
Homemade Kefir Consumption Improves Skin Condition—A Study Conducted in Healthy and Atopic Volunteers

 ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
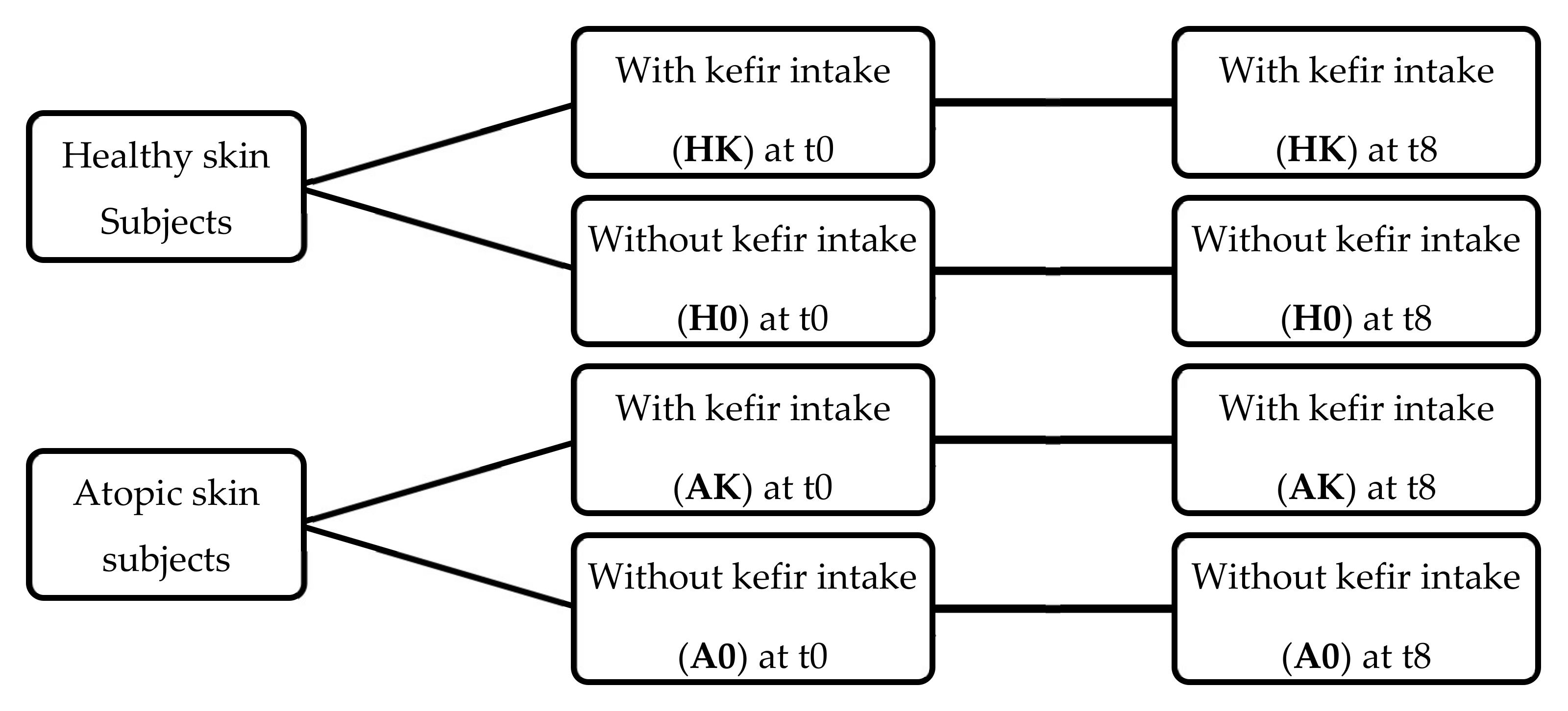
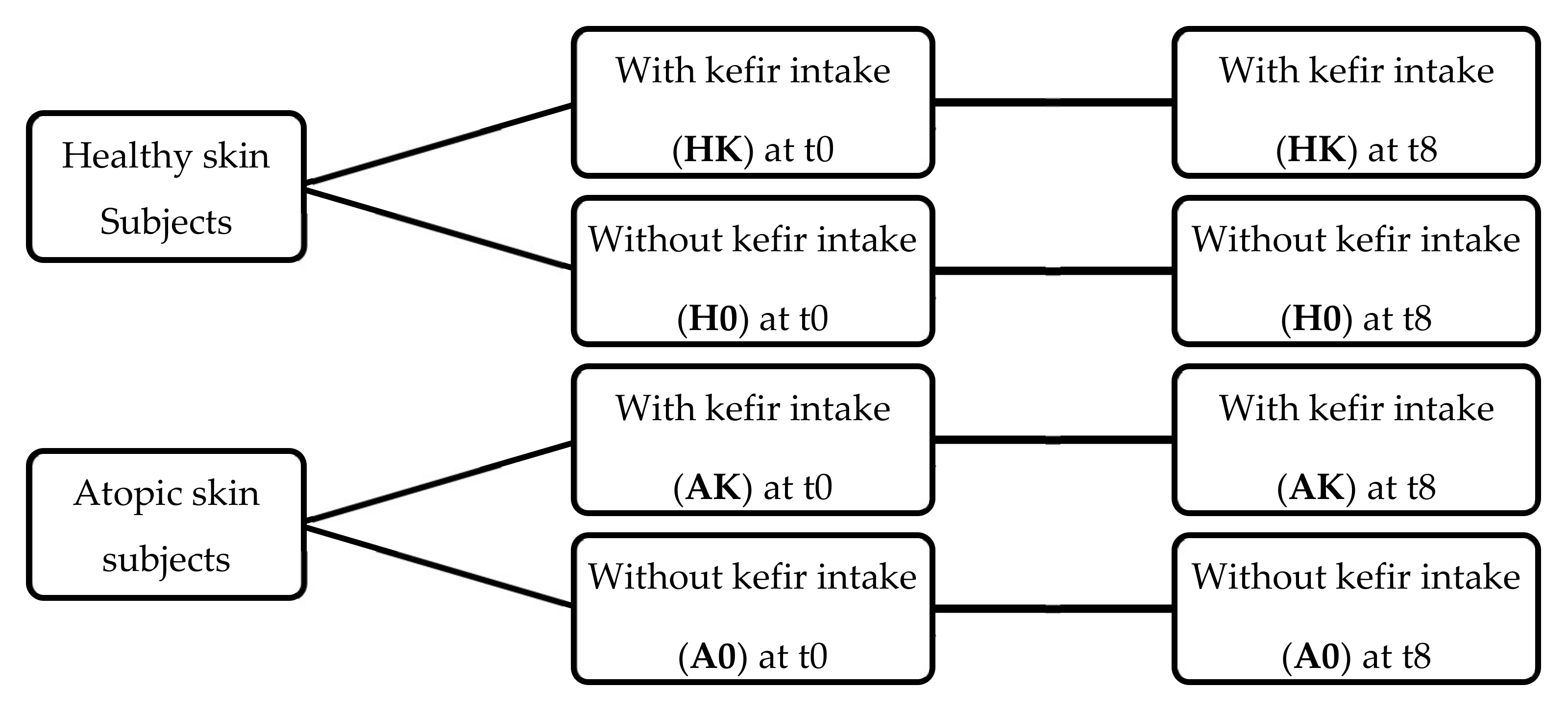
2.1. Study Design
2.2. Assessment of Dietary Intake
2.3. Kefir Intervention
2.4. Skin Measurements
2.5. SCORAD Index Assessment
2.6. Statistical Analysis
3. Results
3.1. Study Groups Characteristics
3.2. Skin Measurements
3.3. SCORAD Index Assessment
3.4. Adjusted Models for Skin Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stefanovic, N.; Irvine, A.D.; Flohr, C. The Role of the Environment and Exposome in Atopic Dermatitis. Curr. Treat. Options Allergy 2021, 8, 222–241. [Google Scholar] [CrossRef]
- Beam, A.; Clinger, E.; Hao, L. Effect of Diet and Dietary Components on the Composition of the Gut Microbiota. Nutrients 2021, 13, 2795. [Google Scholar] [CrossRef] [PubMed]
- Boelsma, E.; Hendriks, H.F.J.; Roza, L. Nutritional Skin Care: Health Effects of Micronutrients and Fatty Acids. Am. J. Clin. Nutr. 2001, 73, 853–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salem, I.; Ramser, A.; Isham, N.; Ghannoum, M.A. The Gut Microbiome as a Major Regulator of the Gut-Skin Axis. Front. Microbiol. 2018, 9, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Kim, H. Microbiome of the Skin and Gut in Atopic Dermatitis (AD): Understanding the Pathophysiology and Finding Novel Management Strategies. J. Clin. Med. 2019, 8, 444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.-Y.; Lee, E.; Park, Y.M.; Hong, S.J. Gut-Skin Axis in Atopic Dermatitis. Allergy Asthma Immunol Res 2018, 10, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Simonyte Sjödin, K.; Vidman, L.; Rydén, P.; West, C.E. Emerging Evidence of the Role of Gut Microbiota in the Development of Allergic Diseases. Curr. Opin. Allergy Clin. Immunol. 2016, 16, 390–395. [Google Scholar] [CrossRef]
- Bosman, E.S.; Albert, A.Y.; Lui, H.; Dutz, J.P.; Vallance, B.A. Skin Exposure to Narrow Band Ultraviolet (Uvb) Light Modulates the Human Intestinal Microbiome. Front. Microbiol. 2019, 10, 1–11. [Google Scholar] [CrossRef]
- O’Neill, C.A.; Monteleone, G.; McLaughlin, J.T.; Paus, R. The Gut-Skin Axis in Health and Disease: A Paradigm with Therapeutic Implications. BioEssays 2016, 38, 1167–1176. [Google Scholar] [CrossRef]
- Wieërs, G.; Belkhir, L.; Enaud, R.; Leclercq, S.; Philippart de Foy, J.-M.; Dequenne, I.; de Timary, P.; Cani, P.D. How Probiotics Affect the Microbiota. Front. Cell. Infect. Microbiol. 2020, 9, 454. [Google Scholar] [CrossRef] [Green Version]
- Makrgeorgou, A.; Leonardi-Bee, J.; Bath-Hextall, F.J.; Murrell, D.F.; Tang, M.L.K.; Roberts, A.; Boyle, R.J. Probiotics for Treating Eczema. Cochrane Database Syst. Rev. 2018, 2018, CD006135. [Google Scholar] [CrossRef]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. Expert Consensus Document: The International Scientific Association for Probiotics and Prebiotics Consensus Statement on the Scope and Appropriate Use of the Term Probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.S.; Trivedi, M.K.; Jha, A.; Lin, Y.F.; Dimaano, L.; García-Romero, M.T. Synbiotics for Prevention and Treatment of Atopic Dermatitis: A Meta-Analysis of Randomized Clinical Trials. JAMA Pediatr. 2016, 170, 236–242. [Google Scholar] [CrossRef]
- Kim, J.; Kim, B.E.; Leung, D.Y.M. Pathophysiology of Atopic Dermatitis: Clinical Implications. Allergy Asthma Proc. 2019, 40, 84–92. [Google Scholar] [CrossRef]
- Kim, B.E.; Leung, D.Y.M.M. Significance of Skin Barrier Dysfunction in Atopic Dermatitis. Allergy. Asthma Immunol. Res. 2018, 10, 207–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, E.B.M.; Skov, L.; Thyssen, J.P.; Jensen, P. Role of the Gut Microbiota in Atopic Dermatitis: A Systematic Review. Acta Derm. Venereol. 2018, 99, 5–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lolou, V.; Panayiotidis, M.I. Functional Role of Probiotics and Prebiotics on Skin Health and Disease. Fermentation 2019, 5, 41. [Google Scholar] [CrossRef] [Green Version]
- Finch, J.; Munhutu, M.N.; Whitaker-Worth, D.L. Atopic Dermatitis and Nutrition. Clin. Dermatol. 2010, 28, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Shen, C.; Ma, L. Treatment Efficacy of Probiotics on Atopic Dermatitis, Zooming in on Infants: A Systematic Review and Meta-Analysis. Int. J. Dermatol. 2018, 57, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Leite, A.M.d.O.; Miguel, M.A.L.; Peixoto, R.S.; Rosado, A.S.; Silva, J.T.; Paschoalin, V.M.F. Microbiological, Technological and Therapeutic Properties of Kefir: A Natural Probiotic Beverage. Brazilian J. Microbiol. 2013, 2, 341–349. [Google Scholar] [CrossRef]
- Farnworth, E.R. Kefir—A Complex Probiotic. Food Sci. Technol. Bull. Funct. Foods 2005, 2, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Aryana, K.J.; Olson, D.W. A 100-Year Review: Yogurt and Other Cultured Dairy Products. J. Dairy Sci. 2017, 100, 9987–10013. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Shevchenko, A.; Knaust, A.; Abuduresule, I.; Li, W.; Hu, X.; Wang, C.; Shevchenko, A. Proteomics Evidence for Kefir Dairy in Early Bronze Age China. J. Archaeol. Sci. 2014, 45, 178–186. [Google Scholar] [CrossRef]
- Garrote, G.L.; Abraham, A.G.; De Antoni, G.L. Inhibitory Power of Kefir: The Role of Organic Acids. J. Food Prot. 2000, 63, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Prado, M.R.; Blandón, L.M.; Vandenberghe, L.P.S.; Rodrigues, C.; Castro, G.R.; Thomaz-Soccol, V.; Soccol, C.R. Milk Kefir: Composition, Microbial Cultures, Biological Activities, and Related Products. Front. Microbiol. 2015, 6, 1177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maeda, H.; Zhu, X.; Omura, K.; Suzuki, S.; Kitamura, S. Effects of an Exopolysaccharide (Kefiran) on Lipids, Blood Pressure, Blood Glucose, and Constipation. BioFactors 2004, 22, 197–200. [Google Scholar] [CrossRef]
- Alves, E.; Ntungwe, E.N.; Gregório, J.; Rodrigues, L.M.; Pereira-Leite, C.; Caleja, C.; Pereira, E.; Barros, L.; Aguilar-Vilas, M.V.; Rosado, C.; et al. Characterization of Kefir Produced in Household Conditions: Physicochemical and Nutritional Profile, and Storage Stability. Foods 2021, 10, 1057. [Google Scholar] [CrossRef]
- Slattery, C.; Cotter, P.D.; O’Toole, P.W. Analysis of Health Benefits Conferred by Lactobacillus Species from Kefir. Nutrients 2019, 11, 1252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosa, D.D.; Dias, M.M.S.; Grześkowiak, Ł.M.; Reis, S.A.; Conceição, L.L.; Peluzio, M.D.C.G. Milk Kefir: Nutritional, Microbiological and Health Benefits. Nutr. Res. Rev. 2017, 30, 82–96. [Google Scholar] [CrossRef]
- Bourrie, B.C.T.; Willing, B.P.; Cotter, P.D. The Microbiota and Health Promoting Characteristics of the Fermented Beverage Kefir. Front. Microbiol. 2016, 7, 647. [Google Scholar] [CrossRef] [Green Version]
- Kesenkaş, H.; Gürsoy, O.; Özbaş, H. Kefir. In Fermented Foods in Health and Disease Prevention; Elsevier Inc.: Amsterdam, The Netherlands, 2016; pp. 339–361. [Google Scholar]
- Guzel-Seydim, Z.B.; Kok-Tas, T.; Greene, A.K.; Seydim, A.C. Review: Functional Properties of Kefir. Crit. Rev. Food Sci. Nutr. 2011, 51, 261–268. [Google Scholar] [CrossRef]
- Azizi, N.F.; Kumar, M.R.; Yeap, S.K.; Abdullah, J.O.; Khalid, M.; Omar, A.R.; Osman, M.A.; Mortadza, S.A.S.; Alitheen, N.B. Kefir and Its Biological Activities. Foods 2021, 10, 1210. [Google Scholar] [CrossRef]
- Rodrigues, K.L.; Carvalho, J.C.T.; Schneedorf, J.M. Anti-Inflammatory Properties of Kefir and Its Polysaccharide Extract. Inflammopharmacology 2005, 13, 485–492. [Google Scholar] [CrossRef]
- Rodrigues, K.L.; Caputo, L.R.; Carvalho, J.C.; Evangelista, J.; Schneedorf, J.M. Antimicrobial and Healing Activity of Kefir and Kefiran Extract. Int. J. Antimicrob. Agents 2005, 25, 404–408. [Google Scholar] [CrossRef]
- Carasi, P.; Racedo, S.M.; Jacquot, C.; Romanin, D.E.; Serradell, M.A.; Urdaci, M.C. Impact of Kefir Derived Lactobacillus Kefiri on the Mucosal Immune Response and Gut Microbiota. J. Immunol. Res. 2015, 2015, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wu, Y.; Wang, Y.; Xu, H.; Mei, X.; Yu, D.; Wang, Y.; Li, W. Antioxidant Properties of Probiotic Bacteria. Nutrients 2017, 9, 521. [Google Scholar] [CrossRef]
- Iraporda, C.; Abatemarco Júnior, M.; Neumann, E.; Nunes, Á.C.; Nicoli, J.R.; Abraham, A.G.; Garrote, G.L. Biological Activity of the Non-Microbial Fraction of Kefir: Antagonism against Intestinal Pathogens. J. Dairy Res. 2017, 84, 339–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huseini, H.F.; Rahimzadeh, G.; Fazeli, M.R.; Mehrazma, M.; Salehi, M. Evaluation of Wound Healing Activities of Kefir Products. Burns 2012, 38, 719–723. [Google Scholar] [CrossRef] [PubMed]
- Garrote, G.L.; Abraham, A.G.; De Antoni, G.L. Microbial Interactions in Kefir: A Natural Probiotic Drink. Biotechnol. Lact. Acid Bact. Nov. Appl. 2010, 327–340. [Google Scholar] [CrossRef]
- Bengoa, A.A.; Iraporda, C.; Garrote, G.L.; Abraham, A.G. Kefir Micro-Organisms: Their Role in Grain Assembly and Health Properties of Fermented Milk. J. Appl. Microbiol. 2019, 126, 686–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, R.M. The Influence of the Gut Microbiota on Host Physiology: In Pursuit of Mechanisms. Yale J. Biol. Med. 2016, 89, 285–297. [Google Scholar] [PubMed]
- Stiemsma, L.T.; Nakamura, R.E.; Nguyen, J.G.; Michels, K.B. Does Consumption of Fermented Foods Modify the Human Gut Microbiota? J. Nutr. 2020, 150, 1680–1692. [Google Scholar] [CrossRef] [PubMed]
- Healey, G.R.; Murphy, R.; Brough, L.; Butts, C.A.; Coad, J. Interindividual Variability in Gut Microbiota and Host Response to Dietary Interventions. Nutr. Rev. 2017, 75, 1059–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzpatrick, T. The Validity and Practicality of Sun-Reactive Skin Types I through VI. Arch. Dermatol. 1988, 124, 869–871. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Body Mass Index—BMI. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 16 October 2019).
- Saito, Y.; Mihara, T.; Maruyama, K.; Saito, J.; Ikeda, M.; Tomonaga, A.; Kumagai, T. Effects of Intake of Lactobacillus Casei Subsp. Casei 327 on Skin Conditions: A Randomized, Double-Blind, Placebo-Controlled, Parallel-Group Study in Women. Biosci. Microbiota Food Health 2017, 36, 111–120. [Google Scholar] [CrossRef] [Green Version]
- Gueniche, A.; Philippe, D.; Bastien, P.; Reuteler, G.; Blum, S.; Castiel-Higounenc, I.; Breton, L.; Benyacoub, J. Randomised Double-Blind Placebo-Controlled Study of the Effect of Lactobacillus Paracasei NCC 2461 on Skin Reactivity. Benef. Microbes 2014, 5, 137–145. [Google Scholar] [CrossRef]
- Ogawa, M.; Saiki, A.; Matsui, Y.; Tsuchimoto, N.; Nakakita, Y.; Takata, Y.; Nakamura, T. Effects of Oral Intake of Heat-Killed Lactobacillus Brevis SBC8803 (SBL88TM) on Dry Skin Conditions: A Randomized, Double-Blind, Placebo-Controlled Study. Exp. Ther. Med. 2016, 12, 3863–3872. [Google Scholar] [CrossRef]
- Roessler, A.; Friedrich, U.; Vogelsang, H.; Bauer, A.; Kaatz, M.; Hipler, U.C.; Schmidt, I.; Jahreis, G. The Immune System in Healthy Adults and Patients with Atopic Dermatitis Seems to Be Affected Differently by a Probiotic Intervention. Clin. Exp. Allergy 2008, 38, 93–102. [Google Scholar] [CrossRef]
- Yoshida, Y.; Seki, T.; Matsunaka, H.; Watanabe, T.; Shindo, M.; Yamada, N.; Yamamoto, O. Clinical Effects of Probiotic Bifidobacterium Breve Supplementation in Adult Patients with Atopic Dermatitis. Yonago Acta Med. 2010, 53, 37–45. [Google Scholar]
- Matsumoto, M.; Ebata, T.; Hirooka, J.; Hosoya, R.; Inoue, N.; Itami, S.; Tsuji, K.; Yaginuma, T.; Muramatsu, K.; Nakamura, A.; et al. Antipruritic Effects of the Probiotic Strain LKM512 in Adults with Atopic Dermatitis. Ann. Allergy Asthma Immunol. 2014, 113, 209–216. [Google Scholar] [CrossRef]
- Illner, A.-K.; Nöthlings, U.; Wagner, K.; Ward, H.; Boeing, H. The Assessment of Individual Usual Food Intake in Large-Scale Prospective Studies. Ann. Nutr. Metab. 2010, 56, 99–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutishauser, I.H. Dietary Intake Measurements. Public Health Nutr. 2005, 8, 1100–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garrote, G.L.L.; Abraham, A.G.G.; De Antoni, G.L.L. Preservation of Kefir Grains, a Comparative Study. LWT—Food Sci. Technol. 1997, 30, 77–84. [Google Scholar] [CrossRef]
- Garrote, G.L.; Abraham, A.G.; De Antoni, G.L. Chemical and Microbiological Characterisation of Kefir Grains. J. Dairy Res. 2001, 68, 639–652. [Google Scholar] [CrossRef]
- Diosma, G.; Romanin, D.E.; Rey-Burusco, M.F.; Londero, A.; Garrote, G.L. Yeasts from Kefir Grains: Isolation, Identification, and Probiotic Characterization. World J. Microbiol. Biotechnol. 2014, 30, 1–11. [Google Scholar] [CrossRef]
- Ouwehand, A.C. A Review of Dose-Responses of Probiotics in Human Studies. Benef. Microbes 2017, 8, 143–151. [Google Scholar] [CrossRef]
- Terpou, A.; Papadaki, A.; Lappa, I.K.; Kachrimanidou, V.; Bosnea, L.A.; Kopsahelis, N. Probiotics in Food Systems: Significance and Emerging Strategies towards Improved Viability and Delivery of Enhanced Beneficial Value. Nutrients 2019, 11, 1591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polańska, A.; Dańczak-Pazdrowska, A.; Silny, W.; Jenerowicz, D.; Osmola-Mańkowska, A.; Olek-Hrab, K. Evaluation of Selected Skin Barrier Functions in Atopic Dermatitis in Relation to the Disease Severity and Pruritus. Adv. Dermatology Allergol. Postepy Dermatologii Alergol. 2012, 29, 373–377. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.W.; Park, J.Y.; Na, G.Y.; Lee, S.J.; Lee, W.J. Correlation of Clinical Features and Skin Barrier Function in Adolescent and Adult Patients with Atopic Dermatitis. Int. J. Dermatol. 2006, 45, 698–701. [Google Scholar] [CrossRef]
- Sotoodian, B.; Maibach, H.I. Noninvasive Test Methods for Epidermal Barrier Function. Clin. Dermatol. 2012, 30, 301–310. [Google Scholar] [CrossRef]
- Alves, E.; Rijo, P.; Rodrigues, L.M.; Rosado, C. Determination of Relevant Endpoints to Evaluate the in Vivo Barrier Function in Cutaneous Health. Biomed. Biopharm. Res. 2019, 16, 80–88. [Google Scholar] [CrossRef]
- Rogiers, V. EEMCO Guidance for the Assessment of the Transepidermal Water Loss (TEWL) in Cosmetic Sciences. Skin Pharmacol. Appl. Skin Physiol. 2001, 14, 117–128. [Google Scholar] [CrossRef]
- Qassem, M.; Kyriacou, P. Review of Modern Techniques for the Assessment of Skin Hydration. Cosmetics 2019, 6, 19. [Google Scholar] [CrossRef] [Green Version]
- Fullerton, A.; Fischer, T.; Lahti, A.; Wlihelm, K.; Takiwaki, H.; Serup, J. Guidelines for Measurements Skin Colour and Erythema—A Report from the Standardization Group of the European Society of Contact Dermatitis. Contact Dermat. 1996, 35, 1–10. [Google Scholar] [CrossRef]
- European Task Force on Atopic Dermatitis Clinical and Laboratory Investigations European Task Force on Atopic Dermatitis Atopic Dermatitis Eczema Scoring Composite Index Severity. Dermatology 1993, 186, 23–31. [CrossRef]
- Oranje, A.P. Practical Issues on Interpretation of Scoring Atopic Dermatitis: SCORAD Index, Objective SCORAD, Patient-Oriented SCORAD and Three-Item Severity Score. Curr. Probl. Dermatol. 2011, 41, 149–155. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation; World Health Organization (WHO): Geneva, Switzerland, 2011; ISBN 9789241501491. [Google Scholar]
- European Food Safety Authority (EFSA). Dietary Reference Values for Nutrients Summary Report. EFSA Support. Publ. 2017, 14, e15121E. [Google Scholar] [CrossRef] [Green Version]
- Sonnenburg, J.L.; Bäckhed, F. Diet–Microbiota Interactions as Moderators of Human Metabolism. Nature 2016, 535, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.; Wu, X.; Yu, S.; Huynh, M.; Jena, P.K.; Nguyen, M.; Wan, Y.J.Y.; Hwang, S.T. Short-Term Exposure to a Western Diet Induces Psoriasiform Dermatitis by Promoting Accumulation of IL-17A–Producing Γδ T Cells. J. Invest. Dermatol. 2020, 140, 1815–1823. [Google Scholar] [CrossRef]
- Rusu, E.; Enache, G.; Cursaru, R.; Alexescu, A.; Radu, R.; Onila, O.; Cavallioti, T.; Rusu, F.; Posea, M.; Jinga, M.; et al. Prebiotics and Probiotics in Atopic Dermatitis (Review). Exp. Ther. Med. 2019, 18, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Lew, L.C.; Liong, M.T. Bioactives from Probiotics for Dermal Health: Functions and Benefits. J. Appl. Microbiol. 2013, 114, 1241–1253. [Google Scholar] [CrossRef]
- Notay, M.; Foolad, N.; Vaughn, A.R.; Sivamani, R.K. Probiotics, Prebiotics, and Synbiotics for the Treatment and Prevention of Adult Dermatological Diseases. Am. J. Clin. Dermatol. 2017, 18, 721–732. [Google Scholar] [CrossRef]
- Peluzio, M.d.C.G.; Dias, M.d.M.; Martinez, J.A.; Milagro, F.I. Kefir and Intestinal Microbiota Modulation: Implications in Human Health. Front. Nutr. 2021, 8, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Dimidi, E.; Cox, S.; Rossi, M.; Whelan, K. Fermented Foods: Definitions and Characteristics, Gastrointestinal Health and Disease. Nutrients 2019, 11, 1806. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.H.; Jeong, D.; Kim, H.; Seo, K.H. Modern Perspectives on the Health Benefits of Kefir in next Generation Sequencing Era: Improvement of the Host Gut Microbiota. Crit. Rev. Food Sci. Nutr. 2019, 59, 1782–1793. [Google Scholar] [CrossRef] [PubMed]
- Üstün-Aytekin, Ö.; Şeker, A.; Arısoy, S. The Effect of in Vitro Gastrointestinal Simulation on Bioactivities of Kefir. Int. J. Food Sci. Technol. 2020, 55, 283–292. [Google Scholar] [CrossRef]
- Lee, D.E.; Huh, C.-S.; Ra, J.; Choi, I.-D.; Jeong, J.-W.; Kim, S.-H.; Ryu, J.H.; Seo, Y.K.; Koh, J.S.; Lee, J.-H.; et al. Clinical Evidence of Effects of Lactobacillus Plantarum HY7714 on Skin Aging: A Randomized, Double Blind, Placebo-Controlled Study. J. Microbiol. Biotechnol. 2015, 25, 2160–2168. [Google Scholar] [CrossRef]
- Mori, N.; Kano, M.; Masuoka, N.; Konno, T.; Suzuki, Y.; Miyazaki, K.; Ueki, Y. Effect of Probiotic and Prebiotic Fermented Milk on Skin and Intestinal Conditions in Healthy Young Female Students. Biosci. Microbiota Food Health 2016, 35, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Kano, M.; Masuoka, N.; Kaga, C.; Sugimoto, S.; Iizuka, R.; Manabe, K.; Sone, T.; Oeda, K.; Nonoka, C.; Miyazaki, K.; et al. Consecutive Intake of Fermented Milk Containing Bifidobacterium Breve Strain Yakult and Galacto-Oligosaccharides Benefits Skin Condition in Healthy Adult Women. Biosci. Microbiota Food Health 2013, 21, 33–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.-J.; Kim, Y.-J.; Kang, M.-J.; Seo, J.-H.; Kim, H.-Y.; Jeong, S.K.; Lee, S.-H.; Kim, J.-M.; Hong, S.-J. A Novel Mouse Model of Atopic Dermatitis with Epicutaneous Allergen Sensitization and the Effect of Lactobacillus Rhamnosus. Exp. Dermatol. 2012, 21, 672–675. [Google Scholar] [CrossRef]
- Baba, H.; Masuyama, A.; Yoshimura, C.; Aoyama, Y.; Takano, T.; Ohki, K. Oral Intake of Lactobacillus Helveticus-Fermented Milk Whey Decreased Transepidermal Water Loss and Prevented the Onset of Sodium Dodecylsulfate-Induced Dermatitis in Mice. Biosci. Biotechnol. Biochem. 2010, 74, 18–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellis, S.R.; Nguyen, M.; Vaughn, A.R.; Notay, M.; Burney, W.A.; Sandhu, S.; Sivamani, R.K. The Skin and Gut Microbiome and Its Role in Common Dermatologic Conditions. Microorganisms 2019, 7, 550. [Google Scholar] [CrossRef] [Green Version]
- Rather, I.A.; Bajpai, V.K.; Kumar, S.; Lim, J.; Paek, W.K.; Park, Y.H. Probiotics and Atopic Dermatitis: An Overview. Front. Microbiol. 2016, 7, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.O.; Ah, Y.M.; Yu, Y.M.; Choi, K.H.; Shin, W.G.; Lee, J.Y. Effects of Probiotics for the Treatment of Atopic Dermatitis: A Meta-Analysis of Randomized Controlled Trials. Ann. Allergy Asthma Immunol. 2014, 113, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Drago, L.; Iemoli, E.; Rodighiero, V.; Nicola, L.; De Vecchi, E.; Piconi, S. Effects of Lactobacillus Salivarius LS01 (DSM 22775) Treatment on Adult Atopic Dermatitis: A Randomized Placebo-Controlled Study. Int. J. Immunopathol. Pharmacol. 2011, 24, 1037–1048. [Google Scholar] [CrossRef]
- Holm, E.A.; Wulf, H.C.; Thomassen, L.; Jemec, G.B.E. Assessment of Atopic Eczema: Clinical Scoring and Noninvasive Measurements. Br. J. Dermatol. 2007, 157, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Iemoli, E.; Trabattoni, D.; Parisotto, S.; Borgonovo, L.; Toscano, M.; Rizzardini, Z.; Clerici, M.; Ricci, E.; Fusi, A.; De Vecchi, E.; et al. Probiotics Reduce Gut Microbial Translocation and Improve Adult Atopic Dermatitis. J. Clin. Gastroenterol. 2012, 46, S33–S40. [Google Scholar] [CrossRef] [PubMed]
- Proksch, E.; Fölster-Holst, R.; Bräutigam, M.; Sepehrmanesh, M.; Pfeiffer, S.; Jensen, J.M. Role of the Epidermal Barrier in Atopic Dermatitis: Academy CME. JDDG—J. Ger. Soc. Dermatol. 2009, 7, 899–911. [Google Scholar] [CrossRef]
- Calabrese, E.J.; Mattson, M.P.; Dhawan, G.; Kapoor, R.; Calabrese, V.; Giordano, J. Hormesis: A Potential Strategic Approach to the Treatment of Neurodegenerative Disease. Int. Rev. Neurobiol. 2020, 155, 271–301. [Google Scholar] [CrossRef]
- Calabrese, E.J.; Baldwin, L.A. Defining Hormesis. Hum. Exp. Toxicol. 2002, 21, 91–97. [Google Scholar] [CrossRef]
- Feng, T.; Wang, J. Oxidative Stress Tolerance and Antioxidant Capacity of Lactic Acid Bacteria as Probiotic: A Systematic Review. Gut Microbes 2020, 12, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Odamaki, T.; Xiao, J.Z.; Yonezawa, S.; Yaeshima, T.; Iwatsuki, K. Improved Viability of Bifidobacteria in Fermented Milk by Cocultivation with Lactococcus Lactis Subspecies Lactis. J. Dairy Sci. 2011, 94, 1112–1121. [Google Scholar] [CrossRef]
- Ji, H.; Li, X.-K. Oxidative Stress in Atopic Dermatitis. Oxid. Med. Cell. Longev. 2016, 2016, 2721469. [Google Scholar] [CrossRef]
- Bertino, L.; Guarneri, F.; Cannavò, S.P.; Casciaro, M.; Pioggia, G.; Gangemi, S. Oxidative Stress and Atopic Dermatitis. Antioxidants 2020, 9, 196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lisowski, P.; Kannan, P.; Mlody, B.; Prigione, A. Mitochondria and the Dynamic Control of Stem Cell Homeostasis. EMBO Rep. 2018, 19, e45432. [Google Scholar] [CrossRef] [PubMed]
- Sreedhar, A.; Aguilera-Aguirre, L.; Singh, K.K. Mitochondria in Skin Health, Aging, and Disease. Cell Death Dis. 2020, 11, 444. [Google Scholar] [CrossRef] [PubMed]
- Vardjan, T.; Mohar Lorbeg, P.; Rogelj, I.; Čanžek Majhenič, A. Characterization and Stability of Lactobacilli and Yeast Microbiota in Kefir Grains. J. Dairy Sci. 2013, 96, 1–8. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| General Inclusion criteria |
|
| Atopic inclusion criteria |
|
| General Non-inclusion/Exclusion criteria |
|
| Physiological Characteristics | Healthy Group (n = 33) | Atopic Group (n = 19) | ||||
|---|---|---|---|---|---|---|
| HK | H0 | p-Value | AK | A0 | p-Value | |
| Gender | 0.208 | 0.330 | ||||
| Female, n (%) | 12 (92.3) | 15 (75.0) | 9 (100) | 9 (90.0) | ||
| Male, n (%) | 1 (7.7) | 5 (25.0) | 0 | 1 (10.0) | ||
| Age, mean (SD), years | 28.9 (13.0) | 25.8 (7.71) | 0.739 * | 30.4 (12.3) | 32.9 (12.1) | 0.538 * |
| Skin Phototype | 0.388 | 0.252 | ||||
| Type II, n (%) | 6 (46.2) | 7 (35.0) | 4 (44.4) | 2 (20.0) | ||
| Type III, n (%) | 5 (38.5) | 12 (60.0) | 5 (55.6) | 8 (80.0) | ||
| Type IV n (%) | 2 (15.3) | 1 (5.0) | 0 | 0 | ||
| BMI, mean (SD), kg/m2 | 22.6 (3.68) | 23.3 (4.19) | 0.439 * | 22.7 (3.40) | 22.8 (2.18) | 0.540 * |
| Waist circumference, mean (SD), cm | 72.4 (9.19) | 77.5 (13.6) | 0.328 * | 77.2 (8.67) | 78.6 (6.02) | 0.653 * |
| Deviation of Skin Parameters | Healthy Group (n = 33) | Atopic Group (n = 19) | ||||
|---|---|---|---|---|---|---|
| HK | H0 | p-Value | AK | A0 | p-Value | |
| TEWL | ||||||
| Forearm | −0.302 (−0.489, 0.0149) | 0.0058 (−0.12, 0.081) | 0.018 | −0.529 (−0.601, −0.428) | 0.148 (−0.571, 0.578) | <0.001 |
| Leg | −0.0976 (−0.321, 0.244) | 0.0143 (−0.248, 0.116) | 0.854 | −0.288 (−0.333, −0.176) | 0.507 (0.0656, 1.36) | <0.001 |
| Forehead | −0.220 (−0.375, −0.0448) | −0.0128 (−0.196, 0.152) | 0.036 | −0.457 (−0.612, −0.243) | 0.150 (−0.0571, 0.636) | <0.001 |
| Hydration | ||||||
| Forearm | −0.0196 (−0.0784, 0.0959) | −0.184 (−0.256, −0.0132) | 0.034 | 0.452 (0.300, 0.560) | −0.0810 (−0.282, 0.119) | 0.001 |
| Leg | 0.143 (−0.134, 0.212) | −0.0270 (−0.246, 0.0896) | 0.320 | 0.250 (0.213, 0.522) | 0.0470 (−0.0894, 0.220) | 0.034 |
| Forehead | 0.128 (−0.0447, 0.373) | −0.127 (−0.325, 0.0356) | 0.012 | 0.244 (0.146, 0.537) | 0.0450 (−0.297, 0.466) | 0.086 |
| Erythema | ||||||
| Forearm | −0.0556 (−0.186, −0.0170) | −0.0745 (−0.111, 0.0119) | 0.685 | −0.133 (−0.185, −0.0692) | −0.0404 (−0.191, 0.129) | 0.221 |
| Deviation of Skin Parameters at Forearm | Healthy Group (n = 33) | ||
|---|---|---|---|
| HK | H0 | p-Value | |
| TEWL SLS | −0.2931 (−0.510, −0.180) | 0.0878 (−0.0924, 0.243) | <0.001 |
| Hydration SLS | 0.0000 (−0.133, 0.106) | 0.0065 (−0.0889, 0.138) | 0.347 |
| Erythema SLS | −0.0287 (−0.0371, 0.0644) | 0.0144 (−0.0775, 0.135) | 0.825 |
| Deviation of SCORAD Index | Atopic Group (n = 19) | ||
|---|---|---|---|
| AK | A0 | p-Value | |
| SCORAD | −0.626 (−0.758, −0.491) | 0.0402 (−0.0293, 0.273) | <0.001 |
| Deviation of Skin Parameters | β for Kefir Intake (p-Value) | ||
|---|---|---|---|
| Model 1 | Model 2 | Model 3 | |
| TEWL | |||
| Forearm | −0.596 (<0.001) | −0.597 (<0.001) | −0.625 (<0.001) |
| Leg | −0.304 (0.029) | −0.323 (0.018) | −0.332 (0.020) |
| Forehead | −0.501 (<0.001) | −0.502 (<0.001) | −0.524 (<0.001) |
| Hydration | |||
| Forearm | 0.481 (<0.001) | 0.458 (<0.001) | 0.539 (<0.001) a |
| Leg | 0.294 (0.034) | 0.267 (0.042) | 0.347 (0.006) a |
| Forehead | 0.362 (0.008) | 0.346 (0.011) | 0.358 (0.012) |
| SCORAD Index (**) | −0.910 (<0.001) | n.a. | −0.866 (<0.001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alves, E.; Gregório, J.; Baby, A.R.; Rijo, P.; Rodrigues, L.M.; Rosado, C. Homemade Kefir Consumption Improves Skin Condition—A Study Conducted in Healthy and Atopic Volunteers. Foods 2021, 10, 2794. https://doi.org/10.3390/foods10112794
Alves E, Gregório J, Baby AR, Rijo P, Rodrigues LM, Rosado C. Homemade Kefir Consumption Improves Skin Condition—A Study Conducted in Healthy and Atopic Volunteers. Foods. 2021; 10(11):2794. https://doi.org/10.3390/foods10112794
Chicago/Turabian StyleAlves, Emília, João Gregório, André Rolim Baby, Patrícia Rijo, Luis M. Rodrigues, and Catarina Rosado. 2021. "Homemade Kefir Consumption Improves Skin Condition—A Study Conducted in Healthy and Atopic Volunteers" Foods 10, no. 11: 2794. https://doi.org/10.3390/foods10112794
APA StyleAlves, E., Gregório, J., Baby, A. R., Rijo, P., Rodrigues, L. M., & Rosado, C. (2021). Homemade Kefir Consumption Improves Skin Condition—A Study Conducted in Healthy and Atopic Volunteers. Foods, 10(11), 2794. https://doi.org/10.3390/foods10112794