
Correlations between Dental Implant Infectious Pathologies and Maxillary Sinusitis: A Review Article

 , ,
, ,  ,
,  ,
,  and
and 
Abstract
1. Introduction
1.1. Dental Implants and Bone Evaluation
1.2. Bone Augmentation Techniques
1.3. Sinus Complications of Surgical Intervention for Bone Augmentation and Implant Placement
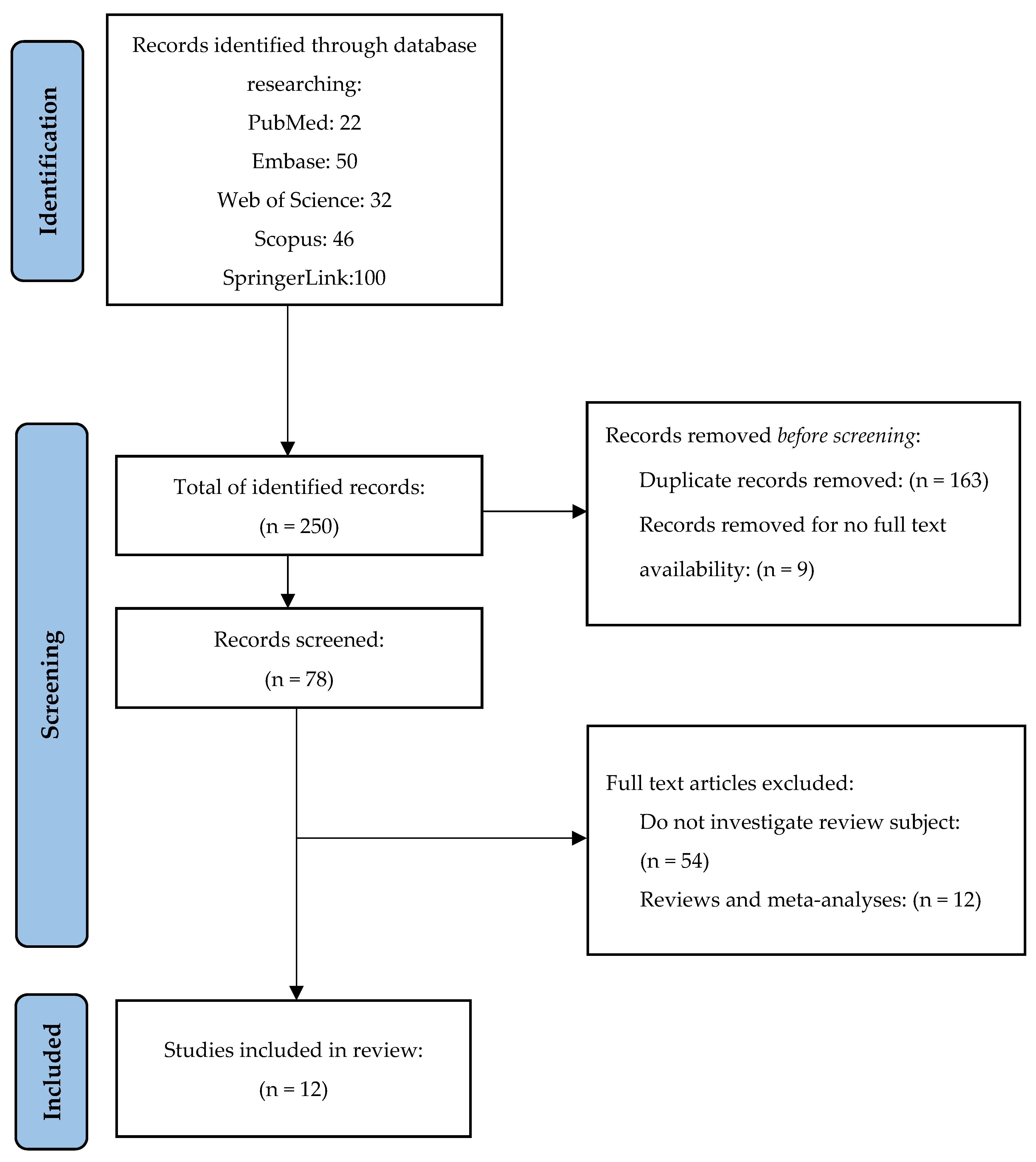
2. Materials and Methods
2.1. Research Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection and Data Collection
2.4. Risk of Bias Assessment (Methodological Quality)
3. Results
3.1. Studies Characteristics
3.2. Correlation among Pathologies
3.2.1. Peri-Implantitis, Sinus Elevation with Bone Augmentation, and Chronic or Acute Sinusitis
3.2.2. Peri-Implantitis Sinusitis and Brain Abscess
3.2.3. Peri-Implantitis and Oro-Antral Communications
3.2.4. Implants Migration/Bone Graft Extrusion into Maxillary Sinus and Sinusitis
3.2.5. Zygomatic Implants and Sinusitis
3.3. Extrapolation of the Result
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kang, D.-W.; Kim, S.-H.; Choi, Y.-H.; Kim, Y.-K. Repeated failure of implants at the same site: A retrospective clinical study. Maxillofac. Plast. Reconstr. Surg. 2019, 41, 27. [Google Scholar] [CrossRef] [PubMed]
- Wolff, R.; Hsu, A.; Heo, Y.; Zhang, L.; Evans, M.; Seong, W. Two-Year Follow-up Comparison of Three Surgical Techniques for Implant Placement in Posterior Maxilla with Limited Alveolar Bone Height. Int. J. Oral Maxillofac. Implant. 2022, 37, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, N.; Maruyama, F.; Takeuchi, Y.; Aikawa, C.; Izumi, Y.; Nakagawa, I. Intraindividual variation in core microbiota in peri-implantitis and periodontitis. Sci. Rep. 2014, 4, 6602. [Google Scholar] [CrossRef] [PubMed]
- Hainarosie, R.; Pietrosanu, C.; Cherecheanu, A.; Stoian, A.P.; Stefanescu, C.; Pituru, S. Risk factors for dental implant failure and medicolegal implications. Rom. J. Leg. Med. 2019, 27, 52–56. [Google Scholar] [CrossRef]
- D’Agostino, A.; Lombardo, G.; Favero, V.; Signoriello, A.; Bressan, A.; Lonardi, F.; Nocini, R.; Trevisiol, L. Complications related to zygomatic implants placement: A retrospective evaluation with 5 years follow-up. J. Cranio-Maxillofac. Surg. 2021, 49, 620–627. [Google Scholar] [CrossRef]
- Park, W.-B.; Kim, Y.-J.; Herr, Y.; Lim, H.-C. Functional Endoscopic Sinus Surgery for Paranasal Sinusitis Originating From a Peri-implantitis–Triggered Infection in the Augmented Maxilla: A Case Report. J. Oral Implant. 2020, 46, 423–429. [Google Scholar] [CrossRef]
- Scarano, A.; Cholakis, A.; Piattelli, A. Histologic Evaluation of Sinus Grafting Materials After Peri-implantitis-Induced Failure: A Case Series. Int. J. Oral Maxillofac. Implant. 2017, 32, e36–e75. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-B.; Yun, P.-Y.; Kim, Y.-K. Clinical evaluation of sinus bone graft in patients with mucous retention cyst. Maxillofac. Plast. Reconstr. Surg. 2016, 38, 35. [Google Scholar] [CrossRef]
- Ganesan, K.; Rathod, N. Maxillary Sinusitis. In Oral and Maxillofacial Surgery for the Clinician; Bonanthaya, K., Panneerselvam, E., Manuel, S., Kumar, V.V., Rai, A., Eds.; Springer: Singapore. [CrossRef]
- Hong, S.O.; Shim, G.-J.; Kwon, Y.-D. Novel approach to the maxillary sinusitis after sinus graft. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 18. [Google Scholar] [CrossRef]
- Kumar, H.; Jain, R.; Douglas, R.G.; Tawhai, M.H. Airflow in the Human Nasal Passage and Sinuses of Chronic Rhinosinusitis Subjects. PLoS ONE 2016, 11, e0156379. [Google Scholar] [CrossRef] [PubMed]
- Cocuzza, S.; Maniaci, A.; Di Luca, M.; La Mantia, I.; Grillo, C.; Spinato, G.; Motta, G.; Testa, D.; Ferlito, S. Long-term results of nasal surgery: Comparison of mini-invasive turbinoplasty. J. Biol. Regul. Homeost. Agents 2020, 34, 1203–1208. [Google Scholar] [CrossRef]
- Galofré, M.; Palao, D.; Vicario, M.; Nart, J.; Violant, D. Clinical and microbiological evaluation of the effect of Lactobacillus reuteri in the treatment of mucositis and peri-implantitis: A triple-blind randomized clinical trial. J. Periodontal Res. 2018, 53, 378–390. [Google Scholar] [CrossRef]
- Rakašević, D.; Lazić, Z.; Rakonjac, B. Efficiency of photodynamic therapy in the treatment of peri-implantitis—A three-month randomized controlled clinical trial. Srp. Arh. Celok. Lek. 2016, 144, 478–484. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 89, 105906. [Google Scholar]
- PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/ (accessed on 1 February 2023).
- Embase. Embase—A Biomedical Research Database. Available online: elsevier.com (accessed on 1 February 2023).
- Web of Science. Available online: https://www.webofscience.com/wos/ (accessed on 1 February 2023).
- Scopus Elsevier. Available online: https://www.elsevier.com/solutions/scopus (accessed on 1 February 2023).
- SpringerLink. Available online: https://link.springer.com/ (accessed on 1 February 2023).
- Wells, G.; Shea, B.; O’Connell, D. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analysis; The Ottawa Health Research Institute: Ottawa, ON, Canada, 2011. [Google Scholar]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef]
- Haffar, S.; Bazerbachi, F.; Prokop, L.; Watt, K.D.; Murad, M.H.; Chari, S.T. Frequency and prognosis of acute pancreatitis associated with fulminant or non-fulminant acute hepatitis A: A systematic review. Pancreatology 2017, 17, 166–175. [Google Scholar] [CrossRef]
- Bazerbachi, F.; Sawas, T.; Vargas, E.J.; Prokop, L.J.; Chari, S.T.; Gleeson, F.C.; Levy, M.J.; Martin, J.; Petersen, B.T.; Pearson, R.K.; et al. Metal stents versus plastic stents for the management of pancreatic walled-off necrosis: A systematic review and meta-analysis. Gastrointest. Endosc. 2018, 87, 30–42e15. [Google Scholar] [CrossRef]
- Bazerbachi, F.; Leise, M.D.; Watt, K.D.; Murad, M.H.; Prokop, L.J.; Haffar, S. Systematic review of mixed cryoglobulinemia associated with hepatitis E virus infection: Association or causation? Gastroenterol. Rep. 2017, 5, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Bazerbachi, F.; Haffar, S.; Szarka, L.A.; Wang, Z.; Prokop, L.J.; Murad, M.H.; Camilleri, M. Secretory diarrhea and hypokalemia associated with colonic pseudo-obstruction: A case study and systematic analysis of the literature. Neurogastroenterol. Motil. 2017, 29, e13120. [Google Scholar] [CrossRef] [PubMed]
- Bazerbachi, F.; Haffar, S.; Hussain, M.T.; Vargas, E.J.; Watt, K.D.; Murad, M.H.; Chari, S.; Abu Dayyeh, B.K. Systematic review of acute pancreatitis associated with interferon-α or pegylated interferon-α: Possible or definitive causation? Pancreatology 2018, 18, 691–699. [Google Scholar] [CrossRef]
- Steiner, C.; Bottini, G.; Gaggl, A. Brain abscess caused by dental peri-implantitis. Br. J. Oral Maxillofac. Surg. 2021, 59, 109–110. [Google Scholar] [CrossRef] [PubMed]
- van de Loo, S.; Kessler, P.; Lethaus, B. Spontaneous Transmaxillary-Transnasal Implant Loss: A Case Report. Implant. Dent. 2013, 22, 117–119. [Google Scholar] [CrossRef]
- Yalçın, M.; Can, S.; Akbaş, M.; Dergin, G.; Garip, H.; Aydil, B.; Varol, A. Retrospective Analysis of Zygomatic Implants for Maxillary Prosthetic Rehabilitation. Int. J. Oral Maxillofac. Implant. 2020, 35, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Park, W.-B.; Han, J.-Y.; Oh, S.-L. Maxillary Sinusitis Associated With Peri-implantitis at Sinus Floor Augmented Sites: Case Series. Implant. Dent. 2019, 28, 484–489. [Google Scholar] [CrossRef]
- Rodriguez, A.; Nowzari, H. The long-term risks and complications of bovine-derived xenografts: A case series. J. Indian Soc. Periodontol. 2019, 23, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Al-Juboori, M.J.; Al-Shaeli, A.J.; Radhi, H.; Filho, L.C.M.; Al-Attas, M.A. Chronic Submerged Implant Infection Treated with Immediate Implantation and Guided Bone Regeneration: A Case Report. Open Dent. J. 2019, 13, 160–164. [Google Scholar] [CrossRef]
- Park, M.J.; Park, H.I.; Ahn, K.; Kim, J.H.; Chung, Y.; Jang, Y.J.; Yu, M.S. Features of Odontogenic Sinusitis Associated with Dental Implants. Laryngoscope 2022, 133, 237–243. [Google Scholar] [CrossRef]
- Kim, W.J.; Cho, Y.-D.; Ku, Y.; Ryoo, H.-M. The worldwide patent landscape of dental implant technology. Biomater. Res. 2022, 26, 59. [Google Scholar] [CrossRef]
- Carinci, F.; Lauritano, D.; Bignozzi, C.A.; Pazzi, D.; Candotto, V.; Santos De Oliveira, P.; Scarano, A.; De Oliveira, S. A New Strategy against Peri-Implantitis: Antibacterial Internal Coating. Int. J. Mol. Sci. 2019, 20, 3897. [Google Scholar] [CrossRef]
- Testori, T.; Drago, L.; Wallace, S.S.; Capelli, M.; Galli, F.; Zuffetti, F.; Parenti, A.; Deflorian, M.; Fumagalli, L.; Weinstein, R.L.; et al. Prevention and Treatment of Postoperative Infections after Sinus Elevation Surgery: Clinical Consensus and Recommendations. Int. J. Dent. 2012, 2012, 365809. [Google Scholar] [CrossRef]
- Nam, K.-Y.; Kim, J.-B. Treatment of dental implant-related maxillary sinusitis with functional endoscopic sinus surgery in combination with an intra-oral approach. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 87–90. [Google Scholar] [CrossRef]
- Stacchi, C.; Troiano, G.; Rapani, A.; Lombardi, T.; Sentineri, R.; Speroni, S.; Berton, F.; Di Lenarda, R. Factors influencing the prevalence of peri-implantitis in implants inserted in augmented maxillary sinuses: A multicenter cross-sectional study. J. Periodontol. 2020, 92, 1117–1125. [Google Scholar] [CrossRef]
- Levin, L. Dealing with dental implant failures. J. Appl. Oral Sci. 2008, 16, 171–175. [Google Scholar] [CrossRef]
- Tomasi, C.; Derks, J. Etiology, occurrence, and consequences of implant loss. Periodontology 2000 2022, 88, 13–35. [Google Scholar] [CrossRef]
- Sakka, S.; Baroudi, K.; Nassani, M.Z. Factors associated with early and late failure of dental implants. J. Investig. Clin. Dent. 2012, 3, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Belibasakis, G.; Manoil, D. Microbial Community-Driven Etiopathogenesis of Peri-Implantitis. J. Dent. Res. 2021, 100, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Baba, Y.; Kato, Y.; Takahashi, K. Proposal for a Paradigm Shift in Personalized Medicine for Patients with a Maxillary Edentulous Jaw by ENT Specialist and Dentist Cooperation. J. Pers. Med. 2022, 12, 1289. [Google Scholar] [CrossRef] [PubMed]
- Little, R.E.; Long, C.M.; Loehrl, T.A.; Poetker, D.M. Odontogenic sinusitis: A review of the current literature. Laryngoscope Investig. Otolaryngol. 2018, 3, 110–114. [Google Scholar] [CrossRef]
- Yoo, B.J.; Jung, S.M.; Na Lee, H.; Kim, H.G.; Chung, J.H.; Jeong, J.H. Treatment Strategy for Odontogenic Sinusitis. Am. J. Rhinol. Allergy 2021, 35, 206–212. [Google Scholar] [CrossRef]
- Molinero-Mourelle, P.; Baca-Gonzalez, L.; Gao, B.; Saez-Alcaide, L.M.; Helm, A.; Lopez-Quiles, J. Surgical complications in zygo-matic implants: A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e751–e757. [Google Scholar] [CrossRef]
- Maniaci, A.; Merlino, F.; Cocuzza, S.; Iannella, G.; Vicini, C.; Cammaroto, G.; Lechien, J.R.; Calvo-Henriquez, C.; La Mantia, I. Endoscopic surgical treatment for rhinogenic contact point headache: Systematic review and meta-analysis. Eur. Arch. Otorhino-Laryngol. Off. J. Eur. Fed. Oto-Rhino-Laryngol. Soc. (EUFOS) Affil. Ger. Soc. Oto-Rhino-Laryngol.-Head Neck Surg. 2021, 278, 1743–1753. [Google Scholar] [CrossRef]


{kind=link}
| First Author/Year | No. of Cases | Question 1 | Question 2 | Question 3 | Question 4 | Question 5 | Methodological Quality | Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| Steiner, C./2021 [28] | 1 | YES | YES | YES | YES | YES | HIGH | LOW |
| Hong, S.O./2017 [10] | 1 | NO | YES | YES | YES | YES | MODERATE | MODERATE |
| D’Agostino, A./2021 [5] | 42 | YES | YES | YES | YES | YES | HIGH | LOW |
| Park, W. -B./2020 [6] | 1 | NO | YES | YES | YES | YES | MODERATE | MODERATE |
| van de Loo, S./2013 [29] | 1 | YES | YES | YES | YES | YES | HIGH | LOW |
| Scarano, A./2017 [7] | 5 | YES | YES | YES | YES | YES | HIGH | LOW |
| Yalçın, M./2020 [30] | 45 | NO | YES | YES | YES | YES | MODERATE | MODERATE |
| Park, W.-B./2019 [31] | 124 | NO | YES | YES | YES | YES | MODERATE | MODERATE |
| Rodriguez, A./2019 [32] | 5 | NO | YES | YES | YES | YES | MODERATE | MODERATE |
| Hainăroșie, R./2019 [4] | 21 | NO | YES | YES | YES | YES | MODERATE | MODERATE |
| Al-Juboori, M.J./2019 [33] | 1 | NO | YES | YES | YES | YES | MODERATE | MODERATE |
| Study | Selection | Comparability | Outcome | NOS Score | Methodological Quality | Risk of Bias |
|---|---|---|---|---|---|---|
| Case–control studies | ||||||
| Park, M.J./2023 [34] | *** | * | *** | 7 | HIGH | LOW |
| First Author/Year | Study Design | Country | No. of Patients | Age/Mean Age of Patients | Gender of Patients | Associated Pathologies/Risk Factors | Type of Intervention | No. of Implants/Localization | Studied Pathologies | Follow-Up Length (Median) |
|---|---|---|---|---|---|---|---|---|---|---|
| Steiner, C./2021 [28] | Case report | Austria | 1 | 62 years | Male | Not mentioned | dental implant insertion | 1/in the left upper jaw | brain abscess in the left frontal lobe left maxillary and frontal sinusitis | 10 months |
| Hong, S.O./2017 [10] | Case report | Republic of Korea | 1 | 47 years | Male | Not mentioned | Sinus elevation, bone graft, and implant insertion 10 days previously | 1/right upper jaw | sinusitis of the right maxilla | 3.5 months |
| D’Agostino, A./2021 [5] | Case series | Italy | 42 | 63 ± 10 years (range 29–81) years | 16 males and 26 females | 8 patients were smokers | Zygomatic implant insertion with 5 years follow-up | Upper jaw | Peri-implantitis, maxillary sinusitis, oroantral communication | 60 months |
| Park, W. -B./2020 [6] | Case report | Republic of Korea | 1 | - | Male | No pathologies | lateral sinus augmentation simultaneously with implant placement, left posterior maxilla, 15 years ago | 2 implants/incisor and premolar area | Peri-implantitis, oroantral communication, left maxillary, ethmoid, and frontal sinusitis | 12 months |
| van de Loo, S./2013 [29] | Case report | Netherlands | 1 | 65 years | Male | Not mentioned | Maxillary implants inserted 7 years ago | Upper jaw | Peri-implantitis, periodontitis, chronic maxillary sinusitis with recurring signs of acute sinusitis | 4 months |
| Scarano, A./2017 [7] | Case series | Italy | 5 | 54 years | 3 males, 2 females | medical history of the patient was noncontributory | maxillary sub antral augmentation procedure and implant insertion | Posterior upper jaw | Peri-implantitis, maxillary sinusitis | 3–6 years |
| Yalçın, M./2020 [30] | Case series | Turkey | 45 | 51.76 years (range: 23 to 72) years. | 24 males, 21 females | Patients with risk factor pathologies were excluded | Zygomatic implants insertion | Upper jaw | zygomatic implants with infection, peri-implantitis, sinusitis, oroantral fistula | 17.2 months |
| Park, W.-B./2019 [31] | Case series | Korea | 8 | 48.3 ± 7 years | 7 males, 1 female | 5 patients were smokers | Implant placement with sinus floor augmentation | Upper jaw | Peri-implantitis, Maxillary sinusitis | 3 years |
| Rodriguez, A./2019 [32] | Case series | California | 5 | 58.7 years | 2 males, 3 females | 1 patient with a medical history of angina, hypercholesterolemia, aortic valve stenosis, and periodontal disease, and another 1 with hypertension, hypercholesterolemia, osteoarthritis, asthma, and periodontitis | Bone augmentation procedures and dental implant insertion | Upper jaw | sinus and maxillary bone pathologies, displacement of the graft materials, oroantral communication, peri-implantitis, maxillary cysts | - |
| Hainăroșie, R./2019 [4] | Case series | Romania | 21 | 47 years | 7 males, 14 females | 5 patients with diabetes mellitus | sinus lift procedure, concomitant with dental implant insertion | Upper jaw | Peri-implantitis, acute bacterial maxillary rhinosinusitis, acute fungal maxillary rhinosinusitis, implant migration into the maxillary sinus, orbital abscess, malar abscess | 6 months |
| Al-Juboori, M. J./2019 [33] | Case report | Iraq | 1 | 45 years | Female | No systemic diseases, no smoking | Implant insertion | Upper right lateral incisor | Chronic sinusitis with sinus discharge at the site of submerged implant | 1 month |
| Park, M.J./2023 [34] | Case-control | South Korea | 60 | 59.5 ± 19.1 | 32 males, 28 females | 15 tobacco smokers and 28 social alcohol drinking | Implant insertion, bone graft | Upper maxilla | Peri-implantitis, maxillary sinusitis. | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iușan, S.A.L.; Costache, C.; Lucaciu, O.P.; Petrescu, B.-N.; Mirică, I.C.; Toc, D.-A.; Albu, S. Correlations between Dental Implant Infectious Pathologies and Maxillary Sinusitis: A Review Article. J. Clin. Med. 2023, 12, 5059. https://doi.org/10.3390/jcm12155059
Iușan SAL, Costache C, Lucaciu OP, Petrescu B-N, Mirică IC, Toc D-A, Albu S. Correlations between Dental Implant Infectious Pathologies and Maxillary Sinusitis: A Review Article. Journal of Clinical Medicine. 2023; 12(15):5059. https://doi.org/10.3390/jcm12155059
Chicago/Turabian StyleIușan, Simina Angela Lăcrimioara, Carmen Costache, Ondine Patricia Lucaciu, Bianca-Nausica Petrescu, Ioana Codruța Mirică, Dan-Alexandru Toc, and Silviu Albu. 2023. "Correlations between Dental Implant Infectious Pathologies and Maxillary Sinusitis: A Review Article" Journal of Clinical Medicine 12, no. 15: 5059. https://doi.org/10.3390/jcm12155059
APA StyleIușan, S. A. L., Costache, C., Lucaciu, O. P., Petrescu, B.-N., Mirică, I. C., Toc, D.-A., & Albu, S. (2023). Correlations between Dental Implant Infectious Pathologies and Maxillary Sinusitis: A Review Article. Journal of Clinical Medicine, 12(15), 5059. https://doi.org/10.3390/jcm12155059