google Scholar] [CrossRef]
- Rivas, M.N.; Chatila, T.A. Regulatory T cells in Allergic Diseases. J. Allergy Clin. Immunol. 2016, 138, 639–652. [Google Scholar] [CrossRef]
- Imamura, S.; Washio, K.; Mizuno, M.; Oda, Y.; Fukunaga, A.; Nishigori, C. Activated steady status and distinctive FcεRI-mediated responsiveness in basophils of atopic dermatitis. Allergol. Int. 2021, 70, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Rambo, I.; Swientoniewski, L.; Rivers, A.; Cheng, H.; McBride, J.; Nesbit, J.; Kulis, M.; Maleki, S. Epitope maps of the peanut and walnut allergens in a 3D spatial context. J. Allergy Clin. Immunol. 2025, 155, AB42. [Google Scholar] [CrossRef]
- Caffarelli, C.; Mastrorilli, C.; Santoro, A.; Criscione, M.; Procaccianti, M. Component-Resolved Diagnosis of Hazelnut Allergy in Children. Nutrients 2021, 13, 640. [Google Scholar] [CrossRef] [PubMed]
- Cousin, M.; Verdun, S.; Seynave, M.; Vilain, A.; Lansiaux, A.; Decoster, A.; Sauvage, C. Phenotypical characterization of peanut allergic children with differences in cross-allergy to tree nuts and other legumes. Pediatr. Allergy Immunol. 2017, 28, 245–250. [Google Scholar] [CrossRef]
- Chitta, S.; Lian, B.X.; Rao, R.; Loh, W.; Goh, A.; Chong, K.W. Cashew nut allergy in Singaporean children. Asia Pac. Allergy 2018, 8, e29. [Google Scholar] [CrossRef]
- Baysal Bakır, D.; Atay, Ö.; Yağmur, H.; Kabadayı, G.; Kangallı Boyacıoğlu, Ö.; Atakul, G.; Asilsoy, S.; Uzuner, N. From Sensitisation to Tolerance: A Retrospective Study of Tree Nut and Peanut Allergy in Pediatric Patients. Int. Arch. Allergy Immunol. 2025, 10, 1–15. [Google Scholar] [CrossRef]
- Klim, L.; Michalik, M.; Cichocka-Jarosz, E.; Jedynak-Wąsowicz, U. Asthma and Multi-Food Allergy Are Risk Factors for Oral Food Challenge Failure—A Single-Center Experience. Nutrients 2025, 17, 2769. [Google Scholar] [CrossRef]
- Chan, A.; Yu, J.E. Food allergy and asthma. J. Food Allergy 2020, 2, 44–47. [Google Scholar] [CrossRef]
- Wang, J.; Liu, A.H. Food allergies and asthma. Curr. Opin. Allergy Clin. Immunol. 2011, 11, 249–254. [Google Scholar] [CrossRef]
- Cottel, N.; Saf, S.; Bourgoin-Heck, M.; Lambert, N.; Amat, F.; Poncet, P.; Senechal, H.; Couderc, R.; Just, J.; Chantran, Y. Two Different Composite Markers Predict Severity and Threshold Dose in Peanut Allergy. J. Allergy Clin. Immunol. Pract. 2021, 9, 275–282.e1. [Google Scholar] [CrossRef]
- Lee, S.-Y.; Ahn, K.; Kim, J.; Jang, G.C.; Min, T.K.; Yang, H.-J.; Pyun, B.Y.; Kwon, J.-W.; Sohn, M.H.; Kim, K.W.; et al. A Multicenter Retrospective Case Study of Anaphylaxis Triggers by Age in Korean Children. Allergy Asthma Immunol. Res. 2016, 8, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Fitzhugh, D.J. Prediction of food allergy reaction severity: Biomarkers and host factors. Front. Allergy 2025, 6, 1578601. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, J.P.; Anderson, B.; Sindher, S.B. New biologics for food allergy. Curr. Opin. Allergy Clin. Immunol. 2024, 24, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Herbert, L.; Shemesh, E.; Bender, B. Clinical Management of Psychosocial Concerns Related to Food Allergy. J. Allergy Clin. Immunol. Pract. 2016, 4, 205–213; quiz 214. [Google Scholar] [CrossRef]
- Wasserman, R.L. A diagnostic approach to IgE-mediated food allergy: A practical algorithm. J. Food Allergy 2024, 6, 15–20. [Google Scholar] [CrossRef]
- Manea, I.; Ailenei, E.; Deleanu, D. Overview of food allergy diagnosis. Clujul Med. 2016, 89, 5–10. [Google Scholar] [CrossRef]
- Sampson, H.A.; Aceves, S.; Bock, S.A.; James, J.; Jones, S.; Lang, D.; Nadeau, K.; Nowak-Wegrzyn, A.; Oppenheimer, J.; Perry, T.T.; et al. Food allergy: A practice parameter update-2014. J. Allergy Clin. Immunol. 2014, 134, 1016–1025.e43. [Google Scholar] [CrossRef]
- Muraro, A.; Werfel, T.; Hoffmann-Sommergruber, K.; Roberts, G.; Beyer, K.; Bindslev-Jensen, C.; Cardona, V.; Dubois, A.; Dutoit, G.; Eigenmann, P.; et al. EAACI food allergy and anaphylaxis guidelines: Diagnosis and management of food allergy. Allergy 2014, 69, 1008–1025. [Google Scholar] [CrossRef]
- Turner, P.J.; Arasi, S.; Ballmer-Weber, B.; Conrado, A.B.; Deschildre, A.; Gerdts, J.; Halken, S.; Muraro, A.; Patel, N.; Van Ree, R.; et al. Risk factors for severe reactions in food allergy: Rapid evidence review with meta-analysis. Allergy 2022, 77, 2634–2652. [Google Scholar] [CrossRef]
- Ho, M.H.K.; Heine, R.G.; Wong, W.; Hill, D.J. Diagnostic accuracy of skin prick testing in children with tree nut allergy. J. Allergy Clin. Immunol. 2006, 117, 1506–1508. [Google Scholar] [CrossRef]
- Sicherer, S.H. Clinical implications of cross-reactive food allergens. J. Allergy Clin. Immunol. 2001, 108, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Muller, T.; Luc, A.; Adam, T.; Jarlot-Chevaux, S.; Dumond, P.; Schweitzer, C.; Codreanu-Morel, F.; Divaret-Chauveau, A. Relevance of sensitization to legumes in peanut-allergic children. Pediatr. Allergy Immunol. 2022, 33, e13846. [Google Scholar] [CrossRef] [PubMed]
- Połomska, J.; Dydak, P.; Sozańska, B.; Sikorska-Szaflik, H. Peanut Allergy and Component-Resolved Diagnostics Possibilities—What Are the Benefits? Nutrients 2023, 15, 5132. [Google Scholar] [CrossRef]
- Corsico, A.G.; De Amici, M.; Ronzoni, V.; Giunta, V.; Mennitti, M.C.; Viscardi, A.; Marseglia, G.L.; Ciprandi, G. Allergen-specific immunoglobulin E and allergic rhinitis severity. Allergy Rhinol. 2017, 8, e1–e4. [Google Scholar] [CrossRef] [PubMed]
- Foong, R.X.; Dantzer, J.A.; Wood, R.A.; Santos, A.F. Improving Diagnostic Accuracy in Food Allergy. J. Allergy Clin. Immunol. Pract. 2021, 9, 71–80. [Google Scholar] [CrossRef]
- Calamelli, E.; Liotti, L.; Beghetti, I.; Piccinno, V.; Serra, L.; Bottau, P. Component-Resolved Diagnosis in Food Allergies. Medicina 2019, 55, 498. [Google Scholar] [CrossRef]
- Hsu, C.; Yong, M.; Pozin, J.; Makhija, M.; Singh, A.M. Clinical Predictors and Outcomes of Oral Food Challenges Illustrate Differences Among Individual Tree Nuts. J. Allergy Clin. Immunol. Pract. 2021, 9, 3728–3734.e1. [Google Scholar] [CrossRef]
- de Weger, W.W.; Sprikkelman, A.B.; Herpertz, C.E.M.; van der Meulen, G.N.; Vonk, J.M.; Koppelman, G.H.; Kamps, A.W.A. Comparison of Double-Blind and Open Food Challenges for the Diagnosis of Food Allergy in Childhood: The ALDORADO Study. Allergy 2025, 80, 248–257. [Google Scholar] [CrossRef]
- Cela, L.; Gravina, A.; Semeraro, A.; Pastore, F.; Morelli, R.; Marchetti, L.; Brindisi, G.; Olivero, F.; Piccioni, M.G.; Zicari, A.M.; et al. Oral Food Challenge in Children with Tree Nut and Peanut Allergy: The Predictive Value of Diagnostic Tests. Diagnostics 2024, 14, 2069. [Google Scholar] [CrossRef]
- Borres, M.P.; Sato, S.; Ebisawa, M. Recent advances in diagnosing and managing nut allergies with focus on hazelnuts, walnuts, and cashew nuts. World Allergy Organ. J. 2022, 15, 100641. [Google Scholar] [CrossRef]
- Brough, H.A.; Gourgey, R.; Radulovic, S.; Caubet, J.C.; Lack, G.; Anagnostou, A. Latest Developments in the Management of Nut Allergies. Curr. Treat. Options Allergy 2021, 8, 97–110. [Google Scholar] [CrossRef]
- Coombs, R.; Simons, E.; Foty, R.G.; Stieb, D.M.; Dell, S.D. Socioeconomic factors and epinephrine prescription in children with peanut allergy. Paediatr. Child. Health 2011, 16, 341–344. [Google Scholar] [CrossRef]
- Wang, J.; Sicherer, S.H.; Immunology, S.O.A.A.; Matsui, E.; Abramson, S.; Dinakar, C.; Irani, A.-M.; Kim, J.S.; Mahr, T.A.; Pistiner, M. Guidance on Completing a Written Allergy and Anaphylaxis Emergency Plan. Pediatrics 2017, 139, e20164005. [Google Scholar] [CrossRef] [PubMed]
- Rancé, P.; Bidat, E. Educational program for children with peanut allergy. Allerg. Immunol. 2000, 32, 209–211. [Google Scholar]
- Kotchetkoff, E.C.A.; de Oliveira, L.C.L.; Sarni, R.O.S. Elimination diet in food allergy: Friend or foe? J. Pediatr. 2023, 100, S65–S73. [Google Scholar] [CrossRef] [PubMed]
- Groetch, M.E.; Christie, L.; Vargas, P.A.; Jones, S.M.; Sicherer, S.H. Food Allergy Educational Needs of Pediatric Dietitians: A survey by the Consortium of Food Allergy Research. J. Nutr. Educ. Behav. 2010, 42, 259–264. [Google Scholar] [CrossRef]
- Sheikh, A.; Nurmatov, U.; Venderbosch, I.; Bischoff, E. Oral immunotherapy for the treatment of peanut allergy: Systematic review of six case series studies. Prim. Care Respir. J. 2012, 21, 41–49. [Google Scholar] [CrossRef]
- Erdle, S.; Cook, V.E. A practical focus on oral immunotherapy to tree nuts. J. Food Allergy 2022, 4, 120–126. [Google Scholar] [CrossRef]
- Calderón, M.A.; Cox, L.; Casale, T.B.; Moingeon, P.; Demoly, P. Multiple-allergen and single-allergen immunotherapy strategies in polysensitized patients: Looking at the published evidence. J. Allergy Clin. Immunol. 2012, 129, 929–934. [Google Scholar] [CrossRef]
- McHenry, M.; Bégin, P.; Chan, E.S.; Latrous, M.; Kim, H. Food oral immunotherapy. Allergy Asthma Clin. Immunol. 2025, 20, 82. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).