

The Use of Vacuum Plasma Surface Treatment to Improve Bone Healing and Regeneration in Socket Preservation and GBR: A Case Series with Histological Analysis

 ,
, 

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
- Patients with at least one hopeless tooth in the mandible or maxilla, with intact post-extractive alveolus, able to understand and provide informed consent were considered eligible for inclusion for socket preservation; or any patients who required single implant-supported restoration and staged horizontal guided bone regeneration (defect of class IV according to Cawed and Howell) in both the mandible or maxilla. A hopeless tooth was defined as a tooth with severe structural, periodontal, or endodontic damage that could not be predictably treated or maintained and was recommended for extraction. Common criteria for classifying a tooth as hopeless include: severe periodontal disease with ≥75% bone loss, mobility (Grade III), or class III furcation involvement; extensive decay or fractures that make the tooth non-restorable; unsuccessful endodontic treatment with persistent infection; and trauma leading to non-viable roots or severe displacement.
- Aged 18 years or older and able to provide informed consent.
- Smokers were categorized as: (1) non-smokers; (2) moderate smokers (smoking up to 10 cigarettes/day); and (3) heavy smokers (smoking more than 11 cigarettes/day). Heavy smokers were excluded, only categories 1 and 2 were included in this study.
- Biotype was categorized as: thin (≤1 mm), medium (>1–<2 mm), or thick (≥2 mm).
- General contraindications to implant surgery
- Patients irradiated in the head and neck area.
- Immunosuppressed or immunocompromised patients.
- Patients treated or under treatment with intravenous amino-bisphosphonates.
- Patients with untreated periodontitis.
- Patients with poor oral hygiene and motivation.
- Uncontrolled diabetes.
- Heavy smokers (more than 11 cigarettes/day).
- Pregnancy or nursing.
- Substance abusers.
- Psychiatric problems or unrealistic expectations.
- Lack of antagonist occluding dentition in the area intended for implant placement.
- Patients with infection and or inflammation in the area intended for implant placement.
- Patients participating in other studies if the present protocol cannot be properly adhered to.
- Patients referred only for implant placement and cannot be followed at the treatment center.
- Patients unable to be followed for 5 years.
2.1. Socket Preservation Procedure
2.2. Post-Surgical Instructions and Prosthetic Phase After Socket Preservation
2.3. Biopsy Retrieval
2.4. Sample Processing and Histological Analysis
2.5. GBR Procedure
2.6. Outcome Measures
- Implant failure defined as mobility, infection, fracture, and/or any other mechanical or biological issue that determined its removal.
- Prosthesis failure was considered at any time it had to be replaced.
- Any biological (e.g., drug-resistant pain, swelling, excessive MBL, suppuration, etc.) and/or technical (e.g., fracture of the veneering material and or framework, screw loosening, etc.) complications were recorded during follow-up.
3. Results
3.1. Clinical Outcomes
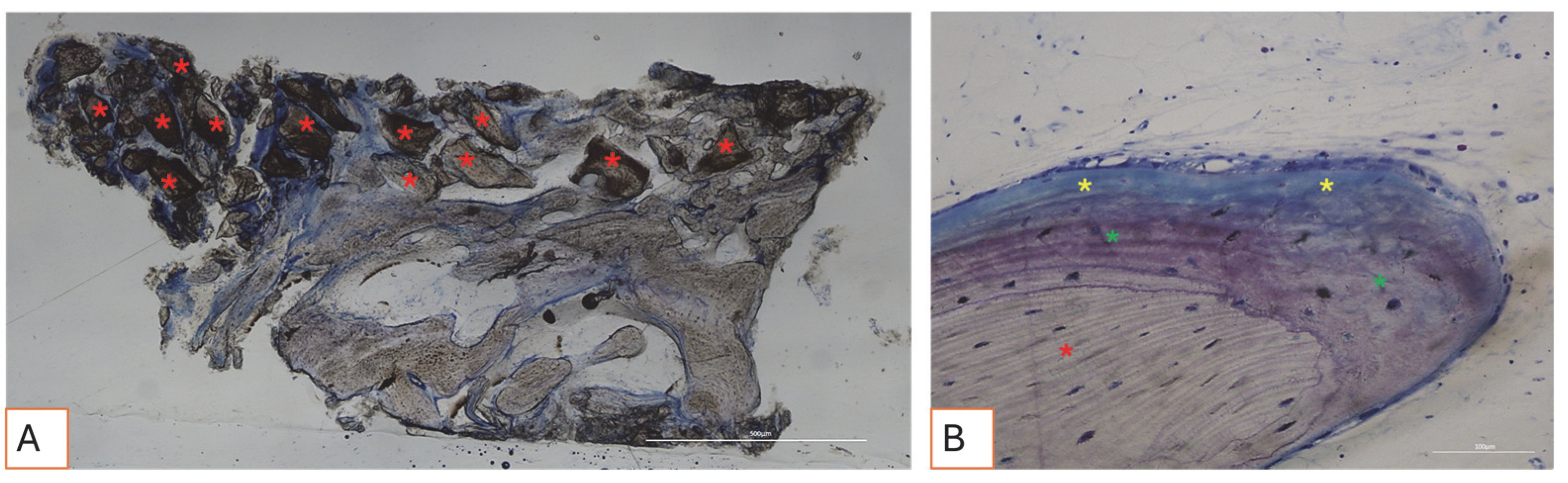
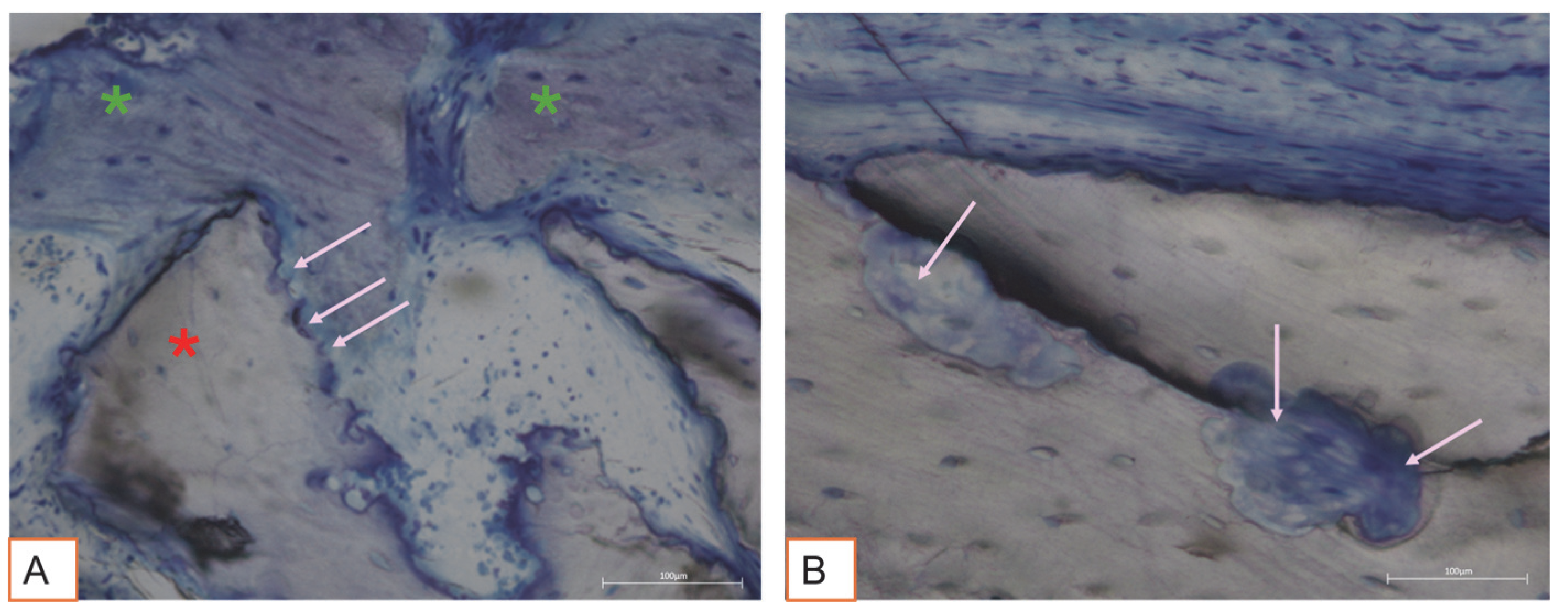
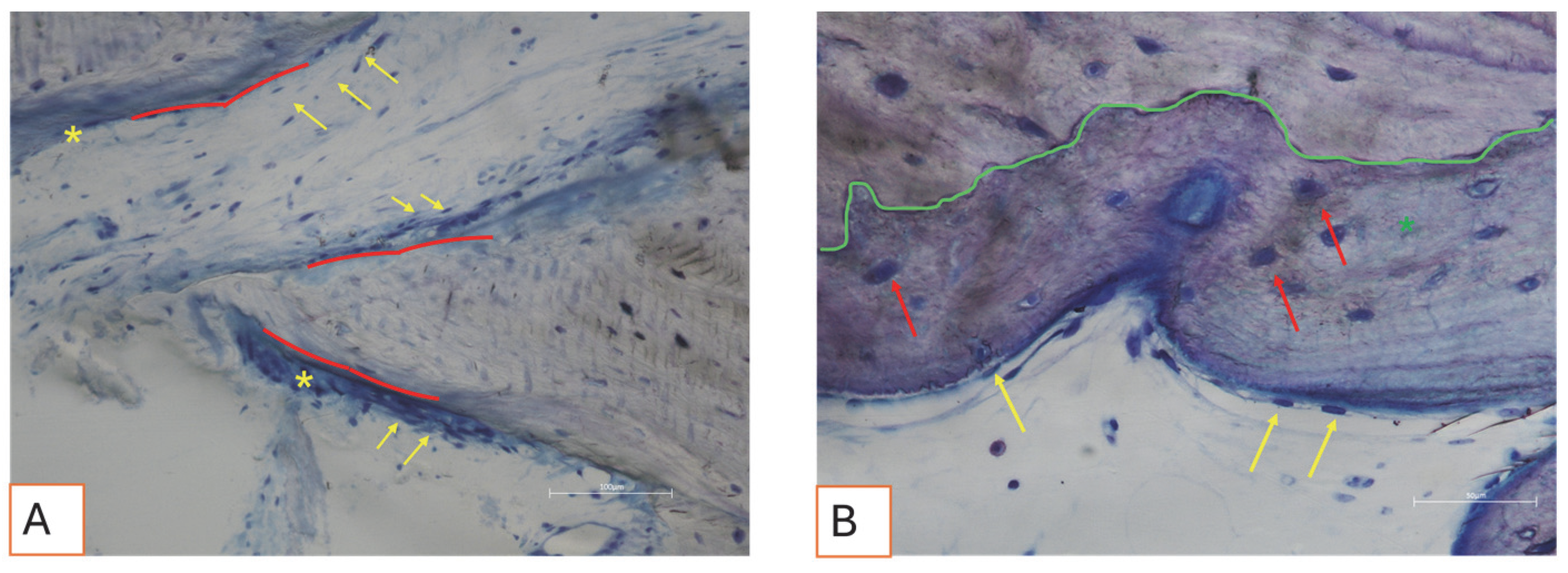
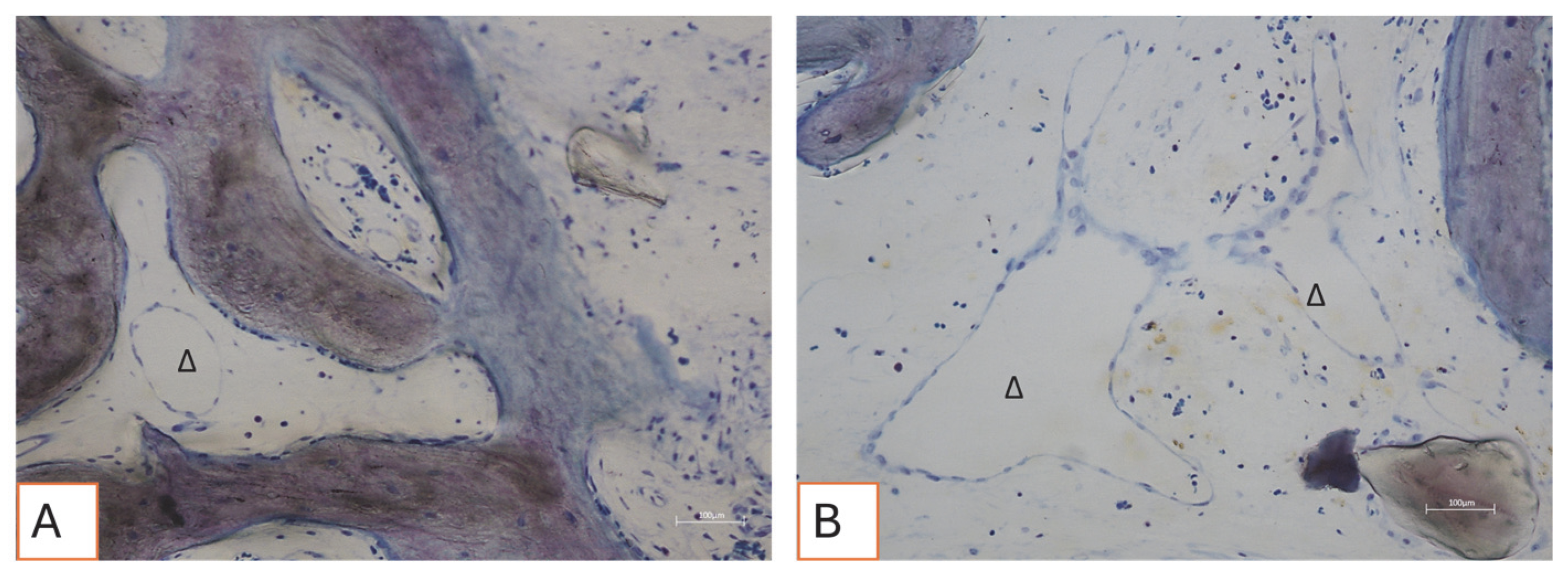
3.2. Histological Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Busenlechner, D.; Fürhauser, R.; Haas, R.; Watzek, G.; Mailath, G.; Pommer, B. Long-term implant success at the Academy for Oral Implantology: 8-year follow-up and risk factor analysis. J. Periodontal Implant. Sci. 2014, 44, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.I. A tribute to Dr. Per-Ingvar Brånemark. J. Periodontal Implant. Sci. 2014, 44, 265. [Google Scholar] [CrossRef] [PubMed]
- Mavrogenis, A.F.; Dimitriou, R.; Parvizi, J.; Babis, G.C. Biology of implant osseointegration. J. Musculoskelet. Neuronal Interact. 2009, 9, 61–71. [Google Scholar]
- Gallucci, G.O.; Hamilton, A.; Zhou, W.; Buser, D.; Chen, S. Implant placement and loading protocols in partially edentulous patients: A systematic review. Clin. Oral Implant. Res. 2018, 29 (Suppl. S16), 106–134. [Google Scholar] [CrossRef]
- Wong, M.; Eulenberger, J.; Schenk, R.; Hunziker, E. Effect of surface topology on the osseointegration of implant materials in trabecular bone. J. Biomed. Mater. Res. 1995, 29, 1567–1575. [Google Scholar] [CrossRef]
- Wennerberg, A.; Albrektsson, T. On implant surfaces: A review of current knowledge and opinions. Int. J. Oral Maxillofac. Implant. 2010, 25, 63–74. [Google Scholar]
- Wennerberg, A.; Albrektsson, T. Effects of titanium surface topography on bone integration: A systematic review. Clin. Oral Implant. Res. 2009, 20 (Suppl. S4), 172–184. [Google Scholar] [CrossRef]
- Kazimierczak, P.; Przekora, A. Osteoconductive and Osteoinductive Surface Modifications of Biomaterials for Bone Regeneration: A Concise Review. Coatings 2020, 10, 971. [Google Scholar] [CrossRef]
- Canullo, L.; Genova, T.; Chinigò, G.; Iacono, R.; Pesce, P.; Menini, M.; Mussano, F. Vacuum Plasma Treatment Device for Enhancing Fibroblast Activity on Machined and Rough Titanium Surfaces. Dent. J. 2024, 12, 71. [Google Scholar] [CrossRef] [PubMed]
- Shibata, Y.; Hosaka, M.; Kawai, H.; Miyazaki, T. Glow discharge plasma treatment of titanium plates enhances adhesion of osteoblast-like cells to the plates through the integrin-mediated mechanism. Int. J. Oral Maxillofac. Implant. 2002, 17, 771–777. [Google Scholar]
- Noro, A.; Kaneko, M.; Murata, I.; Yoshinari, M. Influence of surface topography and surface physicochemistry on wettability of zirconia (tetragonal zirconia polycrystal). J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 101, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Tallarico, M.; Meloni, S.M.; Troia, M.; Cacciò, C.; Lumbau, A.I.; Gendviliene, I.; Ceruso, F.M.; Pisano, M. The Use of Vacuum Plasma Surface Treatment to Improve Hydrophilicity and Wettability of Biomaterials: An In-Vitro Study. Dent. J. 2025, 13, 141. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Pellegrini, G.; Canciani, E.; Heinemann, F.; Galliera, E.; Dellavia, C. Alveolar socket preservation technique: Effect of biomaterial on bone regenerative pattern. Ann. Anat. Anat. Anz. 2016, 206, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, F.; Alla, I.; Gehrke, S.A.; Carmine, M.D.; Tari, S.R.; Scarano, A. Effect of Different Dental Implant Prosthetic Joints on Marginal Bone Loss: Emerging Findings from a Bayesian Network Meta-Analysis (NMA) and Systematic Review. Prosthesis 2024, 6, 186–205. [Google Scholar] [CrossRef]
- Udeabor, S.E.; Heselich, A.; Al-Maawi, S.; Alqahtani, A.F.; Sader, R.; Ghanaati, S. Current Knowledge on the Healing of the Extraction Socket: A Narrative Review. Bioengineering 2023, 10, 1145. [Google Scholar] [CrossRef]
- Perrotti, V.; Nicholls, B.M.; Piattelli, A. Human osteoclast formation and activity on an equine spongy bone substitute. Clin. Oral Implant. Res. 2009, 20, 17–23. [Google Scholar] [CrossRef]
- Di Stefano, D.A.; Zaniol, T.; Cinci, L.; Pieri, L. Chemical, Clinical and Histomorphometric Comparison between Equine Bone Manufactured through Enzymatic Antigen-Elimination and Bovine Bone Made Non-Antigenic Using a High-Temperature Process in Post-Extractive Socket Grafting. A Comparative Retrospective Clinical Study. Dent. J. 2019, 7, 70. [Google Scholar] [CrossRef]
- Le, P.T.M.; Shintani, S.A.; Takadama, H.; Ito, M.; Kakutani, T.; Kitagaki, H.; Terauchi, S.; Ueno, T.; Nakano, H.; Nakajima, Y.; et al. Bioactivation Treatment with Mixed Acid and Heat on Titanium Implants Fabricated by Selective Laser Melting Enhances Preosteoblast Cell Differentiation. Nanomaterials 2021, 11, 987. [Google Scholar] [CrossRef]
- Pellegrini, G.; Rasperini, G.; Obot, G.; Farronato, D.; Dellavia, C. Soft tissue healing in alveolar socket preservation technique: Histologic evaluations. Int. J. Periodontics Restor. Dent. 2014, 34, 531–539. [Google Scholar] [CrossRef]
- Kahm, S.H.; Lee, S.H.; Lim, Y.; Jeon, H.J.; Yun, K.I. Osseointegration of Dental Implants after Vacuum Plasma Surface Treatment In Vivo. J. Funct. Biomater. 2024, 15, 278. [Google Scholar] [CrossRef]
- Pesce, P.; Menini, M.; Santori, G.; Giovanni, E.; Bagnasco, F.; Canullo, L. Photo and Plasma Activation of Dental Implant Titanium Surfaces. A Systematic Review with Meta-Analysis of Pre-Clinical Studies. J. Clin. Med. 2020, 9, 2817. [Google Scholar] [CrossRef] [PubMed]
- Scribante, A.; Ghizzoni, M.; Pellegrini, M.; Pulicari, F.; Manfredini, M.; Poli, P.P.; Maiorana, C.; Spadari, F. Full-Digital Customized Meshes in Guided Bone Regeneration Procedures: A Scoping Review. Prosthesis 2023, 5, 480–495. [Google Scholar] [CrossRef]
- Berger, M.B.; Bosh, K.B.; Cohen, D.J.; Boyan, B.D.; Schwartz, Z. Benchtop plasma treatment of titanium surfaces enhances cell response. Dent. Mater. 2021, 37, 690–700. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tallarico, M.; Troia, M.; Pisano, M.; Meloni, S.M.; Melodia, D.; Della Via, C.; Henin, D.; Ceruso, F.M.; Cacciò, C.; Lumbau, A.I. The Use of Vacuum Plasma Surface Treatment to Improve Bone Healing and Regeneration in Socket Preservation and GBR: A Case Series with Histological Analysis. Appl. Sci. 2025, 15, 6344. https://doi.org/10.3390/app15116344
Tallarico M, Troia M, Pisano M, Meloni SM, Melodia D, Della Via C, Henin D, Ceruso FM, Cacciò C, Lumbau AI. The Use of Vacuum Plasma Surface Treatment to Improve Bone Healing and Regeneration in Socket Preservation and GBR: A Case Series with Histological Analysis. Applied Sciences. 2025; 15(11):6344. https://doi.org/10.3390/app15116344
Chicago/Turabian StyleTallarico, Marco, Michele Troia, Milena Pisano, Silvio Mario Meloni, Dario Melodia, Claudia Della Via, Dolaji Henin, Francesco Mattia Ceruso, Carlotta Cacciò, and Aurea Immacolata Lumbau. 2025. "The Use of Vacuum Plasma Surface Treatment to Improve Bone Healing and Regeneration in Socket Preservation and GBR: A Case Series with Histological Analysis" Applied Sciences 15, no. 11: 6344. https://doi.org/10.3390/app15116344
APA StyleTallarico, M., Troia, M., Pisano, M., Meloni, S. M., Melodia, D., Della Via, C., Henin, D., Ceruso, F. M., Cacciò, C., & Lumbau, A. I. (2025). The Use of Vacuum Plasma Surface Treatment to Improve Bone Healing and Regeneration in Socket Preservation and GBR: A Case Series with Histological Analysis. Applied Sciences, 15(11), 6344. https://doi.org/10.3390/app15116344