
Update on Malignancy in Myositis—Well-Established Association with Unmet Needs

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Epidemiology
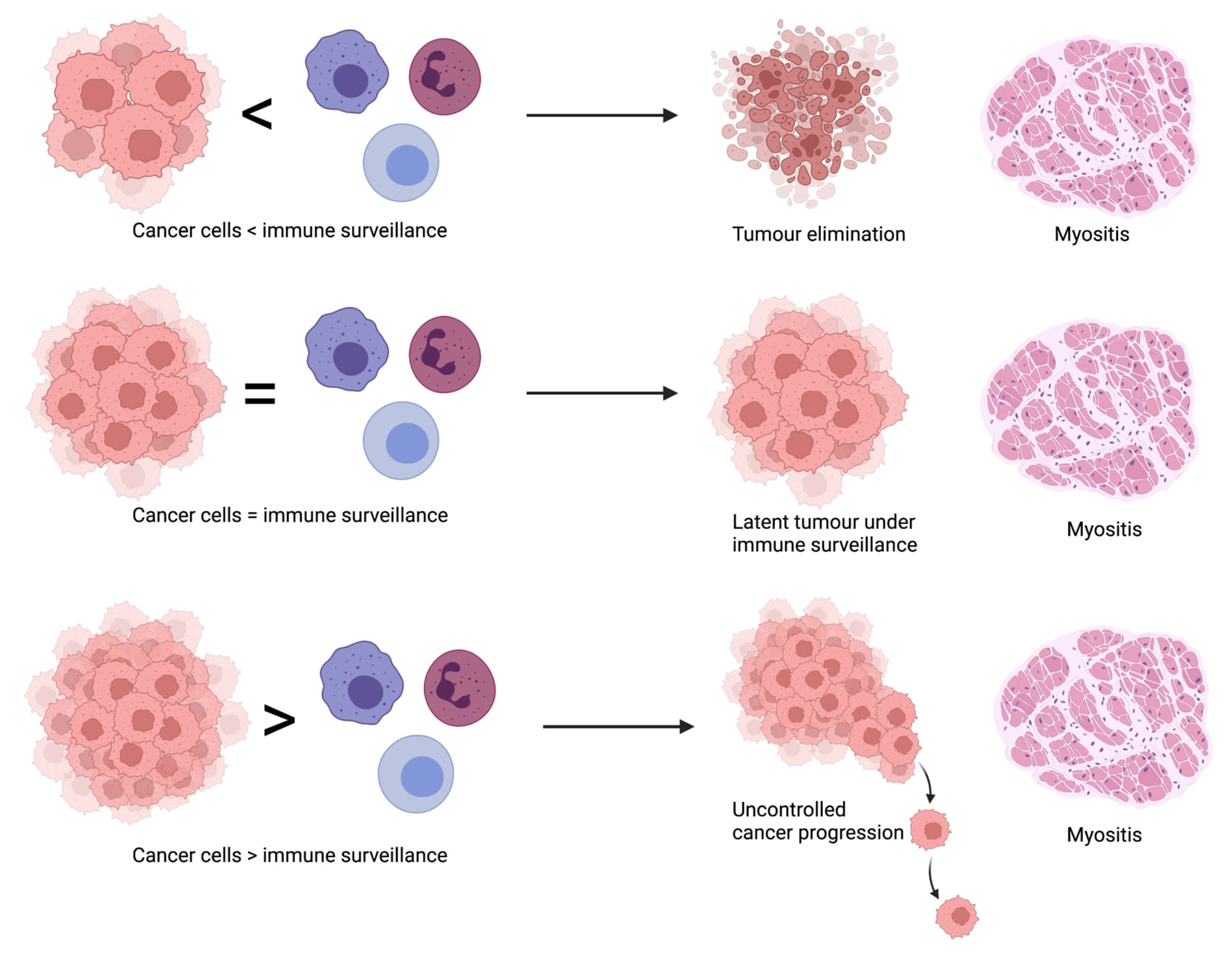
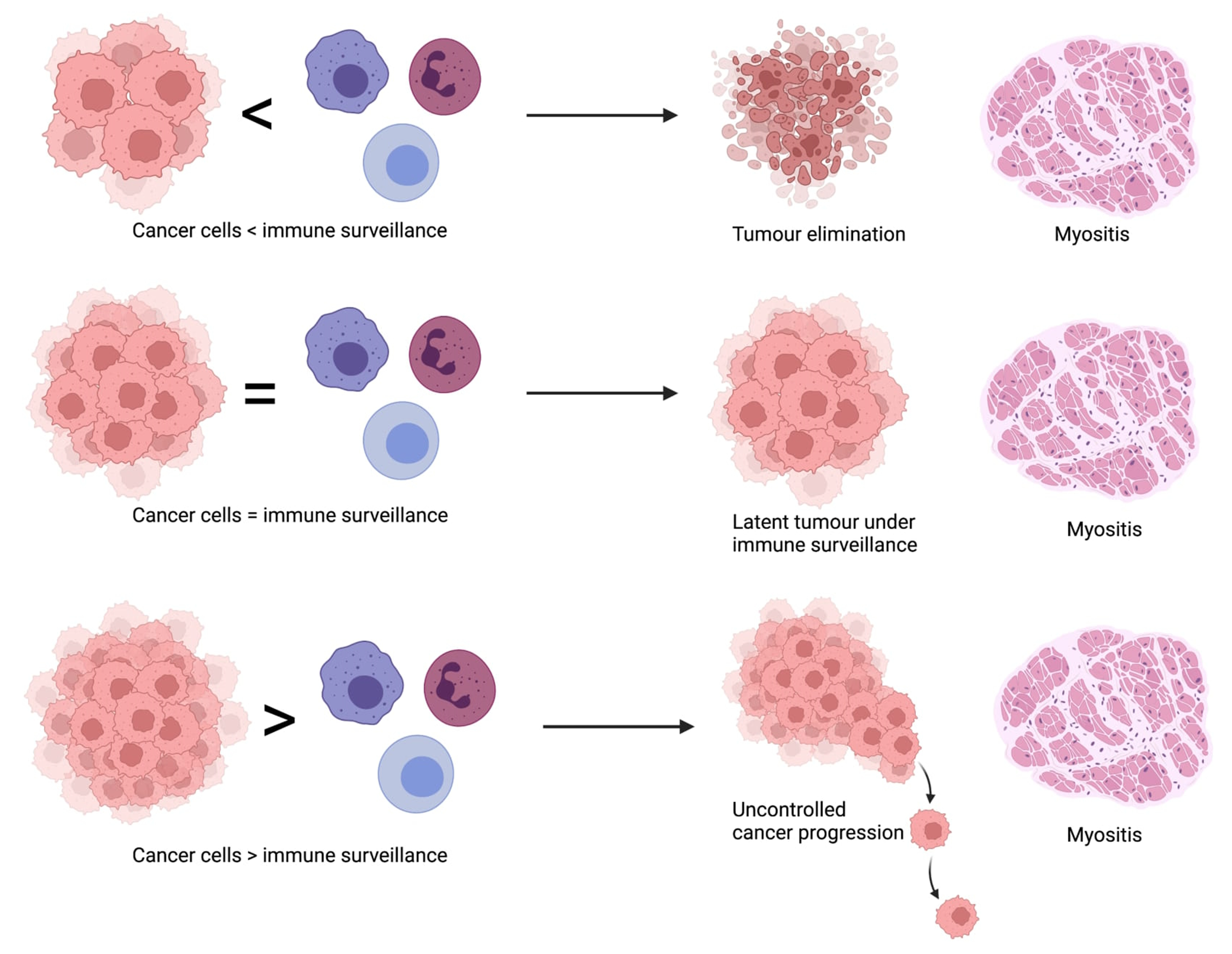
3. Pathogenesis
4. Types of Cancers Associated with Myositis
5. Risk Factors for Malignancy in Myositis
5.1. Clinical Factors Associated with CAM
5.1.1. Demographical Data
5.1.2. Muscle Involvement
5.1.3. Cutaneous Involvement
5.1.4. Biochemical and Serological Tests
5.2. Serological Profiles Associated with CAM
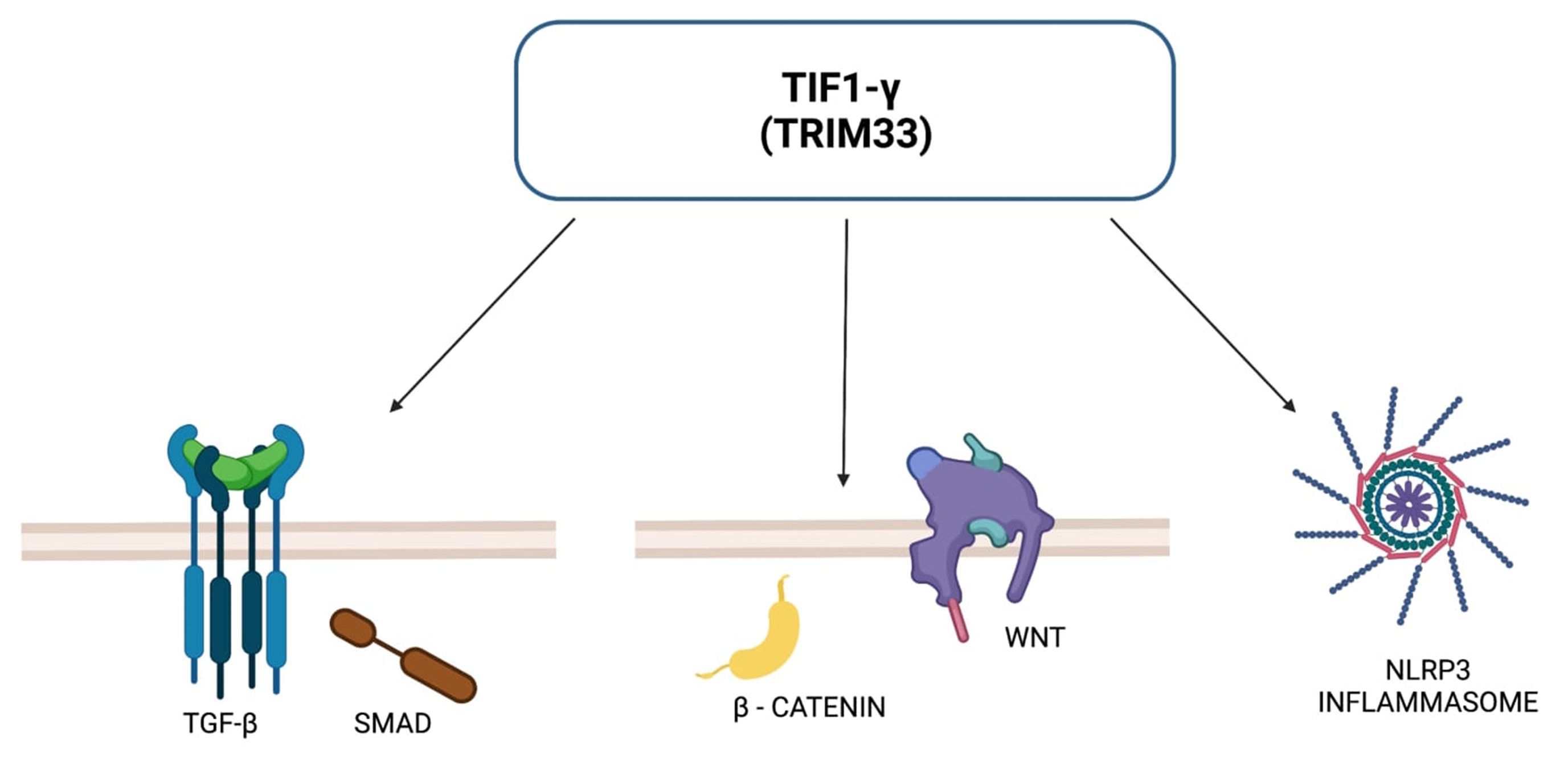
5.2.1. Anti-TIF1-γ Antibodies
5.2.2. Anti-NXP-2 Antibodies
5.2.3. Anti-SAE Antibodies
5.2.4. Remaining Serological Profiles
6. Protective Factors
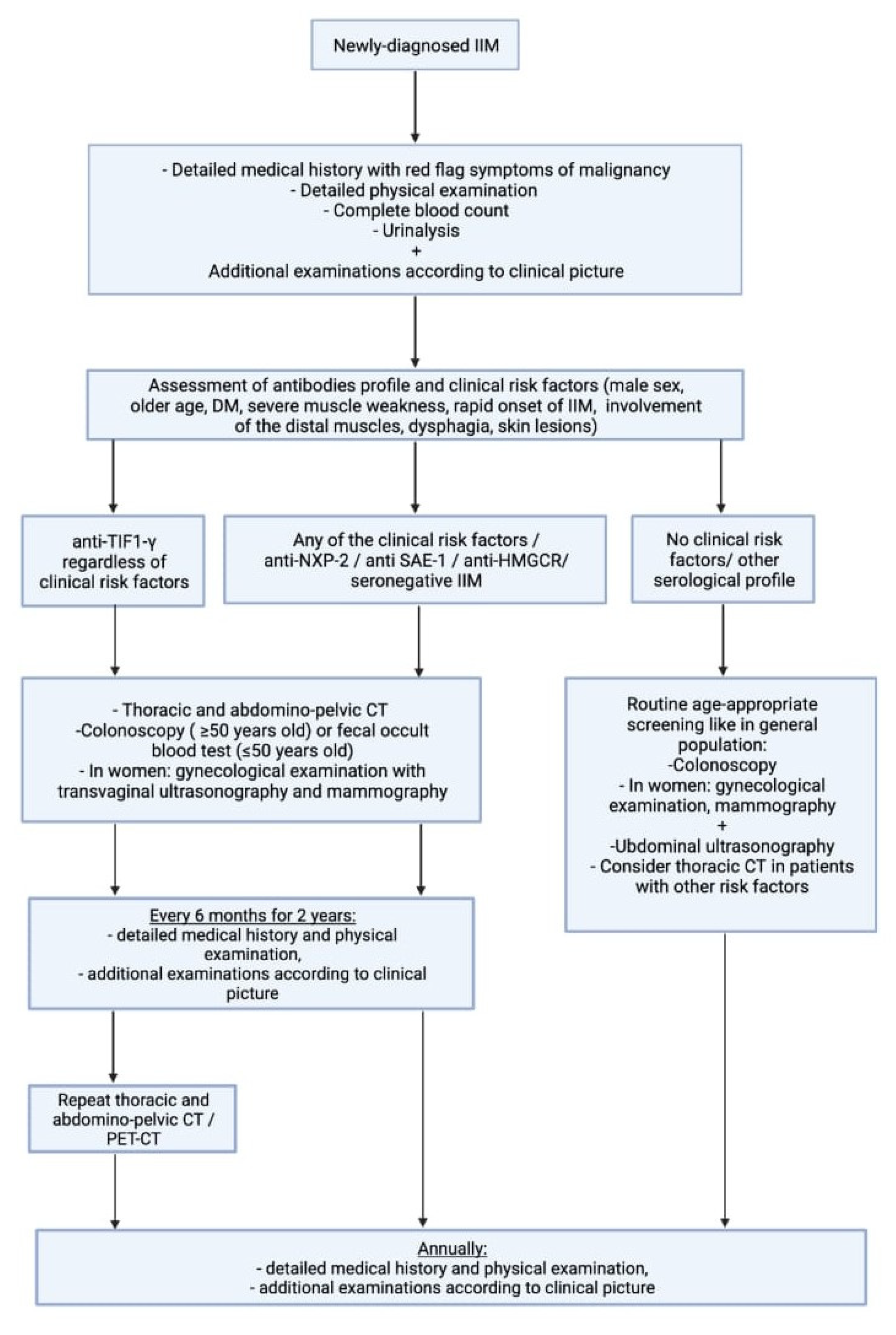
7. Management of Cancer-associated Myositis
8. Prognosis
9. Unmet Needs
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meyer, A.; Meyer, N.; Schaeffer, M.; Gottenberg, J.-E.; Geny, B.; Sibilia, J. Incidence and prevalence of inflammatory myopathies: A systematic review. Rheumatology 2015, 54, 50–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chinoy, H.; Lilleker, J.B. Pitfalls in the diagnosis of myositis. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101486. [Google Scholar] [CrossRef] [PubMed]
- Vencovský, J.; Alexanderson, H.; Lundberg, I.E. Idiopathic inflammatory myopathies. Rheum. Dis. Clin. N. Am. 2019, 45, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Nagai, H.; Kim, Y.H. Cancer prevention from the perspective of global cancer burden patterns. J. Thorac. Dis. 2017, 9, 448–451. [Google Scholar] [CrossRef]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.B.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- Stertz, G.P. Polymyositis. Berl. Klin. Wochenschr. 1916, 53, 489. [Google Scholar]
- Kankelheit, H. Uber primare nichteitrige polymyositis. Dtsch. Arch. Klin. Med. 1916, 120, 335–349. [Google Scholar]
- Moghadam-Kia, S.; Oddis, C.V.; Ascherman, D.P.; Aggarwal, R. Risk factors and cancer screening in myositis. Rheum. Dis. Clin. N. Am. 2020, 46, 565–576. [Google Scholar] [CrossRef]
- Lu, X.; Peng, Q.; Wang, G. The role of cancer-associated autoantibodies as biomarkers in paraneoplastic myositis syndrome. Curr. Opin. Rheumatol. 2019, 31, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Chow, W.-H.; Gridley, G.; Mellemkjær, L.; McLaughlin, J.K.; Olsen, J.H.; Fraumeni, J.F. Cancer risk following polymyositis and dermatomyositis: A nationwide cohort study in Denmark. Cancer Causes Control. 1995, 6, 9–13. [Google Scholar] [CrossRef]
- Wakata, N.; Kurihara, T.; Saito, E.; Kinoshita, M. Polymyositis and dermatomyositis associated with malignancy: A 30-year retrospective study: Polymyositis and dermatomyositis with malignancy. Int. J. Dermatol. 2002, 41, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Ponyi, A.; Constantin, T.; Garami, M.; András, C.; Tállai, B.; Váncsa, A.; Gergely, L.; Dankó, K. Cancer-Associated Myositis: Clinical Features and Prognostic Signs. Ann. N. Y. Acad. Sci. 2005, 1051, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Sigurgeirsson, B.; Lindelöf, B.; Edhag, O.; Allander, E. Risk of Cancer in Patients with Dermatomyositis or Polymyositis. New Engl. J. Med. 1992, 326, 363–367. [Google Scholar] [CrossRef] [PubMed]
- András, C.; Ponyi, A.; Constantin, T.; Csiki, Z.; Szekanecz, E.; Szodoray, P.; Dankó, K. Dermatomyositis and polymyositis associated with malignancy: A 21-year retrospective study. J. Rheumatol. 2008, 35, 438–444. [Google Scholar]
- Qiang, J.K.; Kim, W.B.; Baibergenova, A.; Alhusayen, R. Risk of malignancy in dermatomyositis and polymyositis: A systematic review and meta-analysis. J. Cutan. Med. Surg. 2017, 21, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Peng, Q.; Yin, L.; Li, S.; Shi, J.; Zhang, Y.; Lu, X.; Shu, X.; Zhang, S.; Wang, G. Identification of multiple cancer-associated myositis-specific autoantibodies in idiopathic inflammatory myopathies: A large longitudinal cohort study. Arthritis Res. Ther. 2017, 19, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Jia, X.; Sun, X.; Shi, L.; Lin, F.; Gan, Y.; Zhang, X.; Gao, X.; Miao, M.; Hong, D.; et al. Risk factors for cancer-associated myositis: A large-scale multicenter cohort study. Int. J. Rheum. Dis. 2021, 24, 268–273. [Google Scholar] [CrossRef]
- Lilleker, J.B.; Vencovsky, J.; Wang, G.; Wedderburn, L.R.; Diederichsen, L.P.; Schmidt, J.; Oakley, P.; Benveniste, O.; Danieli, M.G.; Danko, K.; et al. The EuroMyositis registry: An international collaborative tool to facilitate myositis research. Ann. Rheum. Dis. 2018, 77, 30–39. [Google Scholar] [CrossRef]
- Levine, S.M. Cancer and myositis: New insights into an old association. Curr. Opin. Rheumatol. 2006, 18, 620–624. [Google Scholar] [CrossRef]
- András, C.; Bodoki, L.; Nagy-Vincze, M.; Griger, Z.; Csiki, E.; Dankó, K. Retrospective Analysis of Cancer-Associated Myositis Patients over the Past 3 Decades in a Hungarian Myositis Cohort. Pathol. Oncol. Res. 2019, 26, 1749–1755. [Google Scholar] [CrossRef] [Green Version]
- Hill, C.L.; Zhang, Y.; Sigurgeirsson, B.; Pukkala, E.; Mellemkjaer, L.; Airio, A.; Evans, S.R.; Felson, D.T. Frequency of specific cancer types in dermatomyositis and polymyositis: A population-based study. Lancet 2001, 357, 96–100. [Google Scholar] [CrossRef]
- András, C.; Csiki, Z.; Ponyi, A.; Illés, Á.; Dankó, K. Paraneoplastic rheumatic syndromes. Rheumatol. Int. 2006, 26, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Zahr, Z.A.; Baer, A.N. Malignancy in myositis. Curr. Rheumatol. Rep. 2011, 13, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Gerami, P.; Walling, H.W.; Lewis, J.; Doughty, L.; Sontheimer, R.D. A systematic review of juvenile-onset clinically amyopathic dermatomyositis. Br. J. Dermatol. 2007, 157, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Buchbinder, R.; Forbes, A.; Hall, S.; Dennett, X.; Giles, G. Incidence of malignant disease in biopsy-proven inflammatory myopathy: A population-based cohort study. Ann. Intern. Med. 2001, 134, 1087. [Google Scholar] [CrossRef] [PubMed]
- Limaye, V.; Luke, C.; Tucker, G.; Hill, C.; Lester, S.; Blumbergs, P.; Roberts-Thomson, P. The incidence and associations of malignancy in a large cohort of patients with biopsy-determined idiopathic inflammatory myositis. Rheumatol. Int. 2013, 33, 965–971. [Google Scholar] [CrossRef] [PubMed]
- Dobloug, G.C.; Garen, T.; Brunborg, C.; Gran, J.T.; Molberg, Ø. Survival and cancer risk in an unselected and complete Norwegian idiopathic inflammatory myopathy cohort. Semin. Arthritis Rheum. 2015, 45, 301–308. [Google Scholar] [CrossRef] [Green Version]
- Targoff, I.N.; Mamyrova, G.; Trieu, E.P.; Perurena, O.; Koneru, B.; O’Hanlon, T.P.; Miller, F.W.; Rider, L.G.; Childhood Myositis Heterogeneity And International Myositis Collaborative Study Groups. A novel autoantibody to a 155-kd protein is associated with dermatomyositis. Arthritis Rheum 2006, 54, 3682–3689. [Google Scholar] [CrossRef]
- Casciola-Rosen, L.; Nagaraju, K.; Plotz, P.; Wang, K.; Levine, S.; Gabrielson, E.; Corse, A.; Rosen, A. Enhanced autoantigen expression in regenerating muscle cells in idiopathic inflammatory myopathy. J. Exp. Med. 2005, 201, 591–601. [Google Scholar] [CrossRef]
- Kasuya, A.; Hamaguchi, Y.; Fujimoto, M.; Tokura, Y. TIF1γ-overexpressing, highly progressive endometrial carcinoma in a patient with dermato-myositis positive for malignancy-associated anti-p155/140 autoantibody. Acta Derm. Venerol. 2013, 93, 715–716. [Google Scholar] [CrossRef]
- Zampieri, S.; Biral, D.; Adami, N.; Ghirardello, A.; Rampudda, M.E.; Tonello, M.; Doria, A. Expression of myositis specific autoantigens during post-natal myogenesis. Neurol. Res. 2008, 30, 145–148. [Google Scholar] [CrossRef]
- Hengstman, G.J.D.; Egberts, W.V.; Seelig, H.P.; Lundberg, I.E.; Moutsopoulos, H.M.; Doria, A.; Mosca, M.; Vencovsky, J.; Van Venrooij, W.J.; Van Engelen, B.G.M. Clinical characteristics of patients with myositis and autoantibodies to different fragments of the Mi-2 antigen. Ann. Rheum. Dis. 2006, 65, 242–245. [Google Scholar] [CrossRef]
- Zampieri, S.; Valente, M.; Adami, N.; Biral, D.; Ghirardello, A.; Rampudda, M.E.; Vecchiato, M.; Sarzo, G.; Corbianco, S.; Kern, H.; et al. Polymyositis, dermatomyositis and malignancy: A further intriguing link. Autoimmun. Rev. 2010, 9, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Pinal-Fernandez, I.; Ferrer-Fabregas, B.; Trallero-Araguas, E.; Balada, E.; Martínez, M.A.; Milisenda, J.C.; Aparicio-Español, G.; Labrador-Horrillo, M.; Garcia-Patos, V.; Grau-Junyent, J.M.; et al. Tumour TIF1 mutations and loss of heterozygosity related to cancer-associated myositis. Rheumatology 2018, 57, 388–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selva-O’Callaghan, A.; Ros, J.; Gil-Vila, A.; Vila-Pijoan, G.; Trallero-Araguás, E.; Pinal-Fernandez, I. Malignancy and myositis, from molecular mimicry to tumor infiltrating lymphocytes. Neuromuscul. Disord. 2019, 29, 819–825. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Peng, Q.; Yang, H.; Yin, L.; Shi, J.; Zhang, Y.; Wang, G. Increased levels of soluble programmed death ligand 1 associate with malignancy in patients with dermatomyositis. J. Rheumatol. 2018, 45, 835–840. [Google Scholar] [CrossRef] [PubMed]
- Marie, I.; Guillevin, L.; Menard, J.-F.; Hatron, P.Y.; Cherin, P.; Amoura, Z.; Cacoub, P.; Bachelez, H.; Buzyn, A.; Le Roux, G.; et al. Hematological malignancy associated with polymyositis and dermatomyositis. Autoimmun. Rev. 2012, 11, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-J.; Wu, C.-Y.; Shen, J.-L. Predicting factors of malignancy in dermatomyositis and polymyositis: A case-control study. Br. J. Dermatol. 2001, 144, 825–831. [Google Scholar] [CrossRef]
- Huang, Y.L.; Chen, Y.J.; Lin, M.W.; Wu, C.Y.; Liu, P.C.; Chen, T.J.; Chen, Y.C.; Jih, J.S.; Chen, C.C.; Lee, D.D.; et al. Malignancies associated with dermatomyositis and polymyositis in Taiwan: A nationwide population-based study. Br. J. Dermatol. 2009, 161, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Ungprasert, P.; Leeaphorn, N.; Hosiriluck, N.; Chaiwatcharayut, W.; Ammannagari, N.; Raddatz, D.A. Clinical features of inflammatory myopathies and their association with malignancy: A systematic review in asian population. ISRN Rheumatol. 2013, 2013, 509354. [Google Scholar] [CrossRef] [PubMed]
- Tiniakou, E.; Mammen, A.L. Idiopathic inflammatory myopathies and malignancy: A comprehensive review. Clin. Rev. Allergy Immunol. 2017, 52, 20–33. [Google Scholar] [CrossRef]
- Cherin, P.; Piette, J.C.; Herson, S.; Bletry, O.; Wechsler, B.; Frances, C.; Godeau, P. Dermatomyositis and ovarian cancer: A report of 7 cases and literature review. J. Rheumatol. 1993, 20, 1897–1899. [Google Scholar] [PubMed]
- Fujita, J.; Tokuda, M.; Bandoh, S.; Yang, Y.; Fukunaga, Y.; Hojo, S.; Ueda, Y.; Dobashi, N.; Dohmoto, K.; Ishida, T.; et al. Primary lung cancer associated with polymyositis/dermatomyositis, with a review of the literature. Rheumatol. Int. 2001, 20, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Fardet, L.; Dupuy, A.; Gain, M.; Kettaneh, A.; Chérin, P.; Bachelez, H.; Dubertret, L.; Lebbe, C.; Morel, P.; Rybojad, M. Factors associated with underlying malignancy in a retrospective cohort of 121 patients with dermatomyositis. Medicine 2009, 88, 91–97. [Google Scholar] [CrossRef] [PubMed]
- So, M.W.; Koo, B.S.; Kim, Y.-G.; Lee, C.-K.; Yoo, B. Idiopathic inflammatory myopathy associated with malignancy: A retrospective cohort of 151 korean patients with dermatomyositis and polymyositis. J. Rheumatol. 2011, 38, 2432–2435. [Google Scholar] [CrossRef] [PubMed]
- Antiochos, B.B.; Brown, L.A.; Li, Z.; Tosteson, T.D.; Wortmann, R.L.; Rigby, W.F.C. Malignancy is associated with dermatomyositis but not polymyositis in Northern New England, USA. J. Rheumatol. 2009, 36, 2704–2710. [Google Scholar] [CrossRef] [Green Version]
- Prohic, A.; Kasumagic-Halilovic, E.; Simic, D.; Selmanagic, A. Clinical and biological factors predictive of malignancy in dermatomyositis. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 591–592. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Guo, G.; Chen, G.; Wu, B.; Lu, L.; Bao, L. Meta-analysis of the association of dermatomyositis and polymyositis with cancer. Br. J. Dermatol. 2013, 169, 838–847. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Yang, H.; Shu, X.; Chen, F.; Zhang, Y.; Zhang, S.; Peng, Q.; Tian, X.; Wang, G. Factors predicting malignancy in patients with polymyositis and dermatomyostis: A systematic review and meta-analysis. PLoS ONE 2014, 9, e94128. [Google Scholar] [CrossRef] [Green Version]
- Neri, R.; Simone, B.; Iacopetti, V.; Iacopetti, G.; Pepe, P.; d’Ascanio, A.; Tavoni, A.G.; Mosca, M.; Bombardieri, S. Cancer-associated myositis: A 35-year retrospective study of a monocentric cohort. Rheumatol. Int. 2014, 34, 565–569. [Google Scholar] [CrossRef]
- Stockton, D.; Doherty, V.R.; Brewster, D.H. Risk of cancer in patients with dermatomyositis or polymyositis and follow-up implications: A Scottish population-based cohort study. Br. J. Cancer 2001, 85, 41–45. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-J.; Wu, C.-Y.; Huang, Y.-L.; Wang, C.-B.; Shen, J.-L.; Chang, Y.-T. Cancer risks of dermatomyositis and polymyositis: A nationwide cohort study in Taiwan. Arthritis Res. Ther. 2010, 12, R70. [Google Scholar] [CrossRef] [Green Version]
- Oldroyd, A.G.S.; Allard, A.B.; Callen, J.P.; Chinoy, H.; Chung, L.; Fiorentino, D.; George, M.D.; Gordon, P.; Kolstad, K.; Kurtzman, D.J.B.; et al. A systematic review and meta-analysis to inform cancer screening guidelines in idiopathic inflammatory myopathies. Rheumatology 2021, 60, 2615–2628. [Google Scholar] [CrossRef]
- Labeit, B.; Pawlitzki, M.; Ruck, T.; Muhle, P.; Claus, I.; Suntrup-Krueger, S.; Warnecke, T.; Meuth, S.G.; Wiendl, H.; Dziewas, R. The Impact of Dysphagia in Myositis: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 2150. [Google Scholar] [CrossRef]
- Uchino, M.; Yamashita, S.; Uchino, K.; Mori, A.; Hara, A.; Suga, T.; Hirahara, T.; Koide, T.; Kimura, E.; Yamashita, T.; et al. Muscle biopsy findings predictive of malignancy in rare infiltrative dermatomyositis. Clin. Neurol. Neurosurg. 2013, 115, 603–606. [Google Scholar] [CrossRef] [PubMed]
- Hunger, R.E.; Dürr, C.; Brand, C.U. Cutaneous leukocytoclastic vasculitis in dermatomyositis suggests malignancy. Dermatology 2001, 202, 123–126. [Google Scholar] [CrossRef]
- Requena, C.; Alfaro, A.; Traves, V.; Nagore, E.; Llombart, B.; Serra, C.; Martorell, A.; Guillén, C.; Sanmartín, O. Dermatomiositis paraneoplásica: Estudio de 12 casos. Actas Dermo-Sifiliográficas 2014, 105, 675–682. [Google Scholar] [CrossRef]
- Selva-O’Callaghan, A.; Fonollosa-Pla, V.; Trallero-Araguás, E.; Martínez-Gómez, X.; Simeon-Aznar, C.P.; Labrador-Horrillo, M.; Vilardell-Tarrés, M. Nailfold capillary microscopy in adults with inflammatory myopathy. Semin. Arthritis Rheum. 2010, 39, 398–404. [Google Scholar] [CrossRef]
- Amerio, P.; Girardelli, C.R.; Proietto, G.; Forleo, P.; Cerritelli, L.; Feliciani, C.; Colonna, L.; Teofoli, P.; Amerio, P.; Puddu, P.; et al. Usefulness of erythrocyte sedimentation rate as tumor marker in cancer associated dermatomyositis. Eur. J. Dermatol. 2002, 12, 165–169. [Google Scholar]
- Yu, C.; Ding, Z.; Liang, H.; Zhang, B.; Chen, X. The roles of TIF1γ in cancer. Front. Oncol. 2019, 9, 979. [Google Scholar] [CrossRef]
- Kotobuki, Y.; Tonomura, K.; Fujimoto, M. Transcriptional intermediary factor 1 (TIF1) and anti-TIF1γ antibody-positive dermatomyositis. Immunol. Med. 2021, 44, 23–29. [Google Scholar] [CrossRef]
- Li, L.; Liu, C.; Wang, Q.; Wu, C.; Zhang, Y.; Cheng, L.; Wen, X.; Zeng, X.; Zhang, F.; Li, Y. Analysis of myositis autoantibodies in Chinese patients with cancer-associated myositis. J. Clin. Lab. Anal. 2020, 34, e23307. [Google Scholar] [CrossRef]
- Li, S.; Ge, Y.; Yang, H.; Wang, T.; Zheng, X.; Peng, Q.; Lu, X.; Wang, G. The spectrum and clinical significance of myositis-specific autoantibodies in Chinese patients with idiopathic inflammatory myopathies. Clin. Rheumatol. 2019, 38, 2171–2179. [Google Scholar] [CrossRef]
- Aussy, A.; Fréret, M.; Gallay, L.; Bessis, D.; Vincent, T.; Jullien, D.; Drouot, L.; Jouen, F.; Joly, P.; Marie, I.; et al. The IgG2 isotype of anti–transcription intermediary factor 1γ autoantibodies is a biomarker of cancer and mortality in adult dermatomyositis. Arthritis Rheumatol. 2019, 71, 1360–1370. [Google Scholar] [CrossRef]
- Abe, Y.; Ando, T.; Matsushita, M.; Tada, K.; Yamaji, K.; Tamura, N. Changes in antibody titres in patients with anti-transcription intermediary factor 1-gamma antibody-positive idiopathic inflammatory myositis. Rheumatology 2019, 58, 179–181. [Google Scholar] [CrossRef]
- Ogawa-Momohara, M.; Muro, Y.; Mitsuma, T.; Katayama, M.; Yanaba, K.; Nara, M.; Kakeda, M.; Kono, M.; Akiyama, M. Strong correlation between cancer progression and anti-transcription intermediary factor 1γ antibodies in dermatomyositis patients. Clin. Exp. Rheumatol. 2018, 36, 990–995. [Google Scholar]
- Vázquez-Del Mercado, M.; Martínez-García, E.A.; Daneri-Navarro, A.; Gómez-Bañuelos, E.; Martín-Márquez, B.T.; Pizano-Martínez, O.; Wilson-Manríquez, E.A.; Corona-Sánchez, E.G.; Chavarria-Avila, E.; Sandoval-García, F.; et al. Presence of anti-TIF-1γ, anti-Ro52, anti-SSA/Ro60 and anti-Su/AgO2 antibodies in breast cancer: A cross-sectional study. Immunopharmacol. Immunotoxicol. 2021, 43, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Su, L.; Yang, Y.; Jia, Y.; Liu, X.; Zhang, W.; Yuan, Y.; Li, Z. Anti-NXP2-antibody-positive immune-mediated necrotizing myopathy associated with acute myeloid leukemia. Med. 2018, 97, e11501. [Google Scholar] [CrossRef]
- Wang, X.; Ding, Y.; Zhou, Z.; Hou, J.; Xu, Y.; Li, J. Clinical characteristics and poor predictors of anti-NXP2 antibody-associated Chinese JDM children. Pediatr. Rheumatol. 2021, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Satoh, M.; Tanaka, S.; Ceribelli, A.; Calise, S.J.; Chan, E. A Comprehensive Overview on Myositis-Specific Antibodies: New and Old Biomarkers in Idiopathic Inflammatory Myopathy. Clin. Rev. Allergy Immunol. 2017, 52, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aussy, A.; Boyer, O.; Cordel, N. Dermatomyositis and immune-mediated necrotizing myopathies: A window on autoimmunity and cancer. Front. Immunol. 2017, 8, 992. [Google Scholar] [CrossRef]
- Ichimura, Y.; Matsushita, T.; Hamaguchi, Y.; Kaji, K.; Hasegawa, M.; Tanino, Y.; Inokoshi, Y.; Kawai, K.; Kanekura, T.; Habuchi, M.; et al. Anti-NXP2 autoantibodies in adult patients with idiopathic inflammatory myopathies: Possible association with malignancy. Ann. Rheum. Dis. 2012, 71, 710–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiorentino, D.F.; Chung, L.S.; Christopher-Stine, L.; Zaba, L.; Li, S.; Mammen, A.L.; Rosen, A.; Casciola-Rosen, L. Most patients with cancer-associated dermatomyositis have antibodies to nuclear matrix protein NXP-2 or transcription intermediary factor 1γ: Antibodies to NXP-2 and TIF-1γ in cancer-associated dermatomyositis. Arthritis Rheum. 2013, 65, 2954–2962. [Google Scholar] [CrossRef] [PubMed]
- Zhong, L.; Yu, Z.; Song, H. Association of anti-nuclear matrix protein 2 antibody with complications in patients with idiopathic inflammatory myopathies: A meta-analysis of 20 cohorts. Clin. Immunol. 2019, 198, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Bodoki, L.; Nagy-Vincze, M.; Griger, Z.; Betteridge, Z.; Szöllősi, L.; Dankó, K. Four dermatomyositis-specific autoantibodies—anti-TIF1γ, anti-NXP2, anti-SAE and anti-MDA5—in adult and juvenile patients with idiopathic inflammatory myopathies in a Hungarian cohort. Autoimmun. Rev. 2014, 13, 1211–1219. [Google Scholar] [CrossRef] [PubMed]
- Damoiseaux, J.; Vulsteke, J.-B.; Tseng, C.-W.; Platteel, A.C.; Piette, Y.; Shovman, O.; Bonroy, C.; Hamann, D.; De Langhe, E.; Musset, L.; et al. Autoantibodies in idiopathic inflammatory myopathies: Clinical associations and laboratory evaluation by mono- and multispecific immunoassays. Autoimmun. Rev. 2019, 18, 293–305. [Google Scholar] [CrossRef]
- Betteridge, Z.; McHugh, N.J. Myositis-specific autoantibodies: An important tool to support diagnosis of myositis. J. Intern. Med. 2016, 280, 8–23. [Google Scholar] [CrossRef]
- Musset, L.; Allenbach, Y.; Benveniste, O.; Boyer, O.; Bossuyt, X.; Bentow, C.; Phillips, J.; Mammen, A.; Van Damme, P.; Westhovens, R.; et al. Anti-HMGCR antibodies as a biomarker for immune-mediated necrotizing myopathies: A history of statins and experience from a large international multi-center study. Autoimmun. Rev. 2016, 15, 983–993. [Google Scholar] [CrossRef]
- Allenbach, Y.; Keraen, J.; Bouvier, A.M.; Jooste, V.; Champtiaux, N.; Hervier, B.; Schoindre, Y.; Rigolet, A.; Gilardin, L.; Musset, L.; et al. High risk of cancer in autoimmune necrotizing myopathies: Usefulness of myositis specific antibody. Brain 2016, 139, 2131–2135. [Google Scholar] [CrossRef] [Green Version]
- Tiniakou, E.; Pinal-Fernandez, I.; Lloyd, T.E.; Albayda, J.; Paik, J.; Werner, J.L.; Parks, C.A.; Casciola-Rosen, L.; Christopher-Stine, L.; Mammen, A.L. More severe disease and slower recovery in younger patients with anti-3-hydroxy-3-methylglutaryl-coenzyme A reductase-associated autoimmune myopathy. Rheumatology 2017, 56, 787–794. [Google Scholar] [CrossRef] [Green Version]
- Chinoy, H.; Fertig, N.; Oddis, C.V.; Ollier, W.E.R.; Cooper, R.G. The diagnostic utility of myositis autoantibody testing for predicting the risk of cancer-associated myositis. Ann. Rheum. Dis. 2007, 66, 1345–1349. [Google Scholar] [CrossRef] [Green Version]
- Amoura, Z.; Duhaut, P.; Huong, D.L.T.; Wechsler, B.; Costedoat-Chalumeau, N.; Francès, C.; Cacoub, P.; Papo, T.; Cormont, S.; Touitou, Y.; et al. Tumor antigen markers for the detection of solid cancers in inflammatory myopathies. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1279–1282. [Google Scholar] [CrossRef] [Green Version]
- Whitmore, S.E.; Anhalt, G.J.; Provost, T.T.; Zacur, H.A.; Hamper, U.M.; Helzlsouer, K.J.; Rosenshein, N.B. Serum CA-125 screening for ovarian cancer in patients with dermatomyositis. Gynecol. Oncol. 1997, 65, 241–244. [Google Scholar] [CrossRef]
- Leatham, H.; Schadt, C.; Chisolm, S.; Fretwell, D.; Chung, L.; Callen, J.P.; Fiorentino, D. Evidence supports blind screening for internal malignancy in dermatomyositis: Data from 2 large US dermatology cohorts. Medicine 2018, 97, e9639. [Google Scholar] [CrossRef] [PubMed]
- Sparsa, A.; Liozon, E.; Herrmann, F.; Ly, K.; Lebrun, V.; Soria, P.; Loustaud-Ratti, V.; Bouyssou-Gauthier, M.-L.; Boulinguez, S.; Bédane, C.; et al. Routine vs. extensive malignancy search for adult dermatomyositis and polymyositis: A study of 40 patients. Arch. Dermatol. 2002, 138, 885–890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maliha, P.G.; Hudson, M.; Abikhzer, G.; Singerman, J.; Probst, S. 18F-FDG PET/CT versus conventional investigations for cancer screening in autoimmune inflammatory myopathy in the era of novel myopathy classifications. Nucl. Med. Commun. 2019, 40, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Selva-O’Callaghan, A.; Grau, J.M.; Gámez-Cenzano, C.; Vidaller-Palacín, A.; Martínez-Gómez, X.; Trallero-Araguás, E.; Andía-Navarro, E.; Vilardell-Tarrés, M. Conventional cancer screening versus PET/CT in dermatomyositis/polymyositis. Am. J. Med. 2010, 123, 558–562. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Opinc, A.H.; Makowska, J.S. Update on Malignancy in Myositis—Well-Established Association with Unmet Needs. Biomolecules 2022, 12, 111. https://doi.org/10.3390/biom12010111
Opinc AH, Makowska JS. Update on Malignancy in Myositis—Well-Established Association with Unmet Needs. Biomolecules. 2022; 12(1):111. https://doi.org/10.3390/biom12010111
Chicago/Turabian StyleOpinc, Aleksandra H., and Joanna S. Makowska. 2022. "Update on Malignancy in Myositis—Well-Established Association with Unmet Needs" Biomolecules 12, no. 1: 111. https://doi.org/10.3390/biom12010111
APA StyleOpinc, A. H., & Makowska, J. S. (2022). Update on Malignancy in Myositis—Well-Established Association with Unmet Needs. Biomolecules, 12(1), 111. https://doi.org/10.3390/biom12010111