
Use of Rotational Atherectomy-Assisted Balloon Angioplasty in the Treatment of Isolated Below-the-Knee Atherosclerotic Lesions in Patients with Chronic Limb-Threatening Ischemia
 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Selection Criteria
2.2. Endpoints
2.3. Definitions
2.4. Procedure
2.5. Follow-Up
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Bevan, G.H.; White Solaru, K.T. Evidence-Based Medical Management of Peripheral Artery Disease. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 541–553. [Google Scholar] [CrossRef] [PubMed]
- Firnhaber, J.M.; Powell, C.S. Lower Extremity Peripheral Artery Disease: Diagnosis and Treatment. Am. Fam. Physician 2019, 99, 362–369, Erratum in Am. Fam. Physician 2019, 100, 74. [Google Scholar] [PubMed]
- Gallino, A.; Aboyans, V.; Diehm, C.; Cosentino, F.; Stricker, H.; Falk, E.; Schouten, O.; Lekakis, J.; Amann-Vesti, B.; Siclari, F.; et al. European Society of Cardiology Working Group on Peripheral Circulation. Non-coronary atherosclerosis. Eur. Heart J. 2014, 35, 1112–1119. [Google Scholar] [CrossRef] [PubMed]
- Bradbury, A.W.; Adam, D.J.; Bell, J.; Forbes, J.F.; Fowkes, F.G.; Gillespie, I.; Ruckley, C.V.; Raab, G.M. BASIL trial Participants. Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial: An intention-to-treat analysis of amputation-free and overall survival in patients randomized to a bypass surgery-first or a balloon angioplasty-first revascularization strategy. J. Vasc. Surg. 2010, 51 (Suppl. S5), 5S–17S, Erratum in J. Vasc. Surg. 2010, 52, 1751. [Google Scholar] [CrossRef] [PubMed]
- Dormandy, J.A.; Rutherford, R.B. Management of peripheral arterial disease (PAD). TASC Working Group. TransAtlantic Inter-Society Consensus (TASC). J. Vasc. Surg. 2000, 31 (Suppl. S1), S1–S296. [Google Scholar] [PubMed]
- Sena, G.; Gallelli, G. An increased severity of peripheral arterial disease in the COVID-19 era. J. Vasc. Surg. 2020, 72, 758. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.L.; Björck, M.; Brodmann, M.; Cohner, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. Editor’s Choice—2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2018, 55, 305–368. [Google Scholar] [CrossRef] [PubMed]
- Giusca, S.; Hagstotz, S.; Lichtenberg, M.; Heinrich, U.; Eisenbach, C.; Andrassy, M.; Korosoglou, G. Phoenix atherectomy for patients with peripheral artery disease. EuroIntervention 2022, 18, e432–e442. [Google Scholar] [CrossRef]
- Kronlage, M.; Erbel, C.; Lichtenberg, M.; Donas, K.; Frey, N.; Korosoglou, G. Safety, Effectiveness, and Midterm Results of Endovascular Treatment for the Common Femoral Artery: A Two Centre Atherectomy Trial. Eur. J. Vasc. Endovasc. Surg. 2023, 66, 280–281. [Google Scholar] [CrossRef]
- Taneva, G.T.; Pitoulias, A.G.; Avranas, K.; Kazemtash, M.; Bakr, N.A.; Dahi, F.; Donas, K.P. Midterm outcomes of rotational atherectomy-assisted endovascular treatment of severe peripheral arterial disease. J. Vasc. Surg. 2023; Epub ahead of print. [Google Scholar] [CrossRef]
- Kumarasamy, A.; Gombert, A.; Krabbe, J.; Ruprecht, O.; Jacobs, M.J.; Krabbe, H. Assessment of Feasibility and Patency of below the Knee Atherectomy Using the 1.5 mm Phoenix Catheter-A Retrospective Study. Medicina (Kaunas). Medicina 2022, 58, 1594. [Google Scholar] [CrossRef] [PubMed]
- Razavi, M.K.; Mustapha, J.A.; Miller, L.E. Contemporary systematic review and meta-analysis of early outcomes with percutaneous treatment for infrapopliteal atherosclerotic disease. J. Vasc. Interv. Radiol. 2014, 25, 1489–1496.e3. [Google Scholar] [CrossRef] [PubMed]
- Kuntz, R.E.; Safian, R.D.; Carrozza, J.P.; Fishman, R.F.; Mansour, M.; Baim, D.S. The importance of acute luminal diameter in determining restenosis after coronary atherectomy or stenting. Circulation 1992, 86, 1827–1835. [Google Scholar] [CrossRef] [PubMed]
- Korosoglou, G.; Lichtenberg, M.; Celik, S.; Andrassy, J.; Brodmann, M.; Andrassy, M. The evolving role of drug-coated balloons for the treatment of complex femoro- popliteal lesions. J. Cardiovasc. Surg. 2018, 59, 51–59. [Google Scholar]
- Hirsch, A.T.; Criqui, M.H.; Treat-Jacobson, D.; Regensteiner, J.G.; Creager, M.A.; Olin, J.W.; Krook, S.H.; Hunninghake, D.B.; Comerota, A.J.; Walsh, M.E.; et al. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA 2001, 286, 1317–1324. [Google Scholar] [CrossRef] [PubMed]
- Abu Dabrh, A.M.; Steffen, M.W.; Undavalli, C.; Asi, N.; Wang, Z.; Elamin, M.B.; Conte, M.S.; Murad, M.H. The natural history of untreated severe or critical limb ischemia. J. Vasc. Surg. 2015, 62, 1642–1651. [Google Scholar] [CrossRef] [PubMed]
- Barbarawi, M.; Qazi, A.H.; Lee, J.; Barbarawi, O.; Al-Abdouh, A.; Mhanna, M.; Vashist, A. Meta-Analysis Comparing Drug-Coated Balloons and Percutaneous Transluminal Angioplasty for Infrapopliteal Artery Disease. Am. J. Cardiol. 2022, 183, 115–121. [Google Scholar] [CrossRef]
- Ipema, J.; Huizing, E.; Schreve, M.A.; de Vries, J.P.M.; Ünlü, Ç. Editor’s Choice—Drug Coated Balloon Angioplasty vs. Standard Percutaneous Transluminal Angioplasty in Below the Knee Peripheral Arterial Disease: A Systematic Review and Meta-Analysis. Eur. J. Vasc. Endovasc. Surg. 2020, 59, 265–275. [Google Scholar] [CrossRef]
- Korosoglou, G.; Giusca, S.; Andrassy, M.; Lichtenberg, M. The Role of Atherectomy in Peripheral Artery Disease: Current Evidence and Future Perspectives. Vasc. Endovasc. Rev. 2018, 2, 12–18. Available online: https://www.verjournal.com/articles/atherectomy-peripheral-artery-disease (accessed on 6 April 2019). [CrossRef]
- Donas, K.P.; Taneva, G.T.; Pitoulias, G.A.; Jomha, A.; Schröder, M.; Psyllas, A.; Scali, S.; Abu Bakr, N. MORPHEAS Registry. Technical performance and reproducibility following rotational atherectomy of femoropopliteal artery occlusive lesions: Analysis of the multicenter MORPHEAS Registry. J. Cardiovasc. Surg. 2022, 63, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Kronlage, M.; Erbel, C.; Lichtenberg, M.; Heinrich, U.; Katus, H.A.; Frey, N.; Giusca, S.; Korosoglou, G. Safety and effectiveness of Phoenix atherectomy for endovascular treatment in calcified common femoral artery lesions. Vasa 2021, 50, 378–386. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Huang, Q.; Pu, H.; Qin, J.; Wang, X.; Ye, K.; Lu, X. Atherectomy Combined with Balloon Angioplasty versus Balloon Angioplasty Alone for de Novo Femoropopliteal Arterial Diseases: A Systematic Review and Meta-analysis of Randomised Controlled Trials. Eur. J. Vasc. Endovasc. Surg. 2021, 62, 65–73. [Google Scholar] [CrossRef]
- Pitoulias, A.G.; Pitoulias, G.A. The role of atherectomy in BTK lesions: A systematic review. J. Cardiovasc. Surg. 2022, 63, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Hupalo, Y.M.; Denysov, S.Y.; Kutsyn, A.M.; Lebedieva, Y.O.; Grusha, M.M. Percutaneous transluminal rotary atherectomy in patients with atherosclerotic lesions of below the knee arteries. Wiadomości Lek. 2022, 75, 2589–2593. [Google Scholar] [CrossRef] [PubMed]
- Rodoplu, O.; Er, Z.; Erdinc, I.; Ozturk, C. Atherectomy followed by drug-coated balloon angioplasty for below knee lesions in diabetic patients. Cirugía Cir. 2022, 90, 29–35. [Google Scholar] [CrossRef] [PubMed]
- VERN COVER study collaborative; Benson, R.A. Documenting the Recovery of Vascular Services in European Centres Following the Initial COVID-19 Pandemic Peak: Results from a Multicentre Collaborative Study. EJVES Vasc. Forum 2022, 57, 28–34. [Google Scholar] [CrossRef]

{kind=link}
| Total n = 96 | Group A n = 50 | Group B n= 46 | p-Value | |
|---|---|---|---|---|
| Age 1 | 83–15 | 84–15 | 82–16.5 | 0.060 |
| Age > 80 2 | 54 (56%) | 32 (64%) | 22 (48%) | 0.111 |
| Male 2 | 59 (61%) | 29 (58%) | 30 (65%) | 0.468 |
| Smoking history 2 | 45 (47%) | 20 (40%) | 25(54%) | 0.159 |
| Hypertension 2 | 89 (93%) | 44 (88%) | 45 (98%) | 0.064 |
| Hyperlipidemia 2 | 58 (60%) | 26 (52%) | 32 (69%) | 0.079 |
| Diabetis 2 | 57 (59%) | 29 (58%) | 28 (61%) | 0.775 |
| CAD 2 | 49 (51%) | 22 (44%) | 27 (59%) | 0.147 |
| GFR < 30 mL/min 2 | 24 (25%) | 15 (30%) | 9 (9%) | 0.238 |
| Aspirin 2 | 56 (58%) | 27 (54%) | 29 (63%) | 0.369 |
| Clopidogrel 2 | 8 (8%) | 1 (2%) | 7 (15%) | 0.019 |
| OAC 2 | 7 (7%) | 5 (10%) | 2 (4%) | 0.287 |
| DOAC 2 | 30 (31%) | 16 (32%) | 14 (30%) | 0.869 |
| Stenosis 2 | 46 (48%) | 26 (52%) | 20 (44%) | 0.404 |
| Occlusion 2 | 50 (52%) | 24 (48%) | 26 (56%) | 0.404 |
| Preoperative ABI 1 | 0.4–0.1 | 0.3–0.2 | 0.4–0.2 | 0.002 |
| Rutherford Class 5–6 2 | 88 (92%) | 45 (90%) | 43 (93%) | 0.538 |
| Total n = 96 | Group A n = 50 | Group B n= 46 | p-Value | |
|---|---|---|---|---|
| Endovascular specialist 1 | 60 (62%) | 35 (70%) | 25 (54%) | 0.114 |
| Op duration (minutes) 2 | 59–30 | 64–30 | 58–23 | 0.878 |
| Antegrade punction 2 | 83 (86%) | 43 (86%) | 40 (86%) | 0.891 |
| Technical success 1 | 88 (91.7%) | 44 (88%) | 44 (95.7%) | 0.175 |
| Assisted technical success 1 | 96 (100.0%) | 50 (100.0%) | 46 (100.0%) | n/a 3 |
| Bailout stenting 1 | 8 (8%) | 6 (12%) | 2 (4%) | 0.175 |
| Peripheral embolization 1 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | n/a 3 |
| Access site complications 1 | 1 (1%) | 0 (0%) | 1 (2%) | 0.295 |
| Hospital stay (days) 2 | 2.5–5 | 4–6 | 2–3 | <0.001 |
| Postoperative ABI 2 | 0.8–0.2 | 0.7–0.1 | 0.8–0.2 | 0.008 |
| Postoperative ABI >0.8 1 | 38 (48%) | 16 (35%) | 22 (67%) | 0.005 |
| 30 days MACE 1 | 1 (1%) | 1 (2%) | 0 (0) | 0.335 |
| Mortality 1 | 2 (2%) | 2 (4%) | 0 (0%) | 0.170 |
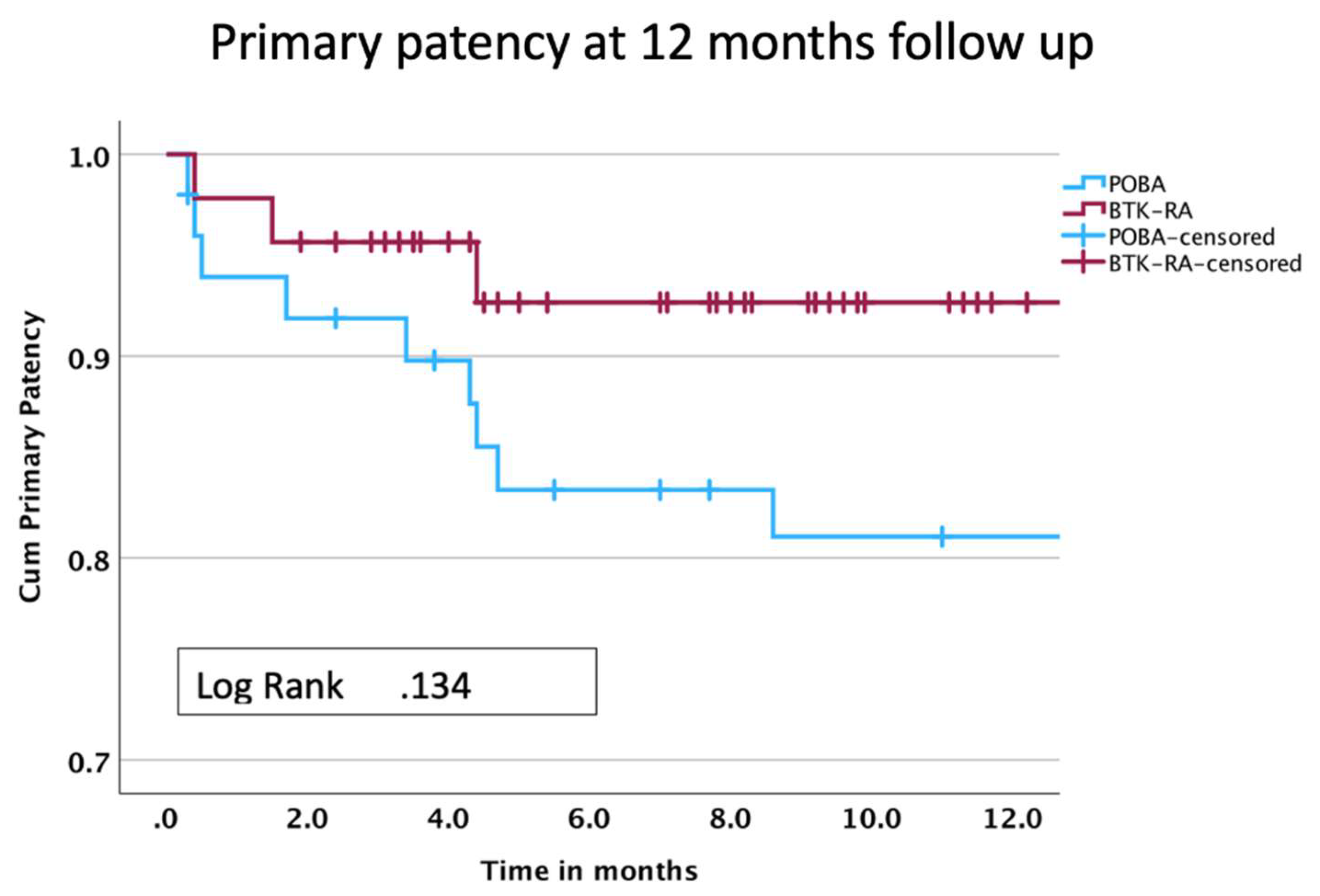
| Primary patency 1 | 79 (82%) | 36 (72%) | 43 (93%) | 0.006 |
| Reintervention (TLR) 1,3 | 13 (76%) 3 | 12 (85%) 3 | 1 (33%) 3 | 0.052 |
| Minor Amputation 1 | 23 (24%) | 20 (40%) | 3 (6%) | <0.001 |
| Limb salvage 1 | 92 (96%) | 47 (94%) | 45 (98%) | 0.349 |
| 0 | 2 | 4 | 6 | 8 | 10 | 12 | |
|---|---|---|---|---|---|---|---|
| Total | |||||||
| Cum Survival (%) | 99 | 98 | 98 | 98 | 97 | 69 | |
| At risk | 96 | 94 | 93 | 90 | 88 | 87 | 50 |
| Std error | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.02 | 0.06 |
| Group A | |||||||
| Cum Survival (%) | 90 | 83 | 83 | 81 | 81 | 60 | |
| At risk | 50 | 44 | 42 | 37 | 36 | 35 | 20 |
| Std error | 0.04 | 0.04 | 0.05 | 0.05 | 0.06 | 0.06 | 0.09 |
| Group B | |||||||
| Cum Survival (%) | 96 | 92 | 92 | 92 | 92 | 92 | |
| At risk | 46 | 39 | 30 | 22 | 14 | 7 | 3 |
| Std error | 0.03 | 0.03 | 0.04 | 0.04 | 0.04 | 0.04 | 0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pitoulias, A.G.; Taneva, G.T.; Avranas, K.; Abu Bakr, N.; Pitoulias, G.A.; Donas, K.P. Use of Rotational Atherectomy-Assisted Balloon Angioplasty in the Treatment of Isolated Below-the-Knee Atherosclerotic Lesions in Patients with Chronic Limb-Threatening Ischemia. J. Clin. Med. 2024, 13, 1346. https://doi.org/10.3390/jcm13051346
Pitoulias AG, Taneva GT, Avranas K, Abu Bakr N, Pitoulias GA, Donas KP. Use of Rotational Atherectomy-Assisted Balloon Angioplasty in the Treatment of Isolated Below-the-Knee Atherosclerotic Lesions in Patients with Chronic Limb-Threatening Ischemia. Journal of Clinical Medicine. 2024; 13(5):1346. https://doi.org/10.3390/jcm13051346
Chicago/Turabian StylePitoulias, Apostolos G., Gergana T. Taneva, Konstantinos Avranas, Nizar Abu Bakr, Georgios A. Pitoulias, and Konstantinos P. Donas. 2024. "Use of Rotational Atherectomy-Assisted Balloon Angioplasty in the Treatment of Isolated Below-the-Knee Atherosclerotic Lesions in Patients with Chronic Limb-Threatening Ischemia" Journal of Clinical Medicine 13, no. 5: 1346. https://doi.org/10.3390/jcm13051346
APA StylePitoulias, A. G., Taneva, G. T., Avranas, K., Abu Bakr, N., Pitoulias, G. A., & Donas, K. P. (2024). Use of Rotational Atherectomy-Assisted Balloon Angioplasty in the Treatment of Isolated Below-the-Knee Atherosclerotic Lesions in Patients with Chronic Limb-Threatening Ischemia. Journal of Clinical Medicine, 13(5), 1346. https://doi.org/10.3390/jcm13051346