Abstract
Background: Endometrial cancer (EC) is the most common gynecological malignancy in developed countries. While early-stage disease has favorable outcomes, advanced or recurrent EC remains associated with poor prognosis. Novel prognostic markers are needed to refine risk stratification. Systemic inflammation-based indices such as Pan-Immune Inflammation Value (PIV), Systemic Inflammation Response Index (SIRI), and Systemic Immune Inflammation Index (SII) have shown prognostic potential in solid tumors. Methods: We retrospectively evaluated 78 patients with endometrioid EC who had undergone hysterectomy with adnexectomy and lymphadenectomy. Demographic, clinicopathological, and laboratory data were extracted from electronic medical records. PIV, SII, and SIRI were calculated from the preoperative complete blood counts. Survival was assessed using Kaplan–Meier analysis, while prognostic factors were determined using univariate and multivariate Cox regression analyses. Results: The median age was 59 years, and 64.1% of the patients presented with early-stage disease. A high PIV (≥802) was significantly associated with a shorter overall survival (64 vs. 111 months, p < 0.001). PIV demonstrated the highest discriminatory accuracy (AUC = 0.776), followed by the SII (0.747) and SIRI (0.718). Univariate analysis identified that age, grade, LVSI, PNI, stage, distant metastasis, and high PIV, SII, SIRI, and NLR were predictors of poor survival. Multivariate analysis confirmed grade, distant metastasis and SIRI ≥ 1.5 as independent prognostic factors. Conclusions: Inflammation-based indices, particularly PIV and SIRI, correlated with survival outcomes in patients with EC. The SIRI retained an independent prognostic value, whereas PIV showed a strong discriminatory capacity. Incorporating these indices into established risk models may improve prognostic precision and support individualized management.
1. Introduction
Endometrial cancer (EC) is the most prevalent gynecological malignancy and its incidence is increasing in developed countries [1]. In 2020, 417,336 women worldwide were diagnosed with EC, making it the sixth most common cancer in women [2]. Although early diagnosis is associated with favorable outcomes, the prognosis remains poor for women diagnosed at later stages or with recurrent or metastatic disease [3]. Endometrial carcinoma accounts for approximately 90% of all uterine cancers, and surgical intervention with or without adjuvant radiotherapy or chemotherapy remains the primary therapeutic approach [4].
Histologically, EC is classified into two main forms: endometrioid (type I), which represents approximately 80% of EC cases, and non-endometrioid (type II), which accounts for the remaining 20% [5]. More recently, molecular classification has further subdivided EC into four groups: EC with polymerase epsilon mutations (POLEmut), EC with mismatch repair deficiency (dMMR), high microsatellite instability (MSI-high), EC with TP53 mutations and abnormal p53 protein expression (p53abn), and EC without a specific molecular profile (NSMP) [6]. Prognosis and therapeutic strategies vary by molecular subtype, with POLEmut tumors generally associated with excellent outcomes and p53abn tumors associated with the poorest prognosis. Accordingly, subtype-specific adjuvant treatments, including targeted therapy and immunotherapy, are increasingly being recommended [7,8]
Although the majority of women with EC achieve favorable outcomes, a notable proportion present with adverse clinicopathological features, indicating poor prognosis [9]. Numerous studies have sought to identify prognostic factors for EC, as the early detection of recurrence with reliable markers may improve treatment outcomes and survival. Established prognostic variables include histologic subtype, tumor grade, lymphovascular space invasion (LVSI), and International Federation of Gynecology and Obstetrics (FIGO) staging [10,11]. However, survival outcomes may vary considerably even among patients with similar established prognostic profiles. This highlights the need to identify novel and more specific biomarkers to improve risk stratification and guide personalized treatment.
Blood-based biomarkers, particularly inflammatory markers, have shown promise for predicting the prognosis of EC [12]. Peripheral blood testing is a convenient and cost-effective method for assessing high-risk patients. Determining the prognostic status at diagnosis may allow for more tailored treatment strategies and potentially improve survival outcomes [13]. Inflammation and immune response play pivotal roles in carcinogenesis, including initiation, invasion, promotion, and metastasis [14]. The interplay between tumor cells and components of the tumor microenvironment, such as neutrophils, lymphocytes, platelets, and monocytes, is thought to drive tumor proliferation and metastasis [15]
Several inflammatory indices derived from routine blood counts, including the Pan-Immune Inflammation Value (PIV), Systemic Inflammatory Response Index (SIRI), and Systemic Immune Inflammation Index (SII), have been associated with poor prognosis in various solid tumors [16,17,18,19]. This correlation is attributed, in part, to the neutrophil-mediated secretion of growth factors such as Vascular Endothelial Growth Factor (VEGF) and proteases that promote metastasis [20]. Conversely, reduced lymphocyte counts may compromise antitumor immunity by impairing cytotoxic cell function and diminishing tumor cell clearance [21].
In this context, our retrospective analysis aimed to evaluate the relationship between peripheral immune cell count and distant metastases in patients with EC. We propose that inflammatory nomograms based on such indices may represent promising novel prognostic markers that complement and potentially surpass traditional staging systems in predicting outcomes and guiding personalized management strategies for advanced gynecological malignancies.
2. Materials and Methods
Study Population: Between 1 January 2015 and 1 January 2023, the clinicopathological data of 150 patients diagnosed with endometrial carcinoma (EC) at our institution were retrospectively collected. Eligible patients underwent hysterectomy with adnexectomy and lymphadenectomy. Preoperative evaluation included gynecological examination, imaging studies, and histopathological assessment.
Exclusion criteria were as follows: 13 patients without a complete blood count within two weeks prior to surgery, 24 patients with insufficient clinicopathological or follow-up data, 5 patients with atypical hyperplasia or carcinoid tumors, 18 patients with non-endometrioid histology, and 12 patients with concurrent malignancies, hematologic disorders, or a history of neoadjuvant therapy. After applying these criteria, 78 patients were included in the final analysis. Comprehensive biochemical evaluations, including complete blood count, were performed within 15 days prior to surgical intervention. Patients with chronic immune or inflammatory disorders, active acute infections, a recent history (within the past month) of medications affecting immune or inflammatory responses (Figure 1).
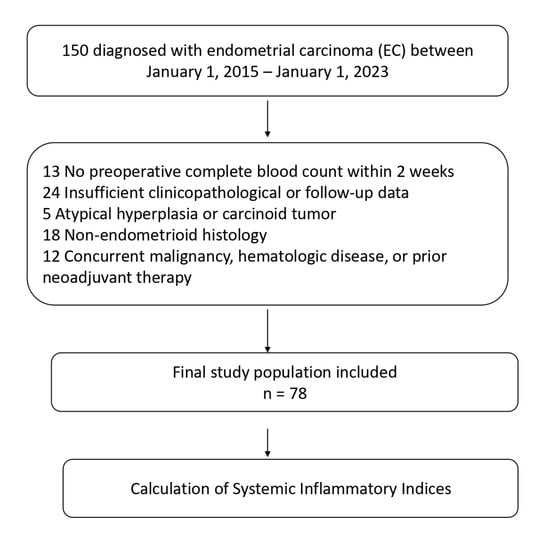
Figure 1.
Flowchart of the study according to CONSORT diagram.
2.1. Data Collection
Clinical data were obtained from the hospital’s archived electronic medical records. Demographic variables included age, menopausal status, comorbidities, smoking status, and obesity (BMI ≥ 30 kg/m2). Pathological parameters included tumor grade, perineural invasion (PNI), lymphovascular space invasion (LVSI), pathological T stage (pT), presence of distant metastasis, and overall stage. Treatment-related variables included administration of adjuvant chemotherapy and radiotherapy. Progression-free survival (PFS) was defined as the interval between the date of pathological diagnosis and the occurrence of disease progression, death, or the last follow-up visit. Overall survival (OS) was defined as the time from the date of pathological diagnosis to death from any cause or the last documented follow-up.
Calculation of Systemic Inflammatory Indices
Peripheral blood samples obtained at baseline were analyzed to determine neutrophil, platelet, monocyte, and lymphocyte counts (expressed as ×103/mm3). Based on these parameters, systemic inflammatory indices were calculated according to previously validated formulas. The systemic immune inflammation index (SII) was defined as neutrophil count × platelet count/lymphocyte count. The systemic inflammation response index (SIRI) was calculated as neutrophil count × monocyte count/lymphocyte count. The pan-immune inflammation value (PIV) was determined as neutrophil count × platelet count × monocyte count/lymphocyte count.
This study was conducted in accordance with the Declaration of Helsinki (revised in 2024). Ethical approval was obtained from the Ethics Committee of Batman Training and Research Hospital, Non-Interventional Clinical Studies, dated 23 January 2025, decision no: 406.
2.2. Statistical Analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) for Windows version 27 (IBM SPSS Inc., Chicago, IL, USA). The normality of the data distribution was assessed using the Kolmogorov–Smirnov test. Continuous variables with normal distribution are expressed as mean ± standard deviation, whereas non-normally distributed variables are presented as medians (min–max).
The diagnostic performance of PIV, SII, SIRI, NLR, and PLR in predicting mortality was evaluated using receiver operating characteristic (ROC) curve analysis. The DeLong method was used to calculate the confidence intervals in the AUC table. The optimal cut-off values for these indices were determined using the Youden index method. Associations between PIV and clinicopathological and laboratory parameters were assessed using the chi-square, Mann–Whitney U, as appropriate.
Overall survival (OS) and progression-free survival (PFS) were estimated using the Kaplan–Meier method and compared using the log-rank test. The potential for multicollinearity was assessed by calculating the Variance Inflation Factor (VIF) values for the inflammatory indices included in the regression model. The VIF values ranged from 0.6 to 3.8, no significant multicollinearity was detected. Therefore, all variables were retained in the multivariate regression analysis. The impact of the variables on survival outcomes was further analyzed using univariate and multivariate Cox proportional hazard regression models. Statistical significance was set at a two-tailed p-value of <0.05.
3. Results
A total of 78 patients with endometrioid carcinoma were included in this study. The median age of the patients was 59 years (range, 24–91 years), and 30 patients (38.5%) were aged ≥65 years. Twenty-eight patients (35.9%) were premenopausal, and 50 (64.1%) were postmenopausal. The ECOG performance status was 0–1 in 65 patients (83.3%) and ≥2 in 13 patients (16.7%). Nineteen patients (24.4%) were smokers, 32 (41.0%) were obese, and 49 (62.8%) had comorbidities. The histological grade was 1 in 32 patients (41.0%), 2 in 17 patients (21.8%), and 3 in 29 patients (37.2%). LVSI was present in 21 patients (26.9%), and PNI in 10 patients (12.8%). Adjuvant radiotherapy and chemotherapy were administered to 36 (46.2%) and 27 (34.6%) patients, respectively. Peritoneal involvement was detected in 13 patients (16.7%), and distant metastases in 15 patients (19.2%). According to risk stratification, 47 (60.3%) were low-risk and 31 (39.7%) were high-risk. Nodal involvement was observed in 19 (24.4%) patients. pT1–2 was present in 50 (64.1%) and pT3–4 in 28 (35.9%). Early-stage disease (I–II) was identified in 50 patients (64.1%) and advanced stage disease (III–IV) in 28 patients (35.9%).
ROC analysis demonstrated that PIV had the highest prognostic accuracy (AUC = 0.776, sensitivity = 70.4%; specificity, 82.4%; cut-off, 802). SII (AUC = 0.747), SIRI (AUC = 0.718), and NLR (AUC = 0.713) also showed significant discriminatory values, whereas PLR had a lower predictive ability (AUC = 0.686) (Figure 2, Table 1).
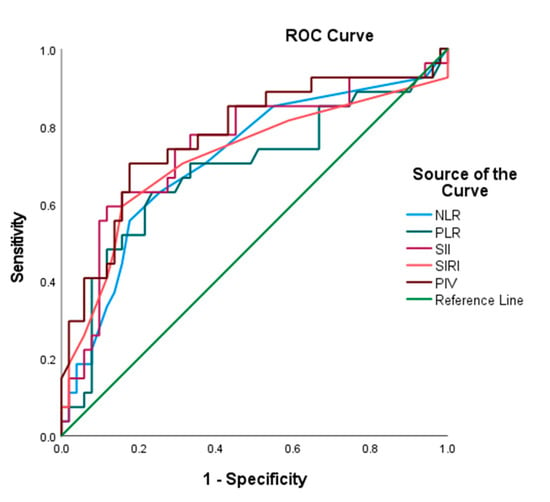
Figure 2.
ROC curves for systemic inflammation indices in predicting mortality of endometrial cancer patients.

Table 1.
Predictive performance of systemic inflammatory indices for mortality according to ROC analysis.
Fifty patients (64.1%) had low PIV (<802) and 28 (35.9%) had high PIV (≥802). SII was <1545 in 53 (67.9%) and ≥1545 in 25 (32.1%). SIRI was <1.5 in 43 (55.1%) and ≥1.5 in 35 (44.9%). NLR was <2.5 in 38 (48.7%) and ≥2.5 in 40 (51.3%). PLR was <120.5 in 22 (28.2%) and ≥120.5 in 56 (71.8%). High PIV was significantly associated with obesity (p = 0.029), PNI (p = 0.022), and adjuvant radiotherapy (p = 0.015) but not with age, menopausal status, ECOG status, smoking, comorbidity, tumor grade, LVSI, chemotherapy, peritoneal involvement, metastasis, risk group, nodal involvement, pT, or FIGO stage. Elevated PIV was strongly correlated with other inflammation-based indices, including SII, SIRI, NLR, and PLR (all p < 0.001) (Table 2).
Table 2.
Association between PIV and clinicopathological variables in endometrial carcinoma.
During a median follow-up period of 87 months, 27 patients (34.6%) died. The median overall survival (OS) was 95.5 months (range, 34.2–146), with significantly longer survival in the low PIV group (111 months [96.0–127.5]) than in the high PIV group (64 months [43.4–85.2], p < 0.001). Disease progression occurred in 24 patients (30.8%), with a median progression-free survival (PFS) of 80 months (range, 43.2–106.6). Median PFS was longer in the low PIV group (105 months [88.5–121.0]) than in the high PIV group (90 months [64.6–116.0]), though the difference was not statistically significant (p = 0.446; Figure 3).
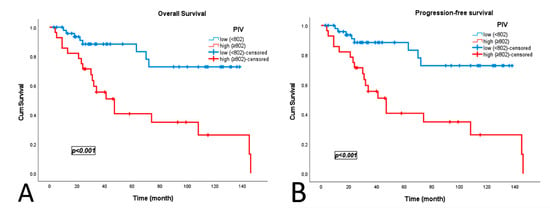
Figure 3.
Kaplan–Meier survival curves according to Pan-Immune Inflammation Value (PIV): (A) overall survival; (B) progression-free survival.
In the univariate Cox regression analysis, advanced age (≥65 years), higher grade, LVSI, PNI, adjuvant chemotherapy, distant metastasis, high-risk classification, advanced pT and stage, and elevated inflammatory indices (PIV ≥ 802, SII ≥ 1545, SIRI ≥ 1.5, NLR ≥ 2.5) were significantly associated with poorer overall survival (OS), while obesity emerged as a protective factor. PLR ≥ 120.5 demonstrated borderline significance. For progression-free survival (PFS), obesity remained protective, whereas grade, LVSI, PNI, chemotherapy, metastasis, high-risk status, advanced pT, stage, and the same inflammatory indices were significant adverse prognostic indicators, with PLR not reaching significance (Table 3).
Table 3.
Univariate Cox regression analysis of prognostic factors for overall survival and progression-free survival.
In the multivariate Cox regression analysis, distant metastasis, higher tumor grade, and elevated SIRI remained independent poor prognostic factors for overall survival, while PIV, SII, and NLR were not significant. For progression-free survival, grade, dis-tant metastasis, and SIRI were also confirmed as independent predictors. PIV and NLR showed a trend toward increased risk but did not reach statistical significance. No significant associations were observed for age, obesity, LVSI, PNI, adjuvant chemotherapy, risk group, pT, or FIGO stage (Table 4).
Table 4.
Multivariate Cox regression analysis of prognostic factors for overall survival and progression-free survival.
4. Discussion
Endometrial carcinoma is the most common gynecological malignancy in developed countries. Because of its heterogeneous biological behavior, accurate identification of prognostic factors is of critical importance for clinical management. Traditional prognostic parameters include tumor stage, histological grade, lymphovascular space invasion (LVSI), and perineural invasion (PNI). However, in recent years, there has been growing evidence regarding the prognostic value of biomarkers that reflect systemic inflammatory responses [22]. In this context, our study comprehensively evaluated the prognostic relevance of the Pan-Immune Inflammation Value (PIV), along with SII, SIRI, NLR, and PLR, in a cohort of patients with endometrioid-type endometrial carcinoma.
Our findings revealed that PIV is the strongest predictor of patient survival. In the ROC analysis, PIV achieved the highest AUC (0.776), and patients with values above the cutoff (802) exhibited significantly shorter overall survival. The median OS was 111 and 64 months in the low-and high-PIV groups, respectively (p < 0.001). This suggests that PIV, by reflecting the magnitude of the systemic inflammatory response and immune cell interactions within the tumor microenvironment, may serve as a powerful prognostic indicator. Previous studies have also shown that elevated PIV predicts poor outcomes in several solid tumors, particularly ovarian and cervical cancers [22,23,24]. Recently published data similarly reported that high PIV levels were significantly associated with reduced survival, supporting the validity of our findings in endometrial carcinoma [25].
In our cohort, PIV showed no significant association with demographic or clinicopathologic variables, including age, menopausal status, ECOG score, comorbidities, tumor grade, LVSI, chemotherapy, peritoneal or nodal involvement, metastasis, or FIGO stage. This pattern suggests that PIV may primarily reflect systemic inflammatory status rather than intrinsic tumor characteristics. While this supports its potential as an independent prognostic biomarker, it also underscores the importance of integrating inflammatory indices with pathological parameters to achieve a more comprehensive assessment of tumor aggressiveness.
SII, SIRI, and NLR were also identified as significant predictors of OS and PFS in the univariate analyses. These results are consistent with those of previous reports, where high SII values correlated with advanced stage and poor prognosis in endometrial cancer [10,26]. Likewise, the prognostic value of NLR has been documented across various gynecological malignancies, with elevated NLR reflecting immune dysfunction and tumor progression [27]. SIRI has been less extensively studied. Tu et al. reported that SIRI values above 1.29 were significantly associated with an increased risk of recurrence and death in patients with endometrial cancer, whereas those in the low-SIRI group demonstrated longer recurrence-free and overall survival, even in the absence of adjuvant therapy. Similarly, in our cohort, a high SIRI was associated with poorer survival and shorter recurrence intervals, and it retained independent prognostic significance for both overall survival (OS) and progression-free survival (PFS) in multivariate analysis [28]. These findings support the potential of SIRI as a strong and reliable prognostic biomarker for endometrial carcinoma.
In contrast, PLR demonstrated only borderline statistical significance in the present study. While this may suggest a potential role of platelets in tumor progression, PLR appears to be a weaker marker than the other indices. Meta-analyses have similarly highlighted the heterogeneity in the prognostic significance of PLR across tumor types [29].
Interestingly, obesity was more common in the low-PIV group. While obesity is a well-established risk factor for endometrial carcinoma, its inverse association with inflammatory indices may reflect the complex interplay between obesity-driven chronic inflammation and systemic immune response [30].
In multivariate Cox regression analysis, only histological grade, distant metastasis, and SIRI ≥ 1.5 remained as independent prognostic factors. This finding reinforces the importance of established histopathological parameters, suggesting that inflammatory indices may serve as complementary, rather than standalone, prognostic tools. Similarly to our results, Huang et al. reported that the prognostic value of inflammatory indices was particularly evident in advanced-stage and high-risk patients [31]. Therefore, PIV and related indices may contribute to risk stratification models, aiding individualized patient management.
This study has certain limitations that should be acknowledged. The retrospective design, relatively small sample size, and single-center nature may limit the generalizability of the results. In addition, blood-derived inflammatory indices can be influenced by comorbidities, obesity, and concurrent infections, which may confound their prognostic interpretation.
Another important limitation is the absence of molecular classification data (e.g., POLEmut, dMMR, p53abn, NSMP) within the study cohort. Although the introduction provides an overview of the contemporary molecular taxonomy of endometrial carcinoma, these molecular subgroups were not available in our dataset and therefore could not be analyzed. In the current era of molecularly guided risk stratification, the lack of such data limits the ability to assess potential interactions between inflammation-based indices and established molecular profiles.
Therefore, future large-scale, prospective, multicenter studies integrating molecular and systemic inflammation parameters are warranted to validate and extend the prognostic value of these indices in endometrial carcinoma.
5. Conclusions
In conclusion, our study demonstrated that inflammatory indices, particularly PIV, may have prognostic value in endometrial carcinoma. Elevated PIV was associated with shorter survival, whereas SIRI was an independent predictor of both OS and PFS. These findings suggested that inflammatory markers should be considered in conjunction with conventional histopathological factors. The incorporation of such indices into future risk stratification models may support more personalized treatment and follow-up strategies for patients with endometrial carcinoma.
Author Contributions
N.O.K.: Conceptualization, Methodology, Resources, Writing—Original draft preparation, Writing—Reviewing and Editing, Visualization, Supervision, Critical Review, Z.U.: Statistical analysis, Writing—Reviewing and Editing, Software, Data Curation, Visualization, Investigation, Validation. B.M.E.: Writing—Reviewing and Editing, Software, Data Curation, Visualization, Investigation. E.B.: Writing—Original draft preparation, Writing—Reviewing and Editing, Visualization, Supervision. H.A.: Data Curation, Writing—Reviewing and Editing, Visualization. M.H.A.: Writing—Original draft preparation, Writing—Reviewing and Editing. Furthermore, all authors agreed to accept responsibility for all aspects of this study, thereby ensuring its accuracy and integrity. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study protocol was reviewed and approved by the Ethics Committee of Batman Training and Research Hospital, Non-Interventional Clinical Studies, dated 23 January 2025, decision no: 406.
Informed Consent Statement
Patient consent was waived due to the fact that the study was conducted on a retrospective file.
Data Availability Statement
The datasets used in this study can be made available by the corresponding author upon reasonable request, with permission from the Batman Training and Research Hospital.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| EC | Endometrial Cancer |
| PIV | Pan-Immune Inflammation Value |
| SII | Systemic Immune Inflammation Index |
| SIRI | Systemic Inflammation Response Index |
| NLR | Neutrophil-to-Lymphocyte Ratio |
| PLR | Platelet-to-Lymphocyte Ratio |
| OS | Overall Survival |
| PFS | Progression-Free Survival |
| ROC | Receiver Operating Characteristic |
| AUC | Area Under the Curve |
| LVSI | Lymphovascular Space Invasion |
| PNI | Perineural Invasion |
| FIGO | International Federation of Gynecology and Obstetrics |
| ECOG PS | Eastern Cooperative Oncology Group Performance Status |
| BMI | Body Mass Index |
| RT | Radiotherapy |
| CT | Chemotherapy |
| pT | Pathological T Stage |
| VEGF | Vascular Endothelial Growth Factor |
| POLEmut | Polymerase Epsilon Mutated |
| dMMR | Deficient Mismatch Repair |
| MSI-high | High Microsatellite Instability |
| p53abn | Abnormal p53 Expression |
| NSMP | No Specific Molecular Profile |
| CI | Confidence Interval |
| HR | Hazard Ratio |
| SPSS | Statistical Package for the Social Sciences |
References
- Henley, S.J.; Ward, E.M.; Scott, S.; Ma, J.; Anderson, R.N.; Firth, A.U.; Thomas, C.C.; Islami, F.; Weir, H.K.; Lewis, D.R.; et al. Annual report to the nation on the status of cancer, part I: National cancer statistics. Cancer 2020, 126, 2225–2249. [Google Scholar] [CrossRef] [PubMed]
- eBioMedicine. Endometrial cancer: Improving management among increasing incidence rates. eBioMedicine 2024, 103, 105159. [Google Scholar] [CrossRef]
- Braun, M.M.; Overbeek-Wager, E.A.; Grumbo, R.J. Diagnosis and management of endometrial cancer. Am. Fam. Physician 2016, 93, 468–474. [Google Scholar]
- Paleari, L.; Pesce, S.; Rutigliani, M.; Greppi, M.; Obino, V.; Gorlero, F.; Vellone, V.G.; Marcenaro, E. New insights into endometrial cancer. Cancers 2021, 13, 1496. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.H.; Broaddus, R.R. Endometrial cancer. N. Engl. J. Med. 2020, 383, 2053–2064. [Google Scholar] [CrossRef]
- Mitric, C.; Bernardini, M.Q. Endometrial cancer: Transitioning from histology to genomics. Curr. Oncol. 2022, 29, 741–757. [Google Scholar] [CrossRef]
- Jamieson, A.; Bosse, T.; McAlpine, J.N. The emerging role of molecular pathology in directing the systemic treatment of endometrial cancer. Ther. Adv. Med. Oncol. 2021, 13, 1–14. [Google Scholar] [CrossRef]
- Njoku, K.; Barr, C.E.; Crosbie, E.J. Current and emerging prognostic biomarkers in endometrial cancer. Front. Oncol. 2022, 12, 890908. [Google Scholar] [CrossRef]
- Huang, Y.; Chen, Y.; Zhu, Y.; Wu, Q.; Yao, C.; Xia, H.; Li, C. Postoperative systemic immune-inflammation index (SII): A superior prognostic factor of endometrial cancer. Front. Surg. 2021, 8, 704235. [Google Scholar] [CrossRef]
- Abu-Shawer, O.; Abu-Shawer, M.; Hirmas, N.; Alhouri, A.; Massad, A.; Alsibai, B.; Sultan, H.; Hammo, H.; Souleiman, M.; Shebli, Y.; et al. Hematologic markers of distant metastases and poor prognosis in gynecological cancers. BMC Cancer 2019, 19, 141. [Google Scholar] [CrossRef] [PubMed]
- Dolan, R.D.; McMillan, D.C. The prevalence of cancer associated systemic inflammation: Implications of prognostic studies using the Glasgow Prognostic Score. Crit. Rev. Oncol. Hematol. 2020, 150, 102962. [Google Scholar] [CrossRef]
- Collde la Rubia, E.; Martinez-Garcia, E.; Dittmar, G.; Gil-Moreno, A.; Cabrera, S.; Colas, E. Prognostic biomarkers in endometrial cancer: A systematic review and meta-analysis. J. Clin. Med. 2020, 9, 1900. [Google Scholar] [CrossRef]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, inflammation, and cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef]
- Elinav, E.; Nowarski, R.; Thaiss, C.A.; Hu, B.; Jin, C.; Flavell, R.A. Inflammation-induced cancer: Crosstalk between tumours, immune cells and microorganisms. Nat. Rev. Cancer. 2013, 13, 759–771. [Google Scholar] [CrossRef]
- Abu-Shawer, M.; Abu-Shawer, O.; Souleiman, M.; Akkawi, M.; Alshakhatreh, O.; Altamimi, T.; Al-Omari, A.; Al-Hussaini, M. Hematologic markers of lung metastasis in stage IV colorectal cancer. J. Gastrointest. Cancer 2019, 50, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Baba, Y.M.; Nakagawa, S.; Toihata, T.; Harada, K.; Iwatsuki, M.M.; Hayashi, H.M.; Miyamoto, Y.M.; Yoshida, N.M.; Baba, H.M. Pan-immune-inflammation value and prognosis in patients with esophageal cancer. Ann. Surg. Open 2022, 3, e113. [Google Scholar] [CrossRef]
- Qiu, Y.; Zhang, Z.; Chen, Y. Prognostic value of pretreatment systemic immune-inflammation index in gastric cancer: A meta-analysis. Front. Oncol. 2021, 11, 537140. [Google Scholar] [CrossRef] [PubMed]
- Jomrich, G.; Gruber, E.S.; Winkler, D.; Hollenstein, M.; Gnant, M.; Sahora, K.; Schindl, M. Systemic immune-inflammation in-dex (SII) predicts poor survival in pancreatic cancer patients undergoing resection. J. Gastrointest. Surg. 2020, 24, 610–618. [Google Scholar] [CrossRef]
- Mouchemore, K.A.; Anderson, R.L.; Hamilton, J.A. Neutrophils, G-CSF and their contribution to breast cancer metastasis. FEBS J. 2018, 285, 665–679. [Google Scholar] [CrossRef]
- Smyth, M.J. Immune surveillance of tumors. J. Clin. Investig. 2007, 117, 1137–1146. [Google Scholar] [CrossRef]
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; Gonzalez-Martin, A.; Ledermann, J.; Marth, C.; Nout, R.; Querleu, D.; Mirza, M.R.; et al. ESMO-ESGO-ESTRO con-sensus conference on endometrial cancer: Diagnosis, treatment and follow-up. Int. J. Gynecol. Cancer 2016, 26, 2–30. [Google Scholar] [CrossRef]
- Liao, W.; Li, J.; Feng, W.; Kong, W.; Shen, Y.; Chen, Z.; Yang, H. Pan-immune-inflammation value: A new prognostic index in epithelial ovarian cancer. BMC Cancer 2024, 24, 1052. [Google Scholar] [CrossRef]
- Guven, D.C.; Sahin, T.K.; Erul, E.; Kilickap, S.; Gambichler, T.; Aksoy, S. The association between the pan-immune-inflammation value and cancer prognosis: A systematic review and meta-analysis. Cancers 2022, 14, 2675. [Google Scholar] [CrossRef]
- Yan, S.; Gong, X.; Liu, R.; Jia, X. Prognostic significance of systemic pan-immune-inflammation value in locally ad-vanced cervical cancer. Front. Oncol. 2024, 14, 1492251. [Google Scholar] [CrossRef]
- Chalabiyev, E.; Ismayilov, R.; Kus, F.; Akyildiz, A.; Guven, D.C.; Yildirim, H.C.; Kirmizigul, B.; Koksal, B.; Kavgaci, G.; Arik, Z. Prognostic and predictive significance of the pan-immune-inflammation value in endometrial cancer patients undergoing adjuvant therapy. Rep. Pract. Oncol. Radiother. 2025, 30, 202–209. [Google Scholar] [CrossRef]
- Ji, Y.; Wang, H. Prognostic prediction of systemic immune-inflammation index for patients with gynecological and breast cancers: A meta-analysis. World J. Surg. Oncol. 2020, 18, 197. [Google Scholar] [CrossRef] [PubMed]
- Cummings, M.; Merone, L.; Keeble, C.; Burland, L.; Grzelinski, M.; Sutton, K.; Begum, N.; Thacoor, A.; Green, B.; Sarveswaran, J.; et al. Preoperative neutrophil:lymphocyte and platelet:lymphocyte ratios predict endometrial cancer survival. Br. J. Cancer 2015, 113, 311–320. [Google Scholar] [CrossRef]
- Tu, Y.; Jiang, P.; Wang, J.; Huang, Y.; Kong, W.; Li, N.; Zheng, Y.; Zhou, Q.; Gou, S.; Tian, C.; et al. A novel systemic inflammation response index (SIRI) for predicting postoperative survival of patients with endometrial cancer. Front. Oncol. 2022, 12, 919422. [Google Scholar] [CrossRef]
- Templeton, A.J.; Ace, O.; McNamara, M.G.; Al-Mubarak, M.; Vera-Badillo, F.E.; Hermanns, T.; Šeruga, B.; Ocaña, A.; Tannock, I.F.; Amir, E. Prognostic role of platelet to lymphocyte ratio in solid tumors: A systematic review and meta-analysis. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1204–1212. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Pandey, A.; Dimri, K.; Sehgal, A.; Bhagat, R.; Gill, G. Endometrial cancer risk factors, treatment, and survival outcomes as per the ESMO-ESGO-ESTRO risk groups and FIGO staging: An experience from developing world. J. Cancer Res. Ther. 2023, 19, 701–707. [Google Scholar] [CrossRef]
- Huang, H.; Liu, Q.; Zhu, L.; Zhang, Y.; Lu, X.; Wu, Y.; Liu, L. Prognostic value of preoperative systemic immune-inflammation index in patients with cervical cancer. Sci. Rep. 2019, 9, 3284. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).