
Effects of Ripasudil on Open-Angle Glaucoma after Circumferential Suture Trabeculotomy Ab Interno


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Surgical Technique
2.3. Data Collection and Statistical Analysis
3. Results
3.1. Disposition and Characteristics of Patients
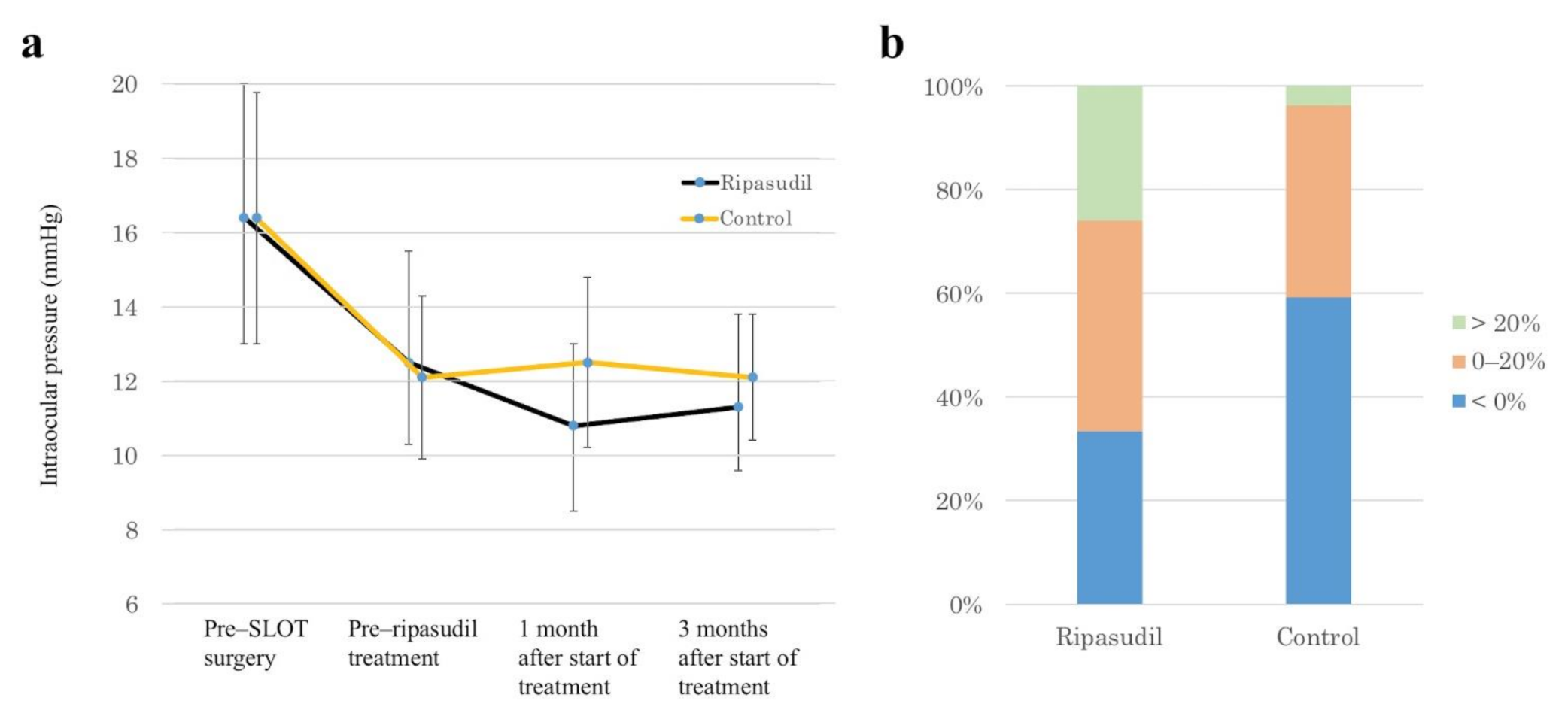
3.2. Efficacy
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Quigley, H.A. Glaucoma. Lancet 2011, 377, 1367–1377. [Google Scholar] [CrossRef]
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- Cohen, L.P.; Pasquale, L.R. Clinical characteristics and current treatment of glaucoma. Cold Spring Harb. Perspect. Med. 2014, 4, a017236. [Google Scholar] [CrossRef] [PubMed]
- Mantravadi, A.V.; Vadhar, N. Glaucoma. Care 2015, 42, 437–449. [Google Scholar] [CrossRef]
- Bill, A.; Phillips, C.I. Uveoscleral drainage of aqueous humour in human eyes. Exp. Eye Res. 1971, 3, 275–281. [Google Scholar] [CrossRef]
- Tamm, E.R. The trabecular meshwork outflow pathways: Structural and functional aspects. Exp. Eye Res. 2009, 88, 648–655. [Google Scholar] [CrossRef]
- Tektas, O.Y.; Lütjen-Drecoll, E. Structural changes of the trabecular meshwork in different kinds of glaucoma. Exp. Eye Res. 2009, 88, 769–775. [Google Scholar] [CrossRef]
- Rosenquist, R.; Epstein, D.; Melamed, S.; Johnson, M.; Grant, W.M. Outflow resistance of enucleated human eyes at two different perfusion pressures and different extents of trabeculotomy. Curr. Eye Res. 1989, 8, 1233–1240. [Google Scholar] [CrossRef]
- Schuman, J.S.; Chang, W.; Wang, N.; De Kater, A.W.; Allingham, R.R. Excimer laser effects on outflow facility and outflow pathway morphology. Investig. Ophthalmol. Vis. Sci. 1999, 40, 1676–1680. [Google Scholar]
- Konopińska, J.; Kozera, M.; Kraśnicki, P.; Mariak, Z.; Rękas, M. The Effectiveness of First-Generation iStent Microbypass Implantation Depends on Initial Intraocular Pressure: 24-Month Follow-Up-Prospective Clinical Trial. J. Ophthalmol. 2020, 2020, 8164703. [Google Scholar] [CrossRef]
- Honjo, M.; Tanihara, H.; Inatani, M.; Kido, N.; Sawamura, T.; Yue, B.Y.; Narumiya, S.; Honda, Y. Effects of rho-associated protein kinase inhibitor Y-27632 on intraocular pressure and outflow facility. Investig. Ophthalmol. Vis. Sci. 2001, 42, 137–144. [Google Scholar]
- Inoue, T.; Tanihara, H. Rho-associated kinase inhibitors: A novel glaucoma therapy. Prog. Retin. Eye Res. 2013, 37, 1–12. [Google Scholar] [CrossRef]
- Tanihara, H.; Inoue, T.; Yamamoto, T.; Kuwayama, Y.; Abe, H.; Fukushima, A.; Suganami, H.; Araie, M. K-115 Clinical Study Group. One-year clinical evaluation of 0.4% ripasudil (K-115) in patients with open-angle glaucoma and ocular hypertension. Acta Ophthalmol. 2016, 94, e26–e34. [Google Scholar] [CrossRef]
- Wang, R.F.; Williamson, J.E.; Kopczynski, C.; Serle, J.B. Effect of 0.04% AR-13324, a ROCK, and norepinephrine transporter inhibitor, on aqueous humor dynamics in normotensive monkey eyes. J. Glaucoma 2015, 24, 51–54. [Google Scholar] [CrossRef]
- Sturdivant, J.M.; Royalty, S.M.; Lin, C.W.; Moore, L.A.; Yingling, J.D.; Laethem, C.L.; Sherman, B.; Heintzelman, G.R.; Kopczynski, C.C.; DeLong, M.A. Discovery of the ROCK inhibitor netarsudil for the treatment of open-angle glaucoma. Bioorg. Med. Chem. Lett. 2016, 26, 2475–2480. [Google Scholar] [CrossRef] [PubMed]
- Kiel, J.W.; Kopczynski, C.C. Effect of AR-13324 on episcleral venous pressure in Dutch belted rabbits. J. Ocul. Pharmacol. Ther. 2015, 31, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Mukherjee, D.; Navarro, I.; Ashpole, N.E.; Sherwood, J.M.; Chang, J.; Overby, D.R.; Yuan, F.; Gonzalez, P.; Kopczynski, C.C.; et al. Visualization of conventional outflow tissue responses to netarsudil in living mouse eyes. Eur. J. Pharmacol. 2016, 787, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Ren, R.; Li, G.; Le, T.D.; Kopczynski, C.; Stamer, W.D.; Gong, H. Netarsudil Increases Outflow Facility in Human Eyes Through Multiple Mechanisms. Investig. Ophthalmol. Vis. Sci. 2016, 57, 6197–6209. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Waxman, S.; Wang, C.; Atta, S.; Loewen, R.; Loewen, N.A. Dose-dependent effects of netarsudil, a Rho-kinase inhibitor, on the distal outflow tract. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 1211–1216. [Google Scholar] [CrossRef]
- Kazemi, A.; McLaren, J.W.; Kopczynski, C.C.; Heah, T.G.; Novack, G.D.; Sit, A.J. The Effects of Netarsudil Ophthalmic Solution on Aqueous Humor Dynamics in a Randomized Study in Humans. J. Ocul. Pharmacol. Ther. 2018, 34, 380–386. [Google Scholar] [CrossRef]
- Sato, T.; Kawaji, T.; Hirata, A.; Mizoguchi, T. 360-degree suture trabeculotomy ab interno to treat open-angle glaucoma: 2-year outcomes. Clin. Ophthalmol. 2018, 12, 915–923. [Google Scholar] [CrossRef]
- Sato, T.; Kawaji, T.; Hirata, A.; Mizoguchi, T. 360-degree suture trabeculotomy ab interno with phacoemulsification in open-angle glaucoma and coexisting cataract: A pilot study. BMJ Open Ophthalmol. 2018, 3, e000159. [Google Scholar] [CrossRef] [PubMed]
- Parikh, H.A.; Loewen, R.T.; Roy, P.; Schuman, J.S.; Lathrop, K.L.; Loewen, N.A. Differential Canalograms Detect Outflow Changes from Trabecular Micro-Bypass Stents and Ab Interno Trabeculectomy. Sci. Rep. 2016, 6, 34705. [Google Scholar] [CrossRef] [PubMed]
- Dang, Y.; Wang, C.; Shah, P.; Waxman, S.; Loewen, R.T.; Hong, Y.; Esfandiari, H.; Loewen, N.A. Outflow enhancement by three different ab interno trabeculectomy procedures in a porcine anterior segment model. Graefes Arch. Clin. Exp. Ophthalmol. 2018, 256, 1305–1312. [Google Scholar] [CrossRef] [PubMed]
- Fallano, K.; Bussel, I.; Kagemann, L.; Lathrop, K.L.; Loewen, N. Training strategies and outcomes of ab interno trabeculectomy with the trabectome. F1000Research 2017, 6, 67. [Google Scholar] [CrossRef]
- McDonnell, F.; Dismuke, W.M.; Overby, D.R.; Stamer, W.D. Pharmacological regulation of outflow resistance distal to Schlemm’s canal. Am. J. Physiol. Cell Physiol. 2018, 315, C44–C51. [Google Scholar] [CrossRef]
- Fellman, R.L.; Feuer, W.J.; Grover, D.S. Episcleral Venous Fluid Wave Correlates with Trabectome Outcomes: Intraoperative Evaluation of the Trabecular Outflow Pathway. Ophthalmology 2015, 122, 2385–2391.e1. [Google Scholar] [CrossRef]
- Fellman, R.L.; Grover, D.S. Episcleral Venous Fluid Wave in the Living Human Eye Adjacent to Microinvasive Glaucoma Surgery (MIGS) Supports Laboratory Research: Outflow is Limited Circumferentially, Conserved Distally, and Favored Inferonasally. J. Glaucoma 2019, 28, 139–145. [Google Scholar] [CrossRef]
- Goda, E.; Hirooka, K.; Mori, K.; Kiuchi, Y. Intraocular pressure-lowering effects of Ripasudil: A potential outcome marker for Trabeculotomy. BMC Ophthalmol. 2019, 19, 243. [Google Scholar] [CrossRef]
- Bovee, C.E.; Pasquale, L.R. Evolving Surgical Interventions in the Treatment of Glaucoma. Semin. Ophthalmol. 2017, 32, 91–95. [Google Scholar] [CrossRef]
- Agrawal, P.; Bradshaw, S.E. Systematic Literature Review of Clinical and Economic Outcomes of Micro-Invasive Glaucoma Surgery (MIGS) in Primary Open-Angle Glaucoma. Ophthalmol. Ther. 2018, 7, 49–73. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Ripasudil | Control | p-Value |
|---|---|---|---|
| No. of patients | 27 | 27 | |
| Age, years, mean ± SD (range) | 79.7 ± 6.8 (63–88) | 78.5 ± 7.6 (64–89) | 0.548 |
| Male/female, n | 15/12 | 11/16 | 0.414 |
| Right/left, n | 11/16 | 13/14 | 0.352 |
| IOP, mmHg, mean ± SD (range) | |||
| Pre-SLOT surgery | 16.4 ± 3.6 (11–26) | 16.4 ± 3.4 (11–25) | 0.785 |
| Pre-ripasudil treatment | 12.5 ± 3.0 (6–21) | 12.1 ± 2.2 (7–16) | 0.775 |
| No. of preoperative medications, mean ± SD (range) | 1.9 ± 1.3 (0–4) | 1.4 ± 1.5 (0–4) | 0.525 |
| BCVA, logMAR, mean ± SD (range) | 0.26 ± 0.21 (0–0.82) | 0.35 ± 0.22 (0–1.10) | 0.295 |
| Visual field, MD (dB), mean ± SD (range) | −8.6 ± 5.4 (−18.4–−0.2) | −9.7 ± 8.1 (−27.9–−1.6) | 0.106 |
| Axial length, mm, mean ± SD (range) | 23.7 ± 0.8 (22.5–25.8) | 24.2 ± 1.5 (21.3–27.4) | 0.569 |
| Type of glaucoma, n (%) | 0.211 | ||
| POAG | 10 | 13 | |
| NTG | 10 | 11 | |
| XFG | 7 | 3 |
| Background Factor | T-Value | p-Value |
|---|---|---|
| IOP (mmHg) before surgery | 1.67 | 0.097 |
| IOP (mmHg) before ripasudil treatment | −7.28 | <0.001 |
| Medication before surgery | 1.99 | 0.050 |
| Age (years) | 0.38 | 0.702 |
| Visual field (mean deviation, dB) | −0.39 | 0.699 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sato, T.; Kawaji, T. Effects of Ripasudil on Open-Angle Glaucoma after Circumferential Suture Trabeculotomy Ab Interno. J. Clin. Med. 2021, 10, 401. https://doi.org/10.3390/jcm10030401
Sato T, Kawaji T. Effects of Ripasudil on Open-Angle Glaucoma after Circumferential Suture Trabeculotomy Ab Interno. Journal of Clinical Medicine. 2021; 10(3):401. https://doi.org/10.3390/jcm10030401
Chicago/Turabian StyleSato, Tomoki, and Takahiro Kawaji. 2021. "Effects of Ripasudil on Open-Angle Glaucoma after Circumferential Suture Trabeculotomy Ab Interno" Journal of Clinical Medicine 10, no. 3: 401. https://doi.org/10.3390/jcm10030401
APA StyleSato, T., & Kawaji, T. (2021). Effects of Ripasudil on Open-Angle Glaucoma after Circumferential Suture Trabeculotomy Ab Interno. Journal of Clinical Medicine, 10(3), 401. https://doi.org/10.3390/jcm10030401