
Efficacy of Birth Dose Vaccination in Preventing Mother-to-Child Transmission of Hepatitis B: A Randomized Controlled Trial Comparing Engerix-B and Sci-B-Vac


 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participant Population
2.2. Primary Endpoint
2.3. Secondary Endpoint
2.4. Statistical Analysis
3. Results
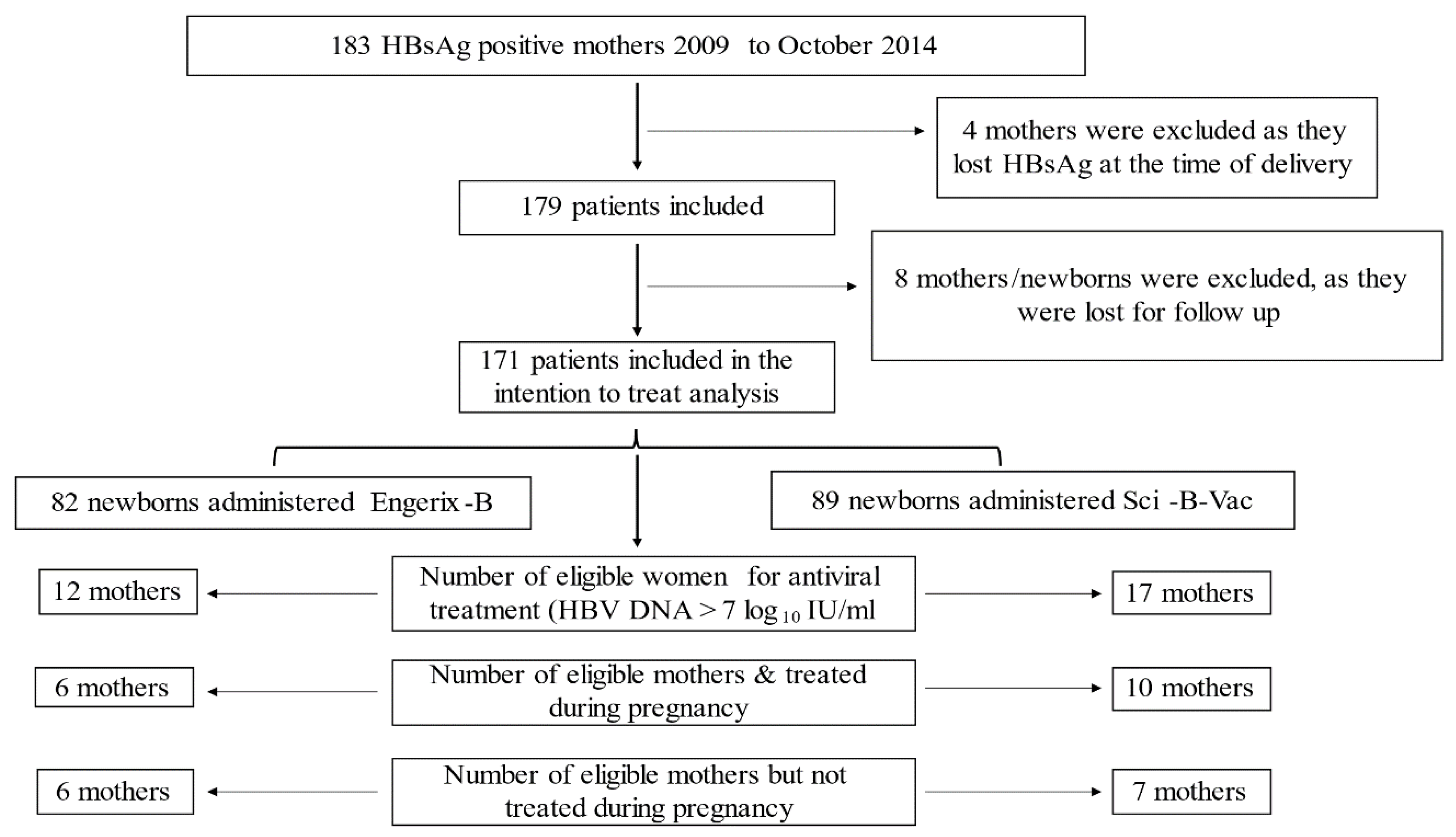
3.1. Participants
3.2. Maternal Characteristics
3.3. Newborn Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HBV | hepatitis B virus |
| HBsAg+ | hepatitis B surface antigen positive |
| HBIG | Hepatitis B Immune Globulin |
| INR | international normalized ratio |
| HBsAg | hepatitis B surface antigen |
| HBeAg | hepatitis B e antigen |
| anti-HBe | antibody to hepatitis B e antigen |
| HCV | hepatitis C virus |
| HDV | hepatitis D virus |
| anti-HBc | antibody to hepatitis B core antigen |
| anti-HBs | antibody to hepatitis B surface antigen |
| WHO | World Health Organization |
| MTCT | mother to child HBV transmission |
| IM | intramuscular |
| ALT | alanine aminotransferase |
| AST | aspartate transferase |
| PCR | polymerase chain reaction |
| SD | standard deviation |
| NUC | nucleoside analogues |
| EASL | Association for the Study of the Liver |
| AASLD | American Association for the Study of Liver Diseases |
References
- Guidelines for the Prevention, Care and Treatment of Persons with Chronic Hepatitis B Infection; WHO: Geneva, Switzerland, 2015.
- Lavanchy, D. Hepatitis B virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. J. Viral. Hepat. 2004, 11, 97–107. [Google Scholar] [CrossRef]
- Tong, M.J.; Pan, C.Q.; Hann, H.W.; Kowdley, K.V.; Han, S.H.; Min, A.D.; Leduc, T.S. The management of chronic hepatitis B in Asian Americans. Dig. Dis. Sci. 2011, 56, 3143–3162. [Google Scholar] [CrossRef]
- Hu, K.Q.; Pan, C.Q.; Goodwin, D. Barriers to screening for hepatitis B virus infection in Asian Americans. Dig. Dis. Sci. 2011, 56, 3163–3171. [Google Scholar] [CrossRef]
- Perumalswami, P.V.; Factor, S.H.; Kapelusznik, L.; Friedman, S.L.; Pan, C.Q.; Chang, C.; Di Clemente, F.; Dieterich, D.T. Hepatitis Outreach Network: A practical strategy for hepatitis screening with linkage to care in foreign-born communities. J. Hepatol. 2013, 58, 890–897. [Google Scholar] [CrossRef]
- Publication, W.H.O. Hepatitis B vaccines: WHO position paper—Recommendations. Vaccine 2010, 28, 589–590. [Google Scholar] [CrossRef]
- Boucheron, P.; Lu, Y.; Yoshida, K.; Zhao, T.; Funk, A.L.; Lunel-Fabiani, F.; Guingane, A.; Tuaillon, E.; van Holten, J.; Chou, R.; et al. Accuracy of HBeAg to identify pregnant women at risk of transmitting hepatitis B virus to their neonates: A systematic review and meta-analysis. Lancet Infect. Dis. 2021, 21, 85–96. [Google Scholar] [CrossRef]
- Michaiel, R.; Margalit, R.C.; Shteyer, E.; Ashur, Y.; Safadi, R. Vertical HBV transmission in Jerusalem in the vaccine era. Harefuah 2012, 151, 671–674, 721, 722. [Google Scholar] [PubMed]
- Stevens, C.E.; Beasley, R.P.; Tsui, J.; Lee, W.C. Vertical transmission of hepatitis B antigen in Taiwan. N. Engl. J. Med. 1975, 292, 771–774. [Google Scholar] [CrossRef]
- Shouval, D.; Roggendorf, H.; Roggendorf, M. Enhanced immune response to hepatitis B vaccination through immunization with a Pre-S1/Pre-S2/S vaccine. Med. Microbiol. Immunol. 2015, 204, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Qawasmi, M.; Samuh, M.; Glebe, D.; Gerlich, W.H.; Azzeh, M. Age-dependent decrease of anti-HBs titers and effect of booster doses using 2 different vaccines in Palestinian children vaccinated in early childhood. Hum. Vaccines Immunother. 2015, 11, 1717–1724. [Google Scholar] [CrossRef]
- Seiz, P.L.; Slanina, H.; Ziebuhr, J.; Gerlich, W.H.; Glebe, D.; Schuttler, C.G. Studies of nosocomial outbreaks of hepatitis B in nursing homes in Germany suggest a major role of hepatitis B e antigen expression in disease severity and progression. Int. J. Med. Microbiol. 2015, 305, 663–672. [Google Scholar] [CrossRef] [PubMed]
- Abdelnabi, Z.; Saleh, N.; Baraghithi, S.; Glebe, D.; Azzeh, M. Subgenotypes and mutations in the s and polymerase genes of hepatitis B virus carriers in the West Bank, palestine. PLoS ONE 2014, 9, e113821. [Google Scholar] [CrossRef]
- Alter, M.J. Epidemiology of hepatitis B in Europe and worldwide. J. Hepatol. 2003, 39 (Suppl. 1), S64–S69. [Google Scholar] [CrossRef]
- Jonas, M.M. Hepatitis B and pregnancy: An underestimated issue. Liver Int. 2009, 29 (Suppl. 1), 133–139. [Google Scholar] [CrossRef]
- Furuncuoglu, Y.; Bolukbas, F.F.; Bolukbas, C.; Torun, P.; Ozturk, R. Changes in the prevalence of HBV infection in pregnant women in Turkey between 1995 and 2015: A 20-year evaluation. Postgrad. Med. J. 2016, 92, 510–513. [Google Scholar] [CrossRef] [PubMed]
- Su, W.J.; Liu, C.C.; Liu, D.P.; Chen, S.F.; Huang, J.J.; Chan, T.C.; Chang, M.H. Effect of age on the incidence of acute hepatitis B after 25 years of a universal newborn hepatitis B immunization program in Taiwan. J. Infect. Dis. 2012, 205, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Kao, J.H.; Chen, D.S. Universal hepatitis B vaccination: Killing 2 birds with 1 stone. Am. J. Med. 2008, 121, 1029–1031. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.H.; Chen, C.J.; Lai, M.S.; Hsu, H.M.; Wu, T.C.; Kong, M.S.; Liang, D.C.; Shau, W.Y.; Chen, D.S. Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children. Taiwan Childhood Hepatoma Study Group. N. Engl. J. Med. 1997, 336, 1855–1859. [Google Scholar] [CrossRef]
- Kao, J.H.; Hsu, H.M.; Shau, W.Y.; Chang, M.H.; Chen, D.S. Universal hepatitis B vaccination and the decreased mortality from fulminant hepatitis in infants in Taiwan. J. Pediatr. 2001, 139, 349–352. [Google Scholar] [CrossRef]
- Chen, H.L.; Lin, L.H.; Hu, F.C.; Lee, J.T.; Lin, W.T.; Yang, Y.J.; Huang, F.C.; Wu, S.F.; Chen, S.C.; Wen, W.H.; et al. Effects of maternal screening and universal immunization to prevent mother-to-infant transmission of HBV. Gastroenterology 2012, 142, 773–781.e772. [Google Scholar] [CrossRef]
- Chen, H.L.; Wen, W.H.; Chang, M.H. Management of Pregnant Women and Children: Focusing on Preventing Mother-to-Infant Transmission. J. Infect. Dis. 2017, 216, S785–S791. [Google Scholar] [CrossRef] [PubMed]
- Ni, Y.H.; Chang, M.H.; Wu, J.F.; Hsu, H.Y.; Chen, H.L.; Chen, D.S. Minimization of hepatitis B infection by a 25-year universal vaccination program. J. Hepatol. 2012, 57, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Madalinski, K.; Sylvan, S.P.; Hellstrom, U.; Mikolajewicz, J.; Dzierzanowska-Fangrat, K. Presence of anti-preS1, anti-preS2, and anti-HBs antibodies in newborns immunized with Bio-Hep-B vaccine. Med. Sci. Monit. 2004, 10, PI10–PI17. [Google Scholar] [PubMed]
- Wiseman, E.; Fraser, M.A.; Holden, S.; Glass, A.; Kidson, B.L.; Heron, L.G.; Maley, M.W.; Ayres, A.; Locarnini, S.A.; Levy, M.T. Perinatal transmission of hepatitis B virus: An Australian experience. Med. J. Aust. 2009, 190, 489–492. [Google Scholar] [CrossRef] [PubMed]
- del Canho, R.; Grosheide, P.M.; Mazel, J.A.; Heijtink, R.A.; Hop, W.C.; Gerards, L.J.; de Gast, G.C.; Fetter, W.P.; Zwijneberg, J.; Schalm, S.W. Ten-year neonatal hepatitis B vaccination program, The Netherlands, 1982–1992: Protective efficacy and long-term immunogenicity. Vaccine 1997, 15, 1624–1630. [Google Scholar] [CrossRef]
- Brown, R.S., Jr.; McMahon, B.J.; Lok, A.S.; Wong, J.B.; Ahmed, A.T.; Mouchli, M.A.; Wang, Z.; Prokop, L.J.; Murad, M.H.; Mohammed, K. Antiviral therapy in chronic hepatitis B viral infection during pregnancy: A systematic review and meta-analysis. Hepatology 2016, 63, 319–333. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. Electronic address, e.e.e.; European Association for the Study of the, L. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef]
- Terrault, N.A.; Bzowej, N.H.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Murad, M.H.; American Association for the Study of Liver, D. AASLD guidelines for treatment of chronic hepatitis B. Hepatology 2016, 63, 261–283. [Google Scholar] [CrossRef]
- Funk, A.L.; Lu, Y.; Yoshida, K.; Zhao, T.; Boucheron, P.; van Holten, J.; Chou, R.; Bulterys, M.; Shimakawa, Y. Efficacy and safety of antiviral prophylaxis during pregnancy to prevent mother-to-child transmission of hepatitis B virus: A systematic review and meta-analysis. Lancet Infect. Dis. 2021, 21, 70–84. [Google Scholar] [CrossRef]
- Nelson, N.P.; Jamieson, D.J.; Murphy, T.V. Prevention of Perinatal Hepatitis B Virus Transmission. J. Pediatric. Infect. Dis. Soc. 2014, 3 (Suppl. 1), S7–S12. [Google Scholar] [CrossRef]
- Stramer, S.L.; Wend, U.; Candotti, D.; Foster, G.A.; Hollinger, F.B.; Dodd, R.Y.; Allain, J.P.; Gerlich, W. Nucleic acid testing to detect HBV infection in blood donors. N. Engl. J. Med. 2011, 364, 236–247. [Google Scholar] [CrossRef] [PubMed]
- Gerlich, W.H. Good news from WHO on prevention of peripartum hepatitis B transmission. Lancet Infect. Dis. 2021, 21, 6–8. [Google Scholar] [CrossRef]
- Bremer, C.M.; Sominskaya, I.; Skrastina, D.; Pumpens, P.; El Wahed, A.A.; Beutling, U.; Frank, R.; Fritz, H.J.; Hunsmann, G.; Gerlich, W.H.; et al. N-terminal myristoylation-dependent masking of neutralizing epitopes in the preS1 attachment site of hepatitis B virus. J. Hepatol. 2011, 55, 29–37. [Google Scholar] [CrossRef]
- Yan, H.; Zhong, G.; Xu, G.; He, W.; Jing, Z.; Gao, Z.; Huang, Y.; Qi, Y.; Peng, B.; Wang, H.; et al. Sodium taurocholate cotransporting polypeptide is a functional receptor for human hepatitis B and D virus. Elife 2012, 3. [Google Scholar] [CrossRef] [PubMed]
- Neurath, A.R.; Kent, S.B.; Parker, K.; Prince, A.M.; Strick, N.; Brotman, B.; Sproul, P. Antibodies to a synthetic peptide from the preS 120–145 region of the hepatitis B virus envelope are virus neutralizing. Vaccine 1986, 4, 35–37. [Google Scholar] [CrossRef]
- Glebe, D.; Aliakbari, M.; Krass, P.; Knoop, E.V.; Valerius, K.P.; Gerlich, W.H. Pre-s1 antigen-dependent infection of Tupaia hepatocyte cultures with human hepatitis B virus. J. Virol. 2003, 77, 9511–9521. [Google Scholar] [CrossRef] [PubMed]
- Milich, D.R.; McLachlan, A.; Thornton, G.B. T-cell recognition of pre-S regions of HBsAg can bypass nonresponse to the S region. Adv. Exp. Med. Biol. 1987, 225, 233–239. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intention to Treat Analysis | Per Protocol Analysis | |||||
|---|---|---|---|---|---|---|
| Variables | Group A (n = 82) | Group B (n = 89) | p Value | Group A (n = 82) | Group B (n = 81) | p Value |
| Engerix-B | Sci-B-Vac | Engerix-B | Sci-B-Vac | |||
| Age, (median ± IQR) | 27.03 ± 9.53 | 28 ± 8.02 | 0.15 | 27.03 ± 9.53 | 28.3 ± 9.14 | 0.09 |
| ALT (U\L), (median ± IQR) | 19 ± 11 | 16 ± 14 | 0.3 | 19 ± 11 | 16 ± 15 | 0.3 |
| AST (U\L), (median ± IQR) | 22 ±12 | 21 ± 13 | 0.7 | 22 ± 12 | 21 ± 13.5 | 0.8 |
| WBC (thousands), (median ± IQR) | 6.86 ± 2.8 | 7.2 ± 2.42 | 0.4 | 6.86 ± 2.8 | 7.4 ± 2.43 | 0.3 |
| Hb (g\dl), (median ± IQR) | 12.2 ± 1.6 | 11.7 ± 2 | 0.054 | 12.2 ± 1.6 | 11.7 ± 2 | 0.051 |
| PLT (thousands), (median ± IQR) | 230 ± 62 | 200 ± 82 | 0.051 | 230 ± 62 | 201 ± 90 | 0.06 |
| INR, (median ± IQR) | 1.04 ± 0.12 | 1.01 ± 0.1 | 0.02 | 1.04 ± 0.12 | 1.01 ± 0.11 | 0.03 |
| HBsAg+ N (%) | 82 (100) | 89 (100) | - | 82 (100) | 81 (100) | - |
| HBeAg+ N (%) | 7 (8.54) | 10 (11.24) | 0.44 | 7 (8.54) | 9 (11.1) | 0.4 |
| Anti-HBe+ N (%) | 74 (90.24) | 69 (77.53) | 0.58 | 74 (90.24) | 64 (79.01) | 0.7 |
| HBV DNA status | ||||||
| Positive mothers, N | 67 (81.7) | 69 (77.5) | 0.1 | 67 (81.7) | 63 (77.8) | 0.2 |
| >log10 IU/mL, (median ± IQR) | 2.6 ± 2.14 | 2.1 ± 3.36 | 0.19 | 2.6 ± 2.14 | 2.33 ± 3.53 | 0.2 |
| * Maternal viral loads, N (%) | ||||||
| 14 (17.1) | 20 (22.5) | 0.4 | 14 (17.1) | 19 (23.5) | 0.3 |
| 39 (47.6) | 40 (44.9) | 0.9 | 39 (47.6) | 37 (45.7) | 0.9 |
| 16 (19.5) | 14 (15.7) | 0.6 | 16 (19.5) | 11 (13.6) | 0.3 |
| 5 (6.1) | 4 (4.5) | 0.8 | 5 (6.1) | 4 (4.9) | 0.8 |
| 7 (8.5) | 7 (7.9) | 0.7 | 7 (8.5) | 6 (7.4) | 0.8 |
| ** Maternal viral loads, N (%) | ||||||
| 14 (17.3) | 20 (23.5) | 0.4 | 14 (17.3) | 19 (24.7) | 0.3 |
| 39 (48.1) | 40 (47.1) | 0.9 | 39 (48.1) | 37 (48.1) | 0.9 |
| 16 (19.8) | 14 (16.5) | 0.6 | 16 (19.8) | 11 (14.3) | 0.3 |
| 5 (6.2) | 5 (5.9) | 0.8 | 5 (6.2) | 4 (5.2) | 0.8 |
| 7 (8.6) | 6 (7.1) | 0.7 | 7 (8.6) | 6 (7.8) | 0.8 |
| Anti-viral treatment, N (%) | ||||||
| 2 (2.4) | 2 (2.5) | 0.2 | 2 (2.4) | 2 (2.5) | 0.2 |
| 4 (4.8) | 4 (4.9) | 0.2 | 4 (4.8) | 4 (4.9) | 0.2 |
| 0 | 4 (4.9) | 0.1 | 0 | 4 (4.9) | 0.1 |
| Serial Number of Mothers Who Had Genetic Analysis | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| HBV subgenotype | D1 | D1 | D2 | D1 | D1 | D1 | D1 | D1 | D2 |
| HBsAg subtype | ayw2 | ayw2 or 4 | ayw3 | ayw2 | ayw2 | ayw2 | ayw2 | ayw2 | ayw2 |
| Mutations in RT | I266T | - | M129L, E271D | R110F | R110G, S119P, L164M Q215S | N238D | L157M, V214A, Q215S, I266K | F221Y | M204V, P237H |
| Mutations in S gene | P203R | T127L | T118A | S174N | Y200F, Y206F, S207R | - | S193L, Y206H, S207R | S207N, L213I | - |
| Vaccine immune escape | no | no | no | no | no | no | no | no | no |
| Drug resistance | no | no | no | no | no | no | no | no | LMV, (ETV) |
| Maternal Characteristics | |||||||||
| Viral load IU/mL | 1860 | <15 | 319000 | 83.9 | 16000 | 10093 | <15 | 109 | 150 |
| HBeAg | Negative | Negative | Positive | Negative | Negative | Negative | Negative | Not available | Negative |
| Therapy | None | None | None | None | None | None | None | None | Entecavir |
| ALT (U/L) | 9 | 20 | 14 | 16 | 18 | 15 | 342 | - | 18 |
| Infants’ Characteristics | |||||||||
| HBsAg | Negative | Negative | Positive | Negative | Negative | Negative | Negative | Negative | Negative |
| Anti-HBs titer mIU/mL | 123.4 | 1100 | 5.68 | 1100 | 1100 | 174.9 | 211.1 | 1100 | 76.9 |
| Anti-HBc | Positive | Positive | Positive | Positive | Positive | Positive | Positive | Positive | Positive |
| Intention to Treat Analysis | Per Protocol Analysis | |||||
|---|---|---|---|---|---|---|
| Variables, N (%) | Group A (n = 82) | Group B (n = 89) | p value | Group A (n = 82) | Group B (n = 81) | p value |
| Engerix-B | Sci-B-Vac | Engerix-B | Sci-B-Vac | |||
| HBsAg+ | 5 (6.1) | 1 (1.1) | 0.05 | 5 (6.1) | 1 (1.2) | 0.05 |
| Anti-HBs titers | ||||||
| 8 (9.8) | 2 (2.2) | 0.05 | 8 (9.9) | 2 (2.5) | 0.09 |
| 73 (90.1) | 85 (97.7) | 0.05 | 73 (90.1) | 79 (97.5) | 0.09 |
| 52 (64.2) | 68 (78.2) | 0.05 | 52 (64.2) | 64 (79) | 0.05 |
| 12 (14.8) | 28 (32.2) | 0.01 | 12 (14.8) | 27 (33.3) | 0.009 |
| Anti-HBc positivity | 28 (34.1) | 26 (29) | 0.4 | 28 (34.1) | 23 (28.4) | 0.4 |
| Anti-HBc positivity according to maternal viral loads at delivery | ||||||
| 6 (7.3) | 1 (1.1) | 0.04 | 6 (7.3) | 1 (1.2) | 0.055 |
| 11 (13.4) | 13 (14.6) | 0.8 | 11 (13.4) | 13 (16) | 0.6 |
| 5 (6.1) | 5 (5.6) | 0.9 | 5 (6.1) | 4 (4.9) | 0.7 |
| 2 (2.4) | 2 (2.2) | 0.9 | 2 (2.4) | 2 (2.5) | 0.99 |
| 4 (4.9) | 3 (3.4) | 0.6 | 4 (4.9) | 3 (3.7) | 0.7 |
| Intention to Treat Analysis | Per Protocol Analysis | |||||
| Variables, N (%) | Group A (n = 75) Engerix-B | Group B (n = 75) Sci-B-Vac | p Value | Group A (n = 75) Engerix-B | Group B (n = 67) Sci-B-Vac | p Value |
| HBsAg positivity in children according to Maternal viral loads | ||||||
| 1/11 | 0/18 | 0.3 | 1/11 | 0/17 | 0.3 |
| (9.1%) | 0 | (9.1%) | 0 | |||
| 1/39 | 0/37 | 1 | 1/39 | 0/34 | 1 |
| (2.6%) | 0 | (2.6%) | 0 | |||
| 0/14 | 0/14 | 1 | 0/14 | 0/11 | 1 |
| 0 | 0 | 0 | 0 | |||
| 1/4 | 0/3 | 1 | 1/4 | 0/2 | 1 |
| (25%) | 0 | (25%) | 0 | |||
| 2/7 | 1/3 | 0.9 | 2/7 | 1/3 | 0.6 |
| (28.6%) | (33.3%) | (28.6%) | (33.3%) | |||
| Anti-HBc positivity in children according to Maternal viral loads | ||||||
| 3/11 | 1/18 | 0.09 | 3/11 | 1/17 | 0.1 |
| (27.3%) | (5.6%) | (27.3%) | (5.9%) | |||
| 11/39 | 12/37 | 0.6 | 11/39 | 12/34 | 0.5 |
| (28.2%) | (32.4%) | (28.2%) | (35.3%) | |||
| 5/14 | 5/14 | 1 | 5/14 | 4/11 | 0.9 |
| (35.7%) | (35.7%) | (35.7%) | (36.4%) | |||
| 1/4 | 2/3 | 0.3 | 1/4 | 2/2 | 0.4 |
| (25%) | (66.7%) | (25%) | (100%) | |||
| 5/7 | 3/3 | 0.9 | 5/7 | 3/3 | 0.9 |
| (71.4%) | (100%) | (71.4%) | (100%) | |||
| Infant Characteristics at 12 Months | |||||
|---|---|---|---|---|---|
| Case Number | Gender | Administered Vaccine | HBsAg | Anti-HBs Titer mIU/mL | Anti-HBc |
| 1 | Male | Engerix-B | Positive | 249.8 | Positive |
| 2 | Male | Engerix-B | Positive | 5.68 | Positive |
| 3 | Male | Engerix-B | Positive | 3.16 | Positive |
| 4 | Female | Engerix-B | Positive | 0.85 | Positive |
| 5 | Female | Engerix-B | Positive | 0.2 | Positive |
| 6 | Female | Sci-B-Vac | Positive | 0.4 | Positive |
| Maternal Characteristics | |||||
| Case number | Age at delivery (Years) | Antiviral therapy | HBeAg | Anti-HBe | HBV DNA Log at Delivery |
| 1 | 23 | No | Negative | Positive | <1.28 |
| 2 | 25 | No | Positive | Negative | 5.5 |
| 3 | 32 | No | Positive | Negative | 8.49 |
| 4 | 21 | No | Negative | Positive | 9.53 |
| 5 | 19 | No | Negative | Positive | <1.28 |
| 6 | 26 | No | Positive | Negative | 9.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Safadi, R.; Khoury, T.; Saed, N.; Hakim, M.; Jamalia, J.; Nijim, Y.; Farah, N.; Nuser, T.; Natur, N.; Mahamid, M.; et al. Efficacy of Birth Dose Vaccination in Preventing Mother-to-Child Transmission of Hepatitis B: A Randomized Controlled Trial Comparing Engerix-B and Sci-B-Vac. Vaccines 2021, 9, 331. https://doi.org/10.3390/vaccines9040331
Safadi R, Khoury T, Saed N, Hakim M, Jamalia J, Nijim Y, Farah N, Nuser T, Natur N, Mahamid M, et al. Efficacy of Birth Dose Vaccination in Preventing Mother-to-Child Transmission of Hepatitis B: A Randomized Controlled Trial Comparing Engerix-B and Sci-B-Vac. Vaccines. 2021; 9(4):331. https://doi.org/10.3390/vaccines9040331
Chicago/Turabian StyleSafadi, Rifaat, Tawfik Khoury, Nizar Saed, Marwan Hakim, Jeryes Jamalia, Yousef Nijim, Nicola Farah, Tawfik Nuser, Nidaa Natur, Mahmud Mahamid, and et al. 2021. "Efficacy of Birth Dose Vaccination in Preventing Mother-to-Child Transmission of Hepatitis B: A Randomized Controlled Trial Comparing Engerix-B and Sci-B-Vac" Vaccines 9, no. 4: 331. https://doi.org/10.3390/vaccines9040331
APA StyleSafadi, R., Khoury, T., Saed, N., Hakim, M., Jamalia, J., Nijim, Y., Farah, N., Nuser, T., Natur, N., Mahamid, M., Amer, J., Roppert, P. L., Gerlich, W. H., & Glebe, D. (2021). Efficacy of Birth Dose Vaccination in Preventing Mother-to-Child Transmission of Hepatitis B: A Randomized Controlled Trial Comparing Engerix-B and Sci-B-Vac. Vaccines, 9(4), 331. https://doi.org/10.3390/vaccines9040331