Abstract
Leisure time physical activity (LTPA) plays a vital role in preventing and managing chronic diseases in people with disabilities (PWD). Using virtual reality (VR) can help people feel more comfortable and confident about LTPA. The aim of this study is to identify research focusing on VR, LTPA, and people with motor disabilities. Methods: A scoping review was completed by searching MEDLINE, CINAHL, SportDiscuss, Academic Search Premier, and Web of Science in June 2024 (updated July 2025). Eighteen studies were included. Results: Most studies examined cycling (56%) and targeted post-stroke (28%) and spinal cord injury (22%) populations. VR interventions showed potential to improve various domains such as functional mobility, motor function, and psychosocial well-being. A total of 35 distinct outcome measures were identified, categorized into motor/balance, physiological, psychological, user experience, and performance themes. Conclusions: While most VR interventions used LTPA primarily as a therapeutic tool, some were designed to teach sport-specific skills to facilitate participation outside the clinical setting. Future research should examine how VR can aid rehabilitation and prepare PWD for sustained engagement in LTPA.
1. Introduction
In 2022, 27% of Canadians aged 15 and over, or 8 million people, reported having at least one disability; 39% of those disabilities are mobility-related [1]. Although population-level data on physical activity among people with disabilities (PWD) in high-income countries are scarce, the promotion of moderate levels of physical activity among PWD is an important public health goal [2]. Physical activity is broadly defined as any bodily movement produced by skeletal muscles that results in energy expenditure [3,4,5] and encompasses various activities, including occupational, sports, household, and recreational pursuits [3]. Since the notion of physical activity is too broad, this scoping review focuses on leisure-time physical activity (LTPA), adapted from Howley’s [6] definition. This term includes all forms of aerobic activities, structured endurance exercise programs, resistance-training programs, and sports, while excluding the notions of gait, balance, quality of life and household tasks. According to the World Health Organization (WHO), regular physical activity helps prevent and manage noncommunicable diseases such as heart disease, stroke, diabetes and many cancers. Physical activity also helps people prevent hypertension, maintain a healthy body weight and improve their mental health, quality of life and well-being [7]. Moreover, the global estimate of the cost of physical inactivity to public health care systems between 2020 and 2030 is about US$300 billion (approximately US$27 billion per year) if levels of physical activity are not increased [7]. In Canada, 16% to 64% of PWD are less likely than the general population to meet the WHO’s guidelines of at least 150 min/week of moderate-intensity physical activity, 75 min/week of vigorous-intensity physical activity, or an equivalent combination of moderate and vigorous physical activity [2,8].
The most frequently mentioned emotional and psychological barriers to physical activity for PWD is the perception that fitness and recreation facilities constitute unfriendly environments [9]. One facilitator may be to allow PWDs to “test the water,” that is, try the facility and determine their level of comfort before joining [9]. Specific to outdoor LTPA for adults with mobility disabilities, the most common facilitators are psychological, related to individuals’ emotions and personality types, self-perceptions and attitudes, and the perceived benefits of outdoor activity. Challenge-seeking personalities and positive attitudes toward outdoor LTPA and toward themselves (e.g., self-confidence) are also identified as facilitators [10]. Meanwhile, the Ministry of Education of Québec (Canada) identified the creation of outdoor discovery and initiation activities for PWD and their families as an important facilitator of physical activity for PWD [11].
Several studies have demonstrated that virtual reality (VR) can have a positive influence on various physical and psychological outcomes. For example, VR has been shown to increase moderate- and vigorous-intensity activity to levels associated with accrued benefits for PWD [12,13]. Other studies conducted with participants without disabilities have reported similar benefits, such as reduced perceived pain after two 15-min VR exercise sessions [14] and increased intrinsic motivation following a 20-min VR cycling session compared to traditional and non-immersive cycling [15]. VR has also shown promise in the field of rehabilitation. For example, studies have shown moderate evidence of VR’s effectiveness in improving balance and overall motor development in children with cerebral palsy [16,17]. For people with Parkinson’s disease, VR interventions have demonstrated substantial improvements in balance, gait, and motor skills compared to traditional physical therapy [18]. In stroke rehabilitation, VR has shown potential to enhance upper extremity motor function, gait, and balance [19,20]. VR-based rehabilitation appears to be feasible and safe for children with sensorimotor deficits, although higher-quality research is needed [21]. The integration of music along with VR technologies in rehabilitation shows promise for promoting motivation, exercise adherence, and positive emotions [22]. Overall, VR offers potential benefits in neurorehabilitation, but further high-quality studies are required to conclusively establish its effectiveness [23].
Qian et al. [24] conducted a systematic review to synthesize the literature examining the effects of VR exercise on a range of outcomes in various disabled populations. Their findings suggest that VR exercise has the potential to exert a more positive impact on individuals’ physiological, psychological, and rehabilitative outcomes than traditional exercise. However, no reviews had been conducted on VR, LTPA and PWD, and more specifically people with motor disability. To address this gap, we approached the use of VR through a conceptual distinction often seen in assistive technology practice: VR can be deployed either (1) as a therapeutic tool aimed at improving body functions and structures, or (2) as an enabling or compensatory tool designed to support participation by allowing individuals to experience or prepare for meaningful activities. This distinction emphasizes the difference between rehabilitation interventions and those that encourage real LTPA participation. Selecting appropriate outcomes is important when developing an intervention using VR to enhance LTPA for PWD. The first steps of an intervention protocol are knowing what to measure, understanding what to test, selecting the right tools and interpreting the results that are already available. To this end, the general purpose of this study was to identify research focusing on VR, LTPA and people with motor disabilities. The specific objectives were to (1) explore VR’s influence on health and psychosocial outcomes, (2) document the outcome measures used to assess VR’s influence, and (3) describe the key components of VR interventions.
2. Materials and Methods
We conducted a scoping review using Arksey and O’Malley’s [25] framework. Our findings are reported according to the scoping review extension of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-ScR) guidelines [26]. The project was registered in the Open Science Framework (OSF #xpfb7).
2.1. Eligibility Criteria
We focused on three concepts: (1) sports, LTPA, or physical activities that included some type of physical effort; (2) diagnoses related to motor disabilities; and (3) research related to VR. Papers were excluded if (1) they were published prior to 2004; (2) they were not in French or English; (3) no physical activities were involved; (4) the participants had mental, visual or hearing disabilities; (5) the topic pertained to gait, balance or treadmill training or to activities of daily living; and (6) the participants were not between 18 and 65 years old. If an article included participants who were both under and over 65, it was included, and the data related to the participants in the relevant age group were extracted. Papers were included if the intervention involved LTPA even if the study evaluated gait, balance or activities of daily living. While this review focuses on LTPA interventions, the literature uses clinical metrics to evaluate leisure-based interventions, such as gait, balance and motor recovery. However, we excluded interventions based solely on conventional rehabilitation exercises (gait, balance, motor function) that did not mention LTPA.
2.2. Literature Sources and Search Strategies
Databases related to rehabilitation, sports and biomedical sciences were used to conduct the literature search: MEDLINE (via Ovid), CINAHL (via Ebsco), Academic Search Premier (via Ebsco), SportDiscuss (via Ebsco) and Web of Science. To ensure comprehensiveness, an initial list of candidate terms (sports and diagnoses) was generated using ChatGPT (May 2024 version, GPT-3.5/GPT-4o model; OpenAI, San Francisco, CA, USA) as a preparatory step. This list was subsequently manually reviewed, refined, and validated by the research team in consultation with a librarian. For VR, we included search terms related to augmented reality, virtual reality, extended reality and mixed reality. The search terms were identified and customized for each database. The final search strategies, including the complete list of keywords used, are fully documented in the Supplementary Table S1. The initial search and data extraction were done by two reviewers (AB and MR) in June 2024. As more than one year had elapsed since the initial search, the databases were queried again in July 2025 to update the review. This update was again performed by two reviewers (AB and AK), applying the same search strategy and eligibility criteria as the initial search. All articles were uploaded to Covidence for screening.
2.3. Article Selection
The study selection process consisted of four stages: (1) identifying relevant articles from the literature, (2) screening the articles by assessing the titles and abstracts according to the criteria, (3) determining the eligibility of the articles by evaluating the full papers against the criteria, and (4) including the articles by reapplying the criteria during data extraction. Following a search of all pertinent databases (identifying), duplicates were automatically eliminated using Covidence software (accessed June 2024; Veritas Health Innovation, Melbourne, Australia). In the subsequent steps (screening, eligibility, and inclusion), two reviewers (AB and MR or AK) carried out the review independently, noted the reasons for exclusion, and then compared their results. Disagreements were resolved by consensus, with a third reviewer intervening to resolve any residual conflicts.
2.4. Charting the Data
Once the articles were appropriately identified, two reviewers (AB and MR or AK) extracted the data using a table containing the following information: authors/year, population, intervention, VR, key findings. The data were then consolidated, and any discrepancies was resolved by discussion between the two reviewers. The Template for Intervention Description and Replication (TIDieR) [27] guided the data extraction. TIDieR is a framework designed to improve the completeness of reports on interventions in research studies. It provides a checklist and guideline to ensure detailed descriptions of interventions, making it easier for others to replicate the studies. Google Gemini was used to revise and optimize the readability of the final manuscript.
3. Results
3.1. General Characteristics of Selected Articles
A total of 37,844 articles were initially imported into Covidence for screening. The PRISMA flowchart and the selection procedure are shown in Figure 1. In total, 24,611 duplicates were identified and removed by Covidence and 16 were eliminated manually. Following title and abstract screening, 13,137 of the resulting 13,217 articles were excluded. The full texts of the remaining 80 records were assessed for eligibility, and 62 were excluded. Thus, a total of 18 studies met the inclusion criteria and were included in the review; 39% of those articles were published in Asia (n = 7), 33% in the United States (n = 6) and 28% in Europe (n = 5). Half of the articles were written in the 2010s and the other half in the 2020s. More than half of the articles (n = 10, 56%) included cycling as the VR intervention. Other LTPA were explored: three studies used sailing (17%), two used canoeing (11%), one used soccer, one used Pilates, and one used boxing (5.5% each). Study designs included seven feasibility, pilot, preliminary, or exploratory studies; six randomized control trials; three usability/development studies; and two studies with a comparative/quasi-experimental design. Sixteen studies employed only quantitative analyses, and two used a mixed-methods design. Most of the participants included in the reviewed articles had had a spinal cord injury or stroke. Five articles (28%) reported on work focusing exclusively on participants with stroke and four (22%) on participants with spinal cord injury. One article included a mixed population of participants with stroke, cancer, spinal fracture, and neurological conditions [28], while two included participants with both spinal cord injury and cerebral palsy [29,30]. The other conditions present in the study samples included Parkinson’s disease, multiple sclerosis, lower limb disorders, motor polyneuropathy, ataxia and hemiparesis.
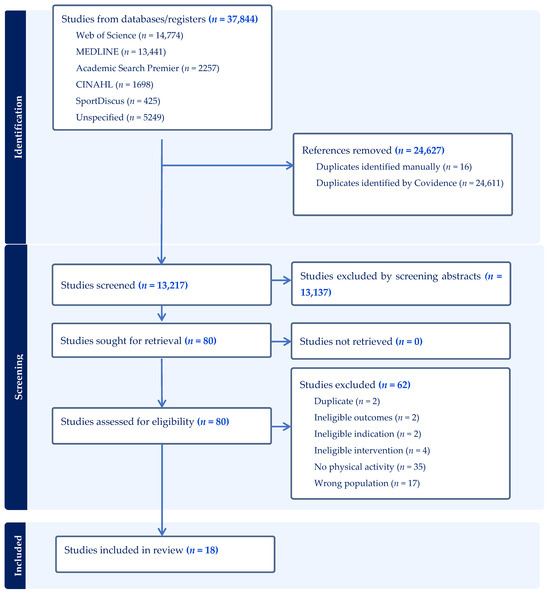
Figure 1.
Flow diagram of the article selection process. The initial search (June 2024) identified 16 eligible studies. An updated search in July 2025, following the same strategy and eligibility criteria, identified two additional studies, bringing the total to 18 included studies.

Table 1.
Data extraction for the selected articles.
Table 1.
Data extraction for the selected articles.
| Author/Year | Population | Study Design | Intervention | VR Components | Outcomes and Key Findings |
|---|---|---|---|---|---|
| Chen et al., 2009 [31] | n = 30, incomplete SCI, mean age 48 y | RCT | VR cycling vs. conventional cycling; single self-paced session | Screen + projector; road scene | ↑ endurance, ↑ calmness, ↓ tension; no cybersickness; HR & RPE no change |
| Deutsch et al., 2013 [32] | n = 5 (1 control), stroke, age 47–65 y | Pilot study | VR augmented cycling, 8 wks, 2×/wk, 20–60 min | LCD screen; feedback on force & HR | Safe (1 dizziness resolved); 100% adherence; ↑ walking endurance, ↑ VO2; high PQ scores |
| Heyn et al., 2014 [33] | n = 6 (SCI, IDD, no disability), mean age 43 y | Pilot study | Mixed-reality exercise, 1 × 60-min session | 3 large monitors; Colorado trail video | ↑ engagement, enjoyment, immersion; motivating environment |
| Gallagher et al., 2015 [34] | n = 8 (older adults, Parkinson’s disease), age 58–79 y | Preliminary study | Cycling with auditory/visual cues & feedback; 14 × 1-min trials | Stationary bike + projector | ↑ pedaling rate with cues/feedback; PD & older adults responsive to visual cues |
| Yin et al., 2016 [35] | n = 9 stroke (6 EG, 3 CG), mean age EG 54 y, CG 61 y | Quasi-experimental | EG: VRCTS cycling 3×/wk, 15 min, 10 sessions + rehab; CG: rehab only | VRCTS device + screen | EG: ↑ pedal force symmetry, ↑ standing balance; CG: no change |
| Lee, 2019 [36] | n = 42 stroke (21 EG, 21 CG), mean age EG 61 y, CG 64 y | RCT | EG: speed-interactive pedaling + therapy, 40 min, 5×/wk, 6 wks; CG: therapy only | Stationary bike + smartphone tracking + projector | EG: ↑ lower limb motor function, ↑ trunk balance, ↑ gait; CG: less improvement |
| Høeg et al., 2023 [28] | n = 11 (stroke, cancer rehab, spinal fracture, others), mean age 60 y | Usability study | Collaborative VR tandem cycling exergame; ~11-min session | Oculus Rift HMD; road loop | High motivation & enjoyment; excellent SUS; low cybersickness |
| Rojo et al., 2023 [37] | n = 38 (18 elderly, 20 LLD), mean age elderly 85 y, LLD 61 y | Usability study | Static pedaling, 2 × 5 min, 1 session | Oculus Quest 2 HMD; “High Flight” env. | High IMI, CEQ, satisfaction; adequate SUS; no cybersickness |
| Rojo et al., 2024 [38] | n = 20 (ataxia, hemiparesis), mean age EG 60 y, CG 59 y | RCT | VR cycling vs. no VR, 3 × 5 min over 1 wk | Oculus Quest 2 HMD | Both groups: ↑ hip/knee ROM; no significant group differences |
| Hasnan et al., 2024 [39] | n = 8 chronic thoracic SCI, mean age 50 y | Comparative study | Indoor VR vs. outdoor FES-assisted arm + leg cycling, 30 min | Large screen; track simulation | Indoor VR: ↑ limb activity & mechanical efficiency; cardioresp. & REP similar; no cybersickness |
| Recio et al., 2013 [40] | n = 3 chronic SCI, mean age 52 y | Pilot study | VR sailing, 1×/wk, 12 wks, 1 h | Vsail-Trainer simulator | ↑ sailing skills; able to sail on water; ↑ quality of life |
| Recio et al., 2024 [41] | n= 20 chronic SCI (13 completed), mean age 45 y | Pilot study | VR sailing, 1×/wk, 12 wks, 1 h; on-water test | Vsail-Trainer simulator | ↑ sailing skills; able to sail adapted boats; mixed QoL & physical outcomes |
| Autry & Anderson, 2022 [29] | n = 7 (SCI, spina bifida, CP), mean age 38 y | Pilot study | VR sailing, 11 wks, ~2 h/wk | VRSS boat + screen | ↑ sailing knowledge & skills (~90%); ↑ confidence; potential for real sailing |
| Lee et al., 2016 [42] | n = 10 subacute stroke, mean age EG 65 y, CG 66 y | RCT | EG: VR canoe paddling 3×/wk, 30 min, 4 wks + rehab; CG: rehab only | Nintendo Wii Sports Resort canoe | EG: ↑ trunk stability, ↑ balance, ↑ UL function; SUS acceptable |
| Lee et al., 2018 [43] | n = 30 subacute stroke, mean age EG 62 y, CG 61 y | RCT | EG: VR canoe paddling 3×/wk, 30 min, 5 wks + rehab; CG: rehab only | Nintendo Wii Sports Resort canoe | EG: ↑ postural balance, ↓ sway, ↑ UL function |
| An & Park, 2022 [44] | n = 40 incomplete SCI, mean age EG 42 y, CG 43 y | RCT | EG: VR soccer 3×/wk, 30 min, 4 wks; CG: seated exercise | HMD (not specified) | EG: ↑ balance, ↓ fall risk, ↑ kick speed; no quadriceps strength change |
| Tacchino et al., 2023 [45] | n = 9 multiple sclerosis, mean age 43 y | Development and usability study | MS-FIT Pilates via Kinect; 30 min/day, ≥5×/wk | Kinect + screen; virtual travel | High usability, enjoyment, satisfaction, acceptance |
| Polechoński et al., 2024 [30] | n = 11 wheelchair users (SCI, CP, spina bifida, neuropathy), mean age 30 y | Pilot study | FitXR VR boxing, 2 × 15 min; with/without 0.5 kg weights | Oculus Quest 2 HMD; immersion 4 | Moderate–vigorous intensity; weights ↑ RPEbut not HR; high satisfaction |
Abbreviations: CEQ = Credibility and expectancy questionnaire; CG = Control Group; CP = Cerebral Palsy; EG = Experimental Group; FES = Functional Electrical Stimulation; HR = heart rate; HMD = Head-Mounted Display; IDD = Intellectual and Developmental Disabilities; IMI = Intrinsic Motivation Inventory; LCD = Liquid Crystal Display; LLD = Lower Limb Disorders; MS-FIT = Microsoft Fit; PQ = Presence Questionnaire; QoL = Quality of Life; RCT = Randomized Controlled Trial; ROM = Range of Motion; RPE = Rate of Perceived Exertion; SCI = Spinal Cord Injury; SUS = System Usability Scale; UL = Upper Limb; VO2 = Volume of Oxygen; VR = Virtual Reality; VRCTS = Virtual Reality-Cycling Training System; VRSS = Virtual Reality Sailing System; Vsail = Virtual Sailing; y = years; ↑ = Increase; ↓ = Decrease.
3.2. Influence of VR on Health and Psychosocial Outcomes
Several of the 18 VR interventions demonstrated positive benefits, such as motor improvement, engagement, motivation and/or psychological well-being (Table 1); only a few reported that some participants felt cybersick. Authors of several studies suggested that VR systems may be used to engage participants in LTPA. More specifically, a VR-Cycling Training System improved bilateral pedal force and standing balance in stroke patients. The symmetry of bilateral pedal force was significantly improved using this system, leading to better performance than in a control group [35]. Game-based VR canoe paddling training, combined with conventional physical rehabilitation programs, led to significantly greater improvement in trunk stability, postural sway, and upper extremity function in patients with subacute stroke [43]. An intervention called Speed-Interactive Pedaling Training, which used a smartphone VR application, was reported to be useful for the functional recovery of lower extremities in stroke patients; it improved their sitting balance, trunk control, and gait [36]. VR rehabilitation was more effective than rehabilitation without VR content for improving balance, gait function, and kick speed in participants recovering from incomplete spinal cord injury [44]. The study by Hasnan et al. [39] compared an outdoor non-VR LTPA session with an indoor VR-assisted session; the indoor VR cycling resulted in greater limb activity and mechanical efficiency. Polechoński et al. [30] examined immersive VR boxing training for wheelchair users with various physical disabilities. They assessed exercise intensity, user experience, and the effect of additional wrist weights, and found that the intervention produced moderate to vigorous physical activity levels; the additional load increased perceived exertion but not heart rate, while user satisfaction and acceptance were high.
Regarding psychological benefits, VR-based rehabilitation therapy demonstrated the capacity to promote calmness and relaxation, improving participants’ mood. Furthermore, it encouraged them to undergo rehabilitation therapy and was helpful in easing their tension, thus benefiting their psychological well-being [31]. VR sailing simulators were an effective means of getting people with spinal injuries sailing, with measurable clinically significant improvements in function, depression, and quality of life [29,41]. Three validated psychological outcomes were used to evaluate presence [32,33,37], motivation [28,37], and arousal [31]. Presence—both a psychological state and a subjective perspective—was reported in three studies and may have contributed to increased involvement; perceived presence was moderate to high in all three. VR positively influenced motivation among people with stroke, cancer rehabilitation, spinal fracture, and lower limb disorder; however, it was not possible to identify the type of motivation. One randomized controlled trial also reported an effect of VR on arousal state, which could influence future participation in LTPA by reducing tension and increasing calmness among people with incomplete low spinal-cord injuries. Qualitative findings from one mixed-methods study reported increased confidence in sailing among eight people with spinal cord injury and cerebral palsy [29].
3.3. Outcome Measurement Tools Used
The assessment tools and the health and psychosocial variables measured by the researchers were categorized in fives themes: motor function and balance assessments, physiological measures, psychological and cognitive measures, user experience measures, and performance measures. The 18 articles used 35 different assessment tools, including questionnaires, physical performance tests, and technological measurements, to evaluate various aspects such as motor function, balance, gait, usability, motivation, and quality of life (Table 2). The most frequently employed assessment tool was the System Usability Scale (SUS) a 10-item questionnaire that measures the perceived usability of a system with Likert scales.
Table 2.
Assessment tools used.
The duration of interventions varied considerably, from very short (1 min) to longer (1.5–2 h per session) (Table 3). The most common duration was 30 min. The frequency of the intervention ranged from once a week to five times a week. The studies were conducted over varying periods, ranging from one week to twelve weeks. The number of sessions ranged from a single session to as many as 30. The study by Deutsch et al. [38] adjusted duration based on individual tolerance, starting with 20 to 30 min and increasing to 60 min. This aligned with recommendations for post-stroke cardiorespiratory fitness training published by the American Heart Association, which range from two to five days a week for 20 to 60 min a session for two to 12 weeks. In the Buddy biking study by Høeg et al. [28], duration was partly determined by participants; two pairs decided to continue the ride once they had completed a lap of the circuit; they went for another lap, resulting in a time of 10.7 (± 3) min. In Chen et al.’s [31] study, exercise duration was determined by when the subject reached 85% of maximum heart rate or needed to stop the test because of fatigue.
Table 3.
Intervention duration and frequency.
3.4. Components of VR Interventions
The 18 studies described the use of various hardware components, software applications, and virtual environments to create interactive, immersive, and engaging VR experiences while processing data and managing the overall experience. Table 4 classifies the hardware and software components of the VR interventions: 56% (n = 10) of the studies used a computer or TV screen, 28% (n = 5) used head-mounted displays (HMDs), and 17% (n = 3) used projectors with a screen. Of the five studies that reported using HMD, three used an Oculus Quest 2, one used an Oculus Rift, and one did not specify the model.
Table 4.
Components of VR intervention.
3.5. Therapeutic Modality vs. Leisure Participation
To better understand how VR is used to engage people in LTPA, we analyzed in more depth the main aims described in the 18 studies included. We assessed whether the LTPA was the core of the intervention, such as learning a new sport or trying to improve participation, or whether it was used just as a therapeutic approach for rehabilitation purposes.
LTPA was used strictly as a therapeutic modality in 10 studies. Cycling, canoeing, soccer and Pilates-based exercises were not used for leisure but to encourage participants to reach rehabilitation goals. The main goals were to improve cardiorespiratory fitness, psychological state, or lower limb motor function. The type of engagement fostered was more about “engaging with therapy” than trying to establish a sustainable, healthy lifestyle based on sports or to increase social participation.
Three studies focused exclusively on technology usability and feasibility. These studies used sports or leisure settings, but their goal was to validate the design of the system, and not to encourage people to be more physically active.
Only five studies positioned LTPA as the central focus, specifically for learning new skills, improving quality of life, or evaluating the intensity of physical exercise in a training context. These were the only studies designed to help participants transition to real-world sports or maintain a long-term active lifestyle.
These findings suggest that, while VR is widely used as therapy and rehabilitation tool, it is rarely used to support ongoing participation in leisure activities.
4. Discussion
4.1. Overview of the Literature
This scoping review successfully mapped the current literature on the use of VR applications for LTPA in individuals with motor disabilities, highlighting the diversity of study designs and outcome measures.
The findings reveal a limited yet expanding body of evidence, primarily centered on cyclical exercise (e.g., cycling, canoeing, sailing) and predominantly targeting post-stroke and spinal cord injury populations. While the overall results report functional and psychosocial improvements, the high degree of methodological heterogeneity—in terms of duration, intensity, technologies, and measurement tools—limits our ability to draw broad, general conclusions. This diversity, however, illustrates a growing interest in VR as a crucial approach to promote motivation, engagement, and the transition between clinical rehabilitation and real-world participation in leisure activities.
4.2. Inconsistency of Outcome Measures
The variety of assessment tools documented highlights a substantial lack of consensus about key indicators. Motor measures (e.g., Fugl-Meyer Assessment, range of motion) dominate, whereas psychosocial, experiential, and ecological assessments are less common. This dominance raises a crucial issue of relevance: the studies mostly measure body function and impairment, while the goal of LTPA interventions should be to target higher-level concepts of activity, participation and quality of life. Few studies effectively combine objective measures (sensors, heart rate) with subjective measures (motivation, presence, satisfaction). This review also noted a serious lack of qualitative data to explore the user experience in depth. Given that VR interventions are inherently multidimensional, their evaluation should reflect this complexity. Furthermore, the lack of long-term follow-up in all the studies included makes it impossible to assess the various interventions’ sustained impact on behavior. Implementing a common assessment framework, such as the International Classification of Functioning, Disability and Health (ICF) [47]—which covers activity, participation, and personal/environmental factors—is a critical step toward standardization. This approach is not merely theoretical: its value for guiding LTPA research in disability has already been shown in a large prospective study that used the ICF framework to identify predictors of LTPA among people with spinal cord injury [48]. This shift in measurement strategy is essential to properly orient future research toward evaluating valuable outcomes that are meaningful for sustained LTPA engagement, moving beyond simple clinical performance.
4.3. Intervention Design and User Involvement
The analysis of intervention design provides crucial insights for future development. Most interventions aimed for a moderate immersion experience (Level 4 out of 6), predominantly utilizing flat-screen monitors rather than HMDs. This trend likely reflects a pragmatic approach to enhance clinical accessibility and limit concerns such as cybersickness. However, studies that did utilize fully immersive HMDs tended to report greater engagement, which aligns with the principle that the level of involvement in an activity is correlated with the level of immersion [49]. In terms of protocol, the studies showed significant variation in intensity, frequency, and total exposure time (ranging from single sessions to multi-week programs). The finding that more frequent, shorter sessions tend to be used in longer programs suggests a focus on consistent, less intensive intervention over time. This protocol aligns with best practices for promoting LTPA in PWD: more frequent but shorter sessions have been shown to be the most effective [2]. Key factors that appeared to promote participant engagement and adherence included the integration of game-like elements, interactive real-time feedback, progressive adjustment of difficulty and the possibility for participants to self-regulate exercise intensity and duration. Despite these positive elements, the review highlights significant gaps: several articles lack detailed descriptions of interventions, and cases of individualized adaptation—taking into account the users’ specific sensory and motor preferences—remain rare. This omission of user involvement represents a critical methodological limitation, as technology-based interventions often fail when usability and user relevance are not prioritized. Frameworks such as Participatory Action Research [50] and Co-design [51] are specifically intended to mitigate this risk by positioning end-users as active partners in the research process. This philosophy of partnership reflects the main focus of the disability rights movement, articulated in the slogan “Nothing about us without us” [52]. This principle asserts the fundamental right of PWD to be included in the creation of any process that impacts their lives, ensuring that their voices and autonomy are central. Such approaches make sure that interventions are developed with users, not simply for them, and integrate their lived experience to address these populations’ complex accessibility, motivational, and sensory needs. Participatory design elements should become central to future research to ensure the long-term accessibility, safety, and transferability of VR interventions for heterogeneous populations.
4.4. Intervention Outcomes
The evidence suggests that VR use can lead to significant motor benefits, such as improved postural stability [36,42,43] and bilateral force symmetry [35]. It can also generate positive psychosocial outcomes, such as reduced tension [31] and increased confidence [40]. However, these positive findings must be viewed with caution because of the various studies’ significant methodological limitations. The predominance of small sample sizes and short durations and the frequent lack of control groups makes it difficult to determine the true effect of these interventions or rule out variability. Furthermore, the conditions under which VR is most beneficial remain unclear. The influence of contextual factors—such as the degree of clinical supervision, the accessibility of the home environment, and the role of social support—was rarely investigated but is critical for real-world implementation. This review found a heavy focus on stroke and spinal cord injury, with a clear shortage of research concerning adolescents, older adults, and individuals with severe motor deficits. Critically, while VR can add value when used as an initiation tool, no study measured its long-term effect on sustained active behaviors, which remains a priority research area [48].
4.5. From Therapy to Participation
A major finding of this scoping review is the clear identification of VR’s dual potential in the context of LTPA. The majority of studies utilized LTPA primarily as a therapeutic tool aimed at functional recovery, rather than as an enabling or compensatory tool to prepare participants for engagement in real-life activities. However, the interventions that focused on activities like sailing, canoeing, and boxing demonstrate that VR can be successfully leveraged to prepare for actual participation in real-world leisure activities. This strategic dual potential—rehabilitative and participatory—positions VR as a powerful catalyst toward autonomy in active leisure. By offering a safe space for exploration, skill development, and confidence building, VR can facilitate the transition from clinical intervention to independent participation. The challenge is still how to overcome structural barriers—such as the cost and accessibility of advanced VR technology—and develop protocols that maximize the transfer of skills and motivation to ensure that active behaviors continue beyond the intervention context.
4.6. Clinical Implications
Despite the potential benefits found in this review, there are still barriers to implementing VR for clinicians who want to use the technology both for rehabilitation purposes and as a tool to implement long-term behavioral changes [53]. The technology itself requires clinicians to choose the right models, invest a substantial amount of money, update the hardware and software regularly, and troubleshoot any malfunctions [54]. Accessibility is another limitation as most commercial VR setups require adaptation to fit the needs of people with motor disabilities [55]. Cybersickness, reported in some studies that used HMDs, can also limit participation [28,32]. The transferability of skills learned in a VR environment to the real world raises the question of the tool’s influence on behavioral changes that could play a role in a sustainable, active lifestyle [56]. For clinicians, the evidence already supports using VR as an effective motivational tool to increase engagement in practice. However, they must remain critical of the gap between clinical performance and community participation and therefore must actively plan how to transfer skills and confidence from the clinical setting to the client’s daily life.
4.7. Limitations
This scoping review has certain limitations inherent to its methodology. First, the search strategy was restricted to articles published in English, which may have excluded relevant data published in other languages. Second, while an exhaustive search was conducted across multiple databases, gray literature was not included in the search strategy. Third, the complexity of our search strategy could limit the replicability of this review. To ensure comprehensive coverage of sports and diagnoses not indexed by MeSH terms, artificial intelligence was utilized to generate exhaustive keyword lists; the list of diagnoses alone was over 12 pages long. While this approach maximized sensitivity, it resulted in a highly complex search string. Nevertheless, the full strategy file is available in Supplementary Table S1 to ensure transparency. Finally, a specific delimitation was applied to focus strictly on “leisure-time physical activity” rather than “physical activity” in the broad sense. Therefore, daily living activities, domestic tasks and occupational or school-based physical activity were excluded.
4.8. Recommendations for Future Research
Based on the gaps identified, this review offers specific guidance for future development. Researchers must move beyond small-scale studies and conduct robust randomized control trials using standardized, ICF-guided outcomes and long-term follow-up to measure behavioral adherence. Furthermore, they must adopt participatory co-design frameworks to ensure that new interventions are relevant for under-represented populations and are built to leverage VR’s dual potential—not just as a therapeutic tool, but as an enabling tool for real-world participation.
5. Conclusions
Our findings highlight the potential of VR to create engaging exercise experiences that lead to promising results in functional mobility, motor function, and psychosocial well-being. Although all the interventions reviewed here took place within rehabilitation contexts, a critical distinction emerged regarding their purpose: while the majority utilized LTPA primarily as a therapeutic modality for functional recovery, a subset of studies successfully employed VR as an enabling tool to teach sport-specific skills (e.g., sailing, canoeing) intended for transfer to real-world participation. This review confirms that VR can play a strategic dual role—serving simultaneously as a rehabilitation treatment and preparation for ongoing engagement in leisure. However, to fully realize its potential, future interventions must move beyond purely clinical metrics and prioritize user-centered designs that explicitly target the transfer of skills and confidence to daily life. These insights provide the rationale for our future work, specifically the design of a VR application dedicated to preparing PWD for sustained, autonomous engagement in LTPA.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/technologies14020137/s1, Table S1: Detailed search strategies for all databases.
Author Contributions
Conceptualization, A.B., P.A. and F.R.; methodology, A.B., P.A., M.G. and F.R.; validation, A.B., M.R. and M.G.; formal analysis, A.B., M.R. and A.K.; investigation, A.B., M.R. and A.K.; data curation, A.B., M.R. and A.K.; writing—original draft preparation, A.B., M.R. and A.K.; writing—review and editing, A.B., M.R., A.K., P.A. and F.R.; supervision, F.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data were created or analyzed in this study. The original contributions presented in the study are included in the article and its Supplementary Materials. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HMD | Head-Mounted Display |
| ICF | International Classification of Functioning, Disability and Health |
| LTPA | Leisure-Time Physical Activity |
| PWD | People with Disabilities |
| TIDieR | Template for Intervention Description and Replication |
| VR | Virtual Reality |
References
- Statistics Canada. Canadian Survey on Disability, 2017 to 2022; Statistics Canada: Ottawa, ON, Canada, 2023.
- Martin Ginis, K.A.; van der Ploeg, H.P.; Foster, C.; Lai, B.; McBride, C.B.; Ng, K.; Pratt, M.; Shirazipour, C.H.; Smith, B.; Vásquez, P.M.; et al. Participation of people living with disabilities in physical activity: A global perspective. Lancet 2021, 398, 443–455. [Google Scholar] [CrossRef]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Gebel, K.; Ding, D. Benefits of Exercise. In Encyclopedia of Behavioral Medicine; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Pirazzi, A.; Gatti, A. Physical Activity Monitoring: Efficacy of Objective Methods to Maintain Adequate Levels of Physical Activity. Public Health Open Access 2022, 6, 2. [Google Scholar] [CrossRef]
- Howley, E.T. Type of activity: Resistance, aerobic and leisure versus occupational physical activity. Med. Sci. Sports Exerc. 2001, 33, S364–S369. [Google Scholar] [CrossRef]
- WHO. Physical Activity. 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 16 February 2026).
- WHO. Global Recommendations on Physical Activity for Health. In Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Rimmer, J.H.; Riley, B.; Wang, E.; Rauworth, A.; Jurkowski, J. Physical activity participation among persons with disabilities: Barriers and facilitators. Am. J. Prev. Med. 2004, 26, 419–425. [Google Scholar] [CrossRef]
- Derakhshan, P.; Miller, W.C.; Bundon, A.; Labbé, D.; Bolt, T.; Mortenson, W.B. Adaptive outdoor physical activities for adults with mobility disability: A scoping review. Front. Rehabil. Sci. 2024, 4, 1331971. [Google Scholar] [CrossRef]
- Ministère de l’Éducation du Québec. Ensemble, Relevons le défi d’une Participation Réussie—Plein Air et Personnes Handicapées; Ministère de l’Éducation du Québec: Québec, QC, Canada, 2020.
- Birenboim, A.; Ben-Nun Bloom, P.; Levit, H.; Omer, I. The Study of Walking, Walkability and Wellbeing in Immersive Virtual Environments. Int. J. Environ. Res. Public Health 2021, 18, 364. [Google Scholar] [CrossRef]
- Polechoński, J.; Nierwińska, K.; Kalita, B.; Wodarski, P. Can Physical Activity in Immersive Virtual Reality Be Attractive and Have Sufficient Intensity to Meet Health Recommendations for Obese Children? A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 8051. [Google Scholar] [CrossRef] [PubMed]
- Matsangidou, M.; Ang, C.S.; Mauger, A.R.; Intarasirisawat, J.; Otkhmezuri, B.; Avraamides, M.N. Is your virtual self as sensational as your real? Virtual Reality: The effect of body consciousness on the experience of exercise sensations. Psychol. Sport Exerc. 2019, 41, 218–224. [Google Scholar] [CrossRef]
- Liu, W.; Zeng, N.; Pope, Z.C.; McDonough, D.J.; Gao, Z. Acute Effects of Immersive Virtual Reality Exercise on Young Adults’ Situational Motivation. J. Clin. Med. 2019, 8, 1947. [Google Scholar] [CrossRef] [PubMed]
- Ravi, D.; Kumar, N.; Singhi, P. Effectiveness of virtual reality rehabilitation for children and adolescents with cerebral palsy: An updated evidence-based systematic review. Physiotherapy 2017, 103, 245–258. [Google Scholar] [CrossRef] [PubMed]
- Fandim, J.V.; Saragiotto, B.T.; Porfírio, G.J.M.; Santana, R.F. Effectiveness of virtual reality in children and young adults with cerebral palsy: A systematic review of randomized controlled trial. Braz. J. Phys. Ther. 2020, 25, 369–386. [Google Scholar] [CrossRef]
- Kashif, M.; Ahmad, A.; Bandpei, M.A.M.; Farooq, M.; Iram, H.; Fatima, R.E. Systematic review of the application of virtual reality to improve balance, gait and motor function in patients with Parkinson’s disease. Medicine 2022, 101, e29212. [Google Scholar] [CrossRef]
- Amirthalingam, J.; Paidi, G.; Alshowaikh, K.; Iroshani Jayarathna, A.I.; Salibindla, D.B.A.M.R.; Karpinska-Leydier, K.; Ergin, H.E. Virtual Reality Intervention to Help Improve Motor Function in Patients Undergoing Rehabilitation for Cerebral Palsy, Parkinson’s Disease, or Stroke: A Systematic Review of Randomized Controlled Trials. Cureus 2021, 13, e16763. [Google Scholar] [CrossRef]
- Laver, K.E.; Lange, B.; George, S.; Deutsch, J.E.; Saposnik, G.; Crotty, M. Virtual reality for stroke rehabilitation. Cochrane Database Syst. Rev. 2017, 11, CD008349. [Google Scholar] [CrossRef]
- Laufer, Y.; Weiss, P.L. Virtual Reality in the Assessment and Treatment of Children With Motor Impairment: A Systematic Review. J. Phys. Ther. Educ. 2011, 25, 59–71. [Google Scholar] [CrossRef]
- Tuominen, P.P.A.; Saarni, L.A. The use of virtual technologies with music in rehabilitation: A scoping systematic review. Front. Virtual Real. 2024, 5, 1290396. [Google Scholar] [CrossRef]
- Massetti, T.; Da Silva, T.D.; Crocetta, T.B.; Guarnieri, R.; De Freitas, B.L.; Bianchi Lopes, P.; Watson, S.; Tonks, J.; De Mello Monteiro, C.B. The Clinical Utility of Virtual Reality in Neurorehabilitation: A Systematic Review. J. Cent. Nerv. Syst. Dis. 2018, 10, 117957351881354. [Google Scholar] [CrossRef]
- Qian, J.; McDonough, D.J.; Gao, Z. The Effectiveness of Virtual Reality Exercise on Individual’s Physiological, Psychological and Rehabilitative Outcomes: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4133. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for Intervention Description and Replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef]
- Høeg, E.R.; Bruun-Pedersen, J.R.; Cheary, S.; Andersen, L.K.; Paisa, R.; Serafin, S.; Lange, B. Buddy biking: A user study on social collaboration in a virtual reality exergame for rehabilitation. Virtual Real. 2023, 27, 245–262. [Google Scholar] [CrossRef]
- Autry, C.E.; Anderson, S.C. Virtual Reality Sailing Simulation for People with Physical Disabilities: Learn to Sail. Ther. Recreat. J. 2022, 56, 177–190. [Google Scholar] [CrossRef]
- Polechoński, J.; Langer, A.; Akbaş, A.; Zwierzchowska, A. Application of immersive virtual reality in the training of wheelchair boxers: Evaluation of exercise intensity and users experience additional load—A pilot exploratory study. BMC Sports Sci. Med. Rehabil. 2024, 16, 80. [Google Scholar] [CrossRef]
- Chen, C.-H.; Jeng, M.-C.; Fung, C.-P.; Doong, J.-L.; Chuang, T.-Y. Psychological benefits of virtual reality for patients in rehabilitation therapy. J. Sport Rehabil. 2009, 18, 258–268. [Google Scholar] [CrossRef]
- Deutsch, J.E.; Myslinski, M.J.; Kafri, M.; Ranky, R.; Sivak, M.; Mavroidis, C.; Lewis, J.A. Feasibility of Virtual Reality Augmented Cycling for Health Promotion of People Poststroke. J. Neurol. Phys. Ther. 2013, 37, 118–124. [Google Scholar] [CrossRef]
- Heyn, P.; Baumgardner, C.; McLachlan, L.; Bodine, C. Mixed-Reality Exercise Effects on Participation of Individuals with Spinal Cord Injuries and Developmental Disabilities: A Pilot Study. Top. Spinal Cord Inj. Rehabil. 2014, 20, 338–345. [Google Scholar] [CrossRef]
- Gallagher, R.; Werner, W.G.; Damodaran, H.; Deutsch, J.E. Influence of cueing, feedback and directed attention on cycling in a virtual environment: Preliminary findings in healthy adults and persons with Parkinson’s disease. In Proceedings of the 2015 International Conference on Virtual Rehabilitation (ICVR), Valencia, Spain, 9–12 June 2015; pp. 11–17. [Google Scholar] [CrossRef]
- Yin, C.; Hsueh, Y.-H.; Yeh, C.-Y.; Lo, H.-C.; Lan, Y.-T. A Virtual Reality-Cycling Training System for Lower Limb Balance Improvement. BioMed Res. Int. 2016, 2016, 9276508. [Google Scholar] [CrossRef] [PubMed]
- Lee, K. Speed-Interactive Pedaling Training Using Smartphone Virtual Reality Application for Stroke Patients: Single-Blinded, Randomized Clinical Trial. Brain Sci. 2019, 9, 295. [Google Scholar] [CrossRef] [PubMed]
- Rojo, A.; Castrillo, A.; López, C.; Perea, L.; Alnajjar, F.; Moreno, J.C.; Raya, R. PedaleoVR: Usability study of a virtual reality application for cycling exercise in patients with lower limb disorders and elderly people. PLoS ONE 2023, 18, e0280743. [Google Scholar] [CrossRef] [PubMed]
- Rojo, A.; Castrillo Calvillo, A.; López, C.; Raya, R.; Moreno, J.C. Effects of a Virtual Reality Cycling Platform on Lower Limb Rehabilitation in Patients with Ataxia and Hemiparesis: Pilot Randomized Controlled Trial. JMIR Serious Games 2024, 12, e39286. [Google Scholar] [CrossRef] [PubMed]
- Hasnan, N.; Hamzaid, N.A.; Magenthran, V.; Davis, G.M. Exercise Responses During Outdoor Versus Virtual Reality Indoor Arm+FES-Leg Cycling in Individuals with Spinal Cord Injury. Games Health J. 2024, 13, 207–214. [Google Scholar] [CrossRef]
- Recio, A.C.; Becker, D.; Morgan, M.; Saunders, N.R.; Schramm, L.P.; McDonald, J.W., III. Use of a Virtual Reality Physical Ride-On Sailing Simulator as a Rehabilitation Tool for Recreational Sports and Community Reintegration: A Pilot Study. Am. J. Phys. Med. Rehabil. 2013, 92, 1104–1109. [Google Scholar] [CrossRef]
- Recio, A.C.; Stiens, S.A.; Morgan, M.; Selvarajah, S.; Mazeh, A.C.; Habgood, M.D.; Saunders, N.R. Realtime physical simulator for virtual reality sailing by patients with spinal cord injury: An innovative voyage. Health Open Res. 2024, 6, 6. [Google Scholar] [CrossRef]
- Lee, M.-M.; Shin, D.-C.; Song, C.-H. Canoe game-based virtual reality training to improve trunk postural stability, balance, and upper limb motor function in subacute stroke patients: A randomized controlled pilot study. J. Phys. Ther. Sci. 2016, 28, 2019–2024. [Google Scholar] [CrossRef]
- Lee, M.M.; Lee, K.J.; Song, C.H. Game-Based Virtual Reality Canoe Paddling Training to Improve Postural Balance and Upper Extremity Function: A Preliminary Randomized Controlled Study of 30 Patients with Subacute Stroke. Med. Sci. Monit. 2018, 24, 2590–2598. [Google Scholar] [CrossRef]
- An, Y.; Park, C. The effects of virtual soccer game on balance, gait function, and kick speed in chronic incomplete spinal cord injury: A randomized controlled trial. Spinal Cord 2022, 60, 504–509. [Google Scholar] [CrossRef]
- Tacchino, A.; Ponzio, M.; Confalonieri, P.; Leocani, L.; Inglese, M.; Centonze, D.; Cocco, E.; Gallo, P.; Paolicelli, D.; Rovaris, M.; et al. An Internet- and Kinect-Based Multiple Sclerosis Fitness Intervention Training With Pilates Exercises: Development and Usability Study. JMIR Serious Games 2023, 11, e41371. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.; Marsh, T.; Duke, D.; Wright, P. Drowning in immersion. In Proceedings of the UK Virtual Reality Special Interest Group Conference (UK-VRSIG ’98), Exeter, UK, 1998; Available online: https://www.researchgate.net/publication/2362590_Drowning_in_Immersion (accessed on 16 February 2026).
- WHO. International Classification of Functioning, Disability, and Health: ICF, Version 1.0; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Ginis, K.A.; Arbour-Nicitopoulos, K.P.; Latimer-Cheung, A.E.; Buchholz, A.C.; Bray, S.R.; Craven, B.C.; Hayes, K.C.; McColl, M.A.; Potter, P.J.; Smith, K.; et al. Predictors of leisure time physical activity among people with spinal cord injury. Ann. Behav. Med. 2012, 44, 104–118. [Google Scholar] [CrossRef]
- Miller, H.L.; Bugnariu, N.L. Level of Immersion in Virtual Environments Impacts the Ability to Assess and Teach Social Skills in Autism Spectrum Disorder. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 246–256. [Google Scholar] [CrossRef] [PubMed]
- Balcazar, F.; Keys, C.; Kaplan, D. Participatory Action Research and People with Disabilities: Principles and Challenges. Can. J. Rehabil. 2006, 12, 105–112. [Google Scholar]
- Sanders, E.; Stappers, P.J. Co-creation and the New Landscapes of Design. CoDesign 2008, 4, 5–18. [Google Scholar] [CrossRef]
- United Nations. Convention on the Rights of Persons with Disabilities; United Nations: New York, NY, USA, 2006. [Google Scholar]
- Glegg, S.M.N.; Levac, D.E. Barriers, Facilitators and Interventions to Support Virtual Reality Implementation in Rehabilitation: A Scoping Review. Pm R 2018, 10, 1237–1251.e1231. [Google Scholar] [CrossRef]
- Ferche, O.-M.; Moldoveanu, A.; Moldoveanu, F.; Voinea, A.; Victor, A.; Negoi, I. CHALLENGES AND ISSUES FOR SUCCESSFULLY APPLYING VIRTUAL REALITY IN MEDICAL REHABILITATION. In Proceedings of the 11th International Scientific Conference eLearning and Software for Education: Rethinking Education by Leveraging the eLearning Millar of the Digital Agenda for Europe, Bucharest, Romania, 23–24 April 2015; p. 3. [Google Scholar] [CrossRef]
- Lukacs, M.J.; Salim, S.; Katchabaw, M.J.; Yeung, E.; Walton, D.M. Virtual reality in physical rehabilitation: A narrative review and critical reflection. Phys. Ther. Rev. 2022, 27, 281–289. [Google Scholar] [CrossRef]
- Michalski, S.C.; Szpak, A.; Loetscher, T. Using Virtual Environments to Improve Real-World Motor Skills in Sports: A Systematic Review. Front Psychol. 2019, 10, 2159. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.