
Evaluate the Effectiveness of Outpatient Parenteral Antimicrobial Therapy (OPAT) Program in Saudi Arabia: A Retrospective Study

 , , ,
, , ,  , and
, and
Abstract
1. Introduction
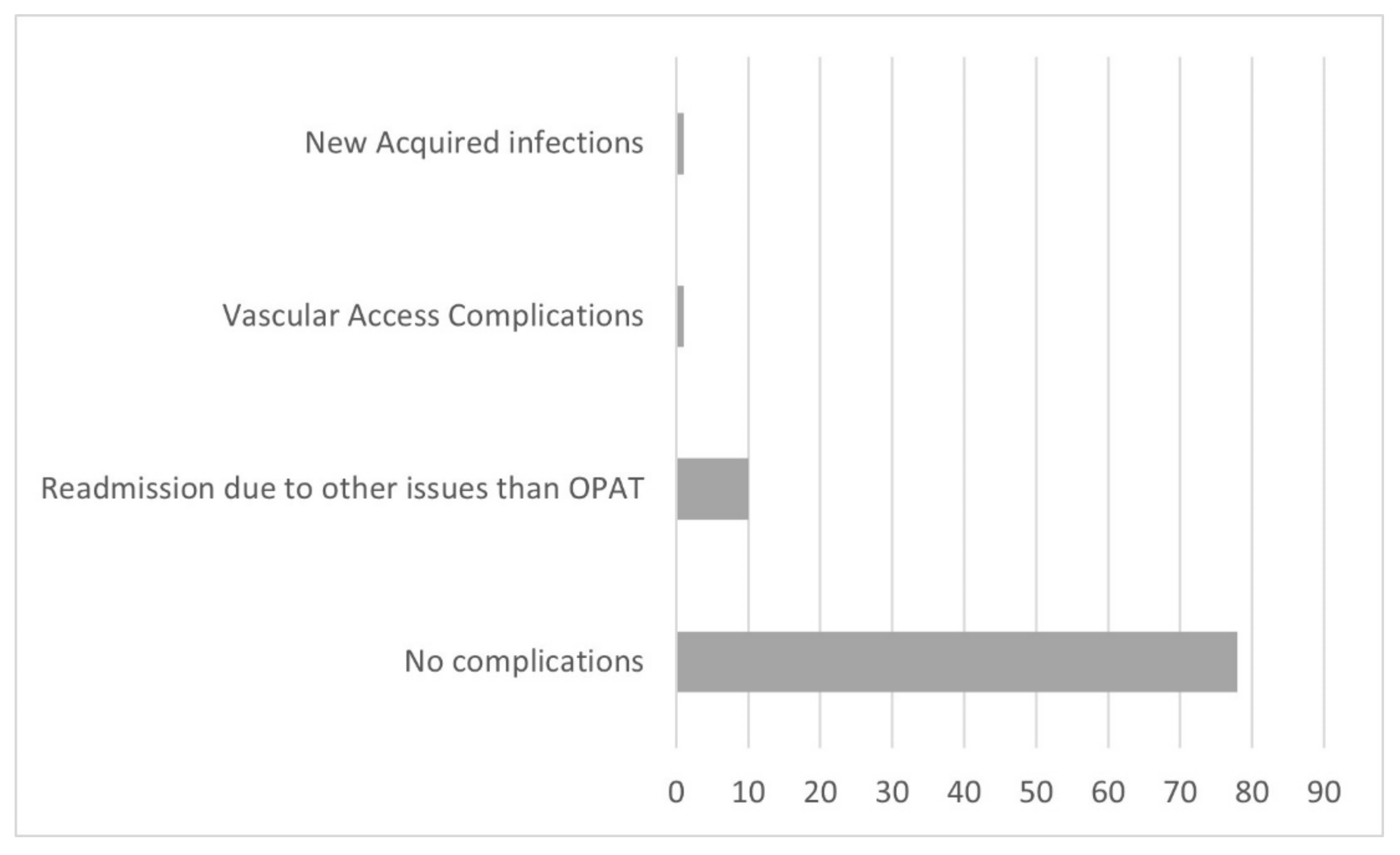
2. Results
3. Discussion
4. Methods
4.1. Study Design and Duration
4.2. Study Population
4.3. Inclusion Criterion
4.4. Data Collection
4.5. Ethics Approval
4.6. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Babiker, A.; El Husseini, M.; Al Nemri, A.; Al Frayh, A.; Al Juryyan, N.; Faki, M.O.; Assiri, A.; Al Saadi, M.; Shaikh, F.; Al Zamil, F. Health care professional development: Working as a team to improve patient care. Sudan. J. Paediatr. 2014, 14, 9. [Google Scholar] [PubMed]
- Friedman, C.; Newsom, W. The Costs of Healthcare-Associated Infections. In IFIC Basic Concepts of Infection Control; International Federation of Infection Control: Portadown, UK, 2011; ISBN 978-0-9555861-0-1. [Google Scholar]
- Laupland, K.B.; Valiquette, L. Outpatient parenteral antimicrobial therapy. Can. J. Infect. Dis. Med. Microbiol. 2013, 24, 9–11. [Google Scholar] [CrossRef] [PubMed]
- Rucker, R.W.; Harrison, G.M. Outpatient intravenous medications in the management of cystic fibrosis. Pediatrics 1974, 54, 358–360. [Google Scholar] [CrossRef] [PubMed]
- Poretz, D.M.; Eron, L.J.; Goldenberg, R.I.; Gilbert, A.F.; Rising, J.; Sparks, S.; Horn, C.E. Intravenous antibiotic therapy in an outpatient setting. JAMA 1982, 248, 336–339. [Google Scholar] [CrossRef]
- Gilchrist, M.; Franklin, B.D.; Patel, J.P. An outpatient parenteral antibiotic therapy (OPAT) map to identify risks associated with an OPAT service. J. Antimicrob. Chemother. 2008, 62, 177–183. [Google Scholar] [CrossRef]
- Yadav, K.; Mattice, A.M.; Yip, R.; Rosenberg, H.; Taljaard, M.; Nemnom, M.-J.; Ohle, R.; Yan, J.; Suh, K.N.; Stiell, I.G. The impact of an outpatient parenteral antibiotic therapy (OPAT) clinic for adults with cellulitis: An interrupted time series study. Intern. Emerg. Med. 2021, 7, 1935–1944. [Google Scholar] [CrossRef]
- Revelas, A. Healthcare-associated infections: A public health problem. Niger. Med. J. 2012, 53, 59. [Google Scholar] [CrossRef]
- Yan, M.; Elligsen, M.; Simor, A.E.; Daneman, N. Patient characteristics and outcomes of outpatient parenteral antimicrobial therapy: A retrospective study. Can. J. Infect. Dis. Med. Microbiol. 2016, 2016, 8435257. [Google Scholar] [CrossRef]
- Bugeja, S.J.; Stewart, D.; Vosper, H. Clinical benefits and costs of an outpatient parenteral antimicrobial therapy service. Res. Soc. Adm. Pharm. 2021, 17, 1758–1763. [Google Scholar] [CrossRef]
- Norris, A.H.; Shrestha, N.K.; Allison, G.M.; Keller, S.C.; Bhavan, K.P.; Zurlo, J.J.; Hersh, A.L.; Gorski, L.A.; Bosso, J.A.; Rathore, M.H. 2018 Infectious Diseases Society of America clinical practice guideline for the management of outpatient parenteral antimicrobial therapy. Clin. Infect. Dis. 2018, 68, e1–e35. [Google Scholar] [CrossRef]
- Farmer, E.C.W.; Seaton, R.A. Recent innovations and new applications of outpatient parenteral antimicrobial therapy. Expert Rev. Anti-Infect. Ther. 2021, 19, 55–64. [Google Scholar] [CrossRef]
- Schmidt, M.; Hearn, B.; Gabriel, M.; Spencer, M.D.; McCurdy, L. Predictors of unplanned hospitalization in patients receiving outpatient parenteral antimicrobial therapy across a large integrated healthcare network. Open Forum Infect. Dis. 2017, 4, ofx086. [Google Scholar] [CrossRef]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O. Implementing an antibiotic stewardship program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef]
- Mitchell, E.; Murray, C.C.; Meads, D.; Minton, J.; Wright, J.; Twiddy, M. Clinical and cost-effectiveness, safety and acceptability of community intravenous antibiotic service models: CIVAS systematic review. BMJ Open 2017, 7, e013560. [Google Scholar] [CrossRef]
- Chapman, A.L.; Dixon, S.; Andrews, D.; Lillie, P.J.; Bazaz, R.; Patchett, J.D. Clinical efficacy and cost-effectiveness of outpatient parenteral antibiotic therapy (OPAT): A UK perspective. J. Antimicrob. Chemother. 2009, 64, 1316–1324. [Google Scholar] [CrossRef]
- Durojaiye, O.C.; Bell, H.; Andrews, D.; Ntziora, F.; Cartwright, K. Clinical efficacy, cost analysis and patient acceptability of outpatient parenteral antibiotic therapy (OPAT): A decade of Sheffield (UK) OPAT service. Int. J. Antimicrob. Agents 2018, 51, 26–32. [Google Scholar] [CrossRef]
- Appa, A.; Marquez, C.; Jain, V. Home-Based Outpatient Parenteral Antibiotic Therapy at an Urban Safety Net Hospital: Comparing Outcomes in Persons with and without Noninjection Drug Use. Open Forum Infect. Dis. 2020, 7, ofaa162. [Google Scholar] [CrossRef]
- Kayley, J.; Berendt, A.; Snelling, M.; Moore, H.; Hamilton, H.; Peto, T.; Crook, D.; Conlon, C. Safe intravenous antibiotic therapy at home: Experience of a UK based programme. J. Antimicrob. Chemother. 1996, 37, 1023–1029. [Google Scholar] [CrossRef][Green Version]
- Rahman, R. The privatization of health care system in Saudi Arabia. Health Serv. Insights 2020, 13, 1178632920934497. [Google Scholar] [CrossRef]
- Mahmood, R.K.; Gillani, S.W.; Saeed, M.W.; Hafeez, M.U.; Gulam, S.M. Systematic Review: Study of the Prescribing Pattern of Antibiotics in Outpatients and Emergency Departments in the Gulf Region. Front. Pharmacol. 2020, 11, 1926. [Google Scholar] [CrossRef]
- Dimitrova, M.; Gilchrist, M.; Seaton, R. Outpatient parenteral antimicrobial therapy (OPAT) versus inpatient care in the UK: A health economic assessment for six key diagnoses. BMJ Open 2021, 11, e049733. [Google Scholar] [CrossRef]
- Quintens, C.; Steffens, E.; Jacobs, K.; Schuermans, A.; Van Eldere, J.; Lagrou, K.; De Munter, P.; Derdelinckx, I.; Peetermans, W.E.; Spriet, I. Efficacy and safety of a Belgian tertiary care outpatient parenteral antimicrobial therapy (OPAT) program. Infection 2020, 48, 357–366. [Google Scholar] [CrossRef]
- Esposito, S.; Noviello, S.; Leone, S.; Tice, A.; Seibold, G.; Nathwani, D.; Scaglione, F.; Registry, I.O. Outpatient parenteral antibiotic therapy (OPAT) in different countries: A comparison. Int. J. Antimicrob. Agents 2004, 24, 473–478. [Google Scholar] [CrossRef]
- Chapman, A.L.; Seaton, R.A.; Cooper, M.A.; Hedderwick, S.; Goodall, V.; Reed, C.; Sanderson, F.; Nathwani, D. Good practice recommendations for outpatient parenteral antimicrobial therapy (OPAT) in adults in the UK: A consensus statement. J. Antimicrob. Chemother. 2012, 67, 1053–1062. [Google Scholar] [CrossRef]
- Carter, B.; Fisher-Smith, D.; Porter, D.; Lane, S.; Peak, M.; Taylor-Robinson, D.; Bracken, L.; Carrol, E.D. Paediatric Outpatient Parenteral Antimicrobial Therapy (OPAT): An e-survey of the experiences of parents and clinicians. PLoS ONE 2021, 16, e0249514. [Google Scholar] [CrossRef]
- Hamad, Y.; Joynt Maddox, K.E.; Powderly, W.G. COVID-19 and outpatient parenteral antimicrobial therapy: The need to protect vulnerable Medicare beneficiaries. Ann. Intern. Med. 2020, 173, 383–384. [Google Scholar] [CrossRef]
- Lorgelly, P.K.; Atkinson, M.; Lakhanpaul, M.; Smyth, A.R.; Vyas, H.; Weston, V.; Stephenson, T. Oral versus iv antibiotics for community-acquired pneumonia in children: A cost-minimisation analysis. Eur. Respir. J. 2010, 35, 858–864. [Google Scholar] [CrossRef]
- Hiew, J.; Whitmore, T.; McEvoy, M.; Weatherall, D.; Ingram, P.R.; Manning, L. Subcutaneous ertapenem delivered by an Australian outpatient parenteral antimicrobial therapy service: A retrospective comparative efficacy study. Intern. Med. J. 2021, 51, 1717–1721. [Google Scholar] [CrossRef] [PubMed]
- Nazli Zeka, A.; Avkan-Oguz, V.; Irmak, C.; Eren Kutsoylu, O.; Alp Cavus, S.; Kuruüzüm, Z.; Ergon, M.C. Daily inpatient ertapenem therapy can be an alternative to hospitalization for the treatment of complicated urinary tract infections during the COVID-19 pandemic. Int. J. Clin. Pract. 2021, 75, e14230. [Google Scholar] [CrossRef] [PubMed]
- Grattan, K.S.; Mohamed Ali, M.; Hosseini-Moghaddam, S.M.; Gilmour, H.J.; Crunican, G.P.; Hua, E.; Muhsin, K.A.; Johnstone, R.; Bondy, L.C.; Devlin, M.K. Evaluating the safety and effectiveness of a nurse-led outpatient virtual IV vancomycin monitoring clinic: A retrospective cohort study. JAC Antimicrob. Resist. 2021, 3, dlaa113. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, M.; Rae, N.; Nathwani, D. Outcomes from global adult outpatient parenteral antimicrobial therapy programmes: A review of the last decade. Int. J. Antimicrob. Agents 2014, 43, 7–16. [Google Scholar] [CrossRef]
- Gardiol, C.; Voumard, R.; Cochet, C.; de Vallière, S. Setting up an outpatient parenteral antimicrobial therapy (OPAT) unit in Switzerland: Review of the first 18 months of activity. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 839–845. [Google Scholar] [CrossRef]
- Means, L.; Bleasdale, S.; Sikka, M.; Gross, A.E. Predictors of hospital readmission in patients receiving outpatient parenteral antimicrobial therapy. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2016, 36, 934–939. [Google Scholar] [CrossRef]
- Huang, V.; Ruhe, J.J.; Lerner, P.; Fedorenko, M. Risk factors for readmission in patients discharged with outpatient parenteral antimicrobial therapy: A retrospective cohort study. BMC Pharmacol. Toxicol. 2018, 19, 50. [Google Scholar] [CrossRef]


{kind=link}
| Diagnosis | Number of Patients | Percentage (%) |
|---|---|---|
| Urinary tract infection | 25 | 26.9 |
| Osteomyelitis | 16 | 17.2 |
| Bacteremia (any source) | 15 | 16.1 |
| Endocarditis | 6 | 6.5 |
| Brucellosis | 4 | 4.3 |
| Tuberculosis | 4 | 4.3 |
| Hepatic microabscess | 5 | 5.4 |
| Diabetic foot | 2 | 2.2 |
| Pyomyositis | 1 | 1.1 |
| Respiratory infection | 1 | 1.1 |
| Septic arthritis | 1 | 1.1 |
| other | 10 | 10.8 |
| Microorganisms | Number of Patients | Percentage (%) |
|---|---|---|
| ESBL E. coli | 40 | 44.9 |
| MRSA | 15 | 16.9 |
| MSSA | 12 | 13.4 |
| Brucella | 4 | 4.5 |
| Mycobacterium tuberculosis | 4 | 4.5 |
| Candida | 3 | 3.4 |
| ESBL K. pneumoniae | 2 | 2.2 |
| Streptococcus mitis | 2 | 2.2 |
| Pseudomonas aeruginosa | 2 | 2.2 |
| CRE K. pneumoniae | 1 | 1.1 |
| CRE E. coli | 1 | 1.1 |
| CoNS | 1 | 1.1 |
| E. cloace | 1 | 1.1 |
| K. pneumoniae | 1 | 1.1 |
| GNB | 1 | 1.1 |
| Antibiotics | Number of Patients | Percentage (%) |
|---|---|---|
| Ertapenem | 40 | 43.0 |
| Vancomycin | 11 | 11.2 |
| Cloxacillin/Flucloxacillin | 9 | 9.7 |
| Gentamycin | 4 | 4.3 |
| Ceftriaxone | 4 | 4.4 |
| Anidulafungin | 4 | 4.4 |
| Cefepime | 3 | 3.2 |
| Meropenem | 3 | 3.2 |
| Amikacin | 2 | 2.2 |
| Cefazolin | 2 | 2.2 |
| Teicoplanin | 2 | 2.2 |
| Ampicillin/sulbactam | 1 | 1.1 |
| Ceftazidime/Avibactam | 1 | 1.1 |
| Flucloxacillin/Rifampin | 1 | 1.1 |
| Piperacillin/tazobactam | 1 | 1.1 |
| Rifampicin/Levofloxacin/Amikacin | 1 | 1.1 |
| Tigecycline | 1 | 1.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Shareef, H.J.; Al Harbi, A.; Alatawi, Y.; Aljabri, A.; Al-Ghanmi, M.A.; Alzahrani, M.S.; Algarni, M.A.; Khobrani, A.; Haseeb, A.; AlSenani, F.; et al. Evaluate the Effectiveness of Outpatient Parenteral Antimicrobial Therapy (OPAT) Program in Saudi Arabia: A Retrospective Study. Antibiotics 2022, 11, 441. https://doi.org/10.3390/antibiotics11040441
Al Shareef HJ, Al Harbi A, Alatawi Y, Aljabri A, Al-Ghanmi MA, Alzahrani MS, Algarni MA, Khobrani A, Haseeb A, AlSenani F, et al. Evaluate the Effectiveness of Outpatient Parenteral Antimicrobial Therapy (OPAT) Program in Saudi Arabia: A Retrospective Study. Antibiotics. 2022; 11(4):441. https://doi.org/10.3390/antibiotics11040441
Chicago/Turabian StyleAl Shareef, Haneen J., Adnan Al Harbi, Yasser Alatawi, Ahmed Aljabri, Mohammed A. Al-Ghanmi, Mohammed S. Alzahrani, Majed Ahmed Algarni, Attiah Khobrani, Abdul Haseeb, Faisal AlSenani, and et al. 2022. "Evaluate the Effectiveness of Outpatient Parenteral Antimicrobial Therapy (OPAT) Program in Saudi Arabia: A Retrospective Study" Antibiotics 11, no. 4: 441. https://doi.org/10.3390/antibiotics11040441
APA StyleAl Shareef, H. J., Al Harbi, A., Alatawi, Y., Aljabri, A., Al-Ghanmi, M. A., Alzahrani, M. S., Algarni, M. A., Khobrani, A., Haseeb, A., AlSenani, F., & Elrggal, M. E. (2022). Evaluate the Effectiveness of Outpatient Parenteral Antimicrobial Therapy (OPAT) Program in Saudi Arabia: A Retrospective Study. Antibiotics, 11(4), 441. https://doi.org/10.3390/antibiotics11040441