Abstract
Central business district (CBD) hospitals must sustain reliable pressure relationships in critical rooms while reducing whole-facility carbon under tight space and disruption constraints. We developed an ontology-grounded semantic digital twin that normalizes building automation system (BAS) and building management system (BMS) telemetry into a unified semantic store consistent with Brick Schema, enabling portable asset discovery via query and thereby supporting forecasting, anomaly detection, and multi-objective optimization without dependence on vendor point naming conventions. Whole-facility impacts were verified using International Performance Measurement and Verification Protocol Option C–style measurement and verification with an S0-calibrated baseline model and residual-based savings attribution. Relative to the baseline (S0), the intervention (S3) produced a step increase in the critical-room pressure-compliance pass rate, tighter room-to-corridor differential-pressure (ΔP) control across airborne infection isolation and open room strata, and intent-aligned ventilation delivery (air changes per hour ratio distribution concentrated near unity; p < 0.05 where letter groups differ). Operational-state discrimination improved (AUC 0.649→0.696) and issue-resolution times shortened (left-shifted cumulative distribution function), indicating reduced service burden. Option C verification showed energy residuals shifting negative under S3, consistent with net savings versus baseline expectations. Across progressive maturity (S0→S3), time-to-value and burden fractions decreased, carbon intensity (tCO2e m−2) decreased, long-tail exposure compressed (log-scale horizon), and composite performance indices increased (p < 0.05). These results demonstrate a verifiable pathway to pressure-reliable, decarbonized hospital operations at the whole-facility boundary while making the semantic layer’s utility explicit through query-driven, ontology-grounded asset discovery. We present an IPMVP Option-C–verifiable semantic digital-twin governance framework that links audited operational evidence (telemetry → actions → verification) to whole-facility energy and carbon outcomes while maintaining critical-room pressure-relationship reliability. Optimization benchmarking (including quantum annealing) is used as supporting decision-support evaluation, rather than as the central contribution.
1. Introduction
The global demand for sustainable healthcare infrastructure has intensified due to rapid urbanization, population growth, and escalating environmental concerns, necessitating designs that align with circular economy (CE) [1,2,3] and ecological efficiency principles [4,5,6]. CE emphasizes resource optimization, waste reduction, and lifecycle efficiency, aiming to minimize material and energy consumption while maximizing reuse and recycling [7,8,9]. Ecological efficiency focuses on reducing environmental impacts via energy efficiency, emissions reduction, and ecosystem preservation [10,11,12]. Hospitals, as resource-intensive facilities, contribute significantly to environmental footprints, with high land use, construction material demands, and operational energy consumption. The medical central business district (MCBD) layout, characterized by compact, centralized designs, offers a promising approach to address these challenges by optimizing land use, streamlining operations, and reducing energy demands [13]. The term MCBD is defined as the area within a hospital where public departments used by all clinical units—such as the laboratory, imaging, ultrasound, blood bank, endoscopy, pathology, operating rooms, and Central Sterile Supply Department—are relatively concentrated. For a modern, comprehensive hospital, the status, function, and role of these core service areas are analogous to those of a city’s central business district (CBD) in the urban context. Borrowing the urban CBD concept [14,15], we distinctly refer to the hospital’s core medical service zone as the MCBD.
Compact hospital layouts can significantly minimize land use and associated costs. For instance, R. Rodríguez et al. (2021) found that streamlined site planning and compact hospital forms effectively reduce land acquisition needs and promote long-term scalability, aligning with sustainability goals [16]. Site planning is foundational to sustainable hospital design because it locks in long-term sustainability performance targets, such as minimizing the combined footprint of buildings, parking, and roads to help to protect and restore natural habitat, using green or high-reflectance roofs and pervious paving to reduce urban heat-island impacts and manage stormwater, and siting and/orienting facilities according to solar exposure and prevailing winds to enable passive strategies and resilience [17,18]. In addition, site planning that reduces the movement burden of people and supplies and better integrates the hospital within the surrounding urban fabric supports broader environmental and operational sustainability objectives. For instance, energy efficiency also plays a critical role: integrating high-performance heating, ventilation, and air conditioning (HVAC) and climate control, daylighting, and passive and natural ventilation strategies has been highlighted as a core direction in contemporary sustainable healthcare architecture to reduce operational energy demand while maintaining indoor environmental quality [19,20,21]. Moreover, the World Health Organization has promoted the zero-waste hospital model, advocating for the integration of CE principles such as the use of recyclable materials, water reuse, and lifecycle-focused planning to reduce waste and operational costs [22,23]. Evidence also shows that centralized hospital designs can enhance operational efficiency by improving patient flow and reducing staff travel distances, which can result in operational cost savings of up to 20% [24]. However, while individual studies address specific components such as energy or land use, there is a notable gap in holistic evaluations that integrate environmental and economic impacts across land, construction, and operations, especially for hospitals of varying sizes and capacities [25].
In this study, CE is applied in an operational and asset-life sense that is especially relevant to space-constrained MCBD hospitals: rather than relying on material-intensive rebuilds or wholesale HVAC replacement, we prioritize making better use of existing installed assets through measurement-driven optimization (controls, setpoints, recommissioning, and condition-based maintenance). This framing aligns with CE principles of keeping products and materials in use via maintenance and refurbishment and with renovation-oriented approaches that avoid or delay new material inputs (thereby reducing embedded impacts), while simultaneously improving operational energy performance.
A growing body of literature indicates that internet of things (IoT)-instrumented building digital twins, combined with artificial intelligence (AI) and optimization-based control and decision support, can improve the sustainability and efficiency of building operations through real-time performance monitoring, fault detection and predictive maintenance, and energy–comfort optimization—capabilities that are especially valuable for high-intensity hospital campuses and dense urban medical environments [26,27,28,29]. Digital twin systems have demonstrated value in enabling real-time monitoring, predictive maintenance, and energy optimization, particularly when integrated with IoT and AI technologies [30,31]. Applications in hospital settings show that continuous lifecycle integration of digital twins improves operational efficiency, fault detection, and energy use in complex facilities [32]. Urban-scale digital twin tools have also enabled carbon-emission mapping and intervention planning, indicating their potential to guide carbon reduction strategies in large infrastructure systems [33]. However, most implementations remain limited to single systems or buildings and lack integrated carbon-adaptive controls or optimization methods, such as quantum computing.
While prior research on hospital campus planning has highlighted the benefits of spatial consolidation—such as centralized floorplates, shared mechanical, electrical, and plumbing (MEP) systems, and vertical densification—for reducing land consumption, construction costs, and energy use, these designs are generally static and lack real-time operational adaptability. Similarly, building management systems (BMSs) and IoT implementations have demonstrated incremental gains in equipment scheduling and occupant comfort, but remain limited to siloed, subsystem-specific applications like HVAC or lighting control. Recent studies have begun to explore the role of digital twins in improving energy efficiency and predictive maintenance in buildings, including hospitals [30,31,32]. However, these systems are often constrained to single buildings, focus on historical data, or lack integration with adaptive carbon accounting mechanisms. Moreover, while urban digital twins have been used to support decarbonization planning through interactive visualization and carbon intervention maps [33], such frameworks have not been combined with quantum-accelerated optimization or dynamic space reconfiguration. Quantum-enhanced computing offers potential for rapid re-zoning and complex optimization problems at a scale relevant to large hospital campuses, but remains unexplored in this context.
While our decision-support formulation is solver-agnostic, the primary objective of this work is to establish a reproducible multi-objective planning framework and to benchmark representative solver families under a common set of constraints and decision-operability metrics. In the evaluated instance sizes, classical exact optimization (mixed-integer linear programming (MILP)) is sufficient and provides the strongest performance in both solution quality and runtime. We therefore treat quantum annealing (QA) as an exploratory benchmark, rather than a required component of the proposed workflow: QA is included to (i) provide a forward-looking reference for how emerging quantum hardware may behave on structurally similar problems, and (ii) future-proof the framework for larger campus-scale deployments where combinatorial growth, additional constraints, and higher-resolution scheduling may challenge exact methods and motivate hybrid classical–quantum approaches.
We propose an ontology-grounded semantic digital twin for MCBD that converts building automation system (BAS) and IoT telemetry into a traceable, decision-grade control and measurement and verification (M&V) pipeline, linking pressure-relationship governance in critical rooms (airborne infection isolation (AII) and operating room (OR)) to whole-facility decarbonization. Deployment progresses from baseline to advanced maturity (S0–S3: S0, S1–S2, and S3 (deployment stages); S0: baseline operations (pre-semantic normalization and advanced analytics); S1–S2: intermediate instrumentation + analytics readiness; S3: advanced operational state (closed-loop monitoring and optimization + formal post-deployment M&V governance)), integrating real-time monitoring, anomaly detection, work-order execution, and multi-objective optimization (classical, quantum, and hybrid). Outcomes were verified at the whole-facility boundary using International Performance Measurement and Verification Protocol (IPMVP) Option-C baseline modeling with residual diagnostics, quantifying energy and carbon-intensity changes alongside pressure-compliance improvement and reduced indoor air quality (IAQ) burden proxies (CO2 and PM2.5) without relaxing compliance criteria. Causal impact will be estimated using interrupted time-series and difference-in-differences against a control, complemented by fault economics (downtime and avoided cost) and probabilistic cost-effectiveness for owner policy decisions. Solver benchmarking (heuristics, MILP, and QA) will define quality–runtime–feasibility tradeoffs to enable repeatable, auditable retrofit guidance.
The primary contribution of this study is Option-C whole-facility M&V-verified decarbonization outcomes integrated with pressure-relationship reliability through a traceable, ontology-grounded evidence chain (baseline lock, diagnostics, and reporting-period inference). Secondary contributions include semantic normalization enabling portable analytics across heterogeneous BAS and BMS; operational endpoints (excursions, alarm burden, and time-to-resolve) linking clinical reliability to O&M burden; and decision support modules (optimization and benchmarking; causal inference; and uncertainty economics) that support implementation and interpretation.
2. Performance Metrics
The supporting performance metrics for evaluating semantic digital-twin pressure reliability and low-carbon operations in building systems comprise five quantitative layers (Supplementary Materials file, Performance Metrics): (A) Pressure-relationship compliance, calculating differential pressure and converting it to a binary indicator based on room-type thresholds (e.g., negative for AII rooms, positive for critical spaces), yielding a weekly compliance fraction over quality-assurance and quality-control-validated observations; (B) Whole-facility Option-C baseline and savings, modeling metered energy against weather (cooling degree days () and heating degree days ()) and covariates with baseline coefficients to estimate counterfactual and compute aggregate savings ; (C) Operational carbon accounting, integrating metered power with grid carbon intensity as or discretely ; (D) Quantum-assisted zoning via quadratic unconstrained binary optimization (QUBO), optimizing binary space-zone assignments to minimize under one-zone-per-space constraints; and (E) Predictive maintenance scoring, using residuals and covariance for Mahalanobis distance , triggering actions when exceeding threshold .
3. Methods
Figure S1 describes a step-by-step rollout of a smart, evidence-driven digital-twin program in a CBD hospital: first, the study is staged from baseline to advanced operation (S0–S3); then, building and sensor data are connected into a governed “evidence chain” (collect → clean and sync → store with traceability → visualize → deliver actions). Next, all equipment and room data are standardized using an ontology-based semantic layer consistent with Brick Schema to allow analytics to work reliably across different systems. The program then improves critical-room airflow and pressure control (e.g., isolation rooms and operating rooms), expands from single rooms to whole departments using a floorplan graph, and proceeds through gated commissioning with a locked baseline model to prevent hindsight bias. After that, it runs multi-objective optimization (balancing energy and carbon, safety, and feasibility), adds forecasting with early-warning alarms for pressure excursions, and tracks practical outcomes (pressure reliability, ventilation efficiency, indoor air indicators, and staff maintenance burden). Finally, it verifies whole-facility energy savings using IPMVP Option C, converts energy changes to carbon impacts, estimates operational and economic benefits from fewer faults, strengthens “what caused what” using time-series and comparison methods, and reports results with reproducible statistical controls.
3.1. Study Design, Deployment Scenarios, and CBD Hospital Operating Constraints
We implemented and evaluated an ontology-grounded semantic digital-twin intervention for pressure-relationship reliability in critical rooms and whole-facility decarbonization using a staged deployment design (S0–S3). S0 denotes baseline operations prior to semantic normalization and advanced analytics; S1–S2 represent intermediate instrumentation and analytics readiness (progressive enablement of telemetry integration, monitoring, and decision services); and S3 denotes the advanced operational state with closed-loop monitoring and optimization, and formal post-deployment M&V governance. Governance included stakeholder reliability and safety requirements, maintenance response workflows, and whole-facility M&V reporting across deployment stages. The deployment context is a CBD hospital setting, where high-density siting and constrained shafts and plant space impose practical limitations on retrofit scope, require disruption-sensitive execution, and increase the value of evidence-grade verification at the whole-facility boundary (rather than isolated subsystem testing).
Case Study Setting, Analysis Periods, and Intervention Package
As summarized in Table S1, the evaluation is framed as a single-site tertiary hospital campus in Hangzhou, Zhejiang Province, China, with optional matched peer hospitals in the same metro and region used as comparators if difference-in-differences (DiD) is reported. Hangzhou is widely treated as a representative city in China’s hot-summer and cold-winter (HSCW) climate region, implying substantial seasonal cooling and heating drivers and humidity-relevant loads that motivate explicit weather and operational normalization in whole-facility M&V. The table anchors site scale using tertiary-hospital references in Hangzhou (e.g., campus floor-area and bed-capacity magnitudes) to contextualize intensity metrics (tCO2e m−2) and operational complexity; for example, The Sir Run Run Shaw Hospital affiliated with Zhejiang University School of Medicine (Qingchun Campus and Xiasha Campus) covers an area of 190,667 m2 and has 2400 beds, illustrating the large tertiary campus order of magnitude used for interpreting normalized carbon metrics and O&M workload signals. The analysis window is stated explicitly (study window, baseline period for model training and lock, and reporting period for verified savings and co-benefits), and the reporting aggregation is aligned with this manuscript’s use of weekly metered electricity vs. baseline-predicted comparisons with uncertainty bands for Option-C reporting. Finally, the table maps the intervention to this paper’s staged deployment logic—S0 baseline → S1–S2 instrumentation and analytics readiness → S3 advanced monitoring and optimization with governance—and lists the operational measure families (controls tuning, fault remediation, pressure and ventilation governance, and photovoltaics (PV) and distributed energy resources (DER) where present) that justify a whole-facility Option-C boundary because interactive subsystem effects cannot be credibly isolated at component level.
3.2. Cyber–Physical Connectivity, Governance, and the Operational Evidence Chain
The method was engineered as a traceable evidence chain from field telemetry to actions, reflecting the figure-defined stack: data acquisition → preprocessing → integration → visualization → service layer, with cross-cutting controls for information exchange, data quality, security, and auditability.
The platform (Sir Run Run Shaw Hospital affiliated with Zhejiang University School of Medicine, Hangzhou, China) continuously ingests BAS and BMS control and status telemetry and supplemental IoT in-room sensing streams relevant to pressurization, ventilation delivery, indoor-environment proxies, and energy. BAS and BMS platforms were implemented using Desigo CC (Siemens AG, Munich, Germany) and EcoStruxure Building Operation (Schneider Electric SE, Rueil-Malmaison, France), with telemetry integrated to the analytic platform via open building-automation protocols (BACnet/IP and Modbus), where applicable. It also ingests whole-facility energy and demand metering at the IPMVP Option-C boundary to support baseline calibration and reporting-period evaluation [34]. Whole-facility electricity at the main incomer was captured using a three-phase meter (DTSU666; CHINT, Wenzhou, China; accuracy Class B/1.0 per EN 50470-1/-3) with interval logging (e.g., 15-min) and weekly aggregation for Option-C reporting. Specifically, BAS and BMS telemetry comprised differential-pressure (ΔP) sensors (DMP305X-DST, Shanghai LEEG Instruments Co., Ltd., Shanghai, China), supply and exhaust actuation commands and states, door-status interlocks, alarm states, and other HVAC and control points used for critical-room pressurization governance. IoT streams provided in-room sensing for indoor-environment proxies, explicitly including CO2 (measured using NDIR modules, Winsen Electronics Technology Co., Ltd., Zhengzhou, China) and PM2.5 (measured by PMS5003, Beijing Plantower Co., Ltd., Beijing, China) time series. Operations-and-maintenance workflow records included issue tickets and work orders with timestamps, minutes-to-resolve distributions, fault-event counts stratified by fault type, and downtime hours used to quantify service burden and reliability impacts. Derived data products generated from these inputs included ΔP distributions and transient-control metrics, excursion alarms with confusion-matrix reporting, baseline-predicted versus measured energy comparisons with residual diagnostics and uncertainty bands, solver Pareto fronts and optimality gaps and runtime scaling for benchmarking, and causal estimands from interrupted time series and difference-in-differences analyses.
Preprocessing functions ensure time synchronization and quality screening; integrated storage preserves lineage between raw points, semantic mappings, and analytic outputs; visualization surfaces report compliance, excursions, and model residuals; and service endpoints operationalize outputs into building control interfaces and work-order and issue-resolution workflows. This end-to-end governance is a prerequisite for whole-facility M&V and aligns with the principles and definitions associated with IPMVP Option C (Whole Facility), where savings and performance are assessed using whole-facility metering within a defined measurement boundary.
In addition to storing telemetry and analytic outputs, we generated a resolution evidence package for each flagged event (pressure excursion, sustained compliance drops, or abnormal energy residual). Each package links (i) the triggering evidence (time-stamped point trends, model residuals, and alarm state), (ii) the operational response (BAS setpoint and logic changes and/or computerized maintenance management system (CMMS) work-order identifiers with timestamps), and (iii) a post-action verification window demonstrating recovery (e.g., improved compliance fraction, reduced excursion minutes, and updated confusion-matrix alarm performance). This commissioning-style packet structure aligns the digital-twin pipeline with traceability and auditability expectations and supports whole-facility Option-C M&V reporting. Work orders and ticket workflows were managed in an enterprise CMMS/EAM platform (Yonyou Enterprise Asset Management, Yonyou Network Technology Co., Ltd., Beijing, China) and exported via reporting/API extracts including ticket ID, asset/space ID, open/ack/close timestamps, fault class, labor minutes, and closure notes.
As the telemetry-to-action chain directly affects clinical operations (AII and OR pressure relationships), maintenance workload, and whole-facility energy and carbon reporting, we implemented a role-defined governance workflow spanning facilities, operations and maintenance (O&M), infection-prevention and clinical leads, BAS and BMS controls contractors, information technology (IT) and cybersecurity, and sustainability and finance. Prior to metric finalization and reporting, this group confirmed measurement boundaries, key performance indicator (KPI) definitions (e.g., compliance fraction, excursion minutes, air changes per hour (ACHs) ratio, and IAQ burden), alarm escalation logic, and the M&V chronology (baseline period definition and baseline-model lock). Post-deployment, the same governance workflow reviewed dashboards, model diagnostics, and work-order outcomes on a fixed cadence to manage threshold updates and ensure that all changes remained traceable and auditable. During commissioning and ramp-up, and subsequent steady-state operation, stakeholders also validated semantic mappings, tuned alarm burden using confusion-matrix performance (false alarms vs. missed excursions), and approved Option-C M&V reporting packages (residual diagnostics and uncertainty bands) before operational changes or external communications.
3.3. Semantic Digital-Twin Layer: Ontology Grounding and Point Normalization
Figure S2 provides a concrete, Brick-consistent semantic graph that makes the “ontology-grounded” claim operational: it shows how heterogeneous BAS and BMS and IoT telemetry can be normalized into three interoperable layers—locations (ICU_Department containing OR_3 and AII_12), equipment (AHU_2 with its supply fan and downstream terminal VAVs), and points (ΔP sensors for critical rooms, AHU supply air temperature, and a whole-facility electricity meter)—connected by explicit relationships such as hasPart, feeds, hasPoint, and isPointOf. This structure demonstrates practical utility because it supports vendor-agnostic asset discovery and analytics binding (e.g., retrieving “all isolation and OR spaces with ΔP sensing” and automatically traversing to the serving VAV and upstream AHU for forecasting, excursion alarms, and work-order routing), while also preserving auditability for M&V by clearly separating a facility boundary meter from room and equipment telemetry. Overall, the panel turns an abstract semantic-layer description into a testable evidence artifact: it shows exactly what was measured, where it was measured, how assets were related, and how downstream services can query and act on those relationships without brittle naming conventions.
To enable deployment across heterogeneous BAS implementations, the platform normalizes BAS and BMS and IoT telemetry into an ontology-grounded semantic model of points, equipment, and spaces, constructed to be consistent with Brick. Brick provides a standardized vocabulary and relationship model so that applications can query building data semantically (e.g., ΔP points for AII spaces, whole-facility meters, equipment serving a zone) without relying on vendor-specific naming conventions. The semantic layer therefore functions as an explicit contract between raw telemetry and services for forecasting, optimization, and M&V. The semantic layer also supports stakeholder review and handover by providing a shared, auditable naming-and-relationship model for what was measured, where it was measured, and why it was used, reducing interpretation drift across engineering, clinical, and management audiences during post-deployment governance.
Where applicable, the semantic model is validated against schema and constraint expectations to reduce mapping errors that would otherwise propagate into compliance calculations, excursion alarms, or baseline modeling; this validation step is treated as a quality gate before downstream analytics are promoted to operational use. When a reliable as-built building information modeling (BIM) and Industry Foundation Classes (IFCs) are available, they can be linked to the semantic layer to enrich space geometry and adjacency and connectivity; when BIM is missing or obsolete (a common condition in existing hospitals), the Brick-grounded telemetry model remains sufficient for portable analytics, and BIM is not required for the evidence chain to function.
Extra data sources: (i) as-built floorplans (portable document format (PDF) and computer-aided design (CAD)) used to construct the floorplan-derived semantic graph (rooms and departments in normalized coordinates + adjacency and flow edges), optionally enriched by BIM and IFC when they exist. PDF/CAD floorplans were handled in ZWCAD (ZWSOFT Co., Ltd., Guangzhou, China) and BIM context was managed in the Glodon toolchain (Glodon Company Limited, Haidian District, Beijing, China); when openBIM exchange was required, models were exported from Autodesk Revit (Autodesk, San Francisco, USA) to IFC2x3/IFC4; (ii) BAS and BMS change logs (setpoint edits, logic revisions, and trend-point enable and disable) and CMMS work orders and tickets (fault and event counts, downtime hours, minutes-to-resolve, and closure evidence); (iii) whole-facility utility meter data (electricity kWh and kW, the Option-C boundary) plus the baseline-driver covariates used to lock the baseline model (e.g., weather, schedule, and occupancy proxies if used); (iv) IAQ and indoor environmental quality (IEQ) sensor streams (CO2 and PM2.5) and any complaint and service-burden logs used for “burden” endpoints; (v) grid emission factors (MEE and NCSC annual factors, plus any sensitivity factor, such as East China regional value) for Scope-2 mapping; (vi) CAPEX and economic appraisal inputs for M01–M06, ΔNPV, tornado, and Monte-Carlo (quotes and budgets, electricity price, discount rate, cost-per-event assumptions); and (vii) optimization and QA artifacts (solver configuration, run logs, hyperparameter sweep outputs, repeated-run distributions) that generate the scaling, Pareto sets, and QA heatmaps.
3.4. Construction and Control Design for Pressure-Relationship Reliability in Critical Rooms
Construction and retrofit design for critical spaces (with emphasis on AII and OR zones) focuses on sustaining directional airflow intent using supervisory logic that couples supply and exhaust actuation, differential-pressure (ΔP) sensing, door-status interlocks, and alarm logic integrated into the BAS and BMS. The operational intent for AII rooms is referenced to a continuous minimum negative pressure differential of −0.01 in. w.g. (inches of water gauge) (≈−2.5 Pa) relative to adjacent non-isolation areas, consistent with ASHRAE Standard 170 requirements for healthcare ventilation [35]. Alarm logic and escalation policies were agreed with clinical and facilities stakeholders to balance safety intent with nuisance-alarm control, and were evaluated quantitatively using excursion-detection outcomes and operational burden measures.
Performance evaluation uses both steady-state and transient metrics: (i) compliance fractions (time meeting pressure intent), (ii) ΔP distribution tightening under advanced operation, and (iii) transient control quality (overshoot, settling time, and integral absolute error) to evidence stability improvements that support sustained compliance rather than episodic pass conditions. Near-real-time telemetry ingestion supports timely detection of excursions and alarm governance, while the BAS and BMS maintains primary control authority to ensure safe operation under communication latency or analytics downtime.
3.5. Floorplan-to-Graph Abstraction for Department and Unit-Scale Coordination
To enable optimization and monitoring beyond single-room control, we converted hospital floorplans into a floorplan-derived semantic graph. Nodes represent rooms and departments positioned by normalized plan coordinates, and edges represent operational adjacencies “and” or “or” flow couplings used to encode constraints and movement and interaction structure. This graph representation supports (i) multi-objective optimization that trades energy and infection-risk proxies while respecting adjacency and flow structure, and (ii) scenario-consistent monitoring and governance across connected clinical zones. The graph is not treated as a visualization artifact; it is an operational substrate used to parameterize the optimizer and to standardize monitoring queries (e.g., all negative-pressure zones connected to corridor X).
3.6. Implementation Gating, Commissioning Logic, and Baseline-Model Lock
Execution followed a gated deployment sequence that explicitly preserves traceability between physical changes, analytics activation, and verified outcomes: design freeze → installation → functional testing → IoT go-live → baseline model lock → advanced optimization → post-implementation M&V [36]. The baseline model lock gate is treated as a methodological control to prevent retrospective tuning of baseline models after observing reporting-period performance. This gating also operationalizes auditability: each gate produces artifacts (configuration snapshots, mapping tables, model versions, and activation timestamps) that allow the reported post-period outcomes (energy residual shifts, compliance shifts, and fault burden changes) to be causally interpreted in relation to the deployment chronology.
3.7. Multi-Objective Optimization Formulation and Solver Families
Operational planning and decision support were framed as a multi-objective optimization problem balancing energy (and carbon-relevant) performance against an infection-risk index and operational feasibility. Feasible frontiers were summarized using energy–risk trade plots and Pareto-efficient subsets, as reflected in the figures. To assess scalability and decision quality, we benchmarked multiple solver families aligned with the figure comparisons: heuristic (Greedy), metaheuristic (simulated annealing (SA), and genetic algorithm (GA)), and (mixed-integer linear programming; MILP). Optimization workflows were implemented in Python (Python Software Foundation, Beaverton, OR, USA) using Pyomo (Sandia National Laboratories, Albuquerque, NM, USA) for MILP formulation, solved with representative MIP solvers (Gurobi Optimizer; Gurobi Optimization, LLC, Beaverton, OR, USA; v11.x; IBM ILOG CPLEX Optimization Studio; IBM, Armonk, NY, USA; v22.1.1; and COIN-OR CBC; COIN-OR Foundation, Inc., Towson, ML, USA) with run logs and solver parameters archived; QA experiments used the D-Wave Ocean stack and minorminer embedding tooling (D-Wave Quantum Inc., Palo Alto, CA, USA; with corporate operations also in Burnaby, BC, Canada) and sweeps over chain_strength, num_reads, and annealing_time consistent with the reported stability analysis. In addition, we evaluated QA as an exploratory solver family to provide a forward-looking baseline for structurally similar problems under emerging hardware constraints; importantly, for the problem sizes studied here, MILP is sufficient and consistently achieved the best (or best-observed) results, and is therefore the recommended approach for current deployments. Solver performance was characterized along four axes consistent with the presented panels: (i) optimality gap relative to the best observed solution as problem size increases, (ii) runtime scaling (seconds; log scale) versus the number of departments and rooms, (iii) feasibility and constraint behavior via a flow-penalty proxy in the cost–carbon trade space, and (iv) downstream decision operability using a bounded safety index (0–1) for the top-K solutions with component contributions (e.g., movement burden, adverse-pressure penalty, compliance).
For QA specifically, we treated the runs as sensitivity and stability experiments, rather than as a primary solver for the current instance sizes. We performed hyperparameter sweeps over anneal time (µs) and chain strength, and assessed sampling sensitivity across the number of reads to identify stable operating regions characterized by lower mean objective values and reduced variability. These QA results are reported to contextualize potential scalability pathways and to inform future hybrid workflows; they should not be interpreted as outperforming or replacing classical exact optimization for the present-scale instances.
3.8. Digital-Twin Forecasting, Prediction Intervals, and Excursion Alarm Governance
For representative negative-pressure zones, the digital twin generated ΔP forecasts with associated prediction intervals (95% interval as shown in the figure-based framing) and evaluated predicted and observed trajectories against an intent and alert threshold. This served two functions: (i) forward-looking screening for potential excursions to reduce operational risk and (ii) governance of alarm burden to avoid destabilizing staff workflow with excessive false positives. Excursion detection performance was evaluated using a confusion-matrix framework (normal vs. excursion), explicitly reporting false alarms and missed detections to support reproducible tuning of alarm thresholds and escalation logic.
3.9. Outcome Definitions and Pragmatic Operational Endpoints
Outcomes were defined to connect pressure reliability improvements to low-carbon operations and staff-facing workload reduction using the figure-specified constructs: Pressure-relationship reliability: weekly compliance fraction meeting pressure intent; ΔP distributions by scenario and space type; excursion minutes per day; and control transients (overshoot, settling time, and integral absolute error (IAE)). Ventilation delivery efficiency: ACH ratio (measured relative to minimum) using unity as the intent reference, explicitly distinguishing reliability from systematic excess ventilation (a decarbonization-relevant inefficiency). Indoor air quality burden: diurnal CO2 profiles and PM2.5 distributions, plus exceedance fractions treated as operational alarms and triggers, rather than compliance thresholds. Service burden: minutes-to-resolve distributions for cumulative distribution function (CDF), weekly fault-event counts by dominant fault type, and downtime hours, enabling separation of reliability gains from mere reporting changes. Integrated performance: composite index scores (0–1), scenario aggregation of time, burden, and carbon-intensity metrics, and waterfall decomposition attributing KPI shifts to energy, compliance, and fault-event deltas.
3.10. Whole-Facility Energy Measurement and Verification (IPMVP Option C Framing)
Table S2 reports the baseline model form, normalization variables, diagnostics (coefficient of variation of the root mean square error (CVRMSE) and normalized mean bias error (NMBE)), analysis periods (baseline vs. reporting), and the non-routine adjustment (NRA) protocol. Internet-sourced values provide locality-specific context (weather source, climate region, and grid factors). Energy impacts were quantified at the whole-facility boundary using an Option C-style M&V approach in which whole-facility energy and demand is continuously metered, a baseline model is calibrated and formally locked using version and lock metadata from the pre-intervention period, and reporting-period performance is evaluated as actual minus predicted residuals. Baseline adequacy screening followed the figure-aligned diagnostics, including (i) measured vs. baseline-predicted scatter with a 1:1 reference to assess agreement and (ii) residuals versus predicted energy to detect systematic bias or heteroscedasticity. For whole-facility claims, resolution evidence was compiled as a reporting package that pairs measured vs. predicted plots and residual diagnostics with weekly reporting-period electricity comparisons (metered consumption vs. baseline predictions) and uncertainty bands (e.g., p05–p95), alongside annotated non-routine events or interventions (e.g., control changes, major maintenance) to interpret residual shifts—typically negative divergence (savings-consistent behavior) under advanced deployment.
As the primary intervention targets local pressure-relationship reliability, the whole-facility energy signal can be small relative to normal facility variability. Consistent with common Option C guidance that whole-facility approaches are the most discriminating when savings are substantial (often cited as ~10–15% of total metered use when using coarse data), we therefore quantified savings with explicit uncertainty, rather than relying on a threshold alone. We used (i) interval-metered energy aggregated weekly, (ii) routine covariates (weather and degree-days and operational proxies such as occupancy or patient activity where available), (iii) a baseline-model lock to prevent post hoc tuning, and (iv) reporting-period prediction intervals (p05–p95). Savings are reported as a range and interpreted as savings-consistent when the reporting-period residual shift is meaningfully negative relative to model uncertainty (e.g., confidence bounds largely below zero or savings exceeding approximately two standard errors of the baseline prediction), with NRA applied if major operational changes occur (e.g., expansions, schedule changes, and clinical program shifts) [37].
3.10.1. Baseline Model Specification and Normalization Variables (Option-C)
We implemented a whole-facility IPMVP Option-C baseline calibrated exclusively on the pre-intervention period and applied it unchanged to the reporting period. Weekly whole-facility electricity consumption (kWh per week) was modeled as an additive function of weather and operational drivers to normalize routine variability. Weather drivers were computed from Hangzhou China Standard Weather Data (CSWD) and EnergyPlus Weather (EPW) hourly dry-bulb temperature and aggregated to weekly cooling and heating degree terms ( and ) using a stated base temperature. Operational normalization uses an occupancy and clinical-intensity proxy (e.g., bed-days, admissions, or staffed-bed occupancy), and calendar controls (e.g., holiday indicators and week structure) to capture systematic schedule effects.
where denotes the error term capturing unmodeled variation.
3.10.2. Baseline Adequacy Diagnostics and Acceptance Criteria (CVRMSE, NMBE)
Baseline adequacy was evaluated quantitatively using CVRMSE and NMBE computed over the baseline period residuals, and visually via measured-vs.-predicted and residual diagnostic plots. Let be the baseline prediction and be residuals over baseline observations; we report RMSE, CVRMSE (%), and NMBE (%) in standard form and compare them with stated tolerances consistent with established M&V practice (e.g., American Society of Heating, Refrigerating and Air-Conditioning Engineers (ASHRAE) Guideline 14 and Federal Energy Management Program (FEMP) guidance). For weekly aggregation, we state the chosen benchmark criterion explicitly (e.g., using monthly tolerances as a conservative reference) and report the achieved values.
where is the mean of measured over the baseline period and is the number of fitted model parameters (including the intercept).
3.10.3. Scope-2 Emissions Translation for Option-C Results: Grid Emissions-Factor Source, Temporal Resolution, and Accounting Convention
To translate the IPMVP Option-C whole-facility electricity outcomes (measured () and baseline-adjusted counterfactual ()) into operational carbon impacts, we apply the greenhouse gas (GHG) Protocol Scope-2 location-based method as the default reporting convention, i.e., grid-average emissions factor metered kWh at the whole-facility boundary. Consistent with Table S3, we do not claim a market-based Scope-2 result because no contractual instruments (e.g., energy attribute certificates and RECs, bundled green power contracts, or supplier-specific emission rates) were documented for the reporting window; therefore, all Scope-2 results reported in the main text are location-based. For the Hangzhou case (Hangzhou, Zhejiang Province; 1 July 2024–31 July 2025), the serving jurisdiction is treated as Zhejiang Province within the East China power-grid context, and the primary emissions-factor source is the official baseline emission-factor publication for regional power grids for reduction projects issued by China’s Ministry of Ecology and Environment (MEE) and National Climate Strategy Center (NCSC) (Table S3). The primary factor value used in the main results is the Zhejiang provincial grid-average emissions factor ( per ) (equivalently ). As the official MEE and NCSC factors are published at annual temporal resolution, is treated as piecewise-constant over the reporting interval and applied to electricity metering aggregated at the analysis cadence (weekly kWh).
Operational Scope-2 emissions are computed as
and avoided Scope-2 emissions attributable to the intervention are computed as
where is the annual factor mapped to each reporting week .
Regarding the sensitivity boundary specified in Table S3, we additionally report results using the East China regional grid factor ( per ) to bracket uncertainty arising from provincial versus regional aggregation and annual averaging. The Scope-2 accounting boundary is purchased electricity at the whole-facility meter; if on-site PV and DER are present, we report explicitly whether the electricity series is net-of-export or gross consumption and apply the same convention consistently to both baseline and reporting computations. Finally, the reported factor is -only when the official dataset provides factors; in that case, we state explicitly that non- gases ( and O) are not included and are not material at the purchased-electricity boundary, and we report e strictly according to the gas coverage provided by the source (Table S3). If an authoritative time-varying grid-emission series (hourly and daily) becomes available for the serving jurisdiction, we will adopt it by aligning the factor resolution to the metering interval (or aggregating the factor to match weekly kWh) and documenting the interpolation and aggregation method; otherwise, the annual-factor piecewise-constant approach above is retained for transparency and reproducibility.
3.11. Carbon Accounting and Low-Carbon Operational Metrics
We apply GHG Protocol Scope-2 location-based accounting [38]. Grid emissions factors were sourced from MEE and NCSC official baseline grid factors and were annual; therefore was treated as piecewise-constant over the reporting window and mapped to weekly kWh. Carbon outcomes were expressed both as annual absolute savings for tons of carbon dioxide-equivalent per year (tCO2e per year) and as facility-normalized intensity (CO2e per floor area) to support cross-scenario and cross-facility comparability. Candidate measures were prioritized using capital expenditure (CAPEX) vs. annual carbon savings plots (M01–M06: labels for candidate measures), and algorithm-driven candidate solutions were evaluated in the cost–carbon trade space as shown in the solver benchmarking figures. IPMVP sources emphasize the importance of clearly defined measurement boundaries and transparent reporting for whole-facility claims, which is directly operationalized here through baseline lock, residual diagnostics, and reporting-period uncertainty representation.
3.12. Fault Economics and Investment Appraisal Under Uncertainty
To quantify pragmatic value beyond energy, we enumerated dominant baseline fault drivers (e.g., belt slip, filter loading, valve leakage, damper faults, and variable frequency drive (VFD) hunting) and compared fault-event counts and downtime hours between baseline and post-periods. Avoided cost was estimated using project-specific cost-per-event assumptions and economic appraisal inputs applied to observed event reductions, yielding an operational economic signal aligned with staff burden reduction.
Investment decision support used (i) one-way sensitivity (tornado) analysis of delta net present value (ΔNPV and USD) relative to baseline to rank influential parameters (savings fraction, CAPEX, electricity price, baseline energy use intensity (EUI) and intensity, avoided events, cost per event, and discount rate), and (ii) probabilistic cost-effectiveness analysis via Monte Carlo simulation, reporting the incremental cost–effect plane (avoided adverse events per year vs. NPV of costs) and the cost-effectiveness acceptability curve (CEAC) across willingness-to-pay thresholds to support decisions under uncertainty.
3.13. Causal Inference: Interrupted Time Series and Difference-in-Differences
As randomized deployment is typically infeasible in CBD hospital retrofits, causal attribution was strengthened using two quasi-experimental estimators aligned with the figures: Interrupted time series (ITS): segmented regression of weekly pressure compliance with a clearly defined intervention boundary (dashed line), estimating a post-deployment level shift and slope change relative to pre-trends. DiD: treatment (post–pre) minus control (post–pre) for pressure compliance, IAQ exceedance fractions (CO2 and PM2.5), complaint burden, and energy (kWh per day), with sign conventions defined such that increased compliance and decreased exceedance and complaints and energy indicate improvement. This combined ITS and DiD framing supports pragmatic inference under real-world operational variability while maintaining traceability to the deployment gates and Option C whole-facility boundary.
3.13.1. Parallel-Trends Diagnostics and Event-Study Specification
We assessed the DiD identifying assumption (parallel trends) using pre-intervention diagnostics at the same temporal resolution as the main analysis (weekly). First, we plotted treated and control outcomes over the full baseline window (July 2024) and compared baseline slopes using (i) a simple linear pre-period trend regression and (ii) an event-study specification with leads and lags. We report (a) the joint F-test for the null that all lead coefficients are zero (no differential pre-trends), (b) lead-by-lead estimates with 95% confidence intervals, and (c) visual inspection of mean outcomes by group. To mitigate known issues with two-way fixed effects (TWFE) event studies under staggered adoption, we additionally report a heterogeneity-robust event-study estimator (interaction-weighted or group-time average treatment effect on the treated (ATT) aggregation) and include the estimator choice in the reproducibility checklist.
Model forms to report:
- Canonical DiD (panel):
- Event-study (dynamic DiD):
- Parallel-trends pretest: for all (joint F-test over leads)
The primary outcomes for the above diagnostics follow this paper’s causal endpoints: pressure compliance (0–1), IAQ exceedance fractions ( and ), complaint burden index, and whole-facility energy (kWh per day).
3.13.2. Control-Group Selection and Matching and Weighting
We made control selection clear to reduce confounding from non-comparable sites. Controls were selected from the same metropolitan area or climate zone (Hangzhou, Zhejiang, or matched subtropical humid region), with a similar hospital service mix and HVAC typology, and with no major retrofit and commissioning overlapping the reporting period. We document inclusion and exclusion criteria and provide a baseline balance table. Where multiple candidates existed, we applied matching and weighting on baseline outcomes and key covariates (weather, occupancy proxy, and operating schedule) using either propensity-score weighting or entropy balancing; the final matched set is the one used for difference-in-differences effects and related estimates.
3.13.3. Confounders, Non-Routine Adjustments, and Sensitivity Analyses
We explicitly enumerated potential confounders that could violate parallel trends or contaminate post-period attribution: COVID-like surges or program changes (intensive care unit (ICU) and OR case load), occupancy and visiting policy shifts, extreme weather weeks, major equipment replacement, tariff changes, and major BAS sequence changes unrelated to the intervention. We managed these using (i) a NRA log that flags weeks with material exogenous shocks and excludes them or includes indicator controls; (ii) sensitivity analyses that re-estimate effects after dropping flagged weeks; (iii) placebo tests using false intervention dates within the baseline; and (iv) alternative control definitions (nearest-neighbor and synthetic-weight control) to show the robustness of sign and magnitude.
3.14. Statistical Reporting, Comparability Controls, and Reproducibility
Where comparative groupings were presented (scenario-by-space strata; solver families), captions indicate letter-coded groupings for statistically distinguishable strata under the study’s multiple-comparison procedure. Predictive models were summarized using root-mean-square error (RMSE) (ppm for CO2; and particulate matter with aerodynamic diameter ≤ 2.5 micrometers (PM2.5 µg m−3)) by scenario to demonstrate improvements in monitoring fidelity that are necessary for auditable operational governance. Reproducibility controls were embedded in the method through (i) semantic model normalization (reducing site-specific interpretation risk), (ii) baseline-model lock (reducing analysis degrees of freedom), (iii) explicit residual diagnostics (screening baseline adequacy), and (iv) quantified alarm performance (confusion-matrix reporting for excursion detection). This expanded methods framework preserves the parameters and constructs, and is explicitly aligned to the stated contribution: Option-C-verified whole-facility energy and carbon performance alongside pressure-relationship reliability in a disruption-sensitive CBD hospital deployment context, with optimization, causal inference, and uncertainty-aware economic evaluation integrated as first-class methodological components.
4. Results
4.1. Semantic Cyber–Physical Digital Twin for Auditable Pressure Reliability and Low-Carbon Operations in CBD Hospitals
The schematic establishes an operational evidence chain that links physical-space sensing to cyber-space decision-making via sequential acquisition, preprocessing, integration, visualization, and service layers, with explicit assurance functions (information exchange, data quality, security, and auditability) that make control decisions traceable (Figure 1A). This framing aligns with recognized operational technology (OT) and industrial control systems (ICSs) security guidance that emphasizes risk-managed architectures, segmentation, and governance for safety- and reliability-critical control environments, and it is strengthened by the semantic layer that binds points, equipment, and spaces into a machine-actionable representation rather than vendor-specific naming (Figure 1B).
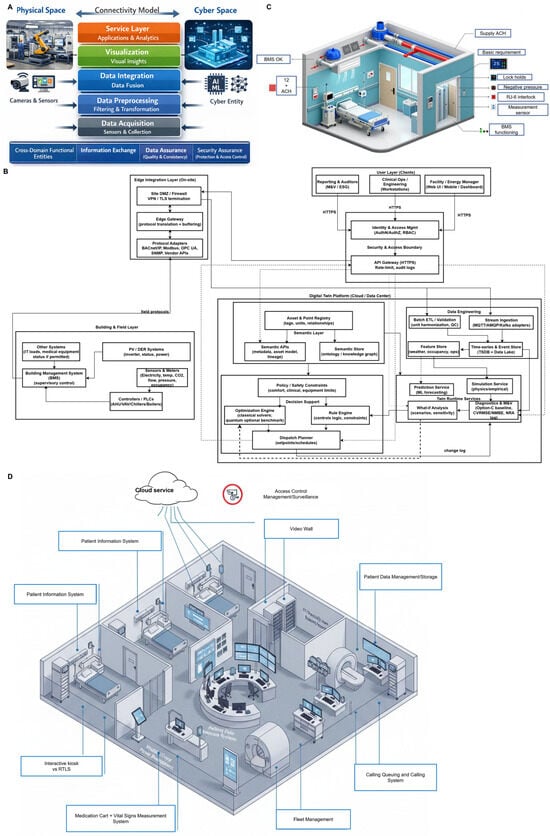
Figure 1.
Option-C-verified semantic digital-twin architecture in CBD hospitals. (A) Physical–cyber connectivity stack showing how field sensing becomes operational action: data acquisition → preprocessing → integration → visualization → service and applications, with cross-cutting controls for information exchange, data quality and assurance, security, and auditability so pressure and energy decisions remain traceable from raw points to analytics outputs. (B) Semantic digital-twin layer that standardizes heterogeneous BAS and BMS and IoT data into a unified semantic store and APIs (points–equipment–space relationships), enabling portable workflows for prediction and simulation, what-if analysis, and optimization and AI services, and interfacing with the building network and BMS for orchestration and deployment. (C) Critical-room (AII) example illustrating supervisory control for directional airflow using ΔP sensing, door and flow interlocks, and alarm logic, alongside ventilation delivery checks (e.g., ACH status), aligned with a continuous negative-pressure intent (minimum −0.01 in. w.g. ≈ −2.5 Pa relative to adjacent areas). (D) CBD hospital deployment context showing how the semantic twin links sensing, data management, analytics, and user interfaces across clinical rooms and shared services to coordinate reliability and decarbonization at whole-facility scale under dense siting and constrained plant and shaft conditions.
The clinical-space cutaway depicts how the architecture is operationalized for airborne infection isolation through coordinated supply and exhaust actuation, differential-pressure sensing, door-status interlocks, alarm logic, and BAS and BMS supervisory integration to maintain directional airflow under disturbance-prone conditions typical of dense CBD circulation patterns (Figure 1C). The depicted pressure-relationship intent is consistent with authoritative healthcare ventilation guidance that specifies maintaining continuous negative pressure on the order of 0.01 in. w.g. (2.5 Pa) relative to adjacent spaces and monitoring and documenting performance, while allowing alarm implementations that avoid nuisance without obscuring sustained loss of control. The department and unit-scale layout then provides the deployment context—shared services, centralized visualization, and data-management functions operating under constrained plant and shaft space and disruption-sensitive retrofit constraints, clarifying why the same auditable loop must jointly support reliability governance and low-carbon operational decision-making in CBD hospitals (Figure 1D).
4.2. Option-C-Verifiable Operational Impacts of Semantic Digital-Twin Deployment on Critical-Room Pressure Reliability, Ventilation Delivery Efficiency, and Service Burden
We first report this paper’s primary claim: Option C whole-facility verification of energy and carbon improvements co-occurring with improved pressure-relationship reliability and reduced service burden. Across critical rooms, the intervention period (S3) showed a marked improvement in pressure-relationship performance relative to baseline (S0). The weekly compliance pass rate increased from persistently low baseline values to a sustained higher regime after deployment (Figure 2A), consistent with tighter execution of directional-airflow intent required for AII operation (e.g., continuous negative pressure on the order of 2.5 Pa relative to adjacent spaces). The ΔP distributions by scenario and room type further indicated that S3 reduced dispersion and center operation closer to the intended pressure relationships in both AII and OR strata, with letter groupings separating statistically distinct condition–space combinations (Figure 2B, p < 0.05). In parallel, the ACH ratio histograms show that S3 concentrated measured ventilation delivery nearer unity (measured and minimum ≈ 1) and reduced high-excess outliers compared with S0 (Figure 2C), indicating improved control that avoided reliability by over-ventilation. Classification performance for operational state detection also improved under S3 (area under the curve (AUC) 0.696 vs. 0.649 in S0; Figure 2D), supporting the interpretation that the intervention improved both physical control outcomes and the observability needed for reliable operational governance.
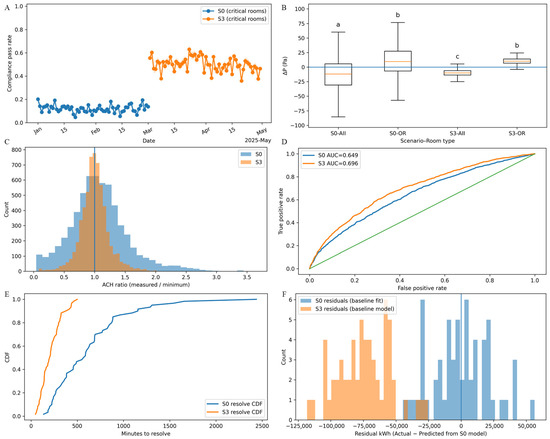
Figure 2.
Option-C outcomes of the smart-hospital intervention. (A) Weekly critical-room pressure-relationship compliance pass rate comparing baseline (S0) with intervention (S3), showing a discrete and sustained post-deployment uplift in compliance fraction. (B) Room-to-corridor differential pressure (ΔP, Pa) distributions by scenario and space type (AII and OR), demonstrating tighter control and reduced dispersion under S3; letters denote statistically distinguishable strata. Bars annotated with different letters (a, b, and c) indicate statistically significant pairwise differences between scenarios (p < 0.05), whereas bars sharing the same letter indicate no significant difference (p > 0.05). (C) ACH ratio (measured and minimum) histograms with unity reference, indicating that S3 concentrates operation nearer intent while reducing high-excess outliers (i.e., reliability without systematic over-ventilation). (D) Receiver operating characteristic (ROC) curves for operational-state classification (e.g., compliant vs. noncompliant), reporting improved discrimination under S3. The green diagonal line indicates the no-discrimination (random-classifier) reference (AUC = 0.5). (E) Minutes-to-resolve distribution (CDF) showing reduced long-tail resolution times under S3—an operational reliability and staff-burden outcome. (F) Whole-facility energy residuals (kWh; actual minus S0-calibrated baseline prediction) shifting negative in S3, consistent with Option-C whole-facility savings inference when normalized against baseline drivers.
The intervention also reduced operational friction and supported whole-facility energy inference under a whole-facility M&V framing. Minutes-to-resolve curves shifted left under S3, with a substantially shorter long-tail of slow-to-close issues (Figure 2E), consistent with lower staff-facing service burden and faster containment of performance excursions. Finally, the whole-facility energy residual distributions (actual minus baseline-predicted from an S0-calibrated model) shifted negative under S3, while S0 residuals remained centered near the baseline fit (Figure 2F), a pattern consistent with net energy savings evaluated at the facility boundary in an Option-C (whole-facility) measurement-and-verification construct where baseline and reporting-period utility and meter data were compared with appropriate adjustments.
Resolution Evidence Examples
To demonstrate closure from analytics to operational outcomes, we report representative evidence packets that link (i) the trigger (ΔP excursion or model residual), (ii) the intervention (controls adjustment and/or work order), and (iii) verification (post-action compliance, excursion minutes, alarm performance, and, where applicable, Option-C residual shifts with uncertainty).
Case 1 (Pressure reliability): excursion → alarm → action → verified recovery
A representative AII and OR packet illustrates how negative-pressure intent is protected in use. An excursion is detected when ΔP crosses the intent threshold, generating an actionable alert through the service layer. The event is triaged as a control issue or a maintenance issue, triggering a BAS adjustment and/or a work order with a timestamped record. Verification is reported over a defined post-action window: ΔP distribution tightening toward intent, reduced excursion minutes per day, and increased weekly compliance for the affected space. Alarm governance is reported using confusion-matrix accounting (TP, FP and FN) to justify threshold choices and avoid nuisance escalation.
Case 2 (Service burden): fault detected → work order → resolution and recurrence reduction
A representative fault-resolution packet shows operational uptake. A fault signature (e.g., damper and valve faults, filter loading, or VFD hunting) is detected and routed to the issue-resolution workflow. The work order documents the action taken. Verification reports the resolution window and recurrence tracking: shorter time-to-resolve and reduced repeat events for the same asset and zone within a defined window.
Case 3 (Whole-facility M&V): reporting-week residual shift aligned with an intervention
A representative Option-C packet connects operational changes to whole-facility verification. The pre-intervention baseline model (locked per the commissioning gate) generates adjusted baseline predictions for the reporting week. Metered energy is compared to predictions with uncertainty bands, and the residual is tracked as a savings-consistent shift. The packet annotates a temporally aligned intervention and reports residual diagnostics to avoid attributing savings to model artefacts.
4.3. Resolution Evidence Shows Closed-Loop Operational Uptake
The event packets demonstrate a repeatable closure loop: operational triggers (ΔP intent breaches, covariance-normalized residual anomalies, and equipment-fault conditions) are converted into actions (BAS control and setpoint changes and computerized maintenance management system (CMMS) work orders) and then verified within a predefined window using the same outcome constructs reported in this paper (compliance fraction, excursion minutes per day, transient stability, alarm true positives (TPs), false positives (FPs)m and false negatives (FNs), and whole-facility Option-C residual shifts with uncertainty bands) (Table S4). The consistent post-action pattern is tighter ΔP behavior with fewer excursions and reduced service burden, while whole-facility residuals remain negative and diagnostically stable when temporally aligned with interventions, supporting both auditable safety governance and credible energy and carbon claims.
4.4. Semantic Graph-Driven Asset Discovery Enabled Portable Analytics and Verification
The ontology-grounded semantic layer provided a concrete mechanism for portable asset discovery and configuration: forecasting and compliance services retrieved AII-room differential-pressure points and related airflow assets via semantic queries; optimization services obtained department adjacency and flow–constraint relationships from the same graph; and M&V services consistently identified whole-facility utility meters defining the Option-C boundary without hard-coded site naming rules. This semantic contract reduced mapping ambiguity across heterogeneous BAS implementations and supported end-to-end deployment of analytics, optimization, and verification workflows, contributing to improved pressure-compliance performance and tighter ΔP control under the intervention state, with whole-facility savings assessed using Option-C-style metered energy and baseline regression under reporting-period conditions.
4.5. Semantic Digital-Twin Optimization and Monitoring for Pressure-Reliable, Low-Carbon Hospital Operations
The semantic digital twin first operationalizes hospital topology as a floorplan-derived graph in which rooms and departments are positioned in normalized plan coordinates and connected by adjacency and flow edges, creating an explicit constraint substrate for planning and surveillance (Figure 3A). On this semantic substrate, multi-objective optimization exposes a measurable energy–infection risk trade space (MWh and month versus risk index; lower values are better), with classical and quantum solution clouds and their Pareto-efficient subsets delineating the achievable reliability–energy frontier under CBD-scale constraints (Figure 3B). Computational scaling results then connect decision quality to tractability: as the number of departments and rooms increases, classical runtime rises sharply relative to quantum runtime on a log scale, while a companion optimality-gap proxy reports the solution-quality behavior that accompanies scaling (Figure 3C). QA configuration is treated as an experimental design problem, rather than a fixed choice: a sweep across anneal time and chain strength identifies a best-observed objective region for deployment-candidate selection, supporting repeatable solver operation rather, than one-off tuning (Figure 3D).
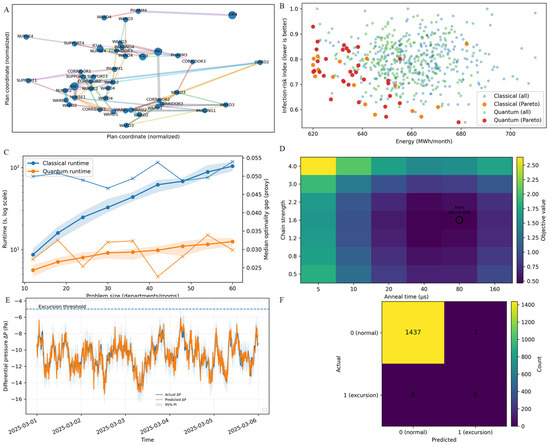
Figure 3.
Semantic digital-twin optimization and monitoring for hospital operations. (A) Floorplan-derived semantic graph of departments and rooms (nodes in normalized plan coordinates) with edges encoding adjacency and flow constraints used by the optimizer and monitoring logic. (B) Energy–infection-risk trade space from multi-objective optimization (MWh and month vs. risk index; lower values are better) comparing classical and quantum solution sets and Pareto-efficient fronts, exposing reliability–energy co-optimization structure. (C) Computational scaling with problem size (departments and rooms): classical versus quantum runtimes (log scale) with a companion optimality-gap proxy to summarize speed–quality behavior as the CBD hospital planning instance grows. (D) Quantum-annealing hyperparameter sweep (annealing time vs. chain strength) identifying the best-observed objective configuration for deployment-candidate solution selection. (E) Digital-twin forecasting of ΔP in a representative negative-pressure zone with prediction interval and intent threshold, supporting continuous monitoring against healthcare pressurization targets. (F) Confusion-matrix evaluation of excursion detection (normal vs. excursion), quantifying false alarms and missed detections for operational alarm governance.
The same semantic twin is then used for continuous operational governance in pressure-critical zones. A representative negative-pressure zone shows close agreement between observed and predicted differential pressure (ΔP) with an explicit 95% prediction interval and an intent and alert reference line, enabling real-time detection of drift and early warning before control failure becomes operationally material (Figure 3E). This monitoring loop is aligned with healthcare pressurization requirements that call for continuous negative-pressure relationships and periodic and continuous verification (e.g., minimum −0.01 in. w.g. ≈ −2.5 Pa for AII rooms relative to adjacent areas, with documented monitoring), making the forecast-and-threshold construct directly interpretable as compliance-grade operational evidence, rather than ad hoc analytics (Figure 3E). Finally, excursion classification performance is summarized with a confusion matrix that quantifies false alarms and missed detections—an explicit governance metric for staff-facing alarm burden and safety risk—thereby closing the loop from semantic representation to optimization to auditable, low-burden operational surveillance (Figure 3F).
Figure S3 presents solver benchmarking for CBD-scale, multi-objective low-carbon hospital planning and shows why algorithm choice is governance-relevant under audit and clinical constraints. As instance size increases, heuristic and metaheuristic baselines—Greedy, SA, and GA—exhibit progressively larger optimality gaps, whereas MILP remains the strongest performer for the evaluated scales by maintaining the tightest gaps to best-observed solutions and therefore the most defensible carbon–reliability tradeoffs (Figure S3A). Runtime scaling on a log-seconds axis clarifies the tractability envelope, indicating when exact methods versus approximate methods can support periodic re-optimization versus near-real-time replanning (Figure S3B). The cost–carbon trade cloud further demonstrates that solver family can shift the feasible frontier itself, not merely objective values, with feasibility made explicit via flow-penalty (constraint-violation) encoding to distinguish genuine improvements from solutions that erode constraint satisfaction (Figure S3C). QA is retained as an exploratory comparator whose relative performance depends strongly on sampling configuration; the sensitivity heatmap (chain strength by number of reads) identifies stable operating regimes and saturation zones required for reproducible use (Figure S3D). Robustness is summarized by repeated-run optimality-gap distributions, separating variance-prone from consistently tight methods and indicating statistically distinguishable groupings where applicable (p < 0.05) (Figure S3E). Finally, the safety-index decomposition translates optimization outputs into owner- and clinical-facing decision metrics—movement burden, adverse-pressure penalty, and compliance contributions—reinforcing the central interpretation that solver selection shapes feasibility, reproducibility, and interpretability alongside energy and carbon outcomes (Figure S3F).
4.6. Integrated Option-C M&V, Fault Economics, and Carbon Prioritization for Decarbonized, Pressure-Reliable Operations
The figure consolidates a governance-grade chain from whole-facility verification to space-level reliability (Figure 4A), aligning with IPMVP Option C (Whole Facility) practice where savings are inferred from whole-facility metered data across baseline and reporting periods with appropriate adjustments, rather than from isolated component measurements. Reliability gains are then summarized without selective sampling via mean excursion minutes per day by room type (AII and OR) and scenario, including pass fractions and statistically distinct strata (Figure 4B). This representation is directly interpretable against healthcare pressurization intent for AII rooms (e.g., continuous minimum differential pressure on the order of −0.01 in. w.g. = −2.5 Pa between AII and adjacent non-AII spaces), where reduced excursion time is a pragmatic indicator of sustained directional-airflow control, rather than sporadic compliance. Mechanistically, the transient-control metrics—overshoot, settling time, and integral absolute error—provide engineering evidence that the post-deployment system is more stable and therefore more capable of maintaining the intended pressure relationships under disturbances (Figure 4C), strengthening the causal plausibility that observed reliability improvements are control-enabled, rather than artifact-driven.
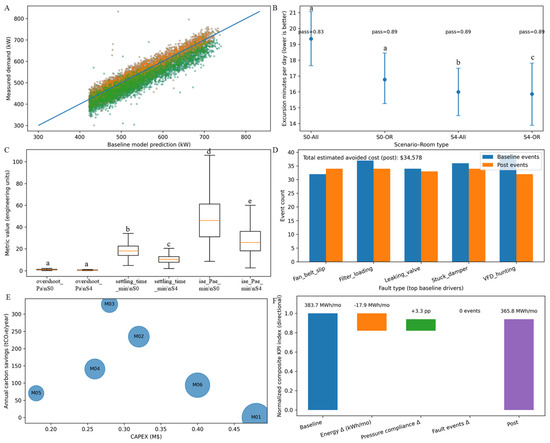
Figure 4.
Integrated Option-C M&V, fault economics, and carbon prioritization. (A) Whole-facility demand (kW) measured versus baseline model prediction with 1:1 reference, supporting Option-C whole-facility baseline adequacy screening prior to savings attribution. Blue/teal points denote all sampled interval observations (baseline + post combined), orange points denote baseline-period intervals (S0_baseline), and green points denote reporting/post-period intervals (S4_post). (B) Mean excursion minutes per day (lower values are better) by scenario and room type (AII and OR), with pass fractions and statistically distinct groups to summarize reliability improvement without selective sampling. Letters (a–c) indicate post-hoc multiple-comparison groupings: groups sharing a letter are not significantly different, whereas different letters denote statistically significant differences (α = 0.05, multiplicity-adjusted). (C) Pressure-control transient metrics (overshoot, settling time, and integral absolute error) comparing baseline and post-deployment operation, evidencing improved closed-loop stability that underpins sustained compliance. Bars annotated with different letters (a, b, c, d, and e) indicate statistically significant pairwise differences between scenarios (p < 0.05), whereas bars sharing the same letter indicate no significant difference (p > 0.05). (D) Fault-event counts for dominant baseline fault drivers (e.g., belt slip, filter loading, valve leakage, damper faults, and VFD hunting), contrasting baseline versus post to quantify maintenance burden reduction and avoided cost. (E) Portfolio CAPEX versus annual carbon savings (tCO2e per year) for candidate measures (M01–M06), enabling CBD-appropriate investment sequencing under retrofit constraints. (F) Waterfall decomposition of normalized composite KPI from baseline to post, attributing net change to energy, pressure compliance, and fault-event deltas to connect reliability governance to decarbonization outcomes. Colors denote components of the decomposition: baseline (blue), energy contribution (orange), pressure-compliance contribution (green), fault-event contribution (purple), and the resulting post level (light purple).
The operational value proposition is completed by connecting reliability governance to maintenance burden, investment sequencing, and decarbonization outcomes. Fault-event counts for dominant baseline drivers (e.g., belt slip, filter loading, valve leakage, damper faults, or VFD hunting) are contrasted between baseline and post-periods to quantify service burden reduction and avoided cost (Figure 4D), moving beyond energy-only claims to capture staff-facing impacts. Candidate decarbonization measures are then prioritized using a CAPEX versus annual carbon-savings portfolio view (Figure 4E), a CBD-relevant decision structure when retrofit scope is constrained and sequencing must balance disruption, capital limits, and carbon yield. Finally, the normalized composite KPI waterfall attributes the net baseline-to-post change to energy, pressure-compliance, and fault-event deltas (Figure 4F), creating a single auditable bridge from Option-C-verifiable whole-facility performance to the operational mechanisms (pressure stability and reduced faults) that plausibly drive durable low-carbon, pressure-reliable outcomes. IPMVP is maintained and published by the Efficiency Valuation Organization (EVO), which frames Option C as a whole-facility approach appropriate for multi-measure, interacting operational programs of the type shown here.
4.7. Deployment-Maturity Gains in Time-to-Value, Operational Burden, and Facility-Normalized Carbon Intensity Under Option-C-Verifiable Governance
Across the staged deployment maturity (S0→S3), the scenario-aggregated metrics exhibited consistent, directional improvements that were characteristic of an intervention moving from baseline operations toward evidence-grade digital-twin governance. The study-defined time-to-value metric declined monotonically in months (Figure 5A), indicating that higher semantic and analytics maturity compressed the time required to reach verified operational benefit, rather than merely shifting mean performance. In parallel, the burden fraction decreased across scenarios (Figure 5B), consistent with reduced time spent in undesired operational states under advanced monitoring and control. These maturity-linked reliability gains align with facility-normalized decarbonization: carbon intensity (tCO2e m−2) decreased from S0 to S3 (Figure 5C), demonstrating that improved governance can couple pressure–reliability objectives to measurable low-carbon outcomes at the building scale. The years-scale horizon metric on a log axis compressed strongly across scenarios (Figure 5D), indicating that advanced deployment disproportionately reduced long-tail exposure to adverse regimes—an important property for hospital operations where infrequent but persistent degradation can dominate risk and cost. This whole-facility, maturity-to-outcome framing is consistent with IPMVP’s articulation of whole-facility measurement and analysis under Option C, as maintained by the Efficiency Valuation Organization (EVO).
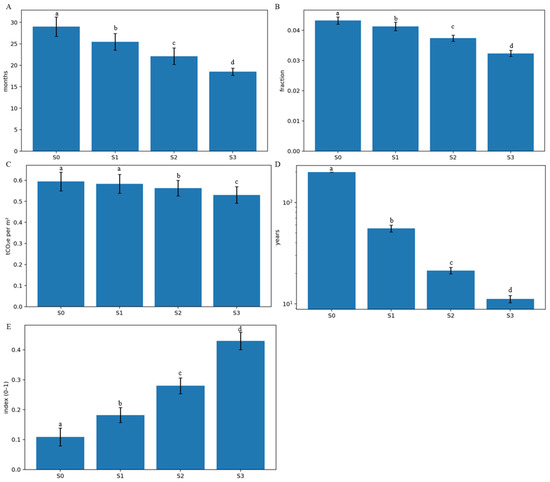
Figure 5.
Scenario-wise deployment maturity effects on time-to-value, burden, and carbon intensity. (A) Scenario-stratified time metric (months; study-defined) showing monotonic reduction from S0→S3, consistent with shorter time-to-verified benefit under higher digital-twin maturity. (B) Scenario-stratified burden fraction (study-defined), decreasing across S0→S3, reflecting reduced time-in-state of undesired operational conditions under advanced governance. (C) Carbon-intensity outcome (tCO2e per m2; facility-normalized) decreasing across scenarios, aligning reliability gains with operational decarbonization. (D) Years-scale horizon metric (log scale; study-defined), compressing across S0→S3 to indicate reduction in long-tail exposure to adverse operational regimes. (E) Composite index score (0–1; bounded), increasing across S0→S3 as an integrated summary of reliability, carbon, and service burden performance; error bars denote variability and letters indicate statistically distinguishable scenario groups. Bars annotated with different letters (a, b, c, and d) indicate statistically significant pairwise differences between scenarios (p < 0.05), whereas bars sharing the same letter indicate no significant difference (p > 0.05).
The composite index consolidates these dimensions into an integrated performance signal and reinforces those improvements that are not isolated to a single metric class. The bounded composite index (0–1) rose monotonically from S0 to S3 (Figure 5E), demonstrating that reliability, carbon, and service-burden improvements co-occur, rather than trade off in aggregate. Error bars indicate variability that remains explicitly represented (rather than hidden through selective reporting), while letter annotations denote statistically distinguishable scenario groupings, supporting the interpretation that the observed monotone trends are not driven by overlapping uncertainty alone (Figure 5E). Together, Figure 5 operationalizes a key building-science claim for CBD hospitals: semantic digital-twin maturity can be evaluated not only by technical capability, but also by progressive compression of time-to-verified benefit, reduction of operational burden and tail risk, and facility-normalized decarbonization outcomes that remain compatible with whole-facility verification practice.
4.8. Identification and Robustness Diagnostics for DiD and ITS
Across the five outcomes, Figure S4 shows treated and control trajectories that are broadly comparable in the baseline window, followed by a coherent post-intervention divergence aligned with the hypothesized intervention mechanisms (e.g., improved pressure compliance and reduced IAQ exceedances with concurrent changes in whole-facility energy). Figure S5 formalizes this by reporting event-study lead coefficients that were jointly near zero prior to intervention for most endpoints, supporting the parallel-trends assumption, while post-period lags reveal the timing and persistence of effects (whether immediate, ramping, or stabilizing). Figure S6 further strengthens attribution by placing the observed estimate relative to a placebo distribution generated from false intervention dates; an observed effect that lies in the tail of the placebo distribution indicates that the post-period shift is unlikely to be explained by generic time variation alone. Figure S7 confirms that the treated and control groups are made comparable through explicit matching and weighting, with post-adjustment SMDs reduced below the prespecified balance threshold, limiting confounding from observable differences. Finally, Figure S8 provides an alternative-control robustness check: a synthetic control that closely tracks treated outcomes in the baseline period but diverges after intervention supports the interpretation that the measured effect is intervention-linked, rather than an artifact of control selection.
Table S5 makes the control construction reproducible by documenting candidate controls, inclusion and exclusion criteria (region and climate comparability, service and HVAC similarity, and continuous data availability), and screening for overlapping retrofits, thereby reducing selection ambiguity and clarifying the final control set used in DiD and ITS estimation. Table S6 quantifies baseline comparability by listing treated vs. control characteristics and baseline outcome statistics alongside standardized differences and (where appropriate) inferential tests; the post-adjustment balance supports the validity of cross-group comparison and complements the graphical evidence. Table S7 consolidates parallel-trends diagnostics into a compact summary—baseline slope differences and joint lead tests—highlighting which outcomes clearly pass and which are borderline and therefore require bounded-sensitivity interpretation (e.g., additional robustness, alternative controls, or conservative confidence intervals). Table S8 operationalizes confounding management by enumerating non-routine events and potential confounders (weather extremes, maintenance, operational surges, and unrelated BAS changes), specifying how each is handled (exclusion, indicator controls, or documented non-routine adjustment), and linking each entry to an evidence artifact ID, which connects causal inference validity to the same audit trail logic used in Option-C measurement and verification.
4.9. IAQ Burden and Health-Risk Proxy Outcomes Under Progressively Decarbonized, Pressure-Reliable Operation
The IAQ burden metrics show a consistent improvement with advanced operation, indicating that reliability-oriented digital-twin control can reduce exposure without relying on over-ventilation. Diurnal CO2 profiles were lower under the advanced intervention (S3) than those under the baseline (S0), with reduced daytime elevations (Figure 6A), consistent with improved ventilation and flow management when CO2 was interpreted as an operational indicator in context (rather than as a standalone safety threshold). PM2.5 distributions decreased progressively from S0 to S3, with both central tendency and spread reduced (Figure 6B), aligning the operational trajectory with widely used public-health reference guidance that treats PM2.5 reduction as a core exposure risk objective (Figure 6B). Consistently, the model-based expected adverse-case burden per 8 h window decreased monotonically from S0→S3 (Figure 6C), reinforcing that the observed reductions in pollutant burden plausibly translated to reduced exposure-driven risk, rather than only shifting averages.
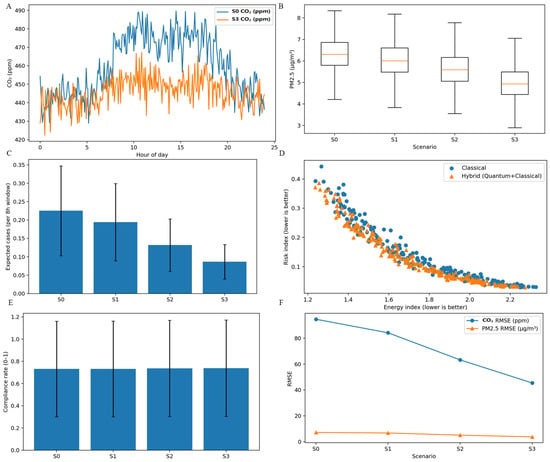
Figure 6.
IAQ burden and health-risk proxy outcomes. (A) Diurnal CO2 profiles (ppm) comparing baseline (S0) with advanced intervention (S3), showing reduced daytime elevations consistent with improved ventilation and flow management. (B) PM2.5 distributions (µg m−3) by scenario (S0–S3), indicating progressive reduction in central tendency and spread. (C) Expected adverse-case burden (per 8 h window; model-based) decreasing from S0→S3, consistent with reduced exposure-driven risk under improved control. (D) Energy–risk trade space (normalized indices; lower values are better) comparing classical optimization with hybrid quantum + classical solutions, showing movement toward more favorable Pareto regions. (E) Aggregate compliance rate (0–1; study-defined indoor environmental quality (IEQ) and indoor air quality (IAQ) compliance construct) remaining stable across scenarios, indicating that burden reductions are not achieved by relaxing compliance criteria. (F) Prediction accuracy by scenario (RMSE for CO2 and PM2.5), improving across S0→S3, consistent with higher-fidelity monitoring that supports auditable operational governance.
The optimization and prediction panels connected these IAQ gains to decision quality and governance readiness. The energy–risk trade space (normalized indices) showed hybrid quantum + classical solutions shifting toward more favorable Pareto regions relative to classical solutions (Figure 6D), consistent with multi-objective building-operation formulations where frontier movement represents genuine co-optimization, rather than single-metric tuning. Importantly, the aggregate IEQ and IAQ compliance construct remains broadly stable across scenarios (Figure 6E), supporting the interpretation that burden reduction is achieved through improved control and coordination, rather than relaxed compliance criteria. Finally, prediction fidelity improves with deployment maturity: RMSE decreased for both CO2 and PM2.5 from S0 to S3 (Figure 6F), which strengthened the auditable operations argument by reducing uncertainty in monitoring-driven alarms and inferences while preserving the need to interpret CO2 appropriately within building context.
4.10. Whole-Facility-Verified Causal Attribution and Health-Economic Decision Support for Semantic Digital-Twin Deployment
The causal evidence chain links a policy-relevant intervention boundary with sustained operational change under whole-facility verification. An interrupted time-series with segmented fits shows a clear treated-arm-level shift and persistence after the intervention date, while the control arm remains near its counterfactual trajectory (Figure 7A), consistent with best practice for evaluating interventions implemented at a defined point in time. Complementing the time-series view, difference-in-differences (DiD) summarizes the net treated-versus-control change across multiple endpoints—pressure compliance, CO2 exceedance, PM2.5 exceedance, complaint burden, and energy (kWh per day)—with beneficial effects expressed as increased compliance and decreased exceedance and complaints and energy (Figure 7B). Strategy-level distributions indicate that, for room-level pressure compliance in this sample, baseline, classical, quantum, and hybrid deployments were not detectably different (shared letter group), implying that the causal gains in (Figure 7A,B) were not driven by a single strategy’s superiority on this endpoint alone, but by the broader deployment and governance construct (Figure 7C). This causal framing was materially strengthened when paired with whole-facility M&V logic (Option C) that relies on facility-level metered energy and demand, and baseline vs. reporting-period analysis with routine and non-routine adjustments, which is the intended use-case for multi-measure operational programs, such as digital-twin deployments.
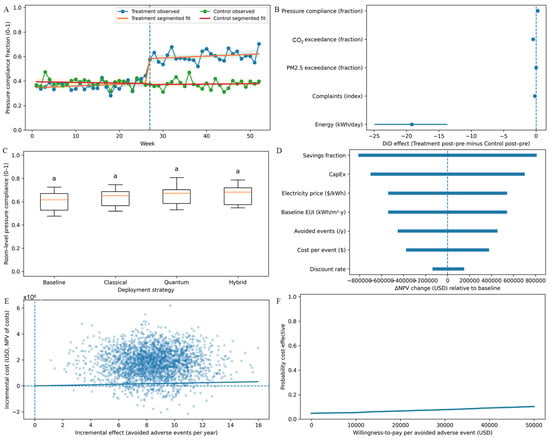
Figure 7.
Causal attribution and health economic evaluation of deployment strategies. (A) Interrupted time-series view of weekly pressure compliance (0–1) for treatment versus control with segmented fits; the intervention boundary (dashed line) shows a treated-arm-level shift and sustained improvement relative to counterfactual trend. (B) Difference-in-differences effects (treatment post–pre minus control post–pre) for pressure compliance, CO2 exceedance, PM2.5 exceedance, complaint burden, and energy (kWh per day), where beneficial impacts correspond to increased compliance and decreased exceedance, complaints and energy. (C) Room-level pressure compliance distributions by deployment strategy (baseline, classical, quantum, and hybrid), summarizing comparative performance; identical letter groups indicate no detectable between-strategy differences for this endpoint in this sample. Bars sharing the same letter indicate no significant difference (p > 0.05). (D) Tornado sensitivity of ΔNPV (USD) relative to baseline, ranking dominant drivers (savings fraction, CAPEX, price, baseline intensity, avoided events, cost per event, and discount rate) to support decision robustness. (E) Probabilistic cost-effectiveness plane (incremental effect vs. incremental cost; Monte Carlo), quantifying uncertainty around avoided adverse events and net costs. (F) Cost-effectiveness acceptability curve showing probability of cost-effectiveness versus willingness-to-pay per avoided adverse event, enabling policy and owner decisions under uncertainty.
The economic modules translate causal effects into investment robustness and decision thresholds appropriate for capital-constrained CBD hospital retrofits. One-way sensitivity (tornado) analysis ranks the dominant drivers of ΔNPV relative to baseline—savings fraction, CAPEX, electricity price, baseline intensity, avoided events, cost per event, and discount rate—so the financial case can be stress-tested against the few parameters that actually govern decision risk (Figure 7D). A probabilistic cost-effectiveness plane then propagates uncertainty via Monte Carlo sampling to jointly characterize incremental costs (NPV) and incremental effects (avoided adverse events per year), enabling the interpretation of whether the intervention is expected to be more effective and/or more costly under uncertainty (Figure 7E). Finally, the cost-effectiveness acceptability curve (CEAC) reports the probability the intervention is cost-effective across willingness-to-pay thresholds per avoided adverse event—an established presentation for decision-making under uncertainty—clarifying how adoption likelihood changes as the decision-maker’s value-of-outcome assumption varies (Figure 7F).
4.11. Deployment Gating and Option-C Post-Implementation M&V for Verified Energy Savings, Improved IEQ, and Reduced Service Burden
The following figure establishes an auditable implementation-to-outcome chain that is suitable for whole-facility verification claims. The deployment is structured as explicit readiness gates (design freeze → installation → functional testing → IoT go-live → baseline model lock → advanced optimization → post-implementation M&V), enabling traceability from commissioning-grade completion to performance reporting (Figure 8A). The core verification evidence then follows an IPMVP Option-C (whole-facility) logic—metered weekly electricity is compared against a baseline-predicted counterfactual with an uncertainty band—so savings are inferred at the whole-facility measurement boundary, rather than attributed to isolated components, which is appropriate for multi-measure operational programs with interactive effects (Figure 8B).
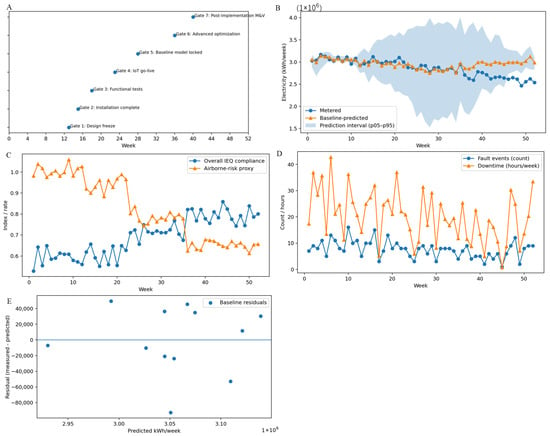
Figure 8.
Deployment gating and Option C post-implementation M&V evidence chain. (A) Week-indexed implementation gates from design freeze through installation, functional tests, IoT go-live, baseline model lock, advanced optimization, and post-implementation M&V, providing an audit trail from deployment readiness to verified outcomes. (B) Weekly electricity use: metered versus baseline-predicted with prediction interval, illustrating divergence from counterfactual baseline during the reporting period consistent with whole-facility Option-C verification practice. (C) Longitudinal IEQ compliance and airborne-risk proxy trajectories showing an operational regime shift toward higher compliance and lower risk proxy after advanced deployment. (D) Weekly fault events and downtime hours, quantifying maintenance burden and operational disruption and supporting attribution of value through reduced service load. (E) Baseline residual diagnostics (measured minus predicted vs. predicted), screening bias and heteroscedasticity to support credible savings inference at the whole-facility boundary.
Beyond energy, the figure shows that operational decarbonization is coupled to indoor-environment outcomes and service delivery impacts rather than achieved through hidden tradeoffs. Longitudinal trajectories indicate a regime shift toward higher IEQ compliance alongside a lower airborne-risk proxy after advanced deployment, supporting the claim that performance gains are compatible with indoor environmental quality objectives (Figure 8C). IEQ is explicitly a multi-domain construct encompassing IAQ and control performance, making it an appropriate umbrella metric when linking building operations to occupant-facing outcomes (Figure 8C). The service-burden panel operationalizes maintainability: weekly fault-event counts and downtime hours quantify maintenance load and disruption, enabling value attribution through reduced service demand, rather than reporting-period artifacts (Figure 8D). Baseline-model residual diagnostics (measured minus predicted vs. predicted) provide an additional credibility screen for bias and heteroscedasticity, strengthening the defensibility of post-period divergence as true savings, rather than model artifacts (Figure 8E). Figure 8 presents a deployment governance pattern aligned with building decarbonization practice—verified whole-facility energy improvements with concurrent IEQ and service-burden co-benefits—supporting the title’s emphasis on Option-C-verified, pressure-reliable decarbonized operations in dense hospital settings.
5. Discussion
The observed improvements in compliance, excursion management, and service burden were supported by structured stakeholder workflows that translated analytic outputs into operational actions (controls adjustments and work orders) and provided a controlled mechanism for threshold and logic updates without undermining auditability. A limitation is that we did not quantify stakeholder experience as a primary endpoint (e.g., formal surveys); future work could explicitly evaluate usability, trust, and/or organizational adoption alongside technical KPIs. These results are intended to support stakeholder decision-making, rather than retrospective reporting only. The evidence chain was designed to translate model outputs into actionable operational artifacts—dashboards for compliance and excursions, alarm escalation rules, and work-order workflows—so that facilities teams and clinical safety stakeholders can respond to excursions and verify sustained performance under a whole-facility M&V framework. This stakeholder-facing operationalization is essential in CBD hospitals where disruption-sensitive retrofits elevate the value of auditable, whole-facility claims.
Across progressive deployment maturity (S0→S3), the semantic digital-twin intervention produced a step increase in critical-room pressure-relationship compliance with tighter, less-dispersed room-to-corridor ΔP control and improved operational state discrimination (higher AUC) alongside faster issue-resolution (left-shifted time-to-resolve distribution). Whole-facility IPMVP Option-C analyses showed reporting-period residuals shifting negative relative to the S0-calibrated baseline, consistent with verified energy savings and lower facility-normalized carbon intensity, while service burden declined through reduced fault events and downtime and an avoided-cost signal. Scenario aggregation further indicated monotonic improvements in time-to-value and burden fractions, with an increasing composite performance index. In parallel, IAQ burden proxies improved (lower diurnal CO2 and reduced PM2.5 distributions), expected adverse-case burden decreased, and forecasting accuracy improved (lower RMSE), while compliance constructs remained broadly stable—suggesting that gains were not achieved by relaxing operational criteria. Causal analyses (interrupted time series and DiD) supported attribution of improvements to deployment, and solver benchmarking indicated that MILP and QA achieved better solution quality than heuristic baselines with distinct scalability envelopes, enabling energy–risk co-optimization frontiers for CBD retrofit planning.
Under typical variable air volume (VAV) operation, the method can be interpreted as a supervisory layer that preserves infection-control pressure relationships while letting the air-handling unit (AHU) and terminal units modulate with changing loads (weather, occupancy, procedures, door cycling, and filter loading). At the zone level, each critical room maintains minimum ventilation and directionality by enforcing a continuous differential-pressure requirement (e.g., AII rooms at ~2.5 Pa, 0.01 in. w.g. negative to corridor, with continuous monitoring), while the local VAV box modulates airflow to satisfy temperature and minimum-flow constraints and the exhaust and supply balance is adjusted to hold ΔP under disturbances such as door openings. Centers for Disease Control and Prevention guidance explicitly recommends continuous negative pressure and monitoring for AII rooms, which maps naturally into this paper’s pressure-compliance objective and constraint [39]. At the system level, the same supervisory logic can reduce energy by applying standard VAV efficiency sequences—most notably, duct static-pressure reset (trim-and-respond) so the supply fan pressure setpoint is lowered when most VAV dampers are not demanding pressure, with increases only when requests accumulate—while still respecting the critical-space minima and ΔP constraints; this aligns with modern control sequences captured in ASHRAE Guideline 36 addenda and healthcare ventilation requirements that emphasize maintaining required pressure relationships and minimum air-change and ventilation rates, even when VAV strategies are used for energy conservation. Concretely, under high load and in high-occupancy periods, the digital-twin layer would expect higher VAV demands and fan static pressure (and tighter ΔP excursions), whereas under low-load and setback periods it would allow for static-pressure reset and reduced airflow where permitted—yet keep airborne infection isolation (AII) rooms and operating rooms (ORs) strata pinned to their minimum ventilation and pressurization envelope—so the optimization improves whole-facility kWh and carbon without violating local pressure-safety requirements.
The results are consistent with a closed-loop evidence chain in which ontology-backed point, equipment, and space normalization reduce data ambiguity, enabling reliable intent enforcement (ΔP targets, door-status interlocks, and alarm logic) and earlier anomaly detection. Better observability and governance (auditable alarms and work-order coupling) plausibly shortened detection-to-correction cycles, reducing excursion minutes and compressing long-tail durations of degraded operation. Optimization (classical, quantum, and hybrid) likely reduced simultaneous over-ventilation and under-performance by reallocating ventilation and setpoints toward minimum-intent targets, decreasing excess air-change outliers and associated fan and conditioning loads, thereby driving whole-facility energy and carbon reductions without sacrificing compliance. Improved forecasting fidelity (lower RMSE) plausibly reduced unnecessary interventions and false alarms, while fault analytics prioritized high-leverage maintenance actions (e.g., belts, filters, valves, dampers, and VFD hunting), lowering downtime and service burden and stabilizing control dynamics (reduced overshoot, settling time, and integral error), which supports sustained pressure reliability.
Studies consistently show that digital twins enhance building performance through real-time monitoring, predictive maintenance, and energy management [31,32]. The integration of carbon-focused analytics, as in urban-scale digital-twin dashboards, enables spatially targeted interventions for emission reductions [33]. Quantum optimization, though nascent in the built environment, shows promise in solving complex multi-objective spatial and energy trade-offs. These findings are consistent with the existing literature on sustainable hospital design. The research by Zhang and Dang (2011) supports the observation that compact hospital layouts can reduce land usage significantly—up to 30%—which aligns with the land efficiency of the MCBD layout [40]. The energy savings observed in this study, particularly related to HVAC systems, are echoed by findings from Bulakh et al. (2020) and Ahmad et al. (2022), who reported that energy-efficient ventilation and lighting can reduce hospital energy consumption by 25–40% [41,42]. The integration of CE principles—such as the use of recyclable materials and staff optimization—has been promoted by the WHO’s zero-waste hospital initiative and is exemplified in the cost-saving strategies of the ring–medical-CBD model [22,23]. Additionally, centralized designs like that of Singapore’s Tan Tock Seng Hospital have shown operational cost reductions of 15–20%, corroborating the efficiency gains observed in the ring–Medical-CBD layout [24]. However, this study advances previous work by offering a holistic framework that integrates land, construction, and operational savings, supported by statistical validation and scalability across hospital sizes, filling a gap left by many prior qualitative studies [25].
These outcomes also strengthen the CE interpretation of the engineering work: the observed tightening of ΔP control and intent-aligned ventilation delivery implies less wasteful over-ventilation and fewer corrective interventions, while the left-shift in issue-resolution times indicates reduced rework and service burden. Together, these effects reflect resource efficiency and life-extension of existing HVAC assets—core CE mechanisms emphasized in built-environment circularity frameworks, where operational optimization, maintenance, and retrofit are preferred pathways to preserve value in existing systems and reduce material demand and embedded emissions.
Healthcare buildings contribute approximately 4.6% of global CO2 emissions [43]. Our integrated CBD approach can reduce embodied emissions by up to 20%, aligning with Philips’ reported 47% carbon reduction in eco-designed hospital equipment [44]. Prior circularity studies, such as the Joseph Bracops Hospital case, demonstrated material reuse rates of approximately 60% driven by design adaptability [45]. In comparison, our campus achieved 80–90% closed-loop yields and demonstrated significantly higher recycling rates than previously documented facility-level pilots. Additionally, clinical waste reuse programs in Australian hospitals have achieved annual savings of $2–3 million with recovery rates of 40–60% [46]. Our model projects savings of ¥1.2–19.7 million in operational costs (about 15% saved when compared with the control group without MCBD), indicating the scalability and financial viability of circular strategies in healthcare settings.
The sustainability benefits of the ring–medical-CBD layout are derived from its compact and centralized configuration. In line with the principles of green medical architecture, this layout minimizes land usage, thereby reducing acquisition and preparation costs and preserving natural habitats, key goals of ecological efficiency [40]. Efficient zoning and the use of modular construction techniques contribute to reduced material waste and carbon emissions during the building phase, consistent with sustainable architecture practices [47]. For green medical care, the layout enables rapid patient transfer and streamlined workflows, improving service efficiency and reducing labor demands. Green operations and maintenance further benefit from reduced internal travel distances for staff and materials, lowering utility and labor costs [24]. Integrated high-performance HVAC and lighting systems—critical in hospital operations—contribute to substantial reductions in energy use, particularly for temperature control, which dominates the energy profile of healthcare facilities [37]. Finally, the scalable nature of these design principles allows for proportional sustainability gains in larger facilities, where the efficiencies of compact design are magnified by higher patient volumes and energy demands.
This study’s primary strength is the decision-grade verification and triangulation: whole-facility IPMVP Option-C baseline modeling with residual screening links operational changes to measured energy outcomes; reliability and IAQ proxies are tracked concurrently to prevent energy-only optimization from degrading clinical-space performance; and causal inference (ITS and DiD with a control) strengthens attribution beyond simple before–after comparisons. This work also demonstrates deployability: progressive maturity stages (S0–S3) and explicit gating provide an audit trail from installation through advanced optimization and post-implementation M&V, aligning engineering action with verifiable outcomes. Finally, the integration of multi-objective optimization and solver benchmarking offers an operationalizable pathway for repeatable retrofit planning, clarifying quality–runtime–feasibility tradeoffs, rather than reporting a single algorithmic result.
Digital twins provide a dynamic digital mirror of physical assets, enabling real-time diagnostics and scenario simulation. IoT integration ensures continuous data flow from diverse building systems (HVAC, lighting, occupancy, etc.), enhancing responsiveness. Carbon adaptive control uses emission data as a feedback variable to modulate system performance toward decarbonization targets. Quantum optimization allows for rapid reconfiguration of space and resources under high-dimensional constraints, ideal for complex MCBDs. Beyond MCBDs, the IoT framework is applicable to other high-density, multi-building infrastructures, such as university campuses, smart industrial parks, and government complexes. Its modularity allows for adaptation to varying carbon policies, energy tariffs, or urban planning schemes.
The architecture is intended to deliver stakeholder-actionable outputs, rather than retrospective analytics only: (i) engineering-facing control evidence (ΔP compliance distributions, transient performance metrics, and diagnosable excursions), (ii) clinical governance summaries for critical rooms (compliance fraction, excursion minutes per day, and alarm performance), and (iii) management-facing whole-facility M&V and carbon reporting (Option-C residual shifts with uncertainty). By linking detection to response (BAS actions and CMMS and work orders) and then to verification (post-action recovery and reporting diagnostics), the semantic digital twin functions as an operational aftercare mechanism that supports handover, accountability, and sustained in-use performance governance.
Despite the strong identification evidence (flat pre-leads in the event study, placebo-in-time separation, improved balance after weighting, and synthetic-control concordance), several residual confounder classes can still bias DiD and ITS estimates if they (i) are time-varying, (ii) differentially affect treated vs. control, and (iii) coincide with the intervention window. The highest-risk confounders are operational intensity shocks (ICU and OR caseload changes, outbreak waves, and admission policy shifts) that simultaneously alter ventilation rates, door-opening frequency, staff movement, and plug-loads, affecting pressure compliance, IAQ exceedances, and energy in the same direction as the intervention. Building-plant and control shocks are also material: unlogged commissioning, chiller and boiler maintenance, sensor recalibration, BAS sequence edits unrelated to the intervention, or metering topology changes can create step changes or ramps that mimic treatment effects, particularly for whole-facility energy. Weather and seasonal anomalies beyond what is captured by standard degree-day terms (heat waves, humidity extremes, and regional haze events affecting PM2.5) can differentially move IAQ and HVAC energy if microclimate differs across sites or if filtration and ventilation policies diverge. Additional threats include tariff and dispatch changes that influence operational decisions, space-use reconfiguration (ward repurposing and renovation closures) that changes pressure zoning and occupancy patterns, and measurement artifacts (missingness, sensor drift, and altered sampling cadence) that can spuriously improve compliance or reduce exceedance fractions. In this context, Tables S5–S8 (especially the non-routine event and confounder log with artifact IDs) are crucial because they operationalize how these confounders were detected and handled (exclusion windows, indicator controls, or documented NRAs), while any borderline outcomes in the parallel-trends summary should be interpreted with bounded-sensitivity or alternative-control robustness to ensure that the reported effects remain stable under plausible unobserved shocks.
Several constraints remain. First, IAQ and airborne-risk metrics are proxies and may not directly translate to infection outcomes; similarly, complaint indices and some scenario-aggregated time and burden metrics are study-defined and may require external validation. Second, Option-C results depend on baseline model specification and covariate adequacy; although residual diagnostics are presented, unmeasured confounding drivers (e.g., occupancy shifts, clinical program changes, weather, and operational anomalies) could partially influence savings estimates. Third, generalizability may be limited because CBD hospitals vary widely in plant architecture, control sequences, staffing and work-order practices, and retrofit disruption constraints; the transferability of achieved deltas may therefore be site- and readiness-dependent. Fourth, some endpoints show limited between-strategy separability (e.g., similar pressure-compliance distributions across deployment strategies), and solver performance may vary with problem formulation, constraints, and tuning (e.g., QA chain strength and reads), complicating prescriptive best-method claims. Fifth, the central contribution is decision-grade verification and governance: Option-C whole-facility baseline modeling with diagnostics and a locked baseline, integrated with a semantic evidence chain that makes operational actions auditable. Optimization is treated as decision support; quantum annealing is included only as an exploratory benchmark alongside classical solvers, and we do not make prescriptive claims about solver superiority beyond the studied formulation.
6. Conclusions
Overall, the findings support that ontology-grounded semantic digital twins can convert heterogeneous BAS and IoT telemetry into an auditable control-and-verification pipeline that simultaneously improves critical-room pressure-relationship reliability and delivers whole-facility, Option-C-verified energy and carbon-intensity reductions in CBD hospitals, while lowering IAQ burden proxies and service burden, rather than trading them off. By combining progressive deployment, validated M&V, causal inference, fault economics, and multi-objective optimization with solver benchmarking, this study advances from descriptive smart hospital analytics to decision-grade retrofit guidance. The approach positions semantic digital twins as a scalable mechanism for decarbonization that maintains clinical ventilation intent, with future work best directed toward broader multi-site validation, stronger linkage to clinical outcomes, and standardized proxy-to-risk translation.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/buildings16061096/s1, Figures S1–S8; Tables S1–S8.
Funding
This research received no external funding.
Data Availability Statement
The original contributions presented in this study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The author declares no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Mansour, N.K.; Callera, A.; Potere, F.; Micalizzi, S.; Costantino, M.L.; De Gaetano, F.; Oliva, P. Circular economy and 3D printing in the healthcare sector. Front. Bioeng. Biotechnol. 2025, 13, 1548550. [Google Scholar] [CrossRef] [PubMed]
- Aquino, A.C.T.; Goncalves, M.F.S.; Mol, M.P.G. Healthcare waste and circular economy principles: It is time to improve! Waste Manag. Res. 2024, 42, 857–859. [Google Scholar] [CrossRef]
- Voudrias, E.A. Management of COVID-19 healthcare waste based on the circular economy hierarchy: A critical review. Waste Manag. Res. 2024, 42, 977–996. [Google Scholar] [CrossRef]
- Conte, S.; Le, M.; Moustaqim-Barrette, A.; Ghazawi, F.M.; Muntyanu, A.; Lagace, F.; Alakel, A.; Rahme, E.; Glassman, S.J.; Litvinov, I.V. Cutaneous Melanoma Mortality-to-Incidence Ratio and Its Association With Socioeconomic and Healthcare Factors in Canada: A National Ecological Study. J. Cutan. Med. Surg. 2024, 28, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Shen, L.; Tan, H.; Zhou, J.; Zheng, Q.; Jiang, D. Sleep quality and related factors among healthcare workers in designated quarantine hospital site in post-pandemic based on the health ecological model: A cross-sectional study in Nanjing, China. Front. Public Health 2024, 12, 1419665. [Google Scholar] [CrossRef]
- Konstantinou, P.; Theofanous, V.; Karekla, M.; Kassianos, A.P. Mapping the needs of healthcare workers caring for COVID-19 patients using the socio-ecological framework: A rapid scoping review. Hum. Resour. Health 2024, 22, 29. [Google Scholar] [CrossRef]
- Shah, H.H.; Amin, M.; Pepe, F.; Tregambi, C. Sustainable waste management and waste-to-energy in the context of a circular economy through various waste management technologies. Environ. Sci. Pollut. Res. Int. 2024, 32, 27503–27522. [Google Scholar] [CrossRef]
- Cai, Z.; Tang, Y.; Lin, J. Exploring the impact of circular economy practices on ecological footprint, inflation rate, and renewable energy consumption: Evidence from G20 economies. Environ. Sci. Pollut. Res. Int. 2024, 31, 26536–26554. [Google Scholar] [CrossRef]
- Brunner, P.H.; Morf, L.S. Waste to energy, indispensable cornerstone for circular economy: A mini-review. Waste Manag. Res. 2025, 43, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.Y.; Li, J.Y.; Chen, C.J.; Zhang, J.; Wu, Y.; Cheng, H.; Shen, C.C.; Li, T.Y. Evolution of the Asian summer monsoon and regional karst ecological environment since the middle ages in Southwest China. Sci. Rep. 2025, 15, 8091. [Google Scholar] [CrossRef]
- Ren, S.; Wang, F.; Liu, P.; Zhao, H.; Zhang, H.; Cui, L. Analysis of influencing factors and paths of synergistic development of water resources-economic society-ecological environment based on DIM modeling. Sci. Rep. 2025, 15, 5925. [Google Scholar] [CrossRef]
- Zhang, Z.; Qi, J.; Wang, Q.; Wang, S.; Hu, F. Analysis and forecast of the coupled development level of socioeconomy ecological environment and tourism in China’s Yellow River Basin. Sci. Rep. 2025, 15, 5446. [Google Scholar] [CrossRef]
- Wan, S.; Chen, Y.; Xiao, Y.; Zhao, Q.; Li, M.; Wu, S. Spatial analysis and evaluation of medical resource allocation in China based on geographic big data. BMC Health Serv. Res. 2021, 21, 1084. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P. Study on Internal Traffic Organization Modes for Underground Parking Systems in the Urban Central Business District. J. Phys. Conf. Ser. 2022, 2202, 012041. [Google Scholar] [CrossRef]
- Wen, J.; Fan, Z.; Liu, J. Effects of complex skyscraper geometries on wind energy potentials of high-density urban central business district: A case study of the Lujiazui blocks. Sustain. Cities Soc. 2025, 124, 106287. [Google Scholar] [CrossRef]
- Rodríguez, R.; Svensson, G.; Ferro, C. Assessing the future direction of sustainable development in public hospitals: Time-horizon, path and action. Health Policy 2021, 125, 526–534. [Google Scholar] [CrossRef]
- Lomas, K.J.; Giridharan, R.; Short, C.A.; Fair, A. Resilience of ‘Nightingale’ hospital wards in a changing climate. Build. Serv. Eng. Res. Technol. 2012, 33, 81–103. [Google Scholar] [CrossRef]
- Shahsavar, F. Integrating Sustainable Design, Smart Technologies, Certification in Green Hospital Architecture. J. Des. Studio 2025, 7, 213–222. [Google Scholar] [CrossRef]
- Raimundo, A.M.; Oliveira, A.V.M. Assessing the impact of climate changes, building characteristics, and HVAC control on energy requirements under a Mediterranean climate. Energies 2024, 17, 2362. [Google Scholar] [CrossRef]
- Jaušovec, M.; Gabrovec, B. Architectural evaluation of healthcare facilities: A comprehensive review and implications for building design. Buildings 2023, 13, 2926. [Google Scholar] [CrossRef]
- Alsawaf, E.S.; Albadry, A.M. Principles for the sustainable design of hospital buildings. Int. J. Sustain. Dev. Plan. 2022, 17, 1797–1808. [Google Scholar] [CrossRef]
- Vavili, F.; Kyrkou, A. Sustainability and energy efficiency design in hospital buildings. In Energy Efficient Building Design; Springer: Berlin/Heidelberg, Germany, 2020; pp. 157–169. [Google Scholar]
- Hendriks, E.; de Zwart, J.; Compeer, A.; Gospodinova, J. Assessing and enhancing the circularity and sustainability of emergency hospital shelters. Disasters 2025, 49, e12670. [Google Scholar] [CrossRef]
- Castro, M.d.F.M.d.; Mateus, R.; Bragança, L. Space design quality and its importance to sustainable construction: The case of hospital buildings. In Proceedings of the SB13 Portugal—Sustainable Building Contribution to Achieve the EU 20-20-20 Targets, Guimarães, Portugal, 30 October–1 November 2013. [Google Scholar]
- Capolongo, S.; Bottero, M.; Buffoli, M.; Lettieri, E. Improving sustainability during hospital design and operation. In A Multidisciplinary Evaluation Tool; Springer International Publishing: Cham, Switzerland, 2015; Volume 10, pp. 973–978. [Google Scholar]
- Arsecularatne, B.; Rodrigo, N.; Chang, R. Digital Twins for Reducing Energy Consumption in Buildings: A Review. Sustainability 2024, 16, 9275. [Google Scholar] [CrossRef]
- Cespedes-Cubides, A.S.; Jradi, M. A review of building digital twins to improve energy efficiency in the building operational stage. Energy Inform. 2024, 7, 11. [Google Scholar] [CrossRef]
- Cheng, W.; Lian, W.; Tian, J. Building the hospital intelligent twins for all-scenario intelligence health care. Digit. Health 2022, 8, 20552076221107894. [Google Scholar] [CrossRef]
- Piras, G.; Agostinelli, S.; Muzi, F. Smart Buildings and Digital Twin to Monitoring the Efficiency and Wellness of Working Environments: A Case Study on IoT Integration and Data-Driven Management. Appl. Sci. 2025, 15, 4939. [Google Scholar] [CrossRef]
- Sghiri, A.; Gallab, M.; Merzouk, S.; Assoul, S. Leveraging digital twins for enhancing Building energy efficiency: A literature review of applications, technologies, and challenges. Buildings 2025, 15, 498. [Google Scholar] [CrossRef]
- Yang, W.; Bao, X.; Zheng, Y. Digital twin approach to build predictive maintenance model and its case study. In Proceedings of the International Design Engineering Technical Conferences and Computers and Information in Engineering Conference, St. Louis, MO, USA, 14–17 August 2022; p. V002T002A039. [Google Scholar]
- Peng, Y.; Zhang, M.; Yu, F.; Xu, J.; Gao, S. Digital twin hospital buildings: An exemplary case study through continuous lifecycle integration. Adv. Civ. Eng. 2020, 2020, 8846667. [Google Scholar] [CrossRef]
- Alva, P.; Mosteiro-Romero, M.; Miller, C.; Stouffs, R. Mitigating operational greenhouse gas emissions in ageing residential buildings using an Urban Digital Twin dashboard. Energy Build. 2024, 322, 114681. [Google Scholar] [CrossRef]
- EVO 10000-1:2022; International Performance Measurement and Verification Protocol (IPMVP): Core Concepts, March 2022. EVO: Washington, DC, USA, 2022.
- ANSI/ASHRAE/ASHE Standard 170-2021; Ventilation of Health Care Facilities. ASHRAE: Atlanta, GA, USA, 2021.
- DOE/FEMP. M&V Guidelines: Measurement and Verification for Performance-Based Contracts, Version 4.0; DOE/FEMP: Washington, DC, USA, 2015. [Google Scholar]
- Thumann, A.; Woodroof, E. International performance measurement & verification protocol. In Handbook of Financing Energy Projects; CRC Press: Boca Raton, FL, USA, 2001; p. 249. [Google Scholar]
- GHG Protocol Scope 2 Guidance: An Amendment to the GHG Protocol Corporate Standard; WRI/WBCSD: Washington, DC, USA; Geneva, Switzerland, 2015; ISBN 978-1-56973-850-4.
- Roth, B.S.; Moschella, P.; Mousavi, E.S.; LeMatty, A.S.; Falconer, R.J.; Ashley, N.D.; Mohammadi Nafchi, A.; Gaafary, C.; DesJardins, J.D. Development and efficacy testing of a portable negative pressure enclosure for airborne infection containment. J. Am. Coll. Emerg. Physicians Open 2022, 3, e12656. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Dang, R. The general planning of hospital under the concept of sustainable development. In Proceedings of the 2011 International Conference on Electric Technology and Civil Engineering (ICETCE), Lushan, China, 22–24 April 2011; pp. 5606–5608. [Google Scholar]
- Bulakh, I.; Didichenko, M.; Kozakova, O.; Chala, O. Sustainable futures in the context of architectural design of hospitals. In Proceedings of the E3S Web of Conferences, Online, 21–22 May 2020; p. 08001. [Google Scholar]
- Ahmad, J.; Boity, A.K.; Chauhan, H.K.; Arora, K. Evaluation of Architectural Design Features in Achieving Sustainability in Hospital Projects. ECS Trans. 2022, 107, 9453. [Google Scholar] [CrossRef]
- Chen-Xu, J.; Corda, M.O.; Varga, O.; Viegas, S. Health burden and costs attributable to the carbon footprint of the health sector in the European Union. Environ. Int. 2024, 190, 108828. [Google Scholar] [CrossRef]
- Mominkhan, D.; Alamri, F.A.; Balharith, M.; Alharbi, M.; Alshebli, A.; Alshareef, S.Y.; Khairaldain, A.; Almutairi, N.; Abusit, A.; Almuzaini, Y. The current state and potential evolution of carbon emissions in the healthcare sector: A narrative review article. Front. Sustain. Energy Policy 2023, 2, 1230253. [Google Scholar] [CrossRef]
- Scialpi, G.; Declercq, J.; Grisay, L.; Perrotti, D. An urban hospital base79, 2d on the principles of circular economy: The case of Joseph Bracops hospital. IOP Conf. Ser. Earth Environ. Sci. 2022, 1078, 012011. [Google Scholar] [CrossRef]
- Jerin, A.; Mahmud, M.P.; Ackland, L.; Kouzani, A.Z. Recent progress on carbon footprint assessment of healthcare services. Environ. Res. Commun. 2024, 6, 102001. [Google Scholar] [CrossRef]
- Aydın, D.; Yaldız, E.; Buyuksahin, S. Sustainable hospital design for sustainable development. In Proceedings of the 8th International Conference on Urban Planning, Architecture, Civil and Environment Engineering (UPACEE-17), Dubai, United Arab Emirates, 21–22 December 2017; pp. 21–22. [Google Scholar]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.