

Gratitude Predicts Meaning in Life in Family Caregivers of Persons with Alzheimer’s Disease

 , , , ,
, , , ,
Abstract
1. Introduction
1.1. Caregiver Burden
1.2. Conceptualizations of Gratitude and Research on Gratitude in Dementia Family Caregivers
1.3. Conceptualizations of Meaning in Life and Research on Meaning in Life in Dementia Family Caregivers
1.4. Theoretical Framework and Current Study Aims
2. Materials and Methods
2.1. Study Design and Participants
2.2. Variables and Measures
2.2.1. Outcome Variables
2.2.2. Predictor Variables
2.3. Data Analysis
3. Results
3.1. Participant Demographics
3.2. Descriptive and Correlational Data
3.3. Independent Effects of Gratitude on Meaning in Life Presence and Search
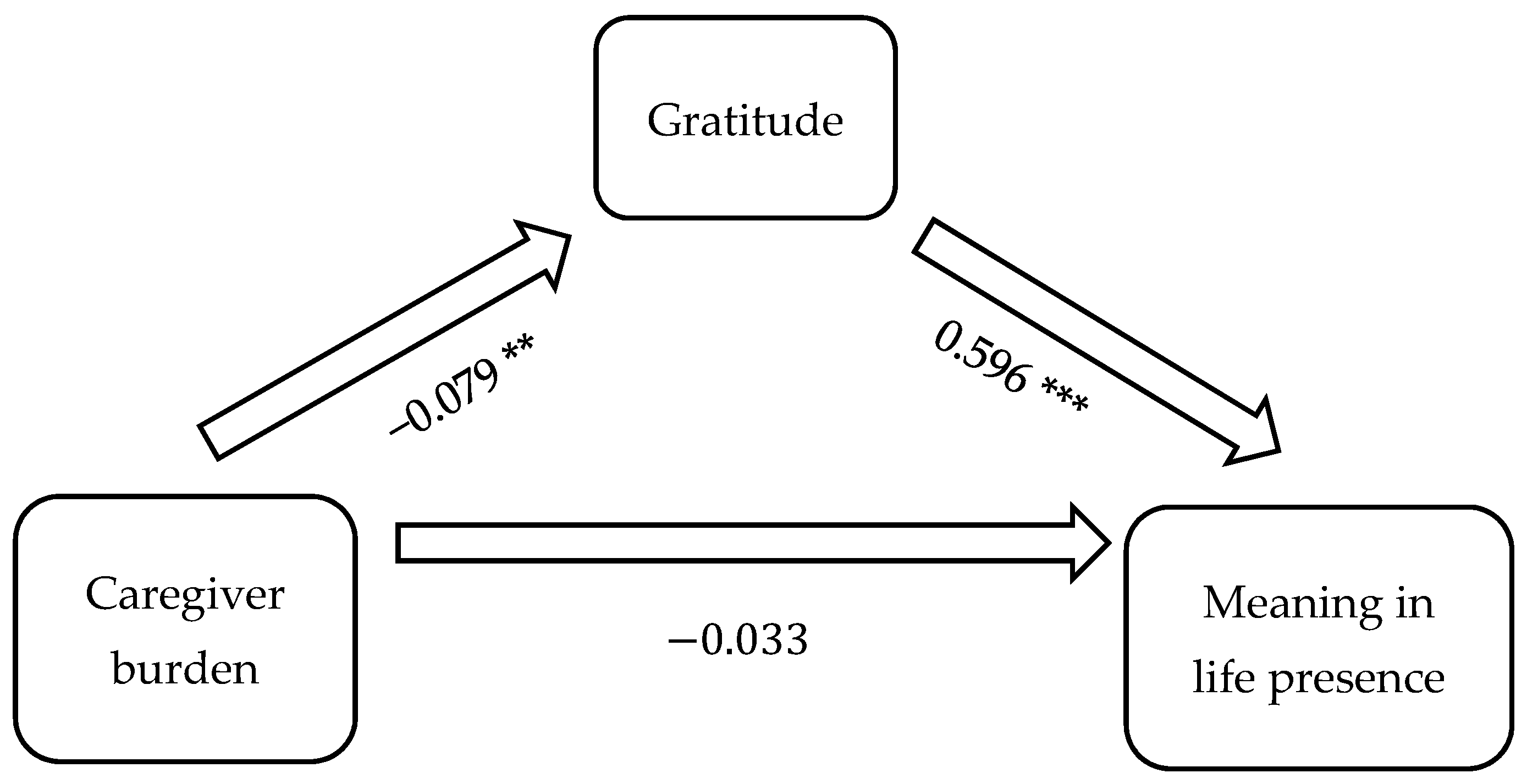
3.4. Gratitude Mediation Effects on Caregiver Burden and Meaning in Life Relationship
4. Discussion
5. Study Limitations
6. Recommendations
6.1. Develop and Test Evidence-Informed Caregiver Gratitude Assessment and Intervention Protocols
6.2. Deepen Understanding of the Caregiver Gratitude and Meaning Relationship
6.3. Focus on Cultural, Ethnic, Gender, and Spiritual Diversity
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schulz, R.; Beach, S.R.; Czaja, S.J.; Martire, L.M.; Monin, J.K. Family caregiving for older adults. Annu. Rev. Psychol. 2020, 71, 635–659. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Badana, A.N.S.; Burgdorf, J.; Fabius, C.D.; Roth, D.L.; Haley, W.E. Systematic review and meta-analysis of racial and ethnic differences in dementia caregivers’ well-being. Gerontologist 2021, 61, e228–e243. [Google Scholar] [CrossRef] [PubMed]
- Beach, S.R.; Schulz, R. Family caregiver factors associated with unmet needs for care of older adults. J. Am. Geriatr. Soc. 2017, 65, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Iecovich, E. Do caregiving burden and satisfaction predict loneliness in older care recipients? Aging Ment. Health 2016, 20, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Pristavec, T.; Luth, E. The effect of caregiving experience on care recipient older adults’ mortality: A survival analysis. Innov. Aging 2019, 3 (Suppl. S1), S217. [Google Scholar] [CrossRef]
- Kim, H.; Chang, M.; Rose, K.; Kim, S. Predictors of caregiver burden in caregivers of individuals with dementia. J. Adv. Nurs. 2012, 68, 846–855. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.-F.; Hwang, W.-S.; Lee, J.-J.; Wang, W.-F.; Huang, L.-C.; Huang, L.-K.; Lee, W.-J.; Sung, P.-S.; Liu, Y.-C.; Hsu, C.-C.; et al. Predictors of caregiver burden in aged caregivers of demented older patients. BMC Geriatr. 2021, 21, 59. [Google Scholar] [CrossRef] [PubMed]
- Kokorelias, K.M.; Naglie, G.; Gignac, M.A.; Rittenberg, N.; Cameron, J.I. A qualitative exploration of how gender and relationship shape family caregivers’ experiences across the Alzheimer’s disease trajectory. Dementia 2021, 20, 2851–2866. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.G.; Flatt, J.D.; Jabson Tree, J.M.; Gross, A.L.; Rose, K.M. Characteristics of sexual and gender minority caregivers of people with dementia. J. Aging Health 2021, 33, 838–851. [Google Scholar] [CrossRef]
- Chappell, N.L.; Dujela, C.; Smith, A. Caregiver well-being: Intersections of relationship and gender. Res. Aging 2015, 37, 623–645. [Google Scholar] [CrossRef]
- Conde-Sala, J.L.; Garre-Olmo, J.; Turró-Garriga, O.; Vilalta-Franch, J.; López-Pousa, S. Differential features of burden between spouse and adult-child caregivers of patients with Alzheimer’s disease: An exploratory comparative design. Int. J. Nurs. Stud. 2010, 47, 1262–1273. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Heffernan, C.; Tan, J. Caregiver burden: A concept analysis. Int. J. Nurs. Sci. 2020, 7, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Shibah, K.; Kondo, N.; Kondo, K. Informal and formal social support and care receiver burden: The AGES Caregiver Survey. J. Epidemiol. 2016, 26, 622–628. [Google Scholar] [CrossRef] [PubMed]
- McGee, J.S.; Davie, M.; Meraz, R.; Myers, D.; Boddie, S.C. Does the tough stuff make us stronger? Spiritual coping in family caregivers of persons with early-stage dementia. Religions 2022, 13, 756. [Google Scholar] [CrossRef]
- McGee, J.S.; Davie, M.; Meraz, R.; Myers, D.; McElroy, M. Does God work in all things for the good of those who love Him? Family caregivers of persons with early-stage dementia share their spiritual struggles. Religions 2022, 13, 645. [Google Scholar] [CrossRef]
- McGee, J.S.; Myers, D.R.; Meraz, R.; Davie, M. Caring for a family member with early-stage Alzheimer’s disease: Caregiver perceptions, connections, and relational dynamics with the sacred. J. Relig. Spiritual. Aging 2021, 34, 196–207. [Google Scholar] [CrossRef]
- Polson, C.P.; Myers, D.R.; McClellan, A.M.; Zhao, H.C.; Meraz, R.; McGee, J.S. Perceived benefit or burden? How positive and negative spiritual/religious coping impacts family caregivers of people with dementia. J. Relig. Spiritual. Aging 2024, 36, 235–257. [Google Scholar] [CrossRef]
- McGee, J.S.; Myers, D.R.; Polson, E.C.; McClellan, A.; Meraz, R.L.; Ke, W. Hope mediates stress to reduce burden in family caregivers of persons with Alzheimer’s. Geriatrics 2024, 9, 38. [Google Scholar] [CrossRef] [PubMed]
- Emmons, R.A. Gratitude as a psychotherapeutic intervention. J. Clin. Psychol. 2013, 69, 846–855. [Google Scholar] [CrossRef]
- Wood, A.M.; Froh, J.J.; Geraghty, A.W.A. Gratitude and well-being: A review and theoretical integration. Clin. Psychol. Rev. 2010, 30, 890–905. [Google Scholar] [CrossRef]
- Xiang, Y.; Yuan, R. Why do people with high dispositional gratitude tend to experience high life satisfaction? A broaden-and-build theory perspective. J. Happiness Stud. 2020, 22, 2485–2498. [Google Scholar] [CrossRef]
- McCullough, M.E.; Emmons, R.A.; Tsang, J.A. The grateful disposition: A conceptual and empirical topography. J. Personal. Soc. Psychol. 2002, 82, 112–127. [Google Scholar] [CrossRef] [PubMed]
- Emmons, R.A.; Crumpler, C.A. Gratitude as a human strength: Appraising the evidence. J. Soc. Clin. Psychol. 2000, 19, 56–69. [Google Scholar] [CrossRef]
- Navarro, J.L.; Tudge, J.R.H. What is gratitude? Ingratitude provides the answer. Hum. Dev. 2020, 64, 83–96. [Google Scholar] [CrossRef]
- Watkins, P.C.; Bell, J. Current theories and research in the psychology of gratitude. In Scientific Advances in Positive Psychology; Warren, M.A., Donaldson, S.I., Eds.; Praeger: Santa Barbara, CA, USA, 2017; pp. 103–129. [Google Scholar]
- Watkins, P.C.; Cruz, L.; Holben, H.; Kolts, R.L. Taking care of business? Grateful processing of unpleasant memories. J. Posit. Psychol. 2008, 3, 87–99. [Google Scholar] [CrossRef]
- Lau, B.H.P.; Cheng, C. Gratitude and coping among familial caregivers of persons with dementia. Aging Ment. Health 2017, 21, 445–453. [Google Scholar] [CrossRef]
- Nah, S.; Martire, L.M.; Zhaoyang, R. Perceived Gratitude, Role Overload, and Mental Health Among Spousal Caregivers of Older Adults. J. Gerontol. Ser. B 2022, 77, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Otobe, Y.; Suzuki, M.; Kimura, Y.; Koyama, S.; Kojima, I.; Ichikawa, T.; Terao, Y.; Yamada, M. Relationship between expression of gratitude by home-based care receivers and caregiver burden among family caregivers. Arch. Gerontol. Geriatr. 2021, 97, 104507. [Google Scholar] [CrossRef]
- McGee, J.S.; Davie, M.; Meraz, R.L.; Ambrose, M.; Boddie, S.C. “I can see the good, even when things around are rough”: Gratitude is a multi-dimensional resource for family caregivers of people with early-stage Alzheimer’s disease. J. Hum. Behav. Soc. Environ. 2024. [Google Scholar] [CrossRef]
- Frankl, V.E. From Death-Camp to Existentialism: A Psychiatrist’s Path to a New Therapy; Beacon Press: Boston, MA, USA, 1959; p. 468. [Google Scholar]
- Steger, M.F. Meaning in life. In Oxford Handbook of Positive Psychology; Lopez, S.J., Snyder, C.R., Eds.; Oxford University Press: New York, NY, USA, 2021; pp. 679–687. [Google Scholar]
- Borawski, D.; Siudak, A.; Pawelec, A.; Rozpara, B.; Zawanda, M. The interplay between loneliness, mindfulness and presence of meaning. Does search for meaning matter? Personal. Individ. Differ. 2021, 172, 110580. [Google Scholar] [CrossRef]
- Newman, D.B.; Nezlek, J.B.; Thrash, T.M. The dynamics of searching for meaning and presence of meaning in daily life. J. Personal. 2018, 86, 368–379. [Google Scholar] [CrossRef] [PubMed]
- Steger, M.F.; Kawabata, Y.; Shimai, S.; Otake, K. The meaningful life in Japan and the United States: Levels and correlates of meaning in life. J. Res. Personal. 2008, 42, 660–678. [Google Scholar] [CrossRef]
- Quinn, C.; Clare, L.; Woods, R.T. The impact of motivations and meanings on the wellbeing of caregivers of people with dementia: A systematic review. Int. Psychogeriatr. 2010, 22, 43–55. [Google Scholar] [CrossRef] [PubMed]
- McLennon, S.M.; Habermann, B.; Rice, M. Finding meaning as a mediator of burden on the health of caregivers of spouses with dementia. Aging Ment. Health 2011, 15, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Farran, C.J.; Miller, B.H.; Kaufman, J.E.; Davis, L. Race, finding meaning, and caregiver distress. J. Aging Health 1997, 9, 316–333. [Google Scholar] [CrossRef] [PubMed]
- Pearlin, L.I.; Bierman, A. Current issues and future directions in research into the stress process. In Handbook of the Sociology of Mental Health. Handbooks of Sociology and Social Research; Aneshensel, C.S., Phelan, J.C., Bierman, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; pp. 325–340. [Google Scholar]
- Pearlin, L.I.; Mullan, J.T.; Semple, S.J.; Skaff, M.M. Caregiving and the stress process: An overview of concepts and their measures. Gerontologist 1990, 30, 583–594. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988. [Google Scholar] [CrossRef]
- Steger, M.F.; Frazier, P.; Oishi, S.; Kaler, M. The Meaning in Life Questionnaire: Assessing the presence and search for meaning in life. J. Couns. Psychol. 2006, 53, 80–93. [Google Scholar] [CrossRef]
- Zarit, S.H.; Reever, K.E.; Bach-Peterson, J. Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist 1980, 20, 649–655. [Google Scholar] [CrossRef]
- Hébert, R.; Bravo, G.; Préville, M. Reliability, validity, and reference values of the Zarit Burden Interview for assessing informal caregivers of community-dwelling older persons with dementia. Can. J. Aging 2000, 19, 494–507. [Google Scholar] [CrossRef]
- Bryant, F.B.; Osowski, K.A.; Smith, J.L. Gratitude as a mediator of the effects of savoring on positive adjustment to aging. Int. J. Aging Hum. Dev. 2021, 92, 275–300. [Google Scholar] [CrossRef]
- Przepiorka, A.; Sobol-Kwapinska, M. People with positive time perspective are more grateful and happier: Gratitude mediates the relationship between time perspective and life satisfaction. J. Happiness Stud. 2020, 22, 113–126. [Google Scholar] [CrossRef]
- Algoe, S.B. Find, remind, and bind: The functions of gratitude in everyday relationships. Soc. Personal. Psychol. Compass 2012, 6, 455–469. [Google Scholar] [CrossRef]
- Manco, N.; Hamby, S. A meta-analytic review of interventions that promote meaning in life. Am. J. Health Promot. 2021, 35, 866–873. [Google Scholar] [CrossRef] [PubMed]
- Wong, P.T. Viktor Frankl’s meaning-seeking model and positive psychology. In Meaning in Positive and Existential Psychology; Springer: Berlin/Heidelberg, Germany, 2014; pp. 149–184. [Google Scholar]
- Cregg, D.R.; Cheavens, J.S. Gratitude interventions: Effective self-help? A meta-analysis of the impact on symptoms of depression and anxiety. J. Happiness Stud. 2021, 22, 413–445. [Google Scholar] [CrossRef]
- Davis, D.E.; Chloe, E.; Meyers, J.; Wade, N.; Varjas, K.; Gifford, A.; Quinn, A.; Hook, J.N.; Van Tongeren, D.R.; Griffin, B.J.; et al. Thankful for the little things: A meta-analysis of gratitude interventions. J. Couns. Psychol. 2016, 63, 20–31. [Google Scholar] [CrossRef]
- Jans-Beken, L.; Jacobs, N.; Janssens, M.; Peters, S.; Reijnders, J.; Lechner, L.; Lataster, J. Gratitude and health: An updated review. J. Posit. Psychol. 2020, 15, 743–782. [Google Scholar] [CrossRef]

{kind=link}
| Mean (SD) | n (%) | |
|---|---|---|
| Caregiver age in years (range: 22–87) | 64.65 (11.22) | |
| Caregiver gender | ||
| Male | 38 (30.2) | |
| Female | 88 (69.8) | |
| Caregiver education | ||
| High school or equivalent | 10 (8.0) | |
| Undergraduate | 82 (65.6) | |
| Graduate | 31 (24.8) | |
| Other | 2 (1.6) | |
| Caregiver ethnicity | ||
| Hispanic or Latino | 4 (3.2) | |
| Not Hispanic or Latino | 122 (96.8) | |
| Caregiver race | ||
| Person of Color | 3 (2.7) | |
| White | 122 (96.8) | |
| Unspecified | 1 (0.8) | |
| Relationship to person with dementia | ||
| Spouse/intimate partner | 83 (65.9) | |
| Adult child/grandchild | 29 (23.0) | |
| Other | 14 (11.1) |
| N | Range | Mean | SD | Cronbach’s Alpha | |
|---|---|---|---|---|---|
| Outcome | |||||
| Meaning in life presence | 126 | 8–30 | 22.78 | 5.30 | 0.81 |
| Meaning in life search | 126 | 0–30 | 13.53 | 8.03 | 0.89 |
| Primary Stressors | |||||
| Objective (intensity of care) * | 126 | 0–8 | 3.29 | 2.31 | N/A |
| Subjective (burden) | 126 | 5–83 | 30.92 | 15.25 | 0.94 |
| Secondary Stressors | |||||
| Caregiver age in years | 126 | 22–87 | 64.65 | 11.22 | N/A |
| Caregiver gender | 126 | 1–2 | 1.70 | 0.46 | N/A |
| Resources | |||||
| Social support | 126 | 10–20 | 17.14 | 2.54 | 0.74 |
| Gratitude | 126 | 17–36 | 30.93 | 5.04 | 0.81 |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| 1. Meaning in life presence | - | |||||||
| 2. Meaning in life search | −0.210 * | - | ||||||
| 3. Intensity of care | 0.129 | −0.131 | - | |||||
| 4. Caregiver burden | −0.260 ** | 0.214 * | 0.243 ** | - | ||||
| 5. Social support | 0.415 *** | −0.186 * | −0.076 | −0.248 ** | - | |||
| 6. Caregiver age | 0.124 | −0.089 | 0.133 | −0.136 | −0.010 | - | ||
| 7. Caregiver gender | 0.139 | −0.142 | 0.052 | 0.262 ** | 0.110 | −0.220 * | - | |
| 8. Gratitude | 0.619 *** | −0.180 * | 0.131 | −0.264 ** | 0.461 *** | −0.02 | 0.153 | - |
| Model 1 | Model 2 | |
|---|---|---|
| Intensity of care | 0.194 * | 0.084 |
| Caregiver burden | −0.253 ** | −0.121 |
| Caregiver age | 0.108 | 0.131 |
| Caregiver gender | 0.181 * | 0.104 |
| Social support | 0.348 *** | 0.155 |
| Gratitude | 0.491 *** | |
| Intercept | 4.769 | −4.096 |
| a F | 9.057 *** | 15.666 *** |
| b R2 | 0.27 | 0.44 |
| c ∆R2 | 0.17 *** | |
| N | 126 | 126 |
| Model 1 | Model 2 | |
|---|---|---|
| Intensity of care | −0.186 * | −0.186 * |
| Caregiver burden | 0.277 ** | 0.277 ** |
| Caregiver age | −0.073 | −0.073 |
| Caregiver gender | −0.209 * | −0.209 * |
| Social support | −0.109 | −0.108 |
| Gratitude | −0.002 | |
| Intercept | 26.64 | 26.69 |
| a F | 3.916 ** | 3.236 ** |
| b R2 | 0.14 | 0.14 |
| c ∆R2 | 0.00 | |
| N | 126 | 126 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McGee, J.S.; Polson, E.C.; Myers, D.R.; McClellan, A.M.; Ke, W.; Zhao, H.C.; Meraz, R. Gratitude Predicts Meaning in Life in Family Caregivers of Persons with Alzheimer’s Disease. Geriatrics 2024, 9, 72. https://doi.org/10.3390/geriatrics9030072
McGee JS, Polson EC, Myers DR, McClellan AM, Ke W, Zhao HC, Meraz R. Gratitude Predicts Meaning in Life in Family Caregivers of Persons with Alzheimer’s Disease. Geriatrics. 2024; 9(3):72. https://doi.org/10.3390/geriatrics9030072
Chicago/Turabian StyleMcGee, Jocelyn Shealy, Edward C. Polson, Dennis R. Myers, Angela M. McClellan, Weiming Ke, Holly Carlson Zhao, and Rebecca Meraz. 2024. "Gratitude Predicts Meaning in Life in Family Caregivers of Persons with Alzheimer’s Disease" Geriatrics 9, no. 3: 72. https://doi.org/10.3390/geriatrics9030072
APA StyleMcGee, J. S., Polson, E. C., Myers, D. R., McClellan, A. M., Ke, W., Zhao, H. C., & Meraz, R. (2024). Gratitude Predicts Meaning in Life in Family Caregivers of Persons with Alzheimer’s Disease. Geriatrics, 9(3), 72. https://doi.org/10.3390/geriatrics9030072