
Arrhythmic Mitral Valve Prolapse and Sports Activity: Pathophysiology, Risk Stratification, and Sports Eligibility Assessment

 ,
,  ,
,  , ,
, , 
Abstract
1. Introduction and Epidemiology
2. Definition and Classification of Arrhythmic Mitral Valve Prolapse
- (1)
- AMVP due to moderate-to-severe/severe mitral regurgitation, in which hemodynamic mechanisms (especially LV volume overload) lead to increased risk of VAs and SCD [9], particularly in the presence of severe heart failure symptoms, reduced LV ejection fraction, and atrial arrhythmias. There is scientific evidence that relieving the hemodynamic burden by surgical mitral regurgitation correction may curtail the risk of both overall mortality and SCD, restoring a normal life expectancy [17].
- (2)
- AMVP due to severe myxomatous MVP independent of MR severity or LV dysfunction. This phenotype often involves MAD, severe myxomatous degeneration with leaflet redundancy, excess leaflet length and thickness, and bileaflet MVP [5,32]. Importantly, the arrhythmic outcome of these patients is independent of gender, MR severity, LVEF, or bileaflet MVP [35] and seems to be associated with distinct substrates and triggers favoring arrhythmogenesis (see following paragraph);
- (3)
- The combination of severe LA dilation (in excess of that expected for the degree of MR), atrial tachyarrhythmias (especially atrial fibrillation [AF]), and MVP may be defined as the atrial arrhythmia phenotype of AMVP. In the presence of severe LA dilation and AF, an excess mortality is commonly observed, independently of MR severity and LV dilation and/or dysfunction [36,37], and surgical MR correction may improve prognosis, highlighting the importance of recognizing this subset for informing management [10,11].
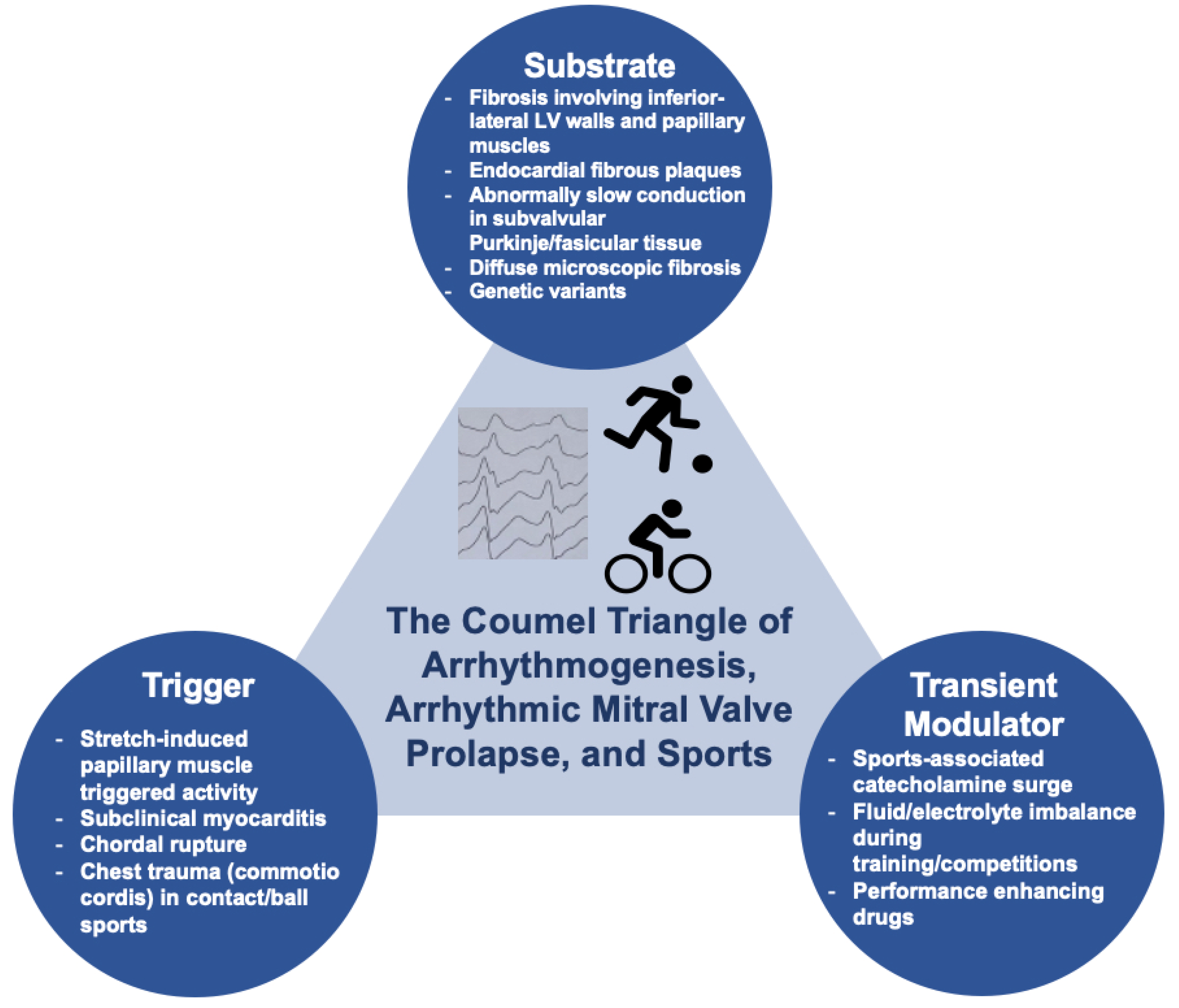
3. Arrhythmogenesis in Mitral Valve Prolapse and Relationship with Physical Exercise
3.1. Abnormal Myocardial Substrate
3.2. Trigger
3.3. Transient Modulator
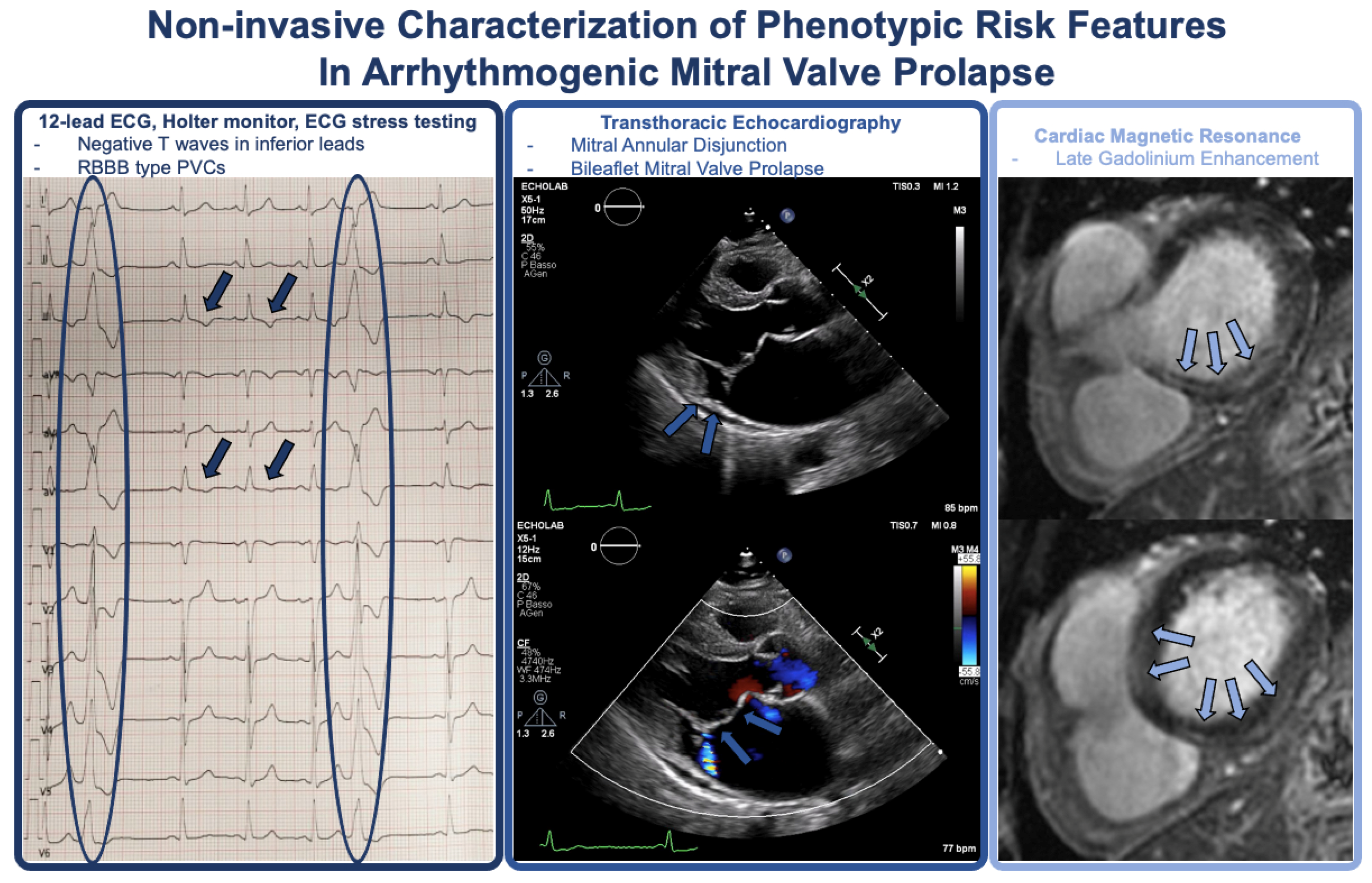
4. Phenotypic Characterization and Risk Stratification
4.1. History and Physical Examination
4.2. Twelve-Lead ECG and Holter Monitoring
- (1)
- High-risk VAs: sustained VT not originating from the right or LV outflow tract, spontaneous polymorphic NSVT, and rapid monomorphic NSVT (>180 bpm);
- (2)
- Intermediate-risk VAs: polymorphic PVCs, monomorphic NSVT at a lower rate (<180 bpm), and highly frequent or complex PVCs (bigeminism and couplets);
- (3)
- Low-risk VAs: frequent PVCs (≥5% total PVC burden) but not complex VAs (and no morphological features suggesting higher risk categories—i.e., patients with monomorphic outflow tract PVCs).
- -
- In patients with unexplained syncope or pre-syncope without high-risk VAs at Holter monitoring;
- -
- In cases of high-risk features, negative CMR, and without indications for an ICD (hemodynamically tolerated VT, NSVT);
- -
- In patients with phenotypical risk features (T-wave inversion in the inferior leads, repetitive documented polymorphic PVCs, MAD, redundant MV leaflets, enlarged left atrium or ejection fraction ≤ 50%) plus positive LGE on CMR.
4.3. Signal Averaged Electrocardiogram
4.4. Exercise Stress Testing
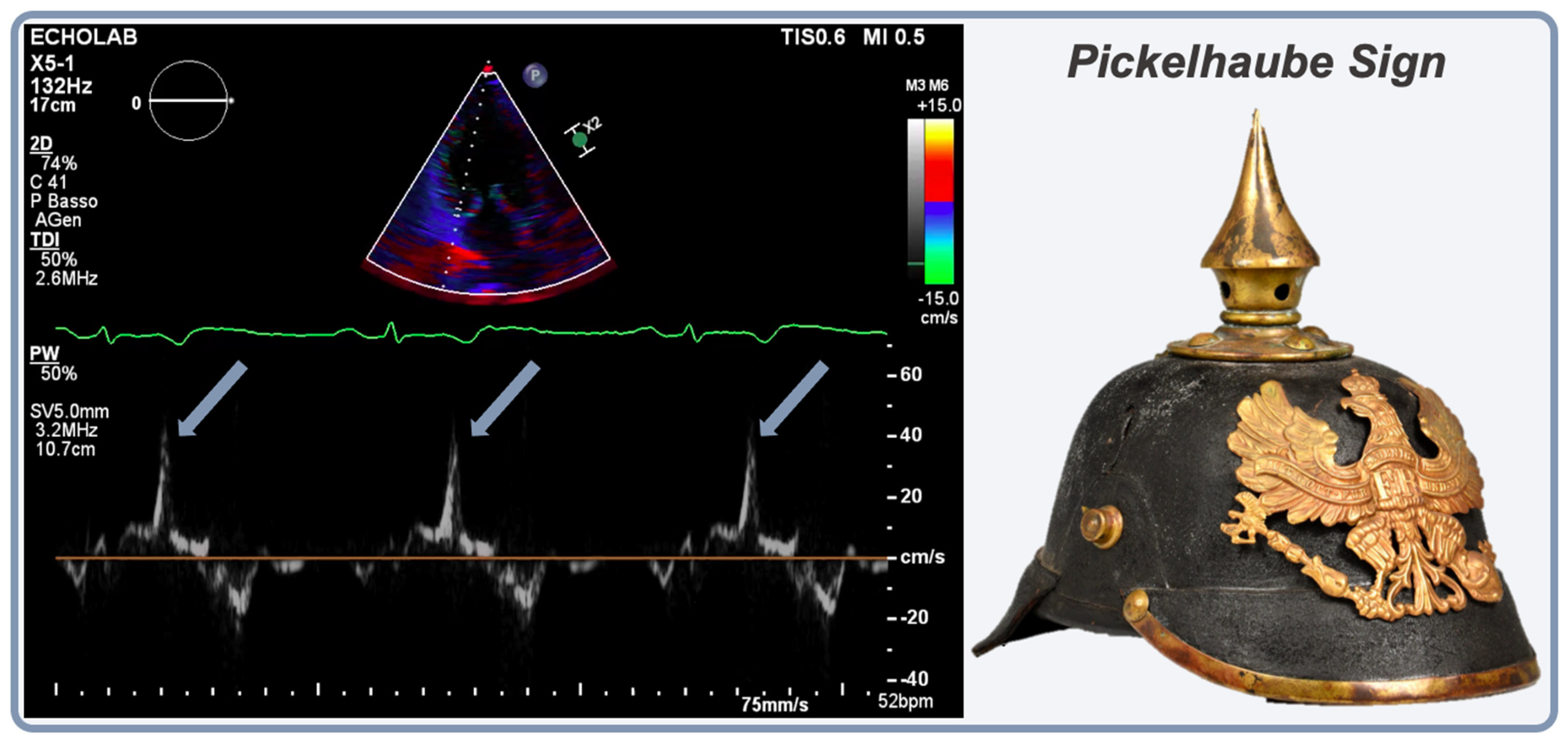
4.5. Transthoracic Echocardiography (TTE)
4.6. Cardiac Magnetic Resonance
- -
- After aborted SCD or sustained VAs, before implanting an ICD;
- -
- In patients with a history of unexplained syncope or documented NSVT;
- -
- In the case of AMVP and at least one phenotypical risk feature;
- -
- In patients in whom echocardiography does not provide an accurate assessment of left/right ventricular function or of MV characteristics.
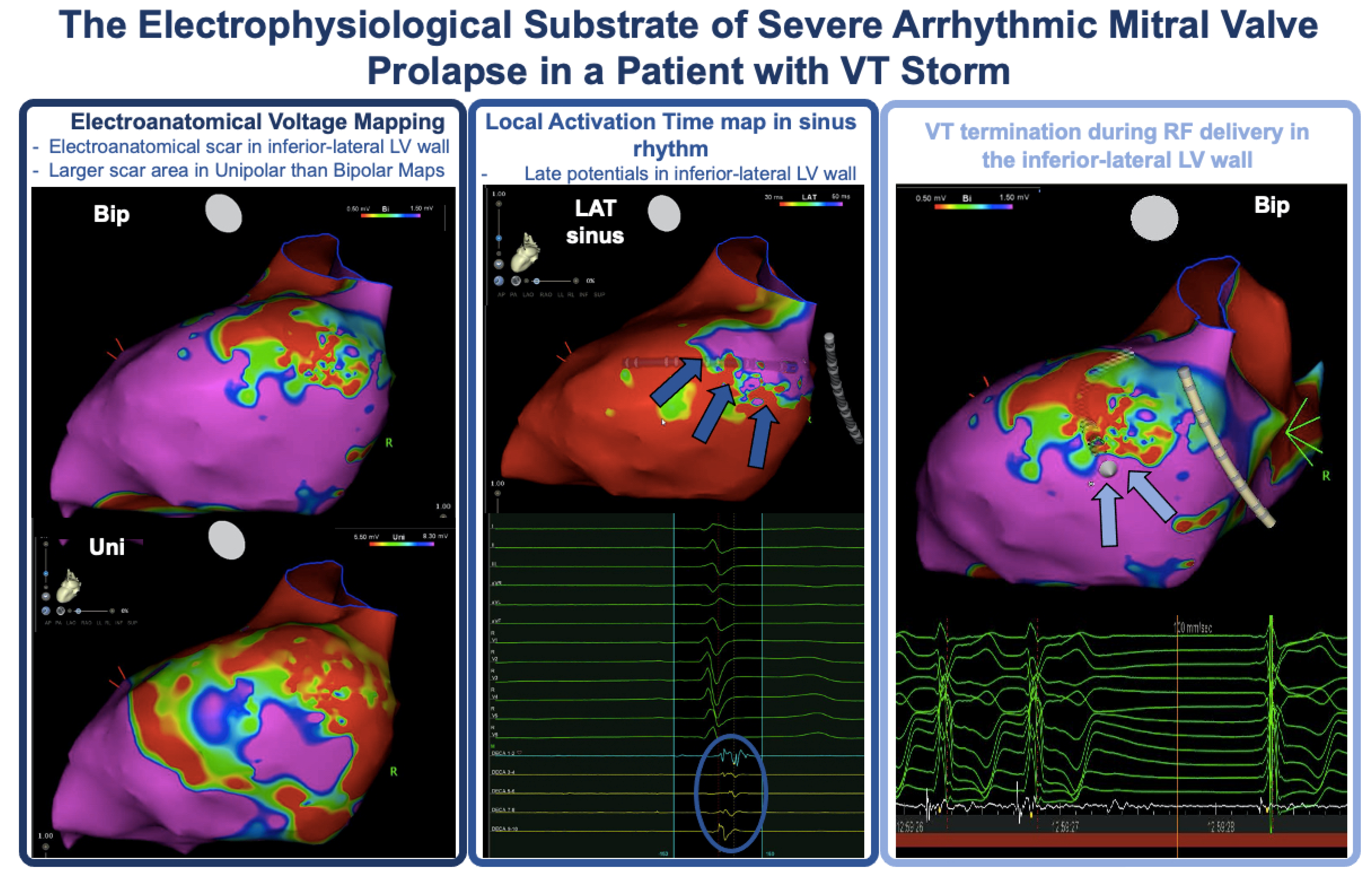
4.7. Electrophysiological Study and Electroanatomical Mapping
5. Sports Eligibility Assessment and Therapy
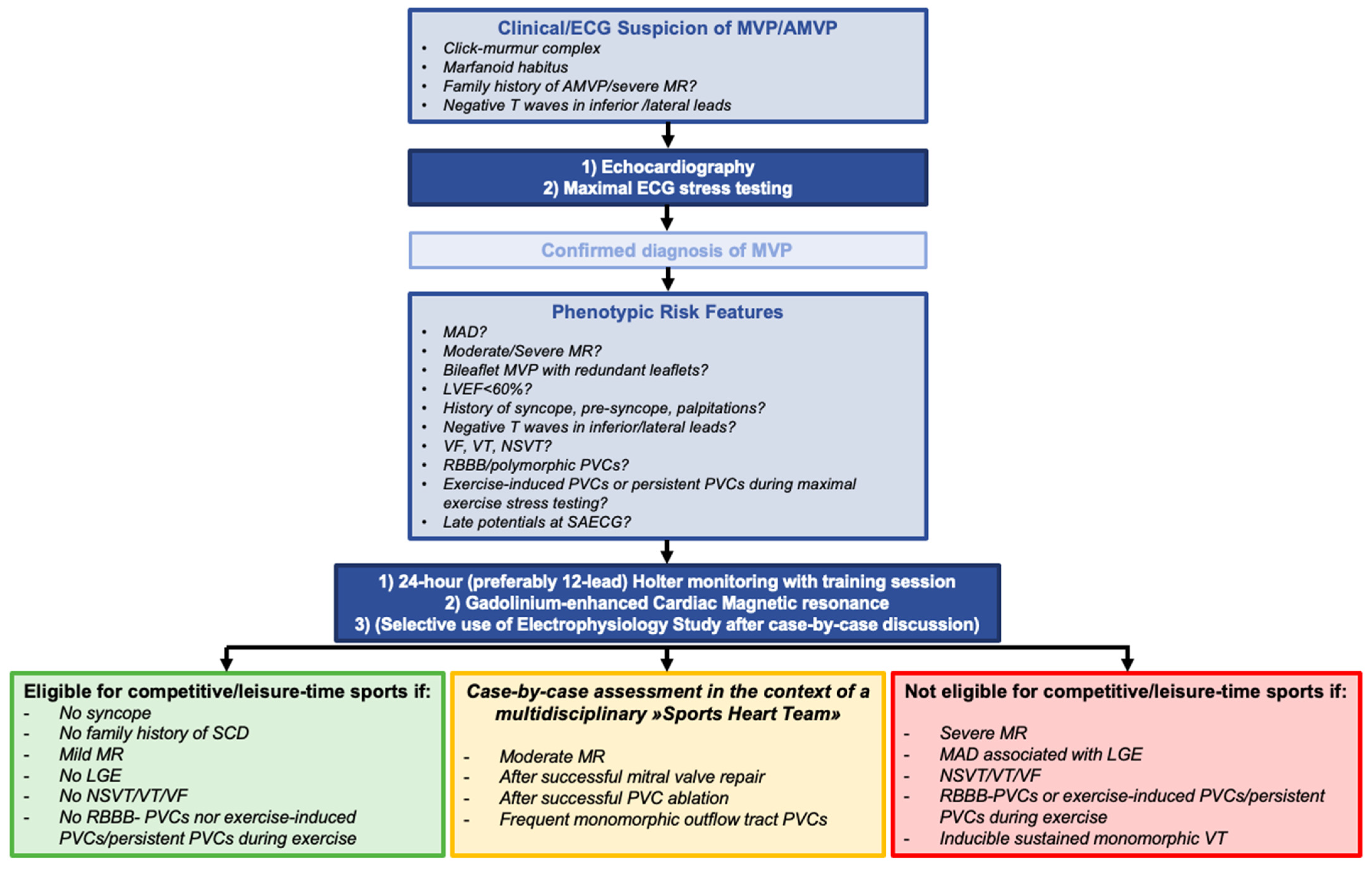
5.1. Sports Eligibility
5.2. Pharmacological Treatment
5.3. PVC/VT Ablation
- (1)
- Ablation of PVCs that trigger recurrent VF;
- (2)
- Ablation of sustained monomorphic VT in cases of recurrent ICD therapies despite antiarrhythmic drug therapy or when pharmacological therapy is contraindicated or not desired/tolerated (Figure 4);
- (3)
- PVC ablation in symptomatic patients, either as an alternative to antiarrhythmic drug treatment or when drugs are not desired, not tolerated, or ineffective;
- (4)
- PVC ablation in patients with PVC-induced LV dysfunction.
5.4. ICD Implantation
5.5. Surgical Correction
6. Gaps in Knowledge and Future Directions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Freed, L.A.; Levy, D.; Levine, R.A.; Larson, M.G.; Evans, J.C.; Fuller, D.L.; Lehman, B.; Benjamin, E.J. Prevalence and clinical outcome of mitral-valve prolapse. N. Engl. J. Med. 1999, 341, 1–7. [Google Scholar] [CrossRef]
- Nkomo, V.T.; Gardin, J.M.; Skelton, T.N.; Gottdiener, J.S.; Scott, C.G.; Enriquez-Sarano, M. Burden of valvular heart diseases: A population-based study. Lancet 2006, 368, 1005–1011. [Google Scholar] [CrossRef]
- Theal, M.; Sleik, K.; Anand, S.; Yi, Q.; Yusuf, S.; Lonn, E. Prevalence of mitral valve prolapse in ethnic groups. Can. J. Cardiol. 2004, 20, 511–515. [Google Scholar] [PubMed]
- Battaglia, V.; Santangelo, G.; Bursi, F.; Simeoli, P.; Guazzi, M. Arrhythmogenic Mitral Valve Prolapse and Sudden Cardiac Death: An Update and Current Perspectives. Curr. Probl. Cardiol. 2023, 48, 101724. [Google Scholar] [CrossRef] [PubMed]
- Sabbag, A.; Essayagh, B.; Barrera, J.D.R.; Basso, C.; Berni, A.; Cosyns, B.; Deharo, J.C.; Deneke, T.; Di Biase, L.; Enriquez-Sarano, M.; et al. EHRA expert consensus statement on arrhythmic mitral valve prolapse and mitral annular disjunction complex in collaboration with the ESC Council on valvular heart disease and the European Association of Cardiovascular Imaging endorsed by the Heart Rhythm Society, by the Asia Pacific Heart Rhythm Society, and by the Latin American Heart Rhythm Society. Europace 2022, 24, 1981–2003. [Google Scholar] [CrossRef]
- Faletra, F.F.; Leo, L.A.; Paiocchi, V.L.; Caretta, A.; Viani, G.M.; Schlossbauer, S.A.; Demertzis, S.; Ho, S.Y. Anatomy of mitral annulus insights from non-invasive imaging techniques. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 843–857. [Google Scholar] [CrossRef]
- Freed, L.A.; Benjamin, E.J.; Levy, D.; Larson, M.G.; Evans, J.C.; Fuller, D.L.; Lehman, B.; Levine, R.A. Mitral valve prolapse in the general population: The benign nature of echocardiographic features in the Framingham Heart Study. J. Am. Coll. Cardiol. 2002, 40, 1298–1304. [Google Scholar] [CrossRef]
- Avierinos, J.F.; Gersh, B.J.; Melton, L.J., 3rd; Bailey, K.R.; Shub, C.; Nishimura, R.A.; Tajik, A.J.; Enriquez-Sarano, M. Natural history of asymptomatic mitral valve prolapse in the community. Circulation 2002, 106, 1355–1361. [Google Scholar] [CrossRef]
- Antoine, C.; Benfari, G.; Michelena, H.I.; Maalouf, J.F.; Nkomo, V.T.; Thapa, P.; Enriquez-Sarano, M. Clinical Outcome of Degenerative Mitral Regurgitation: Critical Importance of Echocardiographic Quantitative Assessment in Routine Practice. Circulation 2018, 138, 1317–1326. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e72–e227. [Google Scholar] [CrossRef]
- Barlow, J.B.; Bosman, C.K. Aneurysmal protrusion of the posterior leaflet of the mitral valve. An auscultatory-electrocardiographic syndrome. Am. Heart J. 1966, 71, 166–178. [Google Scholar] [CrossRef]
- Nishimura, R.A.; McGoon, M.D.; Shub, C.; Miller, F.A., Jr.; Ilstrup, D.M.; Tajik, A.J. Echocardiographically documented mitral-valve prolapse. Long-term follow-up of 237 patients. N. Engl. J. Med. 1985, 313, 1305–1309. [Google Scholar] [CrossRef] [PubMed]
- Düren, D.R.; Becker, A.E.; Dunning, A.J. Long-term follow-up of idiopathic mitral valve prolapse in 300 patients: A prospective study. J. Am. Coll. Cardiol. 1988, 11, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, K.; Uy-Evanado, A.; Teodorescu, C.; Reinier, K.; Nichols, G.A.; Gunson, K.; Jui, J.; Chugh, S.S. Mitral valve prolapse and sudden cardiac arrest in the community. Heart Rhythm. 2016, 13, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Basso, C.; Iliceto, S.; Thiene, G.; Perazzolo Marra, M. Mitral Valve Prolapse, Ventricular Arrhythmias, and Sudden Death. Circulation 2019, 140, 952–964. [Google Scholar] [CrossRef]
- Grigioni, F.; Enriquez-Sarano, M.; Ling, L.H.; Bailey, K.R.; Seward, J.B.; Tajik, A.J.; Frye, R.L. Sudden death in mitral regurgitation due to flail leaflet. J. Am. Coll. Cardiol. 1999, 34, 2078–2085. [Google Scholar] [CrossRef]
- Nalliah, C.J.; Mahajan, R.; Elliott, A.D.; Haqqani, H.; Lau, D.H.; Vohra, J.K.; Morton, J.B.; Semsarian, C.; Marwick, T.; Kalman, J.M.; et al. Mitral valve prolapse and sudden cardiac death: A systematic review and meta-analysis. Heart 2019, 105, 144–151. [Google Scholar] [CrossRef]
- Basso, C.; Perazzolo Marra, M.; Rizzo, S.; De Lazzari, M.; Giorgi, B.; Cipriani, A.; Frigo, A.C.; Rigato, I.; Migliore, F.; Pilichou, K.; et al. Arrhythmic Mitral Valve Prolapse and Sudden Cardiac Death. Circulation 2015, 132, 556–566. [Google Scholar] [CrossRef]
- Delling, F.N.; Aung, S.; Vittinghoff, E.; Dave, S.; Lim, L.J.; Olgin, J.E.; Connolly, A.; Moffatt, E.; Tseng, Z.H. Antemortem and Post-Mortem Characteristics of Lethal Mitral Valve Prolapse Among All Countywide Sudden Deaths. JACC Clin Electrophysiol. 2021, 7, 1025–1034. [Google Scholar] [CrossRef]
- Basso, C.; Calabrese, F.; Corrado, D.; Thiene, G. Postmortem diagnosis in sudden cardiac death victims: Macroscopic, microscopic and molecular findings. Cardiovasc. Res. 2001, 50, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Caselli, S.; Mango, F.; Clark, J.; Pandian, N.G.; Corrado, D.; Autore, C.; Pelliccia, A. Prevalence and Clinical Outcome of Athletes with Mitral Valve Prolapse. Circulation 2018, 137, 2080–2082. [Google Scholar] [CrossRef] [PubMed]
- Finocchiaro, G.; Papadakis, M.; Robertus, J.L.; Dhutia, H.; Steriotis, A.K.; Tome, M.; Mellor, G.; Merghani, A.; Malhotra, A.; Behr, E.; et al. Etiology of Sudden Death in Sports: Insights from a United Kingdom Regional Registry. J. Am. Coll. Cardiol. 2016, 67, 2108–2115. [Google Scholar] [CrossRef]
- Maron, B.J.; Haas, T.S.; Ahluwalia, A.; Murphy, C.J.; Garberich, R.F. Demographics and Epidemiology of Sudden Deaths in Young Competitive Athletes: From the United States National Registry. Am. J. Med. 2016, 129, 1170–1177. [Google Scholar] [CrossRef]
- Burke, A.P.; Farb, A.; Virmani, R.; Goodin, J.; Smialek, J.E. Sports-related and non-sports-related sudden cardiac death in young adults. Am. Heart J. 1991, 121 Pt 1, 568–575. [Google Scholar] [CrossRef]
- Van Camp, S.P.; Bloor, C.M.; Mueller, F.O.; Cantu, R.C.; Olson, H.G. Nontraumatic sports death in high school and college athletes. Med. Sci. Sports Exerc. 1995, 27, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Shirani, J.; Poliac, L.C.; Mathenge, R.; Roberts, W.C.; Mueller, F.O. Sudden death in young competitive athletes. Clinical, demographic, and pathological profiles. JAMA 1996, 276, 199–204. [Google Scholar] [CrossRef]
- Maron, B.J.; Doerer, J.J.; Haas, T.S.; Tierney, D.M.; Mueller, F.O. Sudden deaths in young competitive athletes: Analysis of 1866 deaths in the United States, 1980–2006. Circulation 2009, 119, 1085–1092. [Google Scholar] [CrossRef]
- Maron, B.J.; Haas, T.S.; Murphy, C.J.; Ahluwalia, A.; Rutten-Ramos, S. Incidence and causes of sudden death in U.S. college athletes. J. Am. Coll Cardiol. 2014, 63, 1636–1643. [Google Scholar] [CrossRef]
- Five, C.K.; Hasselberg, N.E.; Aaserud, L.T.; Castrini, A.I.; Vlaisavljevic, K.; Lie, Ø.; Rootwelt-Norberg, C.; Aabel, E.W.; Haugaa, K.H. Lifetime exercise dose and ventricular arrhythmias in patients with mitral valve prolapse. Europace 2023, 25, euad309. [Google Scholar] [CrossRef]
- D’Ascenzi, F.; Valentini, F.; Pistoresi, S.; Frascaro, F.; Piu, P.; Cavigli, L.; Valente, S.; Focardi, M.; Cameli, M.; Bonifazi, M.; et al. Causes of sudden cardiac death in young athletes and non-athletes: Systematic review and meta-analysis: Sudden cardiac death in the young. Trends Cardiovasc. Med. 2022, 32, 299–308. [Google Scholar] [CrossRef]
- Essayagh, B.; Sabbag, A.; El-Am, E.; Cavalcante, J.L.; Michelena, H.I.; Enriquez-Sarano, M. Arrhythmic mitral valve prolapse and mitral annular disjunction: Pathophysiology, risk stratification, and management. Eur. Heart J. 2023, 10, ehad491. [Google Scholar] [CrossRef]
- Zorzi, A.; D’Ascenzi, F.; Andreini, D.; Castelletti, S.; Casella, M.; Cavarretta, E.; Cipriani, A.; Compagnucci, P.; Delise, P.; Dello Russo, A.; et al. Interpretation and management of premature ventricular beats in athletes: An expert opinion document of the Italian Society of Sports Cardiology (SICSPORT). Int. J. Cardiol. 2023, 391, 131220. [Google Scholar] [CrossRef]
- Muser, D.; Tritto, M.; Mariani, M.V.; Di Monaco, A.; Compagnucci, P.; Accogli, M.; De Ponti, R.; Guarracini, F. Diagnosis and Treatment of Idiopathic Premature Ventricular Contractions: A Stepwise Approach Based on the Site of Origin. Diagnostics 2021, 11, 1840. [Google Scholar] [CrossRef] [PubMed]
- Essayagh, B.; Sabbag, A.; Antoine, C.; Benfari, G.; Yang, L.T.; Maalouf, J.; Asirvatham, S.; Michelena, H.; Enriquez-Sarano, M. Presentation and Outcome of Arrhythmic Mitral Valve Prolapse. J. Am. Coll. Cardiol. 2020, 76, 637–649. [Google Scholar] [CrossRef] [PubMed]
- Essayagh, B.; Antoine, C.; Benfari, G.; Messika-Zeitoun, D.; Michelena, H.; Le Tourneau, T.; Mankad, S.; Tribouilloy, C.M.; Thapa, P.; Enriquez-Sarano, M. Prognostic Implications of Left Atrial Enlargement in Degenerative Mitral Regurgitation. J. Am. Coll. Cardiol. 2019, 74, 858–870. [Google Scholar] [CrossRef] [PubMed]
- Grigioni, F.; Benfari, G.; Vanoverschelde, J.L.; Tribouilloy, C.; Avierinos, J.F.; Bursi, F.; Suri, R.M.; Guerra, F.; Pasquet, A.; Rusinaru, D.; et al. MIDA Investigators. Long-Term Implications of Atrial Fibrillation in Patients with Degenerative Mitral Regurgitation. J. Am. Coll. Cardiol. 2019, 73, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.A.; Dukkipati, S.R.; Turagam, M.; Liao, S.L.; Adams, D.H.; Reddy, V.Y. Arrhythmic Mitral Valve Prolapse: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2018, 72 Pt A, 2904–2914. [Google Scholar] [CrossRef]
- Perazzolo Marra, M.; Basso, C.; De Lazzari, M.; Rizzo, S.; Cipriani, A.; Giorgi, B.; Lacognata, C.; Rigato, I.; Migliore, F.; Pilichou, K.; et al. Morphofunctional Abnormalities of Mitral Annulus and Arrhythmic Mitral Valve Prolapse. Circ. Cardiovasc. Imaging 2016, 9, e005030. [Google Scholar] [CrossRef] [PubMed]
- Kitkungvan, D.; Nabi, F.; Kim, R.J.; Bonow, R.O.; Khan, M.A.; Xu, J.; Little, S.H.; Quinones, M.A.; Lawrie, G.M.; Zoghbi, W.A.; et al. Myocardial Fibrosis in Patients with Primary Mitral Regurgitation with and without Prolapse. J. Am. Coll. Cardiol. 2018, 72, 823–834. [Google Scholar] [CrossRef] [PubMed]
- Constant Dit Beaufils, A.L.; Huttin, O.; Jobbe-Duval, A.; Senage, T.; Filippetti, L.; Piriou, N.; Cueff, C.; Venner, C.; Mandry, D.; Sellal, J.M.; et al. Replacement Myocardial Fibrosis in Patients with Mitral Valve Prolapse: Relation to Mitral Regurgitation, Ventricular Remodeling, and Arrhythmia. Circulation 2021, 143, 1763–1774. [Google Scholar] [CrossRef]
- Levy, S.; Sharaf Dabbagh, G.; Giudicessi, J.R.; Haqqani, H.; Khanji, M.Y.; Obeng-Gyimah, E.; Betts, M.N.; Ricci, F.; Asatryan, B.; Bouatia-Naji, N.; et al. Genetic mechanisms underlying arrhythmogenic mitral valve prolapse: Current and future perspectives. Heart Rhythm O2 2023, 4, 581–591. [Google Scholar] [CrossRef]
- Villatore, A.; Sala, S.; Stella, S.; Vignale, D.; Busnardo, E.; Esposito, A.; Basso, C.; Della Bella, P.; Mazzone, P.; Peretto, G. Autoimmune Myocarditis and Arrhythmogenic Mitral Valve Prolapse: An Unexpected Overlap Syndrome. J. Cardiovasc. Dev. Dis. 2021, 8, 151. [Google Scholar] [CrossRef]
- Peretto, G.; Casella, M.; Merlo, M.; Benedetti, S.; Rizzo, S.; Cappelletto, C.; Di Resta, C.; Compagnucci, P.; De Gaspari, M.; Dello Russo, A.; et al. Inflammation on Endomyocardial Biopsy Predicts Risk of MACE in Undefined Left Ventricular Arrhythmogenic Cardiomyopathy. JACC Clin. Electrophysiol. 2023, 9 Pt 1, 951–961. [Google Scholar] [CrossRef]
- Compagnucci, P.; Volpato, G.; Falanga, U.; Cipolletta, L.; Conti, M.A.; Grifoni, G.; Ciliberti, G.; Stronati, G.; Fogante, M.; Bergonti, M.; et al. Myocardial Inflammation, Sports Practice, and Sudden Cardiac Death: 2021 Update. Medicina 2021, 57, 277. [Google Scholar] [CrossRef]
- Casella, M.; Gasperetti, A.; Compagnucci, P.; Narducci, M.L.; Pelargonio, G.; Catto, V.; Carbucicchio, C.; Bencardino, G.; Conte, E.; Schicchi, N.; et al. Different Phases of Disease in Lymphocytic Myocarditis: Clinical and Electrophysiological Characteristics. JACC Clin. Electrophysiol. 2023, 9, 314–326. [Google Scholar] [CrossRef] [PubMed]
- Compagnucci, P.; Volpato, G.; Pascucci, R.; Falanga, U.; Misiani, A.; Molini, S.; Spinucci, G.; Cipolletta, L.; Conti, M.; Grifoni, G.; et al. Impact of the COVID-19 Pandemic on a Tertiary-Level Electrophysiology Laboratory in Italy. Circ. Arrhythm. Electrophysiol. 2020, 13, e008774. [Google Scholar] [CrossRef] [PubMed]
- Franz, M.R. Mechano-electrical feedback. Cardiovasc. Res. 2000, 45, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Gornick, C.C.; Tobler, H.G.; Pritzker, M.C.; Tuna, I.C.; Almquist, A.; Benditt, D.G. Electrophysiologic effects of papillary muscle traction in the intact heart. Circulation 1986, 73, 1013–1021. [Google Scholar] [CrossRef]
- Compagnucci, P.; Casella, M.; Bianchi, V.; Franculli, F.; Vitali, F.; Santini, L.; Savarese, G.; Santobuono, V.E.; Chianese, R.; Lavalle, C.; et al. Implantable defibrillator-detected heart failure status predicts ventricular tachyarrhythmias. J. Cardiovasc. Electrophysiol. 2023, 34, 1257–1267. [Google Scholar] [CrossRef] [PubMed]
- Hong-TaoYuan Yang, M.; Zhong, L.; Lee, Y.H.; Vaidya, V.R.; Asirvatham, S.J.; Ackerman, M.J.; Pislaru, S.V.; Suri, R.M.; Slusser, J.P.; Hodge, D.O.; et al. Ventricular premature contraction associated with mitral valve prolapse. Int. J. Cardiol. 2016, 221, 1144–1149. [Google Scholar] [CrossRef]
- Syed, F.F.; Ackerman, M.J.; McLeod, C.J.; Kapa, S.; Mulpuru, S.K.; Sriram, C.S.; Cannon, B.C.; Asirvatham, S.J.; Noseworthy, P.A. Sites of Successful Ventricular Fibrillation Ablation in Bileaflet Mitral Valve Prolapse Syndrome. Circ. Arrhythm. Electrophysiol. 2016, 9, e004005. [Google Scholar] [CrossRef]
- Marano, P.J.; Lim, L.J.; Sanchez, J.M.; Alvi, R.; Nah, G.; Badhwar, N.; Gerstenfeld, E.P.; Tseng, Z.H.; Marcus, G.M.; Delling, F.N. Long-term outcomes of ablation for ventricular arrhythmias in mitral valve prolapse. J. Interv. Card. Electrophysiol. 2021, 61, 145–154. [Google Scholar] [CrossRef]
- Santoro, F.; Di Biase, L.; Hranitzky, P.; Sanchez, J.E.; Santangeli, P.; Perini, A.P.; Burkhardt, J.D.; Natale, A. Ventricular fibrillation triggered by PVCs from papillary muscles: Clinical features and ablation. J. Cardiovasc. Electrophysiol. 2014, 25, 1158–1164. [Google Scholar] [CrossRef]
- Raina, A.; Gersh, B.J.; Asirvatham, S.J.; Del-Carpio Munoz, F. Characterization of ventricular arrhythmias and sudden cardiac death in subjects with mitral valve prolapse and mitral annular disjunction. Heart Rhythm. 2023, 20, 112–121. [Google Scholar] [CrossRef]
- Franz, M.R.; Cima, R.; Wang, D.; Profitt, D.; Kurz, R. Electrophysiological effects of myocardial stretch and mechanical determinants of stretch-activated arrhythmias. Circulation 1992, 86, 968–978. [Google Scholar] [CrossRef] [PubMed]
- Theofilogiannakos, E.K.; Boudoulas, K.D.; Gawronski, B.E.; Langaee, T.Y.; Dardas, P.S.; Ninios, V.; Kelpis, T.G.; Johnson, J.A.; Pitsis, A.A.; Boudoulas, H. Floppy mitral valve/mitral valve prolapse syndrome: Beta-adrenergic receptor polymorphism may contribute to the pathogenesis of symptoms. J. Cardiol. 2015, 65, 434–438. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Volpato, G.; Falanga, U.; Cipolletta, L.; Conti, M.A.; Grifoni, G.; Ciliberti, G.; Urbinati, A.; Barbarossa, A.; Stronati, G.; Fogante, M.; et al. Sports Activity and Arrhythmic Risk in Cardiomyopathies and Channelopathies: A Critical Review of European Guidelines on Sports Cardiology in Patients with Cardiovascular Diseases. Medicina 2021, 57, 308. [Google Scholar] [CrossRef] [PubMed]
- La Gerche, A.; Brosnan, M.J. Cardiovascular Effects of Performance-Enhancing Drugs. Circulation 2017, 135, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. ESC Scientific Document Group. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef] [PubMed]
- Comitato Organizzativo Cardiologico per l’idoneità allo Sport. Protocolli Cardiologici Per Il Giudizio Di Idoneità Allo Sport Agonistico, 6th ed.; CESI: Rome, Italy, 2023. [Google Scholar]
- Cavarretta, E.; Peruzzi, M.; Versaci, F.; Frati, G.; Sciarra, L. How to manage an athlete with mitral valve prolapse. Eur. J. Prev. Cardiol. 2021, 28, 1110–1117. [Google Scholar] [CrossRef]
- Hiemstra, Y.L.; Wijngaarden, A.L.V.; Bos, M.W.; Schalij, M.J.; Klautz, R.J.; Bax, J.J.; Delgado, V.; Barge-Schaapveld, D.Q.; Marsan, N.A. Familial occurrence of mitral regurgitation in patients with mitral valve prolapse undergoing mitral valve surgery. Eur. J. Prev. Cardiol. 2020, 27, 272–280. [Google Scholar] [CrossRef]
- Chakrabarti, A.K.; Bogun, F.; Liang, J.J. Arrhythmic Mitral Valve Prolapse and Mitral Annular Disjunction: Clinical Features, Pathophysiology, Risk Stratification, and Management. J. Cardiovasc. Dev. Dis. 2022, 9, 61. [Google Scholar] [CrossRef] [PubMed]
- Han, H.C.; Ha, F.J.; Teh, A.W.; Calafiore, P.; Jones, E.F.; Johns, J.; Koshy, A.N.; O’Donnell, D.; Hare, D.L.; Farouque, O.; et al. Mitral Valve Prolapse and Sudden Cardiac Death: A Systematic Review. J. Am. Heart Assoc. 2018, 7, e010584. [Google Scholar] [CrossRef] [PubMed]
- Sriram, C.S.; Syed, F.F.; Ferguson, M.E.; Johnson, J.N.; Enriquez-Sarano, M.; Cetta, F.; Cannon, B.C.; Asirvatham, S.J.; Ackerman, M.J. Malignant bileaflet mitral valve prolapse syndrome in patients with otherwise idiopathic out-of-hospital cardiac arrest. J. Am. Coll. Cardiol. 2013, 62, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Benjanuwattra, J.; Kewcharoen, J.; Phinyo, P.; Swusdinaruenart, S.; Abdelnabi, M.; Del Rio-Pertuz, G.; Leelaviwat, N.; Navaravong, L. High-risk phenotypes of arrhythmic mitral valve prolapse: A systematic review and meta-analysis. Acta Cardiol. 2023, 78, 1012–1019. [Google Scholar] [CrossRef] [PubMed]
- Vergara, P.; Scarfò, I.; Esposito, A.; Colantoni, C.; Palmisano, A.; Altizio, S.; Falasconi, G.; Pannone, L.; Lapenna, E.; Gulletta, S.; et al. Characterization of the electrophysiological substrate in patients with Barlow’s disease. J. Cardiovasc. Electrophysiol. 2021, 32, 3179–3186. [Google Scholar] [CrossRef]
- Enriquez, A.; Shirai, Y.; Huang, J.; Liang, J.; Briceño, D.; Hayashi, T.; Muser, D.; Fulton, B.; Han, Y.; Perez, A.; et al. Papillary muscle ventricular arrhythmias in patients with arrhythmic mitral valve prolapse: Electrophysiologic substrate and catheter ablation outcomes. J. Cardiovasc. Electrophysiol. 2019, 30, 827–835. [Google Scholar] [CrossRef] [PubMed]
- Aabel, E.W.; Chivulescu, M.; Lie, Ø.H.; Hopp, E.; Gjertsen, E.; Ribe, M.; Helle-Valle, T.M.; Edvardsen, T.; Hegbom, F.; Dejgaard, L.A.; et al. Ventricular arrhythmias in arrhythmic mitral valve syndrome-a prospective continuous long-term cardiac monitoring study. Europace 2023, 25, 506–516. [Google Scholar] [CrossRef] [PubMed]
- Gatzoulis, K.A.; Arsenos, P.; Trachanas, K.; Dilaveris, P.; Antoniou, C.; Tsiachris, D.; Sideris, S.; Kolettis, T.M.; Tousoulis, D. Signal-averaged electrocardiography: Past, present, and future. J. Arrhythm. 2018, 34, 222–229. [Google Scholar] [CrossRef]
- Bertoni, P.D.; Cozzi, G.; Guidali, P.; Canziani, R. Studio dei potenziali tardivi in pazienti con prolasso della valvola mitrale [Late potentials in patients with prolapse of the mitral valve]. Minerva Cardioangiol. 1991, 39, 433–436. [Google Scholar]
- Jabi, H.; Burger, A.J.; Orawiec, B.; Touchon, R.C. Late potentials in mitral valve prolapse. Am. Heart J. 1991, 122, 1340–1345. [Google Scholar] [CrossRef]
- Babuty, D.; Cosnay, P.; Breuillac, J.C.; Charniot, J.C.; Delhomme, C.; Fauchier, L.; Fauchier, J.P. Ventricular arrhythmia factors in mitral valve prolapse. Pacing Clin. Electrophysiol. 1994, 17, 1090–1099. [Google Scholar] [CrossRef]
- Maraglino, G.; Sturaro, M.; Toniolo, G.; Accurso, V.; Pastore, G.; Palatini, P. Relazione tra potenziali tardivi ventricolari e aritmie ventricolari nel prolasso valvolare mitralico [Relations between ventricular late potentials and ventricular arrhythmias in mitral valve prolapse]. G. Ital. Cardiol. 1994, 24, 957–964. [Google Scholar] [PubMed]
- Nomura, M.; Nakaya, Y.; Kishi, F.; Kondo, Y.; Yukinaka, M.; Saito, K.; Ito, S. Signal averaged electrocardiogram after exercise in patients with mitral valve prolapse. J. Med. 1997, 28, 62–74. [Google Scholar] [PubMed]
- Koutlianos, N.A.; Kouidi, E.J.; Metaxas, T.I.; Deligiannis, A.P. Non-invasive cardiac electrophysiological indices in soccer players with mitral valve prolapse. Eur. J. Cardiovasc. Prev. Rehabil. 2004, 11, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Gatzoulis, K.A.; Tsiachris, D.; Arsenos, P.; Antoniou, C.K.; Dilaveris, P.; Sideris, S.; Kanoupakis, E.; Simantirakis, E.; Korantzopoulos, P.; Goudevenos, I.; et al. Arrhythmic risk stratification in post-myocardial infarction patients with preserved ejection fraction: The PRESERVE EF study. Eur. Heart J. 2019, 40, 2940–2949. [Google Scholar] [CrossRef]
- Gatzoulis, K.A.; Dilaveris, P.; Arsenos, P.; Tsiachris, D.; Antoniou, C.K.; Sideris, S.; Kolettis, T.; Kanoupakis, E.; Sideris, A.; Flevari, P.; et al. ReCONSIDER study Investigators. Arrhythmic risk stratification in nonischemic dilated cardiomyopathy: The ReCONSIDER study design—A two-step, multifactorial, electrophysiology-inclusive approach. Hellenic J. Cardiol. 2021, 62, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, N.A.; Charron, P.; Corrado, D.; Dagres, N.; de Chillou, C.; et al. ESC Scientific Document Group. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur. Heart J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef] [PubMed]
- Morshedi-Meibodi, A.; Evans, J.C.; Levy, D.; Larson, M.G.; Vasan, R.S. Clinical correlates and prognostic significance of exercise-induced ventricular premature beats in the community: The Framingham Heart Study. Circulation 2004, 109, 2417–2422. [Google Scholar] [CrossRef]
- Refaat, M.M.; Gharios, C.; Moorthy, M.V.; Abdulhai, F.; Blumenthal, R.S.; Jaffa, M.A.; Mora, S. Exercise-Induced Ventricular Ectopy and Cardiovascular Mortality in Asymptomatic Individuals. J. Am. Coll. Cardiol. 2021, 78, 2267–2277. [Google Scholar] [CrossRef]
- Frolkis, J.P.; Pothier, C.E.; Blackstone, E.H.; Lauer, M.S. Frequent ventricular ectopy after exercise as a predictor of death. N. Engl. J. Med. 2003, 348, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Sarto, P.; Zorzi, A.; Merlo, L.; Vessella, T.; Pegoraro, C.; Giorgiano, F.; Graziano, F.; Basso, C.; Drezner, J.A.; Corrado, D. Value of screening for the risk of sudden cardiac death in young competitive athletes. Eur. Heart J. 2023, 44, 1084–1092. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Pibarot, P.; Chambers, J.; La Canna, G.; Pepi, M.; Dulgheru, R.; Dweck, M.; Delgado, V.; Garbi, M.; Vannan, M.A.; et al. Scientific Document Committee of the European Association of Cardiovascular Imaging. Multi-modality imaging assessment of native valvular regurgitation: An EACVI and ESC council of valvular heart disease position paper. Eur. Heart J. Cardiovasc. Imaging 2022, 23, e171–e232. [Google Scholar] [CrossRef] [PubMed]
- van Wijngaarden, A.L.; Kruithof, B.P.T.; Vinella, T.; Barge-Schaapveld, D.Q.C.M.; Ajmone Marsan, N. Characterization of Degenerative Mitral Valve Disease: Differences between Fibroelastic Deficiency and Barlow’s Disease. J. Cardiovasc. Dev. Dis. 2021, 8, 23. [Google Scholar] [CrossRef] [PubMed]
- Essayagh, B.; Sabbag, A.; Antoine, C.; Benfari, G.; Batista, R.; Yang, L.T.; Maalouf, J.; Thapa, P.; Asirvatham, S.; Michelena, H.I.; et al. The Mitral Annular Disjunction of Mitral Valve Prolapse: Presentation and Outcome. JACC Cardiovasc. Imaging 2021, 14, 2073–2087. [Google Scholar] [CrossRef] [PubMed]
- Oliveri, F.; Kakargias, F.; Panday, P.; Arcia Franchini, A.P.; Iskander, B.; Anwer, F.; Hamid, P. Arrhythmic mitral valve prolapse: Diagnostic parameters for high-risk patients: A systematic review and meta-analysis. Pacing Clin. Electrophysiol. 2021, 44, 1746–1755. [Google Scholar] [CrossRef]
- Muthukumar, L.; Rahman, F.; Jan, M.F.; Shaikh, A.; Kalvin, L.; Dhala, A.; Jahangir, A.; Tajik, A.J. The Pickelhaube Sign: Novel Echocardiographic Risk Marker for Malignant Mitral Valve Prolapse Syndrome. JACC Cardiovasc. Imaging 2017, 10, 1078–1080. [Google Scholar] [CrossRef]
- Han, Y.; Peters, D.C.; Salton, C.J.; Bzymek, D.; Nezafat, R.; Goddu, B.; Kissinger, K.V.; Zimetbaum, P.J.; Manning, W.J.; Yeon, S.B. Cardiovascular magnetic resonance characterization of mitral valve prolapse. JACC Cardiovasc. Imaging 2008, 1, 294–303. [Google Scholar] [CrossRef]
- Bui, A.H.; Roujol, S.; Foppa, M.; Kissinger, K.V.; Goddu, B.; Hauser, T.H.; Zimetbaum, P.J.; Ngo, L.H.; Manning, W.J.; Nezafat, R.; et al. Diffuse myocardial fibrosis in patients with mitral valve prolapse and ventricular arrhythmia. Heart 2017, 103, 204–209. [Google Scholar] [CrossRef]
- Dejgaard, L.A.; Skjølsvik, E.T.; Lie, Ø.H.; Ribe, M.; Stokke, M.K.; Hegbom, F.; Scheirlynck, E.S.; Gjertsen, E.; Andresen, K.; Helle-Valle, T.M.; et al. The Mitral Annulus Disjunction Arrhythmic Syndrome. J. Am. Coll. Cardiol. 2018, 72, 1600–1609. [Google Scholar] [CrossRef] [PubMed]
- Dello Russo, A.; Compagnucci, P.; Zorzi, A.; Cavarretta, E.; Castelletti, S.; Contursi, M.; D’Aleo, A.; D’Ascenzi, F.; Mos, L.; Palmieri, V.; et al. Electroanatomic mapping in athletes: Why and when. An expert opinion paper from the Italian Society of Sports Cardiology. Int. J. Cardiol. 2023, 383, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Moya, A.; de Lange, F.J.; Deharo, J.C.; Elliott, P.M.; Fanciulli, A.; Fedorowski, A.; Furlan, R.; Kenny, R.A.; Martín, A.; et al. ESC Scientific Document Group. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur. Heart J. 2018, 39, 1883–1948. [Google Scholar] [CrossRef] [PubMed]
- Gasperetti, A.; Carrick, R.T.; Costa, S.; Compagnucci, P.; Bosman, L.P.; Chivulescu, M.; Tichnell, C.; Murray, B.; Tandri, H.; Tadros, R.; et al. Programmed Ventricular Stimulation as an Additional Primary Prevention Risk Stratification Tool in Arrhythmogenic Right Ventricular Cardiomyopathy: A Multinational Study. Circulation 2022, 146, 1434–1443. [Google Scholar] [CrossRef]
- Ezzeddine, F.M.; Siontis, K.C.; Giudicessi, J.; Ackerman, M.J.; Killu, A.M.; Deshmukh, A.J.; Madhavan, M.; van Zyl, M.; Vaidya, V.R.; Karki, R.; et al. Substrate Characterization and Outcomes of Catheter Ablation of Ventricular Arrhythmias in Patients with Mitral Annular Disjunction. Circ. Arrhythm. Electrophysiol. 2022, 15, e011088. [Google Scholar] [CrossRef] [PubMed]
- Chakrabarti, A.K.; Deshmukh, A.; Liang, J.J.; Madamanchi, C.; Ghannam, M.; Morady, F.; Bogun, F. Mitral Annular Substrate and Ventricular Arrhythmias in Arrhythmogenic Mitral Valve Prolapse with Mitral Annular Disjunction. JACC Clin. Electrophysiol. 2023, 9 Pt 1, 1265–1275. [Google Scholar] [CrossRef]
- Casella, M.; Bergonti, M.; Dello Russo, A.; Maragna, R.; Gasperetti, A.; Compagnucci, P.; Catto, V.; Trombara, F.; Frappampina, A.; Conte, E.; et al. Endomyocardial Biopsy: The Forgotten Piece in the Arrhythmogenic Cardiomyopathy Puzzle. J. Am. Heart Assoc. 2021, 10, e021370. [Google Scholar] [CrossRef]
- Dello Russo, A.; Compagnucci, P.; Casella, M.; Gasperetti, A.; Riva, S.; Dessanai, M.A.; Pizzamiglio, F.; Catto, V.; Guerra, F.; Stronati, G.; et al. Ventricular arrhythmias in athletes: Role of a comprehensive diagnostic workup. Heart Rhythm. 2022, 19, 90–99. [Google Scholar] [CrossRef]
- Vriz, O.; Landi, I.; Eltayeb, A.; Limongelli, G.; Mos, L.; Delise, P.; Bossone, E.; DAndrea, A. Mitral Valve Prolapse and Sudden Cardiac Death in Athletes at High Risk. Curr. Cardiol. Rev. 2023, 19, e201222212066. [Google Scholar] [CrossRef]
- Capucci, A.; Compagnucci, P. Il metoprololo nel trattamento della fibrillazione atriale: Stato dell’arte [Metoprolol for atrial fibrillation: State of the art]. G Ital. Cardiol. 2022, 23, 419–422. [Google Scholar] [CrossRef]
- Aabel, E.W.; Dejgaard, L.A.; Chivulescu, M.; Helle-Valle, T.M.; Edvardsen, T.; Hasselberg, N.E.; Hegbom, F.; Lie, Ø.H.; Haugaa, K.H. Flecainide in patients with arrhythmic mitral valve syndrome: A case series. Heart Rhythm. 2023, 20, 635–636. [Google Scholar] [CrossRef] [PubMed]
- Bumgarner, J.M.; Patel, D.; Kumar, A.; Clevenger, J.R.; Trulock, K.M.; Popović, Z.; Griffin, B.P.; Wazni, O.M.; Menon, V.; Desai, M.Y.; et al. Management and outcomes in mitral valve prolapse with ventricular arrhythmias undergoing ablation and/or implantation of ICDs. Pacing Clin. Electrophysiol. 2019, 42, 447–452. [Google Scholar] [CrossRef]
- Peichl, P.; Baran, J.; Wichterle, D.; Čihák, R.; Skála, T.; Aldhoon, B.; Jan, M.; Antolič, B.; Kautzner, J. The tip of the muscle is a dominant location of ventricular ectopy originating from papillary muscles in the left ventricle. J. Cardiovasc. Electrophysiol. 2018, 29, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Hamilton-Craig, C.; Denman, R.; Haqqani, H.M. Catheter ablation of papillary muscle arrhythmias: Implications of mitral valve prolapse and systolic dysfunction. Pacing Clin. Electrophysiol. 2018, 41, 750–758. [Google Scholar] [CrossRef]
- Rivera, S.; Tomas, L.; Ricapito, M.P.; Nicolas, V.; Reinoso, M.; Caro, M.; Mondragon, I.; Albina, G.; Giniger, A.; Scazzuso, F. Updated results on catheter ablation of ventricular arrhythmias arising from the papillary muscles of the left ventricle. J. Arrhythm. 2018, 35, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Dello Russo, A.; Compagnucci, P.; Bergonti, M.; Cipolletta, L.; Parisi, Q.; Volpato, G.; Santarelli, G.; Colonnelli, M.; Saenen, J.; Valeri, Y.; et al. Microelectrode voltage mapping for substrate assessment in catheter ablation of ventricular tachycardia: A dual-center experience. J. Cardiovasc. Electrophysiol. 2023, 34, 1216–1227. [Google Scholar] [CrossRef] [PubMed]
- Compagnucci, P.; Valeri, Y.; Conti, S.; Volpato, G.; Cipolletta, L.; Parisi, Q.; D’Angelo, L.; Campanelli, F.; Carboni, L.; Sgarito, G.; et al. Technological advances in ventricular tachycardia catheter ablation: The relentless quest for novel solutions to old problems. J. Interv. Card. Electrophysiol. 2023; Online ahead of print. [Google Scholar] [CrossRef]
- Cronin, E.M.; Bogun, F.M.; Maury, P.; Peichl, P.; Chen, M.; Namboodiri, N.; Aguinaga, L.; Leite, L.R.; Al-Khatib, S.M.; Anter, E.; et al. ESC Scientific Document Group. 2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias. Europace 2019, 21, 1143–1144. [Google Scholar] [CrossRef]
- Gulletta, S.; Gasperetti, A.; Schiavone, M.; Vogler, J.; Fastenrath, F.; Breitenstein, A.; Laredo, M.; Palmisano, P.; Mitacchione, G.; Compagnucci, P.; et al. Age-related differences and associated mid-term outcomes of subcutaneous implantable cardioverter-defibrillators: A propensity-matched analysis from a multicenter European registry. Heart Rhythm. 2022, 19, 1109–1115. [Google Scholar] [CrossRef]
- Vaidya, V.R.; DeSimone, C.V.; Damle, N.; Naksuk, N.; Syed, F.F.; Ackerman, M.J.; Ponamgi, S.P.; Nkomo, V.T.; Suri, R.M.; Noseworthy, P.A.; et al. Reduction in malignant ventricular arrhythmia and appropriate shocks following surgical correction of bileaflet mitral valve prolapse. J. Interv. Card. Electrophysiol. 2016, 46, 137–143. [Google Scholar] [CrossRef]
- Naksuk, N.; Syed, F.F.; Krittanawong, C.; Anderson, M.J.; Ebrille, E.; DeSimone, C.V.; Vaidya, V.R.; Ponamgi, S.P.; Suri, R.M.; Ackerman, M.J.; et al. The effect of mitral valve surgery on ventricular arrhythmia in patients with bileaflet mitral valve prolapse. Indian. Pacing Electrophysiol. J. 2016, 16, 187–191. [Google Scholar] [CrossRef]
- Vohra, J.; Sathe, S.; Warren, R.; Totalis, J.; Hunt, D. Malignant ventricular arrhythmias in patients with mitral valve prolapse and mild mitral regurgitation. Pacing Clin. Electrophysiol 1993, 16, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Ascione, G.; Azzola Guicciardi, N.; Lorusso, R.; Boccellino, A.; Lapenna, E.; Del Forno, B.; Carino, D.; Bisogno, A.; Palmisano, A.; D’Angelo, G.; et al. The impact of mitral valve surgery on ventricular arrhythmias in patients with Barlow’s disease: Preliminary results of a prospective study. Interdiscip. Cardiovasc. Thorac. Surg. 2023, 36, ivad073. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Population | Total No. SCD | Sports-Related SCD | Age | Male Sex | Total No. of MVP | Total No. of MVP in Athletes |
|---|---|---|---|---|---|---|---|---|
| Burke et al. [25] | 1991 | Study of sports and non-sports-related SCD | 690 | 34 (5%) | 14–40 years | 532 (77%) | 11 (1.6%) | 0 (0%) |
| Van Camp et al. [26] | 1995 | Study of sports-related death in athletes | 100 | 100 | 13–22 years | 92 (92%) | 1 (1%) | 1 (1%) |
| Maron et al. [27] | 1996 | Registry of SCD in young athletes | 134 | 134 | <35 years | 120 (89.5%) | 3 (2.24%) | 3 (2.24%) |
| Maron et al. [28] | 2009 | Registry of SCD in young athletes | 1049 | 1049 | 13–25 years | 937 (89.3%) | 25 (2.4%) | 25 (2.4%) |
| Maron et al. [29] | 2014 | Registry of SCD in young athletes | 47 | 47 | 18–22 years | 41 (87%) | 1 (2.1%) | 1 (2.1%) |
| Finocchiaro et al. [23] | 2016 | Registry of SCD in athletes | 357 | 357 | 7–67 years | 330 (92%) | 7 (2%) | 7 (2%) |
| Maron et al. [24] | 2016 | Registry of SCD in young athletes | 842 | 842 | 13–25 years | 747 (89%) | 31 (4%) | 31 (4%) |
| Study | Year | Population | No. of Patients | MVP | Age | Male Sex | VAs in MVP | SCD/Aborted SCD | ICD Shock | Sustained VT |
|---|---|---|---|---|---|---|---|---|---|---|
| Caselli et al. [22] | 2018 | Athletes | 7449 | 215 (2.9%) | 17–43 y | 67% | 62 (29%) | 0 (%) | 0 (0%) | 0 (0%) |
| Five et al. [30] | 2023 | Athletes | 136 | 136 (100%) | 37–64 y | 49% | 17 (12.5%) [severe VAs] | 12 (8.8%) | 1 (0.74%) | 4 (2.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Compagnucci, P.; Selimi, A.; Cipolletta, L.; Volpato, G.; Gasperetti, A.; Valeri, Y.; Parisi, Q.; Curcio, A.; Natale, A.; Dello Russo, A.; et al. Arrhythmic Mitral Valve Prolapse and Sports Activity: Pathophysiology, Risk Stratification, and Sports Eligibility Assessment. J. Clin. Med. 2024, 13, 1350. https://doi.org/10.3390/jcm13051350
Compagnucci P, Selimi A, Cipolletta L, Volpato G, Gasperetti A, Valeri Y, Parisi Q, Curcio A, Natale A, Dello Russo A, et al. Arrhythmic Mitral Valve Prolapse and Sports Activity: Pathophysiology, Risk Stratification, and Sports Eligibility Assessment. Journal of Clinical Medicine. 2024; 13(5):1350. https://doi.org/10.3390/jcm13051350
Chicago/Turabian StyleCompagnucci, Paolo, Adelina Selimi, Laura Cipolletta, Giovanni Volpato, Alessio Gasperetti, Yari Valeri, Quintino Parisi, Antonio Curcio, Andrea Natale, Antonio Dello Russo, and et al. 2024. "Arrhythmic Mitral Valve Prolapse and Sports Activity: Pathophysiology, Risk Stratification, and Sports Eligibility Assessment" Journal of Clinical Medicine 13, no. 5: 1350. https://doi.org/10.3390/jcm13051350
APA StyleCompagnucci, P., Selimi, A., Cipolletta, L., Volpato, G., Gasperetti, A., Valeri, Y., Parisi, Q., Curcio, A., Natale, A., Dello Russo, A., & Casella, M. (2024). Arrhythmic Mitral Valve Prolapse and Sports Activity: Pathophysiology, Risk Stratification, and Sports Eligibility Assessment. Journal of Clinical Medicine, 13(5), 1350. https://doi.org/10.3390/jcm13051350