
Leptomeningeal Carcinomatosis: A Clinical Dilemma in Neuroendocrine Neoplasms


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient and Tumor Characteristics
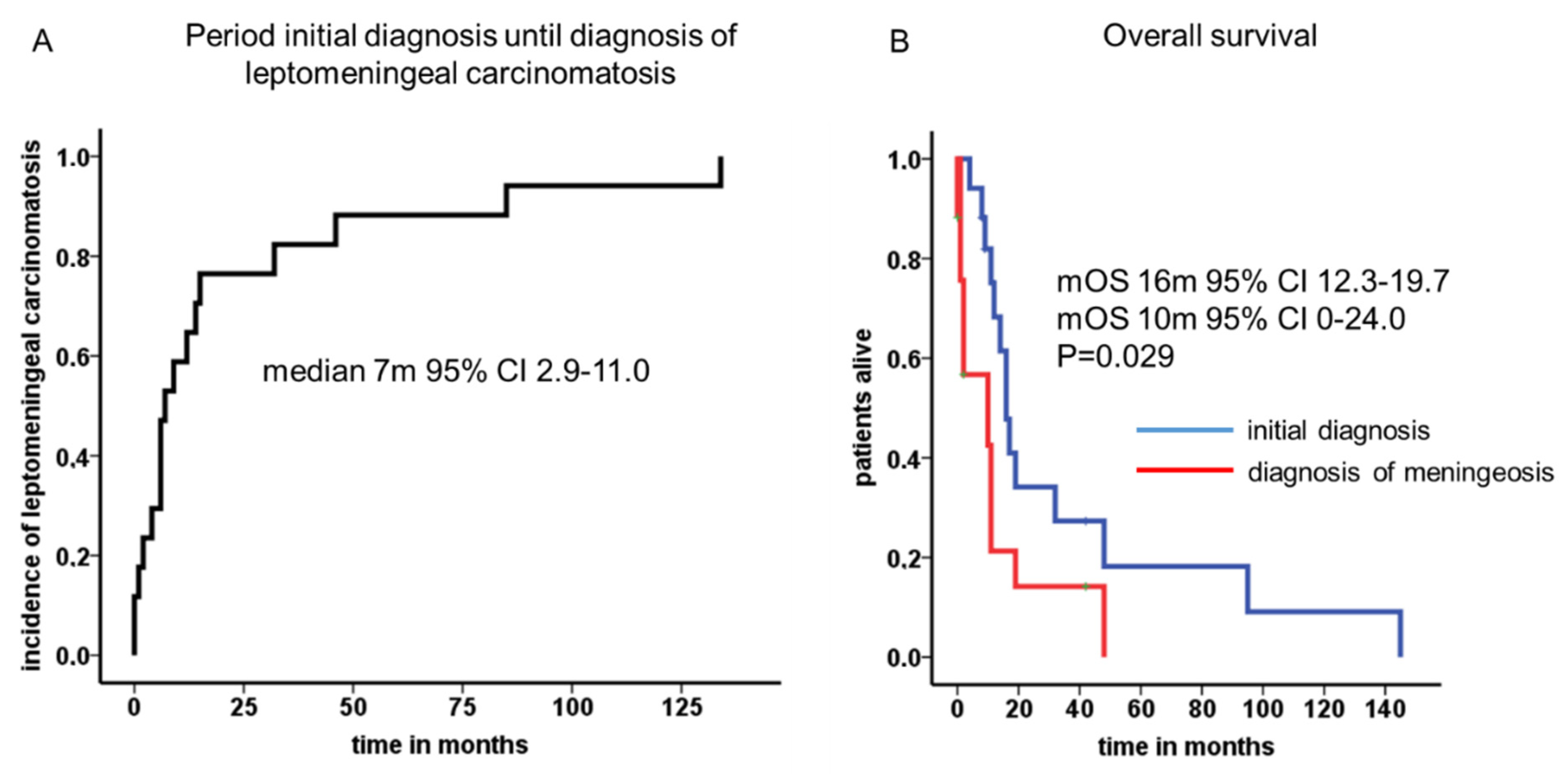
3.2. Latency First Diagnosis to Leptomeningeal Carcinomatosis
3.3. Specific Symptoms in Patients with Leptomeningeal Carcinomatosis
3.4. Tumor Stage at Diagnosis and Localization of Distant Metastases
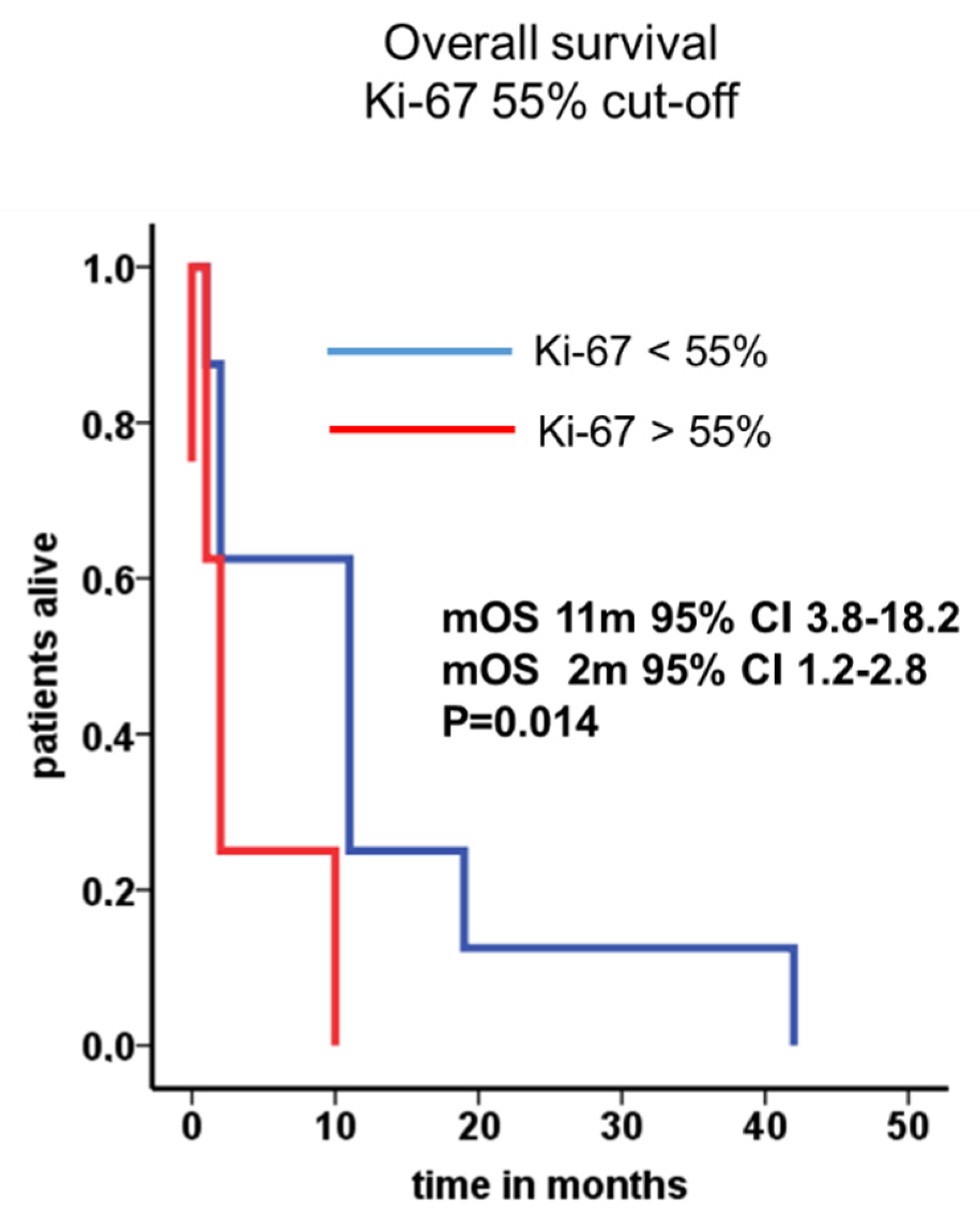
3.5. Treatment and Outcome Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kaplan, J.G.; DeSouza, T.G.; Farkash, A.; Shafran, B.; Pack, D.; Rehman, F.; Fuks, J.; Portenoy, R. Leptomeningeal metastases: Comparison of clinical features and laboratory data of solid tumors, lymphomas and leukemias. J. Neurooncol. 1990, 9, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Kesari, S.; Batchelor, T.T. Leptomeningeal metastases. Neurol. Clin. 2003, 21, 25–66. [Google Scholar] [CrossRef]
- Posner, J.B.; Chernik, N.L. Intracranial metastases from systemic cancer. Adv. Neurol. 1978, 19, 579–592. [Google Scholar]
- Clarke, J.L.; Perez, H.R.; Jacks, L.M.; Panageas, K.S.; Deangelis, L.M. Leptomeningeal metastases in the MRI era. Neurology 2010, 74, 1449–1454. [Google Scholar] [CrossRef] [PubMed]
- Leal, T.; Chang, J.E.; Mehta, M.; Robins, H.I. Leptomeningeal Metastasis: Challenges in Diagnosis and Treatment. Curr. Cancer Ther. Rev. 2011, 7, 319–327. [Google Scholar] [CrossRef]
- Clarke, J.L. Leptomeningeal metastasis from systemic cancer. Contin. Lifelong Learn. Neurol. 2012, 18, 328–342. [Google Scholar] [CrossRef]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef]
- Seute, T.; Leffers, P.; ten Velde, G.P.; Twijnstra, A. Neurologic disorders in 432 consecutive patients with small cell lung carcinoma. Cancer 2004, 100, 801–806. [Google Scholar] [CrossRef]
- Seute, T.; Leffers, P.; ten Velde, G.P.; Twijnstra, A. Leptomeningeal metastases from small cell lung carcinoma. Cancer 2005, 104, 1700–1705. [Google Scholar] [CrossRef] [PubMed]
- Krug, S.; Teupe, F.; Michl, P.; Gress, T.M.; Rinke, A. Brain metastases in patients with neuroendocrine neoplasms: Risk factors and outcome. BMC Cancer 2019, 19, 362. [Google Scholar] [CrossRef] [PubMed]
- Bourg, V.; Foa, C.; Largillier, R.; Gillet, J.Y.; Namer, M.; Magné, N. [Atypical presentation of carcinomatous meningitis in neuroendocrine tumor of the cervix uteri]. Presse Med. 2000, 29, 1763–1764. [Google Scholar] [PubMed]
- Isaka, T.; Maruno, M.; Sato, M.; Kinoshita, M.; Nishida, T.; Kiyohara, H.; Yoshimine, T. Brain metastasis from small-cell neuroendocrine carcinoma of the urinary bladder: A case report. Brain Tumor Pathol. 2002, 19, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Imboden, P.N.; Borruat, F.X.; De Tribolet, N.; Meagher-Villemure, K.; Pica, A.; Gomez, F. Non-functioning pituitary carcinoma. Pituitary 2004, 7, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Brownback, K.R.; Renzulli, J.; Delellis, R.; Myers, J.R. Small-cell prostate carcinoma: A retrospective analysis of five newly reported cases. Indian J. Urol. 2009, 25, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Komiyama, S.; Nishio, E.; Torii, Y.; Kawamura, K.; Oe, S.; Kato, R.; Hasagawa, K.; Abe, M.; Kuroda, M.; Udagawa, Y. A case of primary uterine cervical neuroendocrine tumor with meningeal carcinomatosis confirmed by diagnostic imaging and autopsy. Int. J. Clin. Oncol. 2011, 16, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Nakai, H.; Imaoka, I.; Murakami, T.; Hoshiai, H. Carcinomatous meningitis during systematic chemotherapy in a patient with advanced small-cell neuroendocrine carcinoma of the uterine cervix. J. Obstet. Gynaecol. Res. 2012, 38, 336–339. [Google Scholar] [CrossRef]
- Kumar, S.; Nair, S.; Alexander, M. Carcinomatous meningitis occurring prior to a diagnosis of large cell neuroendocrine carcinoma of the uterine cervix. J. Postgrad. Med. 2004, 50, 311–312. [Google Scholar]
- Bloom, J.R.; Brickman, A.; Yang, F.J.; Park, J.W.; Cheponis, J. Neuroendocrine carcinoma of the colon presenting as acute meningitis. BMC Neurol. 2019, 19, 76. [Google Scholar] [CrossRef] [PubMed]
- Thomson, N.; Pacak, K.; Schmidt, M.H.; Palmer, C.A.; Salzman, K.L.; Champine, M.; Schiffman, J.D.; Cohen, A.L. Leptomeningeal dissemination of a low-grade lumbar paraganglioma: Case report. J. Neurosurg. Spine 2017, 26, 501–506. [Google Scholar] [CrossRef]
- Paydas, S.; Bicakci, K.; Yavuz, S. Dramatic response with capecitabine after cranial radiation to the brain parenchymal and leptomeningeal metastases from lung cancer. Eur. J. Intern. Med. 2009, 20, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Xu, W.; Du, Z.; Sun, B.; Li, F.; Liu, Y. Pathologic Progression, Possible Origin, and Management of Multiple Primary Intracranial Neuroendocrine Carcinomas. World Neurosurg. 2017, 106, 1054.e13–1054.e17. [Google Scholar] [CrossRef]
- Versluis, J.M.; Brandsma, D.; van den Berg, J.G.; Tesselaar, M. Leptomeningeal metastases of a well-differentiated neuroendocrine tumour: A rare entity. BMJ Case Rep. 2018, 2018, bcr-2018-226557. [Google Scholar] [CrossRef]
- Saway, B.F.; Fayed, I.; Dowlati, E.; Derakhshandeh, R.; Sandhu, F.A. Initial Report of an Intradural Extramedullary Metastasis of a Pancreatic Neuroendocrine Tumor to the Cervical Spine: A Case Report and Review of the Literature. World Neurosurg. 2020, 139, 355–360. [Google Scholar] [CrossRef]
- Tuleasca, C.; Al-Risi, A.S.; David, P.; Adam, C.; Aghakhani, N.; Parker, F. Paragangliomas of the spine: A retrospective case series in a national reference French center. Acta Neurochir. 2020, 162, 831–837. [Google Scholar] [CrossRef]
- Andrioli, G.C.; Pennelli, N. [Meningeal carcinomatosis in malignant pheochromocytoma]. Acta Neurol. 1973, 28, 415–424. [Google Scholar]
- Roche, P.H.; Figarella-Branger, D.; Regis, J.; Peragut, J.C. Cauda equina paraganglioma with subsequent intracranial and intraspinal metastases. Acta Neurochir. 1996, 138, 475–479. [Google Scholar] [CrossRef]
- Balbuena-Merle, R.I.; Santé-Pérez, M.; Pérez-Berenguer, J.; Velez-Rosario, R.; Correa-Rivas, M.; Jiménez, A. Leptomeningeal Carcinomatosis as the Initial Manifestation of Metastatic Disease diagnosed in Postmortem Examination: A Case Series. P. R. Health Sci. J. 2019, 38, 64–67. [Google Scholar]
- Ko, Y.; Gwak, H.S.; Park, E.Y.; Joo, J.; Lee, Y.J.; Lee, S.H.; Kwon, J.W.; Shin, S.H.; Yoo, H. Association of MRI findings with clinical characteristics and prognosis in patients with leptomeningeal carcinomatosis from non-small cell lung cancer. J. Neurooncol. 2019, 143, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Franzoi, M.A.; Hortobagyi, G.N. Leptomeningeal carcinomatosis in patients with breast cancer. Crit. Rev. Oncol. Hematol. 2019, 135, 85–94. [Google Scholar] [CrossRef]
- Boch, M.; Rinke, A.; Rexin, P.; Seipelt, M.; Brödje, D.; Schober, M.; Gress, T.M.; Michl, P.; Krug, S. Paraneoplastic brainstem encephalitis in a patient with exceptionally long course of a metastasized neuroendocrine rectum neoplasm. BMC Cancer 2014, 14, 691. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Gesellschaft für Gastroenterologie Vr-uSD; (Patientenvertretung) NNTNeV; (Patientenvertretung) BSNTeVN-s; Deutsche Gesellschaft für Hämatologie und Medizinische Onkologie e.V. (DGHO) uAIOAdDKeV; (DGAV) DGfA-uVeV; (DGCH) DGfC; (DGEBV) DGfEuBV; (DGNM) DGfNeV; (DGIM) DGfIM; (DGE) DGfE; et al. Practice guideline neuroendocrine tumors—AWMF-Reg. 021-27. Z. Gastroenterol. 2018, 56, 583–681. [Google Scholar] [CrossRef]
- Le Rhun, E.; Weller, M.; Brandsma, D.; Van den Bent, M.; de Azambuja, E.; Henriksson, R.; Boulanger, T.; Peters, S.; Watts, C.; Wick, W.; et al. EANO-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up of patients with leptomeningeal metastasis from solid tumours. Ann. Oncol. 2017, 28, iv84–iv99. [Google Scholar] [CrossRef]
- van Bussel, M.T.J.; Pluim, D.; Milojkovic Kerklaan, B.; Bol, M.; Sikorska, K.; Linders, D.T.C.; van den Broek, D.; Beijnen, J.H.; Schellens, J.H.M.; Brandsma, D. Circulating epithelial tumor cell analysis in CSF in patients with leptomeningeal metastases. Neurology 2020, 94, e521–e528. [Google Scholar] [CrossRef]
- Zhao, Y.; He, J.Y.; Zou, Y.L.; Guo, X.S.; Cui, J.Z.; Guo, L.; Bu, H. Evaluating the cerebrospinal fluid ctDNA detection by next-generation sequencing in the diagnosis of meningeal Carcinomatosis. BMC Neurol. 2019, 19, 331. [Google Scholar] [CrossRef]
- Le Rhun, E.; Taillibert, S.; Zairi, F.; Kotecki, N.; Devos, P.; Mailliez, A.; Servent, V.; Vanlemmens, L.; Vennin, P.; Boulanger, T.; et al. A retrospective case series of 103 consecutive patients with leptomeningeal metastasis and breast cancer. J. Neurooncol. 2013, 113, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, H.; Guilhaume, M.N.; Bidard, F.C.; Pierga, J.Y.; Girre, V.; Cottu, P.H.; Laurence, V.; Livartowski, A.; Mignot, L.; Diéras, V. Survival of breast cancer patients with meningeal carcinomatosis. Ann. Oncol. 2010, 21, 2183–2187. [Google Scholar] [CrossRef]
- Grossman, S.A.; Finkelstein, D.M.; Ruckdeschel, J.C.; Trump, D.L.; Moynihan, T.; Ettinger, D.S. Randomized prospective comparison of intraventricular methotrexate and thiotepa in patients with previously untreated neoplastic meningitis. Eastern Cooperative Oncology Group. J. Clin. Oncol. 1993, 11, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Glantz, M.J.; Cole, B.F.; Recht, L.; Akerley, W.; Mills, P.; Saris, S.; Hochberg, F.; Calabresi, P.; Egorin, M.J. High-dose intravenous methotrexate for patients with nonleukemic leptomeningeal cancer: Is intrathecal chemotherapy necessary? J. Clin. Oncol. 1998, 16, 1561–1567. [Google Scholar] [CrossRef]
- Cole, B.F.; Glantz, M.J.; Jaeckle, K.A.; Chamberlain, M.C.; Mackowiak, J.I. Quality-of-life-adjusted survival comparison of sustained-release cytosine arabinoside versus intrathecal methotrexate for treatment of solid tumor neoplastic meningitis. Cancer 2003, 97, 3053–3060. [Google Scholar] [CrossRef] [PubMed]
- Comte, A.; Jdid, W.; Guilhaume, M.N.; Kriegel, I.; Piperno-Neumann, S.; Dieras, V.; Dorval, T.; Pierga, J.Y.; Cottu, P.H.; Mignot, L.; et al. Survival of breast cancer patients with meningeal carcinomatosis treated by intrathecal thiotepa. J. Neurooncol. 2013, 115, 445–452. [Google Scholar] [CrossRef]
- Le Rhun, E.; Taillibert, S.; Devos, P.; Zairi, F.; Turpin, A.; Rodrigues, I.; Cazin, J.L.; Pierret, M.F.; André, C.; Dubois, F.; et al. Salvage intracerebrospinal fluid thiotepa in breast cancer-related leptomeningeal metastases: A retrospective case series. Anticancer Drugs 2013, 24, 1093–1097. [Google Scholar] [CrossRef] [PubMed]
- Welin, S.; Sorbye, H.; Sebjornsen, S.; Knappskog, S.; Busch, C.; Oberg, K. Clinical effect of temozolomide-based chemotherapy in poorly differentiated endocrine carcinoma after progression on first-line chemotherapy. Cancer 2011, 117, 4617–4622. [Google Scholar] [CrossRef]
- Segura, P.P.; Gil, M.; Balañá, C.; Chacón, I.; Langa, J.M.; Martín, M.; Bruna, J. Phase II trial of temozolomide for leptomeningeal metastases in patients with solid tumors. J. Neurooncol. 2012, 109, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Brastianos, P.K.; Lee, E.Q.; Cohen, J.V.; Tolaney, S.M.; Lin, N.U.; Wang, N.; Chukwueke, U.; White, M.D.; Nayyar, N.; Kim, A.; et al. Single-arm, open-label phase 2 trial of pembrolizumab in patients with leptomeningeal carcinomatosis. Nat. Med. 2020, 26, 1280–1284. [Google Scholar] [CrossRef] [PubMed]
- Asensio, N.; Luis, A.; Costa, I.; Oliveira, J.; Vaz, F. Meningeal carcinomatosis and uterine carcinoma: Three different clinical settings and review of the literature. Int. J. Gynecol. Cancer 2009, 19, 168–172. [Google Scholar] [CrossRef]
- Sahu, K.K.; Mishra, A.K.; Sherif, A.A.; Doshi, A.; Koirala, B. An interesting case of pacemaker endocarditis. Neth. Heart J. 2019, 27, 581–582. [Google Scholar] [CrossRef] [PubMed]
- Strommer, K.N.; Brandner, S.; Sarioglu, A.C.; Sure, U.; Yonekawa, Y. Symptomatic cerebellar metastasis and late local recurrence of a cauda equina paraganglioma. Case report. J. Neurosurg. 1995, 83, 166–169. [Google Scholar] [CrossRef]
- Yang, G.; Pan, Z.; Ma, N.; Qu, L.; Yuan, T.; Pang, X.; Yang, X.; Dong, L.; Liu, S. Leptomeningeal metastasis of pulmonary large-cell neuroendocrine carcinoma: A case report and review of the literature. Oncol. Lett. 2017, 14, 4282–4286. [Google Scholar] [CrossRef] [PubMed]
- Pan, Z.; Yang, G.; Wang, Y.; He, H.; Pang, X.; Gao, Y.; Shi, W.; Li, Y.; Dong, L.; Song, Y. Thinprep plus Papanicolaou stain method is more sensitive than cytospin-coupled Wright Giems stain method in cerebrospinal fluid cytology for diagnosis of leptomeningeal metastasis from solid tumors. PLoS ONE 2015, 10, e0122016. [Google Scholar] [CrossRef]
- Tsimpas, A.; Post, N.H.; Moshel, Y.; Frempong-Boadu, A.K. Large cell neuroendocrine carcinoma of the lung metastatic to the cauda equina. Spine J. 2010, 10, e1–e5. [Google Scholar] [CrossRef] [PubMed]
- Patchell, R.A.; Posner, J.B. Neurologic complications of carcinoid. Neurology 1986, 36, 745–749. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Forbes, J.A.; Carr, K.; Highfield Nickols, H.; Utz, A.; Moots, P.; Weaver, K. Response of silent corticotroph pituitary carcinoma to chemotherapy: Case report. J. Neurosurg. Sci. 2016, 60, 272–280. [Google Scholar]
- Okoye, E.; Choi, E.K.; Divatia, M.; Miles, B.J.; Ayala, A.G.; Ro, J.Y. De novo large cell neuroendocrine carcinoma of the prostate gland with pelvic lymph node metastasis: A case report with review of literature. Int. J. Clin. Exp. Pathol. 2014, 7, 9061–9066. [Google Scholar] [PubMed]
- Lyster, M.T.; Kies, M.S.; Kuzel, T.M. Neurologic complications of patients with small cell prostate carcinoma. Report of two cases. Cancer 1994, 74, 3159–3163. [Google Scholar] [CrossRef]
- Dagan, R.; Bryant, C.M.; Mendenhall, W.M.; Amdur, R.J.; Morris, C.G.; Lanza, D.C.; Dziegielewski, P.T.; Justice, J.M.; Lobo, B.C.; Silver, N.L.; et al. Isolated leptomeningeal progression from sinonasal carcinomas: Implications for staging workup and treatment. Head Neck 2019, 41, 2647–2654. [Google Scholar] [CrossRef]
- Cuvilliers, C.; Ahrweiller, F.; Vauléon, E.; Castelli, J.; Palard-Novello, X. FDG PET in Diffuse Spinal Carcinomatous Meningitis. Clin. Nucl. Med. 2019, 44, e418–e419. [Google Scholar] [CrossRef]
- Chang, D.T.; Mancuso, A.A.; Riggs, C.E.; Mendenhall, W.M. Merkel cell carcinoma of the skin with leptomeningeal metastases. Am. J. Otolaryngol. 2005, 26, 210–213. [Google Scholar] [CrossRef] [PubMed]
- Abul-Kasim, K.; Söderström, K.; Hallsten, L. Extensive central nervous system involvement in Merkel cell carcinoma: A case report and review of the literature. J. Med. Case Rep. 2011, 5, 35. [Google Scholar] [CrossRef] [PubMed]
- Snodgrass, S.M.; Landy, H.; Markoe, A.M.; Feun, L. Neurologic complications of Merkel cell carcinoma. J. Neurooncol. 1994, 22, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Eggers, S.D.; Salomao, D.R.; Dinapoli, R.P.; Vernino, S. Paraneoplastic and metastatic neurologic complications of Merkel cell carcinoma. Mayo Clin. Proc. 2001, 76, 327–330. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number of All Patients (%) |
|---|---|
| Total | 17 |
| Mean age at first diagnosis (years) (range) | 55 (27–73) |
| Mean age at diagnosis of leptomeningeal carcinomatosis (years) (range) | 57 (27–73) |
| Primary tumor localization | |
| lung | 3 (17.6) |
| CUP | 7 (41.2) |
| pancreas | 3 (17.6) |
| gastrointestinal tract | 2 (11.8) |
| cervix/prostate | 2 (11.8) |
| Gender | |
| male | 9 (52.9) |
| female | 8 (47.1) |
| Histology WHO 2010 | |
| well/moderately differentiated | 3 (17.6) |
| poorly differentiated | 14 (82.4) |
| unknown | 0 |
| Ki-67 index | |
| G1 (≤2%) | 0 |
| G2 (3–20%) | 3 (17.6) |
| G3 (>20%) | 13 (76.5) |
| <55% | 5 (29.4) |
| >55% | 8 (47.1) |
| unknown | 1 (5.9) |
| Sites of non-meningeal metastases | |
| Brain | 9 (53.9) |
| Liver | 9 (53.9) |
| lymph nodes | 10 (58.8) |
| bone | 9 (53.9) |
| lung/pleural | 4 (23.6) |
| none | 1 (5.9) |
| other | 4 (23.6) |
| Meningeosis confirmed by | |
| Symptoms and radiology | 12 (70.6) |
| CSF cytology | 5 (29.4) |
| Therapy of LC | |
| radiation | 11 (64.7) |
| intrathecal CTx | 2 (11.8) |
| temozolomide-based CTx | 5 (29.4) |
| Symptoms | n | % |
| Headaches | 1/17 | 5.9 |
| Nausea | 1/17 | 5.9 |
| Paraparesis | 3/17 | 17.6 |
| Paresthesia | 3/17 | 17.6 |
| Visual impairment | 3/17 | 17.6 |
| Incontinence | 2/17 | 11.8 |
| None | 2/17 | 11.8 |
| Others | 5/17 | 29.4 |
| Reference | Primary | Histology | Treatment | OS after LC (Months) | Follow-Up after LC (Months) |
|---|---|---|---|---|---|
| [25] | Adrenal gland | Pheochromocytoma | NR | NR | NR |
| [45] | Cervix uteri | NEC | RT, CTx | 7.0 | 7.0 |
| [17] | Cervix uteri | NEC | NR | NR | NR |
| [16] | Cervix uteri | NEC | BSC | 0.5 | 0.5 |
| [15] | Cervix uteri | Atypical carcinoid | RT | 0.3 | 0.3 |
| [11] | Cervix uteri | NEC | NR | NR | NR |
| [18] | Colon | NEC | BSC | 0.2 | 0.2 |
| [19] | Intraspinal | Paraganglioma | RT, intrathecal CTx (ThioTEPA), CTx (temozolomide, capecitabine) | NR | 36.0 |
| [24] | Intraspinal | Paraganglioma | Surgery, RT | NR | 132.0 |
| [24] | Intraspinal | Paraganglioma | Surgery, RT, CTx | NR | 30.0 |
| [24] | Intraspinal | Paraganglioma | Surgery | NR | 144.0 |
| [46] | Intraspinal | Paraganglioma | NR | NR | NR |
| [26] | Intraspinal | Paraganglioma | Surgery, RT | 4.5 | 4.5 |
| [47] | Intraspinal | Paraganglioma | Surgery | NR | 12.0 |
| [48] | Lung | LCNEC | RT, intrathecal CTx (MTX, dexamethasone) | 4.9 | 4.9 |
| [20] | Lung | LCNEC | RT, CTx (capecitabine) | NR | 9.0 |
| [49] | Lung | LCNEC | NR | NR | NR |
| [50] | Lung | LCNEC | Surgery, RT | NR | 12.0 |
| [51] | NR | Carcinoid | NR | NR | NR |
| [10] | Pancreas | NEC | BSC | 1.0 | 1.0 |
| [22] | Pancreas | NET G1 | RT | 4.0 | 4.0 |
| [23] | Pancreas | NET G2 | Surgery | NR | 0.5 |
| [52] | Pituitary | Pituitary carcinoma | CTx (carboplatin, etoposide) | NR | NR |
| [13] | Pituitary | Pituitary carcinoma | BSC | 0.3 | 0.3 |
| [53] | Prostate | LCNEC | BSC | 1.0 | 1.0 |
| [14] | Prostate | NEC | Intrathecal CTx (MTX) | NR | NR |
| [54] | Prostate | SCNEC | Surgery, RT | NR | NR |
| [54] | Prostate | SCNEC | RT | 2.0? | 2.0? |
| [55] | Sinunasal | NEC | RT, CTx | 35.3 | 35.3 |
| [55] | Sinunasal | MiNEN | RT, CTx | 4.5 | 4.5 |
| [55] | Sinunasal | MiNEN | BSC | 4.9 | 4.9 |
| [55] | Sinunasal | SCNEC | RT, CTx | 2.8 | 2.8 |
| [56] | Sinunasal | NEC | NR | NR | NR |
| [57] | Skin | MCC | Intrathecal CTx (MTX), CTx (ifosfamide), RT | NR | 1.0 |
| [58] | Skin | MCC | RT | 8.0 | 8.0 |
| [59] | Skin | MCC | RT, intrathecal CTx | 6.0 | 6.0 |
| [60] | Skin | MCC | RT | 6.0 | 6.0 |
| [21] | Unclear | NEC | Surgery, RT, CTx (temozolomide, endostatin) | NR | 10.0 |
| [12] | Bladder | SCNEC | Intrathecal CTx, RT | 0.9 | 0.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Apostolidis, L.; Schrader, J.; Jann, H.; Rinke, A.; Krug, S. Leptomeningeal Carcinomatosis: A Clinical Dilemma in Neuroendocrine Neoplasms. Biology 2021, 10, 277. https://doi.org/10.3390/biology10040277
Apostolidis L, Schrader J, Jann H, Rinke A, Krug S. Leptomeningeal Carcinomatosis: A Clinical Dilemma in Neuroendocrine Neoplasms. Biology. 2021; 10(4):277. https://doi.org/10.3390/biology10040277
Chicago/Turabian StyleApostolidis, Leonidas, Jörg Schrader, Henning Jann, Anja Rinke, and Sebastian Krug. 2021. "Leptomeningeal Carcinomatosis: A Clinical Dilemma in Neuroendocrine Neoplasms" Biology 10, no. 4: 277. https://doi.org/10.3390/biology10040277
APA StyleApostolidis, L., Schrader, J., Jann, H., Rinke, A., & Krug, S. (2021). Leptomeningeal Carcinomatosis: A Clinical Dilemma in Neuroendocrine Neoplasms. Biology, 10(4), 277. https://doi.org/10.3390/biology10040277