


Optimizing Orthognathic Surgery: Leveraging the Average Skull as a Dynamic Template for Surgical Simulation and Planning in 30 Patient Cases




Abstract
:1. Introduction
2. Materials and Methods
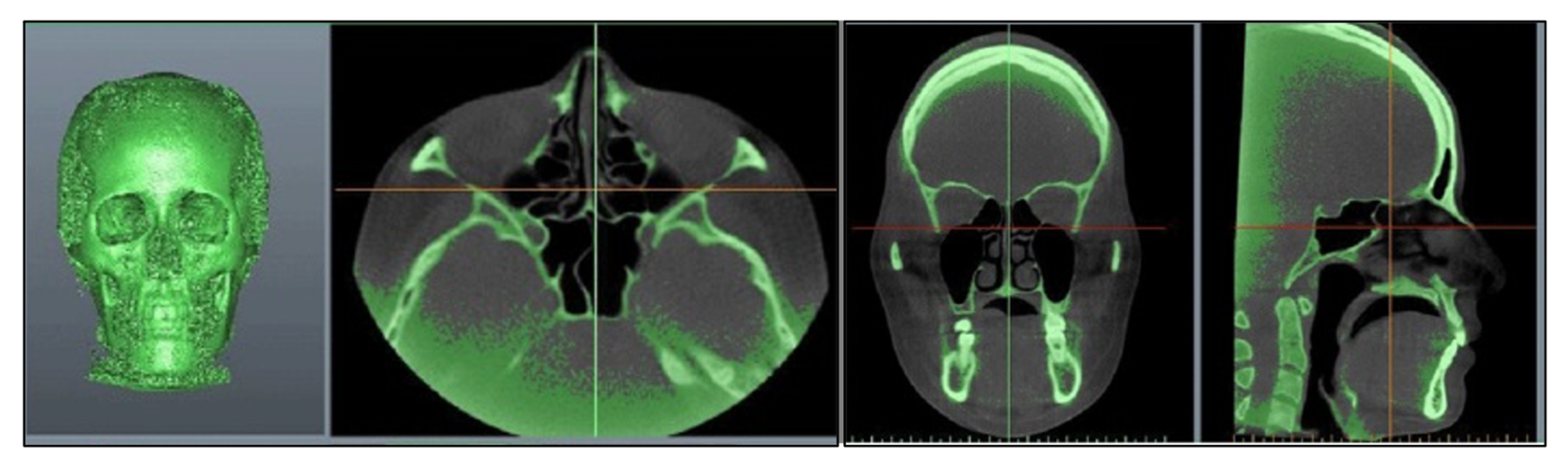
2.1. Three-Dimensional Image Acquisition
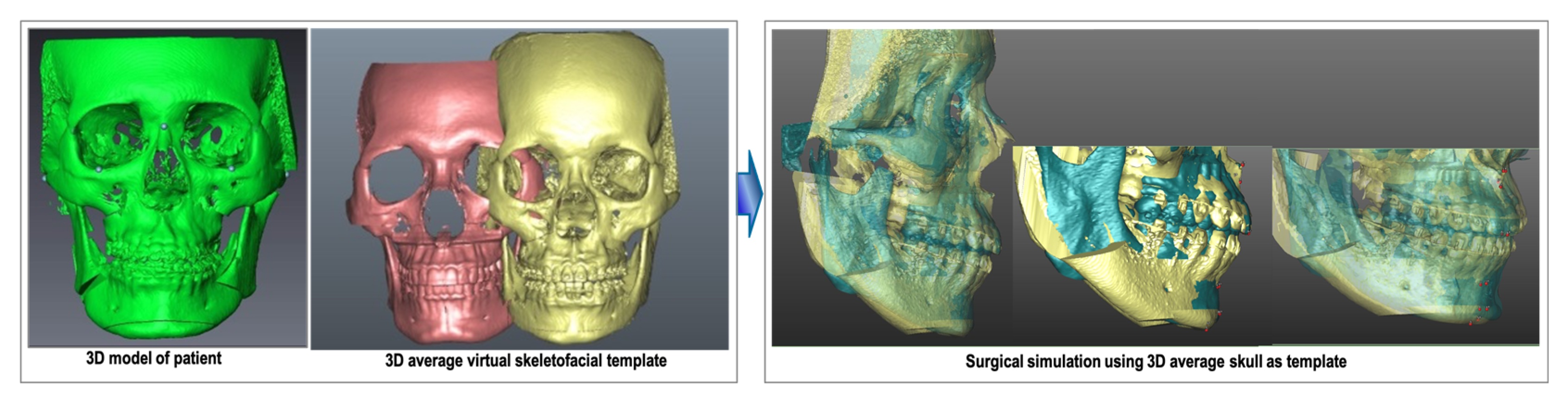
2.2. Surgical Simulation Using 3D Average Skull as Template
2.3. Actual Surgery
2.4. Validation of Post-Operative Outcomes
2.4.1. Quantitative Evaluation of Post-Operative Outcome
2.4.2. Patient-Reported Outcome Questionnaires
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Narayan, H.G.; ChaiKiat, C. Orthodontic-orthognathic interventions in orthognathic surgical cases: “Paper surgery” and “model surgery” concepts in surgical orthodontics. Contemp. Clin. Dent. 2016, 7, 386–390. [Google Scholar]
- Xia, J.J.; Gateno, J.; Teichgraeber, J.F. New clinical protocol to evaluate craniomaxillofacial deformity and plan surgical correction. J. Oral. Maxillofac. Surg. 2009, 67, 2093–2106. [Google Scholar] [CrossRef] [PubMed]
- Naidu, D.; Freer, T.J. Validity, reliability, and reproducibility of the iOC intraoral scanner: A comparison of tooth widths and Bolton ratios. Am. J. Orthod. Dentofacial Orthop. 2013, 144, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Mehl, A.M.; Mörmann, W.H.; Reich, S. Intraoral scanning systems: A current overview. Int. J. Comput. Dent. 2015, 18, 101–129. [Google Scholar] [PubMed]
- Grünheid, T.; McCarthy, S.D.; Larson, B.E. Clinical use of a direct chairside oral scanner: An assessment of accuracy, time, and patient acceptance. Am. J. Orthod. Dentofacial Orthop. 2014, 146, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.T.; Denadai, R.; Lo, L.J.; Lin, H.H. Average 3D Skeletofacial Model as a Template for Maxillomandibular Repositioning During Virtual Orthognathic Surgical Planning. Plast. Reconstr. Surg. 2023, 21, 10–97. [Google Scholar] [CrossRef] [PubMed]
- Proffit, W.R.; Fields, H.W.; Larson, B.; Sarver, D.M. Contemporary Orthodontics, 6th ed.; Mosby Inc.: Maryland Heights, MO, USA, 2013. [Google Scholar]
- Bayome, M.; Park, J.H.; Kook, Y.A. New three-dimensional cephalometric analyses among adults with a skeletal class I pattern and normal occlusion. Korean J. Orthod. 2013, 43, 62–73. [Google Scholar] [CrossRef] [PubMed]
- Cheung, L.K.; Chan, Y.M.; Jayaratne, Y.S.; Lo, J. Three-dimensional cephalometric norms of Chinese adults in Hong Kong with balanced facial profile. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2011, 112, e56–e73. [Google Scholar] [CrossRef]
- Lo, L.J.; Yang, C.T.; Ho, C.T.; Liao, C.H.; Lin, H.H. Automatic Assessment of 3-Dimensional Facial Soft Tissue Symmetry Before and After Orthognathic Surgery Using a Machine Learning Model: A Preliminary Experience. Ann. Plast. Surg. 2021, 3S (Suppl. S2), S224–S228. [Google Scholar] [CrossRef]
- Zhou, X.Y.; Guo, Y.; Shen, M.; Yang, G.Z. Application of artificial intelligence in surgery. Front. Med. 2020, 14, 417–430. [Google Scholar] [CrossRef]
- Bhandari, M.; Zeffiro, T.; Reddiboina, M. Artificial intelligence and robotic surgery: Current perspective and future directions. Curr. Opin. Urol. 2020, 30, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, L.; Yu, C.C.; Chen, Y.R. Single-splint technique for correction of severe facial asymmetry: Correlation between intraoperative maxillomandibular complex roll and restoration of mouth symmetry. Plast. Reconstr. Surg. 2008, 122, 1535–1541. [Google Scholar] [CrossRef] [PubMed]
- Lo, L.J.; Lin, H.H. Applications of three-dimensional imaging techniques in craniomaxillofacial surgery: A literature review. Biomed. J. 2023, 46, 100615. [Google Scholar] [CrossRef] [PubMed]
- Browne, R.H. On the use of a pilot sample for sample size determination. Stat. Med. 1995, 14, 1933–1940. [Google Scholar] [CrossRef] [PubMed]
- Steinhuber, T.; Brunold, S.; Gärtner, C.; Offermanns, V.; Ulmer, H.; Ploder, O. Is virtual surgical planning in orthognathic surgery faster than conventional planning? A time and workflow analysis of an office-based workflow for single-and double-jaw surgery. J. Oral. Maxillofac. Surg. 2018, 76, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Wrzosek, M.K.; Peacock, Z.S.; Laviv, A.; Goldwaser, B.R.; Ortiz, R.; Resnick, C.M.; Troulis, M.J.; Kaban, L.B. Comparison of time required for traditional versus virtual orthognathic surgery treatment planning. Int. J. Oral. Maxillofac. Surg. 2016, 45, 1065–1069. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, C.D.; Manisali, M.; Naini, F.B. Three-dimensional virtual surgical planning (3D-VSP) in orthognathic surgery: Advantages, disadvantages and pitfalls. J. Orthod. 2021, 48, 52–63. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.H.; Chiang, W.C.; Lo, L.J.; Hsu, S.P.; Wang, C.H.; Wan, S.Y. Artifact-resistant superimposition of digital dental models and cone-beam computed tomography images. J. Oral. Maxillofac. Surg. 2013, 71, 1933–1947. [Google Scholar] [CrossRef]
- Baan, F.; Bruggink, R.; Nijsink, J.; Maal, T.J.J.; Ongkosuwito, E.M. Fusion of intra-oral scans in cone-beam computed tomography scans. Clin. Oral. Investig. 2021, 25, 77–85. [Google Scholar] [CrossRef]
- Liao1, Y.F.; Chen, Y.F.; Yao, C.F.; Chen, Y.A.; Chen, Y.R. Long-term outcomes of bimaxillary surgery for treatment of asymmetric skeletal class III deformity using surgery-first approach. Clin. Oral. Investig. 2019, 23, 1685–1693. [Google Scholar] [CrossRef]
- Holte, M.B.; Diaconu, A.; Ingerslev, J.; Thorn, J.J.; Pinholt, E.M. Virtual Analysis of Segmental Bimaxillary Surgery: A Validation Study. J. Oral. Maxillofac. Surg. 2021, 79, 2320–2333. [Google Scholar] [CrossRef]
- Wilson, A.; Gabrick, K.; Wu, R.; Madari, S.; Sawh-Martinez, R.; Steinbacher, D. Conformity of the Actual to the Planned Result in Orthognathic Surgery. Plast. Reconstr. Surg. 2019, 144, 89e–97e. [Google Scholar] [CrossRef] [PubMed]
- de Haan, I.F.; Ciesielski, R.; Nitsche, T.; Koos, B. Evaluation of relapse after orthodontic therapy combined with orthognathic surgery in the treatment of skeletal class III. J. Orofac. Orthop. 2013, 74, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Hsu, S.S.; Gateno, J.; Bell, R.B.; Hirsch, D.L.; Markiewicz, M.R.; Teichgraeber, J.F.; Zhou, X.; Xia, J.J. Accuracy of a computeraided surgical simulation protocol for orthognathic surgery: A prospective multicenter study. J. Oral. Maxillofac. Surg. 2013, 71, 128–142. [Google Scholar] [CrossRef] [PubMed]
- Nelson, E.C.; Eftimovska, E.; Lind, C.; Hager, A.; Wasson, J.H.; Lindblad, S. Patient reported outcome measures in practice. BMJ 2015, 350, g7818. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.W.; Chen, S.H.; Yu, C.C.; Lo, L.J.; Lee, S.R.; Chen, Y.R. Stigma, body image, and quality of life in women seeking orthognathic surgery. Plast. Reconstr. Surg. 2007, 120, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Mani, V.; Panicker, P.; Shenoy, A.; George, A.L.; Chacko, T. Evaluation of Changes in the Alar Base Width Following Lefort 1 and AMO with Conventional Alar Cinch Suturing: A Photographic Study of 100 Cases. J. Maxillofac. Oral. Surg. 2020, 19, 21–25. [Google Scholar] [CrossRef]
- Trevisiol, L.; Lanaro, L.; Favero, V.; Lonardi, F.; Vania, M.; D’Agostino, A. The effect of subspinal Le Fort I osteotomy and alar cinch suture on nasal widening. J. Craniomaxillofac Surg. 2020, 48, 832–838. [Google Scholar] [CrossRef]
- Howley, C.; Ali, N.; Lee, R.; Cox, S. Use of the alar base cinch suture in Le Fort I osteotomy: Is it effective? Br. J. Oral. Maxillofac. Surg. 2011, 49, 127–130. [Google Scholar] [CrossRef]
- Chen, C.M.; Tseng, Y.C.; Ko, E.C.; Chen, M.Y.C.; Chen, K.J.; Cheng, J.H. Comparisons of Jaw Line and Face Line after Mandibular Setback: Intraoral Vertical Ramus versus Sagittal Split Ramus Osteotomie. Biomed. Res. Int. 2018, 2, 1–7. [Google Scholar] [CrossRef]
- Chen, C.M.; Chen Michael, Y.C.; Cheng, J.H.; Chen, K.J.; Tseng, Y.C. Facial profile and frontal changes after bimaxillary surgery in patients with mandibular prognathism. J. Formos. Med. Assoc. 2018, 117, 632–639. [Google Scholar] [CrossRef]
- Yoshioka, I.; Khanal, A.; Tominaga, K.; Horie, A.; Furuta, N.; Fukuda, J. Vertical ramus versus sagittal split osteotomies: Comparison of stability after mandibular setback. J. Oral. Maxillofac. Surg. 2008, 66, 1138–1144. [Google Scholar] [CrossRef]
- Choi, Y.J.; Ha, Y.D.; Lim, H.; Huh, J.K.; Chung, C.J.; Kim, K.H. Long-term changes in mandibular and facial widths afer mandibular setback surgery using intraoral vertical ramus osteotomy. Int. J. Oral. Maxillofac. Surg. 2016, 45, 1074–1080. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Landmark Definition | Mean Difference (mm) | r | p-Value |
|---|---|---|---|
| Nasion (N) | 0.33 | 0.96 | 0.008 * |
| Lateral orbitale (Lo) | 0.31 | 0.98 | 0.003 * |
| External Zygoma (Zy) | 0.44 | 0.88 | 0.002 * |
| Orbitale (Or) | 0.41 | 0.94 | 0.002 * |
| Anterior nasal spine (ANS) | 0.40 | 0.91 | 0.006 * |
| A point (A) | 0.34 | 0.93 | 0.008 * |
| B point (B) | 0.35 | 0.89 | 0.005 * |
| Pogonion (Pog) | 0.37 | 0.93 | 0.006 * |
| Menton (Me) | 0.41 | 0.88 | 0.006 * |
| Gonion (Go) | 0.49 | 0.88 | 0.006 * |
| U1 incisal tip (U1T) | 0.31 | 0.99 | 0.003 * |
| U6 cusp (UR6C, UL6C) | 0.37 | 0.98 | 0.006 * |
| L1 incisal tip (L1T) | 0.34 | 0.93 | 0.005 * |
| L6 cusp (LR6C LL6C) | 0.42 | 0.92 | 0.003 * |
| Mean ± SD | 0.37 ± 0.067 |
| Parameters | Mediolateral | Anteroposterior | Superoinferior | p-Value |
|---|---|---|---|---|
| A point | 0.975 ± 0.805 | 1.150 ± 1.008 | 1.088 ± 0.686 | 0.885 |
| U1 mid | 1.066 ± 0.704 | 1.940 ± 2.082 | 1.216 ± 0.883 | 0.172 |
| B point | 1.379 ± 1.259 | 1.205 ± 0.570 | 1.276 ± 0.832 | 0.908 |
| Pog | 1.475 ± 1.338 | 2.357 ± 0.930 | 1.395 ± 1.397 | 0.148 |
| Me | 1.627 ± 1.376 | 1.672 ± 1.285 | 1.925 ± 1.341 | 0.854 |
| Scale | Orthognathic Surgery-Treated Patients | ||
|---|---|---|---|
| Total | Male | Female | |
| (n = 30) | (n = 18) | (n = 12) | |
| Overall appearance rating (0–100) | 89.6 ± 7.6 | 88.3 ± 8.7 | 89.8 ± 7.2 |
| Facial area satisfaction (0–10) | |||
| Cheek fullness | 8.7 ± 0.9 | 8.8 ± 1.0 | 8.5 ± 0.7 |
| Chin | 9.1 ± 0.9 | 9.1 ± 1.0 | 9.1 ± 0.9 |
| Nose | 8.3 ± 1.1 * | 8.4 ± 1.1 * | 8.2 ± 1.2 |
| Lip | 8.9 ± 1.1 | 8.6 ± 1.3 | 9.3 ± 0.4 |
| Gum show | 8.9 ± 0.9 | 8.9 ± 1.1 | 8.9 ± 0.7 |
| Dental alignment | 9.0 ± 0.9 | 8.9 ± 0.9 | 9.2 ± 0.8 |
| facial width change | 8.6 ± 0.8 | 8.5 ± 0.6 | 8.6 ± 0.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, H.-H.; Kuo, J.-C.; Lo, L.-J.; Ho, C.-T. Optimizing Orthognathic Surgery: Leveraging the Average Skull as a Dynamic Template for Surgical Simulation and Planning in 30 Patient Cases. J. Clin. Med. 2023, 12, 7758. https://doi.org/10.3390/jcm12247758
Lin H-H, Kuo J-C, Lo L-J, Ho C-T. Optimizing Orthognathic Surgery: Leveraging the Average Skull as a Dynamic Template for Surgical Simulation and Planning in 30 Patient Cases. Journal of Clinical Medicine. 2023; 12(24):7758. https://doi.org/10.3390/jcm12247758
Chicago/Turabian StyleLin, Hsiu-Hsia, Jyun-Cheng Kuo, Lun-Jou Lo, and Cheng-Ting Ho. 2023. "Optimizing Orthognathic Surgery: Leveraging the Average Skull as a Dynamic Template for Surgical Simulation and Planning in 30 Patient Cases" Journal of Clinical Medicine 12, no. 24: 7758. https://doi.org/10.3390/jcm12247758
APA StyleLin, H.-H., Kuo, J.-C., Lo, L.-J., & Ho, C.-T. (2023). Optimizing Orthognathic Surgery: Leveraging the Average Skull as a Dynamic Template for Surgical Simulation and Planning in 30 Patient Cases. Journal of Clinical Medicine, 12(24), 7758. https://doi.org/10.3390/jcm12247758