Abstract
Background: The integration of the Internet of Things (IoT) into healthcare promises significant advancements in patient care and operational efficiency, while simultaneously posing substantial cybersecurity threats to sensitive personal data. Methods: This paper employs a systematic literature review (SLR) to investigate the factors influencing IoT adoption in healthcare, clarify research trends, and examine the impact of cybersecurity. Eligibility criteria were established, focusing on peer-reviewed studies published between 2015 and 2025 across five reputable databases, ultimately identifying 79 relevant articles. Results: Analysis revealed active research in countries such as India, Saudi Arabia, the USA, China, Malaysia, and Pakistan, with notable publication peaks in 2019 and 2022. Most studies (60.8%) employed quantitative methods, reflecting a preference for statistical analysis, while personal IoT health devices—particularly wearables and smart home technologies—were prominent, referenced in 27.8% of the literature. The technology acceptance model (TAM) and its variants emerged as dominant frameworks, underscoring a focus on user acceptance. A total of 139 indicators influencing IoT adoption were categorized into individual, technological, security, environmental, and ‘other’ factors. Despite the rigorous search process, some relevant studies may have been overlooked, indicating a limitation in the review. Conclusions: Addressing these gaps is vital for enhancing security measures in IoT applications, contributing to data protection and ensuring continuity of care in an increasingly interconnected healthcare ecosystem. This synthesis of current research underscores the necessity for ongoing exploration of IoT’s implications for both patient care and cybersecurity in healthcare settings.
1. Introduction
Advancements in information technology (IT) continue to enhance service delivery across various sectors. One of the most critical sectors is healthcare which is both vital and continually evolving. The sector’s critical nature can also be attributed to the expansion of precision medicine and the urgent necessity for individuals to be aware of their medical problems in real time [1]. These advancements are resulting in today’s smart objects that are being introduced in an era of apps and devices based on the Internet of Things (IoT). The concept of integrating sensors and intelligence into objects was discussed during the 1980s and 1990s [2]. In 1999, British technology pioneer Kevin Ashton coined the term “Internet of Things” (IoT), which he developed while working at the Massachusetts Institute of Technology (MIT) [3]. Even though the phrase ‘Internet of Things (IoT)’ is extensively used, its meaning remains unclear [4]. In a study by Chebudie et al., it is defined as “a network that connects uniquely identifiable ‘Things’ to the Internet” [5]. The IoT has many uses globally, including in the environmental, transportation, agriculture, industry, infrastructure, and healthcare sectors [6]. With the IoT’s ability to facilitate connectivity between everyday objects and the internet, in healthcare, this can allow monitoring and tracking of patients’ health metrics [7], as well as adopting and integrating smart technology in healthcare, ranging from vital signs devices to managerial procedures. Furthermore, the IoT market is projected to reach USD 94.2 billion by 2026, with a compound annual growth rate (CAGR) of 28.9%, surpassing the moderate growth rate of the medical device market of 5.5% between 2022 and 2026 [8]. Nevertheless, a major concern is gaining an understanding of how individuals perceive IoT products and applications and how to facilitate the adoption of these products and applications [2].
A crucial element to encourage adoption is to explore how market dynamics and regulatory frameworks influence both innovation in medical equipment and the readiness of companies to adopt IoT technologies. Recognizing these interconnections can elucidate how collaborative actions within innovation networks improve the effectiveness and efficiency of IoT applications in enhancing patient outcomes [9].
Another important effect is the involvement of multi-doctors which positively impacts patient adherence to medical instructions. Leader participation and disciplinary variety enhance the positive correlation between multi-doctor involvement and patient adoption [10].
Finally, an important aspect of supporting the adoption of any new technology is security. Security in the context of healthcare is crucial, as the sector is increasingly pushed to adopt advanced technologies through IoT devices. The sensitive nature of patient data necessitates extreme precautions to maintain its confidentiality. Moreover, security in IoT devices is seen as a significant concern as data may be readily compromised by attackers or hackers [11]. The complexity of healthcare systems, characterized by numerous data sources and endpoints, poses distinct obstacles to the implementation of efficient cybersecurity measures [12]. Primary points of focus comprise the safeguarding of electronic health records, assurance of data integrity and confidentiality, and protection of patient privacy. Many techniques have been employed to enhance the security of IoT devices, for example, the radio-frequency identification (RFID) encryption technique [13] and a biometric-based security system [14]. Machine learning (ML) and public security-focused datasets are also being investigated to improve healthcare cybersecurity [15]. In the privacy context, healthcare deals primarily with personal data which governs its management and storage approaches using privacy-preserving techniques. The United States (USA) and the European Union (EU) have established the Healthcare Insurance Portability and Accountability Act 1996 (HIPAA) [16] and the General Data Protection Regulation (GDPR) [17], respectively.
Furthermore, healthcare has an additional feature that increases the challenge of exceeding the current demands for privacy, namely, patient safety [15]. This issue is becoming significant owing to specific attacks on implantable and wearable medical devices (IWMDs) (insulin pumps, health trackers, etc.), which can lead to unfavorable effects. Despite these considerable efforts, security and privacy concerns in the Internet of Things (IoT) remain inadequately addressed.
To better justify the necessity of this review at this time, recent cybersecurity incidents reveal how the COVID-19 pandemic significantly expedited the growth of IoT and elevated cybersecurity risks in healthcare, with an enormous spike in hacks during this time. This study [18] concludes that cyberattacks on healthcare sectors increased by two to three times during the initial wave of the pandemic compared to 2019. Moreover, ref. [19] saw an “exponential growth of Internet of Things (IoT) devices” that significantly expanded the risk landscape for possible attacks in the healthcare sector. Consequently, this paper aims to conduct a systematic literature review (SLR) to compile and analyze the factors influencing the adoption of IoT in the healthcare sector. However, this study expands on these by introducing research gaps in three aspects, thereby contributing to the enrichment of both medical and information technology fields.
This research paper is structured as follows.
Section 2 presents the literature on the previous empirical studies. Section 3 explains the research methodology. Section 4 discusses the results obtained by categorizing the findings into six categories. Section 5 details the gaps and future agenda. Finally, the contributions and conclusions are outlined in Section 6 and Section 7.
2. Literature Review
Previous Empirical Studies
Several studies have been conducted to discover the factors that affect IoT adoption in the healthcare sector. Our study’s systematic literature review (SLR) has narrowed down these studies to the five top-rated articles based on their high index score and being published in well-known journals.
One of the earliest studies, performed by [20], covered 146 articles and identified five approaches: sensor-based, resource-based, communication-based, application-based, and security-based. Each approach was evaluated and compared. In a later study, the researchers in [21] analyzed more than 106 papers, categorizing the challenges of IoT adoption into three classes: system, users, and other challenges. Similarly, the authors in [22] identified 90 factors from 22 articles categorized into five main areas. These areas were individual (16 factors); technology (19 factors); security (7 factors); health (9 factors); and environment (7 factors); this total of 90 factors included a subset of factors for each area that could be either barriers to, or facilitators of, this technology. In the fourth paper [23], the authors conducted a meta-analysis, resulting in the IoT applications in healthcare being categorized into monitoring, locating, and personalized medicine systems, each with many studies and inventions over the years. Finally, an SLR based on 10 articles was performed by [8] to discuss various theories on technology adoption, focusing on socio-technical theory. The study found 94 factors influencing IoT adoption in healthcare that could be classified into 24 themes. The results and limitations of these past studies on IoT adoption in healthcare are presented in Table 1.

Table 1.
Results and limitations of past studies on IoT adoption in healthcare.
3. Methodology
This study took a systematic literature review (SLR) approach, following the Okoli and Schabram protocol [24], with four phases: planning, selection, extraction, and execution. The SLR, focused on IoT adoption in the healthcare sector, was employed to identify, evaluate, and interpret all the literature applicable to the research questions [25]. Systematic literature reviews (SLRs) are essential for implementing evidence-based techniques across many fields, including IT, healthcare, and social sciences. They generally seek to address multiple goals: establishing a theoretical foundation for future study; obtaining knowledge of the extensive research on a subject of interest; or addressing practical inquiries by gaining an understanding of the insights provided by current research on the issue [24]. Their main advantage is that, instead of serving as a foundation for the researcher’s personal goal, they establish a robust starting point for all academic community scholars engaged in a certain field. Systematic literature reviews (SLRs) are especially helpful for meta-analytic studies that collect and synthesize information from prior investigations [26]. The SLR approach provides opportunities to minimize bias and increase clarity via a framework of guidelines and validation processes [27]. This study adheres to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, ensuring transparency and completeness in reporting the methodology and findings of our systematic review. This study was registered on PROSPERO (CRD420251234879) on 19 November 2025.
3.1. Planning Phase
The planning phase involved the identification of the study questions and objectives. These were developed to enhance the research: recognizing and classifying the existing research literature from several sources to investigate factors and theories, either quantitatively or qualitatively, in the adoption of IoT within the healthcare context. Continually, the first phase was adapted to identify the relevant literature, guided by the following objectives:
- -
- To explore the factors affecting the implementation of IoT;
- -
- To clarify academic research trends in the field of IoT in healthcare;
- -
- To understand the role of cybersecurity and its impact on IoT within healthcare.
In light of that, the following research questions (RQs) were formulated:
Q1: What are the key factors that influence the adoption of IoT technologies in healthcare settings?
Q2: What are the main frameworks, models used?
Q3: What role do cybersecurity concerns play in the adoption of IoT technologies in healthcare?
Moreover, for this systematic literature review, papers were gathered from the following five digital databases: Emerald, ScienceDirect, Institute of Electrical and Electronics Engineers (IEEE), Springer, and Taylor & Francis, focusing on articles on IoT acceptance among healthcare workers and patients.
Furthermore, studies were chosen from the databases utilizing the given keyword combinations string: (healthcare <OR> e-Health) [AND] (IoT <OR> “Internet of Things”) (adoption <OR> implementation) (“factors”).
3.2. Selection Phase
Table 2 shows the eligibility criteria employed for study selection in the systematic literature review (SLR). The inclusion criteria specify that studies must focus on factors influencing the adoption of the Internet of Things (IoT) in healthcare; be published in peer-reviewed journals with a high impact factor; be written in English; be available as a full text; and be published within the study’s time frame of 2015–2025. Conversely, the exclusion criteria stipulate the removal from the selection of books, book chapters, and newspapers; studies in languages other than English; those not available as full text; and those published before 2015. These criteria ensure that the selected studies are relevant, of high quality, and contemporary to the research question.
Table 2.
Eligibility criteria for study selection in the systematic literature review.
Kitchenham and Charters [28] emphasized the significance of quality assessment in the selection of studies, also delineating criteria for estimating the relevance and rigor of research publications. Moreover, many suggestions and measurements have been proposed in various studies to enhance the efficacy of quality assessments [29]. Consequently, in addition to the previously established inclusion and exclusion criteria, this study evaluated the quality of individual articles using additional criteria. Selections, especially for conference papers, were made from well-respected conferences that often utilized a rigorous peer-review procedure to ensure elevated quality standards.
3.3. Extraction Phase (PRISMA Flow Diagram)
A PRISMA [preferred reporting items for systematic reviews and meta-analyses] flow diagram was used to illustrate the systematic process of the study selection for the review. Initially, 3002 records were identified through database searches. After removing duplicates (n = 2033) and records with restricted access (n = 254), 715 records underwent screening. Following the screening phase, 400 records were excluded due to being in a non-English language, leaving 315 reports to be sought for retrieval. Of these, 110 reports could not be retrieved, and 205 reports were assessed for eligibility. Finally, a total of 79 studies met the inclusion criteria and were included in the review. The exclusion criteria at the eligibility assessment stage included reasons based on the title (n = 26), abstract (n = 64), and the journal’s index (n = 36). Figure 1 presents the flow diagram [30] which provides a transparent and reproducible overview of the study selection process.
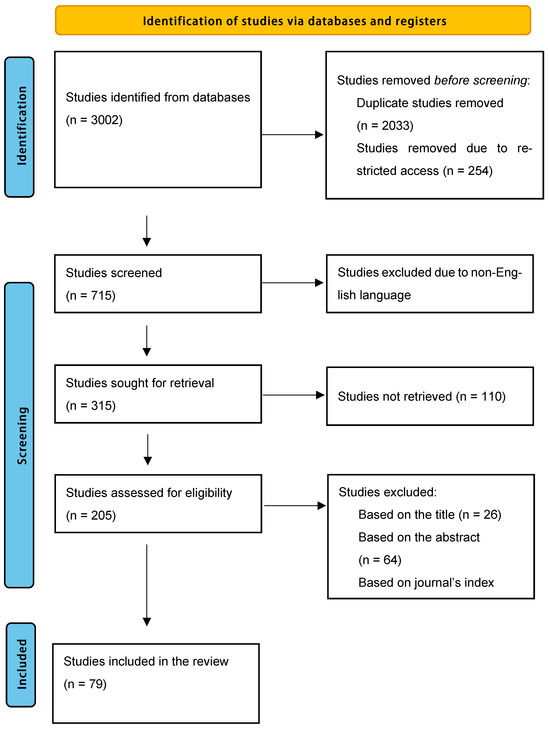
Figure 1.
Identification of studies via databases and registers.
3.4. Execution Phase (Results)
In the execution phase, Excel spreadsheets were utilized to filter the results by summarizing the data in a form that described the researchers’ key findings. The summarized data on the form were further analyzed and translated into charts to illustrate research ratios based on the theories being used, countries where studies took place, the year of publication, research design, technologies used, and, finally, the factors influencing IoT adoption in health sectors. We sought data on factors related to IoT adoption in healthcare. For each outcome, we aimed to collect all relevant measures reported across the studies, including both qualitative and quantitative analyses. However, we prioritized studies that were open-source and available.
4. Findings/Results
In this chapter, results derived from the reviewed literature will be detailed, focusing on six key attributes:
First, we will focus on countries where studies took place, with an analysis of the geographical distribution of research studies, highlighting the countries involved. Also, we recorded the year of publication to provide a chronological overview of when the studies were published, illustrating trends and developments in the field over time. Moreover, we assessed the research designs, creating a description of the various research methodologies employed in the studies and categorizing them into qualitative, quantitative, and mixed methods. We also analyzed the technologies used through an examination of the different technologies utilized in the studies, showcasing how they contributed to research outcomes. Moving on to the theories used, we performed a review of the theoretical frameworks that underpin the studies explaining how these theories informed the research. Lastly, to assess factors influencing IoT adoption in healthcare sectors, we performed an exploration of the key factors that impact the adoption of Internet of Things (IoT) technologies in healthcare
Each attribute will be accompanied by detailed diagrams and tables to provide a clear and comprehensive understanding of the findings.
4.1. Countries Where Studies Took Place
The healthcare sector is a dynamic domain that may captivate the interest of many researchers. Hence, the literature shows diverse countries in which research has examined their intended use of sophisticated technologies, such as the Internet of Things (IoT).
Notably, countries like India, Saudi Arabia (Kingdom of Saudi Arabia [KSA]), the United States (USA), China, Malaysia, and Pakistan have a higher number of studies, indicating active research efforts in these regions. In contrast, several other countries have fewer studies, while a significant number of studies have not mentioned the study region, possibly suggesting gaps in geographic representation. In Table 3, each row represents the number of studies from specific countries. The visualization in Figure 2 highlights the global landscape of research on IoT adoption in healthcare.
Table 3.
Number of studies per country.
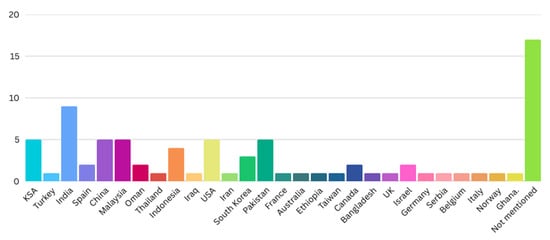
Figure 2.
Global landscape of research on IoT adoption in healthcare.
4.2. Year of Publication
Figure 3 illustrates the distribution of publications selected for the SLR across various years. Each segment of the pie chart represents the proportion of total publications from specific years, highlighting trends in research output over time. Notably, the years 2022 and 2019 each contributed 15% of the selected publications, while 2023 accounted for 13.8%. Other years, such as 2018 and 2017, showed slightly lower percentages, at 11.3% and 10%, respectively. The visualization in Figure 3 and Table 4 helps to identify the years with the highest research activity relevant to the factors influencing the intention to adopt IoT in the healthcare sector.
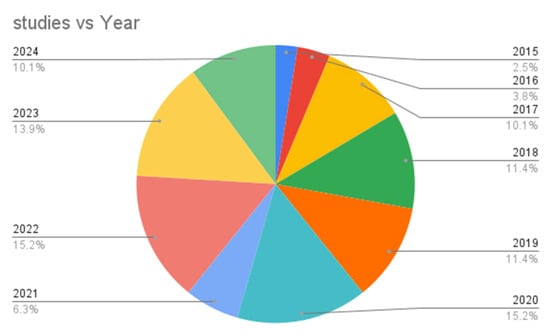
Figure 3.
Distribution of selected publications across various years.
Table 4.
Number of studies per year.
4.3. Research Design
Figure 4 depicts the research designs employed by the reviewed studies on IoT acceptance in the healthcare sector. The pie chart shows that most studies (60.8%) utilized quantitative research methods, indicating a preference for numerical data and statistical analysis. Qualitative methods were used in 12.7% of the studies, while mixed methods accounted for 8.9%. Additionally, 17.7% of the studies did not specify their research design. The visualization in Figure 4 highlights the dominant use of quantitative approaches in examining IoT acceptance in healthcare (Table 5).
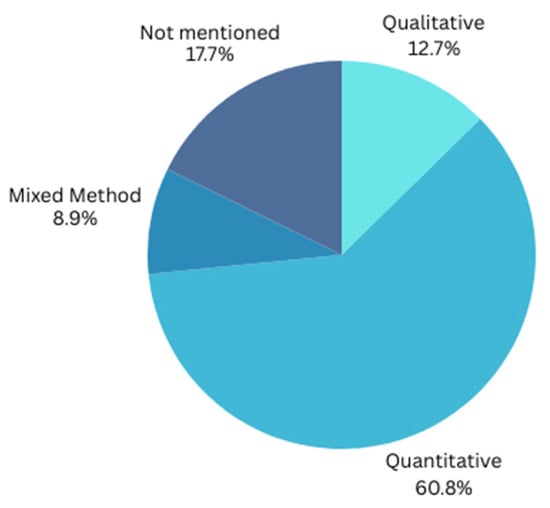
Figure 4.
Research designs in reviewed studies on IoT acceptance in healthcare sector.
Table 5.
Number of studies per research design.
4.4. Technologies Used
Table 6 presents the various technologies integrated with the Internet of Things (IoT) as discussed in the reviewed papers on measuring IoT acceptance in the healthcare sector. Each row represents the number of studies that feature specific technologies. Personal IoT health devices, particularly “wearables,” are the most commonly referenced (27.8%), indicating significant interest in this area, followed by smart homes (7.6%). Other technologies, such as mobile health services (6.3%), e-health management systems (3.8%), and care delivery devices for older adults (2.5%), also appear but with fewer mentions. Most studies (31.6%) did not specify the technology used. The visualization in Figure 5 highlights the diverse technological landscape of IoT acceptance research in healthcare, emphasizing the prominence of wearable devices.
Table 6.
Technologies used in selected studies.
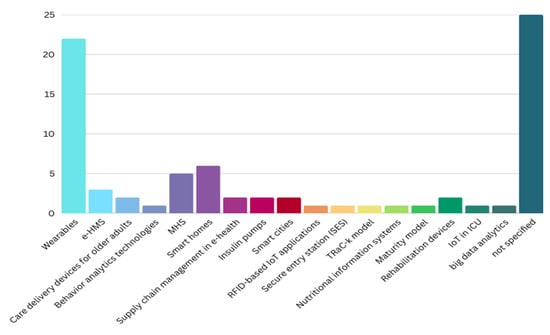
Figure 5.
Technologies integrated with the Internet of Things (IoT).
4.5. Theories Used
Over the years, several theories have been utilized to investigate the influencing factors affecting IoT adoption in healthcare, with a total of 28 theories or/frameworks noted during the review. Identical or derived theories were then unified.
Table 7 presents a comprehensive overview of the various theoretical frameworks identified in the literature, along with the corresponding frequency of studies employing each theory. This quantitative representation serves to highlight the prevalence and relevance of specific theories within the field of technology acceptance. Each row in Figure 6 represents the frequency of studies employing specific theoretical frameworks. The technology acceptance model (TAM) and its variants dominate the research landscape, indicating a strong focus on understanding user acceptance. Other theories, such as the unified theory of acceptance and use of technology (UTAUT), the theory of planned behavior (TPB), innovation diffusion theory (IDT), and the health belief model (HBM), are also represented, although to a lesser extent. The visualization in Figure 6 highlights the predominant theoretical approaches in current research on IoT adoption in healthcare.
Table 7.
Theories used in selected studies.
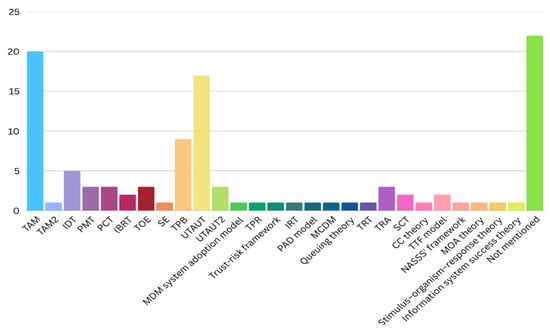
Figure 6.
Predominant theoretical approaches in current research on IoT adoption in healthcare.
4.6. Factors Influencing IoT Adoption in Healthcare Sectors
Upon reviewing the current research, 139 indicators that may or may not influence IoT adoption were identified; the same or duplicate meanings were next eliminated or unified through analysis of the studies. In collecting the factors, we focused on limiting our attention to the presence, or absence, of an indicator’s impact, clarifying the main factors influencing the process of IoT adoption, ultimately explaining the lack of factors, or defective factors, in the field. The indicators were subsequently categorized by classifying and analyzing the factors that influence IoT adoption into individual, technological, security, environmental, and ‘other’ categories to fulfill the study’s objectives. We have relied on established frameworks and categorizations from the prior literature to ensure consistency and comparability. This study aimed to address knowledge gaps by focusing on cybersecurity, IoT, and the healthcare sector dynamics. A brief description of each category is provided below to clarify what they mean. For a comprehensive list of all identified factors, please refer to Appendix A.
4.6.1. Individual Factors
Individual factors refer to the personal characteristics and preferences of patients and healthcare providers, for example, attitudes, with [36] highlighting the significant influence of attitudes on the adoption of IoT healthcare products. By providing a real-life example, the ability to use monitoring devices was determined, meaning that more patients were monitored with fewer checkups. When [46] developed mobile phone-based diabetes monitoring (MDM) technology, they discussed how to ensure the physician’s impact on health improvement through MDM adoption. This revealed health improvement effects, with net benefits ultimately affecting the intention to use MDM technology. In contrast, ref. [31] revealed that attitudes did not directly or indirectly impact behavioral intention. The study by [72] found that preserved health risk, represented by perceived susceptibility, was frequently a non-significant determinant in the context of the same IoT-based device.
4.6.2. Technological Factors
The technological aspects of IoT devices were investigated by [63] in their study, which sought to determine the significance of perceived usefulness (PU) in influencing individuals’ intention to continuously use IoT wearable devices. They emphasized the need for a comprehensive understanding of perceived usefulness (PU) to enhance usage and development of these devices. At the same time, ref. [77] observed that perceived usefulness (PU) had an impact on trust, as well as slightly affecting individuals’ intention to use medical IoT wearable devices. Furthermore, the authors of [38] stressed that the benefits of IoT applications would only accrue positively if the adoption was by institutions as well as consumers: they declared a significant direct effect of facilitating conditions on behavioral intention. In the context of designing a smart IoT home, ref. [40] revealed that facilitating conditions had a non-significant effect.
4.6.3. Security Factors
Security factors refer to the measures taken to protect sensitive health data from breaches and unauthorized access, with [71] addressing this as confidentiality concerns. These authors aimed to identify factors that created obstacles to IoT adoption in the healthcare sector. They found that the security and privacy of data were the most influential factors in identifying medical Internet of Things (MIoT) challenges, although [32] did not classify this as a core factor.
Another important factor was the presence of clear objectives and plans for MIoT systems: in [33], the authors believed that the deployment of MIoT systems could be efficiently supported by clear goals and precisely outlined strategies. In contrast, ref. [75] classified government regulation as a positive factor but found that it was not statistically significant.
Moreover, previous studies [108] revealed that perceived severity and vulnerability originating from the protection motivation theory (PMT) pose higher health risks and have positively influenced the intention of medical professionals in adopting IoT.
Furthermore, according to theories like Social Exchange Theory (SET), studies suggest that concerns over weak authentication mechanisms can lead to a perceived lack of trust in IoT devices [52]. This perception negatively impacts performance expectancy and trust.
Finally, the vulnerability of unencrypted data could raise concerns regarding data breaches and privacy breaches. This issue impacts the perceived risk factor, which, as per the Technology Acceptance Model (TAM), can substantially change consumers’ attitudes towards the technology. If users see their data as insecure, their willingness to use IoT solutions reduces [39].
4.6.4. Environmental Factors
Environmental factors refer to the external conditions that IoT technology can provide, such as [79] providing evidence of the positive influence of performance expectancy (PE) on behavior towards wearable devices, from the consumer perspective. Additionally, ref. [89] illustrated that performance expectancy (PE) was a core factor, especially in healthcare professionals’ adoption of IoT and big data analytics (BDA) technologies.
On the other hand, the social influence (SI) factor tended to be a controversial point in [2], in which its significant effect on behavioral intention was demonstrated based on a techno-psychological point of view. Moreover, ref. [78] concluded that social influence (SI) did not significantly influence the intention of diabetic patients to use wearable health devices that were IoT-reliant.
4.6.5. Other Factors
Factors that did not fit the above categories could fit previously defined categories, such as operational efficiency, customer satisfaction, or product quality, like cost. Cost factors, by their nature, pertained to financial implications in the study by [102], which explored technologies that analyzed behaviors associated with dementia. They revealed the necessity for a cost-effective approach to efficiently collect data, while [81] categorized preserved value as a low-impact factor.
In another context, in [40], the effects of effort expectancy (EE) on smart homes were found to be greater than those of the other evaluated factors. However, ref. [52] found that EE represented an unimportant factor.
5. Gaps and Future Agenda
It is essential to understand the current state of research on IoT technology applications in healthcare, as measured by systematic review and bibliometric analysis, and to address the gaps, as this allows for the optimal use and enhancement of these applications and enriches future studies.
5.1. IoT in the Healthcare Sector
The healthcare sector is a fertile field for creativity and technological invention, making it highly suitable for IoT technology due to its connectivity ability and unlimited applications [37]. Nevertheless, the adoption of IoT technologies in the healthcare industry is progressing at a slow rate. Many reasons can be found, but some researchers [2] attributed it to prior research being primarily focused on enterprise IoT design and usage, neglecting individual perspectives and concerns. Others [86] have noted that numerous studies have provided significant insights into the adoption of IoT-based healthcare technology by employees and patients; nevertheless, the perspectives of health technicians and professionals are rarely examined. Likewise, ref. [109] indicated that challenges, such as security, privacy, standardization, and low-power operations, need to be addressed for widespread adoption. Moreover, ref. [67] indicated that most studies focus on quantitative testing of technology acceptance models; however, qualitative exploratory studies are essential to understand the reasons for and against IoT adoption and use in the healthcare sector.
Finally, the existing research has paid little attention to moderation and mediation analyses, even though these are essential for understanding how different factors influence IoT adoption outcomes. Furthermore, many studies have not examined the relationships between these factors, limiting our understanding of how they interact and affect one another.
5.2. Factors
After considering the final analysis results of the literature review, it is evident that individual factors (33.1%) represent the largest segment, as shown in Figure 7, signifying that personal behaviors, preferences, and adoption rates have been the primary focus of previous studies. This indicates that user involvement and user acceptability are crucial for the effective adoption of IoT technology. Technological factors (24.5%) constitute the second most significant effect, highlighting the importance of the assessment of technological advances, including hardware and software improvements, in either promoting or obstructing IoT implementation. Environmental factors encompass 14.4%, indicating the need to evaluate the impact of external conditions, such as societal attitudes, on IoT adoption or disruption. Factors not classified into any category constitute 19.4%, signifying that additional relevant variables may influence IoT adoption or disruption, indicating a diverse range of difficulties and opportunities in the field of research. Finally, security factors represent only 8.6%, despite the need for strong cybersecurity measures to address concerns related to data protection and privacy. Details of these factors are further discussed in the next section.
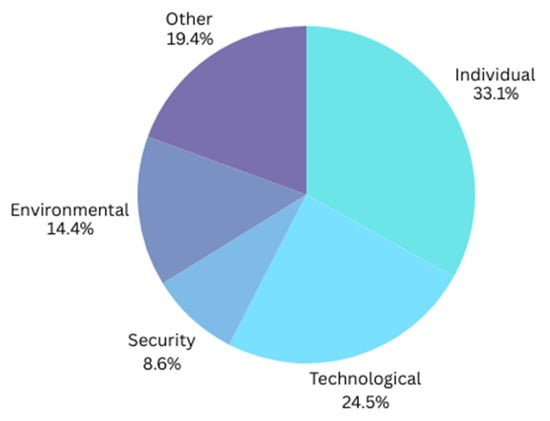
Figure 7.
Research gaps per factor.
As shown in Figure 8a, attitude (12.4%) is the most extensively examined individual factor, underscoring the significance of user motivation and perception in facilitating IoT adoption. Conversely, aspects such as a willingness to learn, desire, and intrinsic motivation are among the least examined, suggesting a research gap that could be explored to improve user experiences and promote broader acceptance of IoT technology in healthcare.
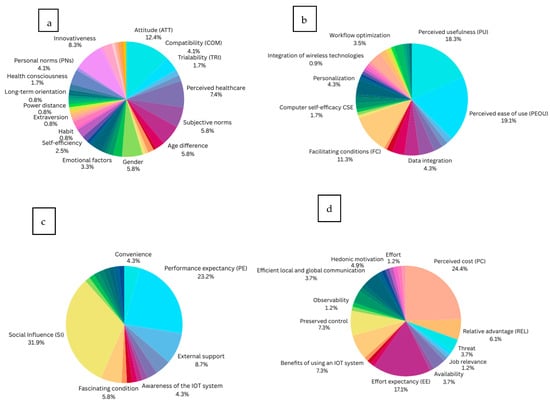
Figure 8.
Individual factors influencing IoT adoption within the healthcare industry: (a) individual factors; (b) technological factors; (c) environmental factors; and (d) ‘other’ factors.
As shown in Figure 8b, we can conclude that the most studied technological factor—perceived ease of use (PEOU) with 19.1%—can be justified as research has generally been concerned with how intuitive interfaces, training, and support may improve PEOU, thereby promoting increased adoption and use of IoT technologies. In contrast, the least studied factor is personalization (at 0.9%), indicating less of a research focus on the influence of personalization on adoption rates. Nonetheless, customization is widely acknowledged as an essential element in improving user engagement and fulfillment, especially in healthcare, where individual patient requirements might differ widely. Addressing this research gap may provide advances in IoT systems that are more adaptive, resulting in enhanced user experiences and adoption rates.
As shown in Figure 8c, social influence (SI) (31.9%) is recognized as the most extensively researched environmental factor. The high number of studies highlights the significance of social dynamics within healthcare, with research investigating how establishing a supportive group and spreading success perspectives can enhance social impact. The least studied environmental factor is physician recommendation (1.4%), which indicates a lack of understanding of the influence of trustworthy physicians’ direct referrals on IoT adoption decisions. Promoting the influence of physician recommendations could increase the reliability and credibility of IoT solutions, ultimately resulting in increased IoT adoption rates.
Additionally, as shown in Figure 8d, we can identify perceived cost (PC) (24.4%) as the most studied uncategorized ‘other’ factor, highlighting the importance of understanding how the perception of high costs can deter IoT adoption, while demonstrating that cost effectiveness can encourage adoption. In contrast, effort (1.2%) is identified as the least studied factor in this context, indicating a gap in comprehension of the effort required to implement and use IoT technologies.
Finally, as for their interaction with technological determinants, the factors shape IoT vulnerability and resilience in healthcare in different ways. For example, inadequate digital literacy among healthcare staff could delay IoT adoption, boosting susceptibility to mistakes and security breaches. On the other hand, training and education programs enhance competence, enabling staff to better utilize and secure IoT systems, thus fostering resilience [22,110]. Furthermore, a change-resistant culture or lack of digital leadership might hinder IoT integration. However, supporting leadership and an innovative culture encourages job creation and adaptation, maximizing the benefits of robust technical solutions [8,111].
5.3. Cybersecurity Aspects
As mentioned earlier, security factors represent only 8.6% of the total identified factors, even though cybersecurity continues to be a critical concern in IoT-based systems. In the healthcare industry, it is imperative that a patient’s health information is easily available to authorized individuals, including physicians and nurses; however, the patient’s confidential health information must remain private.
In this research, we identified 12 security-related factors, with the relevance of their value assessed in previous research by the frequency of mentions. Upon examining Figure 9, we find the following three top-mentioned factors. Privacy (26.2%) has the highest percentage of mentions, signifying that worries about the protection of personal information are a critical element, while trust (16.7%) underscores the importance of confidence in stakeholders. Security has the same percentage of mentions (16.7%) as trust, with these equal proportions highlighting the significance of secure techniques and systems in safeguarding sensitive information.
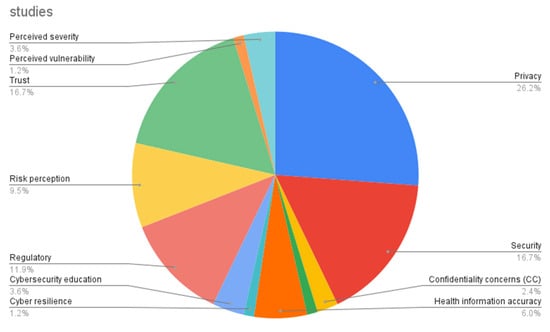
Figure 9.
Research gaps in cybersecurity aspects.
Overall, deeply focused security-related research is scarce, despite its utmost importance in supporting the process of adopting IoT technology in the health sector.
5.4. Future Recommendations
Based on the findings of the study regarding IoT adoption in healthcare, we believe that several recommendations can be made. Healthcare institutions should enhance cybersecurity measures and develop patient education programs to address misconceptions about IoT technologies while investing in user-friendly devices. Regulators need to establish clear guidelines on patient privacy and cybersecurity, promote standardization in device development, support research on barriers to IoT adoption, and monitor compliance with regulations. Technology developers should focus on user-centric design, incorporate advanced privacy protections, engage with stakeholders to ensure solutions meet actual needs, and invest in continuous innovation to adapt to emerging threats. By implementing these strategies, all parties can collaborate to overcome barriers to IoT adoption, ultimately enhancing patient care and safety in the healthcare sector.
As for future research paths, we recommend further investigation into topics such as Multimedia Streaming in Software-Defined Internet of Vehicles (SD-IoV) for healthcare, like OpenFlow or Raspberry Pi. In mobile healthcare contexts (e.g., ambulances, patient transport), dependable multimedia streaming is crucial. Future research may explore the potential of SD-IoV to facilitate real-time video consultations and data sharing between automobiles and medical facilities.
6. Contribution
This study makes several contributions to information security research and has implications for the healthcare sector. It offers an overview of current research on IoT adoption in the healthcare sector. The study seeks to make significant contributions to research, organizations, and society by addressing a critical knowledge gap in the realms of cybersecurity and IoT dynamics within the healthcare sector. By highlighting the importance of cybersecurity in healthcare sector IoT, the research aims to raise public awareness and enhance patient safety, ultimately benefiting society in its entirety. From an organizational perspective, the study’s findings will support the development of policies and strategies, enabling healthcare providers to make informed decisions about technology adoption and risk management.
From a research perspective, one of the study’s most important contributions is the examination of multiple theories and factors that influence the adoption of IoT devices, especially in the healthcare context. Additionally, the study enhances the growing body of research investigating the current state of IoT acceptance. This study is unique as it combines several aspects into a single study. It emphasizes the importance of implementing more theories, such as the fit between individuals, tasks, and technology (FITT) frameworks, which could be more comprehensive in explaining the relationship between the studied factors. Moreover, the study draws attention to the need for more deeply focused security-related research, with the findings providing guidelines for future research focused on IoT adoption within the healthcare sector.
7. Conclusions
This comprehensive literature review examines existing studies that analyze the factors influencing IoT adoption in the healthcare sector. This research is unique as it reviews 79 articles, while exploring the theories being used, countries where studies took place, year of publication, and research design.
The study highlights the significant potential of IoT adoption to enhance patient care. Nonetheless, IoT adoption is impeded by obstacles, such as cybersecurity threats, patient privacy issues, and disparate opinions of IoT technology among patients and caregivers.
The study categorizes IoT adoption in healthcare into five categories (individual, technological, security, environmental, and other). It identifies prevalent areas of IoT adoption and current trends. The research synthesizes key factors influencing IoT adoption from the existing literature, organizing them into different dimensions. The research offers insights for scholars and practitioners seeking to understand IoT adoption in healthcare contexts, providing a structured framework for analysis and future research.
The results reveal that countries like India, Saudi Arabia (KSA), the USA, China, Malaysia, and Pakistan had a higher number of studies, indicating active research efforts in these regions. Notably, the years 2022 and 2019 each contributed 15% of the selected publications, while 2023 accounted for 13.8%. Other years, such as 2018 and 2017, showed slightly lower percentages at 11.3% and 10%, respectively. Most studies (60.8%) utilized quantitative research methods, indicating a preference for numerical data and statistical analysis. Personal IoT health devices, particularly “wearables” and smart homes, were the most frequently referenced (27.8%) in prior studies. In total, 28 theories/frameworks were noted during the review. The technology acceptance model (TAM) and its variants dominated the research landscape, indicating a strong focus on understanding user acceptance. Furthermore, 139 indicators that may or may not influence IoT adoption have been identified. The indicators were subsequently categorized to fulfill this study’s objectives, with the factors classified into, and analyzed in, individual, technological, security, environmental, and ‘other’ categories. This study concludes that research gaps exist in studies on IoT adoption in the healthcare sector, in terms of factors in general and in cybersecurity aspects, in particular. The data not only provides a clearer picture of the current state of IoT adoption in healthcare but also paves the way for future research in these areas. This insight encourages researchers to explore underrepresented regions, theories, and methodologies, ultimately contributing to a more balanced and comprehensive understanding of the field.
As for future recommendations based on the past literature and in-depth investigations, we believe that to enhance IoT healthcare security, actionable solutions must concentrate on establishing standardized cybersecurity frameworks. For example, using blockchain for decentralized trust, strong authentication, and secure data transmission to ensure healthcare device and network interoperability [112,113,114], cross-border data governance models, which must address the confidentiality of data and privacy issues [115,116], and AI-driven threat prediction systems, particularly those employing explainable AI (XAI), are crucial for crisis prediction and transparent decision-making in critical healthcare settings [117].
Recommended research directions can be summarized as edge computing and how it should be incorporated to facilitate low-latency, real-time threat detection [118]; blockchain-based verification that can offer immutable audit trails; decentralized identity management, particularly when integrated with edge and fog computing for scalability [119]; and, lastly, privacy-preserving federated learning that enables collaborative model training among institutions without the exchange of raw data. These recommendations can build on the paper’s findings and contribute to the field [120].
Another important aspect is legal frameworks that must be continually assessed and included in system design, with adaptive procedures to handle evolving rules such as HIPAA, GDPR, and future AI Act frameworks [115].
Lastly, the study outlines the following limitations and offers recommendations for further research. Despite conducting a thorough manual web search to identify studies, the absence of some studies is regarded as a limitation of the study. These missing studies may enhance the study’s outcomes; hence, future research should adopt an automated search approach to maximize the collection of relevant studies. The inclusion and exclusion criteria chosen by the study may also be a limitation (e.g., including only full-text articles while excluding native paid content). Hence, addressing these concerns in future studies may be extremely valuable. Finally, the previously revealed gaps are regarded as an important path for further research.
Author Contributions
Conceptualization, R.A. and A.A.; Methodology, R.A.; Validation, R.A. and A.A.; Formal Analysis, R.A. and A.A.; Investigation, R.A.; Resources, R.A.; Writing—Original Draft Preparation, R.A.; Writing—Review and Editing, A.A.; Visualization, R.A.; Supervision, A.A.; Project Administration, R.A. and A.A. All authors have read and agreed to the published version of the manuscript.
Funding
The APC was funded by [Qassim University for financial support (QU-APC-2025)].
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available in publicly accessible databases, including the Research Information Sharing Service (RISS), CINAHL, MEDLINE, and PubMed. All data were derived from these public domain resources.
Acknowledgments
The Researchers would like to thank the Deanship of Graduate Studies and Scientific Research at Qassim University for financial support (QU-APC-2025).
Conflicts of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Appendix A
Table A1.
Factors from selected studies with extent of effect.
Table A1.
Factors from selected studies with extent of effect.
| Category | Factor | Study Result | |
|---|---|---|---|
| Significant Effect | Slim to No Effect | ||
| Individual | Attitude (ATT) | [2,32,34,37,40,44,52,57,64,65,79,82,86] | [27,35] |
| Compatibility (COM) | [35,57,64] | [31,71] | |
| Trialability (TRI) | [31,57] | ||
| Image (IMA) | [32,57] | ||
| Perceived healthcare Health values (HV) Health motivation (HM) Personal health beliefs (PHBs): Health improvement Health interests Health anxiety Healthcare vulnerability Perceived health risk (PHR) Human attachment concerns | [32,34,42,46,58,65,102] | [68,69] | |
| Subjective norms | [37,40,42,54,66,82,86] | ||
| Age difference | [28,52,72,79] | [56,74,82] | |
| Comfortability | [77] | [35,47] | |
| Trust in the organization and treatment | [93] | ||
| Traditional barrier | [35] | [49] | |
| Value of openness to change | [35] | ||
| Computer and English language self-efficacy (CESE) | [28] | ||
| Gender | [28,72,77,79] | [48,74,82] | |
| Education | [28,48] | [82] | |
| Occupation, experience | [28,82] | ||
| Technology anxiety (TA) | [36] | ||
| Awareness of disease | [88] | ||
| Emotional support: PAD (pleasure, arousal, dominance) model; emotional factors: empathy, interaction, compassion, interactivity | [54,58,59,62] | ||
| Health expectancy | [1] | ||
| Past behavior frequency | [40] | ||
| Perceived susceptibility | [86] | [68] | |
| Self-efficiency | [43,69,103] | ||
| Habit | [74] | ||
| User satisfaction | [43,100] | ||
| Conscientiousness | [56] | ||
| Agreeableness | [56] | ||
| Extraversion | [56] | ||
| Neuroticism | [56] | ||
| Collectivism | [56] | ||
| Power distance | [56] | ||
| Masculinity | [56] | ||
| Uncertainty avoidance | [56] | ||
| Long-term orientation | [56] | ||
| Positive anticipated emotion | [40] | ||
| Negative anticipated emotion | [40] | ||
| Health consciousness | [40,75] | ||
| Personal factors (e.g., activity patterns and exercise schedule), personal norms (PNs), interpersonal influence, user characteristics; user behavior (UB) | [2,46,103] | [54,65] | |
| Lack of knowledge, decreased sensory perception | [61] | ||
| Innovativeness | [27,32,43,59,62,65,66,82,90,102] | ||
| Lack of need for the technology | [61] | ||
| Technology skills | [61,76,79] | ||
| Fashionability | [66] | ||
| Willingness to learn | [61] | ||
| Limited/fixed income | [61] | ||
| Intrinsic motivation | [62] | ||
| Desire | [40] | ||
| Technological | Perceived usefulness (PU) | [2,27,32,37,43,44,45,47,54,56,57,59,61,62,64,66,69,82,86,102] | [73] |
| Perceived ease of use (PEOU), ease of learning, complexity, usage barriers, adaptability | [1,2,27,32,35,37,44,45,47,49,54,57,59,64,82,86,101,103] | [31,62,66,73] | |
| Facilitation, functionality | [33] | [73] | |
| Ubiquity (UQ), ubiquitous control | [34,35] | ||
| Overall quality (system, information, service) | [42,47,100] | ||
| Ease of data collection, data integration, data governance | [29,83,84,87,91] | ||
| Connectedness | [62,64,83] | [27,66] | |
| Unreliability | [73,87] | [39,91] | |
| Facilitated appropriation | [2,56] | ||
| Cognitive instrumental attitude | [2] | ||
| Facilitating conditions (FCs) | [1,34,45,55,62,68,72,74,75,77,85] | [36,50] | |
| Traceability | [29] | ||
| Observational learning | [81] | ||
| Utilitarian monitoring activity | [81] | ||
| Computer self-efficacy (CSE), IT-related self-efficacy | [57] | [65] | |
| Qualification of resources, quantifying resources | [49,76] | ||
| Visualization of complex workflows | [49] | ||
| Personalization, self-configuration of IoT devices, customizability, user-friendliness | [39,47,59,80,103] | ||
| Integration of wireless technologies. | [91] | ||
| Enabled decision support | [92] | ||
| Latency tolerance | [92] | ||
| Robust computational power | [92] | ||
| Optimizing power consumption | [92] | ||
| Expanded data communication rate (F33) (F33 refers to a specific type of data communication rate used in the context of digital communication systems. The “F” usually indicates a frequency or a modulation scheme, while “33” may represent a particular characteristic, such as the number of bits transmitted per symbol or a specific baud rate) | [92] | ||
| Information pervasiveness | [94] | ||
| Care service efficiency, workflow optimization | [87,90,94,101] | ||
| Care process improvement, efficient business process | [39,94] | ||
| Agility | [38] | ||
| Flexibility | [38] | ||
| Interoperability | [39] | ||
| IT infrastructure Poorly designed interface | [39,41,61] | ||
| Infotainment | [66] | ||
| Wearability | [66] | ||
| Technical efficiency | [45] | ||
| Security | Privacy issue, perceived privacy protection (PPR), privacy risks, enhancement of privacy | [27,29,31,32,39,52,57,58,66,67,73,83,87,91,95,96,98] | [40,48,50,60,102] |
| Security concerns, security risk | [29,31,39,48,50,52,67,73,83,87,95,96] | [60,84] | |
| Confidentiality concerns | [67] | [28] | |
| Assurance barriers | [63] | ||
| Defective health information, health information accuracy, precise diagnosis | [63,69,87,102] | [81] | |
| Cyber resilience, | [2] | ||
| Adequate training, cybersecurity education | [61,80,84] | ||
| Regulatory environment, regulatory affairs, government regulations, presence of clear objectives and plans for MIoT systems adoption, legal frameworks, roles and responsibilities, compliance and policy | [29,41,62,67,76,83,84,96,97] | [67,71] | |
| Risk perception, perceived risk, risk barrier | [35,45,49,52,86,99] | [1,72] | |
| Perceived trust (PT) | [2,30,33,36,48,52,60,73,75,86,91,93,100] | [68] | |
| Perceived vulnerability | [69] | ||
| Perceived severity | [68,69,86] | ||
| Environmental | Perceived convenience value (PCV) | [27,35,59] | |
| Performance expectancy (PE) | [28,30,33,36,48,50,55,58,60,68,70,72,74,75,77,85] | ||
| External support (ES) from government entities, consultants, and software suppliers, as well as selection of a reliable and experienced MIoT vendor, skilled IT professionals, vendor credibility | [29,39,71,76,78,101] | ||
| Awareness of the IoT system | [65,76,88] | ||
| Support and commitment of top management, management support (MS) | [29,71] | ||
| Organizational readiness | [71] | ||
| Organizational culture | [83] | ||
| Epidemic ecosystem | [62] | ||
| Monitoring and governance | [83] | ||
| Readiness | [45] | ||
| Opportunity factors: fascinating conditions, preserved fascinating conditions | [30,74] | [60,68] | |
| Social influence (SI), social support, reference group influence, preserved social usefulness, social norms | [1,2,28,34,44,46,48,55,58,60,62,70,72,75,77,85,102,103] | [36,50,68,74] | |
| Awareness of consequences (AoC) | [46] | ||
| Ascription of responsibility (AoR) | [46] | ||
| Digital and data literacy | [85] | ||
| Doctor–patient relationship (D-PR) | [68] | ||
| Collaboration environment | [100] | ||
| Openness | [56] | ||
| Physician recommendation | [61] | ||
| Free equipment | [61] | ||
| Other | Perceived cost (PC), preserved value (PV) | [27,31,36,39,42,49,57,58,60,61,64,67,72,78,87,98] | [1,65,74,77] |
| Relative advantage (REL) | [32,34,35] | [31,71] | |
| Threat | [30,33] | [28] | |
| Job relevance | [42] | ||
| Information quality | [42] | ||
| Application areas | [87] | ||
| Availability | [44,48,89] | ||
| Perceived pressure | [44] | ||
| Effort expectancy (EE) | [36,55,60,68,70,72,74,75,85] | [28,48,50,58,77] | |
| Value creation | [83] | ||
| Expert advice (EA) | [36] | ||
| Life quality expectancy | [58] | ||
| Benefits: functional benefits, informational benefits, psychological benefits, external benefits, benefits of using an IoT system | [42,45,63,88,90,99] | ||
| Preserved control, perceived behavioral control | [39,40,52,64,99] | [37] | |
| Observability | [31] | ||
| Close to action | [68] | ||
| Discomfort | [50] | ||
| Determining the type of signals to be collected, psychological/environmental | [92] | ||
| Hedonic motivation | [60,69,76] | [74] | |
| Moral consideration | [99] | ||
| Preserved as a fuse | [37] | ||
| Preserved novelty | [69] | ||
| e-Loyalty | [43] | ||
| Effort | [100] | ||
| Actual control | [99] | ||
| Overall consistency of internet coverage, efficient local and global communication | [39,41,91] | [66] | |
References
- Yin, Z.; Yan, J.; Fang, S.; Wang, D.; Han, D. User acceptance of wearable intelligent medical devices through a modified unified theory of acceptance and use of technology. Ann. Transl. Med. 2022, 10, 629. [Google Scholar] [CrossRef]
- Tsourela, M.; Nerantzaki, D.M. An internet of things (Iot) acceptance model. assessing consumer’s behavior toward iot products and applications. Future Internet 2020, 12, 191. [Google Scholar] [CrossRef]
- Ashton, K. That ‘Internet of Things’ Thing. 2010. Available online: https://www.rfidjournal.com/expert-views/that-internet-of-things-thing/73881/ (accessed on 4 March 2025).
- HAbdul-Ghani, A.; Konstantas, D. A comprehensive study of security and privacy guidelines, threats, and countermeasures: An IoT perspective. J. Sens. Actuator Netw. 2019, 8, 22. [Google Scholar] [CrossRef]
- Minerva, R.; Rotondi, D. Towards a Definition of the Internet of Things (IoT). 2014. Available online: https://www.researchgate.net/publication/317588072 (accessed on 10 March 2025).
- Nižetić, S.; Šolić, P.; González-de-Artaza, D.L.-D.-I.; Patrono, L. Internet of Things (IoT): Opportunities, issues and challenges towards a smart and sustainable future. J. Clean. Prod. 2020, 274, 122877. [Google Scholar] [CrossRef] [PubMed]
- Ambe, A.H.; Brereton, M.; Soro, A.; Chai, M.Z.; Buys, L.; Roe, P. Older people inventing their personal internet of things with the IoT un-kit experience. In Proceedings of the Conference on Human Factors in Computing Systems, Glasgow, UK, 4–9 May 2019; Association for Computing Machinery: New York, NY, USA, 2019. [Google Scholar] [CrossRef]
- Kronlid, C.; Brantnell, A.; Elf, M.; Borg, J.; Palm, K. Sociotechnical analysis of factors influencing IoT adoption in healthcare: A systematic review. Technol. Soc. 2024, 78, 102675. [Google Scholar] [CrossRef]
- Hu, F.; Yang, H.; Qiu, L.; Wang, X.; Ren, Z.; Wei, S.; Zhou, H.; Chen, Y.; Hu, H. Innovation networks in the advanced medical equipment industry: Supporting regional digital health systems from a local–national perspective. Front. Public Health 2025, 13, 1635475. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhou, L.; Wang, S.; Fan, C.; Huang, D. Facilitating Patient Adoption of Online Medical Advice Through Team-Based Online Consultation. J. Theor. Appl. Electron. Commer. Res. 2025, 20, 231. [Google Scholar] [CrossRef]
- Selvaraj, S.; Sundaravaradhan, S. Challenges and Opportunities in IoT Healthcare Systems: A Systematic Review; Springer Nature: Berlin/Heidelberg, Germany, 2020. [Google Scholar] [CrossRef]
- Javaid, M.; Haleem, A.; Singh, R.P.; Suman, R. Towards insighting cybersecurity for healthcare domains: A comprehensive review of recent practices and trends. Cyber Secur. Appl. 2023, 1, 100016. [Google Scholar] [CrossRef]
- Zhou, W.; Piramuthu, S. IoT security perspective of a flexible healthcare supply chain. Inf. Technol. Manag. 2018, 19, 141–153. [Google Scholar] [CrossRef]
- Pirbhulal, S.; Samuel, O.W.; Wu, W.; Sangaiah, A.K.; Li, G. A joint resource-aware and medical data security framework for wearable healthcare systems. Future Gener. Comput. Syst. 2019, 95, 382–391. [Google Scholar] [CrossRef]
- Martínez, A.L.; Pérez, M.G.; Ruiz-Martínez, A. A Comprehensive Review of the State-of-the-Art on Security and Privacy Issues in Healthcare. ACM Comput. Surv. 2023, 55, 1–38. [Google Scholar] [CrossRef]
- HHS. HIPAA Home. Available online: https://www.hhs.gov/hipaa/index.html (accessed on 5 July 2025).
- General Data Protection Regulation (GDPR)—Legal Text. Available online: https://gdpr-info.eu/ (accessed on 5 July 2025).
- Gafni, R.; Pavel, T. Cyberattacks against the health-care sectors during the COVID-19 pandemic. Inf. Comput. Secur. 2022, 30, 137–150. [Google Scholar] [CrossRef]
- Cartwright, A.J. The elephant in the room: Cybersecurity in healthcare. J. Clin. Monit. Comput. 2023, 37, 1123–1132. [Google Scholar] [CrossRef] [PubMed]
- Kashani, M.H.; Madanipour, M.; Nikravan, M.; Asghari, P.; Mahdipour, E. A systematic review of IoT in healthcare: Applications, techniques, and trends. J. Netw. Comput. Appl. 2021, 192, 103164. [Google Scholar] [CrossRef]
- Jawad, H.H.M.; Hassan, Z.B.; Zaidan, B.B.; Jawad, F.H.M.; Jawad, D.H.M.; Alredany, W.H.D. A Systematic Literature Review of Enabling IoT in Healthcare: Motivations, Challenges, and Recommendations. Electronics 2022, 11, 3223. [Google Scholar] [CrossRef]
- Al-rawashdeh, M.; Keikhosrokiani, P.; Belaton, B.; Alawida, M.; Zwiri, A. IoT Adoption and Application for Smart Healthcare: A Systematic Review. Sensors 2022, 22, 5377. [Google Scholar] [CrossRef]
- Li, C.; Wang, J.; Wang, S.; Zhang, Y. A review of IoT applications in healthcare. Neurocomputing 2024, 565, 127017. [Google Scholar] [CrossRef]
- Okoli, C.; Schabram, K. A Guide to Conducting a Systematic Literature Review of Information Systems Research; Working Papers on Information Systems; Association for Information Systems: Atlanta, GA, USA, 2010. [Google Scholar]
- Wohlin, C.; Mendes, E.; Felizardo, K.R.; Kalinowski, M. Guidelines for the search strategy to update systematic literature reviews in software engineering. Inf. Softw. Technol. 2020, 127, 106366. [Google Scholar] [CrossRef]
- Boell, S.K.; Cecez-Kecmanovic, D. On being ‘systematic’ in literature reviews in IS. J. Inf. Technol. 2015, 30, 161–173. [Google Scholar] [CrossRef]
- Massaro, M.; Dumay, J.; Guthrie, J. On the shoulders of giants: Undertaking a structured literature review in accounting. Account. Audit. Account. J. 2016, 29, 767–801. [Google Scholar] [CrossRef]
- Kitchenham, B.; Charters, S.M. Guidelines for performing Systematic Literature Reviews in Software Engineering. 2007. Available online: https://www.researchgate.net/publication/302924724 (accessed on 12 March 2025).
- Cai, L.; Zhu, Y. The challenges of data quality and data quality assessment in the big data era. Data Sci. J. 2015, 14, 2. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Alanazi, M.; Soh, B. Behavioral Intention to Use IoT Technology in Healthcare Settings. Eng. Technol. Appl. Sci. Res. 2019, 5, 4769–4774. Available online: https://www.etasr.com (accessed on 15 March 2025). [CrossRef]
- Alomari, A.; Soh, B. Determinants of Medical Internet of Things Adoption in Healthcare and the Role of Demographic Factors Incorporating Modified UTAUT. Int. J. Adv. Comput. Sci. Appl. 2023, 14, 17–31. Available online: https://www.ijacsa.thesai.org (accessed on 12 March 2025). [CrossRef]
- Abuabid, A.A. Preliminary Model on Factors Influencing the Adoption of Medical Internet of Things (MIoT) Systems in Small and Medium-sized Hospitals in Saudi Arabia. In Proceedings of the 2024 3rd International Conference on Computational Modelling, Simulation and Optimization, ICCMSO 2024, Phuket, Thailand, 14–16 June 2024; Institute of Electrical and Electronics Engineers Inc.: Singapore, 2024; pp. 127–133. [Google Scholar] [CrossRef]
- Al Moteri, M.; Alojail, M. Factors influencing the Supply Chain Management in e-Health using UTAUT model. Electron. Res. Arch. 2023, 31, 2855–2877. [Google Scholar] [CrossRef]
- Masmali, F.H.; Miah, S.J. Adoption of IoT based innovations for healthcare service delivery in Saudi Arabia. In Proceedings of the 2019 IEEE Asia-Pacific Conference on Computer Science and Data Engineering, CSDE 2019, Melbourne, Australia, 9–11 December 2019; Institute of Electrical and Electronics Engineers Inc.: Singapore, 2019. [Google Scholar] [CrossRef]
- Karahoca, A.; Karahoca, D.; Aksöz, M. Examining intention to adopt to internet of things in healthcare technology products. Kybernetes 2018, 47, 742–770. [Google Scholar] [CrossRef]
- Dadhich, M.; Hiran, K.K.; Rao, S.S.; Sharma, R. Factors Influencing Patient Adoption of the IoT for e-Health Management Systems (e-HMS) Using the UTAUT Model: A High order SeM-ANN Approach. Int. J. Ambient Comput. Intell. 2022, 13, 1–18. [Google Scholar] [CrossRef]
- Dutta, A.; Kovid, R.K.; Thatha, M.; Gupta, J. Adoption of IoT-based healthcare devices: An empirical study of end consumers in an emerging economy. Paladyn J. Behav. Robot. 2023, 14, 20220106. [Google Scholar] [CrossRef]
- Sivathanu, B. Adoption of internet of things (IOT) based wearables for healthcare of older adults—A behavioural reasoning theory (BRT) approach. J. Enabling Technol. 2018, 12, 169–185. [Google Scholar] [CrossRef]
- Pal, D.; Funilkul, S.; Charoenkitkarn, N.; Kanthamanon, P. Internet-of-Things and Smart Homes for Elderly Healthcare: An End User Perspective. IEEE Access 2018, 6, 10483–10496. [Google Scholar] [CrossRef]
- Mital, M.; Chang, V.; Choudhary, P.; Papa, A.; Pani, A.K. Adoption of Internet of Things in India: A test of competing models using a structured equation modeling approach. Technol. Forecast. Soc. Change 2018, 136, 339–346. [Google Scholar] [CrossRef]
- Chakraborty, S.; Bhatt, V.; Chakravorty, T. Impact of iot adoption on agility and flexibility of healthcare organization. Int. J. Innov. Technol. Explor. Eng. 2019, 8, 2673–2681. [Google Scholar] [CrossRef]
- Tripathi, S. System Dynamics perspective for Adoption of Internet of Things: A Conceptual Framework. Available online: https://www.researchgate.net/profile/Shailja-Tripathi/publication/338365676_System_Dynamics_perspective_for_Adoption_of_Internet_of_Things_A_Conceptual_Framework/links/5e143953a6fdcc28375dd24c/System-Dynamics-perspective-for-Adoption-of-Internet-of-Things-A-Conceptual-Framework.pdf (accessed on 20 March 2025).
- Srivastava, N.K.; Chatterjee, N.; Subramani, A.K.; Jan, N.A.; Singh, P.K. Is health consciousness and perceived privacy protection critical to use wearable health devices? Extending the model of goal-directed behavior. Benchmarking 2022, 29, 3079–3096. [Google Scholar] [CrossRef]
- Desingh, V.; Baskaran, R. Internet of Things adoption barriers in the Indian healthcare supply chain: An ISM-fuzzy MICMAC approach. Int. J. Health Plan. Manag. 2022, 37, 318–351. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, S.; Blas, S.S.; Castañeda, J.A. Physicians’ adoption of mobile health monitoring systems in spain: Competing models and impact of prior experience. J. Electron. Commer. Res. 2015, 16, 194. [Google Scholar]
- Martínez-Caro, E.; Cegarra-Navarro, J.G.; García-Pérez, A.; Fait, M. Healthcare service evolution towards the Internet of Things: An end-user perspective. Technol. Forecast. Soc. Change 2018, 136, 268–276. [Google Scholar] [CrossRef]
- Sun, N.; Rau, P.L.P. The acceptance of personal health devices among patients with chronic conditions. Int. J. Med. Inform. 2015, 84, 288–297. [Google Scholar] [CrossRef]
- Liu, D.; Li, Q.; Han, S. Using Extended Technology Acceptance Model to Assess the Adopt Intention of a Proposed IoT-Based Health Management Tool. Sensors 2022, 22, 6092. [Google Scholar] [CrossRef]
- Yang, Q.; Al Mamun, A.; Wu, M.; Naznen, F. Strengthening health monitoring: Intention and adoption of Internet of Things-enabled wearable healthcare devices. Digit Health 2024, 10, 20552076241279199. [Google Scholar] [CrossRef]
- Li, F.; Negera, D.T.; Chudhery, M.A.Z.; Zhao, Q.; Gao, L. IoT and Motion Recognition-based Healthcare Rehabilitation Systems (IMRHRS): An Empirical Examination from Physicians’ Perspective Using Stimulus-Organism-Response Theory. IEEE Access 2024, 12, 142863–142882. [Google Scholar] [CrossRef]
- Jawad, H.H.M.; Hassan, Z.B.; Zaidan, B.B. Factors Influencing the Behavioural Intention of Patients with Chronic Diseases to Adopt IoT-Healthcare Services in Malaysia. J. Hunan Univ. Nat. Sci. 2023, 50, 26–42. [Google Scholar] [CrossRef]
- Arifin, T.R.T.; Mohamad, Z.Z.; Samsuri, A.S.; Hussin, S.M.; Zainol, S.S.; Badaruddin, M.N.A. Resistance and drivers to adopting the internet of things in healthcare services. Platf. A J. Manag. Humanit. 2022, 5, 16–26. [Google Scholar]
- Doualeh, A.I.; Rahman, N.A.A.; Ismail, N. A Survey of Adopting Smart Home Healthcare via IoT Technology. In Proceedings of the International Conference on Developments in eSystems Engineering, DeSE, Sharjah, United Arab Emirates, 7–10 December 2021; Institute of Electrical and Electronics Engineers Inc.: Singapore, 2021; pp. 136–141. [Google Scholar] [CrossRef]
- Malarvizhi, C.A.; Subramaniam, S.S.; Jayashree, S. Analysing the Behaviour Intention of IOT Adoption Among Elderly NCD Patients in Malaysia. In Proceedings of the International Conference on Computational Intelligence and Sustainable Engineering Solution, CISES 2023, Greater Noida, India, 28–30 April 2023; Institute of Electrical and Electronics Engineers Inc.: Singapore, 2023; pp. 1029–1035. [Google Scholar] [CrossRef]
- Alraja, M. Frontline healthcare providers’ behavioural intention to Internet of Things (IoT)-enabled healthcare applications: A gender-based, cross-generational study. Technol. Forecast. Soc. Change 2022, 174, 121256. [Google Scholar] [CrossRef]
- Alraja, M.N.; Farooque, M.M.J.; Khashab, B. The Effect of Security, Privacy, Familiarity, and Trust on Users’ Attitudes Toward the Use of the IoT-Based Healthcare: The Mediation Role of Risk Perception. IEEE Access 2019, 7, 111341–111354. [Google Scholar] [CrossRef]
- Jonas, D.; Maria, E.; Sutarto; Widiasari, I.R.; Rahardja, U.; Wellem, T. Design of a TAM Framework with Emotional Variables in the Acceptance of Health-based IoT in Indonesia. ADI J. Recent Innov. 2023, 5, 146–154. [Google Scholar] [CrossRef]
- Nurhayati, S.; Anandari, D.; Ekowati, W. Unified Theory of Acceptance and Usage of Technology (UTAUT) Model to Predict Health Information System Adoption. J. Kesehat. Masy. 2019, 15, 89–97. [Google Scholar] [CrossRef]
- Prayoga, T.; Abraham, J. Behavioral intention to use IoT health device: The role of perceived usefulness, facilitated appropriation, big five personality traits, and cultural value orientations. Int. J. Electr. Comput. Eng. 2016, 6, 1751–1765. [Google Scholar] [CrossRef]
- Alhasan, A.; Audah, L.; Ibrahim, I.; Al-Sharaa, A.; Al-Ogaili, A.S.; Mohammed, J.M. A case-study to examine doctors’ intentions to use IoT healthcare devices in Iraq during COVID-19 pandemic. Int. J. Pervasive Comput. Commun. 2022, 18, 527–547. [Google Scholar] [CrossRef]
- Alaiad, A.; Zhou, L. Patients’ adoption of WSN-Based smart home healthcare systems: An integrated model of facilitators and barriers. IEEE Trans. Prof. Commun. 2017, 60, 4–23. [Google Scholar] [CrossRef]
- Kang, M.J.; Hwang, Y.C. Exploring the Factors Affecting the Continued Usage Intention of IoT-Based Healthcare Wearable Devices Using the TAM Model. Sustainability 2022, 14, 12492. [Google Scholar] [CrossRef]
- Aldossari, M.Q.; Sidorova, A. Consumer Acceptance of Internet of Things (IoT): Smart Home Context. J. Comput. Inf. Syst. 2020, 60, 507–517. [Google Scholar] [CrossRef]
- Cajita, M.I.; Hodgson, N.A.; Lam, K.W.; Yoo, S.; Han, H.R. Facilitators of and Barriers to mHealth Adoption in Older Adults with Heart Failure. CIN Comput. Inform. Nurs. 2018, 36, 376–382. [Google Scholar] [CrossRef]
- Guerra, K.; Koh, C.; Prybutok, V.; Johnson, V. WIoT Adoption Among Young Adults in Healthcare Crises. J. Comput. Inf. Syst. 2022, 63, 1316–1331. [Google Scholar] [CrossRef]
- Consumer Reasoning Cognition in Adopting IoT for Healthcare Purposes: A Behavioral Reasoning Theory Perspective. Available online: https://ssrn.com/abstract=4241197 (accessed on 20 March 2025).
- Park, E.; Cho, Y.; Han, J.; Kwon, S.J. Comprehensive Approaches to User Acceptance of Internet of Things in a Smart Home Environment. IEEE Internet Things J. 2017, 4, 2342–2350. [Google Scholar] [CrossRef]
- Lee, S.Y.; Lee, K. Factors that influence an individual’s intention to adopt a wearable healthcare device: The case of a wearable fitness tracker. Technol. Forecast. Soc. Change 2018, 129, 154–163. [Google Scholar] [CrossRef]
- Chang, H.S.; Lee, S.C.; Ji, Y.G. Wearable device adoption model with TAM and TTF. Int. J. Mob. Commun. 2016, 14, 518. [Google Scholar] [CrossRef]
- Tariq, M.I.; Mian, N.A.; Sohail, A.; Alyas, T.; Ahmad, R. Evaluation of the challenges in the internet of medical things with multicriteria decision making (AHP and TOPSIS) to overcome its obstruction under fuzzy environment. Mob. Inf. Syst. 2020, 2020, 1–19. [Google Scholar] [CrossRef]
- ZSolangi, A.; Solangi, Y.A.; Maher, Z.A. Adoption of IoT-based Smart Healthcare: An Empirical Analysis in the Context of Pakistan. J. Hunan Univ. Nat. Sci. 2021, 48, 143–153. Available online: https://www.jonuns.com/index.php/journal/article/view/704 (accessed on 20 March 2025).
- Zhang, Q.; Khan, S.; Khan, S.U.; Khan, I.U. Assessing the older population acceptance of healthcare wearable in a developing Country: An extended PMT model. J. Data Inf. Manag. 2023, 5, 39–53. [Google Scholar] [CrossRef]
- Dahri, A.S.; Massan, S.-R.; Thebo, L.A. An overview of AI enabled M-IoT wearable technology and its effects on the conduct of medical professionals in Public Healthcare in Pakistan. 3C Tecnol. Glosas Innov. Apl. Pyme 2020, 9, 87–111. [Google Scholar] [CrossRef]
- Naeem, S.B.; Azam, M.; Boulos, M.N.K.; Bhatti, R. Leveraging the TOE Framework: Examining the Potential of Mobile Health (mHealth) to Mitigate Health Inequalities. Information 2024, 15, 176. [Google Scholar] [CrossRef]
- Arfi, W.B.; Nasr, I.B.; Khvatova, T.; Zaied, Y.B. Understanding Acceptance of eHealthcare by IoT Natives and IoT Immigrants: An Integrated Model of UTAUT, Perceived Risk, and Financial Cost. Technol. Forecast. Soc. Change 2021, 163, 120437. [Google Scholar] [CrossRef]
- Thapa, S.; Bello, A.; Maurushat, A.; Farid, F. Security Risks and User Perception towards Adopting Wearable Internet of Medical Things. Int. J. Environ. Res. Public Health 2023, 20, 5519. [Google Scholar] [CrossRef] [PubMed]
- Walle, A.D.; Jemere, A.T.; Tilahun, B.; Endehabtu, B.F.; Wubante, S.M.; Melaku, M.S.; Tegegne, M.D.; Gashu, K.D. Intention to use wearable health devices and its predictors among diabetes mellitus patients in Amhara region referral hospitals, Ethiopia: Using modified UTAUT-2 model. Inform. Med. Unlocked 2023, 36, 101157. [Google Scholar] [CrossRef]
- Chang, C.-C. Exploring the Usage Intentions of Wearable Medical Devices: A Demonstration Study. Interact. J. Med. Res. 2020, 9, e19776. [Google Scholar] [CrossRef]
- Bele, S.; Cassidy, C.; Curran, J.; Johnson, D.W.; Saunders, C.; Bailey, J.A.M. Barriers and enablers to implementing a virtual tertiary-regional Telemedicine Rounding and Consultation (TRAC) model of inpatient pediatric care using the Theoretical Domains Framework (TDF) approach: A study protocol. BMC Health Serv. Res. 2019, 19, 29. [Google Scholar] [CrossRef]
- Alam, M.Z.; Hoque, M.R.; Hu, W.; Barua, Z. Factors influencing the adoption of mHealth services in a developing country: A patient-centric study. Int. J. Inf. Manag. 2020, 50, 128–143. [Google Scholar] [CrossRef]
- Reidy, C.; A’cOurt, C.; Jenkins, W.; Jani, A.; Ramos, A.; Morys-Carter, M.; Papoutsi, C. ‘The plural of silo is not ecosystem’: Qualitative study on the role of innovation ecosystems in supporting ‘Internet of Things’ applications in health and care. Digit. Health 2023, 9, 20552076221147114. [Google Scholar] [CrossRef]
- Achituv, D.B.; Haiman, L. Physicians’ attitudes toward the use of IoT medical devices as part of their practice. Online J. Appl. Knowl. Manag. 2016, 4, 128–145. [Google Scholar] [CrossRef]
- Gagliardi, A.R.; Carrubbo, L.; Rozenes, S.; Fux, A.; Siano, D. Assessing IoT integration in ICUs’ settings and management: A cross-country analysis among local healthcare organizations. Digit. Policy Regul. Gov. 2024. ahead of print. [Google Scholar] [CrossRef]
- Canhoto, A.I.; Arp, S. Exploring the factors that support adoption and sustained use of health and fitness wearables. J. Mark. Manag. 2016, 33, 32–60. [Google Scholar] [CrossRef]
- Rodić, B.; Stevanović, V.; Labus, A.; Kljajić, D.; Trajkov, M. Adoption Intention of an IoT Based Healthcare Technologies in Rehabilitation Process. Int. J. Hum.–Comput. Interact. 2023, 40, 2873–2886. [Google Scholar] [CrossRef]
- Hasi, F.; Beirens, B.; Serral, E. Maturity model for iot adoption in hospitals. Comput. Inform. 2022, 41, 213–232. [Google Scholar] [CrossRef]
- Cleveland, S.M.; Haddara, M. Internet of Things for diabetics: Identifying adoption issues. Internet Things 2023, 22, 100798. [Google Scholar] [CrossRef]
- Edu, A.S. Configural paths for IoTs and big data analytics acceptance for healthcare improvement: A fuzzy-set qualitative comparative analysis. Aslib J. Inf. Manag. 2024, 76, 800–821. [Google Scholar] [CrossRef]
- Zhao, Y.; Ni, Q.; Zhou, R. What factors influence the mobile health service adoption? A meta-analysis and the moderating role of age. Int. J. Inf. Manag. 2018, 43, 342–350. [Google Scholar] [CrossRef]
- Charyyev, B.; Mansouri, M.; Gunes, M.H. Modeling the Adoption of Internet of Things in Healthcare: A Systems Approach. In Proceedings of the ISSE 2021—7th IEEE International Symposium on Systems Engineering, Proceedings, Vienna, Austria, 13 September–13 October 2021; Institute of Electrical and Electronics Engineers Inc.: Singapore, 2021. [Google Scholar] [CrossRef]
- Johri, A.; Bhadula, S.; Sharma, S.; Shukla, A.S. Assessment of factors affecting implementation of IoT based smart skin monitoring systems. Technol. Soc. 2022, 68, 101908. [Google Scholar] [CrossRef]
- Strielkina, A.; Uzun, D.; Kharchenko, V. IDAACS 2017. Modelling of Healthcare IoT Using the Queueing Theory. In Proceedings of the 2017 IEEE 9th International Conference on Intelligent Data Acquisition and Advanced Computing Systems: Technology and Applications, Bucharest, Romania, 21–23 September 2017; IEEE: Piscataway, NJ, USA, 2017. [Google Scholar]
- Philip, N.Y.; Rodrigues, J.J.P.C.; Wang, H.; Fong, S.J.; Chen, J. Internet of Things for In-Home Health Monitoring Systems: Current Advances, Challenges and Future Directions. IEEE J. Sel. Areas Commun. 2021, 39, 300–310. [Google Scholar] [CrossRef]
- Niranjan, S.K.; Raja, J.; Rajini, A.R. Survey of Smart healthcare systems using Internet of things (IoT). In Proceedings of the 2018 International Conference on Communication, Computing & Internet of Things: IC3IoT 2018, Department of Electronics and Communication Engineering, Sri Sairam Engineering College, Chennai, India, 15–17 February 2018; IEEE: Piscataway, NJ, USA, 2018. [Google Scholar]
- Habibzadeh, H.; Dinesh, K.; Shishvan, O.R.; Boggio-Dandry, A.; Sharma, G.; Soyata, T. A Survey of Healthcare Internet of Things (HIoT): A Clinical Perspective. IEEE Internet Things J. 2019, 7, 53–71. [Google Scholar] [CrossRef]
- Bhatt, V.; Chakraborty, S. Importance of trust in iot based wearable device adoption by patient: An empirical investigation. In Proceedings of the 4th International Conference on IoT in Social, Mobile, Analytics and Cloud, ISMAC 2020, Palladam, India, 7–9, October 2020; Institute of Electrical and Electronics Engineers Inc.: Singapore, 2020; pp. 1226–1231. [Google Scholar] [CrossRef]
- Chakraborty, S.; Bhatt, V. Mobile IoT adoption as antecedent to Care-Service Efficiency and Improvement: Empirical study in Healthcare-context. J. Int. Technol. Inf. Manag. 2019, 28, 101–120. [Google Scholar] [CrossRef]
- Latif, S.; Zafar, N.A.; Khan, R.Y. A Survey of Security and Privacy Issues in IoT for Smart Cities. In Proceedings of the 2017 Fifth International Conference on Aerospace Science & Engineering (ICASE), Islamabad, Pakistan, 14–16 November 2017. [Google Scholar]
- Raje, V.V.; Mohite, R.V.; Srivastava, S.; Lipi, K.; Gavhane, Y.; Devi, T.J. Data Security and Privacy in the Smart Healthcare System. In Proceedings of the 2024 International Conference on Healthcare Innovations, Software and Engineering Technologies, HISET 2024, Karad, India, 18–19 January 2024; Institute of Electrical and Electronics Engineers Inc.: Singapore, 2024; pp. 204–206. [Google Scholar] [CrossRef]
- Abdulghani, H.A.; Nijdam, N.A.; Konstantas, D. Analysis on Security and Privacy Guidelines: RFID-Based IoT Applications. IEEE Access 2022, 10, 131528–131554. [Google Scholar] [CrossRef]
- Newcombe, L.; Yang, P.; Carter, C.; Hanneghan, M. Internet of things enabled technologies for behaviour analytics in elderly person care: A survey. In Proceedings of the 2017 IEEE International Conference on Internet of Things, IEEE Green Computing and Communications, IEEE Cyber, Physical and Social Computing, IEEE Smart Data, iThings-GreenCom-CPSCom-SmartData 2017, Exeter, UK, 21–23 June 2017; Institute of Electrical and Electronics Engineers Inc.: Singapore, 2017; pp. 863–870. [Google Scholar] [CrossRef]
- Princi, E.; Krämer, N.C. Out of Control—Privacy Calculus and the Effect of Perceived Control and Moral Considerations on the Usage of IoT Healthcare Devices. Front. Psychol. 2020, 11, 582054. [Google Scholar] [CrossRef]
- Dauwed, M.A.; Yahaya, J.; Zulkefli, A.M.; Hamdan, R. Human factors for iot services utilization for health information exchange. J. Theor. Appl. Inf. Technol. 2018, 96, 2095–2105. Available online: https://www.jatit.org/volumes/Vol96No8/3Vol96No8.pdf (accessed on 20 March 2025).
- Kadu, M.M.; Gray, C.S.; Berta, W. Assessing Factors that Influence the Implementation of Technologies Enabling Integrated Care Delivery for Older Adults with Complex Needs: A Systematic Review. Int. J. Integr. Care 2018, 18, 374. [Google Scholar] [CrossRef]
- Cheung, M.L.; Chau, K.Y.; Lam, M.H.S.; Tse, G.; Ho, K.Y.; Flint, S.W.; Broom, D.R.; Tso, E.K.H.; Lee, K.Y. Examining consumers’ adoption of wearable healthcare technology: The role of health attributes. Int. J. Environ. Res. Public Health 2019, 16, 2257. [Google Scholar] [CrossRef]
- Abouzahra, M.; Ghasemaghaei, M. The antecedents and results of seniors’ use of activity tracking wearable devices. Health Policy Technol. 2020, 9, 213–217. [Google Scholar] [CrossRef]
- Gao, Y.; Li, H.; Luo, Y. An empirical study of wearable technology acceptance in healthcare. Ind. Manag. Data Syst. 2015, 115, 1704–1723. [Google Scholar] [CrossRef]
- Baker, S.B.; Xiang, W.; Atkinson, I. Internet of Things for Smart Healthcare: Technologies, Challenges, and Opportunities. IEEE Access 2017, 5, 26521–26544. [Google Scholar] [CrossRef]
- Kalsoom, T.; Ramzan, N.; Ahmed, S.; Anjum, N.; Safdar, G.A.; Rehman, M.U. Socio-Organisational Challenges and Impacts of IoT: A Review in Healthcare and Banking. J. Sens. Actuator Netw. 2025, 14, 46. [Google Scholar] [CrossRef]
- Ye, Q. Digital leadership enhances organizational resilience by fostering job crafting: The moderating role of organizational culture. Sci. Rep. 2025, 15, 24640. [Google Scholar] [CrossRef]
- Shukla, S.; Thakur, S.; Hussain, S.; Breslin, J.G.; Jameel, S.M. Identification and Authentication in Healthcare Internet-of-Things Using Integrated Fog Computing Based Blockchain Model. Internet Things 2021, 15, 100422. [Google Scholar] [CrossRef]
- Almaiah, M.A.; Hajjej, F.; Ali, A.; Pasha, M.F.; Almomani, O. A Novel Hybrid Trustworthy Decentralized Authentication and Data Preservation Model for Digital Healthcare IoT Based CPS. Sensors 2022, 22, 1448. [Google Scholar] [CrossRef]
- Ali, A.; Almaiah, M.A.; Hajjej, F.; Pasha, M.F.; Fang, O.H.; Khan, R.; Teo, J.; Zakarya, M. An Industrial IoT-Based Blockchain-Enabled Secure Searchable Encryption Approach for Healthcare Systems Using Neural Network. Sensors 2022, 22, 572. [Google Scholar] [CrossRef]
- Lin, H.; Kaur, K.; Wang, X.; Kaddoum, G.; Hu, J.; Hassan, M.M. Privacy-Aware Access Control in IoT-Enabled Healthcare: A Federated Deep Learning Approach. IEEE Internet Things J. 2023, 10, 2893–2902. [Google Scholar] [CrossRef]
- Singh, S.; Rathore, S.; Alfarraj, O.; Tolba, A.; Yoon, B. A framework for privacy-preservation of IoT healthcare data using Federated Learning and blockchain technology. Future Gener. Comput. Syst. 2022, 129, 380–388. [Google Scholar] [CrossRef]
- Hosain, Y.; Çakmak, M. XAI-XGBoost: An innovative explainable intrusion detection approach for securing internet of medical things systems. Sci. Rep. 2025, 15, 22278. [Google Scholar] [CrossRef] [PubMed]
- Sathya, D.; Veena, S.; Yankanchi, S.R.; Manasa, S. Edge Computing and Blockchain-Based Data Security in IoMT. Int. J. Online Biomed. Eng. 2025, 21, 124–140. [Google Scholar] [CrossRef]
- Pelekoudas-Oikonomou, F.; Zachos, G.; Papaioannou, M.; de Ree, M.; Ribeiro, J.C.; Mantas, G.; Rodriguez, J. Blockchain-Based Security Mechanisms for IoMT Edge Networks in IoMT-Based Healthcare Monitoring Systems. Sensors 2022, 22, 2449. [Google Scholar] [CrossRef]
- Zhang, L.; Xu, J.; Vijayakumar, P.; Sharma, P.K.; Ghosh, U. Homomorphic Encryption-Based Privacy-Preserving Federated Learning in IoT-Enabled Healthcare System. IEEE Trans. Netw. Sci. Eng. 2023, 10, 2864–2880. [Google Scholar] [CrossRef]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).