Spirit-Quieting Traditional Chinese Medicine May Improve Survival in Prostate Cancer Patients with Depression

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
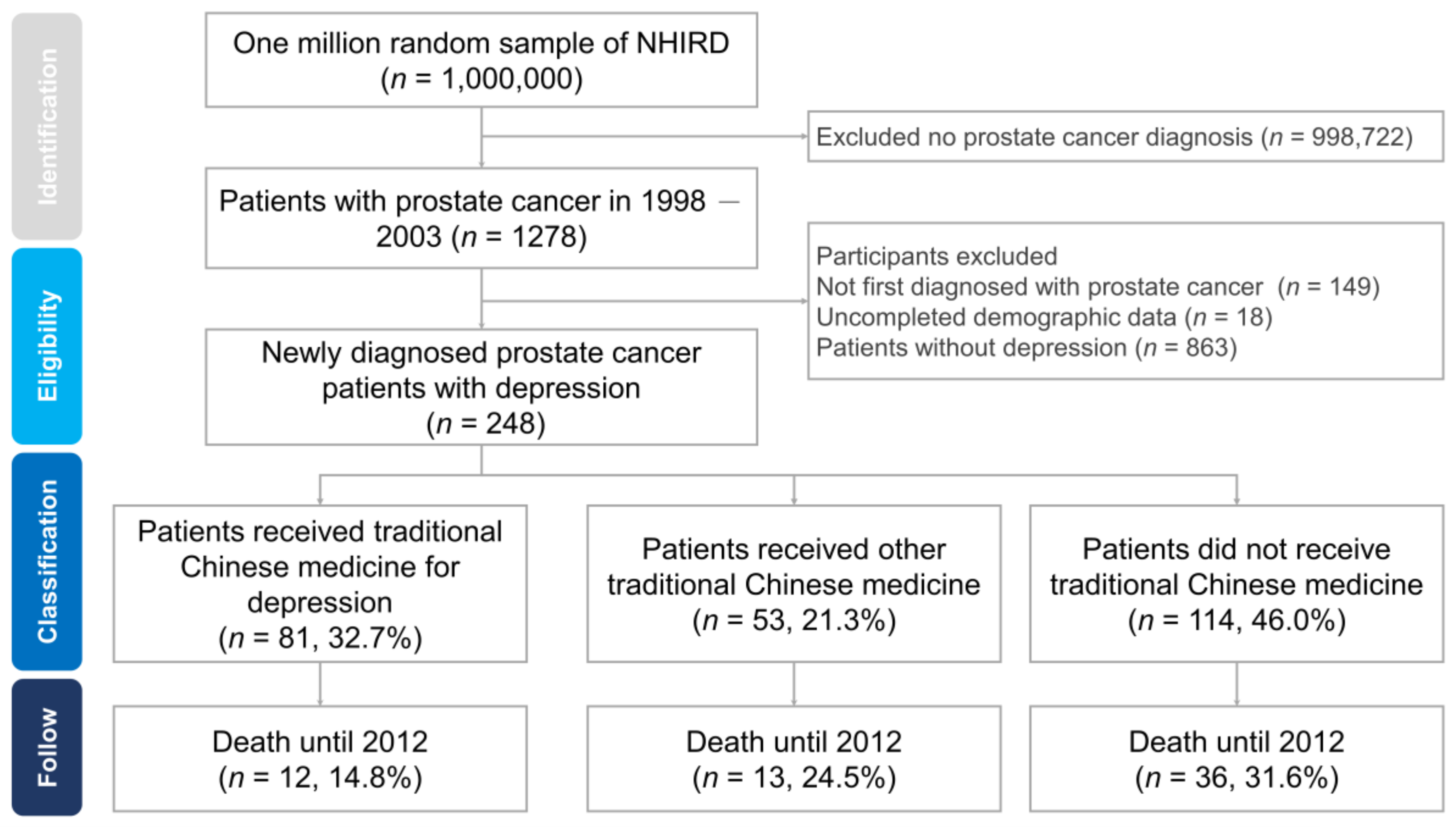
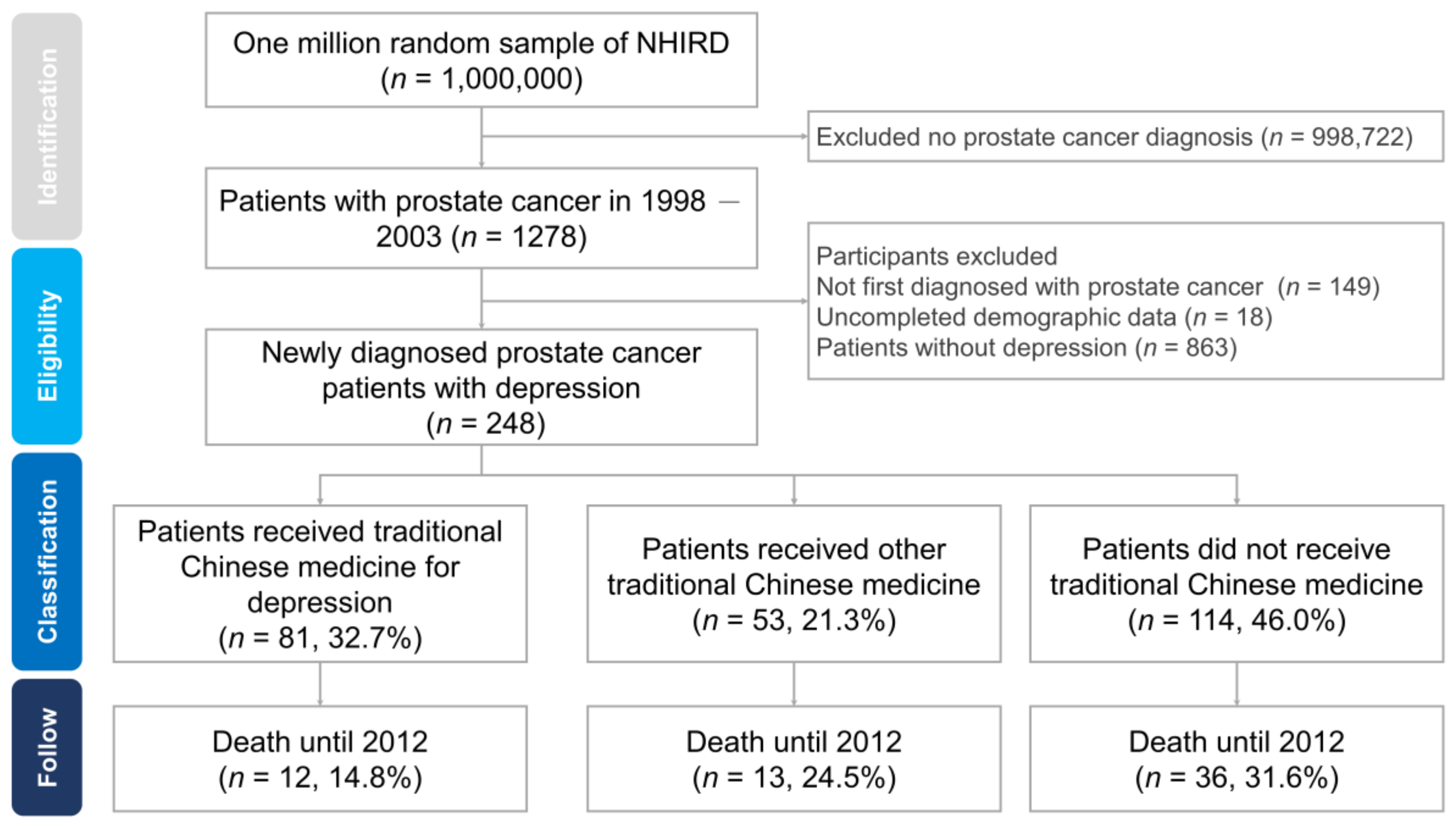
2.2. Study Population
2.3. TCM
2.4. Study Outcomes
2.5. Adjustment of Covariates
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
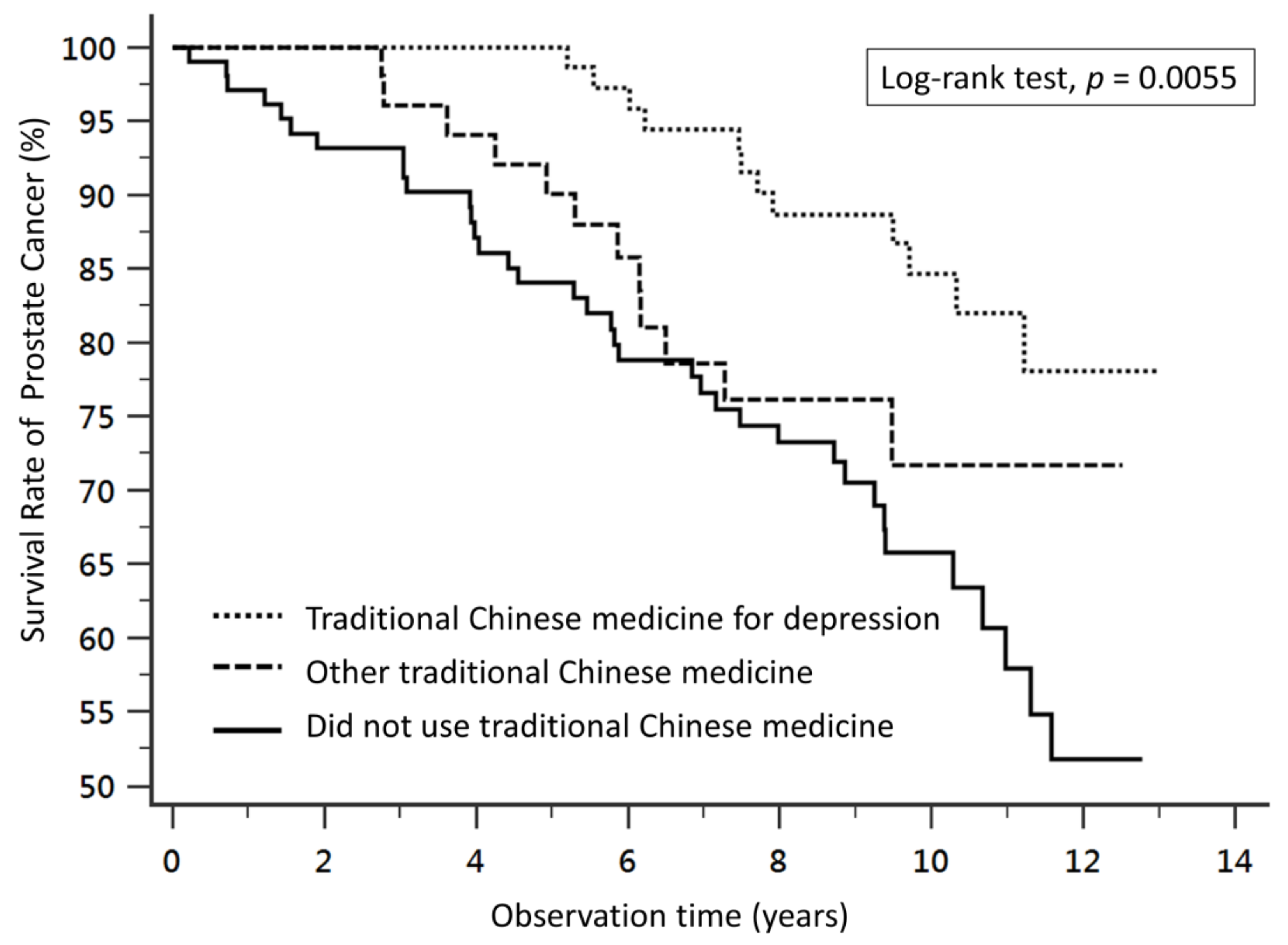
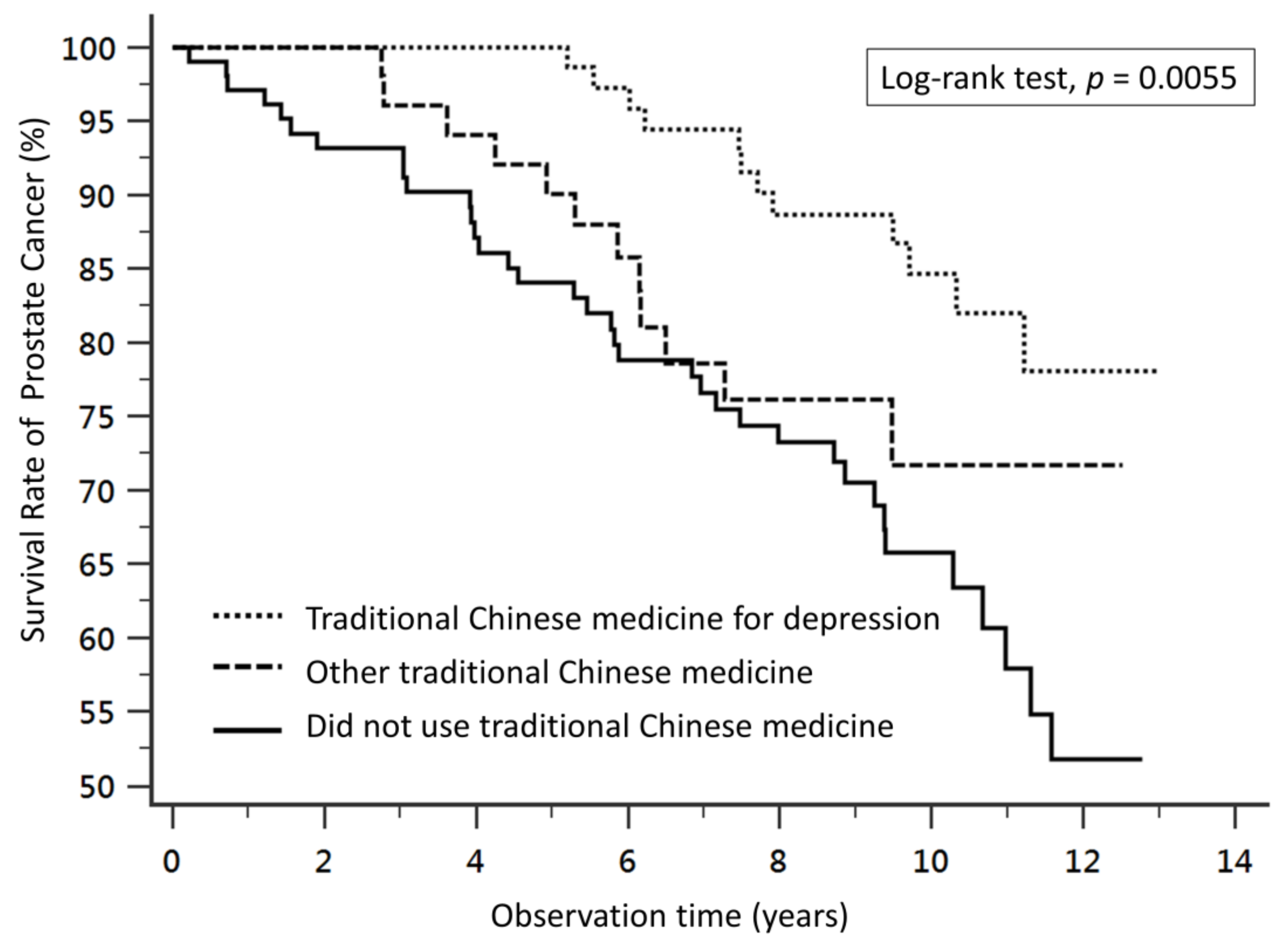
3.2. Longitudinal Analysis of Mortality Risk of Prostate Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hung, C.F.; Yang, C.K.; Ou, Y.C. Urologic cancer in Taiwan. Jpn. J. Clin. Oncol. 2016, 46, 605–609. [Google Scholar] [CrossRef] [PubMed]
- Leonel Almeida, P.; Jorge Pereira, B. Local Treatment of Metastatic Prostate Cancer: What is the Evidence So Far? Prostate Cancer 2018, 2018, 2654572. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.M.; Eggener, S.E.; Lipsitz, S.R.; Irwin, M.R.; Ganz, P.A.; Hu, J.C. Effect of depression on diagnosis, treatment, and mortality of men with clinically localized prostate cancer. J. Clin. Oncol. 2014, 32, 2471–2478. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.H.; Liu, J.M.; Hsu, R.J.; Chuang, H.C.; Chang, S.W.; Pang, S.T.; Chang, Y.H.; Chuang, C.K.; Lin, S.K. Depression Negatively Impacts Survival of Patients with Metastatic Prostate Cancer. Int. J. Environ. Res. Public Health 2018, 15, 2148. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M.; Duberstein, P.R. Depression and cancer mortality: A meta-analysis. Psychol. Med. 2010, 40, 1797–1810. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Kennedy, E.B.; Byrne, N.; Gérin-Lajoie, C.; Katz, M.R.; Keshavarz, H.; Sellick, S.; Green, E. Management of Depression in Patients with Cancer: A Clinical Practice Guideline. J. Oncol. Pract. 2016, 12, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.H.; Chen, K.K.; Chiu, J.H. Use of Chinese medicine among prostate cancer patients in Taiwan: A retrospective longitudinal cohort study. Int. J. Urol. 2011, 18, 383–386. [Google Scholar] [CrossRef]
- Aggarwal, B.B. Prostate cancer and curcumin: Add spice to your life. Cancer Biol. Ther. 2008, 7, 1436–1440. [Google Scholar] [CrossRef]
- Gururaj, A.E.; Belakavadi, M.; Venkatesh, D.A.; Marme, D.; Salimath, B.P. Molecular mechanisms of anti-angiogenic effect of curcumin. Biochem. Biophys. Res. Commun. 2002, 297, 934–942. [Google Scholar] [CrossRef]
- Tamada, S.; Ebisu, K.; Yasuda, S.; Kato, M.; Ninomiya, N.; Yamasaki, T.; Iguchi, T.; Nakatani, T.; Watanabe, Y. Kamikihito improves cancer-related fatigue by restoring balance between the sympathetic and parasympathetic nervous systems. Prostate Int. 2018, 6, 55–60. [Google Scholar] [CrossRef]
- Liu, J.M.; Lin, P.H.; Hsu, R.J.; Chang, Y.H.; Cheng, K.C.; Pang, S.T.; Lin, S.K. Complementary traditional Chinese medicine therapy improves survival in patients with metastatic prostate cancer. Medicine (Baltimore) 2016, 95, e4475. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.M.; Chen, T.H.; Chuang, H.C.; Wu, C.T.; Hsu, R.J. Statin reduces the risk of dementia in diabetic patients receiving androgen deprivation therapy for prostate cancer. Prostate Cancer Prostatic Dis. 2018. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; An, H.; Li, Y.; Duan, L. TCM treatment with the modified wendan tang in 40 cases of melancholia. J. Tradit. Chin. Med. 1999, 19, 296–297. [Google Scholar] [PubMed]
- Chen, F.P.; Jong, M.S.; Chen, Y.C.; Kung, Y.Y.; Chen, T.J.; Chen, F.J.; Hwang, S.J. Prescriptions of Chinese Herbal Medicines for Insomnia in Taiwan during 2002. Evid. Based Complement. Altern. Med. 2011, 2011, 236341. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.L.; Lee, C.Y.; Huang, K.H.; Kuan, Y.H.; Chen, M. Prescription patterns of Chinese herbal products for patients with sleep disorder and major depressive disorder in Taiwan. J. Ethnopharmacol. 2015, 171, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Park, D.M.; Kim, S.H.; Park, Y.C.; Kang, W.C.; Lee, S.R.; Jung, I.C. The comparative clinical study of efficacy of Gamisoyo-San (Jiaweixiaoyaosan) on generalized anxiety disorder according to differently manufactured preparations: Multicenter, randomized, double blind, placebo controlled trial. J. Ethnopharmacol. 2014, 158, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.L.; Lim, S.L.; Lu, K.H.; Sheen, L.Y. Antidepressant-like effects of Gan-Mai-Dazao-Tang via monoamine regulatory pathways on forced swimming test in rats. J. Tradit Complement. Med. 2017, 8, 53–59. [Google Scholar] [CrossRef]
- Kwon, C.Y.; Lee, B.; Chung, S.Y.; Kim, J.W.; Shin, A.; Choi, Y.Y.; Yun, Y.; Leem, J. Herbal medicine Sihogayonggolmoryeo-tang or Chai-Hu-Jia-Long-Gu-Mu-Li-Tang for the treatment of post-stroke depression: A protocol for a systematic review and meta-analysis. Medicine (Baltimore) 2018, 97, e12384. [Google Scholar] [CrossRef]
- Wang, L.; Song, Y.; Li, F.; Liu, Y.; Ma, J.; Mao, M.; Wu, F.; Wu, Y.; Li, S.; Guan, B.; et al. Effects of Wen Dan Tang on insomnia-related anxiety and levels of the brain-gut peptide Ghrelin. Neural Regen Res. 2014, 9, 205–212. [Google Scholar]
- Wu, F.; Song, Y.; Li, F.; He, X.; Ma, J.; Feng, T.; Guan, B.; Wang, L.; Li, S.; Liu, X.; et al. Wen-dan decoction improves negative emotions in sleep-deprived rats by regulating orexin-a and leptin expression. Evid. Based Complement. Altern. Med. 2014, 2014, 872547. [Google Scholar] [CrossRef]
- Tsujimura, A.; Takada, S.; Matsuoka, Y.; Nakayama, J.; Takao, T.; Miyagawa, Y.; Nonomura, N.; Okuyama, A. Clinical trial of treatment with saikokaryukotsuboreito for eugonadal patients with late-inset hypogonadism-related symptoms. Aging Male 2008, 11, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Still, K.; Robson, C.N.; Autzen, P.; Robinson, M.C.; Hamdy, F.C. Localization and quantification of mRNA for matrix metalloproteinase-2 (MMP-2) and tissue inhibitor of matrix metalloproteinase-2 (TIMP-2) in human benign and malignant prostatic tissue. Prostate 2000, 42, 18–25. [Google Scholar] [CrossRef]
- Hidaka, T.; Yonezawa, R.; Saito, S. Kami-shoyo-san, Kampo (Japanese traditional medicine), is effective for climacteric syndrome, especially in hormone-replacement-therapy-resistant patients who strongly complain of psychological symptoms. J. Obstet. Gynaecol. Res. 2013, 39, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Fu, L.; Qin, G.; Shi, P.; Fu, W. The regulatory effect of Xiaoyao San on glucocorticoid receptors under the condition of chronic stress. Cell Mol. Biol. (Noisy-le-grand) 2018, 64, 103–109. [Google Scholar] [CrossRef]
- Yeh, C.H.; Arnold, C.K.; Chen, Y.H.; Lai, J.N. Suan zao ren tang as an original treatment for sleep difficulty in climacteric women: A prospective clinical observation. Evid. Based Complement. Alternat Med. 2011, 2011, 673813. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Xu, X.; Zhang, J.; Chen, Y. Treatment of depression with Chai Hu Shu Gan San: A systematic review and meta-analysis of 42 randomized controlled trials. BMC Complement. Altern. Med. 2018, 18, 66. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.K.; Yan, S.H.; Lai, J.N.; Tsai, T.H. Patterns of Chinese medicine use in prescriptions for treating Alzheimer’s disease in Taiwan. Chin. Med. 2016, 11, 12. [Google Scholar] [CrossRef]
- Liu, J.M.; Yu, C.P.; Chuang, H.C.; Wu, C.T.; Hsu, R.J. Androgen deprivation therapy for prostate cancer and the risk of autoimmune diseases. Prostate Cancer Prostatic Dis. 2019. [Google Scholar] [CrossRef]
- Chung, S.D.; Kao, L.T.; Lin, H.C.; Xirasagar, S.; Huang, C.C.; Lee, H.C. Patients receiving androgen deprivation therapy for prostate cancer have an increased risk of depressive disorder. PLoS ONE 2017, 12, e0173266. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | Traditional Chinese Medicine for Depression No. (%) | Other Traditional Chinese Medicine No. (%) | Did not Use Traditional Chinese Medicine No. (%) | Chi-Square Test p-Value |
|---|---|---|---|---|
| Total | 81 (100.00%) | 53 (100.00%) | 114 (100.00%) | |
| Age at diagnosis | 0.4797 | |||
| <60 | 3 (3.7%) | 4 (7.5%) | 5 (4.4%) | |
| 60–70 | 13 (16.0%) | 9 (17.0%) | 10 (8.8%) | |
| 70–80 | 20 (24.7%) | 14 (26.4%) | 38 (33.3%) | |
| ≥80 | 45 (55.6%) | 26(49.1%) | 61 (53.5%) | |
| Urbanization | 0.0966 | |||
| Very high | 44 (54.3%) | 31 (58.5%) | 60 (52.6%) | |
| High | 22 (27.2%) | 13 (24.5%) | 17 (14.9%) | |
| Moderate | 12 (14.8%) | 7 (13.2%) | 24 (21.1%) | |
| Low | 3 (3.7%) | 2 (3.8%) | 13 (11.4%) | |
| Insured amount (NT$) | 0.4154 | |||
| Dependent | 17 (21.0%) | 8 (15.1%) | 31 (27.2%) | |
| 1–19,999 | 34 (42.0%) | 27 (50.9%) | 49 (43.0%) | |
| 20,000–39,999 | 18 (22.2%) | 9 (17.0%) | 24 (21.1%) | |
| ≥40,000 | 12 (14.8%) | 9 (17.0%) | 10 (8.8%) | |
| Comorbidity | ||||
| Diabetes mellitus | 44 (54.3%) | 29 (54.7%) | 47 (41.2%) | 0.1146 |
| Chronic kidney disease | 20 (24.7%) | 12 (22.6%) | 21 (18.4%) | 0.5563 |
| Cerebrovascular accident | 52 (64.2%) | 29 (54.7%) | 54 (47.4%) | 0.0669 |
| Coronary heart disease | 52 (64.2%) | 30 (56.6%) | 63 (55.3%) | 0.4376 |
| Heart failure | 27 (33.3%) | 12 (22.6%) | 39 (34.2%) | 0.2947 |
| Liver cirrhosis | 42 (51.9%) | 30 (56.6%) | 42 (36.8%) | 0.0252 * |
| Hypertension | 71 (87.7%) | 43 (81.1%) | 95 (83.3%) | 0.5573 |
| Prostate cancer type | ||||
| Localized or Locally advanced | 15 (18.5%) | 8 (15.1%) | 23 (20.2%) | 0.0681 |
| Metastatic | 51 (63.0%) | 36 (67.9%) | 74 (64.9%) | 0.4013 |
| Castration-resistant | 15 (18.5%) | 9 (17.0%) | 17 (14.9%) | 0.0779 |
| Different Treatment | Crude HR (95%CI) | Adjusted Model 1 aHR (95%CI) | Adjusted Model 2 aHR (95%CI) |
|---|---|---|---|
| Patients did not receive traditional Chinese medicine | [Reference] | [Reference] | [Reference] |
| Patients who received traditional Chinese medicine for depression (spirit-quieting TCM) | 0.41 (0.24–0.73) | 0.46 (0.23–0.88) | 0.42 (0.21–0.85) |
| Patients who received other traditional Chinese medicine | 0.83 (0.42–1.66) | 1.02 (0.53–1.96) | 1.02 (0.52–1.99) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, P.-H.; Lin, S.-K.; Hsu, R.-J.; Pang, S.-T.; Chuang, C.-K.; Chang, Y.-H.; Liu, J.-M. Spirit-Quieting Traditional Chinese Medicine May Improve Survival in Prostate Cancer Patients with Depression. J. Clin. Med. 2019, 8, 218. https://doi.org/10.3390/jcm8020218
Lin P-H, Lin S-K, Hsu R-J, Pang S-T, Chuang C-K, Chang Y-H, Liu J-M. Spirit-Quieting Traditional Chinese Medicine May Improve Survival in Prostate Cancer Patients with Depression. Journal of Clinical Medicine. 2019; 8(2):218. https://doi.org/10.3390/jcm8020218
Chicago/Turabian StyleLin, Po-Hung, Shun-Ku Lin, Ren-Jun Hsu, See-Tong Pang, Cheng-Keng Chuang, Ying-Hsu Chang, and Jui-Ming Liu. 2019. "Spirit-Quieting Traditional Chinese Medicine May Improve Survival in Prostate Cancer Patients with Depression" Journal of Clinical Medicine 8, no. 2: 218. https://doi.org/10.3390/jcm8020218
APA StyleLin, P.-H., Lin, S.-K., Hsu, R.-J., Pang, S.-T., Chuang, C.-K., Chang, Y.-H., & Liu, J.-M. (2019). Spirit-Quieting Traditional Chinese Medicine May Improve Survival in Prostate Cancer Patients with Depression. Journal of Clinical Medicine, 8(2), 218. https://doi.org/10.3390/jcm8020218