

Omicron Variant of SARS-CoV-2: An Indian Perspective of Vaccination and Management

 , , , and
, , , and 
Abstract
1. Introduction
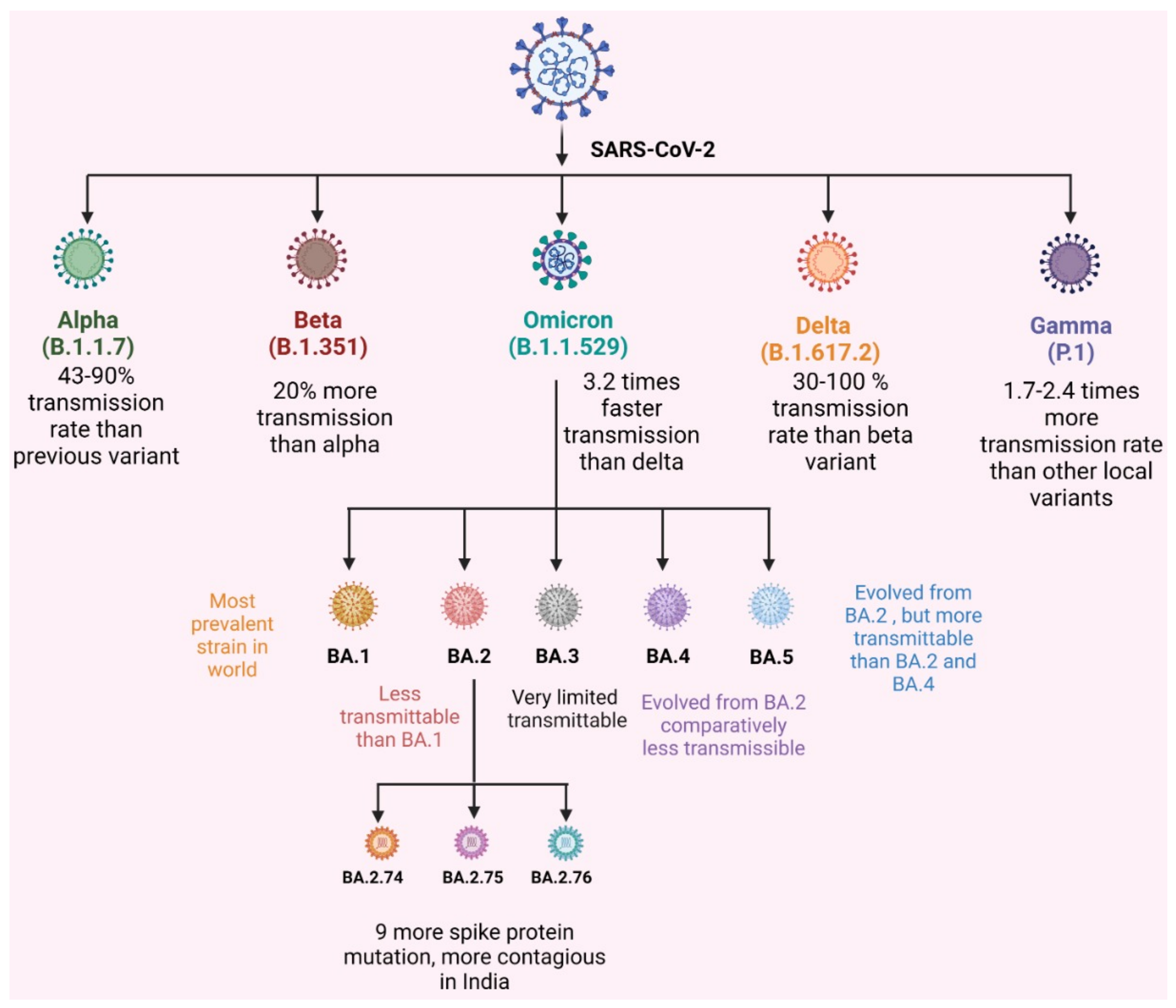
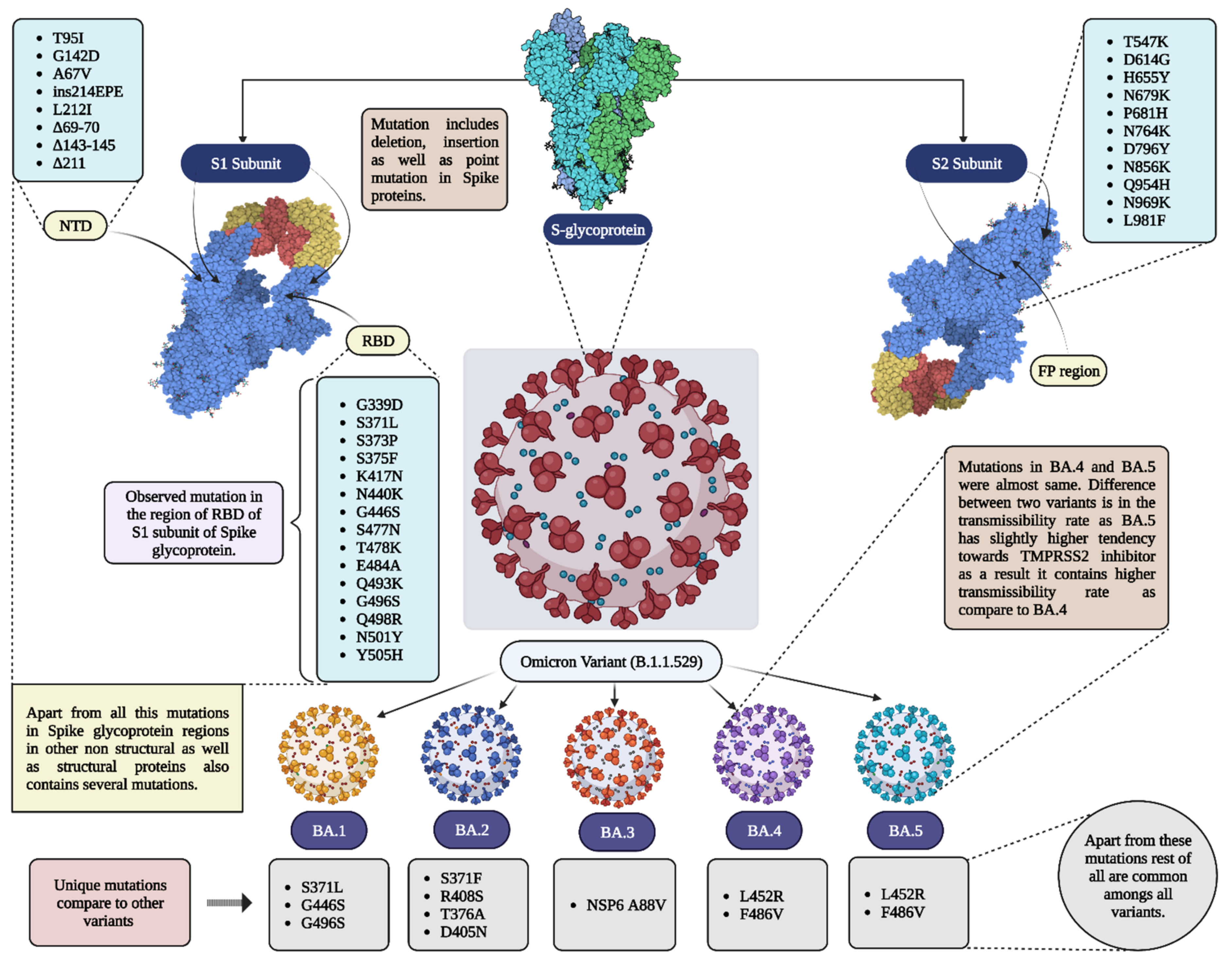
2. Omicron Subvariants
2.1. BA.1
2.2. BA.2
2.3. BA.4 and BA.5
3. Impact of Delta and Omicron Variants in India
4. Diagnostic and Treatment Impact
5. Omicron and Vaccination
6. Vaccine Hesitancy and Current Scenario
7. Omicron, Monkeypox, and Hand, Foot, and Mouth Disease (HFMD)/Tomato Flu
8. Limitations
9. Future Aspects
10. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pal, M.; Berhanu, G.; Desalegn, C.; Kandi, V. Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2): An Update. Cureus 2020, 12, e7423. [Google Scholar] [CrossRef] [PubMed]
- Chavda, V.P.; Apostolopoulos, V. COVID-19 Vaccine Design and Vaccination Strategy for Emerging Variants. Expert Rev. Vaccines 2022, 21, 1359–1361. [Google Scholar] [CrossRef]
- He, X.; Hong, W.; Pan, X.; Lu, G.; Wei, X. SARS-CoV-2 Omicron Variant: Characteristics and Prevention. MedComm 2021, 2, 838–845. [Google Scholar] [CrossRef] [PubMed]
- Chavda, V.P.; Bezbaruah, R.; Deka, K.; Nongrang, L.; Kalita, T. The Delta and Omicron Variants of SARS-CoV-2: What We Know So Far. Vaccines 2022, 10, 1926. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, P.L.C.; Moreira, F.R.R.; de Souza, R.M.; Guimarães, N.R.; Carvalho, N.O.; Adelino, T.E.R.; Alves, H.J.; Alvim, L.B.; Candido, D.S.; Coelho, H.P.; et al. Tracking the Turnover of SARS-CoV-2 VOCs Gamma to Delta in a Brazilian State (Minas Gerais) with a High-Vaccination Status. Virus Evol. 2022, 8, veac064. [Google Scholar] [CrossRef] [PubMed]
- Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/activities/tracking-SARS-CoV-2-variants (accessed on 9 December 2022).
- Chavda, V.P.; Apostolopoulos, V. Global Impact of Delta plus Variant and Vaccination. Expert Rev. Vaccines 2022, 21, 597–600. [Google Scholar] [CrossRef]
- Chavda, V.P.; Patel, A.B.; Vaghasiya, D.D. SARS-CoV-2 Variants and Vulnerability at the Global Level. J. Med. Virol. 2022, 94, 2986–3005. [Google Scholar] [CrossRef]
- Dhawan, M.; Sharma, A.; Priyanka; Thakur, N.; Rajkhowa, T.K.; Choudhary, O.P. Delta Variant (B.1.617.2) of SARS-CoV-2: Mutations, Impact, Challenges and Possible Solutions. Hum. Vaccines Immunother. 2022, 18, 2068883. [Google Scholar] [CrossRef]
- Bian, L.; Gao, Q.; Gao, F.; Wang, Q.; He, Q.; Wu, X.; Mao, Q.; Xu, M.; Liang, Z. Impact of the Delta Variant on Vaccine Efficacy and Response Strategies. Expert Rev. Vaccines 2021, 20, 1201–1209. [Google Scholar] [CrossRef]
- Shrestha, L.B.; Foster, C.; Rawlinson, W.; Tedla, N.; Bull, R.A. Evolution of the SARS-CoV-2 Omicron Variants BA.1 to BA.5: Implications for Immune Escape and Transmission. Rev. Med. Virol. 2022, 32, e2381. [Google Scholar] [CrossRef]
- Ou, J.; Lan, W.; Wu, X.; Zhao, T.; Duan, B.; Yang, P.; Ren, Y.; Quan, L.; Zhao, W.; Seto, D.; et al. Tracking SARS-CoV-2 Omicron Diverse Spike Gene Mutations Identifies Multiple Inter-Variant Recombination Events. Signal Transduct. Target. 2022, 7, 138. [Google Scholar] [CrossRef] [PubMed]
- Karim, S.S.A.; Karim, Q.A. Omicron SARS-CoV-2 Variant: A New Chapter in the COVID-19 Pandemic. Lancet 2021, 398, 2126–2128. [Google Scholar] [CrossRef] [PubMed]
- Chavda, V.P.; Apostolopoulos, V. Is Booster Dose Strategy Sufficient for Omicron Variant of SARS-CoV-2? Vaccines 2022, 10, 367. [Google Scholar] [CrossRef]
- Chavda, V.P.; Yao, Q.; Vora, L.K.; Apostolopoulos, V.; Patel, C.A.; Bezbaruah, R.; Patel, A.B.; Chen, Z.-S. Fast-Track Development of Vaccines for SARS-CoV-2: The Shots That Saved the World. Front. Immunol. 2022, 13, 961198. [Google Scholar] [CrossRef]
- Bolcato, M.; Trabucco Aurilio, M.; Di Mizio, G.; Piccioni, A.; Feola, A.; Bonsignore, A.; Tettamanti, C.; Ciliberti, R.; Rodriguez, D.; Aprile, A. The Difficult Balance between Ensuring the Right of Nursing Home Residents to Communication and Their Safety. Int. J. Environ. Res. Public Health 2021, 18, 2484. [Google Scholar] [CrossRef] [PubMed]
- Chavda, V.P.; Chen, Y.; Dave, J.; Chen, Z.-S.; Chauhan, S.C.; Yallapu, M.M.; Uversky, V.N.; Bezbaruah, R.; Patel, S.; Apostolopoulos, V. COVID-19 and Vaccination: Myths vs Science. Expert Rev. Vaccines 2022, 21, 1603–1620. [Google Scholar] [CrossRef] [PubMed]
- Chavda, V.P.; Feehan, J.; Apostolopoulos, V. A Veterinary Vaccine for SARS-CoV-2: The First COVID-19 Vaccine for Animals. Vaccines 2021, 9, 631. [Google Scholar] [CrossRef]
- Ga, E.; Won, Y.; Hwang, J.; Moon, S.; Yeom, M.; Lyoo, K.; Song, D.; Han, J.; Na, W. A COVID-19 Vaccine for Dogs Prevents Reverse Zoonosis. Vaccines 2022, 10, 676. [Google Scholar] [CrossRef]
- Ni, W.; Yang, X.; Yang, D.; Bao, J.; Li, R.; Xiao, Y.; Hou, C.; Wang, H.; Liu, J.; Yang, D.; et al. Role of Angiotensin-Converting Enzyme 2 (ACE2) in COVID-19. Crit. Care 2020, 24, 422. [Google Scholar] [CrossRef]
- Chavda, V.P.; Prajapati, R.; Lathigara, D.; Nagar, B.; Kukadiya, J.; Redwan, E.M.; Uversky, V.N.; Kher, M.N.; Patel, R. Therapeutic Monoclonal Antibodies for COVID-19 Management: An Update. Expert Opin. Biol. Ther. 2022, 22, 763–780. [Google Scholar] [CrossRef]
- Shao, W.; Zhang, W.; Fang, X.; Yu, D.; Wang, X. Challenges of SARS-CoV-2 Omicron Variant and Appropriate Countermeasures. J. Microbiol. Immunol. Infect. 2022, 55, 387–394. [Google Scholar] [CrossRef]
- Starr, T.N.; Greaney, A.J.; Dingens, A.S.; Bloom, J.D. Complete Map of SARS-CoV-2 RBD Mutations That Escape the Monoclonal Antibody LY-CoV555 and Its Cocktail with LY-CoV016. Cell Rep. Med. 2021, 2, 100255. [Google Scholar] [CrossRef]
- Metzger, C.M.J.A.; Lienhard, R.; Seth-Smith, H.M.B.; Roloff, T.; Wegner, F.; Sieber, J.; Bel, M.; Greub, G.; Egli, A. PCR Performance in the SARS-CoV-2 Omicron Variant of Concern? Swiss Med. Wkly. 2021, 151, w30120. [Google Scholar] [CrossRef]
- Chen, J.; Wang, R.; Gilby, N.B.; Wei, G.-W. Omicron Variant (B.1.1.529): Infectivity, Vaccine Breakthrough, and Antibody Resistance. J. Chem. Inf. Model. 2022, 62, 412–422. [Google Scholar] [CrossRef]
- Yu, J.; Collier, A.Y.; Rowe, M.; Mardas, F.; Ventura, J.D.; Wan, H.; Miller, J.; Powers, O.; Chung, B.; Siamatu, M.; et al. Neutralization of the SARS-CoV-2 Omicron BA.1 and BA.2 Variants. N. Engl. J. Med. 2022, 386, 1579–1580. [Google Scholar] [CrossRef]
- Yamasoba, D.; Kimura, I.; Nasser, H.; Morioka, Y.; Nao, N.; Ito, J.; Uriu, K.; Tsuda, M.; Zahradnik, J.; Shirakawa, K.; et al. Virological Characteristics of SARS-CoV-2 BA.2 Variant. bioRxiv 2022. [Google Scholar] [CrossRef]
- Omicron Subvariants BA.4 and BA.5 in India: Symptoms, Severity, Medtalks. Available online: https://www.medtalks.in/articles/omicron-subvariants-ba-4-and-b-a-5-in-india (accessed on 11 November 2022).
- Dhawan, M.; Saied, A.A.; Emran, T.B.; Choudhary, O.P. Emergence of Omicron Variant’s Sublineages BA.4 and BA.5: Risks Assessment and Possible Countermeasures. New Microbes New Infect. 2022, 48, 100997. [Google Scholar] [CrossRef]
- Aggarwal, A.; Akerman, A.; Milogiannakis, V.; Silva, M.R.; Walker, G.; Stella, A.O.; Kindinger, A.; Angelovich, T.; Waring, E.; Amatayakul-Chantler, S.; et al. SARS-CoV-2 Omicron BA.5: Evolving Tropism and Evasion of Potent Humoral Responses and Resistance to Clinical Immunotherapeutics Relative to Viral Variants of Concern. EBioMedicine 2022, 84, 104270. [Google Scholar] [CrossRef] [PubMed]
- Outbreak.Info SARS-CoV-2 Data Explorer. Available online: https://outbreak.info/ (accessed on 27 November 2022).
- Zappa, M.; Verdecchia, P.; Angeli, F. Knowing the New Omicron BA.2.75 Variant (‘Centaurus’): A Simulation Study. Eur. J. Internal Med. 2022, 105, 7–108. [Google Scholar] [CrossRef] [PubMed]
- Karyakarte, R.; Das, R.; Taji, N.; Yanamandra, S.; Shende, S.; Joshi, S.; Karekar, B.; Bawale, R.; Tiwari, R.; Jadhav, M.; et al. An Early and Preliminary Assessment of the Clinical Severity of the Emerging SARS-CoV-2 Omicron Variants in Maharashtra, India. Cureus 2022, 14, e31352. [Google Scholar] [CrossRef] [PubMed]
- Omicron Subvariant—BA.2.75. Narayana Health Care. 2022. Available online: https://www.narayanahealth.org/blog/omicron-subvariant-ba-2-75/ (accessed on 8 December 2022).
- Wang, P.; Nair, M.S.; Liu, L.; Iketani, S.; Luo, Y.; Guo, Y.; Wang, M.; Yu, J.; Zhang, B.; Kwong, P.D.; et al. Antibody Resistance of SARS-CoV-2 Variants B.1.351 and B.1.1.7. Nature 2021, 593, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Anatomy of Omicron BA.1 and BA.2 Neutralizing Antibodies in COVID-19 MRNA Vaccinees. Nature Communications. Available online: https://www.nature.com/articles/s41467-022-31115-8 (accessed on 24 November 2022).
- Sharma, V.; Rai, H.; Gautam, D.N.S.; Prajapati, P.K.; Sharma, R. Emerging Evidence on Omicron (B.1.1.529) SARS-CoV-2 Variant. J. Med. Virol. 2022, I94, 1876–1885. Available online: https://onlinelibrary.wiley.com/doi/10.1002/jmv.27626 (accessed on 24 November 2022). [CrossRef] [PubMed]
- Cheng, S.M.S.; Mok, C.K.P.; Leung, Y.W.Y.; Ng, S.S.; Chan, K.C.K.; Ko, F.W.; Chen, C.; Yiu, K.; Lam, B.H.S.; Lau, E.H.Y.; et al. Neutralizing Antibodies against the SARS-CoV-2 Omicron Variant BA.1 Following Homologous and Heterologous CoronaVac or BNT162b2 Vaccination. Nat. Med. 2022, 28, 486–489. [Google Scholar] [CrossRef] [PubMed]
- Strasser, Z.H.; Greifer, N.; Hadavand, A.; Murphy, S.N.; Estiri, H. Estimates of SARS-CoV-2 Omicron BA.2 Subvariant Severity in New England. JAMA Netw. Open 2022, 5, e2238354. [Google Scholar] [CrossRef] [PubMed]
- Omicron Infection Is a Poor Booster of COVID-19 Immunity | Imperial News | Imperial College London. Available online: https://www.imperial.ac.uk/news/237315/omicron-infection-poor-booster-covid-19-immunity/ (accessed on 24 November 2022).
- Evans, J.P.; Qu, P.; Zeng, C.; Zheng, Y.-M.; Carlin, C.; Bednash, J.S.; Lozanski, G.; Mallampalli, R.K.; Saif, L.J.; Oltz, E.M.; et al. Neutralization of the SARS-CoV-2 Deltacron and BA.3 Variants. N. Engl. J. Med. 2022, 386, 2340–2342. [Google Scholar] [CrossRef] [PubMed]
- What Omicron’s BA.4 and BA.5 Variants Mean for the Pandemic. Available online: https://www.nature.com/articles/d41586-022-01730-y (accessed on 24 November 2022).
- Chalkias, S.; Harper, C.; Vrbicky, K.; Walsh, S.R.; Essink, B.; Brosz, A.; McGhee, N.; Tomassini, J.E.; Chen, X.; Chang, Y.; et al. A Bivalent Omicron-Containing Booster Vaccine against COVID-19. N. Engl. J. Med. 2022, 387, 1279–1291. [Google Scholar] [CrossRef]
- Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 9 December 2022).
- SARS-CoV-2 Variants of Concern and Variants under Investigation. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1115071/Technical-Briefing-45-9September2022.pdf (accessed on 8 December 2022).
- How Dangerous Is the Delta Variant (B.1.617.2)? Available online: https://asm.org/Articles/2021/July/How-Dangerous-is-the-Delta-Variant-B-1-617-2 (accessed on 9 December 2022).
- Arora, P.; Kempf, A.; Nehlmeier, I.; Graichen, L.; Sidarovich, A.; Winkler, M.S.; Schulz, S.; Jäck, H.-M.; Stankov, M.V.; Behrens, G.M.N.; et al. Delta Variant (B.1.617.2) Sublineages Do Not Show Increased Neutralization Resistance. Cell Mol. Immunol. 2021, 18, 2557–2559. [Google Scholar] [CrossRef]
- Rahman, F.I.; Ether, S.A.; Islam, M.R. The “Delta Plus” COVID-19 Variant Has Evolved to Become the next Potential Variant of Concern: Mutation History and Measures of Prevention. J. Basic Clin. Physiol. Pharm. 2021, 33, 109–112. [Google Scholar] [CrossRef]
- Kumar, S.; Thambiraja, T.S.; Karuppanan, K.; Subramaniam, G. Omicron and Delta Variant of SARS-CoV-2: A Comparative Computational Study of Spike Protein. J. Med. Virol. 2022, 94, 1641–1649. [Google Scholar] [CrossRef]
- Planas, D.; Veyer, D.; Baidaliuk, A.; Staropoli, I.; Guivel-Benhassine, F.; Rajah, M.M.; Planchais, C.; Porrot, F.; Robillard, N.; Puech, J.; et al. Reduced Sensitivity of SARS-CoV-2 Variant Delta to Antibody Neutralization. Nature 2021, 596, 276–280. [Google Scholar] [CrossRef]
- Kannan, S.R.; Spratt, A.N.; Cohen, A.R.; Naqvi, S.H.; Chand, H.S.; Quinn, T.P.; Lorson, C.L.; Byrareddy, S.N.; Singh, K. Evolutionary Analysis of the Delta and Delta Plus Variants of the SARS-CoV-2 Viruses. J. Autoimmun. 2021, 124, 102715. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Delta Variant: 8 Things You Should Know about This COVID-19 Strain. UC Davis Health. Available online: https://health.ucdavis.edu/coronavirus/covid-19-information/delta-variant (accessed on 9 December 2022).
- Tellez, D.; Dayal, S.; Phan, P.; Mawley, A.; Shah, K.; Consunji, G.; Tellez, C.; Ruiz, K.; Sabnis, R.; Dayal, S.; et al. Analysis of COVID-19 on Diagnosis, Vaccine, Treatment, and Pathogenesis with Clinical Scenarios. Clin. Pract. 2021, 11, 309–321. [Google Scholar] [CrossRef]
- Doukky, R.; Mangla, A.; Ibrahim, Z.; Poulin, M.-F.; Avery, E.; Collado, F.M.; Kaplan, J.; Richardson, D.; Powell, L.H. Impact of Physical Inactivity on Mortality in Patients with Heart Failure. Am. J. Cardiol. 2016, 117, 1135–1146. [Google Scholar] [CrossRef]
- Yang, W.; Shaman, J. COVID-19 Pandemic Dynamics in India, the SARS-CoV-2 Delta Variant, and Implications for Vaccination. J. R. Soc. Interface 2021, 19, 20210900. [Google Scholar] [CrossRef] [PubMed]
- Torjesen, I. COVID-19: Delta Variant Is Now UK’s Most Dominant Strain and Spreading through Schools. BMJ 2021, 373, n1445. [Google Scholar] [CrossRef] [PubMed]
- Viral Infection and Transmission in a Large, Well-Traced Outbreak Caused by the SARS-CoV-2 Delta Variant, MedRxiv. Available online: https://www.medrxiv.org/content/10.1101/2021.07.07.21260122v2 (accessed on 9 December 2022).
- World Health Organization (WHO). Available online: https://www.who.int (accessed on 9 December 2022).
- India COVID—Coronavirus Statistics-Worldometer. Available online: https://www.worldometers.info/coronavirus/country/india/ (accessed on 9 December 2022).
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing Antibody Levels Are Highly Predictive of Immune Protection from Symptomatic SARS-CoV-2 Infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Eurosurveillance. Increased Transmissibility and Global Spread of SARS-CoV-2 Variants of Concern as at June 2021. Available online: https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2021.26.24.2100509 (accessed on 9 December 2022).
- Vöhringer, H.S.; Sanderson, T.; Sinnott, M.; De Maio, N.; Nguyen, T.; Goater, R.; Schwach, F.; Harrison, I.; Hellewell, J.; Ariani, C.V.; et al. Genomic Reconstruction of the SARS-CoV-2 Epidemic in England. Nature 2021, 600, 506–511. [Google Scholar] [CrossRef]
- Murhekar, M.V.; Bhatnagar, T.; Thangaraj, J.W.V.; Saravanakumar, V.; Kumar, M.S.; Selvaraju, S.; Rade, K.; Kumar, C.P.G.; Sabarinathan, R.; Turuk, A.; et al. SARS-CoV-2 Seroprevalence among the General Population and Healthcare Workers in India, December 2020–January 2021. Int. J. Infect. Dis. 2021, 108, 145–155. [Google Scholar] [CrossRef]
- Genome Sequencing by INSACOG Shows Variants of Concern and a Novel Variant in India. Available online: https://pib.gov.in/Pressreleaseshare.aspx?PRID=1707177 (accessed on 9 December 2022).
- Lessons from SARS-CoV-2 in India: A Data-Driven Framework for Pandemic Resilience. Science Advances. Available online: https://www.science.org/doi/10.1126/sciadv.abp8621 (accessed on 9 December 2022).
- Sanches, P.R.S.; Charlie-Silva, I.; Braz, H.L.B.; Bittar, C.; Freitas Calmon, M.; Rahal, P.; Cilli, E.M. Recent Advances in SARS-CoV-2 Spike Protein and RBD Mutations Comparison between New Variants Alpha (B.1.1.7, United Kingdom), Beta (B.1.351, South Africa), Gamma (P.1, Brazil) and Delta (B.1.617.2, India). J. Virus Erad. 2021, 7, 100054. [Google Scholar] [CrossRef]
- Zhang, L.; Li, Q.; Liang, Z.; Li, T.; Liu, S.; Cui, Q.; Nie, J.; Wu, Q.; Qu, X.; Huang, W.; et al. The Significant Immune Escape of Pseudotyped SARS-CoV-2 Variant Omicron. Emerg. Microbes Infect. 2022, 11, 1–5. [Google Scholar] [CrossRef]
- India’s First Omicron Cases Detected in Karnataka. Available online: https://www.hindustantimes.com/india-news/indias-first-omicron-cases-detected-in-karnataka-101638445884205.html (accessed on 9 December 2022).
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 Vaccine Acceptance and Hesitancy in Low- and Middle-Income Countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- CDC Coronavirus Disease 2019 (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/index.html (accessed on 9 December 2022).
- Ettaboina, S.K.; Nakkala, K.; Laddha, K.S. A Mini Review on SARS-CoV-19-2 Omicron Variant (B. 1.1. 529). SciMedicine J. 2021, 3, 399–406. [Google Scholar] [CrossRef]
- Livemint Omicron Was Less Severe in India Because of These 2 Reasons, Finds Study. Available online: https://www.livemint.com/science/health/omicron-was-less-severe-in-india-because-of-these-2-reasons-finds-study-read-here-11644411033886.html (accessed on 9 December 2022).
- Zhang, X.; Wu, S.; Wu, B.; Yang, Q.; Chen, A.; Li, Y.; Zhang, Y.; Pan, T.; Zhang, H.; He, X. SARS-CoV-2 Omicron Strain Exhibits Potent Capabilities for Immune Evasion and Viral Entrance. Signal Transduct. Target. 2021, 6, 430. [Google Scholar] [CrossRef]
- Delhi: Genome Sequencing Reveals Omicron Variant in 38% Samples from City. Available online: https://www.indiatoday.in/coronavirus-outbreak/story/delhi-genome-sequencing-omicron-variant-in-samples-1893918-2021-12-29 (accessed on 9 December 2022).
- India News, Omicron Found in Delhi’s 65% Samples Whose Genome Sequencing Report Came out Between Jan 1 and 3, LatestLY. Available online: https://www.latestly.com/agency-news/india-news-omicron-found-in-delhis-65-samples-whose-genome-sequencing-report-came-out-between-jan-1-and-3-3225440.html (accessed on 9 December 2022).
- Mumbai’s Sixth Genome Sequencing: Omicron Found in 2 per Cent Samples. Available online: https://www.mid-day.com/mumbai/mumbai-news/article/mumbais-sixth-genome-sequencing-omicron-found-in-2-per-cent-samples-23205256 (accessed on 9 December 2022).
- Genome Sequencing Shows Omicron Variant Predominant Strain in COVID Cases in Mumbai. Cities News, The Indian Express. Available online: https://indianexpress.com/article/cities/mumbai/mumbai-genome-sequencing-omicron-variant-covid-19-7800080/ (accessed on 9 December 2022).
- INSACOG. Department of Biotechnology. Available online: https://dbtindia.gov.in/insacog (accessed on 9 December 2022).
- Asrani, P.; Tiwari, K.; Eapen, M.S.; Hassan, M.D.I.; Sohal, S.S. Containment Strategies for COVID-19 in India: Lessons from the Second Wave. Expert Rev. Anti-Infect. Ther. 2022, 20, 829–835. [Google Scholar] [CrossRef]
- Ghosh, N.; Saha, I.; Sarkar, J.P.; Maulik, U. Strategies for COVID-19 Epidemiological Surveillance in India: Overall Policies Till June 2021. Front. Public Health 2021, 9, 708224. [Google Scholar] [CrossRef]
- Banerjee, D.; Viswanath, B. Neuropsychiatric Manifestations of COVID-19 and Possible Pathogenic Mechanisms: Insights from Other Coronaviruses. Asian J. Psychiatr. 2020, 54, 102350. [Google Scholar] [CrossRef]
- Archive - Diagnostic Kit Evaluation. Available online: https://www.icmr.gov.in/arcckitevaluation.html (accessed on 9 December 2022).
- Bazargan, M.; Elahi, R.; Esmaeilzadeh, A. OMICRON: Virology, Immunopathogenesis, and Laboratory Diagnosis. J. Gene Med. 2022, 24, e3435. [Google Scholar] [CrossRef]
- Tahmasebi, S.; Khosh, E.; Esmaeilzadeh, A. The Outlook for Diagnostic Purposes of the 2019-novel Coronavirus Disease. J. Cell Physiol. 2020, 235, 9211–9229. [Google Scholar] [CrossRef] [PubMed]
- Alpdagtas, S.; Ilhan, E.; Uysal, E.; Sengor, M.; Ustundag, C.B.; Gunduz, O. Evaluation of Current Diagnostic Methods for COVID-19. APL Bioeng. 2020, 4, 041506. [Google Scholar] [CrossRef] [PubMed]
- Tsang, N.N.Y.; So, H.C.; Ng, K.Y.; Cowling, B.J.; Leung, G.M.; Ip, D.K.M. Diagnostic Performance of Different Sampling Approaches for SARS-CoV-2 RT-PCR Testing: A Systematic Review and Meta-Analysis. Lancet Infect. Dis. 2021, 21, 1233–1245. [Google Scholar] [CrossRef]
- Tahan, S.; Parikh, B.A.; Droit, L.; Wallace, M.A.; Burnham, C.-A.D.; Wang, D. SARS-CoV-2 E Gene Variant Alters Analytical Sensitivity Characteristics of Viral Detection Using a Commercial Reverse Transcription-PCR Assay. J. Clin. Microbiol. 2021, 59, e0007521. [Google Scholar] [CrossRef]
- A Simple and Quick PCR Based Method for Detection of Omicron Variant of SARS-CoV-2 | MedRxiv. Available online: https://www.medrxiv.org/content/10.1101/2021.12.20.21268053v1.full (accessed on 9 December 2022).
- Broughton, J.P.; Deng, X.; Yu, G.; Fasching, C.L.; Servellita, V.; Singh, J.; Miao, X.; Streithorst, J.A.; Granados, A.; Sotomayor-Gonzalez, A.; et al. CRISPR-Cas12-Based Detection of SARS-CoV-2. Nat. Biotechnol. 2020, 38, 870–874. [Google Scholar] [CrossRef] [PubMed]
- Shihong Gao, D.; Zhu, X.; Lu, B. Development and Application of Sensitive, Specific, and Rapid CRISPR-Cas13-Based Diagnosis. J. Med. Virol. 2021, 93, 4198–4204. [Google Scholar] [CrossRef]
- Fernandes, Q.; Inchakalody, V.P.; Merhi, M.; Mestiri, S.; Taib, N.; Moustafa Abo El-Ella, D.; Bedhiafi, T.; Raza, A.; Al-Zaidan, L.; Mohsen, M.O.; et al. Emerging COVID-19 Variants and Their Impact on SARS-CoV-2 Diagnosis, Therapeutics and Vaccines. Ann. Med. 2022, 54, 524–540. [Google Scholar] [CrossRef] [PubMed]
- Falzone, L.; Gattuso, G.; Tsatsakis, A.; Spandidos, D.A.; Libra, M. Current and Innovative Methods for the Diagnosis of COVID-19 Infection (Review). Int. J. Mol. Med. 2021, 47, 100. [Google Scholar] [CrossRef] [PubMed]
- Di Domenico, M.; De Rosa, A.; Boccellino, M. Detection of SARS-CoV-2 Proteins Using an ELISA Test. Diagnostics 2021, 11, 698. [Google Scholar] [CrossRef] [PubMed]
- Edouard, S.; Jaafar, R.; Orain, N.; Parola, P.; Colson, P.; La Scola, B.; Fournier, P.-E.; Raoult, D.; Drancourt, M. Automated Western Immunoblotting Detection of Anti-SARS-CoV-2 Serum Antibodies. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 1309–1317. [Google Scholar] [CrossRef]
- Wratil, P.R.; Stern, M.; Priller, A.; Willmann, A.; Almanzar, G.; Vogel, E.; Feuerherd, M.; Cheng, C.-C.; Yazici, S.; Christa, C.; et al. Three Exposures to the Spike Protein of SARS-CoV-2 by Either Infection or Vaccination Elicit Superior Neutralizing Immunity to All Variants of Concern. Nat. Med. 2022, 28. [Google Scholar] [CrossRef]
- Callaway, E. Omicron Likely to Weaken COVID Vaccine Protection. Nature 2021, 600, 367–368. [Google Scholar] [CrossRef]
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early Remdesivir to Prevent Progression to Severe COVID-19 in Outpatients. N. Engl. J. Med. 2022, 386, 305–315. [Google Scholar] [CrossRef]
- Rosas, I.O.; Bräu, N.; Waters, M.; Go, R.C.; Hunter, B.D.; Bhagani, S.; Skiest, D.; Aziz, M.S.; Cooper, N.; Douglas, I.S.; et al. Tocilizumab in Hospitalized Patients with Severe COVID-19 Pneumonia. N. Engl. J. Med. 2021, 384, 1503–1516. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug. Coronavirus (COVID-19) Update: FDA Limits Use of Certain Monoclonal Antibodies to Treat COVID-19 Due to the Omicron Variant. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-limits-use-certain-monoclonal-antibodies-treat-covid-19-due-omicron (accessed on 9 December 2022).
- Dougan, M.; Nirula, A.; Azizad, M.; Mocherla, B.; Gottlieb, R.L.; Chen, P.; Hebert, C.; Perry, R.; Boscia, J.; Heller, B.; et al. Bamlanivimab plus Etesevimab in Mild or Moderate COVID-19. N. Engl. J. Med. 2021, 385, 1382–1392. [Google Scholar] [CrossRef] [PubMed]
- Razonable, R.R.; Pawlowski, C.; O’Horo, J.C.; Arndt, L.L.; Arndt, R.; Bierle, D.M.; Borgen, M.D.; Hanson, S.N.; Hedin, M.C.; Lenehan, P.; et al. Casirivimab-Imdevimab Treatment Is Associated with Reduced Rates of Hospitalization among High-Risk Patients with Mild to Moderate Coronavirus Disease-19. EClinicalMedicine 2021, 40, 101102. [Google Scholar] [CrossRef]
- Sah, R.; Shrestha, S.; Mehta, R.; Sah, S.K.; Rabaan, A.A.; Dhama, K.; Rodriguez-Morales, A.J. AZD1222 (Covishield) Vaccination for COVID-19: Experiences, Challenges, and Solutions in Nepal. Travel. Med. Infect. Dis. 2021, 40, 101989. [Google Scholar] [CrossRef] [PubMed]
- Bharat Biotech-Vaccines & Bio-Therapeutics Manufacturer in India. Available online: https://www.bharatbiotech.com/ (accessed on 9 December 2022).
- Kuehn, B.M. New COVID-19 Vaccine Aims to Increase Global Vaccine Access. JAMA 2022, 327, 614. [Google Scholar] [CrossRef] [PubMed]
- Dey, A.; Chozhavel Rajanathan, T.M.; Chandra, H.; Pericherla, H.P.R.; Kumar, S.; Choonia, H.S.; Bajpai, M.; Singh, A.K.; Sinha, A.; Saini, G.; et al. Immunogenic Potential of DNA Vaccine Candidate, ZyCoV-D against SARS-CoV-2 in Animal Models. Vaccine 2021, 39, 4108–4116. [Google Scholar] [CrossRef] [PubMed]
- Safety and Immunogenicity of a DNA SARS-CoV-2 Vaccine (ZyCoV-D): Results of an Open-Label, Non-Randomized Phase I Part of Phase I/II Clinical Study by Intradermal Route in Healthy Subjects in India-EClinicalMedicine. Available online: https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(21)00300-X/fulltext (accessed on 9 December 2022).
- Montalti, M.; Soldà, G.; Di Valerio, Z.; Salussolia, A.; Lenzi, J.; Forcellini, M.; Barvas, E.; Guttmann, S.; Messina, R.; Poluzzi, E.; et al. ROCCA Observational Study: Early Results on Safety of Sputnik V Vaccine (Gam-COVID-Vac) in the Republic of San Marino Using Active Surveillance. EClinicalMedicine 2021, 38, 101027. [Google Scholar] [CrossRef]
- Rossi, A.H.; Ojeda, D.S.; Varese, A.; Sanchez, L.; Gonzalez Lopez Ledesma, M.M.; Mazzitelli, I.; Alvarez Juliá, A.; Oviedo Rouco, S.; Pallarés, H.M.; Costa Navarro, G.S.; et al. Sputnik V Vaccine Elicits Seroconversion and Neutralizing Capacity to SARS-CoV-2 after a Single Dose. Cell Rep. Med. 2021, 2, 100359. [Google Scholar] [CrossRef]
- Al-Tawfiq, J.A.; Koritala, T.; Alhumaid, S.; Barry, M.; Alshukairi, A.N.; Temsah, M.-H.; Al Mutair, A.; Rabaan, A.; Tirupathi, R.; Gautret, P. Implication of the Emergence of the Delta (B.1.617.2) Variants on Vaccine Effectiveness. Infection 2022, 50, 583–596. [Google Scholar] [CrossRef]
- Inder, D.; Manak, S.; Akram, M.F.; Kumar, P. Recent Update on Treatment and Preventive Modalities for COVID-19 Omicron Variant (B.1.1.529) in India: A Comprehensive Review. Saudi J. Health Sci. 2022, 11, 83. [Google Scholar] [CrossRef]
- Meenakshi, S.; Kumar, V.U.; Dhingra, S.; Murti, K. Nasal Vaccine as a Booster Shot: A Viable Solution to Restrict Pandemic? Clin. Exp. Vaccine Res. 2022, 11, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Gowrisankar, A.; Priyanka, T.M.C.; Banerjee, S. Omicron: A Mysterious Variant of Concern. Eur. Phys. J. Plus. 2022, 137, 100. [Google Scholar] [CrossRef]
- Thakur, V.; Ratho, R.K. OMICRON (B.1.1.529): A New SARS-CoV-2 Variant of Concern Mounting Worldwide Fear. J. Med. Virol. 2022, 94, 1821–1824. [Google Scholar] [CrossRef]
- COVID-19 Vaccine Effectiveness Against the Omicron (B.1.1.529) Variant, NEJM. Available online: https://www.nejm.org/doi/full/10.1056/NEJMoa2119451 (accessed on 9 December 2022).
- Oxford/AstraZeneca: Vaxzevria–COVID19 Vaccine Tracker. Available online: https://covid19.trackvaccines.org/vaccines/4/ (accessed on 9 December 2022).
- More Than 12.7 Billion Shots Given: COVID-19 Vaccine Tracker. Available online: https://www.bloomberg.com/graphics/covid-vaccine-tracker-global-distribution/ (accessed on 9 December 2022).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 MRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- The Pfizer BioNTech (BNT162b2) COVID-19 Vaccine: What You Need to Know. Available online: https://www.who.int/news-room/feature-stories/detail/who-can-take-the-pfizer-biontech-covid-19--vaccine-what-you-need-to-know (accessed on 9 December 2022).
- Serum Institute of India. ChAdOx1 NCoV-19 Corona Virus Vaccine (Recombinant)-COVISHIELD. Available online: https://www.seruminstitute.com/product_covishield.php (accessed on 9 December 2022).
- Ghosh, S.; Shankar, S.; Chatterjee, K.; Chatterjee, K.; Yadav, A.K.; Pandya, K.; Suryam, V.; Agrawal, S.; Ray, S.; Phutane, V.; et al. COVISHIELD (AZD1222) VaccINe Effectiveness among Healthcare and Frontline Workers of INdian Armed Forces: Interim Results of VIN-WIN Cohort Study. Med. J. Armed India 2021, 77, S264–S270. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug. Moderna COVID-19 Vaccines. FDA. 2022. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/moderna-covid-19-vaccines (accessed on 8 December 2022).
- The Moderna COVID-19 (MRNA-1273) Vaccine: What You Need to Know. Available online: https://www.who.int/news-room/feature-stories/detail/the-moderna-covid-19-mrna-1273-vaccine-what-you-need-to-know (accessed on 9 December 2022).
- Tartof, S.Y.; Slezak, J.M.; Puzniak, L.; Hong, V.; Frankland, T.B.; Ackerson, B.K.; Takhar, H.; Ogun, O.A.; Simmons, S.; Zamparo, J.M.; et al. BNT162b2 Vaccine Effectiveness against SARS-CoV-2 Omicron BA.4 and BA.5. Lancet Infect. Dis. 2022, 22, 1663–1665. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. Effectiveness of COVID-19 Vaccines against the Omicron (B.1.1.529) Variant of Concern. medRxiv 2021. [Google Scholar] [CrossRef]
- COVID-19 Vaccine Tracker and Landscape. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 9 December 2022).
- Trabucco Aurilio, M.; Mennini, F.S.; Gazzillo, S.; Massini, L.; Bolcato, M.; Feola, A.; Ferrari, C.; Coppeta, L. Intention to Be Vaccinated for COVID-19 among Italian Nurses during the Pandemic. Vaccines 2021, 9, 500. [Google Scholar] [CrossRef]
- Dhalaria, P.; Arora, H.; Singh, A.K.; Mathur, M.; S., A.K. COVID-19 Vaccine Hesitancy and Vaccination Coverage in India: An Exploratory Analysis. Vaccines 2022, 10, 739. [Google Scholar] [CrossRef]
- Wouters, O.J.; Shadlen, K.C.; Salcher-Konrad, M.; Pollard, A.J.; Larson, H.J.; Teerawattananon, Y.; Jit, M. Challenges in Ensuring Global Access to COVID-19 Vaccines: Production, Affordability, Allocation, and Deployment. Lancet 2021, 397, 1023–1034. [Google Scholar] [CrossRef]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 Vaccine Acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Kreps, S.; Prasad, S.; Brownstein, J.S.; Hswen, Y.; Garibaldi, B.T.; Zhang, B.; Kriner, D.L. Factors Associated With US Adults’ Likelihood of Accepting COVID-19 Vaccination. JAMA Netw. Open. 2020, 3, e2025594. [Google Scholar] [CrossRef]
- Global Attitudes: COVID-19 Vaccines. Available online: https://www.ipsos.com/en-ro/global-attitudes-covid-19-vaccine-january-2021 (accessed on 9 December 2022).
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A Global Survey of Potential Acceptance of a COVID-19 Vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Overview of Public Health and Social Measures in the Context of COVID-19. Available online: https://www.who.int/publications-detail-redirect/overview-of-public-health-and-social-measures-in-the-context-of-covid-19 (accessed on 9 December 2022).
- Ong, S.W.X.; Young, B.E.; Lye, D.C. Lack of Detail in Population-Level Data Impedes Analysis of SARS-CoV-2 Variants of Concern and Clinical Outcomes. Lancet Infect. Dis. 2021, 21, 1195–1197. [Google Scholar] [CrossRef]
- Castañeda-Vasquez, D.E.; Ruiz-Padilla, J.P.; Botello-Hernandez, E. Vaccine Hesitancy Against SARS-CoV-2 in Health Personnel of Northeastern Mexico and Its Determinants. J. Occup. Environ. Med. 2021, 63, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Quarleri, J.; Galvan, V.; Delpino, M.V. Omicron Variant of the SARS-CoV-2: A Quest to Define the Consequences of Its High Mutational Load. GeroScience 2022, 44, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Omicron Symptoms: Here’s How They Differ from Other Variants. NBC Chicago. Available online: https://www.nbcchicago.com/news/local/omicron-symptoms-heres-how-they-differ-from-other-variants/2723960/ (accessed on 8 December 2022).
- CDCMMWR SARS-CoV-2 B.1.1.529 (Omicron) Variant—United States, December 1–8, 2021. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8675659/ (accessed on 8 December 2022).
- Sah, R.; Mohanty, A.; Siddiq, A.; Singh, P.; Abdelaal, A.; Alshahrani, N.Z.; Dhama, K. Monkeypox Reported in India–South East Asia Region: Health and Economic Challenges. Lancet Reg. Health Southeast Asia 2022, 4, 100063. [Google Scholar] [CrossRef] [PubMed]
- CDC Monkeypox in the U.S. Available online: https://www.cdc.gov/poxvirus/monkeypox/index.html (accessed on 31 October 2022).
- Guidelines for Management of Monkeypox Disease.Pdf. Available online: https://main.mohfw.gov.in/sites/default/files/Guidelines%20for%20Management%20of%20Monkeypox%20Disease.pdf (accessed on 8 December 2022).
- Johnson, P.L.F.; Bergstrom, C.T.; Regoes, R.R.; Longini, I.M.; Halloran, M.E.; Antia, R. Evolutionary Consequences of Delaying Intervention for Monkeypox. Lancet 2022, 400, 1191–1193. [Google Scholar] [CrossRef]
- Isidro, J.; Borges, V.; Pinto, M.; Sobral, D.; Santos, J.D.; Nunes, A.; Mixão, V.; Ferreira, R.; Santos, D.; Duarte, S.; et al. Addendum: Phylogenomic Characterization and Signs of Microevolution in the 2022 Multi-Country Outbreak of Monkeypox Virus. Nat. Med. 2022, 28, 2220–2221. [Google Scholar] [CrossRef] [PubMed]
- Pastula, D.M.; Tyler, K.L. An Overview of Monkeypox Virus and Its Neuroinvasive Potential. Ann. Neurol. 2022, 92, 527–531. [Google Scholar] [CrossRef] [PubMed]
- Head, J.R.; Collender, P.A.; Lewnard, J.A.; Skaff, N.K.; Li, L.; Cheng, Q.; Baker, J.M.; Li, C.; Chen, D.; Ohringer, A.; et al. Early Evidence of Inactivated Enterovirus 71 Vaccine Impact Against Hand, Foot, and Mouth Disease in a Major Center of Ongoing Transmission in China, 2011–2018: A Longitudinal Surveillance Study. Clin. Infect. Dis. 2020, 71, 3088–3095. [Google Scholar] [CrossRef] [PubMed]
- Thiagarajan, K. Reports of “Tomato Flu” Outbreak in India Are Not Due to New Virus, Say Doctors. BMJ 2022, 378, o2101. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.S.Y.; Yip, C.C.Y.; Lau, S.K.P.; Yuen, K.Y. Human Enterovirus 71 and Hand, Foot and Mouth Disease. Epidemiol. Infect. 2010, 138, 1071–1089. [Google Scholar] [CrossRef]
- Shervani, Z.; Bhardwaj, D.; Hasan, S.; Qazi, U.Y.; Purang, M.; Ibbrahim, A.; Vuyyuru, V.P.S.R.; Siddiquie, A.; Sherwani, A.; Khan, A.A.; et al. The Omicron Wave in India, Mumbai, and Delhi: Prevalence and Pathogenicity. Eur. J. Med. Health Sci. 2022, 4, 123–130. [Google Scholar] [CrossRef]
- Jezek, Z.; Grab, B.; Szczeniowski, M.; Paluku, K.M.; Mutombo, M. Clinico-Epidemiological Features of Monkeypox Patients with an Animal or Human Source of Infection. Bull. World Health Organ. 1988, 66, 459–464. [Google Scholar]
- Clinical Characteristics of Human Monkeypox, and Risk Factors for Severe Disease. Clinical Infectious Diseases. Oxford Academic. Available online: https://academic.oup.com/cid/article/41/12/1742/344953 (accessed on 27 November 2022).
- Taneja, P.; News, I.T. HFMD Cases Increase Rapidly in Kids; Know Causes, Symptoms, and Remedies from Dr. Neha Srivastava. Available online: https://www.indiatvnews.com/health/hfmd-cases-increase-rapidly-in-kids-know-causes-symptoms-and-remedies-from-dr-neha-srivastava-2022-10-03-813453 (accessed on 27 November 2022).
- Omicron Variant of COVID 19 - Symptoms, Treatment and Update. Available online: https://www.pacehospital.com/omicron-variant-of-covid-19 (accessed on 27 November 2022).
- Rizk, J.G.; Lippi, G.; Henry, B.M.; Forthal, D.N.; Rizk, Y. Prevention and Treatment of Monkeypox. Drugs 2022, 82, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Niaz, F.; Tariq, S.; Ali, S.M.; Memon, R.; Nashwan, A.J.; Ullah, I. Monkeypox Treatment: Is Tecovirimat the Answer? J. Infect. Public Health 2022, 15, 1297–1298. [Google Scholar] [CrossRef]
- Usefulness of Low-Level Laser for Control of Painful Stomatitis in Patients with Hand-Foot-and-Mouth Disease. Journal of Clinical Laser Medicine & Surgery. Available online: https://www.liebertpub.com/doi/abs/10.1089/104454703322650176 (accessed on 27 November 2022).
- Management of Hand Foot Mouth Disease (HFMD) in Health Care Settings. Available online: https://www.chp.gov.hk/files/pdf/sceifd_management_of_hfmd_in_health_care_settings.pdf (accessed on 8 December 2022).
- Adjei, S. Mortality Risk Among Patients Hospitalized Primarily for COVID-19 During the Omicron and Delta Variant Pandemic Periods—United States, April 2020–June 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1182–1189. [Google Scholar] [CrossRef]
- How Deadly Is Monkeypox? What Scientists Know. Available online: https://www.nature.com/articles/d41586-022-02931-1 (accessed on 28 November 2022).
- Qiu, J.; Yan, H.; Cheng, N.; Lu, X.; Hu, X.; Liang, L.; Xiao, Z.; Tan, L. The Clinical and Epidemiological Study of Children with Hand, Foot, and Mouth Disease in Hunan, China from 2013 to 2017. Sci. Rep. 2019, 9, 11662. [Google Scholar] [CrossRef]
- Rana, R.; Kant, R.; Huirem, R.S.; Bohra, D.; Ganguly, N.K. Omicron Variant: Current Insights and Future Directions. Microbiol. Res. 2022, 265, 127204. [Google Scholar] [CrossRef]
- Explained: Can a RT-PCR Test Detect Infection with Omicron Variant of COVID-19? Explained News, The Indian Express. Available online: https://indianexpress.com/article/explained/can-an-rt-pcr-test-detect-infection-with-omicron-7648176/ (accessed on 24 December 2022).
- Omicron BF.7: Cases of Highly Infectious Strain Rise in India; Experts on Symptoms, Precautions and Fresh Wave. Available online: https://www.hindustantimes.com/lifestyle/health/omicron-bf-7-cases-of-highly-infectious-strain-rise-in-india-experts-on-symptoms-precautions-and-fresh-wave-101671627215813.html (accessed on 24 December 2022).
- Chavda, V.P.; Vora, L.K.; Pandya, A.K.; Patravale, V.B. Intranasal Vaccines for SARS-CoV-2: From Challenges to Potential in COVID-19 Management. Drug Discov. Today 2021, 26, 2619–2636. [Google Scholar] [CrossRef] [PubMed]
- Chavda, V.P.; Vihol, D.R.; Solanki, H.K.; Apostolopoulos, V. The Vaccine World of COVID-19: India’s Contribution. Vaccines 2022, 10, 1943. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Sub Variant | Impact on Severity | Neutralizing Antibody | Reference |
|---|---|---|---|
| BA.1 | BA. 1 was involved with a lower risk of hospitalization and more severe illness than alpha, beta, and delta variants. | The two doses of BNT162B2 mRNA or coronaVac elicit low neutralizing antibodies in infected persons. However, homologous or heterologous booster doses of these two improve neutralizing antibodies level. 14.2% of the antibody panel, was capable to neutralize BA.1. Antibody germlines IGHV1-58, IGHJ3-1 and IGHV1-69, IGHJ4-1, were used in vaccine protection from BA.1 | [36,37,38] |
| BA.2 | BA.2 is less severe than BA.1, and the severity of the variant is decreased in patients with booster dose immunization. Data found that boosters provide 81% of protection against BA.2 Infection. | The neutralizing antibody resistance of BA.2_L452Q was stronger than BA.2_S704 L. 19.9% antibody panel was capable to neutralize BA.2 mAbs EvusheLd(cilagavimab and tixagevimab) can neutralize BA.2 more efficiently than BA.1 | [26,39,40] |
| BA.3 | BA.3 was less severe because there was no specific mutations had been observed in its spike protein. It was said changes were due to the combined mutation of BA.1 and BA.2. | Antibody titers against pseudotyped spike protein from ancestral SARS-CoV-2 bearing the D614G mutation. | [41] |
| BA.4 | The BA.4 subvariants increased severity Worldwide because they can spread faster than another variant, but it was less severe than BA.5. | Three doses of BNT162B2 or booster doses of coronaVac/BNT162B2 elicited detectable BA.4 neutralizing antibody responses BA.4 impact against high resistance of antibodies than the previous variant. However, BA.4 is more sensitive to sotrovimab than BA.2 | [42] |
| BA.5 | BA.5 variant had to be more transmissible and resistant to adaptive immunity. | BA.5 subvariant would be less susceptible to BNT162b2 or CoronaVac, nevertheless, three doses of BNT162b2 can neutralize antibodies. Same as BA.4, BA.5 4 is more sensitive to sotrovimab than BA.2 | [43] |
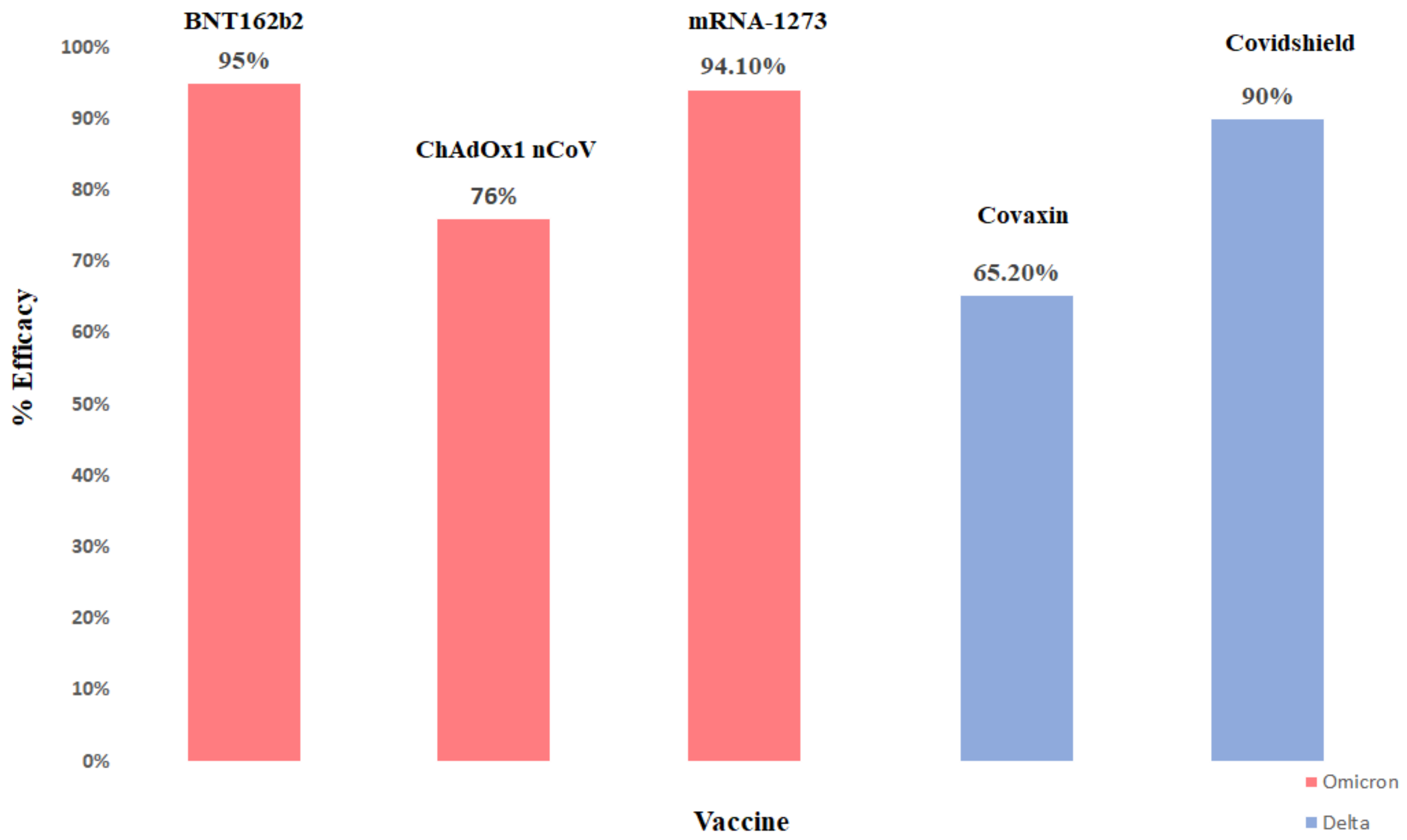
| Name of Vaccine | Route of Administration | Type of Vaccine | Efficacy | Status | Approval in How Many Countries | Ref. |
|---|---|---|---|---|---|---|
| BNT162b2 (Pfizer–BioNTech) | Intramuscular | mRNA | 95.0% | Approved | 149 | [117,118] |
| ChAdOx1 nCoV-19 (AstraZeneca) | Intramuscular | Non replicating viral vector | 76% | Approved | 149 | [119,120] |
| mRNA-1273 (Moderna) | Intramuscular | mRNA | 94.1% | Approved | 88 | [121,122] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chavda, V.P.; Balar, P.; Vaghela, D.; Solanki, H.K.; Vaishnav, A.; Hala, V.; Vora, L. Omicron Variant of SARS-CoV-2: An Indian Perspective of Vaccination and Management. Vaccines 2023, 11, 160. https://doi.org/10.3390/vaccines11010160
Chavda VP, Balar P, Vaghela D, Solanki HK, Vaishnav A, Hala V, Vora L. Omicron Variant of SARS-CoV-2: An Indian Perspective of Vaccination and Management. Vaccines. 2023; 11(1):160. https://doi.org/10.3390/vaccines11010160
Chicago/Turabian StyleChavda, Vivek P., Pankti Balar, Dixa Vaghela, Hetvi K. Solanki, Akta Vaishnav, Vivek Hala, and Lalitkumar Vora. 2023. "Omicron Variant of SARS-CoV-2: An Indian Perspective of Vaccination and Management" Vaccines 11, no. 1: 160. https://doi.org/10.3390/vaccines11010160
APA StyleChavda, V. P., Balar, P., Vaghela, D., Solanki, H. K., Vaishnav, A., Hala, V., & Vora, L. (2023). Omicron Variant of SARS-CoV-2: An Indian Perspective of Vaccination and Management. Vaccines, 11(1), 160. https://doi.org/10.3390/vaccines11010160