Abstract
Background/Objectives: Dysphagia represents a significant global health concern with particularly high prevalence in specific clinical conditions, yet educational gaps persist among healthcare professionals and caregivers. This observational, cross-sectional quantitative study aimed to provide a comprehensive overview of the current self-perceived knowledge and learning needs among stakeholders involved in dysphagia management. Methods: An international online survey was conducted in five European countries (Greece, Italy, Lithuania, Spain, and Turkey) with 463 participants: 297 professionals (healthcare and non-health specialists, educators, students) and 166 non-professionals (patients, family members, caregivers, interested individuals). Two structured questionnaires explored self-perceived knowledge, learning needs, relevancy of thematic areas, and preferred learning methods. Chi-square and Fisher’s exact tests were used for statistical comparisons. Results: Professionals reported higher self-perceived knowledge than non-professionals (p < 0.001), yet both groups expressed comparable needs for further education. Priority learning areas varied by respondent profile: “Identification & Treatment” was prioritized by both speech-language pathologists and healthcare specialists, as well as by non-professionals, while dietitian-nutritionists focused on “Diet & Nutrition” and “Food Preparation”. Short-duration courses and visual, hands-on learning tools were preferred across groups. Conclusions: This study highlights a broad demand for dysphagia education among professionals and non-professionals. Tailored, technology-enhanced learning programs could bridge existing knowledge gaps, strengthen multidisciplinary collaboration, and support better daily management of dysphagia.
1. Introduction
Dysphagia is defined as difficulty or inability to perform normal swallowing, that is, the safe transport of food and liquids from the mouth to the stomach. Dysphagia is commonly observed worldwide, and its trend has been increasing in recent years [1]. Its prevalence varies considerably depending on the population studied. In patients with neurological conditions, the global prevalence reaches 50.4% in Parkinson’s disease [2] and 44.8% in multiple sclerosis [3]. Following acute stroke, the pooled incidence of poststroke dysphagia is 42% [4]. In head and neck cancer patients, dysphagia is present in up to 28% at diagnosis, but can increase to 45–75% due to treatment [5]. In healthcare settings, prevalence ranges from 36.5% in hospitals [6] to 56.1% in residential aged care facilities [7]. Dysphagia is associated with serious complications such as malnutrition, dehydration, and aspiration pneumonia, as well as psychological and social consequences that negatively affect quality of life [8,9].
Proper management of dysphagia involves early detection, active treatment, and compensatory strategies. The latter includes adapting food texture and drink viscosity to individual needs and controlling posture during swallowing [10]. These interventions require a multidisciplinary team, including speech-language pathologists (SLPs), dietitians-nutritionists (D-Ns), nurses, physical and occupational therapists, and auxiliary care staff [4,9]. However, in many clinical settings, limited resources restrict access to comprehensive dysphagia care teams, and individual healthcare providers are often required to take responsibility for all aspects of this management. In this sense, several studies among healthcare professionals indicate a clear demand for improving their competencies and skills in this field. Specifically, research among SLPs in the US [11,12], Japan [13], Norway [14], and Australia [15], as well as among nurses in Norway [16], Portugal [17], and Japan [13], consistently points to gaps in dysphagia-related expertise. Similar findings have been reported for broader groups of healthcare professionals in Iran [18] and Spain [4], and for nursing home staff in the UK [19], care homes in Norway [20], intensive care units in the Netherlands [21], and in multi-country studies covering 26 nations [22]. Importantly, previous studies indicate that more than 40% of professionals working in residential centers lack the necessary knowledge for adequate dysphagia management [23,24]. As a result, there is consensus in the literature on the urgent need for enhanced training for both qualified and unqualified care staff [19,20], supported by structured, high-quality continuing professional development programs [4]. The recent TEAMS international survey (877 health professionals from 54 countries) confirmed inadequate knowledge and inconsistent use of validated nutrition screening tools, highlighting the urgent need for targeted education programs [25]. Furthermore, because compensatory management of dysphagia also involves non-healthcare professionals—including food technologists [26], food service employees [27], and healthcare managers [28]—educational initiatives should extend beyond clinical staff to these groups as well.
On the other hand, caregivers and family members play a crucial role in early recognition and daily management of dysphagia [29,30], but recent studies highlight the challenges they face due to limited knowledge, lack of training, and emotional burden [31,32]. In addition, recent research has shown that dysphagia substantially reduces quality of life for patients, their supporters, and healthcare professionals [33]. This wide-ranging impact underscores the importance of including all perspectives in learning strategies. Furthermore, patients themselves must be involved in these programs, as they require clear and accessible information about their condition [34]. While few studies have explored the perceptions of individuals with dysphagia, existing research supports the role of education in improving management and outcomes [35,36]. Despite its relevance, public awareness of dysphagia remains low. A recent survey of US adults revealed limited understanding of the condition, underscoring the need to extend educational efforts beyond clinical settings [37].
Recent studies have emphasized the need to strengthen knowledge translation and educational strategies in healthcare, both within dysphagia management and in broader clinical contexts. Research has shown that improving caregiver training and communication tools can enhance safety and quality of care for patients with dysphagia [38,39], while other studies highlight the importance of structured learning approaches and skills development among health professionals [40,41,42]. However, designing effective educational interventions requires first understanding the current knowledge levels and learning needs across all stakeholder groups—a gap that remains poorly characterized in the literature. Building on this gap, the present study aimed to provide a comprehensive overview of the current self-perceived knowledge and learning needs among stakeholders involved in dysphagia management. An international survey was conducted among professionals and non-professionals involved in dysphagia management to explore: (1) self-perceived knowledge levels and identified educational and training needs, (2) priority topics of interest for each stakeholder group, and (3) preferred learning formats and methodologies. Understanding these perspectives will support the development of targeted educational interventions for all those involved in dysphagia care: professionals, individuals with dysphagia, and their caregivers.
2. Materials and Methods
2.1. Study Design and Participants
The research formed part of the Erasmus+ project INDEED “Innovative tools for Diets oriented to Education and Health Improvement in Dysphagia condition (KA204-083288)”, which involved five countries: Greece, Italy, Lithuania, Spain, and Turkey.
This observational, cross-sectional quantitative study was conducted in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) [43] guidelines. Participation was voluntary and anonymous. Respondents were eligible for inclusion if they met one of the predefined profiles confirmed within the questionnaire:
- Group P (dysphagia-related professionals): healthcare professionals (healthcare specialists—including medical doctors and clinical nutritionists—D-Ns, nursing specialists, and SLPs), non-health professionals involved in dysphagia care (support workers specialized in dysphagia, cooks, food technologists), and teachers or university students in their final years of degrees directly related to the above fields. For students and teachers, belonging to a relevant field was confirmed by requesting their academic discipline.
- Group non-P (dysphagia-related non-professionals): adults with dysphagia and/or swallowing disorders, family members and caregivers of adults or children with dysphagia, and other people interested in this disorder (for example, members or volunteers of organizations that specifically support people with dysphagia).
Exclusion criteria were applied to remove responses from participants who (a) did not match any of the established profiles, (b) provided incomplete data on the main study variables (self-perceived knowledge level and learning needs), or (c) represented profiles with insufficient sample sizes in their respective countries (n < 5).
2.2. Questionnaire Development and Validation
Two short questionnaires (one per target group) were developed in English by the project research team. The development process adhered to CHERRIES (Checklist for Reporting Results of Internet E-Surveys) [44] recommendations for online survey transparency and validation. The initial versions were reviewed by three experts in dysphagia management for face and content validity, evaluating item clarity, relevance, and comprehensiveness. Revisions were made accordingly to improve question wording and content coverage. A pilot test with 12 participants (6 per target group) assessed usability and comprehension, leading to minor adjustments in terminology and layout. Final questionnaires were translated into Greek, Italian, Turkish, Lithuanian, and Spanish using a forward–backward translation procedure following Eremenco et al. (2005) [45], with semantic and conceptual equivalence verified by bilingual experts.
Both questionnaires consisted of three sections: (1) Participant characteristics (age, sex, country, profile, profession or field of study, and personal or professional experience with dysphagia); (2) Self-perceived knowledge level and learning needs regarding dysphagia; and (3) Opinions on relevant dysphagia thematic areas and preferences for learning methodologies and course characteristics (format, duration, and preferred materials). The thematic areas were defined by consensus among project experts and grouped into four blocks: (a) “Identification & Treatment”—definition, detection and diagnosis, pharmacological and surgical treatment, active/clinical management procedures; (b) “Care & Feeding”—oral hygiene, medication administration, feeding techniques, equipment and mealtime environment; (c) “Diet & Nutrition”—malnutrition and dehydration prevention, nutritional adequacy, balanced diet; (d) “Food Preparation”—texture-modified foods, commercial thickeners, safe and appealing recipes. Question formats included closed-ended multiple-choice items (single-answer and check-all-that-apply), yes/no questions, and Likert scales.
2.3. Data Collection, Recoding of Variables and Statistical Analysis
A non-probabilistic snowball sampling approach was used to recruit participants across Greece, Italy, Lithuania, Spain, and Turkey. Each national team initially distributed the online survey through institutional and professional networks and encouraged recipients to forward it to relevant contacts. This process yielded 513 responses, corresponding to an overall estimated multiplication factor of 1.8 between invitations and responses (see Figure 1).
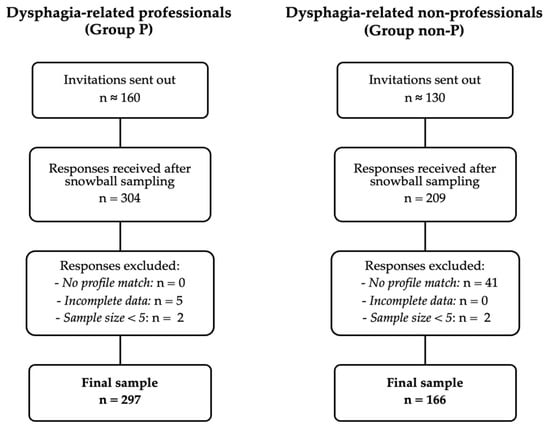
Figure 1.
Flow survey participants.
Questionnaires were administered via Google Forms® (March–April 2021) in accordance with the procedure applied in previous publications [46]. To prevent duplicate submissions, Google Forms’ single-response restriction per user account was enabled.
For analysis, the 1–10 scales for self-perceived knowledge level and learning needs were recoded for easier interpretation and group comparison: 1–4 = low, 5–6 = medium, 7–10 = high. A 4/2/4 distribution was selected instead of equal intervals to more strictly differentiate between high and low levels, maintaining a narrow middle range as medium.
Descriptive statistics (frequencies and percentages) were calculated for all variables. Fisher’s exact tests were used to assess differences between two groups, and Chi-square tests were used to explore differences between several groups. For significant Chi-square tests, standardized residuals were examined to identify which cells showed statistically significant differences from expected frequencies. Statistical analyses were performed using SPSS v26.0 (IBM Corp., Armonk, NY, USA), and significance was set at p < 0.05.
2.4. Ethical and Data-Protection Considerations
Because this study involved anonymous online surveys without personal or sensitive data, ethical committee approval was not required in accordance with institutional and European regulations for minimal-risk research. However, questionnaires were validated by the Data Protection Unit of the University of Zaragoza to ensure compliance with the General Data Protection Regulation (GDPR) as implemented in Spain through Organic Law 3/2018 on Personal Data Protection and Digital Rights.
All participants were informed of the study purpose, data handling procedures, and their right to withdraw at any time before providing consent.
3. Results
3.1. Participants Characteristics
Initially, 304 responses were collected from Group P and 209 from Group non-P. After applying exclusion criteria, 7 cases from Group P and 43 from Group non-P were removed. The final sample comprised 297 participants from Group P and 166 from Group non-P (see Figure 1).
As it is shown in Table 1 Group P comprised health professionals (21% nurses, 15% D-Ns, 15% healthcare specialists, and 8% SLPs), non-health professionals (9% specialists working with patients with dysphagia in institutions, and 2% cook or food industry specialists), University/College lecturers (9%), and University/College students (20%). 40% of the responses came from Spain while the remaining responses (60%) were evenly distributed among Greece, Italy, Lithuania, and Turkey. The respondents were predominantly women (77%) while age was evenly distributed within the ranges. When they were asked about the sources they learned about this disorder, the two most frequently selected options were “At school/studies” (57%), meaning formal academic education, and “In the work environment” (35%), indicating practical workplace experience. Other sources, such as “Courses or training” and “On its own initiative,” yielded relatively lower response rates (24% in both cases).

Table 1.
Description of dysphagia-related professionals’ group (Group P) (n = 297).
Table 2 presents the description of group non-P. This group included adults with dysphagia (19%), family members (25%) or caregivers (30%) of a person with dysphagia, as well as other people interested in this condition (27%). A majority of this group were women (66%) with a homogeneous representation in terms of age, except for the older group (65–79 years old), which presented a lower number of responses (11%). Regarding the use of compensatory procedures for the management of dysphagia, 85% of the respondents (excluding other people interested in dysphagia) selected dysphagia-adapted dishes and beverages, mainly texture-modified foods (35%) and, to a lesser extent, thickened liquids (14%), using commercially available texture-modified foods and thickened beverages (15%), with 20% of them indicating several options. It is remarkable that only 19% of the respondents answered affirmatively to the question “Have you ever attended a training about dysphagia?”.
Table 2.
Description of dysphagia-related non-professionals’ group (Group non-P) (n = 166).
3.2. Self-Perceived Level of Knowledge and Learning Needs
As shown in Table 3, 59% of Group P considered that their knowledge about dysphagia was “Good/Excellent” whereas only 14% rated it as “Poor/Very poor. Statistically significant differences were found among profiles, with a higher percentage of “Good/Excellent” ratings among D-Ns (73%) and a lower one among students (47%), along with a lower percentage of nurses indicating the option “Poor/Very poor” (5%) compared to the highest values, which were observed in university/college students (30%) (p = 0.003). Table 4 reveals that Group non-P participants predominantly rated their dysphagia knowledge as limited, with 53% considering it “Poor/Very poor” compared to only 8% who rated it as “Good/Excellent”. No statistically significant differences were found among the different profiles within Group non-P (p = 0.189).
Table 3.
Self-perceived level of knowledge of dysphagia-related professionals (Group P) (n = 297).
Table 4.
Self-perceived level of knowledge of dysphagia-related non-professionals (Group non-P) (n = 153).
Statistical analysis confirmed that the observed differences between Group P and Group non-P in self-perceived knowledge levels were significant (p < 0.001).
Self-perceived education and training needs for dysphagia management among Group P are presented in Table 5. Most participants (62%) selected “Very probably/Definitely,” while only 12% indicated they did not require additional knowledge and skills in dysphagia. Intra-group analysis revealed statistically significant differences (p = 0.008), with D-Ns and university/college students showing the highest educational needs (80%). Table 6 shows the self-perceived education and training needs among Group non-P participants. Again, most respondents (69%) indicated “Very probably/Definitely” needing additional training, while only 12% felt they did not require further knowledge and skills in dysphagia management. In contrast to Group P, no statistically significant differences were found among the different profiles within Group non-P (p = 0.131).
Table 5.
Self-perceived education and training needs of dysphagia-related professionals (Group P) (n = 297).
Table 6.
Self-perceived education and training needs of dysphagia-related non-professionals (Group non-P) (n = 166).
However, when comparing the overall needs between both groups, no significant differences were found (p = 0.375), suggesting that professional and non-professional stakeholders share similar perceptions regarding their dysphagia learning requirements.
Finally, an exploratory analysis examined whether participants’ experience with dysphagia patients or personal caregiving was associated with their self-perceived knowledge levels and educational and training needs. As presented in Table 7, 70% of those reporting experience considered that their knowledge on dysphagia was “Good/Excellent” compared to 49% of those reporting no experience (p = 0.013). However, no statistically significant differences were found between both groups regarding self-perceived need for education and training, with 61% and 57%, respectively, selecting “Very probably/Definitely” (p = 0.216).
Table 7.
Self-perceived level of knowledge and education and training needs compared across experienced and no experienced dysphagia-related professionals a (n = 209).
3.3. Relevant Dysphagia Thematic Areas and Preferences for Learning Methodologies
Figure 2 presents the perceived relevance of different dysphagia thematic areas among all participants. “Identification & Treatment” was considered relevant by 63% of respondents, while the remaining three areas (“Care & Feeding,” “Diet & Nutrition,” and “Food Preparation”) were selected by approximately 50% each. Only in the area “Identification & Treatment” did people from Group non-P find that they needed more knowledge (72%) than professionals (58%) (p = 0.002). Interest was similar for the remaining areas, with response percentages between 47% and 53%.
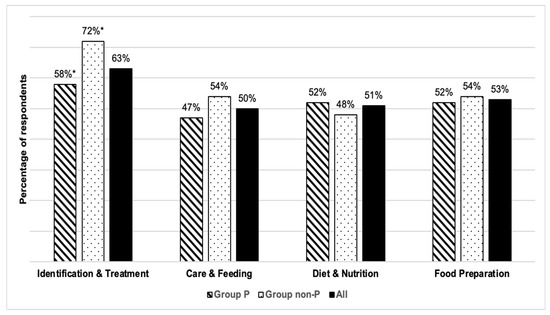
Figure 2.
Relevant dysphagia thematic areas according to survey participants. Note: * Statistically different results, p-value = 0.002, by Fisher’s exact test.
Table 8 and Table 9 display the perceived relevance of dysphagia thematic areas for Group P and Group non-P, respectively. Only Group P displayed statistically significant intra-group differences in interest in the different areas (p < 0.001 in all cases). “Identification & Treatment” was chosen more frequently by SLPs (92%) and healthcare specialists (72%) than by D-Ns (30%). On the other hand, D-Ns were those who expressed the greatest interest in “Care & Feeding” (68%), compared to healthcare specialists (28%) and university lecturers (29%), who expressed less interest. D-Ns were those who expressed a greater degree of preference for the topic “Diet & Nutrition” (86%), whereas healthcare specialists and SLPs selected that option less frequently (35% and 20%, respectively). Once again, D-Ns were the ones with the highest interest in “Food Preparation” (93%) as compared to other health professionals, such as nursing specialists (41%) and healthcare specialists (21%).
Table 8.
Relevant dysphagia thematic areas for dysphagia-related professionals (Group P) (n = 297).
Table 9.
Relevant dysphagia thematic areas for dysphagia-related non-professionals (Group non-P) (n = 166).
Concerning what would be regarded as an acceptable duration of a possible learning program, most participants expressed a preference for short-term training learning courses: 76% favored the option of a course lasting less than 20 h (Figure 3).
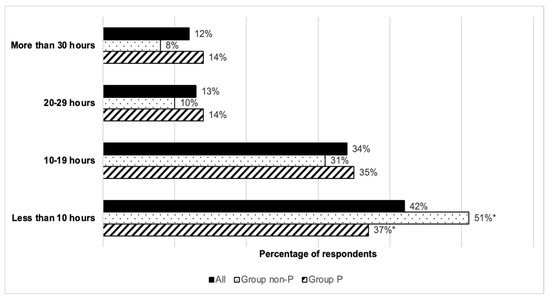
Figure 3.
Preferences regarding the length of the learning courses. Note: * Statistically different results, p-value = 0.030, by Fisher’s exact test.
This was especially evident among the members of Group non-P, in which significant differences could be observed compared to Group P in an expressed preference for training lasting less than 10 h (p = 0.030).
As depicted in Figure 4, the preferred answers to the question “What learning resources would be most effective for you?” were the following: short explanatory videos (75%), practical exercises (55%), the use of images, graphics and illustrations (48%), PowerPoint presentations (37%).
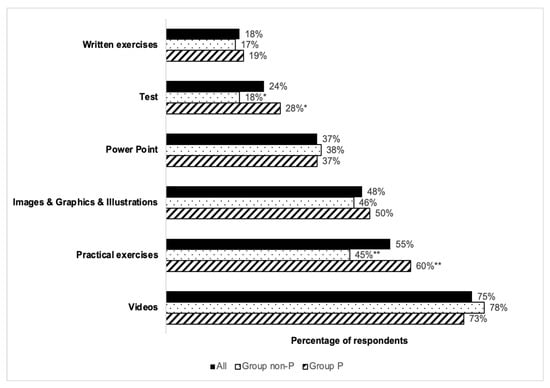
Figure 4.
Preferences regarding the educational resources to be used in learning courses. Note: Statistically different results, * p-value = 0.013 and ** p-value = 0.003, by Fisher’s exact test.
Less popular choices, selected by fewer than 25% of participants, included evaluation tests and written exercises. A comparison of responses between the two surveyed groups revealed statistically significant differences only for practical exercises (p = 0.003) and the use of tests (p = 0.013). In both instances, a higher percentage of respondents in Group non-P opted for each of those respective options.
4. Discussion
This observational, cross-sectional quantitative study aimed to provide a comprehensive overview of the current self-perceived knowledge and learning needs among two multidisciplinary groups—professionals (Group P) and non-professionals (Group non-P)—based on participants’ self-perceptions rather than objective performance measures. The inclusion of healthcare and non-healthcare professionals, as well as patients, relatives, and caregivers, reflects the complexity of dysphagia management. Both groups were predominantly female, consistent with the gender distribution reported in prior studies on health professionals and caregivers [47].
In Group non-P, most participants rated their knowledge as poor or very poor, and 81% reported no prior training. This result aligns with previous research indicating that insufficient caregiver knowledge can hinder adherence to dietary recommendations [48,49,50] and increase perceived burden [51]. Education is valued by caregivers, who often report that improved understanding of dysphagia reduces stress and improves their ability to provide effective support [51,52]. While studies directly exploring patients’ self-perceived knowledge are scarce, findings in individuals with Parkinson’s disease or neuromuscular disorders show that patients and their families often wish to learn more about dysphagia and its treatment [36,53].
In contrast, most professionals in Group P rated their knowledge as good or excellent, although this varied significantly by profession, with D-Ns reporting the highest scores. These differences likely reflect disparities in access to training, professional responsibilities, and country-specific practices [54]. Notably, despite these higher ratings, many professionals—especially D-Ns and nurses—expressed a strong desire for further education. This apparent contradiction suggests that self-reported “good” knowledge may reflect confidence in basic concepts, but not necessarily readiness for complex, real-world clinical scenarios. Similar patterns have been reported in other settings, where professionals acknowledge training gaps despite high self-assessments [4,16,18,20,23,55]. Given the exploratory design of the present study, it was not possible to identify predictors of these differences through multivariate analysis; however, this represents a relevant direction for future research. Recent international evidence further supports this interpretation: the TEAMS survey found that healthcare professionals across multiple countries frequently overestimate their competence in malnutrition and dysphagia management, while still identifying substantial needs for targeted education [25].
Educational needs in Group P were closely linked to professional roles: SLPs and healthcare specialists prioritized “Identification & Treatment,” whereas D-Ns showed greater interest in diet, nutrition, and food adaptation topics. Nurses expressed interest in all areas, reflecting their broad responsibilities in dysphagia care [16,17,24]. In Group non-P, “Identification & Treatment” also emerged as the top priority, followed by diet-related and food preparation topics. This likely reflects a desire to better recognize symptoms, understand the condition, and improve day-to-day management. These findings are consistent with reviews noting insufficient nutritional knowledge among caregivers and the general public [56].
A key finding is that both groups, regardless of self-perceived knowledge level, expressed a clear need for further education and training. This indicates that the decision to seek training is influenced not only by awareness of knowledge gaps, but also by recognition of the complexity of dysphagia management and the need for up-to-date skills. Previous studies support the importance of continuous professional development and tailored education for both healthcare and non-healthcare participants in dysphagia care [16,20,23,57]. The role of caregivers, family members, and acquaintances in early recognition and daily management of dysphagia is crucial; however, this collective often faces significant challenges due to limited knowledge and insufficient training [31,32].
The literature on dysphagia education for non-healthcare professionals—such as chefs, catering managers, and food technologists—remains limited; however, these roles are essential for implementing safe dietary modifications. Studies in the United States have found significant knowledge gaps in food service workers and trainees regarding dysphagia and texture-modified diets [27,58]. Recent advances in dysphagia research, including rheological analysis of modified foods and the implementation of standardized texture levels [26,59,60,61], reinforce the need for targeted education that spans clinical and food science disciplines. Interventions involving food service staff, nurses, and healthcare assistants have shown positive impacts on knowledge and compliance with texture-modified diets [62], but such opportunities are far less available for non-healthcare workers [20,29].
Regarding training formats, our results are consistent with evidence that suggests engagement, interactivity, and concise content are crucial for uptake [28,63]. Consequently, these learning needs could be addressed through technology-enhanced educational interventions. Digital health technologies, including e-learning platforms, mobile health applications, and simulation-based training tools, offer accessible, flexible, and scalable solutions for delivering dysphagia education to diverse stakeholder groups [64]. For healthcare professionals, online continuing education modules and virtual simulation tools provide practice-based learning without time and location constraints [65]. For patients and caregivers, mobile applications and web-based resources could offer practical guidance on safe feeding strategies, texture-modified diets, and symptom recognition in accessible formats [66]. In summary, well-designed digital tools incorporating interactive technologies—such as artificial intelligence-driven personalization, telemonitoring, or Internet of Things-based feedback systems—could further enhance educational delivery and patient management [64]. However, the design and implementation of such technology-based interventions must be grounded in adult learning principles [67] and rigorously evaluated to ensure effectiveness across different user groups and contexts [68].
Limitations and Future Research
This study’s strengths include the variety of profiles of participants obtained thanks to the recruitment methodology, which allowed for comparisons between professional and non-professional groups and across different professional roles. However, the use of a convenience and snowball sampling strategy resulted in unequal representation across participating countries, with a predominance of respondents from Spain. Although this method does not allow for calculating an exact response rate, it was considered appropriate to reach a wide profile of stakeholders. Differences between professional groups observed in this study may reflect variations in access to training, professional responsibilities, and contextual factors among countries. Nevertheless, due to sample size and exploratory design, country-level comparisons and multivariate analyses to identify predictors were not feasible. Future studies with larger and more homogeneous samples are warranted to identify potential predictors of dysphagia-related knowledge and training needs, as well as to explore international variability in educational priorities.
Self-reported measures, which are widely used in exploratory studies [40], may be influenced by recall or social desirability bias, and perceived knowledge may not accurately reflect actual competence. Future research should use validated knowledge assessment tools (e.g., KAP or KAB frameworks) and objective quizzes in combination with consensus methods such as Delphi studies to identify priority topics, optimal learning modalities, and appropriate competence assessment tools for each group.
5. Conclusions
This international observational cross-sectional study reveals that both professionals and non-professionals involved in dysphagia management express a strong need for further learning, despite marked differences in self-perceived knowledge levels. Among professionals, self-reported “good” knowledge often coexists with recognition of the need for advanced and updated skills, whereas among non-professionals, limited baseline knowledge drives the desire for fundamental understanding of the condition and how to manage day-to-day care. Educational and training priorities vary significantly across professional roles: speech and language pathologists and healthcare specialists emphasize “Identification & Treatment,” dietitians and nutritionists focus on “Diet & Nutrition” and “Food Preparation,” while nurses show interest across all areas. In the non-professional group, interest was consistently high across themes, particularly for “Identification & Treatment”, highlighting the need for foundational competence and confidence in recognizing and managing dysphagia. These findings underscore the importance of developing tailored and inclusive learning programs that address role-specific competencies while incorporating accessible and engaging formats. Short, visually rich, and interactive e-learning modules may be particularly effective for enhancing engagement and retention. Incorporating emerging digital and assistive technologies could further enhance these programs, ensuring effective dissemination, sustained engagement, and translation into improved dysphagia care and quality of life. Additionally, as discussed, future studies with larger and more balanced samples across countries are warranted to identify predictors of dysphagia knowledge and to support cross-cultural comparisons, thereby refining educational strategies at the European level.
Author Contributions
Conceptualization, S.R., A.F.-M. and T.S.; methodology, S.R., A.C.C., V.B., A.F.-M. and T.S.; formal analysis, S.R., A.F.-M. and T.S.; data curation, S.R., A.F.-M. and T.S.; writing—original draft preparation, S.R. and T.S.; writing—review and editing, S.R., A.F.-M. and T.S.; project administration, A.F.-M. All authors have read and agreed to the published version of the manuscript.
Funding
The present work was co-funded by the European project INDEED (2020-1-ES01-KA204-083288) founded within the Erasmus+ call.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to its design as an anonymous online survey that did not collect personal identifiers or sensitive data and posed minimal risk to participants, in accordance with the legislation applicable in Spain (General Data Protection Regulation – GDPR, and Organic Law 3/2018 on Personal Data Protection and Guarantee of Digital Rights).
Informed Consent Statement
Participants were informed, on the Google Forms landing page, about the voluntary and anonymous nature of the study; completion of the survey was taken as an indication of informed consent.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. All data relevant to the analysis are already included within the manuscript, while the raw files are not publicly distributed due to format limitations.
Acknowledgments
The authors would like to thank all members of the INDEED consortium for their participation in the collection of the survey data: CADIS-HUESCA (España), Governorship of Kocaeli–Bureau for EU and Foreign Affairs (Turkey), IDEC S.A. (Greece), Kaunas University of Technology (Lithuania) and Universidad de Zaragoza (España). We would also like to thank all the participants, professionals and non-professionals, who voluntarily responded to the survey and collaborated in its dissemination. ChatGPT (GPT-5, OpenAI’s advanced language model) was used to assist with writing and stylistic improvement of this manuscript. The authors critically reviewed, edited, and validated all generated content. The tool was not used to generate unverified scientific content. The authors assume complete and final responsibility for the accuracy, integrity, originality, and validity of all content in the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Rajati, F.; Ahmadi, N.; Naghibzadeh, Z.A.; Kazeminia, M. The global prevalence of oropharyngeal dysphagia in different populations: A systematic review and meta-analysis. J. Transl. Med. 2022, 20, 175. [Google Scholar] [CrossRef] [PubMed]
- Aghaz, A.; Ghelichi, L.; Shahriyari, A.; Noori, S.; Banari, A. The Prevalence of Dysphagia in Parkinson’s Disease: A Systematic Review and Meta-Analysis. J. Iran Med. Counc. 2024, 7, 414–429. [Google Scholar] [CrossRef]
- Mirmosayyeb, O.; Ebrahimi, N.; Shekarian, A.; Afshari-Safavi, A.; Shaygannejad, V.; Barzegar, M.; Bagherieh, S. Prevalence of dysphagia in patients with multiple sclerosis: A systematic review and meta-analysis. J. Clin. Neurosci. 2023, 108, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Gu, H.; Ren, D. Prevalence and Risk Factors of Poststroke Dysphagia: A Meta-Analysis. Cerebrovasc. Dis. 2025, 54, 236–259. [Google Scholar] [CrossRef]
- Kuhn, M.A.; Gillespie, M.B.; Ishman, S.L.; Ishii, L.E.; Brody, R.; Cohen, E.; Dhar, S.I.; Hutcheson, K.; Jefferson, G.; Johnson, F.; et al. Expert Consensus Statement: Management of Dysphagia in Head and Neck Cancer Patients. Otolaryngol. Head Neck Surg. 2023, 168, 571–592. [Google Scholar] [CrossRef]
- Rivelsrud, M.C.; Hartelius, L.; Bergström, L.; Løvstad, M.; Speyer, R. Prevalence of Oropharyngeal Dysphagia in Adults in Different Healthcare Settings: A Systematic Review and Meta-analyses. Dysphagia 2023, 38, 76–121. [Google Scholar] [CrossRef]
- Roberts, H.; Lambert, K.; Walton, K. The Prevalence of Dysphagia in Individuals Living in Residential Aged Care Facilities: A Systematic Review and Meta-Analysis. Healthcare 2024, 12, 649. [Google Scholar] [CrossRef]
- McGinnis, C.M.; Homan, K.; Solomon, M.; Taylor, J.; Staebell, K.; Erger, D.; Raut, N. Dysphagia: Interprofessional Management, Impact, and Patient-Centered Care. Nutr. Clin. Pract. 2019, 34, 80–95. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Júnior, H.J.; Álvarez-Bustos, A.; Pérez Ramírez, C.; Russo, A.; Rodriguez-Mañas, L.; Landi, F.; Marzetti, E. Exploring the Associations Between Dysphagia and Health-Related Outcomes in Older Adults: Results from the ilSirente Study. Nutrients 2025, 17, 2149. [Google Scholar] [CrossRef]
- Yang, S.; Park, J.W.; Min, K.; Lee, Y.S.; Song, Y.J.; Choi, S.H.; Choi, K.H. Clinical Practice Guidelines for Oropharyngeal Dysphagia. Ann. Rehabil. Med. 2023, 47 (Suppl. S1), S1–S26. [Google Scholar] [CrossRef]
- Carnaby, G.D.; Harenberg, L. What is “usual care” in dysphagia rehabilitation: A survey of USA dysphagia practice patterns. Dysphagia 2013, 28, 567–574. [Google Scholar] [CrossRef]
- Dumican, M.; Thijs, Z.; Harper, K. Clinical practice patterns of speech-language pathologists for screening and identifying dysphagia. Int. J. Lang. Commun. Disord. 2023, 58, 2062–2076. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Ikeda, R.; Suzuki, J.; Hirano-Kawamoto, A.; Kamakura, Y.; Fujiu-Kurachi, M.; Katori, Y. Questionnaire survey on nurses and speech therapists regarding dysphagia rehabilitation in Japan. Auris. Nasus. Larynx 2021, 48, 241–247. [Google Scholar] [CrossRef]
- Moore, J.L.; Rosseland, I.; Nordvik, J.E.; Glittum, J.; Halvorsen, J.; Henderson, C.E.; Speyer, R. Identification of a know-do gap: An observational study of the assessment and treatment of dysphagia during inpatient stroke rehabilitation in primary healthcare in Norway. Top Stroke Rehabil. 2024, 31, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Rumbach, A.; Coombes, C.; Doeltgen, S. A Survey of Australian Dysphagia Practice Patterns. Dysphagia 2018, 33, 216–226. [Google Scholar] [CrossRef]
- Engh, M.C.N.; Speyer, R. Management of Dysphagia in Nursing Homes: A National Survey. Dysphagia 2022, 37, 266–276. [Google Scholar] [CrossRef]
- Olímpio, P.B.; Pereira, A.S.; Bettencourt, F.A.; Machado, S.P.G.; Oliveira, I.J. Nurses’ knowledge regarding dysphagia: A cross-sectional study. Rev. Cient. Soc. Esp. Enferm. Neurol. 2023, in press. [Google Scholar] [CrossRef]
- Farpour, S.; Farpour, H.R.; Smithard, D.; Kardeh, B.; Ghazaei, F.; Zafarghasempour, M. Dysphagia Management in Iran: Knowledge, Attitude and Practice of Healthcare Providers. Dysphagia 2019, 34, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Pownall, S.; Barnett, E.; Skilbeck, J.; Jimenez-Aranda, A.; Fowler-Davis, S. The Development of a Digital Dysphagia Guide with Care Homes: Co-Production and Evaluation of a Nutrition Support Tool. Geriatrics 2019, 4, 48. [Google Scholar] [CrossRef]
- Speyer, R.; Cordier, R.; Farneti, D.; Nascimento, W.; Pilz, W.; Verin, E.; Woisard, V. White Paper by the European Society for Swallowing Disorders: Screening and Non-instrumental Assessment for Dysphagia in Adults. Dysphagia 2022, 37, 333–349. [Google Scholar] [CrossRef]
- Van Snippenburg, W.; Kröner, A.; Flim, M.; Hofhuis, J.; Buise, M.; Hemler, R.; Spronk, P. Awareness and Management of Dysphagia in Dutch Intensive Care Units: A Nationwide Survey. Dysphagia 2019, 34, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Spronk, P.E.; Spronk, L.E.J.; Egerod, I.; McGaughey, J.; McRae, J.; Rose, L.; Brodsky, M.B. DICE study investigators. Dysphagia in Intensive Care Evaluation (DICE): An International Cross-Sectional Survey. Dysphagia 2022, 37, 1451–1460. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.R.; Wei, J.Y.; Zhang, X.M. A multicenter cross-sectional survey of the knowledge, attitudes, and practices of geriatric nurses regarding dysphagia care. Ann. Palliat. Med. 2022, 11, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Zugasti Murillo, A.; Gonzalo Montesinos, I.; Cancer Minchot, E.; Botella Romero, F. Hospital management of the patient with dysphagia. Survey and recommendations of SEEN nutrition area. Endocrinol. Diabetes Nutr. (Engl. Ed.) 2023, 70 (Suppl. 3), 1–9. [Google Scholar] [CrossRef]
- Cheng, I.; Rommel, N.; Duchac, S.; Regan, J.; Speyer, R.; Dziewas, R. Understanding health care professionals’ knowledge and practice regarding malnutrition and dysphagia: Insights from Targeted Education to Address Malnutrition and Swallowing disorders (TEAMS) international survey. Nutrition 2025, 139, 112858. [Google Scholar] [CrossRef]
- Giura, L.; Urtasun, L.; Belarra, A.; Ansorena, D.; Astiasarán, I. Exploring Tools for Designing Dysphagia-Friendly Foods: A Review. Foods 2021, 10, 1334. [Google Scholar] [CrossRef]
- Broz, C.C. Healthcare foodservice workers’ knowledge of the dysphagia diet. Nutr. Food Sci. 2012, 42, 339–346. [Google Scholar] [CrossRef]
- Fitzgerald, C.; Pagnucci, N.; Kearns, T.; Hallissy, M.; Walsh, N.; Kelly, C.; Killeen, C.; White, M.; Aleo, G. The experience and attitudes of long-term care workers with teaching and learning modalities for the delivery of continuing professional development activities: A mixed-methods study. Nurse Educ. Pract. 2023, 72, 103774. [Google Scholar] [CrossRef]
- Ghaddar, Z.; Matar, N.; Noujaim, J.; Diep, A.N.; Tohmé, A.; Pétré, B. Consensus on the Objectives of an Educational Intervention for Patients with Oropharyngeal Dysphagia and Their Informal Caregivers: A Delphi Study. Patient Prefer. Adherence 2022, 16, 1511–1524. [Google Scholar] [CrossRef]
- Park, Y.; Oh, S.; Chang, H.; Bang, H.L. Effects of the Evidence-Based Nursing Care Algorithm of Dysphagia for Nursing Home Residents. J. Gerontol. Nurs. 2015, 41, 30–39. [Google Scholar] [CrossRef]
- Demetriou, M.; Tziirkalli, D.; Georgiou, A.M. Caregivers’ Knowledge and Experiences in Recognizing and Managing Dysphagia in Patients with Myopathy. Clin. Pract. 2025, 15, 61. [Google Scholar] [CrossRef] [PubMed]
- Ninfa, A.; Morandi, G.; Schindler, A.; Fave, A.D. The Daily Experience of Family Members Caring for Persons With Chronic Oropharyngeal Dysphagia: A Qualitative Investigation. Int. J. Lang. Commun. Disord. 2025, 60, e70094. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.; Bryant, L.; Hemsley, B. ‘I only eat because I have to-to live’: The impacts of dysphagia on quality of life from the perspectives of people with dysphagia, supporters of people with dysphagia and allied health professionals. Int. J. Lang. Commun. Disord. 2024, 59, 1966–1980. [Google Scholar] [CrossRef]
- Steiner, S.M.; Slavych, B.K.; Zraick, R.I. Assessment of Online Patient Education Material About Dysphagia. Dysphagia 2023, 38, 990–1000. [Google Scholar] [CrossRef]
- Bartlett, R.S.; Walters, A.S.; Stewart, R.S.; Wayment, H.A. Perceptions of Dysphagia Evaluation and Treatment Among Individuals with Parkinson’s Disease. Dysphagia 2024, 40, 248–262. [Google Scholar] [CrossRef]
- Gilheaney, Ó.; Hussey, J.; McTiernan, K. The lived experiences of oropharyngeal dysphagia in adults living with fibromyalgia. Health Expect. 2024, 27, e13932. [Google Scholar] [CrossRef]
- Molfenter, S.M.; Jones-Rastelli, R.B.; Barfield, A.; Cooks, D.; Crossman, C.; Jackson, K.; Price, D.; Robinson, J.C.; Johnson, A.M. Assessing Public Awareness and Understanding of Dysphagia: A Representative Survey of US Adults. Dysphagia 2025, 40, 1316–1324. [Google Scholar] [CrossRef]
- Neves, R.N.; Matos, M.A.; Carvalho, I.P. Communicating Risks and Food Procedures through a Visual Poster for Caregivers of Patients with Dysphagia in Inpatient Care: Usability and Impact. Healthcare 2024, 12, 148. [Google Scholar] [CrossRef] [PubMed]
- Ielo, A.; De Cola, M.C.; Corallo, F.; D’Aleo, G.; Mento, A.; Cardile, D.; Cappadona, I.; Pagano, M.; Bramanti, P.; Ciurleo, R. Improving Knowledge of Audit and Feedback among Health Care Professionals in Sicily. Healthcare 2023, 11, 1987. [Google Scholar] [CrossRef] [PubMed]
- Zota, D.; Diamantis, D.V.; Katsas, K.; Karnaki, P.; Tsiampalis, T.; Sakowski, P.; Christophi, C.A.; Ioannidou, E.; Darias-Curvo, S.; Batury, V.-L.; et al. Essential Skills for Health Communication, Barriers, Facilitators and the Need for Training: Perceptions of Healthcare Professionals from Seven European Countries. Healthcare 2023, 11, 2058. [Google Scholar] [CrossRef]
- Thang, C.K.; Guerrero, A.D.; Garell, C.L.; Leader, J.K.; Lee, E.; Ziehl, K.; Carpenter, C.L.; Boyce, S.; Slusser, W. Impact of a Teaching Kitchen Curriculum for Health Professional Trainees in Nutrition Knowledge, Confidence, and Skills to Advance Obesity Prevention and Management in Clinical Practice. Nutrients 2023, 15, 4240. [Google Scholar] [CrossRef]
- Kim, M.; Kim, J.; Lee, Y.; Kim, H.; Lee, S.-E.; Choi, S.H.; Nam, S.I.; You, H. Analysis of Stakeholder Requirements for the Development of Swallowing Health Management Services. Appl. Sci. 2024, 14, 3596. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef]
- Eysenbach, G. Improving the Quality of Web Surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Eremenco, S.L.; Cella, D.; Arnold, B.J. A comprehensive method for the translation and cross-cultural validation of health status questionnaires. Eval. Health Prof. 2005, 28, 212–232. [Google Scholar] [CrossRef]
- Rayhan, R.U.; Zheng, Y.; Uddin, E.; Timbol, C.; Adewuyi, O.; Baraniuk, J.N. Administer and collect medical questionnaires with Google documents: A simple, safe, and free system. Appl. Med. Inform. 2013, 33, 12–21. [Google Scholar]
- Boniol, M.; McIsaac, M.; Xu, L.; Wuliji, T.; Diallo, K.; Campbell, J. Gender Equity in the Health Workforce: Analysis of 104 Countries; Working Paper 1; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Krekeler, B.N.; Broadfoot, C.K.; Johnson, S.; Connor, N.P.; Rogus-Pulia, N. Patient Adherence to Dysphagia Recommendations: A Systematic Review. Dysphagia 2018, 33, 173–184. [Google Scholar] [CrossRef]
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Nagshabandi, B.S.; Zinnershine, L.; Shune, S.E. A Review of Factors Contributing to Adults’ Adherence to Dysphagia Dietary Recommendations Through an Ecological Lens. Am. J. Speech Lang. Pathol. 2023, 32, 341–357. [Google Scholar] [CrossRef] [PubMed]
- Howells, S.R.; Cornwell, P.L.; Ward, E.C.; Kuipers, P. Client perspectives on living with dysphagia in the community. Int. J. Speech Lang. Pathol. 2021, 23, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Yi, Q.; Mao, L.; Li, W.; Shen, F.; Liao, Z.; Huang, H.; Li, L. The perceptions and experiences of caregivers of patients with dysphagia: A qualitative meta-synthesis. Nurs. Open. 2024, 11, e2223. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.; Stone-Ghariani, A.; Quezada, G.; Banks, D.; Rose, F.; Knight, W.; Newman, J.; Newman, W.; Anderson, P.; Smith, C. Living with Dysphagia: A Survey Exploring the Experiences of Adults Living with Neuromuscular Disease and their Caregivers in the United Kingdom. J. Neuromuscul. Dis. 2024, 11, 389–410. [Google Scholar] [CrossRef] [PubMed]
- Rivelsrud, M.C.; Hartelius, L.; Speyer, R.; Løvstad, M. Qualifications, professional roles and service practices of nurses, occupational therapists and speech-language pathologists in the management of adults with oropharyngeal dysphagia: A Nordic survey. Logoped Phoniatr. Vocol. 2024, 49, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Audag, N.; Toussaint, M.; Liistro, G.; Vandervelde, L.; Cugy, E.; Reychler, G. European Survey: Dysphagia Management in Patients with Neuromuscular Diseases. Dysphagia 2022, 37, 1279–1287. [Google Scholar] [CrossRef] [PubMed]
- Livne, N. Need for nutrition education in health professional programs: A review of the literature. Internet J. Allied Health Sci. Pract. 2019, 17, 5. [Google Scholar] [CrossRef]
- McHutchion, L.D.; Pringle, J.M.; Tran, M.N.; Ostevik, A.V.; Constantinescu, G. A survey of public awareness of dysphagia. Int. J. Speech Lang. Pathol. 2021, 23, 614–621. [Google Scholar] [CrossRef]
- Broz, C.C.; Hammond, R.K. Dysphagia. Education needs assessment for future health-care foodservice employees. Nutr. Food Sci. 2014, 44, 407–413. [Google Scholar] [CrossRef]
- Cichero, J.A.; Lam, P.; Steele, C.M.; Hanson, B.; Chen, J.; Dantas, R.O.; Stanschus, S. Development of International Terminology and Definitions for Texture-Modified Foods and Thickened Fluids Used in Dysphagia Management: The IDDSI Framework. Dysphagia 2017, 32, 293–314. [Google Scholar] [CrossRef]
- Cichero, J.A.Y. Evaluating chewing function: Expanding the dysphagia field using food oral processing and the IDDSI framework. J. Texture Stud. 2020, 51, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Hadde, E.K.; Nicholson, T.M.; Cichero, J.A.Y. Evaluation of Thickened Fluids Used in Dysphagia Management Using Extensional Rheology. Dysphagia 2020, 35, 242–252. [Google Scholar] [CrossRef]
- Wu, X.S.; Miles, A.; Braakhuis, A. An Evaluation of Texture-Modified Diets Compliant with the International Dysphagia Diet Standardization Initiative in Aged-Care Facilities Using the Consolidated Framework for Implementation Research. Dysphagia 2022, 37, 1314–1325. [Google Scholar] [CrossRef]
- Walter, J.K.; Terry, L.M. Factors influencing nurses’ engagement with CPD activities: A systematic review. Br. J. Nurs. 2021, 30, 60–68. [Google Scholar] [CrossRef]
- Borges do Nascimento, I.J.; Abdulazeem, H.M.; Vasanthan, L.T.; Martinez, E.Z.; Zucoloto, M.L.; Østengaard, L.; Azzopardi-Muscat, N.; Zapata, T.; Novillo-Ortiz, D. The global effect of digital health technologies on health workers’ competencies and health workplace: An umbrella review of systematic reviews and lexical-based and sentence-based meta-analysis. Lancet Digit Health 2023, 5, e534–e544. [Google Scholar] [CrossRef] [PubMed]
- Chaker, R.; Hajj-Hassan, M.; Ozanne, S. The Effects of Online Continuing Education for Healthcare Professionals: A Systematic Scoping Review. Open Educ. Stud. 2024, 6, 20220226. [Google Scholar] [CrossRef]
- Kelley, M.M.; Powell, T.; Camara, D.; Shah, N.; Norton, J.M.; Deitelzweig, C.; Vaidy, N.; Hsiao, C.J.; Wang, J.; Bierman, A.S. Mobile Health Apps, Family Caregivers, and Care Planning: Scoping Review. J. Med. Internet Res. 2024, 26, e46108. [Google Scholar] [CrossRef] [PubMed]
- St. Clair, R. Andragogy: Past and present potential. New Dir. Adult Contin. Educ. 2024, 184, 7–13. [Google Scholar] [CrossRef]
- Van Haastrecht, M.; Haas, M.; Brinkhuis, M.; Spruit, M. Understanding validity criteria in technology-enhanced learning: A systematic literature review. Comput. Educ. 2024, 220, 105128. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).