Abstract
Globally, one in eight people experience a mental disorder, which constitutes a leading cause of years lived with disability and disproportionately affects young people. Gaps in scientific knowledge have been identified, with limited studies in university students. This article presents an open-access database on mental health and family functioning, collected through a survey of undergraduate students in health sciences programs at a private university in Cali (Colombia). The purpose was to explore suicide risk, substance abuse and family functioning using three structured questionnaires (Family APGAR, Dast-10, and PANSI), together with sociodemographic variables, organized in four sections (family and peer support, substance use, suicidal ideation, and background). The results of the article correspond to the database description, which includes finally 574 records obtained from students of health sciences programs (medicine, dentistry, psychology, prehospital care, nursing, dental mechanics). The data are provided as raw, analyzable files (spreadsheet formats) free of charge from Mendeley Data. In conclusion, the scientific impact of these data lies in their potential to be reused by researchers and higher-education decision-makers for secondary analyses that guide the development of mental and family health interventions for groups linked to undergraduate programs in the health sector.
Dataset: Doi: 10.17632/yn9ptx7mnd.1 (accessed on 23 January 2026)
Dataset License: CC BY 4.0. Repository name: Mendeley data
1. Summary
The youth are a relevant vulnerability group from a public health perspective, given the multiple challenges they face during this stage of life, including normative and non-normative family changes, as well as family crises. Furthermore, university students face challenges related to the academic environment, which can generate risky behaviors that affect mental health in these population groups [1,2,3].
The 2022 World Mental Health Report highlights that mental disorders are very common in all countries and represent the leading cause of years lived with disability, generating both direct costs for the required healthcare and indirect costs for society related to lost productivity. The WHO estimates that one in eight people in the world live with a mental disorder, with suicide leading the cause of death among young people. Consequently, reducing suicide mortality is one of the targets of the United Nations Sustainable Development Goals [4].
In Colombia, reporting suicide attempts is mandatory for healthcare providers. Between 2018 and 2022, there was an increasing trend in incidence rates, ranging from 57.4 to 72.4 suicide attempts per 100,000 inhabitants [5], while in 2024, the rate was 73.5 [6]. Among the risk factors reported in analyses for this country between 2021 and 2024, persistent suicidal ideation stands out, ranging from 33.5% to 39.3%, as does the use of psychoactive substances, ranging from 12.8% to 15.1%, while other related factors included family problems, ranging from 30.0% to 36.7%.
Recent systematic literature reviews have found that family functioning and drug use are factors related to suicidal ideation in students, and gaps in scientific knowledge have also been identified, with limited studies on this problematic area in university students [1,2,3,7].
Previous studies have examined the Family APGAR questionnaire (used as a screening tool in healthcare for identifying potential family dysfunction) and have shown robust construct validity and unidimensional structure in Colombian and Latin American settings [8,9]. In parallel, the DAST-10 (used as a brief screening tool for problematic drug use) has also been validated among undergraduate students and other young populations [10,11,12,13], while other studies have examined the psychometric properties of the Positive and Negative Suicide Ideation (PANSI) inventory in clinical and non-clinical youth and university samples, showing adequate reliability and validity across diverse contexts [14,15,16,17].
However, there is still a paucity of openly accessible datasets that simultaneously integrate suicidal ideation, substance use and family functioning measures in university students from health sciences programs in Latin America, particularly in Colombia. This article therefore offers a novel contribution by providing a well-documented, open-access dataset that combines three standardized instruments (Family APGAR, DAST-10 and PANSI) and includes the sociodemographic information of participants in the survey [18], thereby facilitating secondary analyses, cross-study comparisons and methodological work in mental health research. This database is also useful in providing various analytical categories to guide decision-makers regarding interventions targeting mental health problems of high social burden.
2. Data Description
Information on specific characteristics and access to the database is presented in Table 1.

Table 1.
Characteristics of the database.
This manuscript introduces a database of responses to a survey conducted among university students in the Faculty of Health Sciences at a private university in Cali (a city in southwestern Colombia), which offers a wide range of academic programs in the health field. The objective of this article is to document an open-access database (Mendeley repository) with variables related to family functionality, suicidal ideation and drug use among university students in health sciences programs [18]. The data were collected using validated and widely used instruments, making them useful for other researchers in related fields. The database includes four sections: (i) Family APGAR and friend support test (ii) the Drug Use Questionnaire (Dast-10), (iii) PANSI suicidal ideation test, and (iv) sociodemographic data. The data are provided as a raw, analyzable file (spreadsheet format) and this is free-of-charge from Mendeley Data (doi: 10.17632/yn9ptx7mnd.1) under a CC BY 4.0 license. A detailed data dictionary is also provided in this available file, specifying the variable names and description, data types, and level of measurement for each item. A summary table is included in Appendix A (Table A1) with the total number of variables, their different types, and the scales used. The survey was administered in Spanish and subsequently translated into English for this manuscript, allowing reuse for secondary analyses. In the dataset file, each column represents a variable, and each row corresponds to one participant [18].
The survey was submitted by 583 university students, nine of whom were not considered due to inaccurate or missing information, and finally, 574 responses were included in the public database and the descriptive tables shown in the Appendix section of the manuscript. No imputation procedures were applied, and variables with missing values (when present) are explicitly coded as “no data” in the descriptive tables.
The survey results are presented in summary tables that describe the distribution of total scores and risk levels for Family APGAR, DAST-10 and PANSI subscales, as well as key sociodemographic and academic characteristics of the participants. Detailed frequency tables for each instrument and item are provided as supplementary materials to preserve completeness while avoiding excessively long tables in the main body of the manuscript (see Appendix B).
2.1. Sociodemographic Data Section
The sociodemographic section of the dataset contains variables that describe the basic profile of the participating university students, as detailed in Appendix B (Table A2). These variables include sex, gender identity, age, health insurance scheme, and academic program within the Faculty of Health Sciences, among other background characteristics
In the dataset file, each sociodemographic variable is organized as a separate column and coded according to the categories specified in the accompanying data dictionary. Categorical variables (e.g., sex, gender identity, health insurance scheme, academic program) are represented by labeled codes, while age is recorded using ordered categories, depending on the original questionnaire.
2.2. Family APGAR and Friend Support Section
This section of the database includes variables based on the Family APGAR and friend support test as shown in Appendix B (Table A3). The Family APGAR test is an instrument designed and developed by Gabriel Smilkstein in 1978 to approximate the patient’s family functioning, evaluating five dimensions: adaptation (A), participation (P), growth (G), affection (A), and resolve (R). Around 1987, Smilkstein incorporated two questions related to the support of friends into the questionnaire. The test is characterized by incorporating one item for each dimension (APGAR) through one question for each item and four answer options on a Likert-type scale, whose value is from 0 (never) to 4 (always), with a maximum possible score of 20 and a minimum possible score of 0 [8,9].
The score based on the Family APGAR test classifies the family function and is widely used across various international studies [9]. The distribution of the total score found through the survey among undergraduate students in health sciences programs at a private university in the city of Cali (Colombia) is shown in Table 2.
Table 2.
Distribution of total score and interpretation based on the Family APGAR test [9].
2.3. Drug Abuse Screening Test (DAST-10) Section
This section of the database includes ten variables based on the Drug Abuse Screening Test (DAST-10) test, as shown in Appendix B (Table A4). This questionnaire includes ten items through dichotomous Yes/No questions about drug use and its effects over the past year. A score of one is awarded for a “Yes” response and zero for a “No” response, except for one question (item #3), for which a “No” response receives 1 point. The total score is simply the sum of the 10 item scores. This total score can range from 0 to 10. It is used as a screening test to identify abuse of psychoactive drugs (excluding alcohol and tobacco) and recognizes five levels of risk. The classification of drug abuse derived from the DAST-10 is widely used across various international studies [10,11,12,13]. The distribution of total score found through the survey among undergraduate students in health sciences programs at a private university in the city of Cali (Colombia) is shown in Table 3.
Table 3.
Distribution of total score and interpretation based on the Drug Abuse Screening Test (DAST-10) [10,11,12,13].
2.4. PANSI Section
This section of the database includes variables with each item-level responses derived from the Positive and Negative Suicidal Ideation Inventory (PANSI) as shown in Appendix B (Table A5). In the dataset, each PANSI item is stored as an ordinal variable following the original 5-point response scale (0 = never to 4 = always).
Subscale scores are computed as the sum of eight items for the Positive Ideation (PI) and the remaining items for the Negative Suicidal Ideation (NSI) subscale. The PI subscale score reflects the frequency of positive, protective thoughts, whereas the NSI subscale score reflects the frequency of Negative Suicidal Ideation. Consistent with the original instrument, lower PI scores and higher NSI scores indicate greater risk of suicidal behavior.
The distribution of PI and NSI subscale scores found through the survey among undergraduate students in health sciences programs at a private university in the city of Cali (Colombia) is shown in Table 4, providing an overview of central tendency and variability for each dimension.
Table 4.
Score on the Positive Ideation (PI) subscale and Negative Suicidal Ideation (NSI) subscale.
2.5. Internal Consistency Reliability of the Measurement Instruments
Internal consistency reliability was assessed using Cronbach’s alpha coefficient, supplemented by Guttman’s Lambda 6 (G6) and Spearman–Brown (Table 5). For the DAST-10, which contains dichotomous items, Cronbach’s alpha is mathematically equivalent to the Kuder–Richardson formula 20 (KR-20). Item–total correlations were examined to identify potentially problematic items. Coefficients ≥ 0.70 were considered acceptable, 0.80–0.89 good, and ≥0.90 excellent [19,20].
Table 5.
Distribution internal consistency reliability of the measurement instruments (n = 574).
The internal consistency of the Family APGAR in this sample was good (Cronbach’s α = 0.88). The DAST-10 showed acceptable internal consistency in this sample (Spearman–Brown = 0.69, Guttman’s λ6 = 0.62), consistent with values reported in low-prevalence populations [21]. Item analysis revealed that item 3 (‘Are you unable to stop using drugs when you want to?’) had a low corrected item–total correlation (r = 0.13), and its removal would increase alpha to 0.70. The low prevalence of drug use in this sample (13.1% reported any use; items 7, 9, and 10 had prevalence < 1%) contributed to restricted variance and attenuated inter-item correlations.
The PANSI showed excellent internal consistency for the Negative Suicidal Ideation subscale (Cronbach’s α = 0.95) and acceptable consistency for the Positive Ideation subscale (Cronbach’s α = 0.79).
3. Methods
The database was obtained as part of a cross-sectional observational research project using a survey method. The study population consists of university students from Cali (the most populated city in southwest Colombia), enrolled in a private non-profit university that stands out for its long history and offers a wide range of academic programs in various disciplines in the field of health.
A convenience sampling strategy was used, inviting all undergraduate students enrolled in health sciences programs in the Faculty of Health during the data collection period. Given the descriptive and exploratory nature of this data descriptor, no a priori probabilistic sample size calculation was performed; instead, the aim was to obtain the largest possible number of respondents from the target population within the available time frame. The inclusion criterion was that participants had academic affiliations as students in one of the following undergraduate programs at the Faculty of Health Sciences: Dental Mechanics, Prehospital Care, Medicine, Dentistry, Psychology, and Nursing. The exclusion criterion was refusal to participate in the study during the informed consent process.
Data quality procedures included checking duplicated records, inconsistent responses and extensive missing information. Of the 583 submitted questionnaires, nine were excluded due to incomplete, duplicated or clearly inconsistent data, yielding a final analytic dataset of 574 students. A recruitment flow diagram summarizing the criterion of invited students, respondents, and excluded and included cases is also provided to illustrate the selection process (see Figure 1). The survey used Google Forms, which was distributed by emailing students and their student leaders. Face-to-face interviews were also conducted by trained personnel to ensure broader coverage of the study population. The data collection period was between April and May 2024.
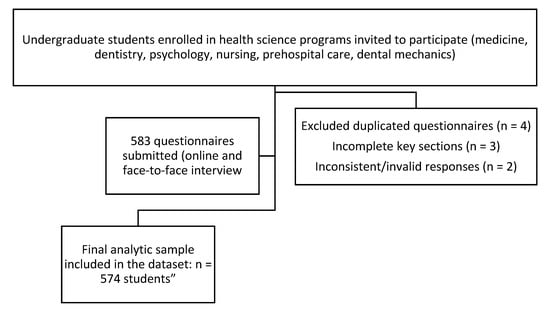
Figure 1.
Recruitment flow diagram for the survey.
To characterize the family functioning of university students and analyze relevant mental health issues, the survey used three structured questionnaires as instruments, which have been validated in previous research: (a) the Apgar test for family functioning and friend support, (b) the Drug Use Questionnaire (Dast-10), and (c) the PANSI suicide ideation test (risk factors and positive factors).
The Family APGAR instrument is widely used internationally and has been validated in multiple studies since its development by Gabriel Smilkstein in 1978, including validation for the Colombian population [8,9]. The Family APGAR score is used to determine family function level and interventions as shown in Table 6.
Table 6.
Family APGAR—interpretation of score [9].
The DAST-10 (Drug Abuse Screening Test) is a tool validated in various contexts [10,13], initially developed in 1982 by Skinner et al. Although no specific psychometric validation for the Colombian population has been reported, the DAST-10 has been used in Colombia as a screening tool in various contexts, and the Ministry of Health includes it among the recommended screening tests for the country [13]. The classification of drug abuse derived from DAST-10 is widely used across various international studies [10,11,12,13] as it simultaneously suggests intervention options as shown in Table 7.
Table 7.
DAST-10 (Drug Abuse Screening Test) —interpretation of score [11,12].
The PANSI (Positive and Negative Suicidal Ideation Inventory) questionnaire was developed by Osman et al. in 1998 [14]. This instrument is widely used to assess suicidal ideation and has been validated in various contexts, including validation for the Colombian population and university students [14,15,16,17]. This test identifies both risk (Negative Suicidal Ideation—NSI) and protective factors (Positive Ideation—PI) over the past two weeks [14,15,16,17]. Lower scores on the PANSI-PI subscale and higher scores on the PANSI-NSI reflect greater risk for suicidal behavior.
The survey included an initial section with information for the informed consent process, and at the end of the sections corresponding to the test mentioned above, questions regarding sociodemographic characteristics were also included.
It is worth noting that the strategy employed to avoid information bias consisted of using instruments with structured questionnaires validated in previous studies. In turn, to guarantee the quality of the data, the survey’s development was supervised by faculty members of the participating institution. Furthermore, a training phase was conducted for those responsible for data collection through face-to-face interviews, to familiarize them with the survey’s characteristics and the instruments it comprised.
The study protocol was approved by the Ethics Committee of Universidad Santiago de Cali (Act 17, 21 October 2022), and all participants provided informed consent prior to completing the survey. Survey data were collected anonymously, in accordance with national regulations for research involving human participants and the principles of the Declaration of Helsinki. Recognizing that the mental health topics included in the Google Form questionnaires are highly sensitive, we emphasized that the informed consent process included information on available healthcare services, as well as an email address for a healthcare professional. Furthermore, those identified as critical cases in the screening data analysis were subsequently contacted for appropriate follow-up.
4. User Notes and Limitations
The present Data Descriptor article focuses exclusively on the descriptive and structural aspects of the dataset to promote reproducibility and transparency, and can also support replication studies and facilitate secondary analyses. This open-access dataset enables analysis was aimed at examining associations between family functioning, drug use, and suicidal ideation; for developing and testing predictive models of suicide risk; exploring the joint effects of family functioning, peer support and substance use on mental health indicators; and comparing risk profiles across different health science programs. It can also be reused for methodological research, such as evaluating cut-off points or testing measurement invariance, and for teaching purposes in epidemiology and public health.
Nevertheless, some limitations are related to the cross-sectional design—the use of convenience sampling and the fact that data were obtained from a single private university in Cali, which may restrict the generalizability of findings to other institutional and regional contexts. It is also important to acknowledge the potential for participation bias. Recruitment relied on voluntary responses to an online Google Form and supplementary face-to-face interviews, which may have attracted students who were more available, more engaged with the institution, or more interested in mental health topics. Conversely, students experiencing more severe distress, higher academic overload, or lower institutional attachment might have been less likely to participate. As a result, the distribution of suicidal ideation, substance use, and family functioning scores in the dataset could differ from that of the broader population of health science students, and findings derived from secondary analyses should be interpreted with caution.
The moderate internal consistency of the DAST-10 (α = 0.60) in this sample may limit the precision of individual scores; however, the instrument remains appropriate for screening purposes at the group level [21].
Author Contributions
Conceptualization, N.A.-R. and A.B.-C.; methodology, N.A.-R. and J.M.A.-M.; software, J.M.A.-M.; formal analysis, J.M.A.-M.; data curation, N.A.-R. and J.M.A.-M.; writing—original draft preparation, N.A.-R.; writing—review and editing, A.B.-C. and J.M.A.-M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by “Dirección General de Investigaciones” of Universidad Santiago de Cali, project code: 445-621122-108; Title: Phase II: implementation of promotion and prevention strategies with social participation, for the improvement of the health of the population in social vulnerability of Cali. This research has been funded by Dirección General de Investigaciones of Universidad Santiago de Cali under call No. DGI-01-2026.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of Universidad Santiago de Cali (Act No 17, 21 October 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The dataset is open-access and can be found at Doi: 10.17632/yn9ptx7mnd.1.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| DAST | Drug Abuse Screening test |
| NSI | Negative Suicidal Ideation |
| PANSI | Positive and Negative Suicide Ideation Inventory |
| PI | Positive Ideation |
| WHO | World Health Organization |
Appendix A
A summary table is included with the total number of variables, their different types, and the scales used.
Table A1.
Summary table of the database.
Table A1.
Summary table of the database.
| Section/Category | Variables (Total Number) | Type of Variable | Scale Used/Measurement |
|---|---|---|---|
| Informed consent | one | Dichotomous categorical variable | Yes/no |
| Family APGAR | Nine | Polytomous categorical variable | Never = 0 Almost never = 1 Sometimes = 2 Almost always = 3 Always = 4 |
| DAST-10 | Ten | Dichotomous categorical variable | Yes/no |
| Gender identity Sex | one | Polytomous categorical variable | Female = 0 Male = 1 LGBTIQ+ = 2 No response = 3 |
| one | Dichotomous categorical variable | Female = 0 Male = 1 | |
| Age Relationship status | one | Polytomous categorical variable | Under 18 years old 18–22 years old 23–27 years old 28–32 years old |
| one | Polytomous categorical variable | Free relationship Married Single With boyfriend/girlfriend | |
| Health insurance scheme | one | Polytomous categorical variable | Contributory Linked or not affiliated Special (teachers, armed forces, police, Ecopetrol, other) Subsidized |
| Academic program | one | Polytomous categorical variable | Dental Mechanics Dentistry Medicine Nursing Prehospital Care Psychology |
| Apgar score | one | Discrete quantitative variable | 1, 2, 3, etc. |
| DAST-10 Score | one | Discrete quantitative variable | 1, 2, 3, etc. |
| Apgar score Interpretation | one | Polytomous categorical variable | Mild dysfunction (13–16) Moderate dysfunction (9–12) Normal family functioning (17–20) Severe dysfunction (0–8) |
| Apgar Classification | one | Discrete quantitative variable | 1, 2, 3, 4. |
| DAST-10 Classification | one | Discrete quantitative variable | 1, 2, 3, 4. |
| DAST-10 score Interpretation | one | Polytomous categorical variable | Low level (1–2) Moderate level (3–5) No problems reported (0) Severe level (9–10) Substantial level (6–8) |
Appendix B
The following tables provide detailed information on the survey results for each section and questionnaire included in the dataset described in this article.
Appendix B.1
Table A2.
Sociodemographic data of participants in the survey.
Table A2.
Sociodemographic data of participants in the survey.
| Item | Scale Used/Measurement | Frequency (n) | Percentage (%) |
|---|---|---|---|
| What gender do you identify with? | Female (0) Male (1) LGTBIQ+ (2) I prefer not to say (3) | 409 147 12 6 | 71.25 25.61 2.09 1.05 |
| Please indicate your sex (biological characteristics). | Women (0) Man (1) | 420 154 | 73.17 26.83 |
| How old are you? | 18–22 years old 23–27 years old 28–32 years old 33 or more years old 18 years old or less | 358 86 38 16 76 | 62.37 14.98 6.62 2.79 13.24 |
| What is your relationship status? | Single With boyfriend/girlfriend Free relationship Married No data | 322 213 21 14 4 | 56.10 37.11 3.66 2.44 0.70 |
| Please indicate the academic program in which you are enrolled at the University | Medicine Psychology Nursing Dental mechanics Prehospital care Dentistry No data | 214 105 93 59 57 41 5 | 37.28 18.29 16.20 10.28 9.93 7.14 0.87 |
Appendix B.2
Table A3.
Distribution of responses based on the Family APGAR and friend support test [8,9].
Table A3.
Distribution of responses based on the Family APGAR and friend support test [8,9].
| Item | Scale Used/Measurement | Frequency (n) | Percentage (%) |
|---|---|---|---|
| “I am satisfied with the help I receive from my family when I have a problem and/or need” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 10 19 91 166 288 | 1.74 3.31 15.85 28.92 50.17 |
| “I am satisfied with the way my family talks over things and shares problems with me” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 38 48 157 163 168 | 6.62 8.36 27.35 28.40 29.27 |
| “I am satisfied that my family accepts and supports my wishes to take on new activities or directions” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 10 14 90 143 317 | 1.74 2.44 15.68 24.91 55.23 |
| “I am satisfied with the way my family expresses affection and responds to my emotions, such as anger, sorrow, and love.” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 31 60 147 167 169 | 5.40 10.45 25.61 29.09 29.44 |
| “I am satisfied with the way my family and I share time together.” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 14 28 138 163 231 | 2.44 4.88 24.04 28.40 40.24 |
| “I am satisfied with the way my family and I share space” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 20 25 127 152 240 | 3.48 6.20 22.13 26.48 41.81 |
| “I am satisfied with the way my family and I share money” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 19 28 101 169 257 | 3.31 4.88 17.60 29.44 44.77 |
| “Do you have any close friends to whom you can search when you need help?” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 30 40 105 134 265 | 5.23 6.97 18.29 23.34 46.17 |
| “I am satisfied with the support I receive from my friends?” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 24 39 133 170 208 | 4.18 6.79 23.17 29.63 36.24 |
Appendix B.3
Table A4.
Distribution of responses based on the Drug Abuse Screening Test (DAST-10) [10,11,12,13].
Table A4.
Distribution of responses based on the Drug Abuse Screening Test (DAST-10) [10,11,12,13].
| Item | Scale Used/Measurement | Frequency (n) | Percentage (%) |
|---|---|---|---|
| “Have you used drugs other than those required for medical reasons?” | No (0) | 499 | 86.93 |
| Yes (1) | 75 | 13.07 | |
| “Do you abuse more than one drug at a time?” | No (0) | 562 | 97.91 |
| Yes (1) | 12 | 2.09 | |
| “Are you unable to stop abusing drugs when you want to?” | No (1) | 262 | 45.64 |
| Yes (0) | 312 | 54.36 | |
| “Have you ever had blackouts or flashbacks as a result of drug use?” | No (0) Yes (1) | 552 22 | 96.17 3.83 |
| “Do you ever feel bad or guilty about your drug use?” | No (0) Yes (1) | 520 54 | 90.59 9.41 |
| “Does your spouse (or parents) ever complain about your involvement with drugs?” | No (0) Yes (1) | 534 40 | 93.03 6.97 |
| “Have you neglected your family because of your use of drugs?” | No (0) Yes (1) | 569 5 | 99.13 0.87 |
| “Have you engaged in illegal activities in order to obtain drugs?” | No (0) Yes (1) | 565 9 | 98.43 1.57 |
| “Have you experienced withdrawal symptoms (felt sick) when you stopped taking drugs?” | No (0) Yes (1) | 569 5 | 99.13 0.87 |
| “Have you had medical problems as a result of your drug use (e.g., memory loss, hepatitis, convulsions, bleeding)?” | No (0) Yes (1) | 569 5 | 99.13 0.87 |
Appendix B.4
Table A5.
Distribution of responses based on PANSI (Positive and Negative Suicidal Ideation Inventory) [14,15,16,17].
Table A5.
Distribution of responses based on PANSI (Positive and Negative Suicidal Ideation Inventory) [14,15,16,17].
| Item | Scale Used/Measurement | Frequency (n) | Percentage (%) |
|---|---|---|---|
| “Seriously considered killing yourself because you could not live up to the expectations of other people?” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 424 77 55 12 6 | 73.87 13.41 9.58 2.09 1.05 |
| “Felt that you were in control of most situations in your life?” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 24 61 210 221 58 | 4.18 10.63 36.59 38.50 10.1 |
| “Felt hopeless about the future and you wondered if you should kill yourself?” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 405 69 77 14 9 | 70.56 12.02 13.41 2.44 1.57 |
| “Felt so unhappy about your relationship with someone you wished you were dead?” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 400 69 75 19 11 | 69.69 12.02 13.07 3.31 1.92 |
| “Thought about killing yourself because you could not accomplish something important in your life?” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 435 61 54 13 11 | 75.78 10.63 9.41 2.26 1.92 |
| “Felt hopeful about the future because things were working out well for you?” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 43 21 145 221 144 | 7.49 3.66 25.26 38.50 25.09 |
| “Thought about killing yourself because you could not find a solution to a personal problem?” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 413 72 59 18 12 | 71.95 12.54 10.28 3.14 2.09 |
| “Felt excited because you were doing well at school or at work?” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 16 5 104 147 302 | 2.79 0.87 18.12 25.61 52.61 |
| “Thought about killing yourself because you felt like a failure in life?” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 435 52 63 11 13 | 75.78 9.06 10.98 1.92 2.26 |
| “Thought that your problems were so overwhelming that suicide was seen as the only option to you?” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 430 67 49 16 12 | 74.91 11.67 8.54 2.79 2.09 |
| “Felt so lonely or sad you wanted to kill yourself so that you could end your pain?” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 406 72 58 20 18 | 70.73 12.54 10.10 3.48 3.14 |
| “Felt confident about your ability to handle most of the problems in your life?” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 31 36 133 222 152 | 5.40 6.27 23.17 38.68 26.48 |
| “Felt confident about achieving your goals in the future?” | Never (0) Hardly ever (1) Sometimes (2) Almost always (3) Always (4) | 11 26 109 184 244 | 1.92 4.53 18.99 32.06 42.51 |
References
- Sheldon, E.; Simmonds-Buckley, M.; Bone, C.; Mascarenhas, T.; Chan, N.; Wincott, M.; Gleeson, H.; Sow, K.; Hind, D.; Barkham, M. Prevalence and risk factors for mental health problems in university undergraduate students: A systematic review with meta-analysis. J. Affect. Disord. 2021, 287, 282–292. [Google Scholar] [CrossRef] [PubMed]
- Gastelu Soto, S.J.; Hurtado Deudor, L.E. Salud Mental en universitarios: Una revisión de la literatura científica en el tiempo. J. Neurosci. Public Health 2022, 2, 253–263. [Google Scholar] [CrossRef]
- Cancino Cedeño, E.M.; Párraga Mendoza, J.H.; Castillo Peña, D. Revisión Sistemática Sobre Salud Mental y Rendimiento Académico. Cienc. Lat. 2024, 8, 1833–1851. [Google Scholar] [CrossRef]
- WHO. World Mental Health Report: Transforming Mental Health for All. Executive Summary; World Health Organization: Geneva, Switzerland, 2022; Available online: https://www.who.int/es/publications/i/item/9789240050860 (accessed on 13 November 2025).
- INS. Informe de Evento Intento de Suicidio, 2022; Instituto Nacional de Salud-INS: Bogotá, Colombia, 2022. Available online: https://www.ins.gov.co/buscador-eventos/Informesdeevento/INTENTO%20DE%20SUICIDIO%20INFORME%202022.pdf (accessed on 11 September 2025).
- INS. Informe de Evento Intento de Suicidio 2024; Instituto Nacional de Salud-INS: Bogotá, Colombia, 2024. Available online: https://www.ins.gov.co/buscador-eventos/Informesdeevento/INTENTO%20DE%20SUICIDIO%20INFORME%20DE%20EVENTO%202024.pdf (accessed on 11 September 2025).
- Siabato Macías, E.F.; Salamanca Camargo, Y. Factores asociados a ideación suicida en universitarios. Psychol. Av. Discip. 2015, 9, 71–81. [Google Scholar] [CrossRef]
- Benítez Molina, A.; Caballero Badillo, M.C. Estudio psicométrico de las escalas de depresión ansiedad y funcionalidad familiar en estudiantes de la Universidad Industrial de Santander. Acta Colomb. Psicol. 2017, 20, 221–231. [Google Scholar] [CrossRef]
- Ascanio, C. Herramientas para trabajar con las familias. In Medicina, Amor y Familia; Saénz Lozada, M.L., Ed.; Universidad Nacional de Colombia: Bogotá, Colombia, 2017; Volume 1, pp. 39–60. [Google Scholar]
- Pautrat, M.; Barbier, E.; Lebeau, J.P. Identifying available substance use disorder screening tests feasible for use in primary care: A systematic review. Prev. Med. Rep. 2024, 38, 102610. [Google Scholar] [CrossRef] [PubMed]
- ASAM-American Society of Addiction Medicine. Drug Abuse Screening Test (DAST-10). Available online: https://www.asam.org/docs/default-source/education-docs/drug-abuse-screening-test_dast10_8-28-2017.pdf (accessed on 13 November 2025).
- Gómez Maqueo, E.; Gómez Hernández, H.; Morales Rodríguez, B.; Pérez Ramos, M. Uso del AUDIT y el DAST-10 para la identificación de abuso de sustancias psicoactivas y alcohol en adolescentes. Rev. Colomb. Psicol. 2009, 18, 9–17. [Google Scholar]
- Torres Sepúlveda, J.A.; Vallejo Zapata, V.J.; Villada Zapata, J. Consumo de alcohol y sustancias psicoactivas en estudiantes de la seccional oriente de la Universidad de Antioquia. Rev. Psicol. Univ. Antioq. 2015, 7, 97–108. [Google Scholar] [CrossRef]
- Osman, A.; Gutierrez, P.M.; Kopper, B.A.; Barrios, F.X.; Chiros, C.E. The positive and negative suicide ideation inventory: Development and validation. Psychol. Rep. 1998, 82, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Aloba, O.; Adefemi, S.; Aloba, T. Positive and Negative Suicide Ideation (PANSI) Inventory: Initial psychometric properties as a suicide risk screening tool among nigerian university students. Clin. Med. Insights Psychiatry 2018, 9, 1179557317751910. [Google Scholar] [CrossRef]
- Avendaño-Prieto, B.L.; Toro, R.; González, C.J.; Mejía-Vélez, S.; Hernández-Ortiz, M. Análisis factorial confirmatorio del inventario de ideación suicida positiva y negativa Pansi con muestras de Colombia y México. Divers. Perspect. Psicol. 2021, 17, 21–30. [Google Scholar] [CrossRef]
- Villalobos-Galvis, F.H. Validez y fiabilidad del Inventario de Ideación Suicida Positiva y Negativa-PANSI, en estudiantes colombianos. Univ. Psychol. 2010, 9, 509–520. [Google Scholar] [CrossRef]
- Acosta, N.; Angulo, J.M.; Botero Carvajal, A. Dataset on Suicide Risk, Substance Abuse, and Family Functioning Among University Students in a Health Faculty, 1st ed.; Mendeley Data: Cali, Colombia, 2025. [Google Scholar] [CrossRef]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Sijtsma, K. On the use, the misuse, and the very limited usefulness of Cronbach’s alpha. Psychometrika 2009, 74, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Yudko, E.; Lozhkina, O.; Fouts, A. A comprehensive review of the psychometric properties of the Drug Abuse Screening Test. J. Subst. Abus. Treat. 2007, 32, 189–198. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.