
The Role of Transjugular Intrahepatic Portosystemic Shunt for the Management of Ascites in Patients with Decompensated Cirrhosis

 , ,
, ,
Abstract
1. Introduction
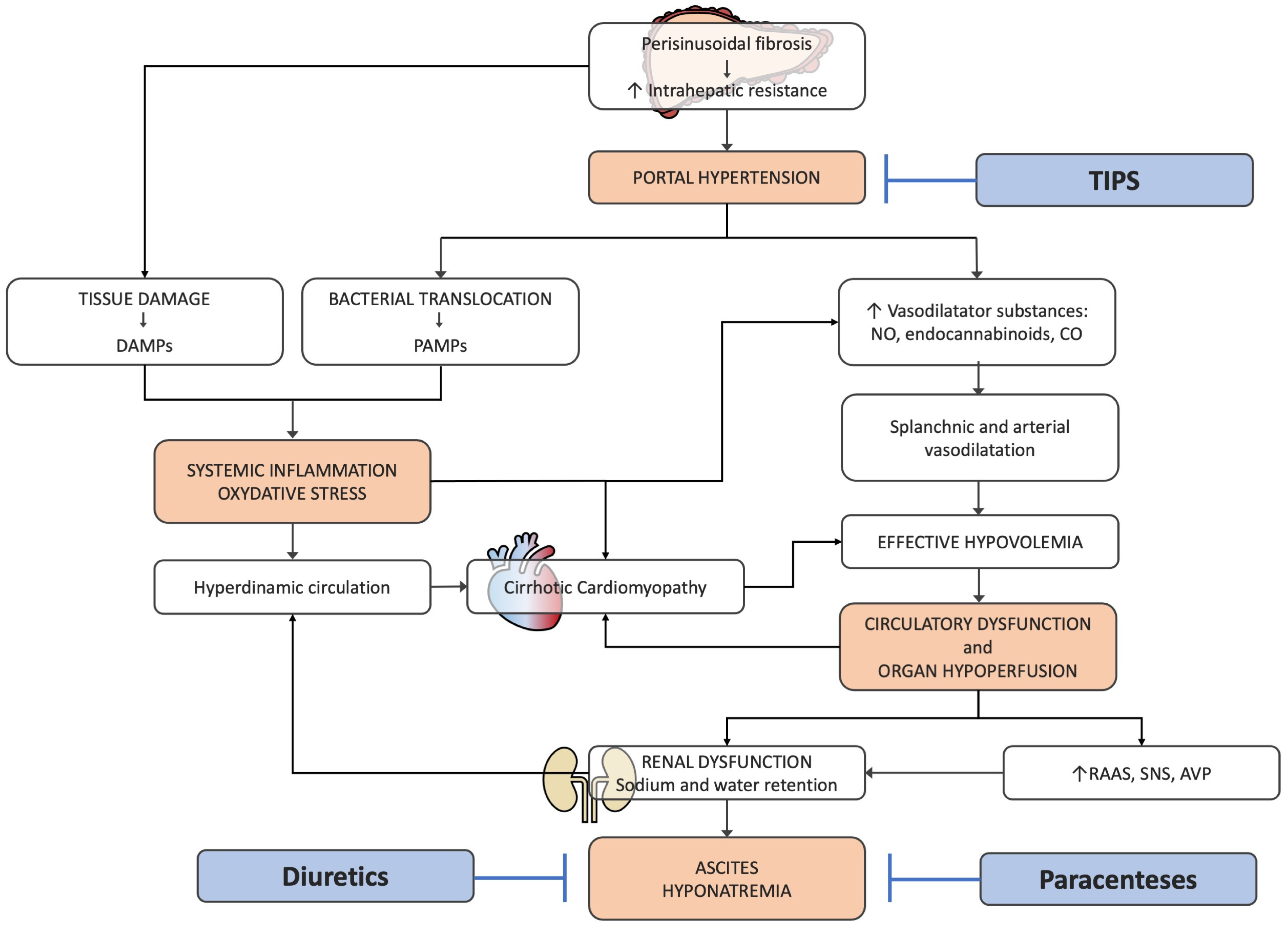
2. Pathophysiology of Ascites in Patients with Cirrhosis
3. Current Standard of Care for Patients with Ascites
4. Technical Aspects and Characteristics of Stent
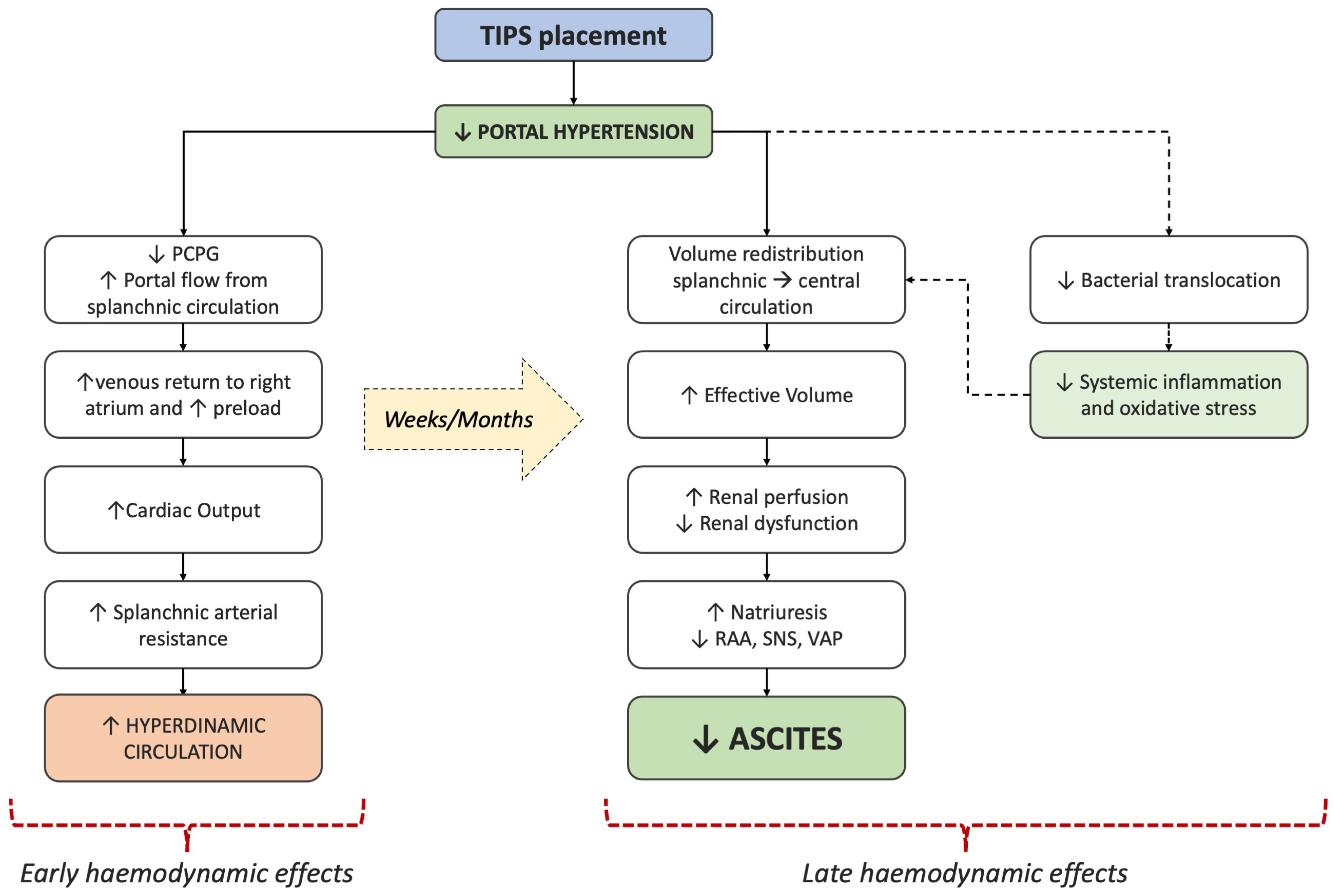
5. Hemodynamic Consequences of TIPS Placement
6. Evidence Supporting the Use of TIPS for Ascites Management

{kind=link}
{kind=link}
| Author, Year | Setting | Treatment | Main Findings in TIPS Group |
|---|---|---|---|
| Lebrec (1996) [34] | Refractory ascites | Uncovered TIPS vs. LVP |
|
| Rössle (2000) [35] | Refractory or recurrent ascites | Uncovered TIPS vs. LVP+HA |
|
| Ginès (2002) [36] | Refractory ascites | Uncovered TIPS vs. LVP+HA |
|
| Sanyal (2003) [37] | Refractory ascites | Uncovered TIPS + SMT (sodium restriction, diuretics, LVP+HA) vs. SMT alone |
|
| Salerno (2004) [38] | Refractory or recidivant ascites | Uncovered TIPS vs. LVP+HA |
|
| Narahara (2011) [39] | Refractory ascites with good renal and liver function | Uncovered TIPS vs. LVP+HA |
|
| Bureau (2017) [40] | Recurrent ascites (≥2 LVPs in at least 3 weeks) | Covered TIPS vs. LVP+HA |
|
7. Patient Selection and Contraindications to TIPS
- -
- Severe congestive or valvular heart disease;
- -
- Moderate–severe pulmonary hypertension (assessed with invasive methods) despite an optimized medical treatment;
- -
- Ongoing uncontrolled systemic infection and sepsis;
- -
- Refractory overt HE;
- -
- Unrelieved biliary obstruction;
- -
- Parenchymal liver lesions (e.g., multiple cysts or tumors) that preclude TIPS insertion.
- Age: <65 years.
- Liver function: Child–Pugh score ≤ 13; MELD score ≤ 19; no recurrent or persistent HE without precipitants; total bilirubin level < 3 mg/dL; platelet count > 75,000 × 109/L.
- Cardiac function: no systolic or diastolic dysfunction; no aortic stenosis; normal value of BNP or pro-BNP.
8. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Angeli, P.; Bernardi, M.; Villanueva, C.; Francoz, C.; Mookerjee, R.P.; Trebicka, J.; Krag, A.; Laleman, W.; Gines, P. EASL Clinical Practice Guidelines for the Management of Patients with Decompensated Cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef]
- D’Amico, G.; Garcia-Tsao, G.; Pagliaro, L. Natural History and Prognostic Indicators of Survival in Cirrhosis: A Systematic Review of 118 Studies. J. Hepatol. 2006, 44, 217–231. [Google Scholar] [CrossRef]
- Zipprich, A.; Garcia-Tsao, G.; Rogowski, S.; Fleig, W.E.; Seufferlein, T.; Dollinger, M.M. Prognostic Indicators of Survival in Patients with Compensated and Decompensated Cirrhosis. Liver Int. 2012, 32, 1407–1414. [Google Scholar] [CrossRef]
- Biggins, S.W.; Angeli, P.; Garcia-Tsao, G.; Ginès, P.; Ling, S.C.; Nadim, M.K.; Wong, F.; Kim, W.R. Diagnosis, Evaluation, and Management of Ascites, Spontaneous Bacterial Peritonitis and Hepatorenal Syndrome: 2021 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2021, 74, 1014–1048. [Google Scholar] [CrossRef]
- Caraceni, P.; Riggio, O.; Angeli, P.; Alessandria, C.; Neri, S.; Foschi, F.G.; Levantesi, F.; Airoldi, A.; Boccia, S.; Svegliati-Baroni, G.; et al. Long-Term Albumin Administration in Decompensated Cirrhosis (ANSWER): An Open-Label Randomised Trial. Lancet 2018, 391, 2417–2429. [Google Scholar] [CrossRef]
- Di Pascoli, M.; Fasolato, S.; Piano, S.; Bolognesi, M.; Angeli, P. Long-Term Administration of Human Albumin Improves Survival in Patients with Cirrhosis and Refractory Ascites. Liver Int. 2019, 39, 98–105. [Google Scholar] [CrossRef]
- Schrier, R.W.; Arroyo, V.; Bernardi, M.; Epstein, M.; Henriksen, J.H.; Rodés, J. Peripheral Arterial Vasodilation Hypothesis: A Proposal for the Initiation of Renal Sodium and Water Retention in Cirrhosis. Hepatology 1988, 8, 1151–1157. [Google Scholar] [CrossRef]
- Bernardi, M.; Moreau, R.; Angeli, P.; Schnabl, B.; Arroyo, V. Mechanisms of Decompensation and Organ Failure in Cirrhosis: From Peripheral Arterial Vasodilation to Systemic Inflammation Hypothesis. J. Hepatol. 2015, 63, 1272–1284. [Google Scholar] [CrossRef]
- Engelmann, C.; Clària, J.; Szabo, G.; Bosch, J.; Bernardi, M. Pathophysiology of Decompensated Cirrhosis: Portal Hypertension, Circulatory Dysfunction, Inflammation, Metabolism and Mitochondrial Dysfunction. J. Hepatol. 2021, 75, S49–S66. [Google Scholar] [CrossRef]
- Henriksen, J.H.; Stage, J.G.; Schlichting, P.; Winkler, K. Intraperitoneal Pressure: Ascitic Fluid and Splanchnic Vascular Pressures, and Their Role in Prevention and Formation of Ascites. Scand. J. Clin. Lab. Investig. 1980, 40, 493–501. [Google Scholar] [CrossRef]
- Tonon, M.; Piano, S.; Gambino, C.G.; Romano, A.; Pilutti, C.; Incicco, S.; Brocca, A.; Sticca, A.; Bolognesi, M.; Angeli, P. Outcomes and Mortality of Grade 1 Ascites and Recurrent Ascites in Patients With Cirrhosis. Clin. Gastroenterol. Hepatol. 2021, 19, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Morando, F.; Rosi, S.; Gola, E.; Nardi, M.; Piano, S.; Fasolato, S.; Stanco, M.; Cavallin, M.; Romano, A.; Sticca, A.; et al. Adherence to a Moderate Sodium Restriction Diet in Outpatients with Cirrhosis and Ascites: A Real-life Cross-sectional Study. Liver Int. 2015, 35, 1508–1515. [Google Scholar] [CrossRef]
- Angeli, P.; Fasolato, S.; Mazza, E.; Okolicsanyi, L.; Maresio, G.; Velo, E.; Galioto, A.; Salinas, F.; D’Aquino, M.; Sticca, A.; et al. Combined versus Sequential Diuretic Treatment of Ascites in Non-Azotaemic Patients with Cirrhosis: Results of an Open Randomised Clinical Trial. Gut 2010, 59, 98–104. [Google Scholar] [CrossRef]
- Moore, K.P.; Wong, F.; Gines, P.; Bernardi, M.; Ochs, A.; Salerno, F.; Angeli, P.; Porayko, M.; Moreau, R.; Garcia-Tsao, G.; et al. The Management of Ascites in Cirrhosis: Report on the Consensus Conference of the International Ascites Club. Hepatology 2003, 38, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Solà, E.; Solé, C.; Simón-Talero, M.; Martín-Llahí, M.; Castellote, J.; Garcia-Martínez, R.; Moreira, R.; Torrens, M.; Márquez, F.; Fabrellas, N.; et al. Midodrine and Albumin for Prevention of Complications in Patients with Cirrhosis Awaiting Liver Transplantation. A Randomized Placebo-Controlled Trial. J. Hepatol. 2018, 69, 1250–1259. [Google Scholar] [CrossRef]
- Pompili, E.; Zaccherini, G.; Baldassarre, M.; Iannone, G.; Caraceni, P. Albumin Administration in Internal Medicine: A Journey between Effectiveness and Futility. Eur. J. Intern. Med. 2023, 117, 28–37. [Google Scholar] [CrossRef]
- Caraceni, P.; Angeli, P.; Prati, D.; Bernardi, M.; Berti, P.; Bennardello, F.; Fiorin, F.; Piccoli, P. AISF-SIMTI Position Paper on the Appropriate Use of Albumin in Patients with Liver Cirrhosis: A 2020 Update. Blood Transfus. 2021, 19, 9–13. [Google Scholar] [CrossRef] [PubMed]
- de Franchis, R.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C.; Abraldes, J.G.; Albillos, A.; Baiges, A.; Bajaj, J.; Bañares, R.; et al. Baveno VII—Renewing Consensus in Portal Hypertension. J. Hepatol. 2022, 76, 959–974. [Google Scholar] [CrossRef]
- Casado, M.; Bosch, J.; García-Pagán, J.C.; Bru, C.; Bañares, R.; Bandi, J.C.; Escorsell, A.; Rodríguez-Láiz, J.M.; Gilabert, R.; Feu, F.; et al. Clinical Events after Transjugular Intrahepatic Portosystemic Shunt: Correlation with Hemodynamic Findings. Gastroenterology 1998, 114, 1296–1303. [Google Scholar] [CrossRef]
- Parvinian, A.; Bui, J.T.; Knuttinen, M.G.; Minocha, J.; Gaba, R.C. Transjugular Intrahepatic Portosystemic Shunt for the Treatment of Medically Refractory Ascites. Diagn. Interv. Radiol. 2013, 20, 58–64. [Google Scholar] [CrossRef]
- Boike, J.R.; Thornburg, B.G.; Asrani, S.K.; Fallon, M.B.; Fortune, B.E.; Izzy, M.J.; Verna, E.C.; Abraldes, J.G.; Allegretti, A.S.; Bajaj, J.S.; et al. North American Practice-Based Recommendations for Transjugular Intrahepatic Portosystemic Shunts in Portal Hypertension. Clin. Gastroenterol. Hepatol. 2022, 20, 1636–1662. [Google Scholar] [CrossRef]
- Perarnau, J.M.; Le Gouge, A.; Nicolas, C.; d’Alteroche, L.; Borentain, P.; Saliba, F.; Minello, A.; Anty, R.; Chagneau-Derrode, C.; Bernard, P.H.; et al. Covered vs. Uncovered Stents for Transjugular Intrahepatic Portosystemic Shunt: A Randomized Controlled Trial. J. Hepatol. 2014, 60, 962–968. [Google Scholar] [CrossRef]
- Wang, Q.; Lv, Y.; Bai, M.; Wang, Z.; Liu, H.; He, C.; Niu, J.; Guo, W.; Luo, B.; Yin, Z.; et al. Eight Millimetre Covered TIPS Does Not Compromise Shunt Function but Reduces Hepatic Encephalopathy in Preventing Variceal Rebleeding. J. Hepatol. 2017, 67, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Bureau, C.; Pagan, J.C.G.; Layrargues, G.P.; Metivier, S.; Bellot, P.; Perreault, P.; Otal, P.; Abraldes, J.-G.; Peron, J.M.; Rousseau, H.; et al. Patency of Stents Covered with Polytetrafluoroethylene in Patients Treated by Transjugular Intrahepatic Portosystemic Shunts: Long-Term Results of a Randomized Multicentre Study. Liver Int. 2007, 27, 742–747. [Google Scholar] [CrossRef] [PubMed]
- Bucsics, T.; Hoffman, S.; Grünberger, J.; Schoder, M.; Matzek, W.; Stadlmann, A.; Mandorfer, M.; Schwabl, P.; Ferlitsch, A.; Peck-Radosavljevic, M.; et al. ePTFE-TIPS vs Repetitive LVP plus Albumin for the Treatment of Refractory Ascites in Patients with Cirrhosis. Liver Int. 2018, 38, 1036–1044. [Google Scholar] [CrossRef] [PubMed]
- Trebicka, J.; Bastgen, D.; Byrtus, J.; Praktiknjo, M.; Terstiegen, S.; Meyer, C.; Thomas, D.; Fimmers, R.; Treitl, M.; Euringer, W.; et al. Smaller-Diameter Covered Transjugular Intrahepatic Portosystemic Shunt Stents Are Associated With Increased Survival. Clin. Gastroenterol. Hepatol. 2019, 17, 2793–2799. [Google Scholar] [CrossRef] [PubMed]
- Praktiknjo, M.; Abu-Omar, J.; Chang, J.; Thomas, D.; Jansen, C.; Kupczyk, P.; Schepis, F.; Garcia-Pagan, J.C.; Merli, M.; Meyer, C.; et al. Controlled Underdilation Using Novel VIATORR® Controlled Expansion Stents Improves Survival after Transjugular Intrahepatic Portosystemic Shunt Implantation. JHEP Rep. 2021, 3, 100264. [Google Scholar] [CrossRef] [PubMed]
- Mansour, S.; Lemmers, A.; Trépo, E.; Moreno, C.; Deltenre, P. The Clinical Advantage of Fixed 8-Mm Diameter VCX Stents over Underdilated VTS Stents Is Not Established in Refractory Ascites. JHEP Rep. 2021, 3, 100319. [Google Scholar] [CrossRef] [PubMed]
- Filì, D.; Falletta, C.; Luca, A.; Hernandez Baravoglia, C.; Clemenza, F.; Miraglia, R.; Scardulla, C.; Tuzzolino, F.; Vizzini, G.; Gridelli, B.; et al. Circulatory Response to Volume Expansion and Transjugular Intrahepatic Portosystemic Shunt in Refractory Ascites: Relationship with Diastolic Dysfunction. Dig. Liver Dis. 2015, 47, 1052–1058. [Google Scholar] [CrossRef]
- Wong, F.; Sniderman, K.; Liu, P.; Blendis, L. The Mechanism of the Initial Natriuresis after Transjugular Intrahepatic Portosystemic Shunt. Gastroenterology 1997, 112, 899–907. [Google Scholar] [CrossRef]
- Wong, W.; Liu, P.; Blendis, L.; Wong, F. Long-Term Renal Sodium Handling in Patients with Cirrhosis Treated with Transjugular Intrahepatic Portosystemic Shunts for Refractory Ascites. Am. J. Med. 1999, 106, 315–322. [Google Scholar] [CrossRef]
- Rössle, M. TIPS: 25 years Later. J. Hepatol. 2013, 59, 1081–1093. [Google Scholar] [CrossRef] [PubMed]
- Jansen, C.; Möller, P.; Meyer, C.; Kolbe, C.C.; Bogs, C.; Pohlmann, A.; Schierwagen, R.; Praktiknjo, M.; Abdullah, Z.; Lehmann, J.; et al. Increase in Liver Stiffness after Transjugular Intrahepatic Portosystemic Shunt Is Associated with Inflammation and Predicts Mortality. Hepatology 2018, 67, 1472–1484. [Google Scholar] [CrossRef] [PubMed]
- Lebrec, D.; Giuily, N.; Hadengue, A.; Vilgrain, V.; Moreau, R.; Poynard, T.; Gadano, A.; Lassen, C.; Benhamou, J.P.; Erlinger, S. Transjugular Intrahepatic Portosystemic Shunts: Comparison with Paracentesis in Patients with Cirrhosis and Refractory Ascites: A Randomized Trial. French Group of Clinicians and a Group of Biologists. J. Hepatol. 1996, 25, 135–144. [Google Scholar] [CrossRef]
- Rössle, M.; Ochs, A.; Gülberg, V.; Siegerstetter, V.; Holl, J.; Deibert, P.; Olschewski, M.; Reiser, M.; Gerbes, A.L. A Comparison of Paracentesis and Transjugular Intrahepatic Portosystemic Shunting in Patients with Ascites. N. Engl. J. Med. 2000, 342, 1701–1707. [Google Scholar] [CrossRef] [PubMed]
- Ginès, P.; Uriz, J.; Calahorra, B.; Garcia-Tsao, G.; Kamath, P.S.; Del Arbol, L.R.; Planas, R.; Bosch, J.; Arroyo, V.; Rodés, J. Transjugular Intrahepatic Portosystemic Shunting versus Paracentesis plus Albumin for Refractory Ascites in Cirrhosis. Gastroenterology 2002, 123, 1839–1847. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, A.J.; Genning, C.; Rajender Reddy, K.; Wong, F.; Kowdley, K.V.; Benner, K.; McCashland, T.; Tisnado, J.; Sargeant, C.; Luketic, V.A.; et al. The North American Study for the Treatment of Refractory Ascites. Gastroenterology 2003, 124, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Salerno, F.; Merli, M.; Riggio, O.; Cazzaniga, M.; Valeriano, V.; Pozzi, M.; Nicolini, A.; Salvatori, F. Randomized Controlled Study of TIPS versus Paracentesis plus Albumin in Cirrhosis with Severe Ascites. Hepatology 2004, 40, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Narahara, Y.; Kanazawa, H.; Fukuda, T.; Matsushita, Y.; Harimoto, H.; Kidokoro, H.; Katakura, T.; Atsukawa, M.; Taki, Y.; Kimura, Y.; et al. Transjugular Intrahepatic Portosystemic Shunt versus Paracentesis plus Albumin in Patients with Refractory Ascites Who Have Good Hepatic and Renal Function: A Prospective Randomized Trial. J. Gastroenterol. 2011, 46, 78–85. [Google Scholar] [CrossRef]
- Bureau, C.; Thabut, D.; Oberti, F.; Dharancy, S.; Carbonell, N.; Bouvier, A.; Mathurin, P.; Otal, P.; Cabarrou, P.; Péron, J.M.; et al. Transjugular Intrahepatic Portosystemic Shunts with Covered Stents Increase Transplant-Free Survival of Patients with Cirrhosis and Recurrent Ascites. Gastroenterology 2017, 152, 157–163. [Google Scholar] [CrossRef]
- Salerno, F.; Cammà, C.; Enea, M.; Rössle, M.; Wong, F. Transjugular Intrahepatic Portosystemic Shunt for Refractory Ascites: A Meta-Analysis of Individual Patient Data. Gastroenterology 2007, 133, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Bai, M. TIPS Improves Liver Transplantation-Free Survival in Cirrhotic Patients with Refractory Ascites: An Updated Meta-Analysis. World J. Gastroenterol. 2014, 20, 2704. [Google Scholar] [CrossRef] [PubMed]
- Albillos, A.; Bañares, R.; González, M.; Catalina, M.-V.; Molinero, L.-M. A Meta-Analysis of Transjugular Intrahepatic Portosystemic Shunt versus Paracentesis for Refractory Ascites. J. Hepatol. 2005, 43, 990–996. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, G.; Luca, A.; Morabito, A.; Miraglia, R.; D’amico, M. Uncovered Transjugular Intrahepatic Portosystemic Shunt for Refractory Ascites: A Meta-Analysis. Gastroenterology 2005, 129, 1282–1293. [Google Scholar] [CrossRef] [PubMed]
- Deltenre, P.; Mathurin, P.; Dharancy, S.; Moreau, R.; Bulois, P.; Henrion, J.; Pruvot, F.R.; Ernst, O.; Paris, J.C.; Lebrec, D. Transjugular Intrahepatic Portosystemic Shunt in Refractory Ascites: A Meta-Analysis. Liver Int. 2005, 25, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Saab, S.; Nieto, J.M.; Lewis, S.K.; Runyon, B.A. TIPS versus Paracentesis for Cirrhotic Patients with Refractory Ascites. Cochrane Database Syst. Rev. 2006, 2006, CD004889. [Google Scholar] [CrossRef] [PubMed]
- Vizzutti, F.; Celsa, C.; Calvaruso, V.; Enea, M.; Battaglia, S.; Turco, L.; Senzolo, M.; Nardelli, S.; Miraglia, R.; Roccarina, D.; et al. Mortality after Transjugular Intrahepatic Portosystemic Shunt in Older Adult Patients with Cirrhosis: A Validated Prediction Model. Hepatology 2023, 77, 476–488. [Google Scholar] [CrossRef] [PubMed]
- Modha, K.; Kapoor, B.; Lopez, R.; Sands, M.J.; Carey, W. Symptomatic Heart Failure After Transjugular Intrahepatic Portosystemic Shunt Placement: Incidence, Outcomes, and Predictors. Cardiovasc. Intervent. Radiol. 2018, 41, 564–571. [Google Scholar] [CrossRef]
- Billey, C.; Billet, S.; Robic, M.A.; Cognet, T.; Guillaume, M.; Vinel, J.P.; Péron, J.M.; Lairez, O.; Bureau, C. A Prospective Study Identifying Predictive Factors of Cardiac Decompensation After Transjugular Intrahepatic Portosystemic Shunt: The Toulouse Algorithm. Hepatology 2019, 70, 1928–1941. [Google Scholar] [CrossRef]
- Song, T.; Rössle, M.; He, F.; Liu, F.; Guo, X.; Qi, X. Transjugular Intrahepatic Portosystemic Shunt for Hepatorenal Syndrome: A Systematic Review and Meta-Analysis. Dig. Liver Dis. 2018, 50, 323–330. [Google Scholar] [CrossRef]
- Ponzo, P.; Campion, D.; Rizzo, M.; Roma, M.; Caviglia, G.P.; Giovo, I.; Rizzi, F.; Bonetto, S.; Saracco, G.M.; Alessandria, C. Transjugular Intrahepatic Porto-Systemic Shunt in Cirrhotic Patients with Hepatorenal Syndrome-Chronic Kidney Disease: Impact on Renal Function. Dig. Liver Dis. 2022, 54, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- Riggio, O.; Angeloni, S.; Salvatori, F.M.; De Santis, A.; Cerini, F.; Farcomeni, A.; Attili, A.F.; Merli, M. Incidence, Natural History, and Risk Factors of Hepatic Encephalopathy after Transjugular Intrahepatic Portosystemic Shunt with Polytetrafluoroethylene-Covered Stent Grafts. Am. J. Gastroenterol. 2008, 103, 2738–2746. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, S.; Lattanzi, B.; Torrisi, S.; Greco, F.; Farcomeni, A.; Gioia, S.; Merli, M.; Riggio, O. Sarcopenia Is Risk Factor for Development of Hepatic Encephalopathy after Transjugular Intrahepatic Portosystemic Shunt Placement. Clin. Gastroenterol. Hepatol. 2017, 15, 934–936. [Google Scholar] [CrossRef] [PubMed]
- Benmassaoud, A.; Roccarina, D.; Arico, F.; Leandro, G.; Yu, B.; Cheng, F.; Yu, D.; Patch, D.; Tsochatzis, E. Sarcopenia Does Not Worsen Survival in Patients with Cirrhosis Undergoing Transjugular Intrahepatic Portosystemic Shunt for Refractory Ascites. Am. J. Gastroenterol. 2020, 115, 1911–1914. [Google Scholar] [CrossRef] [PubMed]
- Montomoli, J. Body Composition Changes after Transjugular Intrahepatic Portosystemic Shunt in Patients with Cirrhosis. World J. Gastroenterol. 2010, 16, 348. [Google Scholar] [CrossRef]
- Deltenre, P.; Zanetto, A.; Saltini, D.; Moreno, C.; Schepis, F. The Role of Transjugular Intrahepatic Portosystemic Shunt in Patients with Cirrhosis and Ascites: Recent Evolution and Open Questions. Hepatology 2023, 77, 640–658. [Google Scholar] [CrossRef]
- Bettinger, D.; Sturm, L.; Pfaff, L.; Hahn, F.; Kloeckner, R.; Volkwein, L.; Praktiknjo, M.; Lv, Y.; Han, G.; Huber, J.P.; et al. Refining Prediction of Survival after TIPS with the Novel Freiburg Index of Post-TIPS Survival. J. Hepatol. 2021, 74, 1362–1372. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iannone, G.; Pompili, E.; De Venuto, C.; Pratelli, D.; Tedesco, G.; Baldassarre, M.; Caraceni, P.; Zaccherini, G. The Role of Transjugular Intrahepatic Portosystemic Shunt for the Management of Ascites in Patients with Decompensated Cirrhosis. J. Clin. Med. 2024, 13, 1349. https://doi.org/10.3390/jcm13051349
Iannone G, Pompili E, De Venuto C, Pratelli D, Tedesco G, Baldassarre M, Caraceni P, Zaccherini G. The Role of Transjugular Intrahepatic Portosystemic Shunt for the Management of Ascites in Patients with Decompensated Cirrhosis. Journal of Clinical Medicine. 2024; 13(5):1349. https://doi.org/10.3390/jcm13051349
Chicago/Turabian StyleIannone, Giulia, Enrico Pompili, Clara De Venuto, Dario Pratelli, Greta Tedesco, Maurizio Baldassarre, Paolo Caraceni, and Giacomo Zaccherini. 2024. "The Role of Transjugular Intrahepatic Portosystemic Shunt for the Management of Ascites in Patients with Decompensated Cirrhosis" Journal of Clinical Medicine 13, no. 5: 1349. https://doi.org/10.3390/jcm13051349
APA StyleIannone, G., Pompili, E., De Venuto, C., Pratelli, D., Tedesco, G., Baldassarre, M., Caraceni, P., & Zaccherini, G. (2024). The Role of Transjugular Intrahepatic Portosystemic Shunt for the Management of Ascites in Patients with Decompensated Cirrhosis. Journal of Clinical Medicine, 13(5), 1349. https://doi.org/10.3390/jcm13051349