
Effectiveness of COVID-19 Vaccine Booster Shot Compared with Non-Booster: A Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Study Quality Assessment
2.4. Data Synthesis and Analysis
3. Results
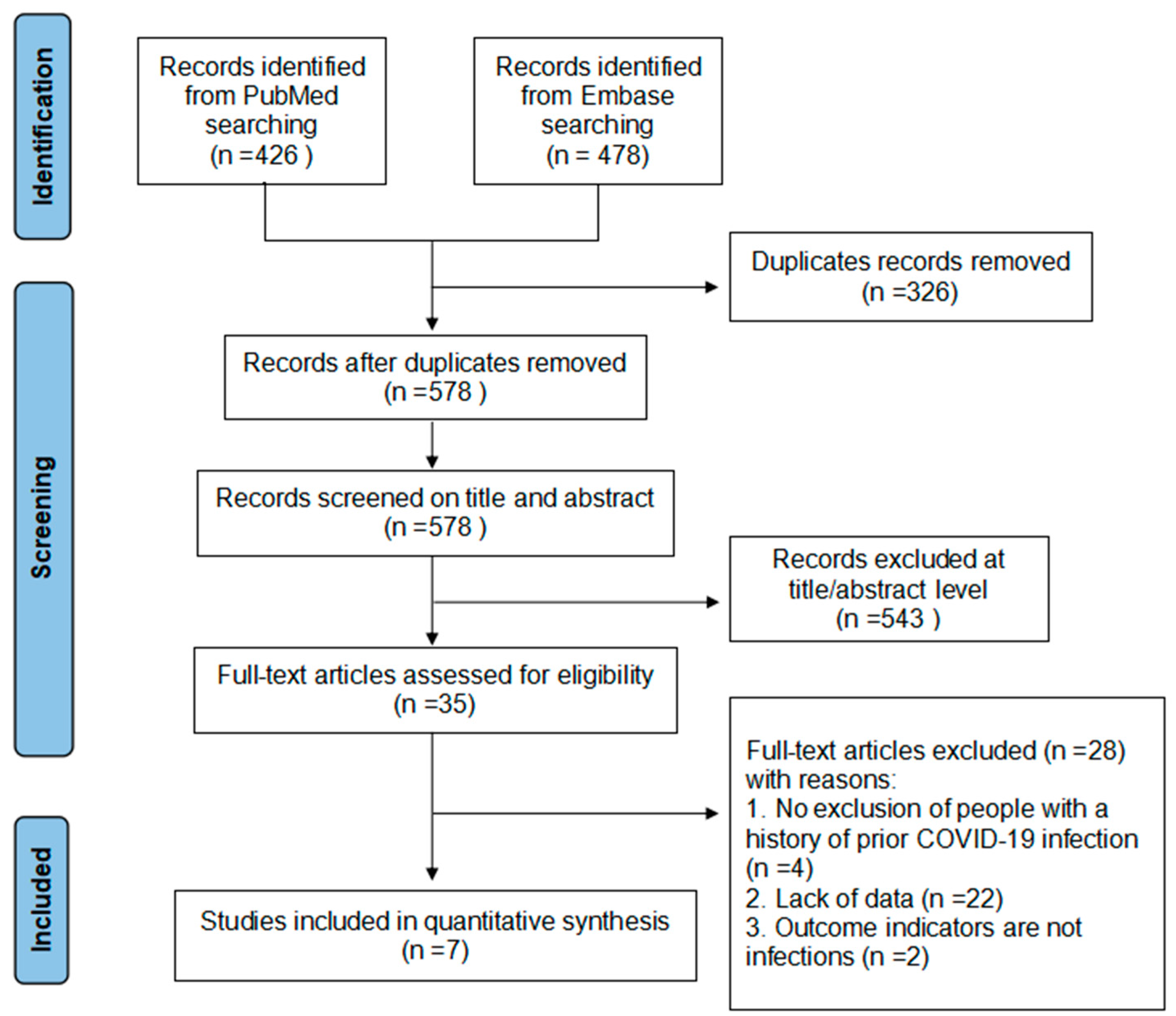
3.1. Literature Retrieval and Literature Quality Evaluation
3.2. Effectiveness of COVID-19 Vaccine Booster versus Non-Booster Doses
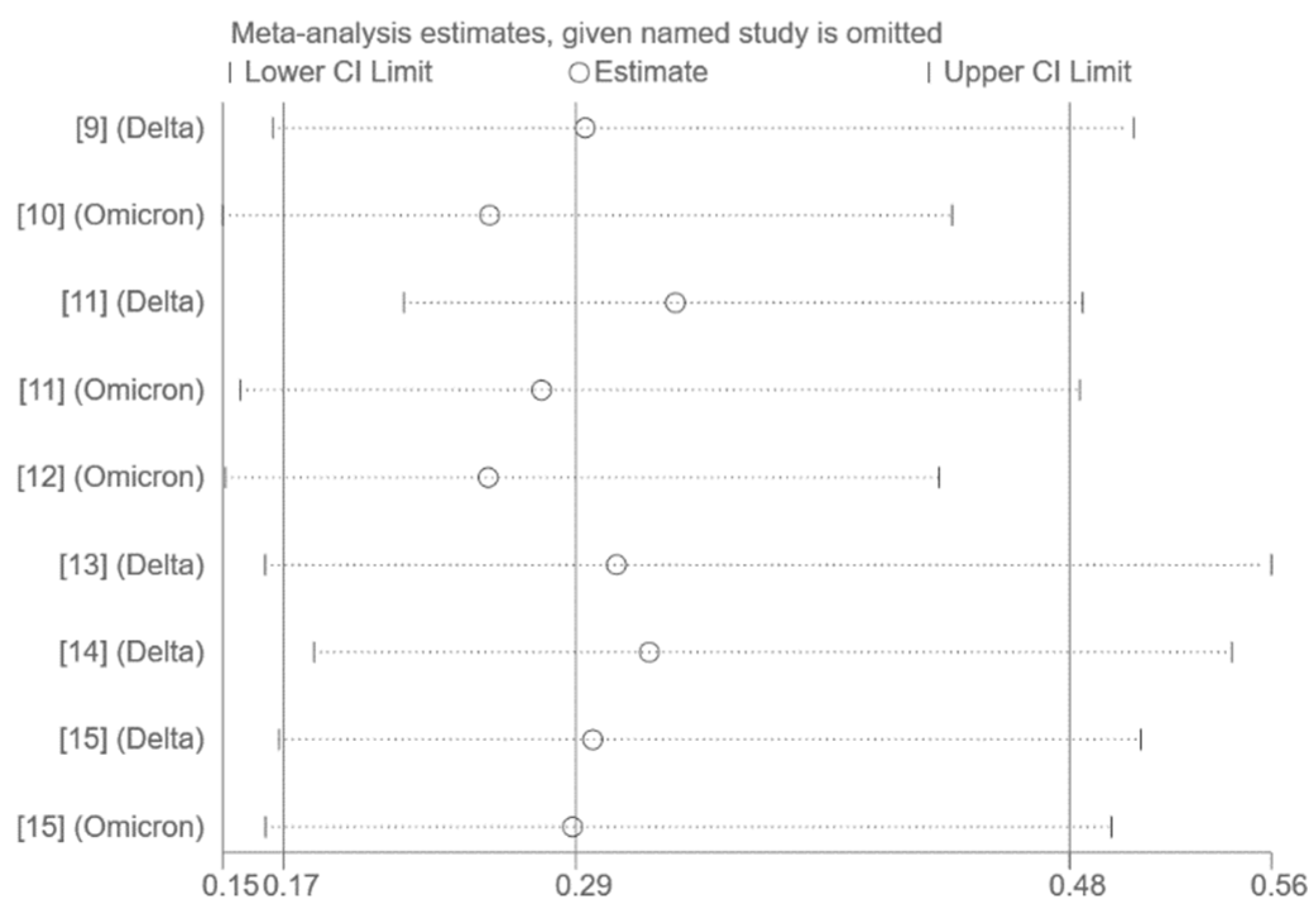
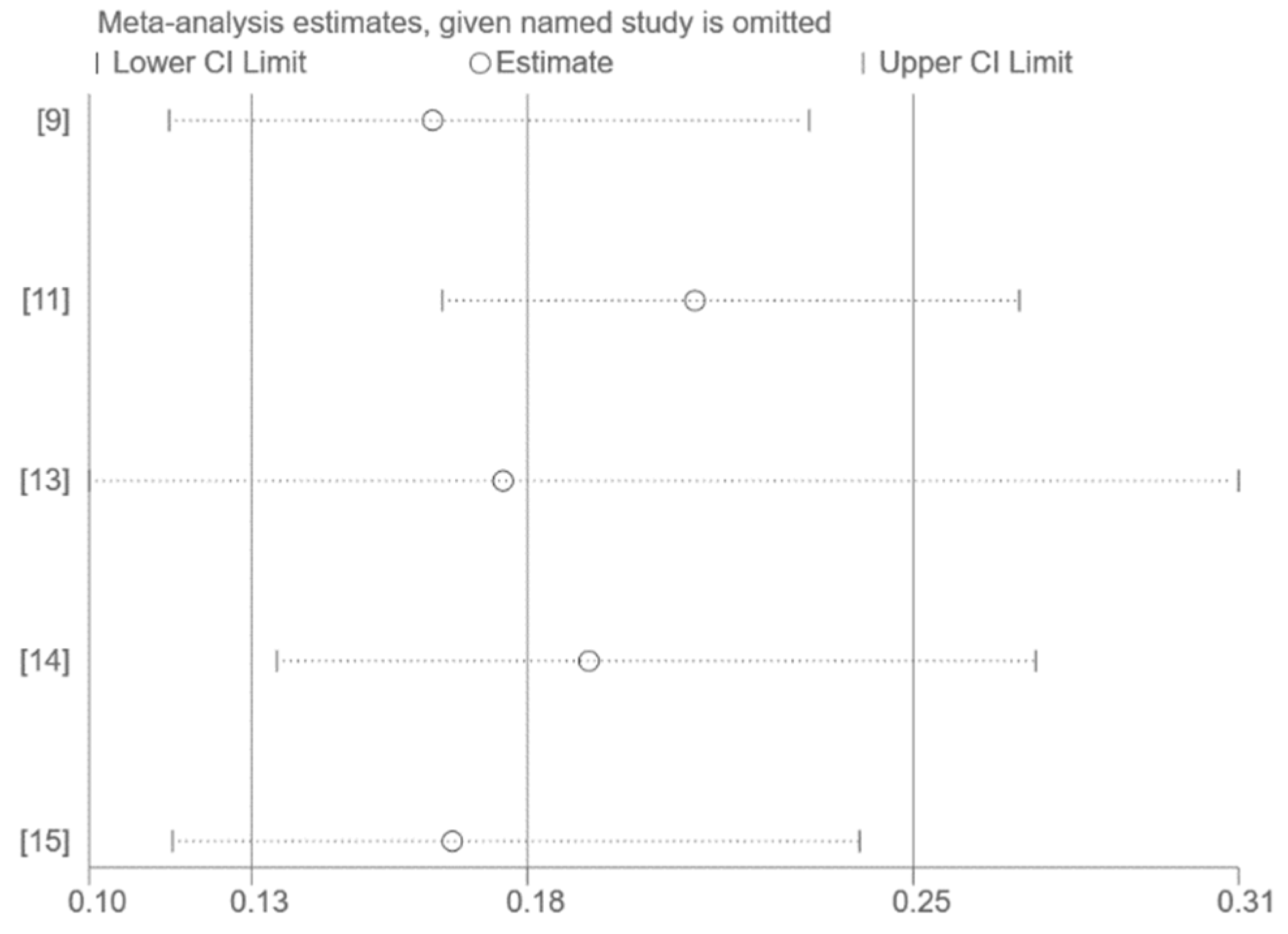
3.3. Publication Bias and Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Director-General’s Opening Remarks at the Mission Briefing on COVID-19—12 March 2020[EB/OL]. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-mission-briefing-on-covid-19---12-march-2020 (accessed on 14 July 2022).
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; et al. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: Results of a systematic review and meta-regression. Lancet 2022, 399, 924–944. [Google Scholar] [CrossRef]
- Zeng, G.; Wu, Q.; Pan, H.; Li, M.; Yang, J.; Wang, L.; Wu, Z.; Jiang, D.; Deng, X.; Chu, K.; et al. Immunogenicity and safety of a third dose of CoronaVac, and immune persistence of a two-dose schedule, in healthy adults: Interim results from two single-centre, double-blind, randomised, placebo-controlled phase 2 clinical trials. Lancet Infect Dis. 2022, 22, 483–495. [Google Scholar] [CrossRef]
- Zhou, R.; Liu, N.; Li, X.; Peng, Q.; Yiu, C.K.; Huang, H.; Yang, D.; Du, Z.; Kwok, H.Y.; Au, K.K.; et al. Three-Dose Vaccination-induced Immune Responses Protect against SARS-CoV-2 Omicron-BA.2. bioRxiv 2022. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard [EB/OL]. Available online: https://covid19.who.int/ (accessed on 25 July 2022).
- Saban, M.; Myers, V.; Wilf-Miron, R. Changes in infectivity, severity and vaccine effectiveness against delta COVID-19 variant ten months into the vaccination program: The Israeli case. Prev. Med. 2022, 154, 106890. [Google Scholar] [CrossRef] [PubMed]
- Chemaitelly, H.; Ayoub, H.H.; AlMukdad, S.; Coyle, P.; Tang, P.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Hasan, M.R.; Al-Kanaani, Z.; et al. Duration of mRNA vaccine protection against SARS-CoV-2 Omicron BA.1 and BA.2 subvariants in Qatar. Nat. Commun. 2022, 13, 3082. [Google Scholar] [CrossRef] [PubMed]
- Barda, N.; Dagan, N.; Cohen, C.; Hernán, M.A.; Lipsitch, M.; Kohane, I.S.; Reis, B.Y.; Balicer, R.D. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: An observational study. Lancet 2021, 398, 2093–2100. [Google Scholar] [CrossRef]
- Drawz, P.E.; DeSilva, M.; Bodurtha, P.; Vazquez Benitez, G.; Murray, A.; Chamberlain, A.M.; Dudley, R.A.; Waring, S.; Kharbanda, A.B.; Murphy, D.; et al. Effectiveness of BNT162b2 and mRNA-1273 Second Doses and Boosters for SARS-CoV-2 infection and SARS-CoV-2 Related Hospitalizations: A Statewide Report from the Minnesota Electronic Health Record Consortium. Clin. Infect Dis. 2022. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Oda, G.; Holodniy, M. Effectiveness of mRNA-based vaccines during the emergence of SARS-CoV-2 Omicron variant. Clin. Infect Dis. 2022, ciac325. [Google Scholar] [CrossRef] [PubMed]
- Suah, J.L.; Tng, B.H.; Tok, P.S.; Husin, M.; Thevananthan, T.; Peariasamy, K.M.; Sivasampu, S. Real-world effectiveness of homologous and heterologous BNT162b2, CoronaVac, and AZD1222 booster vaccination against Delta and Omicron SARS-CoV-2 infection. Emerg. Microbes Infect. 2022, 11, 1343–1345. [Google Scholar] [CrossRef] [PubMed]
- Butt, A.A.; Talisa, V.B.; Shaikh, O.S.; Omer, S.B.; Mayr, F.B. Relative Vaccine Effectiveness of a SARS-CoV-2 mRNA Vaccine Booster Dose Against the Omicron Variant. Clin. Infect. Dis. 2022. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Sachdeva, R.; Gower, C.; Ramsay, M.; Lopez Bernal, J. Effectiveness of COVID-19 booster vaccines against COVID-19-related symptoms, hospitalization and death in England. Nat. Med. 2022, 28, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Sritipsukho, P.; Khawcharoenporn, T.; Siribumrungwong, B.; Damronglerd, P.; Suwantarat, N.; Satdhabudha, A.; Chaiyakulsil, C.; Sinlapamongkolkul, P.; Tangsathapornpong, A.; Bunjoungmanee, P.; et al. Comparing real-life effectiveness of various COVID-19 vaccine regimens during the delta variant-dominant pandemic: A test-negative case-control study. Emerg. Microbes Infect. 2022, 11, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Ferdinands, J.M.; Rao, S.; Dixon, B.E.; Mitchell, P.K.; DeSilva, M.B.; Irving, S.A.; Lewis, N.; Natarajan, K.; Stenehjem, E.; Grannis, S.J.; et al. Waning 2-Dose and 3-Dose Effectiveness of mRNA Vaccines Against COVID-19-Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance—VISION Network, 10 States, August 2021–January 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 255–263. [Google Scholar]
- Arbel, R.; Hammerman, A.; Sergienko, R.; Friger, M.; Peretz, A.; Netzer, D.; Yaron, S. BNT162b2 Vaccine Booster and Mortality Due to Covid-19. N. Engl. J. Med. 2021, 385, 2413–2420. [Google Scholar] [CrossRef] [PubMed]
- Björk, J.; Bonander, C.; Moghaddassi, M.; Rasmussen, M.; Malmqvist, U.; Inghammar, M.; Kahn, F. COVID-19 vaccine effectiveness against severe disease from SARS-CoV-2 Omicron BA.1 and BA.2 subvariants—Surveillance results from southern Sweden, December 2021 to March 2022. Eurosurveillance 2022, 27, 2200322. [Google Scholar] [CrossRef] [PubMed]
- Chenchula, S.; Karunakaran, P.; Sharma, S.; Chavan, M. Current evidence on efficacy of COVID-19 booster dose vaccination against the Omicron variant: A systematic review. J. Med. Virol. 2022, 94, 2969–2976. [Google Scholar] [CrossRef] [PubMed]
- Sohan, M.; Hossain, M.J.; Islam, M.R. The SARS-CoV-2 Omicron (B.1.1.529) variant and effectiveness of existing vaccines: What we know so far. J. Med. Virol. 2022, 94, 1796–1798. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.; Hong, H.; Wang, S.; Ma, L.; Liu, C.; Bai, Y.; Adam, D.C.; Tian, L.; Wang, L.; Lau, E.H.; et al. Reproduction Number of the Omicron Variant Triples That of the Delta Variant. Viruses 2022, 14, 821. [Google Scholar] [CrossRef] [PubMed]
- Duong, B.V.; Larpruenrudee, P.; Fang, T.; Hossain, S.I.; Saha, S.C.; Gu, Y.; Islam, M.S. Is the SARS CoV-2 Omicron Variant Deadlier and More Transmissible Than Delta Variant? Int. J. Environ. Res. Public Health 2022, 19, 4586. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Author, Year | Country | Study Type | Vaccine | Dominant Variant | Study Periods | Age Range | Booster | No booster | Outcome | NOS | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Positive | Negative | Positive | Negative | |||||||||
| Paul E Drawz, et al. (2022) [9] | United States | Test-negative case–control design | BNT162b2 or mRNA-1273 | Delta | From 29 August 2021 to 27 November 2021 | ≥19 | 1347 | 46,526 | 15,702 | 139,718 | Infection | 6 |
| Aditya Sharma, et al. (2022) [10] | United States | Test-negative case–control design | BNT162b2 or mRNA-1273 | Omicron | From 1 December 2021 to 12 March 2022 | NA | 4226 | 404,548 | 5356 | 403,418 | Infection | 8 |
| Jing Lian Suah, et al. (2022) [11] | Malaysia | Test-negative case–control design | BNT162b2 or CoronaVac or AZD1222 | Delta | From 27 October 2021 to 4 February 2022 | ≥18 | 38567 | 882,109 | 280,560 | 720,077 | Infection | 8 |
| Jing Lian Suah, et al. (2022) [11] | Malaysia | Test-negative case–control design | BNT162b2 or CoronaVac or AZD1222 | Omicron | From 5 February 2022 to 22 February 2022 | ≥18 | 135,425 | 424,968 | 171,058 | 224,378 | Infection | 8 |
| Adeel A Butt, et al. (2022) [12] | United States | Retrospective cohort study | BNT162b2 or mRNA-1273 | Omicron | From 1 January 2022 to 20 February 2022 | ≥21 | 8444 | 454,506 | 10,462 | 452,488 | Infection | 5 |
| Nick Andrews, et al. (2022) [13] | England | Test-negative case–control design | ChAdOx1-S or BNT162b2 | Delta | From 13 September 2021 to 5 November 2021 | ≥18 | 17,655 | 143,001 | 159,593 | 234,684 | Symptom | 8 |
| Paskorn Sritipsukho, et al. (2022) [14] | Thailand | Test-negative case–control design | CoronaVac or BNT162b2 or ChAdOx1-S | Delta | From 25 July 2021 to 23 October 2021 | ≥18 | 13 | 478 | 181 | 787 | Infection | 5 |
| Jill M. Ferdinands, et al. (2022) [15] | United States | Test-negative case–control design | mRNA vaccine | Delta | From 26 August 2021 to 22 January 2022 * | ≥18 | 347 | 13,860 | 8136 | 77,235 | Infection | 6 |
| Jill M. Ferdinands, et al. (2022) [15] | United States | Test-negative case–control design | mRNA vaccine | Omicron | From 26 August 2021 to 22 January 2022 * | ≥18 | 1938 | 8993 | 8351 | 11,471 | Infection | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, Y.; Liu, S.; Zhang, D. Effectiveness of COVID-19 Vaccine Booster Shot Compared with Non-Booster: A Meta-Analysis. Vaccines 2022, 10, 1396. https://doi.org/10.3390/vaccines10091396
Zhu Y, Liu S, Zhang D. Effectiveness of COVID-19 Vaccine Booster Shot Compared with Non-Booster: A Meta-Analysis. Vaccines. 2022; 10(9):1396. https://doi.org/10.3390/vaccines10091396
Chicago/Turabian StyleZhu, Yajuan, Shuang Liu, and Dingmei Zhang. 2022. "Effectiveness of COVID-19 Vaccine Booster Shot Compared with Non-Booster: A Meta-Analysis" Vaccines 10, no. 9: 1396. https://doi.org/10.3390/vaccines10091396
APA StyleZhu, Y., Liu, S., & Zhang, D. (2022). Effectiveness of COVID-19 Vaccine Booster Shot Compared with Non-Booster: A Meta-Analysis. Vaccines, 10(9), 1396. https://doi.org/10.3390/vaccines10091396