
Spontaneous Coronary Artery Dissection Unveiled: Pathophysiology, Imaging, and Evolving Management Strategies

 ,
,
Abstract
1. Introduction
1.1. Definition
1.2. Epidemiology
1.3. Demographics
1.4. Risk Factors
2. Pathophysiology
2.1. Vascular Vulnerability
2.2. Hormonal and Mechanical Factors
2.3. Inflammatory and Other Factors
3. Clinical Presentation
4. Diagnosis of SCAD
4.1. The Role of Invasive Coronary Angiography in SCAD Diagnosis
- SCAD Type 1 (classic aspect)—double lumen and longitudinal filling defect, indicating the presence of a false lumen (wall contrast staining) and visible intimal flap. This aspect is pathognomonic for dissection and easily recognizable; however, it is present in fewer than a third of diagnosed SCAD cases. The presence of contrast inside the coronary wall (“dye hang-up” sign) suggests an already formed dissection, often with a late presentation and fewer chances of further progression [4,32] (Figure 1).
- SCAD Type 2—long, diffuse, usually tubular lesion, longer than 20–30 mm, without a visible intimal flap or double lumen. The Type 2 lesion does not ameliorate after intracoronary nitroglycerine administration (in contrast with coronary spasm). This type is the most common angiography pattern, being present in over half of SCAD cases (60–70%) [5,9,33] (Figure 2).
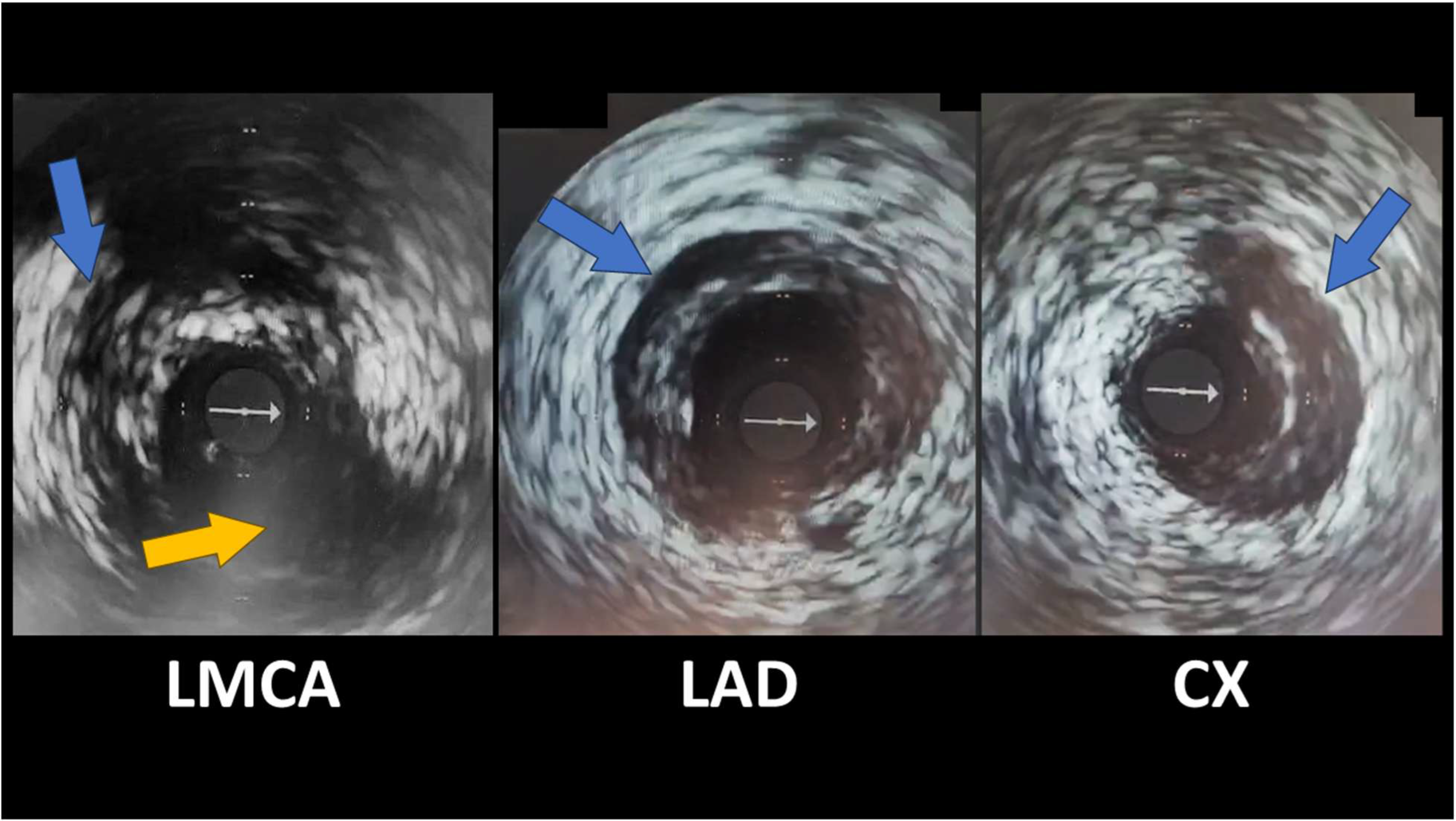
- SCAD Type 3—focal coronary stenosis, usually <20 mm, that mimics an obstructive atherosclerotic lesion on angiography. In reality, these lesions are also caused by an intramural hematoma (of shorter dimensions), but angiographically, they cannot be reliably differentiated from atherosclerotic plaque without additional imaging. Type 3 SCAD is identified in less than 5–10% of cases and usually requires confirmation by additional investigations—intravascular ultrasound (IVUS) or optical coherence tomography (OCT)—to identify wall dissection and exclude atheroma [5,6,33].
4.2. Non-Invasive Imaging Methods in SCAD
4.2.1. CT Coronary Angiography
4.2.2. Cardiac Magnetic Resonance
5. Treatment
5.1. Invasive Treatment
5.2. Pharmacotherapy
5.2.1. Antiplatelet Agents
5.2.2. Anticoagulants and Thrombolytics
5.2.3. Beta-Blockers
5.2.4. Statins
5.2.5. Angiotensin-Converting Enzyme Inhibitors (ACEIs) and Angiotensin II Receptor Blockers (ARBs)
5.2.6. Other Symptomatic Therapies
6. SCAD in Pregnancy and Postpartum
7. Recurrence and Long-Term Outcomes
8. Further Research
- Identification of Genetic Markers: Discovering genetic markers and connective tissue signatures can help better define at-risk populations, enabling preemptive counseling and screening.
- Longitudinal Studies on Hormonal Influences: Conducting long-term studies on hormonal influences, particularly in peripartum SCAD, will help clarify the roles of estrogen, progesterone, and relaxin in arterial wall fragility.
- Development of Standardized Imaging Protocols: Creating standardized imaging protocols can optimize early diagnosis in emergency settings while minimizing reliance on invasive techniques.
- Evaluation of Tailored Pharmacologic Regimens: Assessing customized medication regimens is crucial, particularly regarding the risks and benefits of antiplatelet drugs and statins in patients undergoing conservative management.
- Exploration of Quality-of-Life Outcomes: Investigating quality-of-life outcomes and the psychosocial burdens faced by SCAD survivors is crucial, with a focus on issues such as persistent angina, anxiety, and fears of recurrence.
- Clinical Trials for Novel Therapeutics: Initiating clinical trials for innovative therapeutic strategies, including vascular-stabilizing agents or hormone-modulating therapies, is vital, particularly for selected high-risk groups.
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACEI | Angiotensin-Converting Enzyme Inhibitor |
| ACS | Acute Coronary Syndrome |
| AHA | American Heart Association |
| ARB | Angiotensin II Receptor Blocker |
| CABG | Coronary Artery Bypass Grafting |
| CMR | Cardiac Magnetic Resonance |
| CT | Computer Tomography |
| DAPT | Dual Antiplatelet Therapy |
| ECS | European Society of Cardiology |
| FMD | Fibromuscular Dysplasia |
| IVUS | Intravascular Ultrasound |
| LAD | Left Anterior Descending (artery) |
| LGE | Late Gadolinium Enhancement |
| MACE | Major Adverse Cardiac Events |
| MI | Myocardial Infarction |
| MINOCA | Myocardial Infarction with Non-Obstructive Coronary Arteries |
| NOAC | Non-Vitamin K Antagonist Oral Anticoagulant |
| NSTEMI | Non-ST-Elevation Myocardial Infarction |
| OCT | Optical Coherence Tomography |
| PCI | Percutaneous Coronary Intervention |
| SCAD | Spontaneous Coronary Artery Dissection |
| STEMI | ST-Elevation Myocardial Infarction |
| TIMI | Thrombolysis In Myocardial Infarction (flow grade) |
References
- Abdelmaseih, R.; Hasan, M.; Patel, J.; Elhag, A.; Patel, J. Spontaneous Coronary Artery Dissection in a Healthy Male: A Case Report and Literature Review. Cureus 2020, 12, e7568. [Google Scholar] [CrossRef]
- Pender, P.; Zaheen, M.; Dang, Q.M.; Dang, V.; Xu, J.; Hollings, M.; Lo, S.; Negishi, K.; Zaman, S. Spontaneous Coronary Artery Dissection: A Narrative Review of Epidemiology and Public Health Implications. Medicina 2025, 61, 650. [Google Scholar] [CrossRef]
- Bergmark, B.A.; Mathenge, N.; Merlini, P.A.; Lawrence-Wright, M.B.; Giugliano, R.P. Acute coronary syndromes. Lancet 2022, 399, 1347–1358. [Google Scholar] [CrossRef]
- Dang, Q.; Burgess, S.; Psaltis, P.J.; Fairley, S.; Saw, J.; Zaman, S. Spontaneous coronary artery dissection: A clinically oriented narrative review. npj Cardiovasc. Health 2024, 1, 4. [Google Scholar] [CrossRef]
- Saw, J.; Starovoytov, A.; Aymong, E.; Inohara, T.; Alfadhel, M.; McAlister, C.; Samuel, R.; Grewal, T.; Parolis, J.A.; Sheth, T.; et al. Canadian Spontaneous Coronary Artery Dissection Cohort Study. J. Am. Coll. Cardiol. 2022, 80, 1585–1597. [Google Scholar] [CrossRef] [PubMed]
- Saw, J. Coronary angiogram classification of spontaneous coronary artery dissection. Catheter. Cardiovasc. Interv. 2013, 84, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Saw, J.; Mancini, G.J.; Humphries, K.; Fung, A.; Boone, R.; Starovoytov, A.; Aymong, E. Angiographic appearance of spontaneous coronary artery dissection with intramural hematoma proven on intracoronary imaging. Catheter. Cardiovasc. Interv. 2015, 87, E54–E61. [Google Scholar] [CrossRef]
- Mori, R.; Macaya, F.; Giacobbe, F.; Salinas, P.; Rolfo, C.; Porto, I.; Gonzalo, N.; Varbella, F.; Cerrato, E.; Escaned, J. Clinical and angiographic features of SCAD type 4. Int. J. Cardiol. 2023, 377, 22–25. [Google Scholar] [CrossRef]
- Mortensen, K.; Thuesen, L.; Kristensen, I.; Christiansen, E. Spontaneous coronary artery dissection: A Western Denmark Heart Registry Study. Catheter. Cardiovasc. Interv. 2009, 74, 710–717. [Google Scholar] [CrossRef]
- Daoulah, A.; Al-Faifi, S.M.; Alhamid, S.; Youssef, A.A.; Alshehri, M.; Al-Murayeh, M.; Farghali, T.; Maghrabi, M.; Balghith, M.; ElSayed, O.; et al. Spontaneous Coronary Artery Dissection in the Gulf: G-SCAD Registry. Angiology 2020, 72, 32–43. [Google Scholar] [CrossRef]
- Tokura, M.; Taguchi, I.; Kageyama, M.; Nasuno, T.; Nishiyama, Y.; Koshiji, N.; Koizumi, S.; Uehara, D.; Ogino, Y.; Toyoda, S.; et al. Clinical features of spontaneous coronary artery dissection. J. Cardiol. 2014, 63, 119–122. [Google Scholar] [CrossRef]
- Rigatelli, G.; Rigatelli, G.; Rossi, P.; Docali, G. Normal angiogram in acute coronary syndromes: The underestimated role of alternative substrates of myocardial ischemia. Int. J. Cardiovasc. Imaging 2004, 20, 471–475. [Google Scholar] [CrossRef]
- Stanojevic, D.; Apostolovic, S.; Kostic, T.; Mitov, V.; Kutlesic-Kurtovic, D.; Kovacevic, M.; Stanojevic, J.; Milutinovic, S.; Beleslin, B. A review of the risk and precipitating factors for spontaneous coronary artery dissection. Front. Cardiovasc. Med. 2023, 10, 1273301. [Google Scholar] [CrossRef] [PubMed]
- Saw, J.; Aymong, E.; Mancini, G.J.; Sedlak, T.; Starovoytov, A.; Ricci, D. Nonatherosclerotic Coronary Artery Disease in Young Women. Can. J. Cardiol. 2014, 30, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Nishiguchi, T.; Tanaka, A.; Ozaki, Y.; Taruya, A.; Fukuda, S.; Taguchi, H.; Iwaguro, T.; Ueno, S.; Okumoto, Y.; Akasaka, T. Prevalence of spontaneous coronary artery dissection in patients with acute coronary syndrome. Eur. Heart J. Acute Cardiovasc. Care 2013, 5, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, T.; Noguchi, T.; Haruta, S.; Yamamoto, Y.; Oshima, S.; Nakao, K.; Taniguchi, Y.; Yamaguchi, J.; Tsuchihashi, K.; Seki, A.; et al. Prognostic impact of spontaneous coronary artery dissection in young female patients with acute myocardial infarction: A report from the Angina Pectoris–Myocardial Infarction Multicenter Investigators in Japan. Int. J. Cardiol. 2016, 207, 341–348. [Google Scholar] [CrossRef]
- Djokovic, A.; Krljanac, G.; Matic, P.; Zivic, R.; Djulejic, V.; Haljilji, M.M.; Popovic, D.; Filipovic, B.; Apostolovic, S. Pathophysiology of spontaneous coronary artery dissection: Hematoma, not thrombus. Front. Cardiovasc. Med. 2023, 10, 1260478. [Google Scholar] [CrossRef]
- Apostolović, S.; Ignjatović, A.; Stanojević, D.; Radojković, D.D.; Nikolić, M.; Milošević, J.; Filipović, T.; Kostić, K.; Miljković, I.; Djoković, A.; et al. Spontaneous coronary artery dissection in women in the generative period: Clinical characteristics, treatment, and outcome—A systematic review and meta-analysis. Front. Cardiovasc. Med. 2024, 11, 1277604. [Google Scholar] [CrossRef]
- Saw, J.; Ricci, D.; Starovoytov, A.; Fox, R.; Buller, C.E. Spontaneous Coronary Artery Dissection. JACC: Cardiovasc. Interv. 2013, 6, 44–52. [Google Scholar] [CrossRef]
- Tweet, M.S.; Hayes, S.N.; Pitta, S.R.; Simari, R.D.; Lerman, A.; Lennon, R.J.; Gersh, B.J.; Khambatta, S.; Best, P.J.; Rihal, C.S.; et al. Clinical Features, Management, and Prognosis of Spontaneous Coronary Artery Dissection. Circulation 2012, 126, 579–588. [Google Scholar] [CrossRef]
- Saw, J.; Mancini, G.J.; Humphries, K.H. Contemporary Review on Spontaneous Coronary Artery Dissection. J. Am. Coll. Cardiol. 2016, 68, 297–312. [Google Scholar] [CrossRef]
- Yang, C.; Offen, S.; Saw, J. What Is New in Spontaneous Coronary Artery Dissection? CJC Open 2023, 6, 417–424. [Google Scholar] [CrossRef]
- Lobo, A.S.; Cantu, S.M.; Sharkey, S.W.; Grey, E.Z.; Storey, K.; Witt, D.; Benson, G.; Garberich, R.F.; Kubota, Y.; Merz, C.N.B.; et al. Revascularization in Patients with Spontaneous Coronary Artery Dissection and ST-Segment Elevation Myocardial Infarction. J. Am. Coll. Cardiol. 2019, 74, 1290–1300. [Google Scholar] [CrossRef]
- García-Guimarães, M.; Sanz-Ruiz, R.; Sabaté, M.; Velázquez-Martín, M.; Veiga, G.; Ojeda, S.; Avanzas, P.; Cortés, C.; Trillo-Nouche, R.; Pérez-Guerrero, A.; et al. Spontaneous coronary artery dissection and ST-segment elevation myocardial infarction: Does clinical presentation matter? Int. J. Cardiol. 2022, 373, 1–6. [Google Scholar] [CrossRef]
- Elkaryoni, A.; Klappa, A.; Doukas, D.; Luke, D.; John, A.; Allen, S.; Bakir, M.; Leya, F.; Lewis, B.; Darki, A.; et al. Outcomes of ST-Elevation Myocardial Infarction due to spontaneous coronary artery dissection: A nationwide cohort sample. Eur. Hear. J. 2021, 42. [Google Scholar] [CrossRef]
- Motreff, P.; Malcles, G.; Combaret, N.; Barber-Chamoux, N.; Bouajila, S.; Pereira, B.; Amonchot, A.; Citron, B.; Lusson, J.-R.; Eschalier, R.; et al. How and when to suspect spontaneous coronary artery dissection: Novel insights from a single-centre series on prevalence and angiographic appearance. EuroIntervention 2017, 12, e2236–e2243. [Google Scholar] [CrossRef] [PubMed]
- da Silva, P.A.; Bucciarelli-Ducci, C.; Sousa, A. Myocardial infarction with non-obstructive coronary arteries: Etiology, diagnosis, treatment and prognosis. Rev. Port. Cardiol. 2023, 42, 655–666. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, A.N.; Taduru, S.S.; Mentias, A.; Mahtta, D.; Barakat, A.F.; Saad, M.; Elgendy, A.Y.; Mojadidi, M.K.; Omer, M.; Abuzaid, A.; et al. Trends of Incidence, Clinical Presentation, and In-Hospital Mortality Among Women with Acute Myocardial Infarction with or without Spontaneous Coronary Artery Dissection. JACC Cardiovasc. Interv. 2018, 11, 80–90. [Google Scholar] [CrossRef]
- Agewall, S.; Beltrame, J.F.; Reynolds, H.R.; Niessner, A.; Rosano, G.; Caforio, A.L.P.; De Caterina, R.; Zimarino, M.; Roffi, M.; Kjeldsen, K.; et al. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur. Heart J. 2016, 38, ehw149–ehw153. [Google Scholar] [CrossRef]
- D’amato, A.; Mariani, M.V.; Prosperi, S.; Colombo, L.; De Prisco, A.; Lavalle, C.; Mancone, M.; Vizza, C.D.; Severino, P. Spontaneous Coronary Artery Dissection in Clinical Practice: Pathophysiology and Therapeutic Approaches. Medicina 2024, 60, 217. [Google Scholar] [CrossRef]
- Severino, P.; D’amato, A.; Prosperi, S.; Myftari, V.; Colombo, L.; Tomarelli, E.; Piccialuti, A.; Di Pietro, G.; Birtolo, L.I.; Maestrini, V.; et al. Myocardial Infarction with Non-Obstructive Coronary Arteries (MINOCA): Focus on Coronary Microvascular Dysfunction and Genetic Susceptibility. J. Clin. Med. 2023, 12, 3586. [Google Scholar] [CrossRef] [PubMed]
- Adlam, D.; Tweet, M.S.; Gulati, R.; Kotecha, D.; Rao, P.; Moss, A.J.; Hayes, S.N. Spontaneous Coronary Artery Dissection. JACC Cardiovasc. Interv. 2021, 14, 1743–1756. [Google Scholar] [CrossRef] [PubMed]
- Tweet, M.S.; Eleid, M.F.; Best, P.J.; Lennon, R.J.; Lerman, A.; Rihal, C.S.; Holmes, D.R.; Hayes, S.N.; Gulati, R. Spontaneous Coronary Artery Dissection. Circ. Cardiovasc. Interv. 2014, 7, 777–786. [Google Scholar] [CrossRef] [PubMed]
- Eleid, M.F.; Guddeti, R.R.; Tweet, M.S.; Lerman, A.; Singh, M.; Best, P.J.; Vrtiska, T.J.; Prasad, M.; Rihal, C.S.; Hayes, S.N.; et al. Coronary Artery Tortuosity in Spontaneous Coronary Artery Dissection. Circ. Cardiovasc. Interv. 2014, 7, 656–662. [Google Scholar] [CrossRef]
- Margaritis, M.; Saini, F.; Baranowska-Clarke, A.A.; Parsons, S.; Vink, A.; Budgeon, C.; Allcock, N.; Wagner, B.E.; Samani, N.J.; von der Thüsen, J.; et al. Vascular histopathology and connective tissue ultrastructure in spontaneous coronary artery dissection: Pathophysiological and clinical implications. Cardiovasc. Res. 2021, 118, 1835–1848. [Google Scholar] [CrossRef]
- Adlam, D.; Alfonso, F.; Maas, A.; Vrints, C. European Society of Cardiology, acute cardiovascular care association, SCAD study group: A position paper on spontaneous coronary artery dissection. Eur. Heart J. 2018, 39, 3353–3368. [Google Scholar] [CrossRef]
- Hayes, S.N.; Tweet, M.S.; Adlam, D.; Kim, E.S.; Gulati, R.; Price, J.E.; Rose, C.H. Spontaneous Coronary Artery Dissection: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 76, 961–984. [Google Scholar] [CrossRef]
- Combaret, N.; Motreff, P. Registre national des dissections coronaires spontanées: Le registre DISCO. Ann. Cardiol. Angéiol. 2023, 72, 101684. [Google Scholar] [CrossRef]
- Barbieri, L.; D’eRrico, A.; Avallone, C.; Gentile, D.; Provenzale, G.; Guagliumi, G.; Tumminello, G.; Carugo, S. Optical Coherence Tomography and Coronary Dissection: Precious Tool or Useless Surplus? Front. Cardiovasc. Med. 2022, 9, 822998. [Google Scholar] [CrossRef]
- Tweet, M.S.; Gulati, R.; Hayes, S.N. Spontaneous Coronary Artery Dissection. Curr. Cardiol. Rep. 2016, 18, 1–6. [Google Scholar] [CrossRef]
- Prakash, R.; Starovoytov, A.; Heydari, M.; Mancini, G.J.; Saw, J. Catheter-Induced Iatrogenic Coronary Artery Dissection in Patients with Spontaneous Coronary Artery Dissection. JACC Cardiovasc. Interv. 2016, 9, 1851–1853. [Google Scholar] [CrossRef]
- Pristera, N.; Chaudhury, P.; Van Iterson, E.H.; Cho, L.S. Spontaneous coronary artery dissection: Principles of management. Clevel. Clin. J. Med. 2021, 88, 623–630. [Google Scholar] [CrossRef]
- Eleid, M.F.; Tweet, M.S.; Young, P.M.; Williamson, E.; Hayes, S.N.; Gulati, R. Spontaneous coronary artery dissection: Challenges of coronary computed tomography angiography. Eur. Heart J. Acute Cardiovasc. Care 2017, 7, 609–613. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Meyersohn, N.M.; Wood, M.J.; Steigner, M.L.; Blankstein, R.; Ghoshhajra, B.B.; Hedgire, S.S. Role of Coronary CT Angiography in Spontaneous Coronary Artery Dissection. Radiol. Cardiothorac. Imaging 2020, 2, e200364. [Google Scholar] [CrossRef] [PubMed]
- Petropoulos, T.; Shah, A.; Dueck, A.; Hawkes, C.; Tobe, S.W.; Kingston, W.; Madan, M. Fibromuscular Dysplasia: A Focused Review for the Cardiologist. CJC Open 2024, 6, 1274–1288. [Google Scholar] [CrossRef] [PubMed]
- Offen, S.; Kang, M.; Grewal, T.; Fung, A.; Aymong, E.; Sheth, T.; Saw, J. Safety of Intracoronary Imaging in Patients with Spontaneous Coronary Artery Dissection. Can. J. Cardiol. 2024, 40, 2089–2091. [Google Scholar] [CrossRef]
- Mehmedbegović, Z.; Ivanov, I.; Čanković, M.; Perišić, Z.; Kostić, T.; Maričić, B.; Krljanac, G.; Beleslin, B.; Apostolović, S. Invasive imaging modalities in a spontaneous coronary artery dissection: When “believing is seeing”. Front. Cardiovasc. Med. 2023, 10, 1270259. [Google Scholar] [CrossRef]
- Gudenkauf, B.; Hays, A.G.; Tamis-Holland, J.; Trost, J.; Ambinder, D.I.; Wu, K.C.; Arbab-Zadeh, A.; Blumenthal, R.S.; Sharma, G. Role of Multimodality Imaging in the Assessment of Myocardial Infarction with Nonobstructive Coronary Arteries: Beyond Conventional Coronary Angiography. J. Am. Heart Assoc. 2022, 11, e022787. [Google Scholar] [CrossRef]
- Spînu, M.; Onea, L.H.; Homorodean, C.; Olinic, M.; Ober, M.C.; Olinic, D.M. Optical Coherence Tomography—OCT for Characterization of Non-Atherosclerotic Coronary Lesions in Acute Coronary Syndromes. J. Clin. Med. 2022, 11, 265. [Google Scholar] [CrossRef]
- Offen, S.; Saw, J.; Kang, M.; Grewal, T.; Fung, A.; Aymong, E. Intracoronary Imaging in Spontaneous Coronary Artery Dissection (SCAD). Can. J. Cardiol. 2023, 39, S211. [Google Scholar] [CrossRef]
- Marrazzo, G.; Palermi, S.; Pastore, F.; Ragni, M.; De Luca, M.; Gambardella, M.; Quaranta, G.; Messalli, G.; Riegler, L.; Pergola, V.; et al. Multimodality Imaging Approach to Spontaneous Coronary Artery Dissection. J. Clin. Med. 2022, 12, 154. [Google Scholar] [CrossRef]
- Bezerra, H.G.; Costa, M.A.; Guagliumi, G.; Rollins, A.M.; Simon, D.I. Intracoronary Optical Coherence Tomography: A Comprehensive Review. JACC Cardiovasc. Interv. 2009, 2, 1035–1046. [Google Scholar] [CrossRef] [PubMed]
- Saia, F.; Komukai, K.; Capodanno, D.; Sirbu, V.; Musumeci, G.; Boccuzzi, G.; Tarantini, G.; Fineschi, M.; Tumminello, G.; Bernelli, C.; et al. Eroded Versus Ruptured Plaques at the Culprit Site of STEMI. JACC Cardiovasc. Imaging 2015, 8, 566–575. [Google Scholar] [CrossRef] [PubMed]
- Räber, L.; Mintz, G.S.; Koskinas, K.C.; Johnson, T.W.; Holm, N.R.; Onuma, Y.; Radu, M.D.; Joner, M.; Yu, B.; Jia, H.; et al. Clinical use of intracoronary imaging. Part 1: Guidance and optimization of coronary interventions. An expert consensus document of the European Association of Percutaneous Cardiovascular Interventions. Eur. Heart J. 2018, 39, 3281–3300. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.N.; Kim, E.S.; Saw, J.; Adlam, D.; Arslanian-Engoren, C.; Economy, K.E.; Ganesh, S.K.; Gulati, R.; Lindsay, M.E.; Mieres, J.H.; et al. Spontaneous Coronary Artery Dissection: Current State of the Science: A Scientific Statement from the American Heart Association. Circulation 2018, 137, E523–E557. [Google Scholar] [CrossRef]
- Hebsgaard, L.; Nielsen, T.M.; Tu, S.; Krusell, L.R.; Maeng, M.; Veien, K.T.; Raungaard, B.; Terkelsen, C.J.; Kaltoft, A.; Reiber, J.H.; et al. Co-registration of optical coherence tomography and X-ray angiography in percutaneous coronary intervention. The Does Optical Coherence Tomography Optimize Revascularization (DOCTOR) fusion study. Int. J. Cardiol. 2015, 182, 272–278. [Google Scholar] [CrossRef]
- Paulo, M.; Sandoval, J.; Lennie, V.; Dutary, J.; Medina, M.; Gonzalo, N.; Jimenez-Quevedo, P.; Escaned, J.; Bañuelos, C.; Hernandez, R.; et al. Combined Use of OCT and IVUS in Spontaneous Coronary Artery Dissection. JACC Cardiovasc. Imaging 2013, 6, 830–832. [Google Scholar] [CrossRef]
- Nissen, S.E.; Gurley, J.C.; Grines, C.L.; Booth, D.C.; McClure, R.; Berk, M.; Fischer, C.; DeMaria, A.N. Intravascular ultrasound assessment of lumen size and wall morphology in normal subjects and patients with coronary artery disease. Circulation 1991, 84, 1087–1099. [Google Scholar] [CrossRef]
- Morena, A.; Giacobbe, F.; De Filippo, O.; Angelini, F.; Bruno, F.; Siliano, S.; Giannino, G.; Dusi, V.; Bianco, M.; Biolé, C.; et al. Advances in the Management of Spontaneous Coronary Artery Dissection (SCAD): A Comprehensive Review. Rev. Cardiovasc. Med. 2024, 25, 345. [Google Scholar] [CrossRef]
- Nasr, M.S.; Haber, M.; Nasr, S.R. A Noninvasive Diagnostic Approach for Identifying Spontaneous Coronary Artery Dissection (SCAD) in Young Women: A Case Report and Review of the Literature. Cureus 2025, 17, e79167. [Google Scholar] [CrossRef]
- Tweet, M.S.; Akhtar, N.J.; Hayes, S.N.; Best, P.J.; Gulati, R.; Araoz, P.A. Spontaneous coronary artery dissection: Acute findings on coronary computed tomography angiography. Eur. Heart J. Acute Cardiovasc. Care 2018, 8, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Pozo-Osinalde, E.; García-Guimaraes, M.; Bastante, T.; Aguilera, M.C.; Rodríguez-Alcudia, D.; Rivero, F.; Hernández, S.; Jiménez-Borreguero, L.J.; Alfonso, F. Characteristic findings of acute spontaneous coronary artery dissection by cardiac computed tomography. Coron. Artery Dis. 2020, 31, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Kaadan, M.I.; Duran, J.M.; Ponzini, F.; Mishra, S.; Tsiaras, S.V.; Scott, N.S.; Weinberg, I.; Ghoshhajra, B.; Lindsay, M.; et al. Risk Factors, Imaging Findings, and Sex Differences in Spontaneous Coronary Artery Dissection. Am. J. Cardiol. 2019, 123, 1783–1787. [Google Scholar] [CrossRef] [PubMed]
- Brízido, C.; Madeira, S.; Silva, C.; Strong, C.; Tralhão, A.; Almeida, M. Spontaneous coronary artery dissection: A review for clinical and interventional cardiologists. Rev. Port. Cardiol. 2023, 42, 269–276. [Google Scholar] [CrossRef]
- Pergola, V.; Continisio, S.; Mantovani, F.; Motta, R.; Mattesi, G.; Marrazzo, G.; Dellino, C.M.; Montonati, C.; De Conti, G.; Galzerano, D.; et al. Spontaneous coronary artery dissection: The emerging role of coronary computed tomography. Eur. Heart J. Cardiovasc. Imaging 2023, 24, 839–850. [Google Scholar] [CrossRef]
- Lionakis, N.; Briasoulis, A.; Zouganeli, V.; Dimopoulos, S.; Kalpakos, D.; Kourek, C. Spontaneous coronary artery dissection: A review of diagnostic methods and management strategies. World J. Cardiol. 2022, 14, 522–536. [Google Scholar] [CrossRef]
- Chandrasekhar, J.; Thakkar, J.; Starovoytov, A.; Mayo, J.; Saw, J. Characteristics of spontaneous coronary artery dissection on cardiac magnetic resonance imaging. Cardiovasc. Diagn. Ther. 2020, 10, 636–638. [Google Scholar] [CrossRef]
- Feldbaum, E.; Thompson, E.W.; Cook, T.S.; Sanghavi, M.; Wilensky, R.L.; Fiorilli, P.N.; Lewey, J. Management of spontaneous coronary artery dissection: Trends over time. Vasc. Med. 2023, 28, 131–138. [Google Scholar] [CrossRef]
- Hassan, S.; Prakash, R.; Starovoytov, A.; Saw, J. Natural History of Spontaneous Coronary Artery Dissection with Spontaneous Angiographic Healing. JACC Cardiovasc. Interv. 2019, 12, 518–527. [Google Scholar] [CrossRef]
- Saw, J.; Humphries, K.; Aymong, E.; Sedlak, T.; Prakash, R.; Starovoytov, A.; Mancini, G.J. Spontaneous Coronary Artery Dissection. J. Am. Coll. Cardiol. 2017, 70, 1148–1158. [Google Scholar] [CrossRef]
- Pepe, M.; Cecere, A.; Napodano, M.; Ciccone, M.M.; Bartolomucci, F.; Navarese, E.P.; Iacovelli, F.; Zanna, D.; Mele, M. How to Approach a Spontaneous Coronary Artery Dissection: An Up-To-Date. Interv. Cardiol. J. 2017, 3, 1–9. [Google Scholar] [CrossRef]
- Maričić, B.; Perišić, Z.; Kostić, T.; Božinović, N.; Petrović, M.; Čanković, M.; Mehmedbegović, Z.; Juričić, S.; Vasilev, V.; Dakić, S.; et al. An analysis of published cases of cutting balloon use in spontaneous coronary artery dissection. Front. Cardiovasc. Med. 2023, 10, 1270530. [Google Scholar] [CrossRef] [PubMed]
- Alfonso, F.; Fernández-Pérez, C.; del Prado, N.; García-Guimaraes, M.; Bernal, J.L.; Bastante, T.; del Val, D.; Rosillo, N.; Elola, J. Primary Percutaneous Coronary Intervention in Patients with Spontaneous Coronary Artery Dissection vs Coronary Artery Disease. JACC Cardiovasc. Interv. 2023, 16, 1860–1869. [Google Scholar] [CrossRef] [PubMed]
- Macaya, F.; Salinas, P.; Gonzalo, N.; Fernández-Ortiz, A.; Macaya, C.; Escaned, J. Spontaneous coronary artery dissection: Contemporary aspects of diagnosis and patient management. Open Hear. 2018, 5, e000884. [Google Scholar] [CrossRef] [PubMed]
- Macaya, F.; Peral, V.; Alameda, M.; Pascual, M.; Gomez-Jaume, A.; Asmarats, L.; Maristany, J.; Ojeda, M.; Bethencourt, A. Bioresorbable Scaffolds to Treat Spontaneous Coronary Artery Dissection. Circ. Cardiovasc. Interv. 2016, 9, e003133. [Google Scholar] [CrossRef]
- Thistlethwaite, P.A.; Tarazi, R.Y.; Giordano, F.J.; Jamieson, S.W. Surgical management of spontaneous left main coronary artery dissection. Ann. Thorac. Surg. 1998, 66, 258–260. [Google Scholar] [CrossRef]
- Cerrato, E.; Giacobbe, F.; Quadri, G.; Macaya, F.; Bianco, M.; Mori, R.; Biolè, C.A.; Boi, A.; Bettari, L.; Rolfo, C.; et al. Antiplatelet therapy in patients with conservatively managed spontaneous coronary artery dissection from the multicentre DISCO registry. Eur. Heart J. 2021, 42, 3161–3171. [Google Scholar] [CrossRef]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.-A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes: Developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC). Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef]
- Chi, G.; Najafi, H.; Montazerin, S.M.; Lee, J.J. Factors associated with recurrent spontaneous coronary artery dissection: A systematic review and meta-analysis. Coron. Artery Dis. 2022, 33, 566–573. [Google Scholar] [CrossRef]
- Sedlak, T.; Starovoytov, A.; Humphries, K.; Saw, J. Coronary Flow Reserve in Patients with Prior Spontaneous Coronary Artery Dissection and Recurrent Angina. J. Am. Heart Assoc. 2020, 9, e015834. [Google Scholar] [CrossRef]
- Tweet, M.S.; Hayes, S.N.; Codsi, E.; Gulati, R.; Rose, C.H.; Best, P.J. Spontaneous Coronary Artery Dissection Associated with Pregnancy. J. Am. Coll. Cardiol. 2017, 70, 426–435. [Google Scholar] [CrossRef]
- Ito, H.; Taylor, L.; Bowman, M.; Fry, E.T.; Hermiller, J.B.; Van Tassel, J.W. Presentation and Therapy of Spontaneous Coronary Artery Dissection and Comparisons of Postpartum Versus Nonpostpartum Cases. Am. J. Cardiol. 2011, 107, 1590–1596. [Google Scholar] [CrossRef]
- Cade, J.R.; Szarf, G.; de Siqueira, M.E.M.; Chaves, Á.; Andréa, J.C.M.; Figueira, H.R.; Gomes, M.M.; Freitas, B.P.; Medeiros, J.F.; dos Santos, M.R.; et al. Pregnancy-associated spontaneous coronary artery dissection: Insights from a case series of 13 patients. Eur. Heart J. Cardiovasc. Imaging 2016, 18, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Havakuk, O.; Goland, S.; Mehra, A.; Elkayam, U. Pregnancy and the Risk of Spontaneous Coronary Artery Dissection. Circ. Cardiovasc. Interv. 2017, 10, e004941. [Google Scholar] [CrossRef] [PubMed]
- Regitz-Zagrosek, V.; Roos-Hesselink, J.W.; Bauersachs, J.; Blomström-Lundqvist, C.; Cífková, R.; De Bonis, M.; Iung, B.; Johnson, M.R.; Kintscher, U.; Kranke, P.; et al. 2018 ESC Guidelines for the Management of Cardiovascular Diseases during Pregnancy: The Task Force for the Management of Cardiovascular Diseases during Pregnancy of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 3165–3241. [Google Scholar] [CrossRef] [PubMed]
- Vrints, C.J.M. Spontaneous coronary artery dissection. Heart 2010, 96, 801–808. [Google Scholar] [CrossRef]
- Adlam, D.; García-Guimaraes, M.; Maas, A.H.E.M. Spontaneous coronary artery dissection: No longer a rare disease. Eur. Hear. J. 2019, 40, 1198–1201. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SCAD Type (Angiographic) | Features | Comments |
|---|---|---|
| Type 1 (Classic) | Multiple lumens or contrast staining (visible flap) through vessel wall [7]. | Pathognomonic (“flap”). <30% of SCAD; suggests an intimal tear. Often managed conservatively. |
| Type 2 (Diffuse) | Long, smooth narrowing (>20 mm) of the mid-to-distal artery; lumen caliber tapers over the segment [7]. | The most common type. Variant 2A: normal distal segment; 2B: extends to vessel tip. Typically heals with conservative treatment. |
| Type 3 (Focal) | Short (<20 mm) tubular stenosis mimicking an atherosclerotic plaque [7]. | Rarest. Requires OCT 1/IVUS 2 for confirmation of intramural hematoma. |
| Type 4 (Occlusion) | Total occlusion of the vessel, with abrupt cutoff on angiography [8]. | Less common. Often presents as STEMI 3; may require PCI 4. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rusali, C.A.; Lupu, I.C.; Rusali, L.M.; Cojocaru, L. Spontaneous Coronary Artery Dissection Unveiled: Pathophysiology, Imaging, and Evolving Management Strategies. J. Cardiovasc. Dev. Dis. 2025, 12, 286. https://doi.org/10.3390/jcdd12080286
Rusali CA, Lupu IC, Rusali LM, Cojocaru L. Spontaneous Coronary Artery Dissection Unveiled: Pathophysiology, Imaging, and Evolving Management Strategies. Journal of Cardiovascular Development and Disease. 2025; 12(8):286. https://doi.org/10.3390/jcdd12080286
Chicago/Turabian StyleRusali, Constantin Andrei, Ioana Caterina Lupu, Lavinia Maria Rusali, and Lucia Cojocaru. 2025. "Spontaneous Coronary Artery Dissection Unveiled: Pathophysiology, Imaging, and Evolving Management Strategies" Journal of Cardiovascular Development and Disease 12, no. 8: 286. https://doi.org/10.3390/jcdd12080286
APA StyleRusali, C. A., Lupu, I. C., Rusali, L. M., & Cojocaru, L. (2025). Spontaneous Coronary Artery Dissection Unveiled: Pathophysiology, Imaging, and Evolving Management Strategies. Journal of Cardiovascular Development and Disease, 12(8), 286. https://doi.org/10.3390/jcdd12080286