
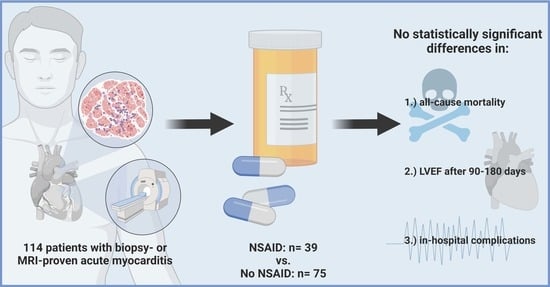
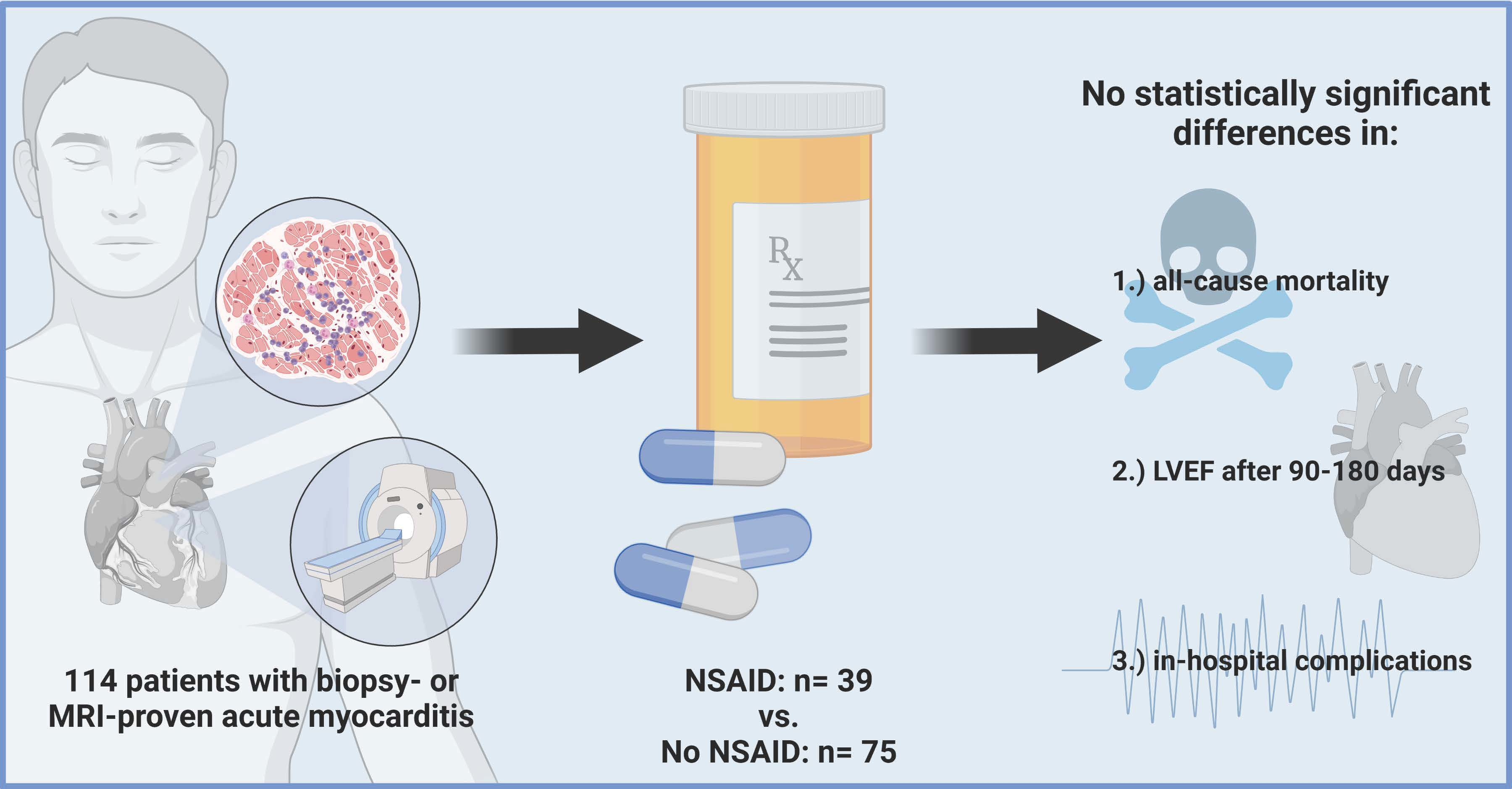
Treatment with Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) Does Not Affect Outcome in Patients with Acute Myocarditis or Myopericarditis

 ,
,  ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Primary and Secondary Study Endpoints
2.3. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Primary and Secondary Study Endpoints before Propensity Score Matching
3.2.1. All-Cause Mortality within Follow-Up
3.2.2. In-Hospital Complications
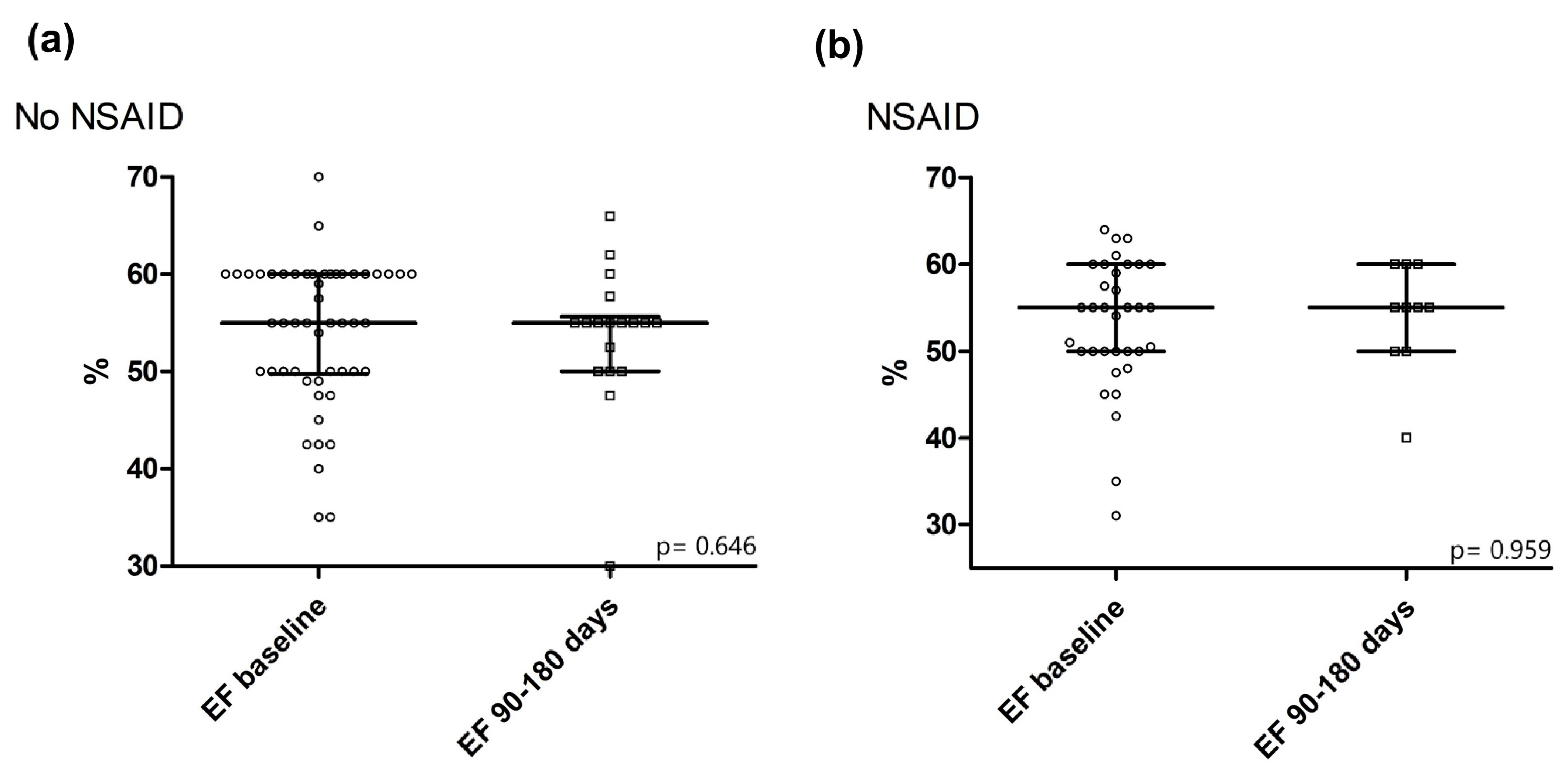
3.2.3. LVEF after 90–180 Days
3.3. Primary and Secondary Study Endpoints after Propensity Score Matching
4. Discussion
Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schwier, N.; Tran, N. Non-Steroidal Anti-Inflammatory Drugs and Aspirin Therapy for the Treatment of Acute and Recurrent Idiopathic Pericarditis. Pharmaceuticals 2016, 9, 17. [Google Scholar] [CrossRef] [Green Version]
- Imazio, M.; Adler, Y. Treatment with aspirin, NSAID, corticosteroids, and colchicine in acute and recurrent pericarditis. Heart Fail. Rev. 2012, 18, 355–360. [Google Scholar] [CrossRef]
- Tonini, M.; De Melo, D.T.P.; Fernandes, F. Acute pericarditis. Rev. Assoc. Med. Bras. 2015, 61, 184–190. [Google Scholar]
- Monzonís, A.M.; García, O.O.; Johk, C.A.; Juanatey, A.G.C. Acute pericarditis. Medicine 2021, 13, 2495–2507. [Google Scholar]
- Caforio, A.L.P.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef]
- Meune, C.; Spaulding, C.; Mahé, I.; Lebon, P.; Bergmann, J.-F. Risks versus Benefits of NSAIDs Including Aspirin in Myocarditis. Drug Saf. 2003, 26, 975–981. [Google Scholar] [CrossRef]
- Costanzo-Nordin, M.R.; Reap, E.A.; O’Connell, J.B.; Robinson, J.A.; Scanlon, P.J. A nonsteroid anti-inflammatory drug exacerbates coxsackie B3 murine myocarditis. J. Am. Coll. Cardiol. 1985, 6, 1078–1082. [Google Scholar] [CrossRef] [Green Version]
- Khatib, R.; Reyes, M.P.; Smith, F.; Khatib, G.; Rezkalla, S. Enhancement of coxsackievirus B4 virulence by indomethacin. J. Lab. Clin. Med. 1990, 116, 116–120. [Google Scholar]
- Rezkalla, S.; Khatib, G.; Khatib, R. Coxsackievirus B3 murine myocarditis: Deleterious effects of nonsteroidal anti-inflammatory agents. J. Lab. Clin. Med. 1986, 107, 393–395. [Google Scholar]
- Mirna, M.; Paar, V.; Topf, A.; Kraus, T.; Sotlar, K.; Aigner, A.; Ewe, A.; Watzinger, S.; Podesser, B.K.; Hackl, M.; et al. A new player in the game: Treatment with antagomiR-21a-5p significantly attenuates histological and echocardiographic effects of experimental autoimmune myocarditis. Cardiovasc. Res. 2021. [Google Scholar] [CrossRef]
- Sagar, S.; Liu, P.P.; Cooper, L.T. Myocarditis. Lancet 2012, 379, 738–747. [Google Scholar]
- Imazio, M.; Cooper, L.T. Management of myopericarditis. Expert Rev Cardiovasc Ther 2013, 11, 193–201. [Google Scholar]
- Adler, Y.; Charron, P.; Imazio, M.; Badano, L.; Barón-Esquivias, G.; Bogaert, J.; Brucato, A.; Gueret, P.; Klingel, K.; Lionis, C.; et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur. Heart J. 2015, 36, 2921–2964. [Google Scholar] [CrossRef]
- Buiatti, A.; Merlo, M.; Pinamonti, B.; De Biasio, M.; Bussani, R.; Sinagra, G. Clinical presentation and long-term follow-up of perimyocarditis. J. Cardiovasc. Med. 2013, 14, 235–241. [Google Scholar] [CrossRef]
- Imazio, M.; Brucato, A.; Barbieri, A.; Ferroni, F.; Maestroni, S.; Ligabue, G.; Chinaglia, A.; Cumetti, D.; Della Casa, G.; Bonomi, F.; et al. Good prognosis for pericarditis with and without myocardial involvement: Results from a multicenter, prospective cohort study. Circulation 2013, 128, 42–49. [Google Scholar]
- Berg, J.; Lovrinovic, M.; Baltensperger, N.; Kissel, C.K.; Kottwitz, J.; Manka, R.; Patriki, D.; Scherff, F.; Schmied, C.; Landmesser, U.; et al. Non-steroidal anti-inflammatory drug use in acute myopericarditis: 12-month clinical follow-up. Open Heart 2019, 6, e000990. [Google Scholar] [CrossRef] [Green Version]
- Little, W.C.; Freeman, G.L. Pericardial disease. Circulation 2006, 113, 1622–1632. [Google Scholar]
- Yang, F.; Wang, J.; Li, W.; Xu, Y.; Wan, K.; Zeng, R.; Chen, Y. The prognostic value of late gadolinium enhancement in myocarditis and clinically suspected myocarditis: Systematic review and meta-analysis. Eur. Radiol. 2020, 30, 2616–2626. [Google Scholar] [CrossRef]
- Georgiopoulos, G.; Figliozzi, S.; Sanguineti, F.; Aquaro, G.D.; di Bella, G.; Stamatelopoulos, K.; Chiribiri, A.; Garot, J.; Masci, P.G.; Ismail, T.F. Prognostic Impact of Late Gadolinium Enhancement by Cardiovascular Magnetic Resonance in Myocarditis: A Systematic Review and Meta-Analysis. Circ. Cardiovasc. Imaging 2021, 14, e011492. [Google Scholar]
- Mirna, M.; Paar, V.; Rezar, R.; Topf, A.; Eber, M.; Hoppe, U.C.; Lichtenauer, M.; Jung, C. MicroRNAs in Inflammatory Heart Diseases and Sepsis-Induced Cardiac Dysfunction: A Potential Scope for the Future? Cells 2019, 8, 1352. [Google Scholar]
- Zavodovsky, B.V.; Sivordova, L.E. Cardiovascular safety of non-steroidal anti-inflammatory drugs in chronic inflammatory rheumatic diseases. Ter. Arkhiv 2018, 90, 101–106. [Google Scholar]
- Bindu, S.; Mazumder, S.; Bandyopadhyay, U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: A current perspective. Biochem. Pharmacol. 2020, 180, 114147. [Google Scholar] [CrossRef]
- Tai, F.W.D.; McAlindon, M.E. Non-steroidal anti-inflammatory drugs and the gastrointestinal tract. Clin. Med. 2021, 21, 131–134. [Google Scholar] [CrossRef]
- Ruschitzka, F.; Borer, J.S.; Krum, H.; Flammer, A.J.; Yeomans, N.D.; Libby, P.; Lüscher, T.F.; Solomon, D.H.; Husni, M.E.; Graham, D.Y.; et al. Differential blood pressure effects of ibuprofen, naproxen, and celecoxib in patients with arthritis: The PRECISION-ABPM (Prospective Randomized Evaluation of Celecoxib Integrated Safety Versus Ibuprofen or Naproxen Ambulatory Blood Pressure Measurement) Trial. Eur. Heart J. 2017, 38, 3282–3292. [Google Scholar] [CrossRef] [Green Version]
- Whelton, A.; Hamilton, C.W. Nonsteroidal Anti-Inflammatory Drugs: Effects on Kidney Function. J. Clin. Pharmacol. 1991, 31, 588–598. [Google Scholar] [CrossRef]
- Roubille, C.; Martel-Pelletier, J.; Davy, J.-M.; Haraoui, B.; Pelletier, J.-P. Cardiovascular adverse effects of anti-inflammatory drugs. Anti-Inflamm. Anti-Allergy Agents Med. Chem. 2013, 12, 55–67. [Google Scholar] [CrossRef]
- Bacchi, S.; Palumbo, P.; Sponta, A.; Coppolino, M. Clinical Pharmacology of Non-Steroidal Anti-Inflammatory Drugs: A Review. Anti-Inflamm. Anti-Allergy Agents Med. Chem. 2012, 11, 52–64. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NSAID (n = 39) | No NSAID (n = 75) | ||||
|---|---|---|---|---|---|
| Baseline characteristics | median | IQR | median | IQR | p-value |
| Age (years) | 29 | 21–38 | 37 | 27–49 | 0.005 |
| % | n | % | n | p-value | |
| Myopericarditis | 61.5 | 24 | 25.3 | 19 | <0.0001 |
| Male sex | 84.6 | 33 | 77.3 | 58 | 0.463 |
| Diabetes mellitus | 0.0 | 0 | 1.3 | 1 | 0.658 |
| Hyperlipidemia | 12.8 | 5 | 17.3 | 13 | 0.599 |
| Obesity (BMI >30 kg/m2) | 15.4 | 6 | 12.0 | 9 | 0.771 |
| Arterial hypertension | 10.3 | 4 | 17.3 | 13 | 0.411 |
| History of smoking | 28.2 | 11 | 34.7 | 26 | 0.533 |
| Coronary artery disease | 2.6 | 1 | 1.3 | 1 | 0.569 |
| Cerebral artery disease | 0.0 | 0 | 1.3 | 1 | 0.658 |
| Peripheral artery disease | 0.0 | 0 | 0.0 | 0 | NA |
| Chronic infectious disease | 0.0 | 0 | 0.0 | 0 | NA |
| Autoimmune disease | 7.1 | 3 | 6.9 | 5 | 0.621 |
| Active malignancy | 2.4 | 1 | 1.4 | 1 | 0.454 |
| Laboratory data | median | IQR | median | IQR | p-value |
| Serum creatinine (mg/dL) | 0.90 | 0.78–1.10 | 0.90 | 0.80–1.00 | 0.987 |
| CRP (mg/dL) | 7.35 | 1.45–12.55 | 1.90 | 0.60–6.45 | 0.004 |
| Bilirubin (mg/dL) | 0.55 | 0.43–0.88 | 0.60 | 0.40–0.88 | 0.972 |
| Creatinine kinase (CK) (IU/L) | 240 | 114–528 | 260 | 130–451 | 0.902 |
| CK-MB (%) | 9.35 | 6.98–11.23 | 10.90 | 8.30–13.90 | 0.192 |
| High-sensitivity troponin (hsTnT) (ng/L) | 417 | 195–1043 | 216 | 30–584 | 0.059 |
| Pro brain natriuretic peptide (pBNP) (ng/L) | 503 | 238–1220 | 278 | 122–780 | 0.164 |
| Hemoglobin (mg/dL) | 14.60 | 13.20–15.75 | 14.65 | 13.63–15.68 | 0.964 |
| Leukocyte count (G/L) | 9.85 | 7.62–13.11 | 7.87 | 6.49–11.23 | 0.048 |
| Thrombocyte count (G/L) | 210 | 198–252 | 219 | 172–261 | 0.580 |
| Initial ECG and TTE | % | n | % | n | p-value |
| ECG changes | 76.3 | 29 | 68.9 | 51 | 0.510 |
| ST-seg. elevation | 58.6 | 17 | 54.0 | 27 | 0.815 |
| ST-seg. depression | 24.1 | 7 | 24.0 | 12 | 0.989 |
| median | IQR | median | IQR | p-value | |
| LV end-diastolic diameter (mm) | 48 | 45–50 | 48 | 45–51 | 0.573 |
| Interv. septum thickness (mm) | 11 | 9–12 | 11 | 10–13 | 0.583 |
| Ejection fraction (%) | 56 | 50–60 | 55 | 50–60 | 0.378 |
| NSAID (n = 39) | No NSAID (n = 75) | ||||
|---|---|---|---|---|---|
| Treatment for myocarditis/myopericarditis | % | n | % | n | p-value |
| NSAID | 100 | 39 | NA | NA | NA |
| Acetylsalicylic acid | 51.3 | 20 | NA | NA | NA |
| Ibuprofen | 46.2 | 18 | NA | NA | NA |
| Diclofenac | 2.6 | 1 | NA | NA | NA |
| Colchicine | 20.5 | 8 | 1.3 | 1 | 0.001 |
| Steroid | 0.0 | 0 | 2.7 | 2 | 0.546 |
| Beta blocker | 12.8 | 5 | 25.3 | 19 | 0.150 |
| ACEI/ARB | 10.3 | 4 | 16.0 | 12 | 0.572 |
| MCRA | 2.6 | 1 | 4.0 | 3 | 0.693 |
| mean | SD | mean | SD | p-value | |
| Duration of NSAID, weeks | 2.9 | 2.2 | NA | NA | NA |
| Dosage of acetylsalicylic acid per day, mg | 1260 | 395 | NA | NA | NA |
| Dosage of ibuprofen per day, mg | 1248 | 391 | NA | NA | NA |
| Dosage of diclofenac per day, mg | 100 | NA | NA | NA | NA |
| NSAID (n = 39) | No NSAID (n = 75) | ||||
|---|---|---|---|---|---|
| Primary and secondary study endpoints | % | n | % | n | p-value |
| 12-month mortality | 0.0 | 0 | 0.0 | 0 | NA |
| 24-month mortality | 5.1 | 2 | 0.0 | 0 | 0.115 |
| Arrhythmias, total | 12.8 | 5 | 12.0 | 9 | 0.899 |
| In-hospital complications | 12.8 | 5 | 8.0 | 6 | 0.507 |
| Admission to IMC/ICU | 53.8 | 21 | 46.7 | 35 | 0.555 |
| median | IQR | median | IQR | p-value | |
| EF at follow-up (%) | 55 | 54–60 | 55 | 50–56 | 0.228 |
| FC of EF (ratio) | 1.03 | 0.92–1.21 | 1.00 | 0.88–1.14 | 0.898 |
| Δ EF (%) | 1.25 | −4.13–8.75 | 0.00 | −7.00–7.75 | 0.831 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mirna, M.; Schmutzler, L.; Topf, A.; Boxhammer, E.; Sipos, B.; Hoppe, U.C.; Lichtenauer, M. Treatment with Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) Does Not Affect Outcome in Patients with Acute Myocarditis or Myopericarditis. J. Cardiovasc. Dev. Dis. 2022, 9, 32. https://doi.org/10.3390/jcdd9020032
Mirna M, Schmutzler L, Topf A, Boxhammer E, Sipos B, Hoppe UC, Lichtenauer M. Treatment with Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) Does Not Affect Outcome in Patients with Acute Myocarditis or Myopericarditis. Journal of Cardiovascular Development and Disease. 2022; 9(2):32. https://doi.org/10.3390/jcdd9020032
Chicago/Turabian StyleMirna, Moritz, Lukas Schmutzler, Albert Topf, Elke Boxhammer, Brigitte Sipos, Uta C. Hoppe, and Michael Lichtenauer. 2022. "Treatment with Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) Does Not Affect Outcome in Patients with Acute Myocarditis or Myopericarditis" Journal of Cardiovascular Development and Disease 9, no. 2: 32. https://doi.org/10.3390/jcdd9020032
APA StyleMirna, M., Schmutzler, L., Topf, A., Boxhammer, E., Sipos, B., Hoppe, U. C., & Lichtenauer, M. (2022). Treatment with Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) Does Not Affect Outcome in Patients with Acute Myocarditis or Myopericarditis. Journal of Cardiovascular Development and Disease, 9(2), 32. https://doi.org/10.3390/jcdd9020032