Development and Validation of the Social Network Addiction Scale (SNAddS-6S)



Abstract
1. Introduction
1.1. Social Network Addiction: Concept and Measurement
1.2. Social Network Addiction and Related Variables
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. Social Networks Addiction
2.3.2. Social Network Overuse
2.3.3. Social Anxiety
2.3.4. Loneliness
2.3.5. Life Satisfaction
2.3.6. Self-Esteem
2.4. Statistical Analyses
3. Results
3.1. Preliminary Analyses: Common Method Variance
3.2. Stage 1: Reducing the Items and Exploring the Factorial Analysis
3.2.1. Missing Data, Correlation between Items, and Reliability Analyses
3.2.2. Exploratory Factorial Analysis for the Social Networks Addiction (SNAdd) Scale
3.2.3. Exploratory Factorial Analysis for the Short SNAddS-6S
3.3. Stage 2: Confirming the Factorial Analysis
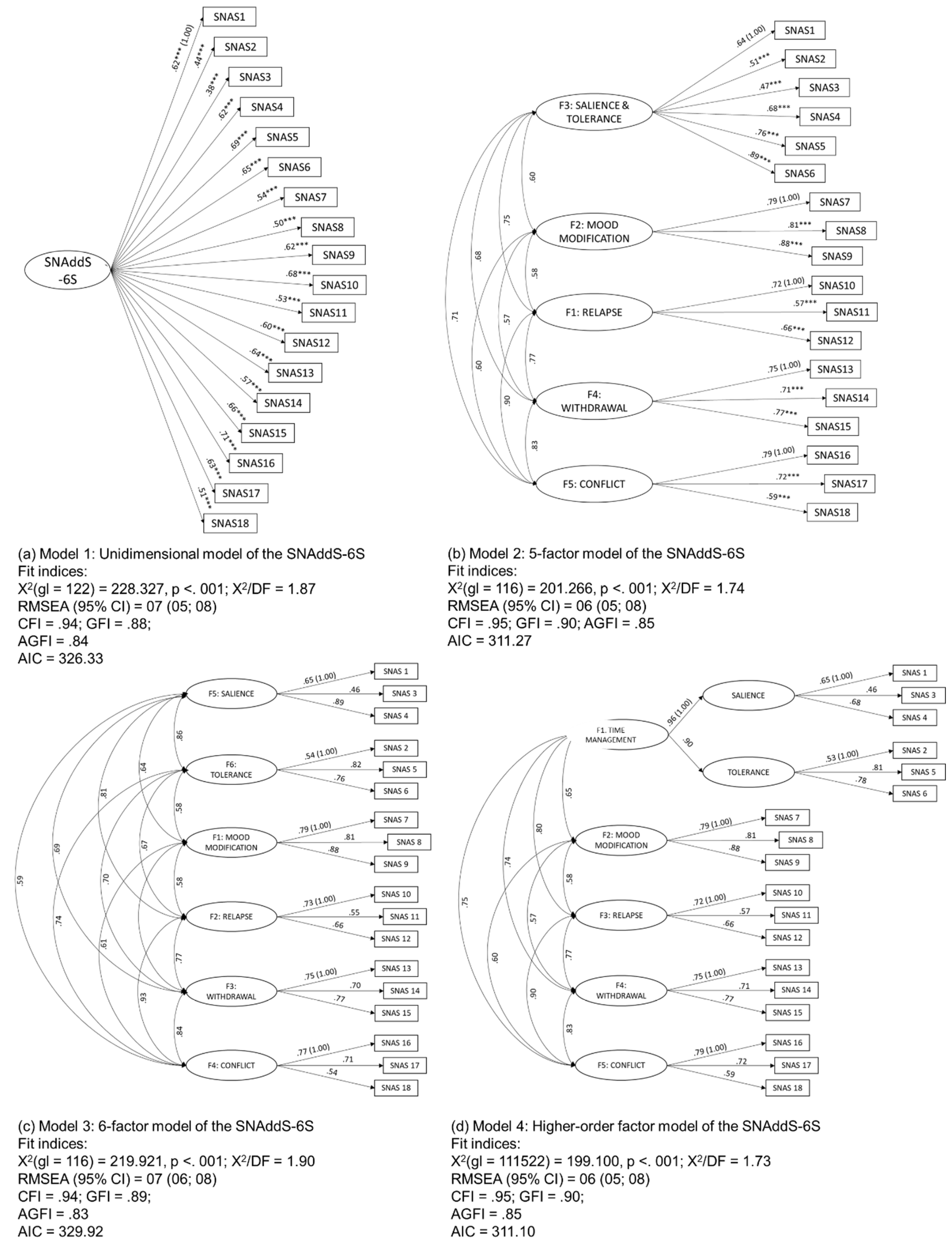
3.3.1. Confirmatory Factorial Analysis for the SNAddS-6S
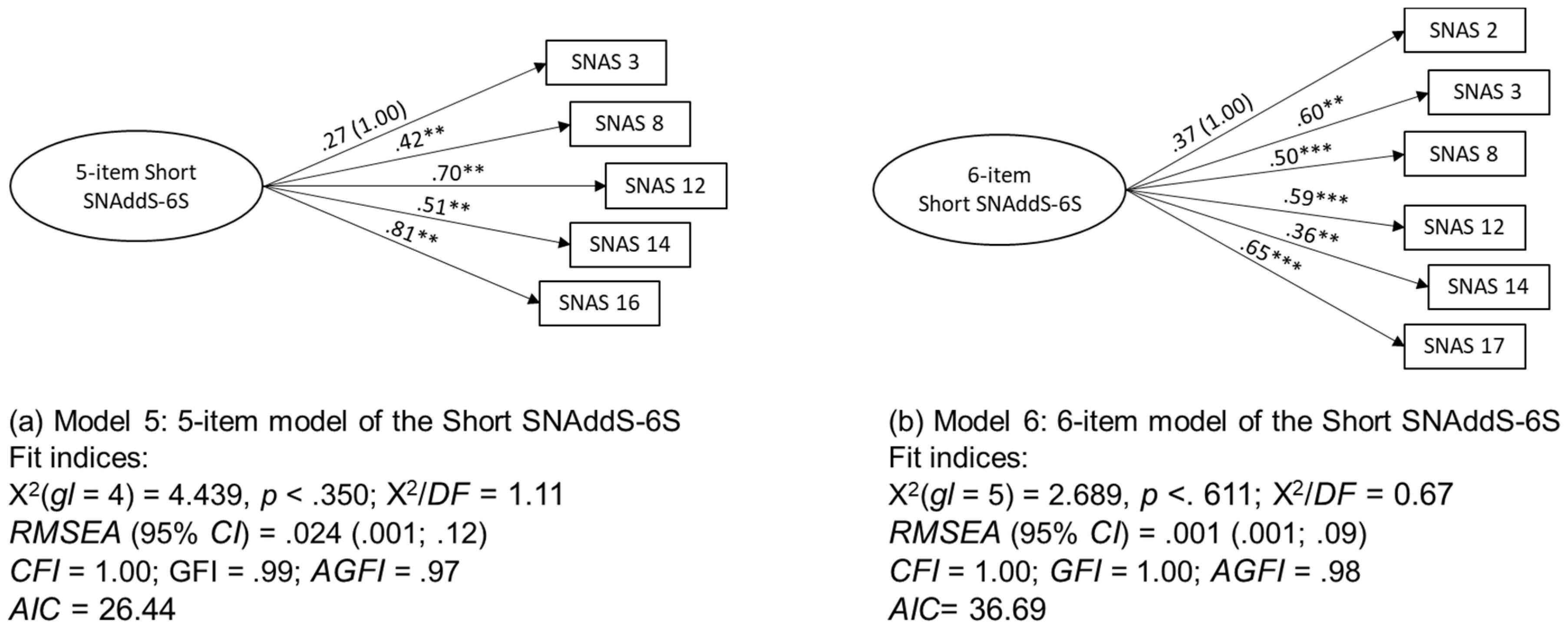
3.3.2. Confirmatory Factorial Analysis for the Short SNAddS-6S
3.4. Exploring the External Validity of the Large and Short SNAddS-6S
4. Discussion
4.1. The SNAddS-6S, a Multidimensional Valid and Reliable Scale, and the Short SNAddS-6S, a Unidimensional Valid and Reliable Scale
4.2. Limitations and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kuss, D.; Griffiths, M. Social Networking Sites and Addiction: Ten Lessons Learned. Int. J. Environ. Res. Public Health 2017, 14, 311. [Google Scholar] [CrossRef]
- Liu, D.; Kirschner, P.A.; Karpinski, A.C. A meta-analysis of the relationship of academic performance and Social Network Site use among adolescents and young adults. Comput. Hum. Behav. 2017, 77, 148–157. [Google Scholar] [CrossRef]
- Marino, C.; Gini, G.; Vieno, A.; Spada, M.M. The associations between problematic Facebook use, psychological distress and well-being among adolescents and young adults: A systematic review and meta-analysis. J. Affect. Disord. 2018, 226, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Bankoglu, T.; Cerkez, Y. The Social Network Addiction Scale: A Scale Development Study. Rev. Cercet. Interv. Soc. 2019, 66, 378–388. [Google Scholar] [CrossRef]
- Carbonell, X.; Panova, T. A critical consideration of social networking sites’ addiction potential. Addict. Res. Theory 2017, 25, 48–57. [Google Scholar] [CrossRef]
- Oberst, U.; Renau, V.; Chamarro, A.; Carbonell, X. Gender stereotypes in Facebook profiles: Are women more female online? Comput. Hum. Behav. 2016, 60, 559–564. [Google Scholar] [CrossRef]
- Oberst, U.; Wegmann, E.; Stodt, B.; Brand, M.; Chamarro, A. Negative consequences from heavy social networking in adolescents: The mediating role of fear of missing out. J. Adolesc. 2017, 55, 51–60. [Google Scholar] [CrossRef]
- Andreassen, C.S.; Billieux, J.; Griffiths, M.D.; Kuss, D.J.; Demetrovics, Z.; Mazzoni, E.; Pallesen, S. The relationship between addictive use of social media and video games and symptoms of psychiatric disorders: A large-scale cross-sectional study. Psychol. Addict. Behav. 2016, 30, 252–262. [Google Scholar] [CrossRef]
- Blachnio, A.; Przepiorka, A.; Pantic, I. Association between Facebook addiction, self-esteem and life satisfaction: A cross-sectional study. Comput. Hum. Behav. 2016, 55, 701–705. [Google Scholar] [CrossRef]
- Xanidis, N.; Brignell, C.M. The association between the use of social network sites, sleep quality and cognitive function during the day. Comput. Hum. Behav. 2016, 55, 121–126. [Google Scholar] [CrossRef]
- Andreassen, C.S.; Pallesen, S. Social Network Site Addiction—An Overview. Curr. Pharm. Des. 2014, 20, 4053–4061. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, M. A ‘components’ model of addiction within a biopsychosocial framework. J. Subst. Use 2005, 10, 191–197. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5TM, 5th ed.; American Psychiatric Association Publishing, Inc.: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- García del Castillo, J.A. Technological addictions: The rise of social networks. Heal. Addict. 2013, 13, 5–14. [Google Scholar]
- Siddiqui, S.; Singh, T. Social media its impact with positive and negative aspects. Int. J. Comput. Appl. Technol. Res. 2016, 5, 71–75. [Google Scholar] [CrossRef]
- O’Connor, K.M.; Gladstone, E. Beauty and social capital: Being attractive shapes social networks. Soc. Netw. 2018, 52, 42–47. [Google Scholar] [CrossRef]
- Kesici, Ş.; Şahin, İ. A Comparative Study of Uses of the Internet among College Students with and without Internet Addiction. Psychol. Rep. 2009, 105 (Suppl. 3), 1103–1112. [Google Scholar] [CrossRef]
- Andreassen, C.S. Online Social Network Site Addiction: A Comprehensive Review. Curr. Addict. Rep. 2015, 2, 175–184. [Google Scholar] [CrossRef]
- Andreassen, C.S.; Pallesen, S.; Griffiths, M.D. The relationship between addictive use of social media, narcissism, and self-esteem: Findings from a large national survey. Addict. Behav. 2017, 64, 287–293. [Google Scholar] [CrossRef]
- Monacis, L.; de Palo, V.; Griffiths, M.D.; Sinatra, M. Social networking addiction, attachment style, and validation of the Italian version of the Bergen Social Media Addiction Scale. J. Behav. Addict. 2017, 6, 178–186. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Broström, A.; Nilsen, P.; Griffiths, M.D.; Pakpour, A.H. Psychometric validation of the Persian Bergen Social Media Addiction Scale using classic test theory and Rasch models. J. Behav. Addict. 2017, 6, 620–629. [Google Scholar] [CrossRef]
- Baumeister, R.F.; Leary, M.R. The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychol. Bull. 1995, 117, 497–529. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Wiederhold, B.K.; Cipresso, P. Psychology of social media: From technology to identity. In The Psychology of Social Networking: Personal Experience in Online Communities; Riva, G., Wiederhold, B.K., Cipresso, P., Eds.; De Gruyter Open: Warsaw, Poland, 2016; pp. 1–11. [Google Scholar]
- Kuss, D.J.; Griffiths, M.D. Internet Addiction in Psychotherapy; Palgrave: London, UK, 2015. [Google Scholar]
- Kuss, D.J.; Griffiths, M.D. Internet Gaming Addiction: A Systematic Review of Empirical Research. Int. J. Ment. Health Addict. 2012, 10, 278–296. [Google Scholar] [CrossRef]
- Gökdaş, İ.; Kuzucu, Y. Social Network Addiction Scale: The Validity and Reliability Study of Adolescent and Adult Form. Int. J. Assess. Tools Educ. 2019, 6, 396–414. [Google Scholar] [CrossRef]
- Andreassen, C.S.; Torsheim, T.; Brunborg, G.S.; Pallesen, S. Development of a Facebook Addiction Scale. Psychol. Rep. 2012, 110, 501–517. [Google Scholar] [CrossRef] [PubMed]
- Guedes, E.; Sancassiani, F.; Carta, M.G.; Campos, C.; Machado, S.; Spear King, A.L.; Nardi, A.E. Internet Addiction and Excessive Social Networks Use: What About Facebook? Clin. Pract. Epidemiol. Ment. Heal. 2016, 12, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Müller, K.W.; Dreier, M.; Beutel, M.E.; Duven, E.; Giralt, S.; Wölfling, K. A hidden type of Internet addiction? Intense and addictive use of social networking sites in adolescents. Comput. Hum. Behav. 2016, 55, 172–177. [Google Scholar] [CrossRef]
- Dias, P.C.; Cadime, I.; Del Castillo-López, Á.G.; García-Castillo, F.; García del Castillo, J.A. Excessive Facebook use among Portuguese university students: Contributes of the adaptation of the Bergen Facebook Addiction. Heal Addict. 2018, 18, 131–139. [Google Scholar]
- Echeburúa, E. Factores de riesgo y factores de protección en la adicción a las nuevas tecnologías y redes sociales en jóvenes y adolescentes. Rev. Española Drogodepend. 2012, 4, 435–448. [Google Scholar]
- Shepherd, R.-M.; Edelmann, R.J. Reasons for Internet use and social anxiety. Pers. Individ. Differ. 2005, 39, 949–958. [Google Scholar] [CrossRef]
- Enez Darcin, A.; Noyan, C.; Nurmedov, S.; Yilmaz, O.; Dilbaz, N. Smartphone Addiction in Relation with Social Anxiety and Loneliness Among University Students in Turkey. Eur. Psychiatry 2015, 30, 505. [Google Scholar] [CrossRef]
- Enez Darcin, A.; Kose, S.; Noyan, C.O.; Nurmedov, S.; Yilmaz, O.; Dilbaz, N. Smartphone addiction and its relationship with social anxiety and loneliness. Behav. Inf. Technol. 2016, 35, 520–525. [Google Scholar] [CrossRef]
- Fayazi, M.; Hasani, J. Structural relations between brain-behavioral systems, social anxiety, depression and Internet addiction: With regard to revised Reinforcement Sensitivity Theory (r-RST). Comput. Hum. Behav. 2017, 72, 441–448. [Google Scholar] [CrossRef]
- Ozsaker, M.; Muslu, G.K.; Kahraman, A.; Beytut, D.; Yardimci, F.; Basbakkal, Z. A Study on the Effects of Loneliness, Depression and Perceived Social Support on Problematic Internet Use among University Students. Anthropologist 2015, 19, 533–542. [Google Scholar] [CrossRef]
- Bozoglan, B.; Demirer, V.; Sahin, I. Loneliness, self-esteem, and life satisfaction as predictors of Internet addiction: A cross-sectional study among Turkish university students. Scand. J. Psychol. 2013, 54, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Yao, M.Z.; Zhong, Z. Loneliness, social contacts and Internet addiction: A cross-lagged panel study. Comput. Hum. Behav. 2014, 30, 164–170. [Google Scholar] [CrossRef]
- Cheng, C.; Li, A.Y. Internet Addiction Prevalence and Quality of (Real) Life: A Meta-Analysis of 31 Nations across Seven World Regions. Cyberpsychol. Behav. Soc. Netw. 2014, 17, 755–760. [Google Scholar] [CrossRef]
- Cash, H.; Rae, C.D.; Steel, A.H.; Winkler, A. Internet Addiction: A Brief Summary of Research and Practice. Curr. Psychiatry Rev. 2012, 8, 292–298. [Google Scholar] [CrossRef]
- Samaha, M.; Hawi, N.S. Relationships among smartphone addiction, stress, academic performance, and satisfaction with life. Comput. Hum. Behav. 2016, 57, 321–325. [Google Scholar] [CrossRef]
- Garrido, E.C.; Delgado, S.C. Phubbing. Conectados a la red y desconectados de la realidad. Un análisis en relación al bienestar psicológico. Pixel-Bit Rev. Medios y Educ. 2017, 50, 173–185. [Google Scholar] [CrossRef]
- Hawi, N.S.; Samaha, M. The Relations among Social Media Addiction, Self-Esteem, and Life Satisfaction in University Students. Soc. Sci. Comput. Rev. 2017, 35, 576–586. [Google Scholar] [CrossRef]
- Duradoni, M.; Innocenti, F.; Guazzini, A. Well-Being and Social Media: A Systematic Review of Bergen Addiction Scales. Future Internet 2020, 12, 24. [Google Scholar] [CrossRef]
- de Vries, D.A.; Kühne, R. Facebook and self-perception: Individual susceptibility to negative social comparison on Facebook. Pers. Individ. Differ. 2015, 86, 217–221. [Google Scholar] [CrossRef]
- Fernández-Montalvo, J.; Peñalva-Vélez, M.A.; Irazabal, I. Internet Use Habits and Risk Behaviours in Preadolescence. Comunicar 2015, 22, 113–121. [Google Scholar] [CrossRef]
- Tzavela, E.C.; Karakitsou, C.; Dreier, M.; Mavromati, F.; Wölfling, K.; Halapi, E.; Macarie, G.; Wójcik, S.; Veldhuis, L.; Tsitsika, A.K. Processes discriminating adaptive and maladaptive Internet use among European adolescents highly engaged online. J. Adolesc. 2015, 40, 34–47. [Google Scholar] [CrossRef] [PubMed]
- Seo, M.; Kim, J.-H.; David, P. Always Connected or Always Distracted? ADHD Symptoms and Social Assurance Explain Problematic Use of Mobile Phone and Multicommunicating. J. Comput. Commun. 2015, 20, 667–681. [Google Scholar] [CrossRef]
- Jiménez López, L.M.; Valencia Cruz, A.; Sánchez Aragón, R. Escala de Ansiedad Social para Adolescentes: Confiabilidad y validez en una muestra mexicana. Psicol. Iberoam. 2013, 21, 72–84. [Google Scholar]
- Russell, D.; Peplau, L.A.; Cutrona, C.E. The revised UCLA Loneliness Scale: Concurrent and discriminant validity evidence. J. Pers. Soc. Psychol. 1980, 39, 472–480. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Marsh, H.W. Positive and negative global self-esteem: A substantively meaningful distinction or artifactors? J. Pers. Soc. Psychol. 1996, 70, 810–819. [Google Scholar] [CrossRef]
- Tehseen, S.; Ramayah, T.; Sajilan, S. Testing and Controlling for Common Method Variance: A Review of Available Methods. J. Manag. Sci. 2017, 4, 142–168. [Google Scholar] [CrossRef]
- Cabrera-Nguyen, P. Author Guidelines for Reporting Scale Development and Validation Results in the Journal of the Society for Social Work and Research. J. Soc. Social. Work Res. 2010, 1, 99–103. [Google Scholar] [CrossRef]
- Williams, B.; Onsman, A.; Brown, T. Exploratory factor analysis: A five-step guide for novices. Australas J. Paramed. 2010, 8, 1–13. [Google Scholar] [CrossRef]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the fit of structural equation models: Tests of significance and descriptive goodness-of-fit measures. Methods Psychol. Res. Online 2003, 8, 23–74. [Google Scholar]
- Chang, M.K.; Man Law, S.P. Factor structure for Young’s Internet Addiction Test: A confirmatory study. Comput. Hum. Behav. 2008, 24, 2597–2619. [Google Scholar] [CrossRef]
- Charlton, J.P.; Danforth, I.D.W. Distinguishing addiction and high engagement in the context of online game playing. Comput. Hum. Behav. 2007, 23, 1531–1548. [Google Scholar] [CrossRef]
- Lemos, I.L.; Cardoso, A.; Sougey, E.B. Validity and reliability assessment of the Brazilian version of the game addiction scale (GAS). Compr. Psychiatry 2016, 67, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Peris, M.; Maganto, C.; Garaigordobil, M. Escala de riesgo de adicción-adolescente a las redes sociales e Internet: Fiabilidad y validez (ERA-RSI). Rev. Psicol Clínica con Niños y Adolesc. 2018, 5, 30–36. [Google Scholar] [CrossRef]
- Sarabia, I.; Estévez, A. Sexualized behaviors on Facebook. Comput. Hum. Behav. 2016, 61, 219–226. [Google Scholar] [CrossRef]
- Caplan, S.E. Preference for Online Social Interaction. Commun. Res. 2003, 30, 625–648. [Google Scholar] [CrossRef]
- Zhang, Y.; Mei, S.; Li, L.; Chai, J.; Li, J.; Du, H. The Relationship between Impulsivity and Internet Addiction in Chinese College Students: A Moderated Mediation Analysis of Meaning in Life and Self-Esteem. Weinstein, A.M.; ed. PLoS ONE 2015, 10, e0131597. [Google Scholar] [CrossRef]
- van den Eijnden, R.J.J.M.; Lemmens, J.S.; Valkenburg, P.M. The Social Media Disorder Scale. Comput. Hum. Behav. 2016, 61, 478–487. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Items | Highest Loading for Each One of the Five Factors | ||||
|---|---|---|---|---|---|
| F1 | F2 | F3 | F4 | F5 | |
| SNAdd 1 | 0.642 | ||||
| SNAdd 2 | 0.633 | ||||
| SNAdd 3 | 0.662 | ||||
| SNAdd 4 | 0.531 | ||||
| SNAdd 5 | 0.638 | ||||
| SNAdd 6 | 0.548 | ||||
| SNAdd 7 | 0.863 | ||||
| SNAdd 8 | 0.882 | ||||
| SNAdd 9 | 0.864 | ||||
| SNAdd 10 | 0.409 | ||||
| SNAdd 11 | 0.815 | ||||
| SNAdd 12 | 0.865 | ||||
| SNAdd 13 | 0.760 | ||||
| SNAdd 14 | 0.803 | ||||
| SNAdd 15 | 0.662 | ||||
| SNAdd 16 | 0.808 | ||||
| SNAdd 17 | 0.754 | ||||
| SNAdd 18 | 0.669 | ||||
| Scale reliability estimates | |||||
| Cronbach’s Alpha values | 0.81 | 0.89 | 0.80 | 0.80 | 0.78 |
| Percentage of explained variance | 14.77 | 14.42 | 13.61 | 13.46 | 12.74 |
| Items | Highest Loading for Each One of the Six Factors | |||||
|---|---|---|---|---|---|---|
| F1 | F2 | F3 | F4 | F5 | F6 | |
| SNAdd 1 | 0.659 | |||||
| SNAdd 2 | 0.694 | |||||
| SNAdd 3 | 0.732 | |||||
| SNAdd 4 | 0.667 | |||||
| SNAdd 5 | 0.634 | |||||
| SNAdd 6 | 0.629 | |||||
| SNAdd 7 | 0.865 | |||||
| SNAdd 8 | 0.883 | |||||
| SNAdd 9 | 0.862 | |||||
| SNAdd 10 | 0.400 | |||||
| SNAdd 11 | 0.806 | |||||
| SNAdd 12 | 0.859 | |||||
| SNAdd 13 | 0.779 | |||||
| SNAdd 14 | 0.829 | |||||
| SNAdd 15 | 0.472 | |||||
| SNAdd 16 | 0.797 | |||||
| SNAdd 17 | 0.801 | |||||
| SNAdd 18 | 0.668 | |||||
| Scale reliability estimates | ||||||
| Cronbach’s Alpha values | 0.89 | 0.80 | 0.80 | 0.78 | 0.75 | 0.70 |
| Percentage of explained variance | 14.36 | 12.87 | 12.25 | 12.11 | 11.25 | 10.52 |
| SN Abuse | Loneliness | Social Anxiety | Life Satisfaction | Self-Esteem | |
|---|---|---|---|---|---|
| SNAddS-6S | 0.54 *** | 0.28 *** | 0.31 *** | −0.27 *** | −0.35 *** |
| Time-management higher-order factor | 0.49 *** | 0.16 *** | 0.20 *** | −0.13 *** | −0.21 *** |
| Salience sub-factor | 0.48 *** | 0.10 *** | 0.16 *** | −0.11 *** | −0.18 *** |
| Tolerance sub-factor | 0.40 *** | 0.18 *** | 0.20 *** | −0.12 *** | −0.19 *** |
| Mood modification factor | 0.42 *** | 0.32 *** | 0.34 *** | −0.34 *** | −0.40 *** |
| Relapse factor | 0.33 *** | 0.24 *** | 0.22 *** | −0.17 *** | −0.24 *** |
| Withdrawal factor | 0.41 *** | 0.16 *** | 0.23 *** | −0.19 *** | −0.26 *** |
| Conflict factor | 0.41 *** | 0.22 *** | 0.22 *** | −0.25 *** | −0.28 *** |
| Six-items Short SNAddS-6S | 0.50 *** | 0.28 *** | 0.30 *** | −0.27 *** | −0.36 *** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuadrado, E.; Rojas, R.; Tabernero, C. Development and Validation of the Social Network Addiction Scale (SNAddS-6S). Eur. J. Investig. Health Psychol. Educ. 2020, 10, 763-778. https://doi.org/10.3390/ejihpe10030056
Cuadrado E, Rojas R, Tabernero C. Development and Validation of the Social Network Addiction Scale (SNAddS-6S). European Journal of Investigation in Health, Psychology and Education. 2020; 10(3):763-778. https://doi.org/10.3390/ejihpe10030056
Chicago/Turabian StyleCuadrado, Esther, Rocío Rojas, and Carmen Tabernero. 2020. "Development and Validation of the Social Network Addiction Scale (SNAddS-6S)" European Journal of Investigation in Health, Psychology and Education 10, no. 3: 763-778. https://doi.org/10.3390/ejihpe10030056
APA StyleCuadrado, E., Rojas, R., & Tabernero, C. (2020). Development and Validation of the Social Network Addiction Scale (SNAddS-6S). European Journal of Investigation in Health, Psychology and Education, 10(3), 763-778. https://doi.org/10.3390/ejihpe10030056