Case vignette
A 69-year-old, right-handed man was admitted to our department because of anterograde amnesia. Additionally, signs of retrograde amnesia were present affecting the day before admission and events from the recent past in particular. The episode started during gardening. The patient was oriented regarding his personal identity, location and situation, but was disoriented about the time. There was no clouding of consciousness. In addition to repetitive questioning, we noticed an amnestic aphasia. There were no pre-existing diseases and he had not experienced a similar episode before. The neurological examination revealed no other neurological deficits, especially no focal motor or sensory signs. A laboratory examination did not reveal any abnormalities except for dyslipidaemia. The EEG showed an alpha basic rhythm with a few, scattered, left-sided accentuated steep transients without focal slowing and without typical epileptiform discharges.
On day 1 after admission, the patient’s symptoms had resolved completely, but an amnesic gap of about 8 hours remained.
Questions
- What are typical clinical and neuropsychological findings of your assumed diagnosis? Would you expect any results on MRI?
Further examinations: On the day after admission, bedside-testing of neurocognitive functions revealed mild continuing deficits, for example delayed recall of objects was still impaired. Therefore, we performed cerebral magnetic resonance imaging (MRI; fig. 1 and fig. 2).
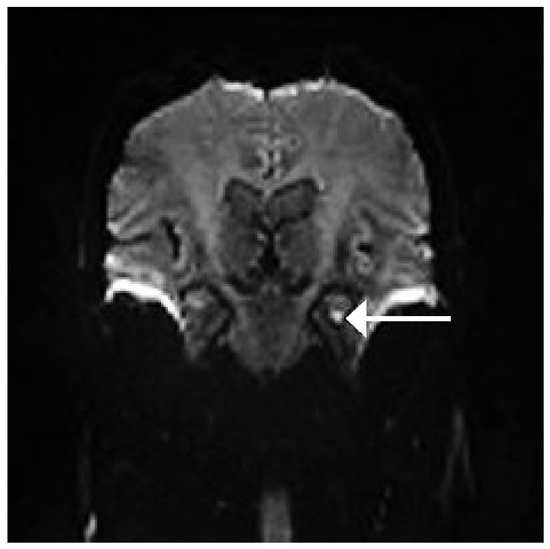
Figure 1.
Coronal DWI MRI. Arrow indicates diffusion restriction in the left hippocampus.
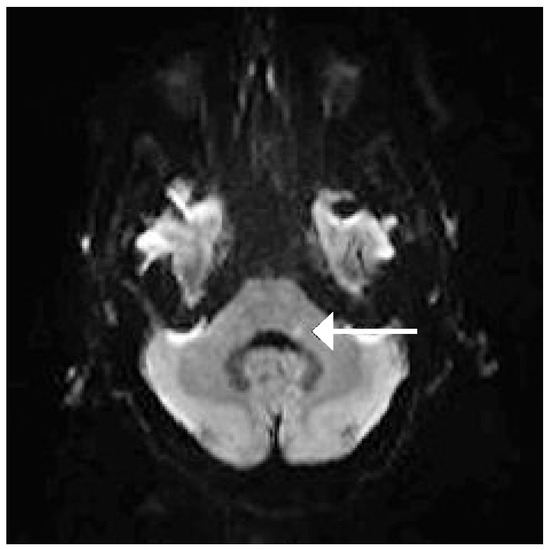
Figure 2.
Axial DWI MRI. Arrow indicates diffusion restriction in the ponto-cerebellar region.
- 2.
- What are the main findings of this cerebral MRI and are they consistent with your expectations?
- 3.
- Specify relevant differential diagnoses of acute amnesic syndromes and “red flags” of every diagnosis.
Diagnosis
Acute cerebral ischaemia in the posterior circulation with 2 small separated lesions in the hippocampus region and the ponto-cerebellar region.
Further examinations (cont.): Following the diagnosis of cerebral ischaemia in the posterior circulation, we initiated further aetiological examinations. A cardiac embolic source could not be detected. Duplex sonography of cranial vessels revealed a mild general atheromatosis without relevant stenoses. A recently diagnosed arterial hypertension and dyslipidaemia constituted vascular risk factors. Neuropsychological assessment, carried out 4 days after, exposed a mild cognitive impairment of the visual memory.
Epicrisis: We initiated a secondary stroke prophylaxis with aspirin and treatment of vascular risk factors. The patient was discharged and was able to return to work without significant impairment.
Take-home message
- –
- An alert neurocognitive and physical examination is essential for clinical diagnosis of transient global amnesia (TGA). Focal neurological signs or persistent neurocognitive deficits are “red flags” and might indicate a different aetiology.
- –
- Remember, differential diagnoses like transient ischaemic attack (TIA) or cerebral ischaemia in the posterior circulation or transient epileptic amnesia which might present as amnesic syndromes as well.
- –
- Although diagnosis of TGA is primarily based on clinical findings, neuroimaging with a high-resolution scan can support the diagnosis.
- –
- TGA is a transient functional and structural perturbation in memory-relevant structures of the hippocampus.
- –
- There is no recommendation for aspirin in TGA.
- –
- Several studies did not find an association between stroke risk factors and TGA.
- –
- Patients with TGA have a better prognosis with regard to further cerebrovascular events compared to patients with a TIA.
- –
- Hyperintense DWI lesions with corresponding hypointense lesions in the ADC map are highly suspicious for cerebral ischaemia but are not of definite evidence. They have also been observed in nonischaemic events like multiple sclerosis, encephalitis, epilepsia, venous thrombosis [1].
- –
- DWI lesions of the hippocampus are not related to an increased rate of vascular risk factors or increase of microangiopathic white matter hyperintensities and lacunar lesions [2].
Answers
Answer 1
Typical clinical and neuropsychological findings of TGA
- –
- Acute and unpredictable onset of anterograde amnesia (from few minutes, most often from 4 to 8 hours) with impairment of new learning ability for verbal and non-verbal learning, and accompanied by repetitive questioning.
- –
- Retrograde amnesia (spanning several days to several years), including executive function and recognition.
- –
- Disorientation of time and place, preserved auto-orientation.
- –
- Consciousness remains undisturbed.
- –
- Lack of concomitant focal neurological symptoms or epileptic signs.
- –
- Resolution of symptoms within 24 hours.
- –
- Cognitive impairment is limited to amnesia.
- –
- Memory impairments are unspecific (deficits of recent semantic information and episodic memories).
- –
- Procedural memory is preserved.
- –
- Mild vegetative symptoms (headache, nausea, emesis, dizziness) might be present during acute phase.
- –
- In >50%, precipitating events occur before attacks: emotional stress, physical effort (gardening, housework) and water contact/temperature change [5].
- –
- In 2006, Bartsch et al. stated that verbal memory deficits represent lesions of the dominant hemisphere, while deficits in the visuo-spatial memory are associated with the non-dominant hemisphere [3].
- –
- Some mild neuropsychological deficits might last for some days and weeks after an acute TGA episode [4].
MRI findings in patients with TGA
- –
- In 85% of TGA patients, a lesion can be detected if highresolution MRI is used.
- –
- A small focal hyperintense lesion is found in the lateral hippocampus, corresponding to the CA1 sector (sommer sector = border zone between the upper and lower hippocampal artery [1] of the hippocampal cornu ammonis). CA1 neurons are likely to be involved in memory consolidation [3] and place memory [6].
- –
- The size of lesions ranges from 1 to 5 mm.
- –
- Lesions can be seen on DWI with a correlate in the ADC map and T2-weighted images. A disturbance in diffusion indicates a cytotoxic oedema which is found in ischaemic and non-ischaemic disorders (multiple sclerosis, encephalitis, epilepsy).
- –
- Detection of DWI lesions depends on time: 24–72 h after onset, at the latest within 48–72 h after onset.
- –
- After 4–6 months, the lesions are completely reversible and do not leave any structural sequelae or neuropsychological deficits [3].
Answer 2
- –
- There are two hyperintense lesions on DWI (with corresponding hypointense lesions in the ADC map; not shown):
- –
- one at the typical location for a transient global amnesia at the left hippocampus cornu ammonis, although too large compared to those lesions typically seen in TGA patients;
- –
- another one in the left dorsolateral medulla oblongata.
Answer 3
- –
- Cerebral ischaemia or haemorrhage in the posterior circulation (hippocampal/thalamic). Red flags might be focal neurological signs and impairment of consciousness as well as headache.
- –
- Epileptic seizures may present as transient epileptic amnesia. Red flags might be duration of less than 1 hour, more than 2 episodes within 6 months, loss of personal identity, stereotyped movements, no repetitive questions and pathological interictal EEG. If there is a strong suspicion of epileptic seizure, then long-term sleep-EEG is recommended.
- –
- Post-traumatic amnesia. Red flags are history of trauma and transient loss of consciousness.
- –
- Intoxication. Red flags are altered consciousness, pathological laboratory findings and toxicological screening as well as a suggestive history in most cases.
- –
- Psychogenic amnesia, dissociative disorders. Red flags are a history of psychiatric disorders, young age, and often retrograde amnesia only.
References
- Sedlaczek, O.; Hirsch, JG; Grips, E; Peters, CNA; Gass, A; Wöhrle, J; et al. Detection of delayed focal MR changes in the lateral hippocampus in transient global amnesia. Neurology 2004, 62, 2165–70. [Google Scholar] [CrossRef] [PubMed]
- Enzinger, C; Thimary, F; Kapeller, P; Ropele, S; Schmidt, R; Ebner, F; Fazekas, F. Transient Global Amnesia: Diffusion-Weighted Imaging Lesions and cerebrovascular disease. Stroke 2008, 39, 2219–25. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, T; Alfke, K; Stingele, R; Rohr, A; Freitag-Wolf, S; Jansen, O; Deuschl, G. Selective affection of hippocampal CA-1 neurons in patients with transient global amnesia without long-term sequelae. Brain 2006, 129, 2874–84. [Google Scholar] [CrossRef] [PubMed]
- Quinette, P; Guillery, B; Desgranges, B; de la Sayette, V; Viader, F; Eustache, F. Working memory and executive functions in transient global amnesia. Brain 2003, 126, 1917–34. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Quinette, P; Guillery-Girard, B; Dayan, B; de la Sayette, V; Marqius, S; Viader, F; et al. What does transient global amnesia really mean? Review of the literature and thorough study of 142 cases. Brain 2006, 129, 1640–58. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, T; Schönfeld, R; Müller, FJ; Alfke, K; Leplow, B; Aldenhoff, J; et al. Focal lesions of human hippocampal CA1 neurons in transient global amnesia impair place memory. Science 2010, 328(5984), 1412–5. [Google Scholar] [CrossRef] [PubMed]


This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial No Derivatives (CC BY-NC-ND) 4.0 License.