Abstract
In recent years, with the deepening research on exoskeletons for children with cerebral palsy, increasing evidence has highlighted their unique characteristics. Unlike adult exoskeletons, pediatric exoskeletons cannot be simply realized by scaling down adult designs; instead, special attention must be given to their unique training requirements. Although current studies have incorporated specific design adaptations and summarized the distinct features of these devices, a comprehensive review of control strategies remains lacking. This study adopts a structured narrative review approach, referencing the PRISMA framework to enhance transparency in the literature selection. Relevant publications were identified based on clearly defined inclusion and exclusion criteria, but no formal systematic review or meta-analysis was conducted. The exoskeleton control strategies from the 106 selected articles are classified using a hierarchical framework, dividing them into the supervision layer, action layer, and execution layer, with a further categorization into 12 specific control methods. Findings indicate that the supervision level primarily employs finite state machines and linear phase estimation, while the action level predominantly utilizes position trajectory control, torque trajectory control, and impedance control. At the execution level, closed-loop torque control and position control are commonly adopted. Overall, existing studies still face challenges in personalized adaptation, real-time control, and application scenarios. With advancements in controller hardware and the introduction of novel actuators, emerging technologies such as machine learning, virtual constraints, and sliding mode control may offer promising directions for future pediatric exoskeleton control design.
1. Introduction
Children with cerebral palsy (CP) experience motor impairments due to neurological damage. Improving their walking ability requires effective support from assistive devices, among which the cerebral palsy lower-limb exoskeleton (CPLLE) is a critical tool. Unlike adult exoskeleton systems, CPLLE—similar to other pediatric rehabilitation robots—remains at an early stage of clinical application, and there is still no consensus on the optimal characteristics such devices should possess for children. Early CPLLE designs were adapted from adult exoskeletons by simply scaling down their size; however, this approach was later dismissed due to the failure to account for critical pediatric-specific factors such as lower joint torque and limited cognitive abilities [1].
With deeper research, the target population for CPLLE has been more clearly identified, highlighting features such as a wide developmental span, low load-bearing capacity, limited cognitive understanding, significant individual variability, and complex gait patterns. As a result, design considerations have expanded beyond their basic function to emphasize usability, adjustability, and customization to meet the specific needs of children with CP [2]. While it is now widely accepted that “CPLLE is not a scaled-down version of adult exoskeletons”, existing studies still lack a structured examination and in-depth analyzes on how control strategies should be adapted to the unique characteristics of children.
As a core component of CPLLE systems, control strategies facilitate efficient human–machine interaction, provide dynamic motion assistance, and support the modulation of rehabilitation goals. They also help compensate for actuator rigidity, improve compliance, and enhance adaptability. Although existing reviews on CPLLE control strategies [3,4] have proposed hierarchical classifications, their limited scope has led to coarse categories that offer insufficient guidance for practical system development. In the development of CPLLE control strategies, researchers often still rely on well-established reviews in the field of adult lower-limb rehabilitation exoskeletons [5,6] as a foundational reference. However, due to the lack of systematic summaries specific to CPLLE as a distinct subcategory, directly applying control logic from adult exoskeletons may lead to strategies that fail to adequately accommodate the physiological and cognitive characteristics of children with CP, thereby hindering clinical adoption and commercial translation.
To further advance the clinical application and engineering optimization of CPLLEs, there is an urgent need to develop a targeted and structured classification framework for control strategies, clarify the specific needs of children with CP, and define a functional architecture that ensures comparability and reusability. Therefore, this study aims to bridge the current gap in the literature by reviewing nearly two decades of CPLLE research, with a particular focus on control strategy developments from the past five years.
Specifically, Section 2 introduces the objectives of control strategies, Section 3 outlines the classification methodology and literature search, Section 4 summarizes existing methods in a structured manner according to control hierarchy, and Section 5 presents control strategies that have been proven clinically effective. Finally, Section 6 draws key conclusions and highlights implications. By adopting a functional decomposition approach and employing a three-layer control theory classification, this study aims to help readers understand the implementation details of existing controllers, identify their distinguishing patterns, and provide theoretical support for future device design and clinical translation.
2. Control Strategy Design Objectives
2.1. Overall Design Objectives
From a system-level perspective, CPLLE control strategies must resolve two core challenges: firstly, aligning with the changing physiological and cognitive development of children with CP rather than relying on traditional static training methods; secondly, overcoming hardware constraints to enable personalized and compliant control.
2.1.1. Adapting to Pediatric CP Population Characteristics
Children with CP exhibit unique requirements in control strategy design that differ substantially from those of adults. While adult exoskeletons often target compensation and daily assistance, pediatric systems aim to promote neuroplasticity and motor recovery. Long-term and adaptive rehabilitation is essential to accommodate the evolving patient profile.
Unlike adults, children undergo continuous physiological and cognitive development, which is especially complex and variable in those with CP. As they grow, their height, weight, joint flexibility, muscle strength, and neuromotor control change significantly [7,8]. In addition to adjustable mechanical dimensions, control strategies must also adapt accordingly. Given the limited attention and cognitive maturity of pediatric users, the system should minimize reliance on active input and emphasize automation and user-friendly interaction.
In contrast to adult exoskeletons, which are often categorized into fully or partially assistive modes [5], rehabilitation in children with CP is a dynamic process. As recovery progresses, the level of active participation gradually increases. A binary classification of “active” versus “passive” control is insufficient to describe this gradual transition [4]. As illustrated in Figure 1, the level of machine assistance should adjust in response to the patient’s active participation , ranging from 0% to 100%. In early stages, children may rely entirely on passive support; as function improves, partial voluntary control should be encouraged, eventually progressing to active training or even resistance training. Therefore, CPLLE control strategies should dynamically adjust assistance intensity to cover a continuous segment of the rehabilitation spectrum, aiming to maximize voluntary motor engagement and promote gradual neuromotor recovery.
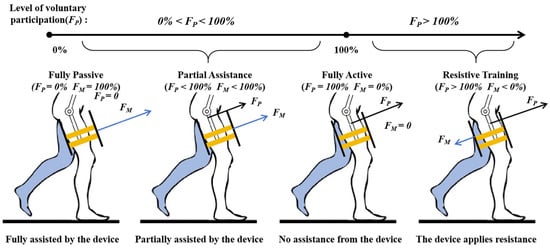
Figure 1.
Illustrations of the rehabilitation spectrum, depicting the progressive transition as a function of a patient’s active participation and machine assistance .
2.1.2. Compensation for Inherent Hardware Limitations
Despite differences in mechanical structures and actuation designs, all lower-limb exoskeletons exhibit inherent hardware limitations. For children with CP, these limitations are amplified due to their physiological fragility and cognitive immaturity [9], which may compromise both the safety and efficacy of rehabilitation. Therefore, control strategies must compensate for these hardware constraints.
Multi-joint exoskeletons often feature heavy rigid linkages and a large distal mass, leading to poor backdrivability and reduced transparency. In contrast, single-joint designs are lightweight and cost-effective but provide limited gait intervention and reduced kinematic feedback, constraining control performance and adaptability.
Although electric actuators are the mainstream choice for CPLLE due to their favorable torque-to-weight ratio and high control precision [2], they also introduce several challenges. These include a high structural rigidity, limited compliance, poor multi-dimensional interaction capability, high cost, and reduced adaptability [10].
In summary, every mechanical configuration entails trade-offs, and effective rehabilitation relies on adaptable control strategies to mitigate these limitations.
2.2. Specific Design Objectives
At the control level, the uniqueness of CPLLE lies in the need to establish specialized training objectives tailored to specific symptoms and target users, selecting appropriate control methods accordingly. The commonly identified training objectives can be categorized as follows:
2.2.1. Gait Improvement
Gait improvement is a fundamental objective in CPLLE design, encompassing both walking posture and walking energy consumption.
Posture improvement focuses on the geometric characteristics and motor control of gait, including postural stability, joint range of motion, gait symmetry, and rhythm. Among these, gait cycle symmetry and stability depend on joint coordination. This is typically achieved through time-linear gait phase (TLP) estimation, FSM-based phase recognition using sensor feedback, or model-predictive trajectory planning. Enhancing the joint range of motion relies on a precise control of the external torque applied by the exoskeleton through mechanical torque interventions. For instance, ankle exoskeletons may employ fixed assistive/resistive interventions [11], dynamically adjust torque according to joint angle variations [12], or utilize real-time knee joint prediction to provide adaptive assistance [13]. Energy efficiency aims to reduce the high metabolic cost associated with muscle weakness or spasticity by providing mechanical support and personalized assistance. This can involve minimizing muscle activation through targeted joint support [14], estimating real-time torque demands to optimize force delivery [15,16], or adjusting motion parameters to avoid over- or under-assistance [17,18].
2.2.2. Muscle Strength Training
CPLLE systems typically include muscle strength training functions, using motors or actuators to assist lower-limb movement, promote correct gait patterns, and enhance muscle activation. However, studies have shown [19] that muscle loading remains relatively low during gait training, with a limited engagement of the nervous system, thereby constraining training effectiveness. To further improve training outcomes, targeted muscle strength training strategies must be introduced.
Resistive training differs from traditional assistive training. It applies resistance during the gait cycle to encourage patients to exert a greater force actively, thereby enhancing neuromuscular engagement and improving lower-limb strength and motor control. In practical applications, this strategy is commonly used for knee extension [18,19] and ankle push-off [20], which are key gait actions. It relies on closed-loop control to dynamically adjust resistance in real time, ensuring adaptability to user needs and optimizing rehabilitation outcomes. The resistance is typically applied through magnetic braking mechanisms [21,22] or actively regulated via Bowden cable systems [20]. Notably, as resistive training requires a certain level of baseline muscle strength, and it is often combined with other training modalities to accommodate early-stage rehabilitation patients. For patients with insufficient muscle strength who cannot tolerate resistive training, functional electrical stimulation (FES)-assisted training offers an alternative. It is specifically designed for individuals with potential muscle responsiveness but inadequate strength [23,24]. This approach utilizes electrical stimulation as an external intervention, ensuring synchronization between electrical stimulation and CPLLE assistance at critical gait phases through FSM or similar control methods. By minimizing unintended stimulation that could disrupt natural motor patterns, this approach enhances the efficacy of neuromuscular training.
2.2.3. Abnormal Gait Correction
Another key design objective of CPLLE is the correction of abnormal gait patterns. Based on the anatomical regions affected and the kinematic characteristics of gait, abnormal gait in CP can be classified into spastic hemiplegia and spastic diplegia. Spastic hemiplegic gait includes drop foot and the unilateral equinus gait, while spastic diplegic gait encompasses crouch gait and jump gait [25]. Correspondingly, existing CPLLE correction strategies can be broadly categorized into hemiplegic exoskeletons, crouch gait exoskeletons, and equinus gait exoskeletons.
Hemiplegic exoskeletons primarily aim to correct gait asymmetry and improve patients’ weight-bearing capacity and abnormal movement trajectories. For example, HAL [26] employs a hybrid control strategy combining electromyography (EMG) and gait phase estimation to assist knee joint motion, while SLE [27] utilizes gravity compensation based on a dynamic model and impedance control (IC) to optimize gait adjustment and reduce the exoskeleton’s mechanical load. Additionally, a system described in [28] adapts real-time torque control to automatically adjust ankle assistance for different hemiplegic patients. Crouch gait exoskeletons focus on correcting excessive knee flexion during the gait cycle. These exoskeletons commonly adopt FSM-based gait phase recognition to provide adaptive assistance. For instance, P.REX [29] implements stepwise torque assistance for fine-tuned knee control, while the system in [30] employs an electromagnetic braking unit to actively prevent excessive knee flexion during the stance phase. Additionally, neuromuscular electrical stimulation (NMES) has been used in [24] to facilitate knee extension. Other approaches, such as the IC strategy in [12], dynamically adjust assistance between the stance and swing phases to enhance gait stability and adaptability. The correction of the tiptoe gait primarily targets plantar flexion abnormalities caused by neurological impairments, which result in the heel failing to contact the ground during walking. Exoskeletons designed for this abnormal gait aim to address ankle drop and heel strike difficulties in children with CP. These devices emphasize restoring proper foot placement, such as heel contact, and improving lower-limb motor coordination. For instance, the designs in [31,32] integrate position and torque control, utilizing the deformation of elastic elements to achieve torque regulation while assisting in the functional rehabilitation of the ankle and knee joints.
2.2.4. Specific Movements
Rehabilitation training for children with CP primarily focuses on gait training, while research on other daily movements remains relatively limited. However, rehabilitation should not be confined to the improvement of physiological functions alone. Assistive training tailored to specific movements can enhance psychological support and boost confidence. Moreover, it contributes to an improved social participation, establishing it as a critical design consideration in CPLLE development. Existing studies in this area primarily focus on sit-to-stand/squat-to-stand transitions and stair climbing/oblique walking training.
Sit-to-stand and squat-to-stand transitions are commonly implemented using position profile-based PID position control [33,34] or online torque profile-based closed-loop torque control [35,36]. These control strategies emphasize maintaining dynamic balance, often relying on zero moment point (ZMP) analysis or inertial measurement unit (IMU) feedback to evaluate stability. Stair climbing and oblique walking training predominantly utilize a FSM combined with torque estimation and PID closed-loop torque control [28,37,38,39,40]. FSMs are responsible for detecting key gait phases, while adaptive adjustments to gait parameters and assistive torques are achieved through biological torque estimation [37,39] or center-of-mass trajectory analysis [40]. These adaptive mechanisms enable CPLLE to accommodate diverse terrains, including flat surfaces, slopes, and staircases [34].
3. Search and Classification Methods
3.1. Scope and Methodological Steps
This study retrieved relevant publications from two databases: Web of Science and IEEE/IET Electronic Library (IEL). To ensure a comprehensive coverage while maintaining relevance, the search strategy was based on three thematic keyword groups combined using Boolean logic. The search keywords were structured as follows:
- Topic 1: (Foot OR Ankle OR Knee OR Hip OR Lower Limb OR Lower Body)
- Topic 2: (Exoskeleton) OR (Assistive Robot*) OR (Wearable Robot*) OR (Robot* Suit) OR (Portable Robot*) OR (Powered Orthotic System)
- Topic 3: (Children OR Pediatric OR Young Patient OR Cerebral Palsy)
It is important to note that the search was designed to maximize sensitivity; therefore, Topic 3 was not strictly required to contain both population and condition terms in a single entry. To avoid omissions, the above search terms did not explicitly constrain both the target population and medical condition simultaneously. As a result, additional manual screening was conducted in a subsequent step, ensuring that the final selected publications explicitly addressed both criteria: (1) the population involved children or pediatric patients, and (2) the condition involved CP-related gait disorders.
Using these search terms, a total of 696 relevant publications (up to January 2025) were retrieved as follows: 489 from Web of Science and 207 from IEL, with 126 duplicates between the two databases. After reviewing titles and abstracts, 304 publications unrelated to the review topic were excluded. A full-text examination of the remaining publications led to further exclusions: 98 studies did not target CP children, 37 did not mention control strategies in exoskeleton design, 31 focused on control strategies still in the simulation stage without physical prototypes, and 3 investigated passive exoskeletons that relied solely on mechanical mechanisms rather than active control, which were beyond the scope of this study. Ultimately, 97 publications met the inclusion criteria. During the subsequent review process, nine additional relevant studies were identified, bringing the total number of fully reviewed articles to 106. The literature selection process followed the PRISMA flowchart, as illustrated in Figure 2.
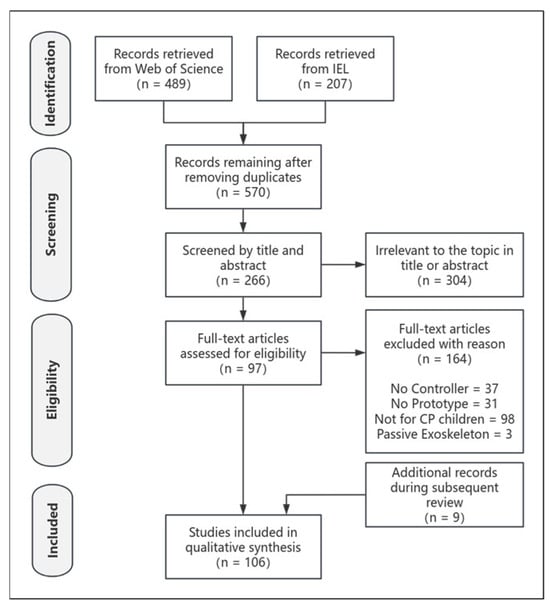
Figure 2.
The preferred reporting items for the systematic reviews and meta-analysis (PRISMA) flowchart.
3.2. Proposed Classification Method
CPLLEs vary substantially in hardware configurations, control approaches, target user groups, and usage scenarios. Treating all control strategies as a uniform whole in a generalized discussion not only hinders the extraction of representative common features across designs but also leads to redundant descriptions of functionally similar components. Therefore, the control strategy analysis should focus on the core objective of facilitating effective rehabilitation training. As shown in Figure 3, the core functional modules of CPLLEs related to lower-limb rehabilitation are typically organized into a three-layer structure: intent recognition, motion planning, and actuator execution. This structure provides a systematic foundation for analyzing control architectures.
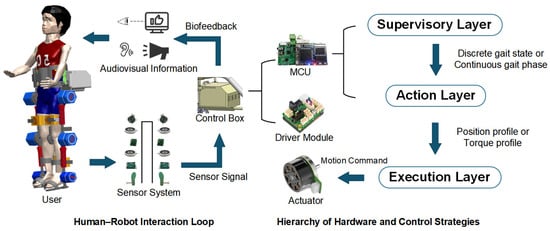
Figure 3.
The hierarchical control architecture and signal flow of the exoskeleton system.
As illustrated in Figure 4, this study focuses exclusively on the control processes directly related to rehabilitation training in different types of CPLLEs. To ensure terminological consistency, a complete CPLLE control system is uniformly referred to in this study as a “controller” or “control strategy”. It is further decomposed into multiple “functional units” based on their respective roles. Functional units identified in the reviewed literature are structurally analyzed and hierarchically organized into corresponding “control modules”. Ultimately, these control modules serve as the fundamental analytical units of this review, supporting a hierarchical examination of CPLLE control systems. This structured approach not only clarifies the commonalities and differences among diverse studies but also highlights the varying implementations of similar control strategies across different device types.
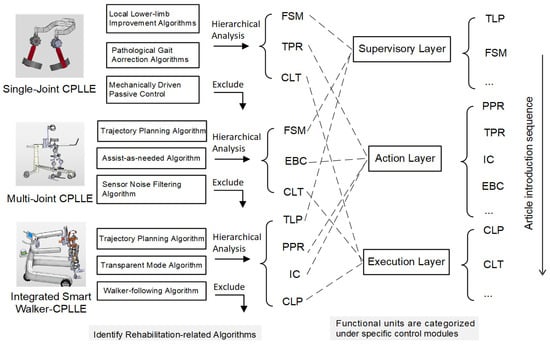
Figure 4.
A schematic diagram of exoskeleton control strategy functional unit decomposition and control module organization.
The primary advantage of this classification method is its ability to structurally group functional units of different CPLLE controllers into control modules. This allows for a direct comparison of implementation details within the same module, while also avoiding redundant descriptions of identical functions. Additionally, the hierarchical nature of control modules enables flexible combinations to describe the CPLLE controller designs found in all of the reviewed studies, thereby providing a clearer understanding of the overall design rationale of a given controller. It is important to note that while this three-layer classification applies to most CPLLEs, some control strategies may not fully encompass all hierarchical levels, particularly in early-stage development.
The studies included in the scope of this review, based on the literature screening strategy proposed in this paper, were categorized using the previously described classification method, resulting in the following 46 CPLLE controller studies summarized in Table 1.

Table 1.
The structured classification of control strategies for pediatric lower-limb exoskeletons.
4. A Hierarchical Review of the Control Strategies
4.1. Supervisory-Layer Control: Gait Phase Recognition
The supervisory layer is typically responsible for identifying gait phases and providing continuous or discrete gait state inputs to lower-level control strategies. In CPLLE systems, compared to adult rehabilitation devices, challenges such as unstable gait rhythm, poor inter-joint coordination, and significant variation in volitional participation across training stages require phase detection strategies with a higher robustness and adaptive capability. The supervisory-layer controller is often integrated with the action-layer controller into a high-level exoskeleton controller, which is deployed within the CPLLE microcontroller unit (MCU).
4.1.1. Time-Linear Gait Phase (TLP)
The TLP is a simple and effective phase recognition method that correlates the CPLLE gait phase with time, allowing it to increase linearly over a known gait duration during training.
In passive training, TLP synchronizes joint actuator positions and velocities under a unified phase reference, thereby stabilizing gait rhythm and enhancing motion coordination. Additionally, during early-stage exoskeleton development or low-level control validation, TLP facilitates phase progression using a linear time-based approach, reducing the computational burden of nonlinear control and simplifying debugging. For instance, in Laubscher’s early studies on a hip–knee exoskeleton [7], where higher-level control strategies were not yet developed, TLP was combined with PID closed-loop control for gait tracking validation. In hip–knee–ankle exoskeleton research [68,69,70,71,72,73], TLP was used to execute position profiles, allowing for the evaluation of low-level algorithm improvements.
In soft CPLLEs, as precise gait correction and walking efficiency enhancement remain exploratory, achieving high-precision force control remains challenging. As a result, TLP is frequently utilized for exoskeleton performance validation. For example, in a hip–knee exoskeleton [61] driven by shape memory alloy (SMA), contraction and extension are controlled via temperature regulation to provide gait assistance. The system allows users to set a reference gait cycle, and with TLP-based phase progression, SMA actuators modulate current to precisely track the gait phase. Similarly, another exoskeleton driven by twisted coiled polymer (TCP) actuators [83] employs nickel–chromium wires embedded in polymer fibers (e.g., nylon) and also utilizes TLP-based training.
However, due to its limited adaptability to non-periodic gait patterns and individual variability, the TLP approach is constrained in handling the progressively increasing volitional participation and gait variability in children with CP. It is therefore more suitable for passive training in the early rehabilitation stage or for system performance validation.
4.1.2. Finite State Machine (FSM)
In CPLLE rehabilitation training, different gait phases present distinct control objectives—for example, support during stance and assistance during swing. The FSM enables real-time gait perception and automatic phase transitions by defining gait states (such as stance and swing) and corresponding transition conditions, thereby facilitating precise control. Due to its simple logic and clear response characteristics, the FSM approach is well suited for the early to mid-stages of rehabilitation in children with CP, where cognitive capacity is limited and a stable gait rhythm needs to be established.
The most common FSM-based strategy divides the gait cycle into stance and swing phases, using force-sensitive resistors (FSRs) embedded in footbeds for state transitions. Lerner’s team has applied FSR-based FSM across hip, knee, and ankle exoskeletons. For example, in an ankle exoskeleton [15,16,41,42,43,44,45,46,47,48,49], FSM determines the gait phase based on foot pressure, providing assistance during stance to compensate for plantarflexor weakness (triceps surae), while minimizing interference during swing. A hip exoskeleton developed by the same group [37] follows a similar approach, where FSM modulates flexion and extension assistance to adapt to pathological gait variations.
In multi-joint exoskeletons, FSM is often combined with IC to dynamically regulate joint stiffness. Studies such as [65,66,67] utilize FSM to increase impedance during the stance phase to enhance stability while reducing impedance during the swing phase to optimize gait flexibility. In another approach, Gait Guidance Control [35,77] applies damping forces only during the swing phase to correct abnormal gait deviations. Additionally, research combining FSM with NMES [19,23,24,29,53,54] applies electrical stimulation during the stance phase to enhance muscle strength, improve motor function, and reduce spasticity, thereby optimizing crouch gait correction.
FSM-based gait segmentation can also incorporate multi-sensor data such as knee joint angle and angular velocity. A study in [57] utilizes knee joint kinematics to refine swing phase segmentation, allowing for precise assistance timing. Further research [29,53,54] subdivides the gait cycle into 2–5 distinct states, enabling a more refined, personalized assistance. To address challenges in weight shifting among CP children, an FSM strategy with six states and eight transition conditions was developed in [33], integrating ground reaction force (GRF) sensing and joint angle data to ensure stable gait transitions.
FSM can also be deployed within distributed control architectures to improve system efficiency. Studies in [31,32] implement FSM on secondary (slave) nodes, allowing the master node to manage coordination while each slave node independently performs gait recognition, torque computation, and command execution. This approach reduces communication dependency and enhances system response speed.
For abnormal gait correction, several studies have improved traditional FSM gait detection methods. A study in [64] integrates real-time signal processing and sensor fusion techniques, developing a Gait Event Detection algorithm that uses IMU-derived shank rotation data and low-pass filtering to optimize gait phase segmentation, achieving a higher real-time adaptability and detection accuracy than conventional FSM. Addressing the high power consumption and excessive weight in existing CPLLE systems, research in [30] designs a lightweight electromagnetic braking unit, where FSM activates braking during stance and disengages it during swing, effectively controlling excessive knee flexion and providing a more user-friendly gait correction solution for children with muscle weakness.
Although FSMs are widely used in CPLLE systems, their discrete state transitions limit the ability to continuously regulate lower-level controllers. This constrains the dynamic adjustment of training intensity and assistive strategies, making it difficult to fully meet the compliant control requirements in the mid-to-late stages of rehabilitation.
4.1.3. Machine Learning (ML)
ML presents significant potential and challenges in CPLLE control, with applications in gait pattern recognition, motion intent prediction, real-time control optimization, and personalized rehabilitation strategies. Theoretically, an ideal ML model could achieve real-time, continuous, and highly accurate gait phase recognition, offering a greater adaptability to complex gait patterns and reducing the need for manual parameter tuning compared to FSM and TLP. Particularly in children with CP, where gait rhythm is unstable and volitional participation varies widely, traditional rule-based state segmentation methods often fail to accurately capture individualized gait patterns. In contrast, ML models offer the potential to develop adaptive recognition mechanisms.
One of the earliest applications of ML in pediatric exoskeletons was introduced in [112], where a single-layer perceptron neural network was used to adjust PWM signals, allowing motor angular velocity to better match the gait velocity profile of healthy children. However, the training data only included angular velocity from gait cycle curves and did not explicitly compute gait phase transitions.
Later studies have focused primarily on gait pattern recognition. For example, ref. [55] applied a long short-term memory (LSTM) network, training the model using IMU data to estimate the gait phase in real time and retrieve reference torque values from biological torque curves. Similarly, ref. [13] utilized a gated recurrent unit (GRU) network with an attention mechanism to estimate knee joint angles and predict gait phases based on surface EMG signals, guiding motion command generation. These studies have preliminarily demonstrated the capability of ML methods to perform dynamic prediction and coordinated command generation under complex signal conditions, showing a certain degree of generalization potential.
Despite recent progress, current ML-based approaches face several key limitations. Firstly, most of the existing models are trained and validated on extremely small datasets or limited to offline analysis and small-scale laboratory testing [13,55], making it difficult to generalize control strategies to broader populations and complex environments. Secondly, current deep learning approaches (e.g., LSTM [55]) generally demand high computational resources and hardware performance, highlighting the urgent need for real-time control through device miniaturization, energy optimization, and algorithmic simplification (e.g., using MCUNet). Furthermore, to enhance system responsiveness, exoskeleton actuators must be sufficiently lightweight, provide a low backdrivability, and ensure a high bandwidth to accommodate sudden changes in gait speed and non-periodic movements.
4.1.4. A Summary of Supervisory-Layer Control
In CPLLE, gait phase recognition primarily relies on TLP and FSM methods. TLP offers computational simplicity, making it suitable for passive training and algorithm validation. It can also serve as a low-cost initialization method when gait rhythm has not yet been established. However, its adaptability is limited, making it difficult to handle training scenarios with frequent gait variations or gradually increasing volitional participation. FSM, through phase segmentation and event-triggered transitions, provides a clear structure and stable logic, making it suitable for children with a limited cognitive capacity and partially established gait rhythm; however, its discrete-state nature restricts continuous adjustments at lower control levels, hindering fine-tuned regulation for personalized assistance. In contrast, ML-based approaches offer gait prediction capabilities and can output continuous gait phases, making them theoretically more suitable for recognizing complex features in CP training, such as dynamic changes, multi-modal inputs, and non-periodic gait patterns. However, due to requirements for large datasets, system performance, and real-time execution, their deployment in CPLLE remains challenging.
Therefore, the selection of supervisory control methods should comprehensively consider the patient’s training stage, gait complexity, cognitive capacity, and processor capability, to achieve a stable, safe, and progressively adaptive gait phase recognition mechanism. The specific characteristics and applicability of each method are summarized in Table 2.
Table 2.
A comparison of several supervisory-layer control strategies.
4.2. Action-Layer Control: Command Generation
As another component of the high-level controller, the action layer is responsible for converting gait phase information from the supervisory layer into specific displacement or torque commands, thereby driving CPLLE actuators to execute the desired movement. Functioning as the interface between gait phase recognition and actuator control, this layer plays a pivotal role in CPLLE architecture and is central to nearly all exoskeleton control strategies. In pediatric CP rehabilitation, due to stage-dependent differences in volitional participation and motor control accuracy, action layer strategies must offer a high adjustability and compliance to balance precise execution with individual adaptation.
4.2.1. Position Profile (PPR)
PPR is the most straightforward method for planning CPLLE actuator trajectories, ensuring that actuators track predefined target points or motion trajectories during training.
- Predefined Position Profiles
A predefined position profile is one of the simplest and most direct trajectory planning methods, commonly utilized in the initial stages of exoskeleton development or in passive mode design. As illustrated in Figure 5a, this method involves the device strictly following a pre-set gait trajectory (dashed line) to adjust the patient’s lower-limb joint angles (solid line). The shaded area in the figure represents the deviation between the target and actual trajectories, where larger areas generally indicate higher levels of passive intervention torque applied by the system to enforce the prescribed motion rhythm. These methods have a low computational cost and provide clear rhythmic patterns, making them practical for early-stage rehabilitation in children with CP who have limited muscle strength and underdeveloped motor control.
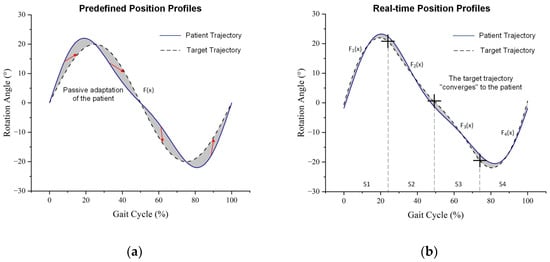
Figure 5.
Illustrations of joint angle changes in the patient and CPLLE under two position profile modes (shaded areas indicate deviations between the patient and device trajectories): (a) predefined position profiles; (b) real-time position profiles.
Reference gait trajectories can be obtained by extracting discrete data from standard gait databases and fitting them using polynomial functions or Fourier series, thereby converting discrete motion data into continuous target motion trajectories. When existing database records do not fully meet specific requirements, motion capture (MOCAP) systems can be employed to construct customized reference gait trajectories. For instance, studies [68,69,70,71,72] utilized a Kinect-LabVIEW motion capture system to record healthy gait trajectories, which were subsequently applied in a series of improved sliding mode controllers to achieve gait tracking. Furthermore, if additional constraints on the reference trajectory are required, mathematical modeling can be incorporated to generate reference trajectories. For example, in study [99], to ensure smoothness and physical feasibility, a mathematical model was employed to generate a trajectory that mimics a healthy gait, characterized by a bounded position and velocity and possessing second-order differentiability.
An alternative and more flexible approach involves generating motion trajectories based on predefined input conditions prior to training. For instance, in study [61], the exoskeleton system enables users to select different operating modes and specify movement cycle speeds (e.g., 1 to 5 km/h). The system then generates synchronized trajectory signals based on predefined gait models. Similarly, in study [62], the exoskeleton control system employs a high-level controller to generate gait patterns, sinusoidal waveforms, or user-defined custom trajectories. The system autonomously adjusts knee flexion and extension angles according to the selected mode, thereby facilitating adaptive rehabilitation training. However, most of these trajectory generation mechanisms do not account for the dynamic variability in motor abilities and training responses among children, posing challenges in balancing generalization and personalization.
- 2.
- Real-time Position Profile Generation
Although predefined trajectories are easy to implement and robust to disturbances, they exhibit limitations in complex training environments and under higher rehabilitation demands. To address these challenges, some CPLLE systems adopt online motion trajectory generation. As shown in Figure 5b, the system generates real-time trajectories based on either predefined temporal nodes (e.g., S1–S4) or key gait events (such as initial contact and toe-off), allowing for adaptation to the user’s current motion state. Compared to the predefined trajectory shown in Figure 5a, the deviation between the user’s actual motion and the system trajectory (represented by the shaded area) is significantly reduced, indicating that this method can effectively decrease the required corrective torque and enable a smoother, more personalized assistive control. This approach is particularly important for the mid-to-late stages of rehabilitation in children with CP, as it enables control strategies that better align with their improved motor abilities and volitional intent.
In a weight-shifting-based exoskeleton study [33], online trajectory generation focused on center-of-mass (COM) transitions during double support and on real-time gait-triggered adjustments. This system computes gait parameters (e.g., step length and step height) based on user inputs (e.g., lower-limb length) and employs an inverse kinematics model to dynamically generate joint motion trajectories.
Similarly, in [83], a TCP-driven artificial muscle exoskeleton used a mathematical model to generate motion trajectories online, establishing a relationship between input power and angular displacement, while further optimizing controller performance through experimental validation.
Machine learning has also been integrated into position profile generation. For instance, ref. [75] applied an adaptive neuro-fuzzy inference system (ANFIS) to handle parameter uncertainties and external disturbances. When the actual trajectory deviated from the expected motion, ANFIS computed compensation signals, guiding the system back onto the correct trajectory. These methods hold promise for dynamically responding to individual differences and gait variability. However, they have so far been validated primarily in healthy subjects or simulation settings, and further investigation is needed to assess their stability and effectiveness in rehabilitation training for children with CP.
4.2.2. Torque Profile (TPR)
In CPLLE rehabilitation training, actuators can operate not only based on position profiles but also following torque profiles, where the applied torque varies over time. Compared to adult patients, children with CP experience ongoing development in muscle control and volitional participation. This requires a higher precision in torque amplitude, timing, and compliance. Therefore, torque control strategies must offer stronger dynamic adjustment and individual adaptability.
- Constant Torque Profile
The simplest torque profile involves applying a constant torque by the actuator, which is a rarely predefined profile in CPLLE torque profile design. As shown in Figure 6, studies [19,29,53,54] proposed two torque output modes, one of which is the Constant mode (red curve) that delivers a constant extension torque. Gait phases were segmented using an FSM, and the system applied constant torque during specific moments of the early stance, mid-stance, and swing phases, while no intervention was applied in other phases. This method is simple to implement and can enhance knee joint stability and assist gait progression. In contrast, study [64] allowed users to incrementally adjust the assistive torque to provide personalized support.
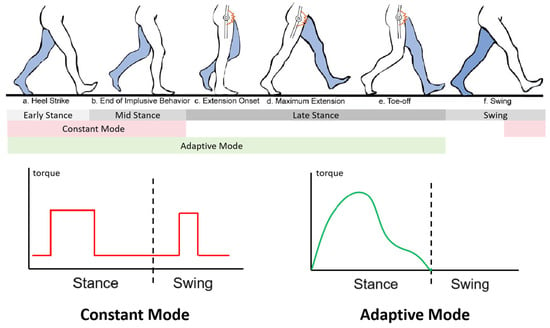
Figure 6.
Two torque output modes designed in P.REX [54]: constant torque output (red curve), and online torque profile generation (green curve).
Such constant torque is often used as a supplement when impedance control alone cannot provide sufficient instantaneous support. It offers immediate assistance when the user requires rapid support to counteract ground impact forces. Additionally, after prolonged active training, constant torque can be used for brief muscle and joint relaxation to alleviate fatigue. However, this strategy lacks the ability to dynamically respond to individual states and training stages in children, making it unsuitable for long-term reliance.
- 2.
- Real-Time Torque Profile
Unlike position profiles, the torque variation of exoskeleton actuators is influenced by the environment and the user’s voluntary movements, exhibiting rapid fluctuations that make it difficult to meet ideal rehabilitation needs through predefined trajectories. Therefore, most torque profiles must be generated online in real-time, requiring the system to have a high robustness and real-time performance. For children with CP, who often exhibit unstable gait rhythms and varying training compliance, online torque profiling provides a crucial means to adjust assistance intensity and direction as needed. It plays a key role in delivering compliant support and facilitating the gradual transition to active training.
As illustrated in Figure 6 [19,29,53,54], the Adaptive mode (green curve) represents a typical example of real-time torque profile generation. Unlike the Constant mode, which delivers uniform assistance, the Adaptive mode applies torque only during the stance phase and dynamically adjusts its output based on joint angles and gait phase. As shown in the right panel of the figure, the torque output varies continuously, with the peak typically occurring in early stance and gradually decreasing thereafter. This pattern reflects a high degree of synchrony with the user’s voluntary joint torques, enabling a more natural and responsive assistance. Similar studies [15,16,41,42,43,44,45,46,47,48,49] proposed the Proportional Joint-Moment Control algorithm. This method uses insole force sensors to measure ground reaction forces, estimate ankle joint biomechanical torque, and dynamically adjust exoskeleton assistance to achieve personalized support. Building on this, the research team further applied a Sigmoid function to smooth the torque signal, enhancing user comfort [47], and extended the approach to a resistance training mode that enhances neuromuscular engagement [11,20,50,51,52]. Additionally, study [101] introduced an impedance reduction control algorithm, which integrates a low-inertia motor with an ankle force sensor to achieve real-time torque adjustments, thereby reducing user discomfort during walking.
Other studies have adopted different technological approaches to dynamically adjust the torque output of exoskeleton actuators in real-time. For instance, study [78] used a momentum-based controller to assist children during the squat-to-stand transition. The controller aims to drive both the system’s angular momentum and its derivative toward zero, thereby achieving static balance. By continuously measuring angular momentum, the actuator torque is computed in real-time to adjust posture. Such strategies enhance the naturalness of assistance and user acceptance, and are particularly suitable for children with limited cognitive engagement. Additionally, ML can be used to compensate for gait uncertainties. Study [76] employed an Adaptive Radial Basis Function Neural Network (ARBFNN) to generate torque profiles online. Leveraging the powerful approximation capability of RBFNN, this approach enables the estimation and compensation of dynamic parameter uncertainties and external disturbances.
Real-time torque profile generation does not necessarily require complex control algorithms. In some exoskeletons, the unique actuation mechanisms enable precise torque control, making them inherently suitable for real-time torque profile generation. For example, study [30] introduced a modular electromagnetic braking unit that generates frictional torque via electromagnetic adhesion. By integrating gait phase detection and dynamic voltage regulation, it provides adaptive torque support. Similarly, study [32] explored Series Elastic Actuators (SEA), where assistance or correction of joint motion is achieved by adjusting spring deflection and stiffness. Such hardware–software co-adaptive strategies offer practical value in mitigating excessive actuator rigidity and unnatural human–machine interaction in children with CP, thereby improving device transparency and training comfort.
4.2.3. Impedance Control (IC)
Beyond torque profile control, IC is another commonly used active training control strategy. Unlike PPR and TPR, which directly regulate position or force, IC does not explicitly dictate motion trajectories. Instead, it dynamically regulates the force–position relationship, influencing the system’s motion response. The controller computes torque output based on a virtual dynamic model, enabling compliant interaction between user and device, and allowing the CPLLE to provide both assistance and adaptability to user-initiated movement. This control approach is particularly suited for the transitional phase in gait training for children with CP, where they gradually shift from fully passive to active participation. It helps to balance external guidance with voluntary output.
- Impedance Control Based on Inertia–Stiffness–Damping Dynamic Systems
This approach models a virtual mechanical system comprising inertia, stiffness, and damping to simulate exoskeleton dynamics, making it particularly suitable for tasks requiring a high interactive adaptability. For instance, in [65,66,67], an IC-based lower-limb exoskeleton was developed to assist CP children in gait rehabilitation. The “transparent mode” control strategy employed in this system was built upon a feedback zero-torque controller, which incorporated a double-pendulum model for inertia compensation and a LuGre friction model for friction compensation, effectively eliminating dynamic interference from the exoskeleton and actuator impedance. Similarly, ref. [27] introduced a unilateral exoskeleton designed for hemiplegic CP children, with a primary emphasis on IC. This system incorporated position and velocity feedback, along with a gravity compensation term. By accurately computing the gravity vector, the controller effectively compensated for additional loads induced by the exoskeleton’s weight, enabling users to move more freely and naturally. Such strategies offer a control-level solution to compensate for system rigidity in scenarios where hardware cannot be fully lightweight or compliant.
- 2.
- Force-Field-Based Impedance Control
In CPLLE, most impedance controllers adjust assistance levels based on joint motion states (i.e., joint angle and velocity). The core control strategy directly computes assistive torque from joint position and velocity, without explicitly incorporating inertia or acceleration control. This approach modulates stiffness and damping to establish a “force-field”, allowing the system to respond to deviations from the desired joint trajectory, thereby optimizing gait control and providing adaptive assistance. Compared to traditional position control methods, force-field impedance control can respond more naturally to the child’s movement intent and external disturbances, making it suitable for the mid-stage of rehabilitation when volitional participation is gradually recovering.
For instance, in [12], a knee exoskeleton utilized bidirectional assistance (flexion and extension) to improve the kinematic characteristics of crouch gait, dynamically adjusting assistance levels based on joint state to reduce oscillations and enhance gait control. The CPLLE assistive torque was proportional to the deviation of the joint angle from the target angle, with linear variations at state transitions to avoid abrupt torque fluctuations. A similar control principle was applied in [81], where an ankle exoskeleton controller computed assistive torque from the difference between the actual and target ankle angles, incorporating phase-specific stiffness adjustments.
Other studies have explored similar force-field-based approaches. In [29,53,54], a “virtual wall mode” was proposed, defining a desired trajectory as a virtual boundary. When the joint angle deviated, the controller applied dynamic resistance or assistance to restore the joint to the target trajectory. The resistance magnitude adapted to user effort and was independent of predefined timing parameters. Similarly, ref. [101] introduced an “impedance reduction algorithm”, precisely controlling system impedance to minimize mechanical resistance, reducing device interference with active user movements, achieving transparent assistance, and enhancing training comfort and adherence.
Additionally, a “virtual spring” approach has been widely adopted in IC design. This method constructs a virtual model analogous to a physical spring, which dynamically adjusts in response to body movement, ensuring appropriate assistive force delivery. In [64], a CPLLE system was developed to support either a constant torque mode or a virtual spring mode, where the latter calculated output torque based on the difference between measured and target joint angles. Another study [84] introduced an Adaptive Assistance on Demand (AAN) control strategy, optimizing stiffness and compliance to enhance user-exoskeleton interaction adaptability. Expanding on this concept, ref. [17,85,86,87,88] integrated AAN with virtual spring behavior, dynamically adjusting elasticity and compliance. By employing torque sensors to measure micro-deformations in the joint housing, the system delivered precise assistance while maintaining a compact joint module design.
4.2.4. Virtual Constraints (VC)
In CPLLE control algorithms, gait control can be reformulated as a constraint tracking problem, where gait phases are represented by parameterized configuration-dependent variables. This approach allows users to maintain active control over walking movements while ensuring that the gait trajectory conforms to predefined patterns, thereby enhancing stability and control performance. For children with CP, VC can maintain the stability of fundamental gait structures while allowing moderate space for volitional participation. It is particularly suitable for patients with preserved cognitive function and the emerging ability to express voluntary intent during the mid-to-late stages of rehabilitation.
For example, in [80], a virtual constraint control method based on hybrid zero dynamics (HZD) was proposed. By constructing a zero dynamics manifold, this method ensured a dynamic stability of the gait trajectory. The gait phase variable was defined as a monotonically increasing scalar, computed using hip position, IMU data, and joint angle sensors. The optimized control strategy then guided the gait evolution accordingly. HZD control reduces reliance on time-based gait progression, allowing for a more natural gait execution while maintaining virtual constraints within the zero dynamics manifold. Simulation results demonstrated that this method successfully generated stable human-like gait trajectories and improved system robustness.
A subsequent study [79] further refined the gait phase variable definition and validated the VC control approach on a physical exoskeleton prototype. Experimental results indicated that, compared to traditional PD control, VC control significantly reduced gait variability (hip joint: 36.72%, knee joint: 16.28%), lowered the average torque consumption (hip joint: 35.89%, knee joint: 4.44%), and was reported by users as more intuitive and user-friendly.
In summary, the VC method shows potential in guiding gait and enhancing user autonomy. However, its application remains limited to validation in healthy children, lacking systematic evaluation in patients with gait impairments. Moreover, it exhibits an insufficient adaptability to natural gait fluctuations during practical use, where disturbances and phase errors may compromise control stability. Although it improves motor autonomy, a trade-off exists between gait correction and increased muscular load, indicating that further optimization is required to balance stability, load management, and adaptability for clinical applications.
4.2.5. Electromyography-Based Control (EBC)
Unlike the binary switching applications of EMG signals, muscle activity amplification relies on real-time EMG monitoring and analysis. This method amplifies weak EMG signals via electrodes, enabling precise user intent detection. The processed EMG signals are used to estimate the required joint torque, establishing a linear relationship between muscle activity and joint torque, allowing the CPLLE to dynamically adjust assistive force in response to user effort. This method is suitable for children with CP who retain some voluntary motor intent and residual muscle strength. It can directly respond to their volitional control needs and provide a data foundation for refined, personalized assistance.
The HAL exoskeleton system has continuously refined muscle activity amplification as a core control strategy, enhancing joint torque estimation accuracy and expanding its application to hemiplegic rehabilitation training [26] and stair-climbing assistance [40]. While this method integrates enhanced EMG signals with motion control algorithms to effectively support patients with motor impairments, improving natural motion and assistance efficiency, EMG signal reliability is affected by skin conductivity, individual variability, and motion artifacts, leading to signal fluctuations that reduce accuracy. Additionally, signal processing latency, particularly during rapid movements or complex environments, can impact real-time exoskeleton torque adjustment, limiting the applicability of EMG-based control in CPLLE.
4.2.6. A Summary of Action-Layer Control
In the action layer, PPR and TPR are categorized as direct output control methods. PPR focuses on trajectory tracking and is suitable for early rehabilitation when gait rhythm is not yet established, but it lacks adaptability to individual differences. TPR adjusts joint torque in real time, supporting active gait progression in mid-to-late stages. It offers a better compliance and assistive force modulation but requires a higher sensor accuracy and computational resources. IC and VC represent interaction-oriented strategies. IC compensates for complex gait patterns and fluctuations in motor ability during mid-stage rehabilitation but depends on accurate system modeling. VC uses trajectory constraints to guide gait evolution, enhancing user autonomy and control consistency. It is suitable for users with emerging volitional control but is sensitive to disturbances and requires additional robustness mechanisms. EMG-based methods estimate joint torque to improve gait naturalness and user engagement. However, variability in signal quality and latency poses challenges for real-time and stable control.
Therefore, action-layer control in CPLLE must be dynamically matched to the child’s cognitive status, muscle strength, rehabilitation stage, and actuator characteristics. A hybrid, adaptable, and fault-tolerant control architecture is often required to accommodate individual variability and the progressive nature of rehabilitation. The control method selection should consider functional goals, user adaptability, real-time performance, and system complexity. The differences between various methods are shown in Table 3.
Table 3.
A comparison of several action-layer control strategies.
4.3. Execution-Layer Control: Command Execution
The command execution layer represents the lowest level of the CPLLE control architecture. It is responsible for executing position or torque commands issued by the higher-level control strategies and is typically highly dependent on the actuation hardware used in the exoskeleton. Low-level control can be custom programmed within the MCU or directly implemented using servo motors with built-in control functions. The primary objective of this layer is to achieve accurate and stable command tracking and execution. In addition to ensuring control precision, it must also account for the safety of pediatric users, tolerance to response errors, and the compliance of device actuation.
4.3.1. Closed-Loop Position Control (CLP)
The CLP is one of the most widely used low-level control methods in CPLLE. Its strength lies in the precise tracking of actuator trajectories, facilitating structured movement guidance and rhythm establishment during early rehabilitation. It is particularly suitable for providing clear and stable training output in fully passive or low-participation stages.
- Rigid Actuation Mechanisms
Rigid transmission systems utilize high-precision gears or harmonic reducers, ensuring a precise force transmission through rigid connections. These mechanisms offer a high load capacity and superior trajectory tracking accuracy, relying on closed-loop feedback control through motors and sensors.
For example, in [33], a brushless DC motor (Maxon EC-flat) was connected to a harmonic reducer, with PID control integrated within the Maxon EPOS4 driver and gain tuning performed at the main controller level, ensuring precise trajectory tracking. The CP-Walker system [17,86,87,88] implemented PID trajectory control using harmonic drives coupled with potentiometer feedback. In [77], a passive-mode exoskeleton incorporated a high-reduction gearbox with PD control, optimizing dynamic performance. Additionally, studies employing 3D-printed rigid structures (e.g., [80,84]) integrated embedded encoder feedback and PID control, achieving a balance between a lightweight design and high-precision control. However, the rigid structure may lead to high mechanical impedance and non-compliant human–robot interaction. This can limit adaptability, especially in the later stages of rehabilitation for CP, where gait variability increases and force control demands become more prominent.
- 2.
- Flexible Actuation Mechanisms
Flexible transmission systems utilize elastic components or smart materials to buffer force and motion, enhancing safety and adaptability. However, their nonlinear characteristics impose higher control requirements. Commercial actuators compatible with flexible CPLLE designs are relatively scarce, often necessitating customized low-level control strategies.
For instance, in [83], a TCP actuator was employed to mimic muscle contraction, with PID parameter optimization conducted in MATLAB/Simulink (MathWorks, https://www.mathworks.com/, accessed on 19 May 2025). Similarly, in [31,32], a SEA was integrated with an embedded position controller, allowing for the precise regulation of assistance while maintaining safety and control accuracy. Flexible actuator systems are particularly well suited for the mid-to-late stages of rehabilitation, when patients begin to exhibit voluntary motor output. They can absorb excessive force feedback and reduce the risk of injury from sudden errors. Their low-level position control strategies often incorporate displacement estimation and feedback regulation of elastic elements to achieve controllable dynamic compliance.
4.3.2. Closed-Loop Torque Control (CLT)
CLT is typically integrated with IC or TPR to precisely track target-torque values and execute high-level motion commands. Compared to position control, torque control better captures the dynamic interaction forces between the device and the user. In CP rehabilitation, it is particularly suitable for mid-to-late training stages, where it supports the gradual facilitation of voluntary output, compliant intervention, and neuromuscular engagement. However, most CPLLE actuators lack direct torque measurement capabilities. Some modern servo motors estimate torque output based on current values and torque constants, but these estimates are inherently limited in accuracy. Therefore, implementing CLT generally requires an additional torque measurement system to provide reference data for closed-loop control.
- Rigid Torque Transmission
Rigid transmission systems are the most common torque delivery mechanisms. As demonstrated in [27,63], brushless DC (BLDC) motors are coupled with harmonic drives, with real-time sensor feedback monitoring joint angle, velocity, and torque. A PD-based impedance controller utilizes these feedback signals to adjust actuator output, achieving precise target-torque tracking.
Some studies [17,65,66,67,84,86,87,88] further enhance torque sensing resolution by embedding strain gauges on metal rods and employing Wheatstone bridge circuits for increased sensitivity, enabling the real-time measurement of user–robot interaction forces and supporting both zero-torque and IC modes. This structure offers high precision and strong signal stability, making it suitable for rehabilitation stages requiring accurate force control. However, in children with CP, the high mechanical impedance of rigid structures may reduce comfort and safety. In cases of significant gait variability or muscle weakness, it may lead to overcompensation or interference in force feedback.
- 2.
- Flexible Torque Transmission
Flexible transmission systems utilize Bowden cables [15,16,37,41,42,43,44,45,46,47,48,49,110], sprockets [45], or Kevlar cables [103,104] to connect the motor to the joint, where torque sensors on single-joint exoskeletons enable PID-based closed-loop control. Another approach is the SEA, as seen in [32,64,82], where a spring is placed between the motor and the joint, allowing joint torque estimation based on spring deflection. By integrating motion monitoring and adaptive control algorithms, dynamic torque adjustments can be made to meet rehabilitation requirements.
Additionally, torque feedback can be derived through computational estimation rather than direct measurement. For instance, in [64], a 12-bit incremental encoder was used to measure the actuator angle and velocity, with torque calculated using impedance control equations, eliminating the need for dedicated torque sensors. These methods are suitable for compact systems with limited hardware integration but require high modeling accuracy and real-time control performance. They are susceptible to the effects of non-periodic gait patterns and fluctuations in muscle output in children.
4.3.3. Sliding Mode Control (SMC)
PID (or PD) closed-loop control is widely applied in CPLLE due to its simplicity and stability. However, comparative experiments in [115] indicate that individual variability, gait fluctuations, and system parameter uncertainties can impact its effectiveness in human–exoskeleton interaction. For example, variations in limb mass, segment length, and muscle strength in children, as well as random interactive forces during training, may increase PID control errors, ultimately affecting rehabilitation outcomes [116,117]. Consequently, some studies have introduced SMC to enhance system robustness.
SMC exhibits a strong resilience to uncertainties and disturbances, particularly Terminal Sliding Mode Control (TSM), which ensures asymptotic error convergence within a finite time. However, TSM suffers from singularity issues and chattering effects caused by the sign function, leading researchers to propose several improvements. For instance, ref. [116] implemented Fuzzy Sliding Mode Control (FSMC), where control parameters are adaptively adjusted based on error magnitude, thereby reducing chattering and excessive torque output. Similarly, ref. [115] introduced a function to replace , mitigating chattering effects while preserving control precision.
In the CPLLE domain, SMC has been successfully implemented in exoskeleton prototypes. For example, in [115], an adaptive high-order sliding mode control approach was introduced, integrating the Super-Twisting Algorithm to reduce chattering effects. In 2022, Narayan’s team proposed a non-singular terminal sliding mode control (SFTSM) [68], incorporating boundary layer techniques and saturation functions to enhance error convergence and chattering suppression, demonstrating a superior performance compared to ERL-SM and LQR-ANFIS methods. In 2023, the same team introduced an Improved Fast Non-Singular Terminal Sliding Mode Control (IFNSTSM) [69,70], integrating a double-exponential reaching law, which achieved a better stability and lower energy consumption than FNSTSM and TSSM. Further advancing this research, in 2024, they developed a Fast Terminal Sliding Mode Control with Rapid Reaching Law (FTSM-RRL) [71]. Experimental results confirmed that this approach significantly outperformed PID and FTSM-ERL in terms of error reduction and convergence speed.
Regarding the limitations of this method, it should be noted that, similar to other less widely applied control strategies, even in the comprehensive studies on SMC by Narayan’s team [68,69,70,71], validation was mostly conducted on small cohorts of healthy children or within laboratory settings, lacking systematic evaluation of the heterogeneous characteristics of children with gait impairments. Furthermore, SMC imposes high demands on actuator responsiveness and system modeling accuracy. When implemented on low-cost hardware platforms, the control precision and energy efficiency may not reach optimal levels. These factors constrain the broader application of this method in CPLLE controller design.
4.3.4. Backstepping Control (BC)
Similar to SMC, BC is designed to handle external disturbances and system uncertainties. As a recursive control method, it constructs virtual control variables to progressively stabilize the system. This approach is particularly effective in non-matching disturbance scenarios, where control inputs and disturbance terms are distributed across different system equations, making compensation challenging for conventional control methods. BC gradually introduces control variables, ensuring system stability, and can parameterize unknown disturbances (e.g., sinusoidal signal decomposition), thereby enhancing robustness and environmental adaptability.
In [57], a typical Adaptive Backstepping Control (ABC) was implemented in an Ankle–Foot Orthosis. This algorithm used virtual control inputs to compensate for unknown disturbances, such as ground reaction forces and foot weight variations, while employing Lyapunov stability theory to ensure error convergence. Compared to PID control, ABC demonstrated a superior trajectory tracking accuracy and adaptability across different gait cycles and disturbance conditions.
A Robust Adaptive Backstepping Control (RABS) approach was later introduced in [107], modeling the system in strict-feedback form and designing control laws based on Lyapunov stability theory to guarantee error convergence. Compared to traditional BC, RABS utilized virtual control laws to mitigate parameter overestimation and the explosion of derivative terms, thereby improving computational efficiency and control stability.
Although the BC method offers strong stability guarantees and a robust disturbance rejection, its application in pediatric exoskeletons remains limited. Firstly, existing studies are primarily based on healthy adult samples, lacking systematic validation in children with gait impairments, resulting in an insufficient practical adaptability. Secondly, this method requires a high system modeling accuracy and actuator performance, leading to an increased hardware complexity and cost. Although it improves trajectory tracking precision, it may suppress patient participation, which is detrimental to promoting active engagement during rehabilitation training.
4.3.5. A Summary of Execution-Layer Control
Unlike typical exoskeletons that often combine open- and closed-loop control [5], CPLLE relies more heavily on high-stability, low-latency closed-loop control mechanisms to meet the greater demands for safety, accuracy, and responsive feedback in training children. Currently, CLP and CLT are the two primary approaches used. Position control is commonly used in early-stage development or fully assistive modes, where rigid transmission ensures high-precision trajectory tracking, while flexible transmission enhances interaction safety. Torque control, on the other hand, integrates real-time feedback to dynamically adjust joint torque, allowing adaptive gait assistance. SMC offers a high robustness, making it suitable for complex environments and uncertain disturbances. BC, by recursively constructing virtual control variables, provides a more precise compensation under non-matching disturbances and is better suited than SMC for handling dynamically complex system behaviors.
The selection of low-level control strategies in CPLLE depends not only on control precision and system load but also requires a comprehensive assessment of individual patient characteristics, rehabilitation stage, and platform resources. Emphasis is placed on multi-strategy integration to establish a closed-loop execution system that balances stability, compliance, and adaptability. The details of different execution-level controls are compared in Table 4.
Table 4.
A comparison of several execution-layer control strategies.
5. Clinical Effectiveness
Beyond the technical design of CPLLE control strategies, a clinical validation of their effectiveness is equally critical. Although various types of CPLLE control strategies have been developed, exoskeleton devices that have undergone clinical validation in patients with CP remain scarce [47]. Most strategies have only demonstrated functional feasibility at the technical level or have been tested in healthy children or adults, neglecting the specific gait abnormalities in CP patients. Given the high heterogeneity of gait characteristics in CP [3], the effectiveness of control strategies must be verified through multi-cohort, large-sample clinical studies that can directly link gait improvements to control design.
5.1. Clinical Characteristics of the Participants
Based on the above strict selection criteria, five representative CPLLE devices were selected from 46 control strategies for analysis, including two single-joint CPLLEs (developed by the Lerner team) [15,16,44,45,56,58,59,60], HAL [96,97,98], CPWalker [17,54,86,88], and Lokomat [54,106,118]. According to the available reports, after excluding cases of paraplegia and subjects with unspecified diagnoses, a total of 96 valid participant data were recorded. Among them, 5 participants were classified as Gross Motor Function Classification System (GMFCS) level I, 49 as level II, 18 as level III, and 4 as level IV. Regarding CP types, spastic diplegia was the most prevalent, accounting for 69 cases.
5.2. Clinical Validation of the Control Strategy
In the field of volitional intent recognition control strategies, the HAL system is representative. Its Cybernic Voluntary Control (CVC) mode, driven by electromyographic signals, demonstrated improvements in self-selected walking speed (SWS) and step length among patients with GMFCS levels I–III. The GMFM total score increased from 157.7 ± 19.9 to 166.2 ± 23.4 (p = 0.012), with particularly notable improvements in standing and walking-related functions. Nevertheless, changes in walking speed and step length in some patients did not reach statistical significance, suggesting that insufficient muscle strength or neuromuscular activity may limit the effectiveness of the CVC mode [96]. To enhance adaptability, the HAL system switches via a FSM to a ground reaction force-based assistance mode, highlighting the need for volitional intent recognition to be integrated with stable and reliable control mechanisms in clinical applications.
Action-layer control strategy design has a more direct impact on clinical rehabilitation. Mature multi-joint CPLLE devices generally adopt multi-mode transition strategies, emphasizing active participation and functional recovery during training. CPWalker integrates position trajectory control (PPR), zero-impedance transparency control (IC), and AAN strategies, with clinical effectiveness validated through 10 sessions of personalized training over 5 weeks in 14 sessions involving GMFCS II–III spastic diplegic patients. Lokomat, based on standard trajectory control, incorporates body weight support adjustment, impedance control, and enhanced feedback modules, covering 30–34 similar patient sessions over 4–8 weeks and 12–16 training sessions. Clinical data show that in the CPWalker group, walking speed increased by 51.94% and step length by 26.49%; in the Lokomat group, walking speed improved by 14%, and step length increased by approximately 0.05 m for both legs. Additionally, the single support phase was prolonged, and the double support phase shortened, leading to significant improvements in gait symmetry and stability. In terms of functional outcomes, GMFM dimension D and E scores showed statistically significant improvements in both groups, and patient feedback indicated that AAN-based assistance modulation enhanced their training comfort, sense of achievement, and autonomy.
In comparison, single-joint CPLLEs, characterized by lightweight structures and a superior backdrivability, have lower transparency requirements and focus clinical validation on improving key joint functions and gait correction [45]. In the ankle and knee exoskeletons developed by the Lerner team, training or testing was conducted over 2–10 weeks in 23–26 and 20–22 sessions involving patients with GMFCS levels I–III, respectively. For the ankle CPLLE, experiments demonstrated a 7–8% increase in walking speed, a 0.15–0.17 m increase in step length, a 22–25% reduction in soleus muscle activity, and a 15–18% reduction in metabolic energy expenditure, indicating an enhanced push-off propulsion and improved energy efficiency. For the knee CPLLE, results showed an 8–13° increase in the knee extension angle during the stance phase, a 6.8° improvement in the initial contact angle, and a 35–76% reduction in support phase joint torque loads, effectively alleviating joint burden. Both devices employed FSM for precise gait event detection and incorporated adaptive assistance strategies to optimize output, achieving significant improvements in local lower-limb functions on lightweight platforms.
In summary, current clinical studies suggest that EMG-based intention recognition is suitable for patients with sufficient muscle strength, while traditional methods such as FSM or TLP approaches are more appropriate otherwise. Based on commonly used biomechanical and clinical indicators across different types of exoskeletons, multi-joint exoskeletons tend to produce more significant overall improvements. In contrast, single-joint exoskeletons offer more targeted control strategies for correcting specific abnormal gait patterns and improving localized lower-limb function.
6. Discussion
This review highlights the growing complexity of CPLLE controller design and the lack of comprehensive summaries in current research. By considering the unique objectives of CPLLE, this study structurally categorizes existing control strategies in CPLLE controllers based on a hierarchical classification framework. The proposed classification method examines 106 referenced studies, identifying 46 distinct CPLLE controller designs. These controllers are further structured into functional units based on their roles and input–output relationships. The control strategies are categorized into three hierarchical layers: the supervisory layer, responsible for gait phase recognition; the action layer, responsible for command generation; and the execution layer, responsible for executing motion commands. These layers are further classified into 12 specific control strategies, providing a systematic discussion of existing CPLLE control methodologies.
6.1. Characteristics of Controller Design
By reviewing and summarizing the CPLLE controllers discussed in the referenced studies, it becomes evident that the CPLLE controller design must not only meet the basic requirements for lower-limb gait rehabilitation but also account for the specific characteristics of CP children. As previously discussed, the control strategy should remain flexible and adaptive to accommodate fluctuations in physiological and cognitive states, varying levels of volitional participation during different training stages, and the hardware limitations of the system.
At the control hierarchy level, the design logic and selection criteria for control methods differ from those in typical adult exoskeleton systems. At the supervisory level, the instability of gait rhythm and limited cognitive capacity in children with CP require phase recognition strategies with a greater robustness and adaptability. At the action level, control strategies must deliver precise assistive forces or displacements. They must also accommodate stage transitions driven by changes in volitional participation. At the execution level, hardware constraints such as safety prioritization, limited resources, and the need for a lightweight structure make compliant modulation and multi-strategy integration essential for maintaining system stability.
For specific targeted objectives, current research on gait improvement primarily employs FSM, model predictive control, and dynamic torque modulation to optimize gait symmetry, stability, and energy efficiency. In muscle strength training, resistive training and functional electrical stimulation (FES) show complementary potential across different rehabilitation stages. However, further research is needed to tailor training protocols more precisely to individual needs. Regarding gait correction, specialized control strategies have been developed for the crouch gait, hemiplegic gait, and equinus gait. Control strategies for other abnormal gait patterns remain limited. This may be because these three gait types are more prevalent in children with CP, display clearer kinematic features, are relatively easier to address through control implementation, and allow for an easier access to clinical validation samples. For the evaluation of correction effectiveness, the biomechanical indicators related to localized joint torque loading and EMG activity reported in [15,16,44,45,56,58,59,60] provide valuable reference. Additionally, although existing research has devoted less attention to stand-to-sit transitions and stair climbing, these functional training modalities are crucial for improving CP children’s daily living abilities and psychological confidence, warranting a greater focus in future studies.
In summary, CPLLE control strategies must be designed with a full consideration of their fundamental differences from adult exoskeletons in objectives, user characteristics, and system limitations. When adapting or innovating based on adult exoskeleton strategies, special attention should be paid to the distinct nature of CPLLE devices and their specific rehabilitation goals. To achieve diverse rehabilitation outcomes, control systems must support coordinated optimization across multiple layers, with high-level modules—particularly at the supervisory and action levels—playing a critical role in overall system performance. Existing studies [17,31,32,85,86,87,88] indicate that systems with multiple training functions are often associated with increased controller complexity. Therefore, generic control solutions are insufficient. Therefore, rather than applying generic solutions, a structured hierarchical framework—tailored to user profiles, rehabilitation objectives, and hardware limitations—should be adopted to ensure therapeutic effectiveness and safety.
6.2. A Summary of Current Research
Building on the discussion of rehabilitation objectives, this study provides a structured, hierarchical overview of CPLLE control strategies, categorized into supervisory, action, and execution layers. Among the 106 reviewed publications, this study employs a classification framework to decompose CPLLE controllers into distinct functional units, facilitating a structured analysis. The usage of control strategies at different levels is illustrated in Figure 7 below.
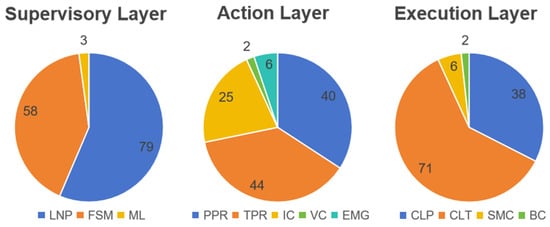
Figure 7.
The distribution of control strategy usage across different levels.
- A wide range of control strategies have been applied across the three-layer architecture. At the supervisory layer, most studies adopted either time-linear phase (TLP) or finite state machine (FSM) approaches, while machine learning (ML) remains in an exploratory stage.
- At the action layer, position and torque profile controls (PPR and TPR) are the most frequently used, whereas advanced adaptive methods such as impedance control (IC), electromyography-based control (EBC), and virtual constraints (VC) have received comparatively limited attention.
- In the execution layer, closed-loop torque (CLT) and position control (CLP) dominate, while nonlinear control strategies such as sliding mode control (SMC) and backstepping control (BC) are found only in a few isolated cases.
- Despite the diversity in design, only a small subset of these strategies—five out of the 43 identified—have been supported by multiple clinical studies demonstrating significant improvements in CP rehabilitation outcomes. This highlights a considerable gap between technical exploration and clinical validation in the current CPLLE research landscape.
The current CPLLE controller strategies are relatively concentrated, with most designs specifically tailored to the rehabilitation needs of children with CP. Specifically, for patients with severely limited mobility, CPLLE controllers predominantly employ a TLP + PPR + CLP combination to enable fully assistive passive training. In contrast, for patients retaining partial motor function, an FSM + TPR/IC + CLT combination is commonly implemented to promote user engagement and active participation. Clinical validations, including the HAL system and the single-joint knee/ankle CPLLEs by the Lerner group, confirm the effectiveness of these approaches. The adoption of FSM facilitates a natural segmentation of the gait cycle, enhancing state recognition and transitions, thereby improving adaptability across different patients and gait conditions. Similarly, applications such as CPWalker and Lokomat demonstrate that the TLP + PPR strategy offers stable and reliable trajectory guidance during the early stages of rehabilitation when patients are not yet capable of active training. Moreover, motion planning strategies employed in CPWalker and the Lerner group’s single-joint CPLLEs highlight the advantages of TPR in achieving localized improvements and correcting pathological gait patterns, while the IC strategy has been shown to significantly enhance system transparency in multi-joint CPLLEs. Collectively, these strategies align well with the biomechanical and clinical requirements of pediatric CP rehabilitation.
Despite the widespread application of traditional control methods, certain limitations remain in adaptability and personalized rehabilitation matching. For instance, TLP is primarily suited for cyclic gait patterns and lacks flexibility for real-time adjustments. Similarly, FSM-based control relies on predefined transition rules, making it less adaptive to complex gait variations. Additionally, traditional trajectory planning combined with closed-loop control exhibits constraints when addressing individual patient variability, gait fluctuations, and system parameter uncertainties, highlighting the need for more adaptive and intelligent control approaches.
To address the limitations of traditional control strategies, a range of novel control methods has emerged in recent years, including ML, VC, SMC, and BC. Among the reviewed studies in this paper, 13 publications explored these advanced control approaches. Notably, apart from a 2018 study on ML-based control [112], all other research in this category has been conducted since 2021. Although successful implementations of these novel control strategies in exoskeleton prototypes remain limited, an increasing number of studies have entered the simulation and preliminary design stages. The exploration of these emerging methods is expected to provide new solutions to overcome the limitations of traditional CPLLE control strategies.
However, it is regrettable that these emerging control methods currently lack sufficient clinical data to demonstrate their effectiveness. In practice, these strategies face several recurring challenges. Firstly, due to the high heterogeneity and collection difficulty of gait data, existing studies are generally based on very small sample sizes, lacking systematic evaluation in populations with gait impairments. Secondly, most strategies remain validated only under standardized experimental conditions, with a limited verification of their adaptability to real-world gait fluctuations and complex terrains. Thirdly, both deep learning models and nonlinear control approaches exhibit a high dependency on hardware performance and modeling accuracy, increasing the cost and difficulty of practical deployment. Finally, the lack of large-scale clinical trials and clearly defined regulatory pathways significantly constrains the translational potential of these novel control strategies.
Additionally, most current CPLLE controllers focus on three primary goals: providing adaptive assistance, ensuring the stable execution of assistive movements, and promoting gait reconstruction and neuromuscular rehabilitation. While the three-layer control framework—comprising gait phase recognition, command generation, and motion execution—has been well established, research on biological and environmental signal recognition for guiding the overall exoskeleton behavior transitions remains underdeveloped. Some studies classify such strategies as the highest control layer within the exoskeleton controller hierarchy [6], yet among the reviewed literature, fewer than 10% of studies have implemented intelligent behavior adaptation strategies that operate without manual switching by caregivers or users.
This limitation may stem from the fact that current CPLLE designs remain primarily tailored for controlled environments with high-intensity training protocols, rather than being optimized for complex and dynamic real-world conditions [5].
6.3. Discussion on Future Development Directions
CPLLE design has evolved from merely miniaturizing adult exoskeletons to developing tailored solutions for children with CP. Its training functions have expanded from single-mode passive assistance to support multi-objective adaptability and applications across diverse scenarios. As controllers and actuators continue to improve in performance, future CPLLE will face increasing demands for both enhanced assistive motion capabilities and improved environmental adaptability.
In terms of high-level control strategies, traditional FSM and their variants suffer from a limited flexibility, restricting functional expansion. Future designs may integrate lightweight models such as MobileNet or TinyML. They may also leverage embedded platforms capable of on-device inference, including NVIDIA Jetson, Google Coral, or K210, to enhance control optimization. Furthermore, advancements in edge computing, neural network pruning, and Transformer-based AI models have significantly enhanced the inference capabilities of low-power devices, driving progress in intelligent motion pattern recognition, environmental perception, and adaptive control. For instance, integrating reinforcement learning to train personalized gait models and dynamically adjusting assistive strategies based on real-time sensor feedback could greatly enhance training efficiency and user experience. Additionally, due to cost constraints, future research may explore new phase recognition algorithms such as adaptive oscillators [119,120], which can function without relying on high-performance processors, further optimizing CPLLE controller design.
Low-level control strategies in CPLLE are highly dependent on actuator selection and material properties. With advancements in lightweight, high-elasticity, and intelligent response materials, as well as the integration of AI, adaptive control, and predictive control, traditional servo motor-based commercial control systems may gradually be replaced by more flexible, custom-designed control algorithms. Techniques such as SMC and BC are expected to see wider adoption, offering not only cost reductions but also more personalized and adaptive control strategies.
Regarding clinical translation, most CPLLEs reported in current studies remain at the experimental stage and have not progressed to clinical trials or commercial deployment. Beyond the frequently discussed issues of regulatory compliance and ethical considerations, this review suggests that a critical additional factor may be the excessive focus on technical aspects during control strategy design, with insufficient attention to the practical demands of clinical rehabilitation. Based on previous analyzes, several recommendations for control strategy development can be proposed as follows: for instance, EMG-driven strategies, which suffer from unstable signal recognition, should be targeted toward specific patient groups and combined with more adaptable control modes in practice; for multi-joint exoskeletons, improving system transparency is essential; in addition, given that some patients cannot immediately engage in active training, multi-strategy transitional control designs are needed; and for single-joint exoskeletons, control strategies should prioritize targeted functional improvements and enhancements in energy efficiency.
Furthermore, as CPLLE development continues to mature, future research may extend beyond gait training to focus more on real-world applications and daily activities, emphasizing the need for rapid mode transitions and enhanced environmental adaptability. This shift will likely lead to a greater emphasis on higher-level control strategies, such as motion recognition and terrain adaptation, to further improve patient mobility in dynamic environments.
6.4. Limitations
It should be noted that this review has certain limitations:
This study conducted a literature search through the Web of Science and IEL databases, restricting the selection to publications in English. As a result, there may be limitations in the search scope, and some commercially available CPLLEs, for which only performance testing data are publicly available without detailed control strategy documentation, were excluded from the review [121,122,123,124,125,126]. It primarily focuses on active lower-limb exoskeletons designed specifically for CP children, excluding devices intended for spinal cord injuries, traumatic brain injuries, and other pediatric neurological disorders. Additionally, purely mechanical orthotic devices and studies limited to simulation without prototype validation were not included. While this narrow scope helps identify key patterns in CPLLE control systems, it may limit the applicability of findings to a broader range of pediatric rehabilitation devices.
In terms of clinical validation, although the representative CPLLE control strategies discussed in this review (e.g., HAL, CPWalker, and Lokomat) have been verified through moderately sized experimental trials and demonstrate a relatively high credibility, a considerable portion of the remaining studies involve only healthy children, adults, or a very limited number of patients. Some are confined to technical-level validations and lack direct evidence of clinical effectiveness. Therefore, these strategies are more appropriate as design references for controller development rather than established approaches with demonstrated rehabilitation outcomes.
Moreover, current clinical research on CPLLEs tends to focus on children with mild to moderate spastic CP (GMFCS levels I–III), while validation for those with more severe motor impairments (GMFCS IV–V) or other CP types (e.g., dyskinetic or ataxic CP) remains limited. Clinical evaluation indicators are predominantly biomechanical, such as walking speed, step length, and joint angles, whereas broader rehabilitation outcomes—such as daily functional independence (e.g., activities of daily living), quality of life (e.g., the Pediatric Quality of Life Inventory), user compliance, and satisfaction—are rarely assessed in a systematic manner. These limitations constrain the clinical scope of CPLLE control strategy evaluation and restrict the generalizability of this review’s conclusions to more severely affected patients and broader real-world applications.
7. Conclusions
This paper begins by addressing the specific challenges in CPLLE design, summarizes the differences in control strategy design compared to typical adult exoskeletons, and outlines the corresponding design objectives. A hierarchical, function-unit-based classification method for control strategies is proposed, which enables the systematic organization of CPLLE controllers across three key levels: the supervisory layer, action layer, and execution layer. This review focuses on the implementation methods of each control strategy at different levels and structurally categorizes their impact on rehabilitation, refining the fundamental design principles of exoskeleton controllers and providing a structured reference for controller development and control method implementation. It further highlights the patient-centered specificity of control strategy selection in CPLLE. This study addresses a gap in the current literature, where the unique characteristics of CPLLE have been acknowledged, but a systematic summary of control strategies reflecting these distinctions has been lacking.
Findings indicate that CPLLE controllers are typically optimized for specific rehabilitation goals, requiring clear objective definition before selecting an appropriate control strategy. Currently, most CPLLE control methods employ either TLP + PPR + CLP for fully assistive training or FSM + TPR/IC + CLT for partially assistive training, covering the entire rehabilitation cycle. However, adaptability and personalized matching remain significant challenges, driving recent research efforts toward exploring novel control methods to enhance CPLLE adaptability. Additionally, current CPLLE studies lack an effective utilization of biological and environmental signals, with control strategies still limited to predefined conditions, constraining exoskeleton applications in dynamic environments.
This study consolidates a wide range of control strategies, though direct performance comparisons are challenging due to variations in rehabilitation objectives and evaluation metrics. Nevertheless, trends in CPLLE development indicate that controller performance is continuously improving, with future designs expected to be more intelligent, flexible, and capable of adapting to complex environments while better meeting the needs of CP children. Advanced control strategies may incorporate lightweight machine learning models and embedded AI hardware, while low-power, high-precision phase recognition methods (e.g., approaches based on adaptive frequency oscillators) could be explored. At the low-level control layer, CPLLE may shift away from traditional commercial servo motor presets, adopting more precise autonomous control techniques such as SMC and BC. With growing emphasis on exoskeleton mode transitions and automatic adaptation in dynamic environments, future CPLLE controllers may integrate higher-level control strategies to facilitate full-system behavior adjustments.
In summary, CPLLE is no longer merely a downsized adaptation of adult exoskeletons. Its control strategy must be closely tailored to the unique physiological characteristics, cognitive abilities, and rehabilitation pathways of children with CP, while also addressing the implementation constraints imposed by lightweight structures and limited hardware resources. As a result, its child-centered design features have become increasingly prominent.
Author Contributions
Conceptualization, H.Y.; methodology, Z.K.; validation, Z.K. and Y.W.; investigation, Z.K. and Y.W.; resources, H.Y.; data curation, Y.W.; writing—original draft preparation, Z.K.; writing—review and editing, H.L. and H.Y.; visualization, Y.W.; supervision, H.L. and H.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
This work was supported in part by the National key research and development program of China (2023YFC3604800). We extend our gratitude to all contributors involved in the writing and refinement of this manuscript for their valuable insights and efforts.
Conflicts of Interest
The authors declare that there are no financial, commercial, or personal relationships that could be construed as potential conflicts of interest in this study.
References
- Gonzalez, A.; Garcia, L.; Kilby, J.; McNair, P. Robotic Devices for Paediatric Rehabilitation: A Review of Design Features. Biomed. Eng. OnLine 2021, 20, 89. [Google Scholar] [CrossRef] [PubMed]
- Gesta, A.; Achiche, S.; Mohebbi, A. Design Considerations for the Development of Lower Limb Pediatric Exoskeletons: A Literature Review. IEEE Trans. Med. Robot. Bionics 2023, 5, 768–779. [Google Scholar] [CrossRef]
- Sarajchi, M.; Al-Hares, M.K.; Sirlantzis, K. Wearable Lower-Limb Exoskeleton for Children with Cerebral Palsy: A Systematic Review of Mechanical Design, Actuation Type, Control Strategy, and Clinical Evaluation. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 2695–2720. [Google Scholar] [CrossRef] [PubMed]
- Narayan, J.; Dwivedy, S.K. Lower Limb Exoskeletons for Pediatric Gait Rehabilitation: A Brief Review of Design, Actuation, and Control Schemes. In Proceedings of the 2023 IEEE International Conference on Advanced Systems and Emergent Technologies (IC_ASET), Hammamet, Tunisia, 29 April–1 May 2023; IEEE: New York, NY, USA, 2023; pp. 1–6. [Google Scholar]
- Baud, R.; Manzoori, A.R.; Ijspeert, A.; Bouri, M. Review of Control Strategies for Lower-Limb Exoskeletons to Assist Gait. J. NeuroEngineering Rehabil. 2021, 18, 119. [Google Scholar] [CrossRef]
- Narayan, J.; Auepanwiriyakul, C.; Jhunjhunwala, S.; Abbas, M.; Dwivedy, S.K. Hierarchical Classification of Subject-Cooperative Control Strategies for Lower Limb Exoskeletons in Gait Rehabilitation: A Systematic Review. Machines 2023, 11, 764. [Google Scholar] [CrossRef]
- Laubscher, C.A.; Farris, R.J.; Sawicki, J.T. Design and Preliminary Evaluation of a Powered Pediatric Lower Limb Orthosis. In Proceedings of the International Design Engineering Technical Conferences and Computers and Information in Engineering Conference, Cleveland, OH, USA, 6 August 2017; American Society of Mechanical Engineers: Cleveland, OH, USA, 2017; Volume 5A, p. V05AT08A061. [Google Scholar]
- Lefmann, S.; Russo, R.; Hillier, S. The Effectiveness of Robotic-Assisted Gait Training for Paediatric Gait Disorders: Systematic Review. J. NeuroEngineering Rehabil. 2017, 14, 1. [Google Scholar] [CrossRef]
- Grau, A.; Morel, Y.; Puig-Pey, A.; Cecchi, F. (Eds.) Tracts in Advanced Robotics, In Advances in Robotics Research: From Lab to Market: ECHORD++: Robotic Science Supporting Innovation; Springer International Publishing: Cham, Switzerland, 2020; Volume 132, ISBN 978-3-030-22326-7. [Google Scholar]
- Reinkensmeyer, D.J.; Dietz, V. (Eds.) Neurorehabilitation Technology; Springer International Publishing: Cham, Switzerland, 2016; ISBN 978-3-319-28601-3. [Google Scholar]
- Harshe, K.; Tagoe, E.; Bowersock, C.; Lerner, Z.F. Priming Robotic Plantarflexor Resistance with Assistance to Improve Ankle Power During Exoskeleton Gait Training. IEEE Robot. Autom. Lett. 2024, 9, 10511–10518. [Google Scholar] [CrossRef]
- Lee, D.; Mulrine, S.C.; Shepherd, M.K.; Westberry, D.E.; Rogozinski, B.M.; Herrin, K.R.; Young, A.J. Mitigating Crouch Gait with an Autonomous Pediatric Knee Exoskeleton in the Neurologically Impaired. J. Biomech. Eng. 2024, 146, 121005. [Google Scholar] [CrossRef]
- Abdelhady, M.; Damiano, D.L.; Bulea, T.C. Attention-Based Deep Recurrent Neural Network to Estimate Knee Angle During Walking from Lower-Limb EMG. In Proceedings of the 2023 International Conference on Rehabilitation Robotics (ICORR), Singapore, 24–28 September 2023; IEEE: New York, NY, USA, 2023; pp. 1–6. [Google Scholar]
- Goo, A.; Laubscher, C.A.; Farris, R.J.; Sawicki, J.T. Design and Evaluation of a Pediatric Lower-Limb Exoskeleton Joint Actuator. Actuators 2020, 9, 138. [Google Scholar] [CrossRef]
- Tagoe, E.A.; Fang, Y.; Williams, J.R.; Lerner, Z.F. Walking on Real-World Terrain with an Ankle Exoskeleton in Cerebral Palsy. IEEE Trans. Med. Robot. Bionics 2024, 6, 202–212. [Google Scholar] [CrossRef]
- Fang, Y.; Orekhov, G.; Lerner, Z.F. Adaptive Ankle Exoskeleton Gait Training Demonstrates Acute Neuromuscular and Spatiotemporal Benefits for Individuals with Cerebral Palsy: A Pilot Study. Gait Posture 2022, 95, 256–263. [Google Scholar] [CrossRef]
- Bayón, C.; Ramírez, O.; Serrano, J.I.; Castillo, M.D.D.; Pérez-Somarriba, A.; Belda-Lois, J.M.; Martínez-Caballero, I.; Lerma-Lara, S.; Cifuentes, C.; Frizera, A.; et al. Development and Evaluation of a Novel Robotic Platform for Gait Rehabilitation in Patients with Cerebral Palsy: CPWalker. Robot. Auton. Syst. 2017, 91, 101–114. [Google Scholar] [CrossRef]
- Snodgrass, J.; Yan, S.; Lim, H.; Hameedduddin, I.; Wu, M. Design and Implementation of a Portable Knee Actuator for the Improvement of Crouch Gait in Children with Cerebral Palsy. In Proceedings of the 2023 45th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Sydney, Australia, 24–27 July 2023; IEEE: New York, NY, USA, 2023; pp. 1–4. [Google Scholar]
- Bulea, T.C.; Molazadeh, V.; Thurston, M.; Damiano, D.L. Interleaved Assistance and Resistance for Exoskeleton Mediated Gait Training: Validation, Feasibility and Effects. In Proceedings of the 2022 9th IEEE RAS/EMBS International Conference for Biomedical Robotics and Biomechatronics (BioRob) Seoul, Republic of Korea, 21 August 2022; IEEE: New York, NY, USA; pp. 1–8. [Google Scholar]
- Conner, B.C.; Remec, N.M.; Orum, E.K.; Frank, E.M.; Lerner, Z.F. Wearable Adaptive Resistance Training Improves Ankle Strength, Walking Efficiency and Mobility in Cerebral Palsy: A Pilot Clinical Trial. IEEE Open J. Eng. Med. Biol. 2020, 1, 282–289. [Google Scholar] [CrossRef]
- Washabaugh, E.P.; Claflin, E.S.; Gillespie, R.B.; Krishnan, C. A Novel Application of Eddy Current Braking for Functional Strength Training During Gait. Ann. Biomed. Eng. 2016, 44, 2760–2773. [Google Scholar] [CrossRef]
- Washabaugh, E.P.; Krishnan, C. A Wearable Resistive Robot Facilitates Locomotor Adaptations during Gait. Restor. Neurol. Neurosci. 2018, 36, 215–223. [Google Scholar] [CrossRef]
- Devine, T.M.; Alter, K.E.; Damiano, D.L.; Bulea, T.C. A Randomized Cross-over Study Protocol to Evaluate Long-Term Gait Training with a Pediatric Robotic Exoskeleton Outside the Clinical Setting in Children with Movement Disorders. PLoS ONE 2024, 19, e0304087. [Google Scholar] [CrossRef]
- Shideler, B.L.; Bulea, T.C.; Chen, J.; Stanley, C.J.; Gravunder, A.J.; Damiano, D.L. Toward a Hybrid Exoskeleton for Crouch Gait in Children with Cerebral Palsy: Neuromuscular Electrical Stimulation for Improved Knee Extension. J. NeuroEngineering Rehabil. 2020, 17, 121. [Google Scholar] [CrossRef]
- Rodda, J.; Graham, H.K. Classification of Gait Patterns in Spastic Hemiplegia and Spastic Diplegia: A Basis for a Management Algorithm. Eur. J. Neurol. 2001, 8, 98–108. [Google Scholar] [CrossRef]
- Kawamoto, H.; Hayashi, T.; Sakurai, T.; Eguchi, K.; Sankai, Y. Development of Single Leg Version of HAL for Hemiplegia. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; IEEE: New York, NY, USA, 2009; pp. 5038–5043. [Google Scholar]
- Sarajchi, M.; Sirlantzis, K. Design and Control of a Single-Leg Exoskeleton with Gravity Compensation for Children with Unilateral Cerebral Palsy. Sensors 2023, 23, 6103. [Google Scholar] [CrossRef]
- Fang, Y.; Lerner, Z.F. How Ankle Exoskeleton Assistance Affects the Mechanics of Incline Walking and Stair Ascent in Cerebral Palsy. In Proceedings of the 2022 International Conference on Rehabilitation Robotics (ICORR), Rotterdam, The Netherlands, 25 July 2022; IEEE: New York, NY, USA; pp. 1–6. [Google Scholar]
- Bulea, T.C.; Chen, J.; Damiano, D.L. Exoskeleton Assistance Improves Crouch during Overground Walking with Forearm Crutches: A Case Study. In Proceedings of the 2020 8th IEEE RAS/EMBS International Conference for Biomedical Robotics and Biomechatronics (BioRob), New York City, NY, USA, 29 November–1 December 2020; IEEE: New York, NY, USA, 2020; pp. 679–684. [Google Scholar]
- Yamada, T.; Kadone, H.; Shimizu, Y.; Suzuki, K. An Exoskeleton Brake Unit for Children with Crouch Gait Supporting the Knee Joint During Stance. In Proceedings of the 2018 International Symposium on Micro-NanoMechatronics and Human Science (MHS), Nagoya, Japan, 9–12 December 2018; IEEE: New York, NY, USA, 2018; pp. 1–7. [Google Scholar]
- Patane, F.; Rossi, S.; Del Sette, F.; Taborri, J.; Cappa, P. WAKE-Up Exoskeleton to Assist Children With Cerebral Palsy: Design and Preliminary Evaluation in Level Walking. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 906–916. [Google Scholar] [CrossRef]
- Rossi, S.; Patane, F.; Del Sette, F.; Cappa, P. WAKE-up: A Wearable Ankle Knee Exoskeleton. In Proceedings of the 5th IEEE RAS/EMBS International Conference on Biomedical Robotics and Biomechatronics, Sao Paulo, Brazil, 12–15 August 2014; IEEE: New York, NY, USA, 2014; pp. 504–507. [Google Scholar]
- Zhang, Y.; Bressel, M.; De Groof, S.; Domine, F.; Labey, L.; Peyrodie, L. Design and Control of a Size-Adjustable Pediatric Lower-Limb Exoskeleton Based on Weight Shift. IEEE Access 2023, 11, 6372–6384. [Google Scholar] [CrossRef]
- Villani, M.; Avaltroni, P.; Scordo, G.; Rubeca, D.; Kreynin, P.; Bereziy, E.; Berger, D.; Cappellini, G.; Sylos-Labini, F.; Lacquaniti, F.; et al. Evaluation of EMG Patterns in Children during Assisted Walking in the Exoskeleton. Front. Neurosci. 2024, 18, 1461323. [Google Scholar] [CrossRef] [PubMed]
- Laubscher, C.A.; Sawicki, J.T. Gait Guidance Control for Damping of Unnatural Motion in a Powered Pediatric Lower-Limb Orthosis. In Proceedings of the 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), Toronto, ON, Canada, 24–28 June 2019; IEEE: New York, NY, USA, 2019; pp. 676–681. [Google Scholar]
- Garcia, E.; Sancho, J.; Sanz-Merodio, D.; Prieto, M. ATLAS 2020: The Pediatric Gait Exoskeleton Project. In Proceedings of the CLAWAR 2017: 20th International Conference on Climbing and Walking Robots and the Support Technologies for Mobile Machines, Porto, Portugal, 11–13 September 2017; World Scientific: Singapore, 2017; pp. 29–38. [Google Scholar]
- Pour Aji Bishe, S.S.; Liebelt, L.; Fang, Y.; Lerner, Z.F. A Low-Profile Hip Exoskeleton for Pathological Gait Assistance: Design and Pilot Testing. In Proceedings of the 2022 International Conference on Robotics and Automation (ICRA), Philadelphia, PA, USA, 23–27 May 2022; IEEE: New York, NY, USA, 2022; pp. 5461–5466. [Google Scholar]
- Fang, Y.; Orekhov, G.; Lerner, Z.F. Improving the Energy Cost of Incline Walking and Stair Ascent With Ankle Exoskeleton Assistance in Cerebral Palsy. IEEE Trans. Biomed. Eng. 2022, 69, 2143–2152. [Google Scholar] [CrossRef]
- Bishe, S.S.P.A.; Nguyen, T.; Fang, Y.; Lerner, Z.F. Adaptive Ankle Exoskeleton Control: Validation Across Diverse Walking Conditions. IEEE Trans. Med. Robot. Bionics 2021, 3, 801–812. [Google Scholar] [CrossRef]
- Taketomi, T.; Sankai, Y. Stair Ascent Assistance for Cerebral Palsy with Robot Suit HAL. In Proceedings of the 2012 IEEE/SICE International Symposium on System Integration (SII), Fukuoka, Japan, 16–18 December 2012; IEEE: New York, NY, USA, 2012; pp. 331–336. [Google Scholar]
- Fang, Y.; Lerner, Z.F. Feasibility of Augmenting Ankle Exoskeleton Walking Performance With Step Length Biofeedback in Individuals with Cerebral Palsy. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 442–449. [Google Scholar] [CrossRef]
- Harshe, K.; Williams, J.R.; Hocking, T.D.; Lerner, Z.F. Predicting Neuromuscular Engagement to Improve Gait Training With a Robotic Ankle Exoskeleton. IEEE Robot. Autom. Lett. 2023, 8, 5055–5060. [Google Scholar] [CrossRef]
- Gasparri, G.M.; Luque, J.; Lerner, Z.F. Proportional Joint-Moment Control for Instantaneously Adaptive Ankle Exoskeleton Assistance. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 751–759. [Google Scholar] [CrossRef]
- Orekhov, G.; Fang, Y.; Cuddeback, C.F.; Lerner, Z.F. Usability and Performance Validation of an Ultra-Lightweight and Versatile Untethered Robotic Ankle Exoskeleton. J. NeuroEngineering Rehabil. 2021, 18, 163. [Google Scholar] [CrossRef]
- Orekhov, G.; Fang, Y.; Luque, J.; Lerner, Z.F. Ankle Exoskeleton Assistance Can Improve Over-Ground Walking Economy in Individuals with Cerebral Palsy. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 461–467. [Google Scholar] [CrossRef]
- Orekhov, G.; Luque, J.; Lerner, Z.F. Closing the Loop on Exoskeleton Motor Controllers: Benefits of Regression-Based Open-Loop Control. IEEE Robot. Autom. Lett. 2020, 5, 6025–6032. [Google Scholar] [CrossRef]
- Lerner, Z.F.; Gasparri, G.M.; Bair, M.O.; Lawson, J.L.; Luque, J.; Harvey, T.A.; Lerner, A.T. An Untethered Ankle Exoskeleton Improves Walking Economy in a Pilot Study of Individuals with Cerebral Palsy. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1985–1993. [Google Scholar] [CrossRef]
- Spomer, A.M.; Conner, B.C.; Schwartz, M.H.; Lerner, Z.F.; Steele, K.M. Audiovisual Biofeedback Amplifies Plantarflexor Adaptation during Walking among Children with Cerebral Palsy. J. NeuroEngineering Rehabil. 2023, 20, 164. [Google Scholar] [CrossRef]
- Lerner, Z.F.; Harvey, T.A.; Lawson, J.L. A Battery-Powered Ankle Exoskeleton Improves Gait Mechanics in a Feasibility Study of Individuals with Cerebral Palsy. Ann. Biomed. Eng. 2019, 47, 1345–1356. [Google Scholar] [CrossRef]
- Conner, B.C.; Luque, J.; Lerner, Z.F. Adaptive Ankle Resistance from a Wearable Robotic Device to Improve Muscle Recruitment in Cerebral Palsy. Ann. Biomed. Eng. 2020, 48, 1309–1321. [Google Scholar] [CrossRef]
- Conner, B.C.; Schwartz, M.H.; Lerner, Z.F. Pilot Evaluation of Changes in Motor Control after Wearable Robotic Resistance Training in Children with Cerebral Palsy. J. Biomech. 2021, 126, 110601. [Google Scholar] [CrossRef]
- Conner, B.C.; Lerner, Z.F. Improving Ankle Muscle Recruitment via Plantar Pressure Biofeedback during Robot Resisted Gait Training in Cerebral Palsy. In Proceedings of the 2022 International Conference on Rehabilitation Robotics (ICORR), Rotterdam, The Netherlands, 25 July 2022; IEEE: New York, NY, USA, 2022; pp. 1–6. [Google Scholar]
- Chen, J.; Hochstein, J.; Kim, C.; Damiano, D.; Bulea, T. Design Advancements Toward a Wearable Pediatric Robotic Knee Exoskeleton for Overground Gait Rehabilitation. In Proceedings of the 2018 7th IEEE International Conference on Biomedical Robotics and Biomechatronics (Biorob), Enschede, The Netherlands, 26–29 August 2018; IEEE: New York, NY, USA, 2018; pp. 37–42. [Google Scholar]
- Chen, J.; Hochstein, J.; Kim, C.; Tucker, L.; Hammel, L.E.; Damiano, D.L.; Bulea, T.C. A Pediatric Knee Exoskeleton with Real-Time Adaptive Control for Overground Walking in Ambulatory Individuals with Cerebral Palsy. Front. Robot. AI 2021, 8, 702137. [Google Scholar] [CrossRef]
- Zhang, S.; Zhu, J.; Huang, T.-H.; Yu, S.; Huang, J.S.; Lopez-Sanchez, I.; Devine, T.; Abdelhady, M.; Zheng, M.; Bulea, T.C.; et al. Actuator Optimization and Deep Learning-Based Control of Pediatric Knee Exoskeleton for Community-Based Mobility Assistance. Mechatronics 2024, 97, 103109. [Google Scholar] [CrossRef]
- Chen, J.; Damiano, D.L.; Lerner, Z.F.; Bulea, T.C. Validating Model-Based Prediction of Biological Knee Moment During Walking with an Exoskeleton in Crouch Gait: Potential Application for Exoskeleton Control. In Proceedings of the 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), Toronto, ON, Canada, 24–28 June 2019; IEEE: New York, NY, USA, 2019; pp. 778–783. [Google Scholar]
- Lerner, Z.F.; Damiano, D.L.; Park, H.-S.; Gravunder, A.J.; Bulea, T.C. A Robotic Exoskeleton for Treatment of Crouch Gait in Children with Cerebral Palsy: Design and Initial Application. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 650–659. [Google Scholar] [CrossRef]
- Lerner, Z.F.; Damiano, D.L.; Bulea, T.C. A Robotic Exoskeleton to Treat Crouch Gait from Cerebral Palsy: Initial Kinematic and Neuromuscular Evaluation. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; IEEE: New York, NY, USA, 2016; pp. 2214–2217. [Google Scholar]
- Lerner, Z.F.; Damiano, D.L.; Bulea, T.C. A Lower-Extremity Exoskeleton Improves Knee Extension in Children with Crouch Gait from Cerebral Palsy. Sci. Transl. Med. 2017, 9, eaam9145. [Google Scholar] [CrossRef]
- Lerner, Z.F.; Damiano, D.L.; Bulea, T.C. The Effects of Exoskeleton Assisted Knee Extension on Lower-Extremity Gait Kinematics, Kinetics, and Muscle Activity in Children with Cerebral Palsy. Sci. Rep. 2017, 7, 13512. [Google Scholar] [CrossRef]
- Mansilla Navarro, P.; Copaci, D.; Arias, J.; Blanco Rojas, D. Design of an SMA-Based Actuator for Replicating Normal Gait Patterns in Pediatric Patients with Cerebral Palsy. Biomimetics 2024, 9, 376. [Google Scholar] [CrossRef] [PubMed]
- Mansilla Navarro, P.; Copaci, D.; Blanco Rojas, D. Design and Control of a Soft Knee Exoskeleton for Pediatric Patients at Early Stages of the Walking Learning Process. Bioengineering 2024, 11, 188. [Google Scholar] [CrossRef] [PubMed]
- Sarajchi, M.; Sirlantzis, K. Pediatric Robotic Lower-Limb Exoskeleton: An Innovative Design and Kinematic Analysis. IEEE Access 2023, 11, 115219–115230. [Google Scholar] [CrossRef]
- De Groof, S.; Zhang, Y.; Peyrodie, L.; Labey, L. Design and Control of an Individualized Hip Exoskeleton Capable of Gait Phase Synchronized Flexion and Extension Torque Assistance. IEEE Access 2023, 11, 96206–96220. [Google Scholar] [CrossRef]
- Andrade, R.M.; Sapienza, S.; Fabara, E.E.; Bonato, P. Trajectory Tracking Impedance Controller in 6-DoF Lower-Limb Exoskeleton for Over-Ground Walking Training: Preliminary Results. In Proceedings of the 2021 International Symposium on Medical Robotics (ISMR), Atlanta, GA, USA, 17–19 November 2021; IEEE: New York, NY, USA, 2021; pp. 1–6. [Google Scholar]
- Andrade, R.M.; Sapienza, S.; Mohebbi, A.; Fabara, E.E.; Bonato, P. Experimental Evaluation of a Transparent Operation Mode for a Lower-Limb Exoskeleton Designed for Children with Cerebral Palsy. In Proceedings of the 2023 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Detroit, MI, USA, 1–5 October 2023; IEEE: New York, NY, USA, 2023; pp. 6062–6067. [Google Scholar]
- Andrade, R.M.; Sapienza, S.; Bonato, P. Development of a “Transparent Operation Mode” for a Lower-Limb Exoskeleton Designed for Children with Cerebral Palsy. In Proceedings of the 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), Toronto, ON, Canada, 24–28 June 2019; IEEE: New York, NY, USA, 2019; pp. 512–517. [Google Scholar]
- Narayan, J.; Abbas, M.; Patel, B.; Dwivedy, S.K. A Singularity-Free Terminal Sliding Mode Control of an Uncertain Paediatric Exoskeleton System. In Proceedings of the 2022 5th International Conference on Advanced Systems and Emergent Technologies (IC_ASET), Hammamet, Tunisia, 22–25 March 2022; IEEE: New York, NY, USA, 2022; pp. 198–203. [Google Scholar]
- Narayan, J.; Abbas, M.; Dwivedy, S.K. Design and Validation of a Pediatric Gait Assistance Exoskeleton System with Fast Non-Singular Terminal Sliding Mode Controller. Med. Eng. Phys. 2024, 123, 104080. [Google Scholar] [CrossRef]
- Narayan, J.; Abbas, M.; Dwivedy, S.K. Robust Non-Singular Fast Terminal Sliding Mode Gait Tracking Control of a Pediatric Exoskeleton. In Proceedings of the 2023 5th International Conference on Bioengineering for Smart Technologies (BioSMART), Paris, France, 7–9 June 2023; IEEE: New York, NY, USA, 2023; pp. 1–4. [Google Scholar]
- Narayan, J.; Gritli, H.; Dwivedy, S.K. Fast Terminal Sliding Mode Control with Rapid Reaching Law for a Pediatric Gait Exoskeleton System. Int. J. Intell. Robot. Appl. 2024, 8, 76–95. [Google Scholar] [CrossRef]
- Narayan, J.; Dwivedy, S.K. Robust Gait Tracking Control of a Pediatric Exoskeleton System: An Adaptive Non-Singular Fast Terminal Sliding Mode Approach. In Proceedings of the 2023 9th International Conference on Control, Decision and Information Technologies (CoDIT), Rome, Italy, 3–6 July 2023; IEEE: New York, NY, USA, 2023; pp. 2337–2341. [Google Scholar]
- Narayan, J.; Abbas, M.; Dwivedy, S.K. Robust Adaptive Backstepping Control for a Lower-Limb Exoskeleton System with Model Uncertainties and External Disturbances. Automatika 2023, 64, 145–161. [Google Scholar] [CrossRef]
- Narayan, J.; Patel, B.M.; Abbas, M.; Shivhare, G.; Dwivedy, S.K. Cooperative Control of a Pediatric Exoskeleton System for Active-Assist Gait Rehabilitation. In Proceedings of the 2022 IEEE International Conference on Electronics, Computing and Communication Technologies (CONECCT), Bangalore, India, 8–10 July 2022; IEEE: New York, NY, USA, 2022; pp. 1–6. [Google Scholar]
- Narayan, J.; Dwivedy, S.K. Towards Neuro-Fuzzy Compensated PID Control of Lower Extremity Exoskeleton System for Passive Gait Rehabilitation. IETE J. Res. 2023, 69, 778–795. [Google Scholar] [CrossRef]
- Narayan, J.; Abbas, M.; Patel, B.; Dwivedy, S.K. Adaptive RBF Neural Network-Computed Torque Control for a Pediatric Gait Exoskeleton System: An Experimental Study. Intell. Serv. Robot. 2023, 16, 549–564. [Google Scholar] [CrossRef]
- Laubscher, C.A.; Farris, R.J.; Van Den Bogert, A.J.; Sawicki, J.T. An Anthropometrically Parameterized Assistive Lower Limb Exoskeleton. J. Biomech. Eng. 2021, 143, 105001. [Google Scholar] [CrossRef]
- Laubscher, C.A.; Farris, R.J.; Sawicki, J.T. Angular Momentum-Based Control of an Underactuated Orthotic System for Crouch-to-Stand Motion. Auton. Robots 2020, 44, 1469–1484. [Google Scholar] [CrossRef]
- Goo, A.C.; Laubscher, C.A.; Wajda, D.A.; Sawicki, J.T. Preliminary Virtual Constraint-Based Control Evaluation on a Pediatric Lower-Limb Exoskeleton. Bioengineering 2024, 11, 590. [Google Scholar] [CrossRef] [PubMed]
- Goo, A.; Laubscher, C.A.; Wiebrecht, J.J.; Farris, R.J.; Sawicki, J.T. Hybrid Zero Dynamics Control for Gait Guidance of a Novel Adjustable Pediatric Lower-Limb Exoskeleton. Bioengineering 2022, 9, 208. [Google Scholar] [CrossRef]
- Everaert, L.; Sevit, R.; Dewit, T.; Janssens, K.; Vanloocke, J.; Van Campenhout, A.; Labey, L.; Muraru, L.; Desloovere, K. Evaluation of the Working Mechanism of a Newly Developed Powered Ankle–Foot Orthosis. Sensors 2024, 24, 6562. [Google Scholar] [CrossRef]
- Mohammadi, V.; Tajdani, M.; Masaei, M.; Mohammadi Ghalehney, S.; Lee, S.C.K.; Behboodi, A. DE-AFO: A Robotic Ankle Foot Orthosis for Children with Cerebral Palsy Powered by Dielectric Elastomer Artificial Muscle. Sensors 2024, 24, 3787. [Google Scholar] [CrossRef]
- Gonzalez-Vazquez, A.; Garcia, L.; Kilby, J. Paediatric Ankle Rehabilitation System Based on Twisted and Coiled Polymer Actuators. Smart Mater. Struct. 2024, 33, 075009. [Google Scholar] [CrossRef]
- Eguren, D.; Cestari, M.; Luu, T.P.; Kilicarslan, A.; Steele, A.; Contreras-Vidal, J.L. Design of a Customizable, Modular Pediatric Exoskeleton for Rehabilitation and Mobility. In Proceedings of the 2019 IEEE International Conference on Systems, Man and Cybernetics (SMC), Bari, Italy, 6–9 October 2019; IEEE: New York, NY, USA, 2019; pp. 2411–2416. [Google Scholar]
- Bayon, C.; Ramirez, O.; Del Castillo, M.D.; Serrano, J.I.; Raya, R.; Belda-Lois, J.M.; Poveda, R.; Molla, F.; Martin, T.; Martinez, I.; et al. CPWalker: Robotic Platform for Gait Rehabilitation in Patients with Cerebral Palsy. In Proceedings of the 2016 IEEE International Conference on Robotics and Automation (ICRA), Stockholm, Sweden, 16–21 May 2016; IEEE: New York, NY, USA, 2016; pp. 3736–3741. [Google Scholar]
- Bayón, C.; Martín-Lorenzo, T.; Moral-Saiz, B.; Ramírez, Ó.; Pérez-Somarriba, Á.; Lerma-Lara, S.; Martínez, I.; Rocon, E. A Robot-Based Gait Training Therapy for Pediatric Population with Cerebral Palsy: Goal Setting, Proposal and Preliminary Clinical Implementation. J. NeuroEngineering Rehabil. 2018, 15, 69. [Google Scholar] [CrossRef]
- Bayon, C.; Ramirez, O.; Velasco, M.; Serrano, J.I.; Lerma Lara, S.; Martinez-Caballero, I.; Rocon, E. IEEE Pilot Study of a Novel Robotic Platform for Gait Rehabilitation in Children with Cerebral Palsy; IEEE: New York, NY, USA, 2016; pp. 882–887. [Google Scholar]
- Cifuentes, C.A.; Bayon, C.; Lerma, S.; Frizera, A.; Rocon, E. IEEE Human-Robot Interaction Strategy for Overground Rehabilitation in Patients with Cerebral Palsy; IEEE: New York, NY, USA, 2016; pp. 729–734. [Google Scholar]
- Mohd Adib, M.A.H.; Han, S.Y.; Ramani, P.R.; You, L.J.; Yan, L.M.; Mat Sahat, I.; Mohd Hasni, N.H. Restoration of Kids Leg Function Using Exoskeleton Robotic Leg (ExRoLEG) Device. In Proceedings of the 10th National Technical Seminar on Underwater System Technology 2018, Singapore, 26–27 September 2018; Md Zain, Z., Ahmad, H., Pebrianti, D., Mustafa, M., Abdullah, N.R.H., Samad, R., Mat Noh, M., Eds.; Lecture Notes in Electrical Engineering. Springer: Singapore, 2019; Volume 538, pp. 335–342, ISBN 978-981-13-3707-9. [Google Scholar]
- Sanz-Merodio, D.; Cestari, M.; Carlos Arevalo, J.; Garcia, E. IEEE A Lower-Limb Exoskeleton for Gait Assistance in Quadriplegia; IEEE: New York, NY, USA, 2012. [Google Scholar]
- Tokhi, M.O.; Virk, G.S. Advances in Cooperative Robotics. In Proceedings of the 19th International Conference on CLAWAR, London, UK, 12–14 September 2016; World Scientific: Singapore, 2016. ISBN 978-981-314-912-0. [Google Scholar]
- Cestari, M.; Sanz-Merodio, D.; Arevalo, J.C.; Garcia, E. ARES, a Variable Stiffness Actuator with Embedded Force Sensor for the ATLAS Exoskeleton. Ind. Robot Int. J. 2014, 41, 518–526. [Google Scholar] [CrossRef]
- Sanz-Merodio, D.; Cestari, M.; Arevalo, J.C.; Carrillo, X.A.; Garcia, E. Generation and Control of Adaptive Gaits in Lower-Limb Exoskeletons for Motion Assistance. Adv. Robot. 2014, 28, 329–338. [Google Scholar] [CrossRef]
- Garcia, E.; Cestari, M.; Sanz-Merodio, D. Wearable Exoskeletons for the Physical Treatment of Children with Quadriparesis. In Proceedings of the 2014 IEEE-RAS International Conference on Humanoid Robots, Madrid, Spain, 18–20 November 2014; IEEE: New York, NY, USA, 2015; pp. 425–430. [Google Scholar]
- Kawamoto, H.; Sankai, Y. Power Assist System HAL-3 for Gait Disorder Person. In Computers Helping People with Special Needs; Miesenberger, K., Klaus, J., Zagler, W., Eds.; Lecture Notes in Computer Science; Springer: Berlin/Heidelberg, Germany, 2002; Volume 2398, pp. 196–203. ISBN 978-3-540-43904-2. [Google Scholar]
- Matsuda, M.; Mataki, Y.; Mutsuzaki, H.; Yoshikawa, K.; Takahashi, K.; Enomoto, K.; Sano, K.; Mizukami, M.; Tomita, K.; Ohguro, H.; et al. Immediate Effects of a Single Session of Robot-Assisted Gait Training Using Hybrid Assistive Limb (HAL) for Cerebral Palsy. J. Phys. Ther. Sci. 2018, 30, 207–212. [Google Scholar] [CrossRef]
- Matsuda, M.; Iwasaki, N.; Mataki, Y.; Mutsuzaki, H.; Yoshikawa, K.; Takahashi, K.; Enomoto, K.; Sano, K.; Kubota, A.; Nakayama, T.; et al. Robot-Assisted Training Using Hybrid Assistive Limb® for Cerebral Palsy. BRAIN Dev. 2018, 40, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Mataki, Y.; Kamada, H.; Mutsuzaki, H.; Shimizu, Y.; Takeuchi, R.; Mizukami, M.; Yoshikawa, K.; Takahashi, K.; Matsuda, M.; Iwasaki, N.; et al. Use of Hybrid Assistive Limb (HAL) for a Postoperative Patient with Cerebral Palsy: A Case Report. BMC Res. Notes 2018, 11, 201. [Google Scholar] [CrossRef]
- Pérez-San Lázaro, R.; Salgado, I.; Chairez, I. Adaptive Sliding-Mode Controller of a Lower Limb Mobile Exoskeleton for Active Rehabilitation. ISA Trans. 2021, 109, 218–228. [Google Scholar] [CrossRef]
- Zaway, I.; Jallouli-Khlif, R.; Maalej, B.; Medhaffar, H.; Derbel, N. From PD to Fractional Order PD Controller Used for Gait Rehabilitation. In Proceedings of the 2021 18th International Multi-Conference on Systems, Signals & Devices (SSD), Monastir, Tunisia, 22–25 March 2021; IEEE: New York, NY, USA, 2021; pp. 948–953. [Google Scholar]
- Kim, S.K.; Park, D.; Yoo, B.; Shim, D.; Choi, J.-O.; Choi, T.Y.; Park, E.S. Overground Robot-Assisted Gait Training for Pediatric Cerebral Palsy. Sensors 2021, 21, 2087. [Google Scholar] [CrossRef]
- Kawasaki, S.; Ohata, K.; Yoshida, T.; Yokoyama, A.; Yamada, S. Gait Improvements by Assisting Hip Movements with the Robot in Children with Cerebral Palsy: A Pilot Randomized Controlled Trial. J. NeuroEngineering Rehabil. 2020, 17, 87. [Google Scholar] [CrossRef]
- Delgado-Oleas, G.; Romero-Sorozabal, P.; Lora-Millan, J.; Gutierrez, A.; Rocon, E. Bioinspired Hierarchical Electronic Architecture for Robotic Locomotion Assistance: Application in Exoskeletons. IEEE Access 2023, 11, 131610–131622. [Google Scholar] [CrossRef]
- Varela, I.D.; Romero-Sorozabal, P.; Delgado-Oleas, G.; Gutiérrez, Á.; Muñoz, J.; Rocon, E. A Cable-Driven Exoskeleton to Control Ankle Mobility During Gait in Children with Cerebral Palsy. In Proceedings of the 2024 7th Iberian Robotics Conference (ROBOT), Madrid, Spain, 6–8 November 2024; IEEE: New York, NY, USA, 2024; pp. 1–6. [Google Scholar]
- Maalej, B.; Jribi, R.; Ayadi, N.; Abdelhedi, F.; Derbel, N. On a Robotic Application for Rehabilitation Systems Dedicated to Kids Affected by Cerebral Palsy. In Proceedings of the 2018 15th International Multi-Conference on Systems, Signals & Devices (SSD), Yasmine Hammamet, Tunisia, 19–22 March 2018; IEEE: New York, NY, USA; pp. 414–419. [Google Scholar]
- Patritti, B.; Sicari, M.; Deming, L.; Romaguera, F.; Pelliccio, M.; Benedetti, M.G.; Nimec, D.; Bonato, P. Enhancing robotic gait training via augmented feedback. In Proceedings of the 32nd Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC 2010), Buenos Aires, Argentina, 31 August–4 September 2010; IEEE: New York, NY, USA; pp. 2271–2274. [Google Scholar]
- Kirtas, O.; Savas, Y.; Bayraker, M.; Baskaya, F.; Basturk, H.; Samur, E. Design, Implementation, and Evaluation of a Backstepping Control Algorithm for an Active Ankle–Foot Orthosis. Control Eng. Pract. 2021, 106, 104667. [Google Scholar] [CrossRef]
- Wu, Y.-N.; Hwang, M.; Ren, Y.; Gaebler-Spira, D.; Zhang, L.-Q. Combined Passive Stretching and Active Movement Rehabilitation of Lower-Limb Impairments in Children with Cerebral Palsy Using a Portable Robot. Neurorehabil. Neural Repair 2011, 25, 378–385. [Google Scholar] [CrossRef]
- Eguren, D.; Luu, T.P.; Kilicarslan, A.; Akinwande, S.; Zanovello, M.; Arunkumar, A.; Gorges, J.; Contreras-Vidal, J.L. Development of a Pediatric Lower-Extremity Gait System. In Proceedings of the 2017 International Symposium on Wearable Robotics and Rehabilitation (WeRob), Houston, TX, USA, 5–8 November 2017; IEEE: New York, NY, USA, 2017; p. 1. [Google Scholar]
- Park, E.J.; Kang, J.; Su, H.; Stegall, P.; Miranda, D.L.; Hsu, W.-H.; Karabas, M.; Phipps, N.; Agrawal, S.K.; Goldfield, E.C.; et al. Design and Preliminary Evaluation of a Multi-Robotic System with Pelvic and Hip Assistance for Pediatric Gait Rehabilitation; Amirabdollahian, F., Burdet, E., Masia, L., Eds.; IEEE: New York, NY, USA, 2017; pp. 332–339. [Google Scholar]
- Tong, S.F.; Liang, D.; Su, Y.; Liu, M.; Kai-yu Tong, R. A Soft Pneumatic Hip-Assistive Robot for Reducing Scissor Gait on a Five-Year Old Child with Cerebral Palsy. In Proceedings of the 2024 17th International Convention on Rehabilitation Engineering and Assistive Technology (i-CREATe), Shanghai, China, 23–26 August 2024; IEEE: New York, NY, USA, 2024; pp. 1–6. [Google Scholar]
- Alcivar-Molina, E.; Hurel, J.; Teran, E.; Zamora-Olea, G.; Ponguillo, R.; Loayza, F.R. Six-Axis Lower-Limb Exoskeleton Control System Based on Neural Networks. In Proceedings of the 2018 IEEE Third Ecuador Technical Chapters Meeting (ETCM), Cuenca, Ecuador, 15–19 October 2018; IEEE: New York, NY, USA, 2018; pp. 1–5. [Google Scholar]
- Durfee, W.; Hashemi, S.; Ries, A. Hydraulic Ankle Foot Orthosis Emulator for Children with Cerebral Palsy. In Proceedings of the BATH/ASME 2020 Symposium on Fluid Power and Motion Control; American Society of Mechanical Engineers, Virtual, Online, 9 September 2020; ASME: New York, NY, USA; p. V001T01A044. [Google Scholar]
- Ding, Y.; Wang, Z.; Yang, P.; Yu, S. Design and Experiment of a Compact Intelligent Mobile Rehabilitation Exoskeleton Robot for Children with Cerebral Palsy Aged 3 to 6 Years. In Proceedings of the 2024 17th International Convention on Rehabilitation Engineering and Assistive Technology (i-CREATe), Shanghai, China, 23–26 August 2024; IEEE: New York, NY, USA, 2024; pp. 1–6. [Google Scholar]
- Maalej, B.; Chemori, A.; Derbel, N. Towards an Effective Robotic Device for Gait Rehabilitation of Children with Cerebral Palsy. In Proceedings of the 2019 International Conference on Signal, Control and Communication (SCC), Hammamet, Tunisia, 16–18 December 2019; IEEE: New York, NY, USA, 2019; pp. 268–273. [Google Scholar]
- Maalej, B.; Medhaffar, H.; Chemori, A.; Derbel, N. A Fuzzy Sliding Mode Controller for Reducing Torques Applied to a Rehabilitation Robot. In Proceedings of the 2020 17th International Multi-Conference on Systems, Signals & Devices (SSD), Monastir, Tunisia, 20 July 2020; IEEE: New York, NY, USA; pp. 740–746. [Google Scholar]
- Narayan, J.; Bharti, R.R.; Dwivedy, S.K. Robust Sliding Mode Control with Reaching Laws for a Pediatric Lower-Limb Exoskeleton System. In Proceedings of the 2022 Second International Conference on Power, Control and Computing Technologies (ICPC2T), Raipur, India, 1–3 March 2022; p. 6. [Google Scholar]
- Wallard, L.; Dietrich, G.; Kerlirzin, Y.; Bredin, J. Robotic-Assisted Gait Training Improves Walking Abilities in Diplegic Children with Cerebral Palsy. Eur. J. Paediatr. Neurol. 2017, 21, 557–564. [Google Scholar] [CrossRef]
- Lora-Millan, J.S.; Sanchez-Cuesta, F.J.; Romero, J.P.; Moreno, J.C.; Rocon, E. A Unilateral Robotic Knee Exoskeleton to Assess the Role of Natural Gait Assistance in Hemiparetic Patients. J. NeuroEngineering Rehabil. 2022, 19, 109. [Google Scholar] [CrossRef]
- Qian, Y.; Wang, Y.; Geng, H.; Du, H.; Xiong, J.; Leng, Y.; Fu, C. Adaptive Oscillator-Based Gait Feature Extraction Method of Hip Exoskeleton for Stroke Patients. IEEE Trans. Med. Robot. Bionics 2024, 6, 235–244. [Google Scholar] [CrossRef]
- Diot, C.M.; Thomas, R.L.; Raess, L.; Wrightson, J.G.; Condliffe, E.G. Robotic Lower Extremity Exoskeleton Use in a Non-Ambulatory Child with Cerebral Palsy: A Case Study. Disabil. Rehabil. Assist. Technol. 2023, 18, 497–501. [Google Scholar] [CrossRef]
- Bradley, S.S.; De Holanda, L.J.; Chau, T.; Wright, F.V. Physiotherapy-Assisted Overground Exoskeleton Use: Mixed Methods Feasibility Study Protocol Quantifying the User Experience, as Well as Functional, Neural, and Muscular Outcomes in Children with Mobility Impairments. Front. Neurosci. 2024, 18, 1398459. [Google Scholar] [CrossRef]
- Kolakowsky-Hayner, S.A.; Jones, K.; Kleckner, A.; Kuchinski, K.; Metzger, A.; Schueck-Plominski, J. Preliminary Assessment of a Robotic System for Overground Gait in Children with Cerebral Palsy. J. Enabling Technol. 2024, 18, 276–287. [Google Scholar] [CrossRef]
- Castro, P.; Martí, M.; Oliván-Blázquez, B.; Boñar, N.; García, V.; Gascón-Santos, S.; Panzano, A.; Vela, S.; Tajadura, S.; Peña, A.; et al. Benefits of Robotic Gait Assistance with ATLAS 2030 in Children with Cerebral Palsy. Front. Pediatr. 2024, 12, 1398044. [Google Scholar] [CrossRef]
- Cumplido-Trasmonte, C.; Ramos-Rojas, J.; Delgado-Castillejo, E.; Garcés-Castellote, E.; Puyuelo-Quintana, G.; Destarac-Eguizabal, M.A.; Barquín-Santos, E.; Plaza-Flores, A.; Hernández-Melero, M.; Gutiérrez-Ayala, A.; et al. Effects of ATLAS 2030 Gait Exoskeleton on Strength and Range of Motion in Children with Spinal Muscular Atrophy II: A Case Series. J. NeuroEngineering Rehabil. 2022, 19, 75. [Google Scholar] [CrossRef]
- Delgado, E.; Cumplido, C.; Ramos, J.; Garcés, E.; Puyuelo, G.; Plaza, A.; Hernández, M.; Gutiérrez, A.; Taverner, T.; Destarac, M.A.; et al. ATLAS2030 Pediatric Gait Exoskeleton: Changes on Range of Motion, Strength and Spasticity in Children with Cerebral Palsy. A Case Series Study. Front. Pediatr. 2021, 9, 753226. [Google Scholar] [CrossRef]
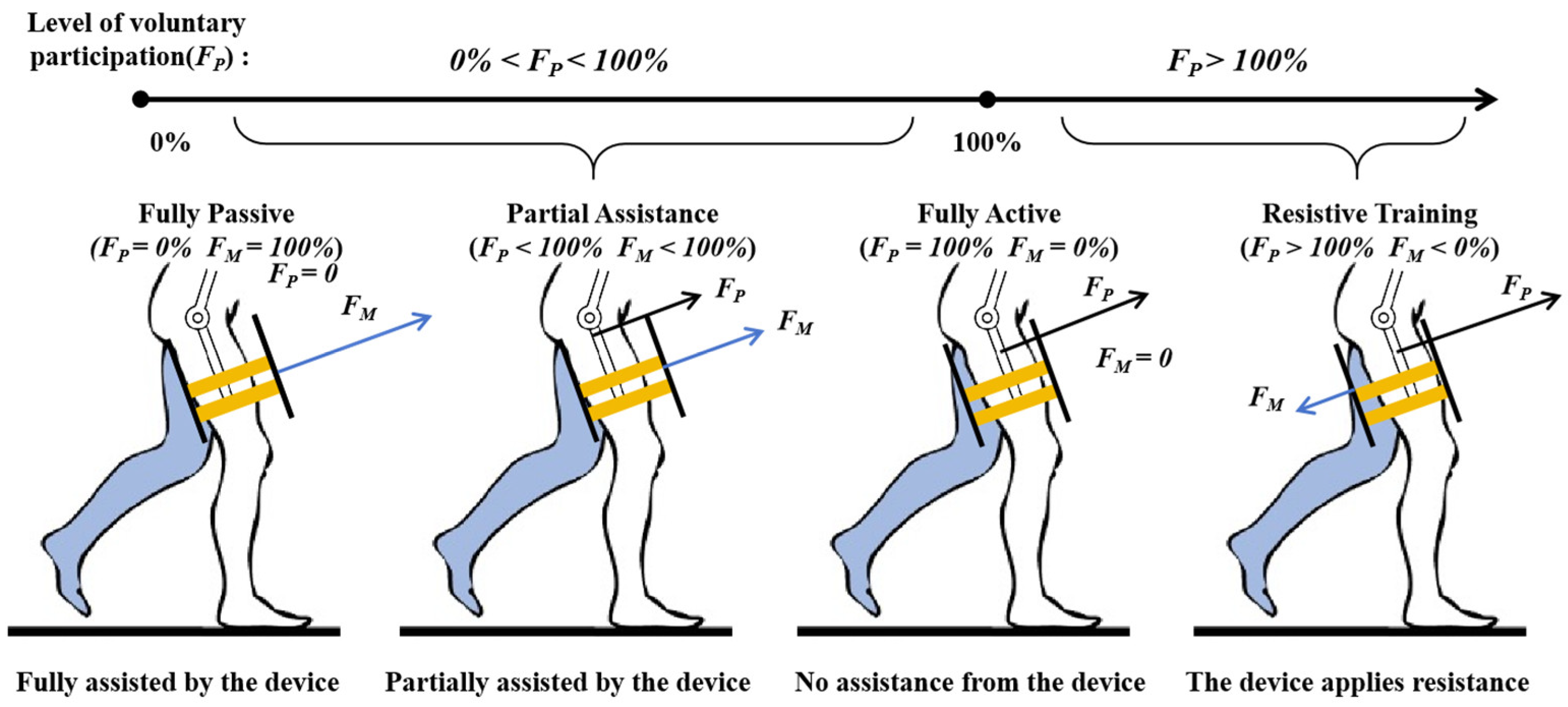
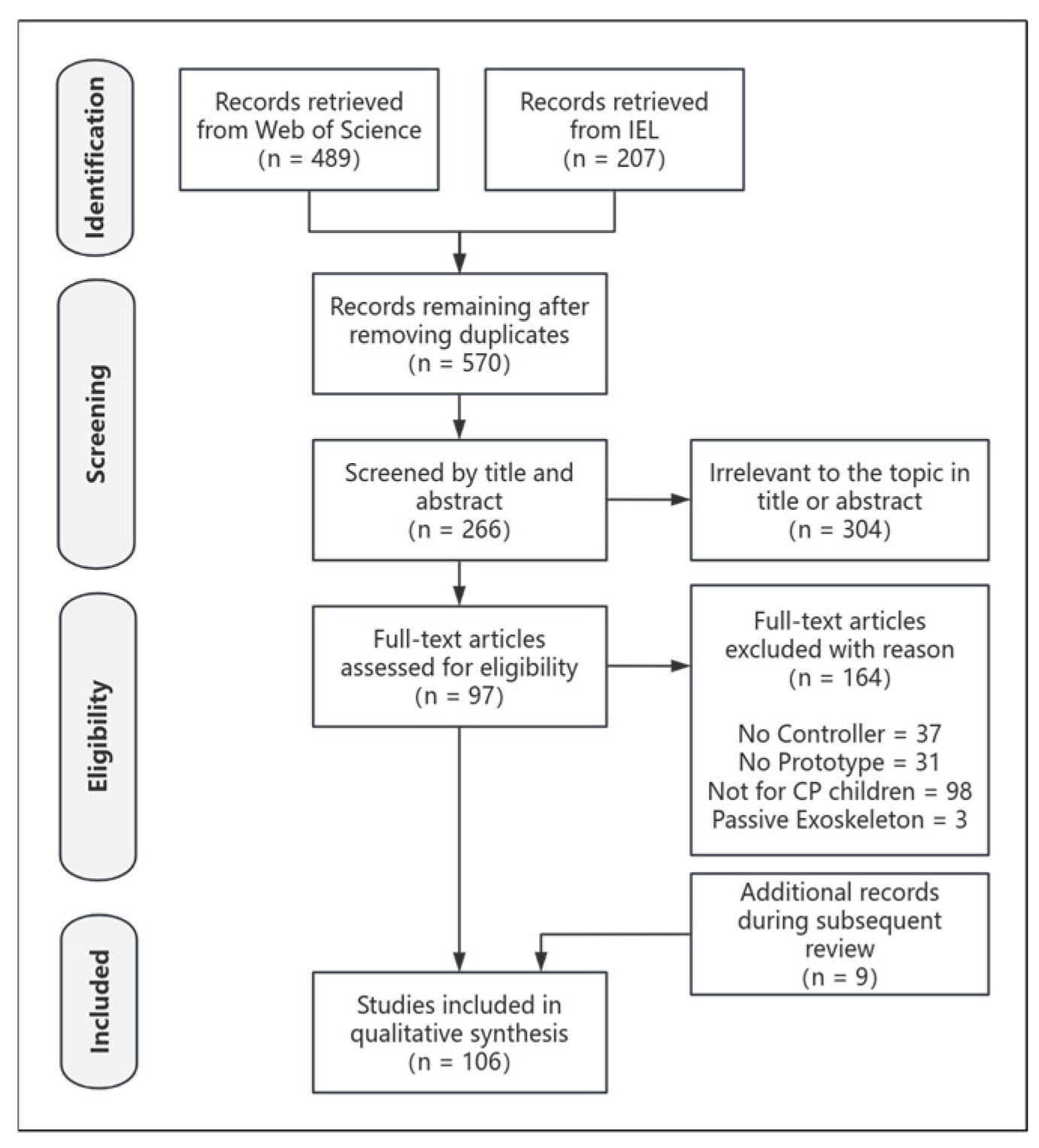
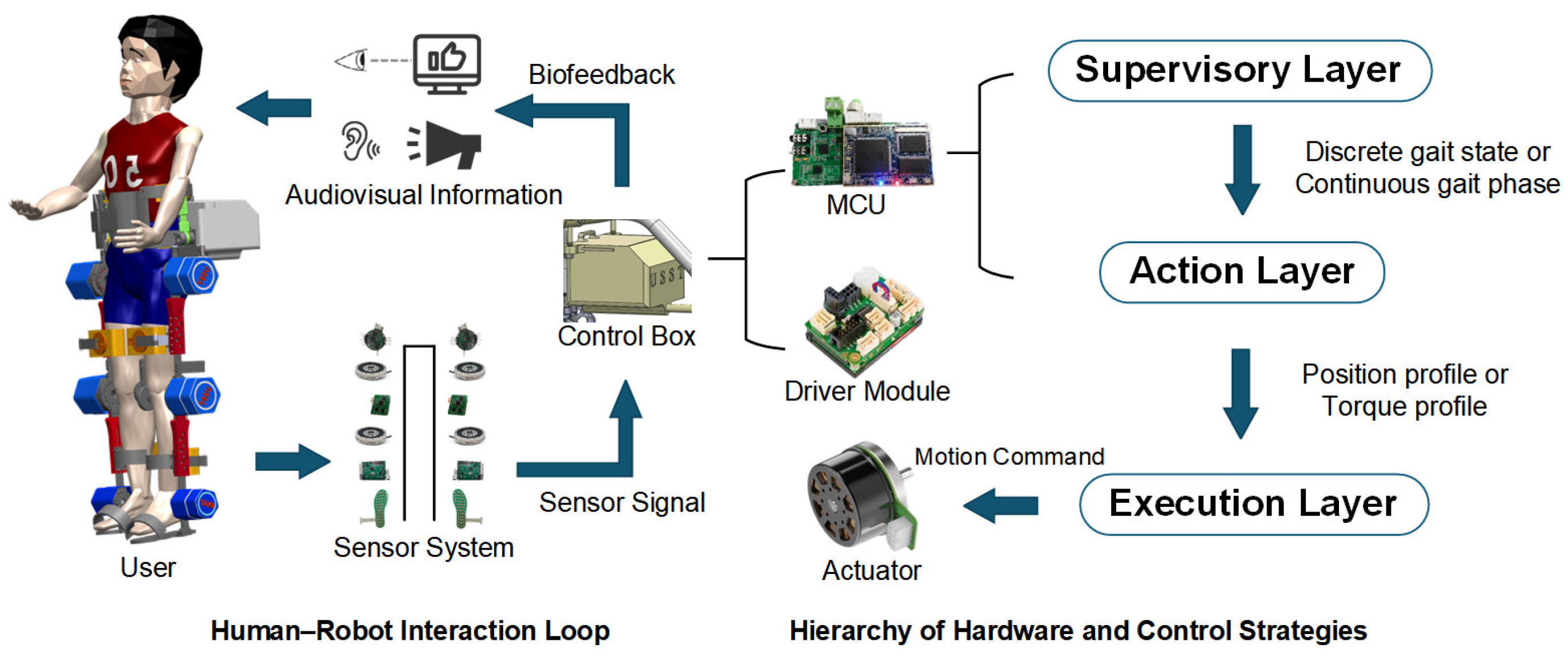
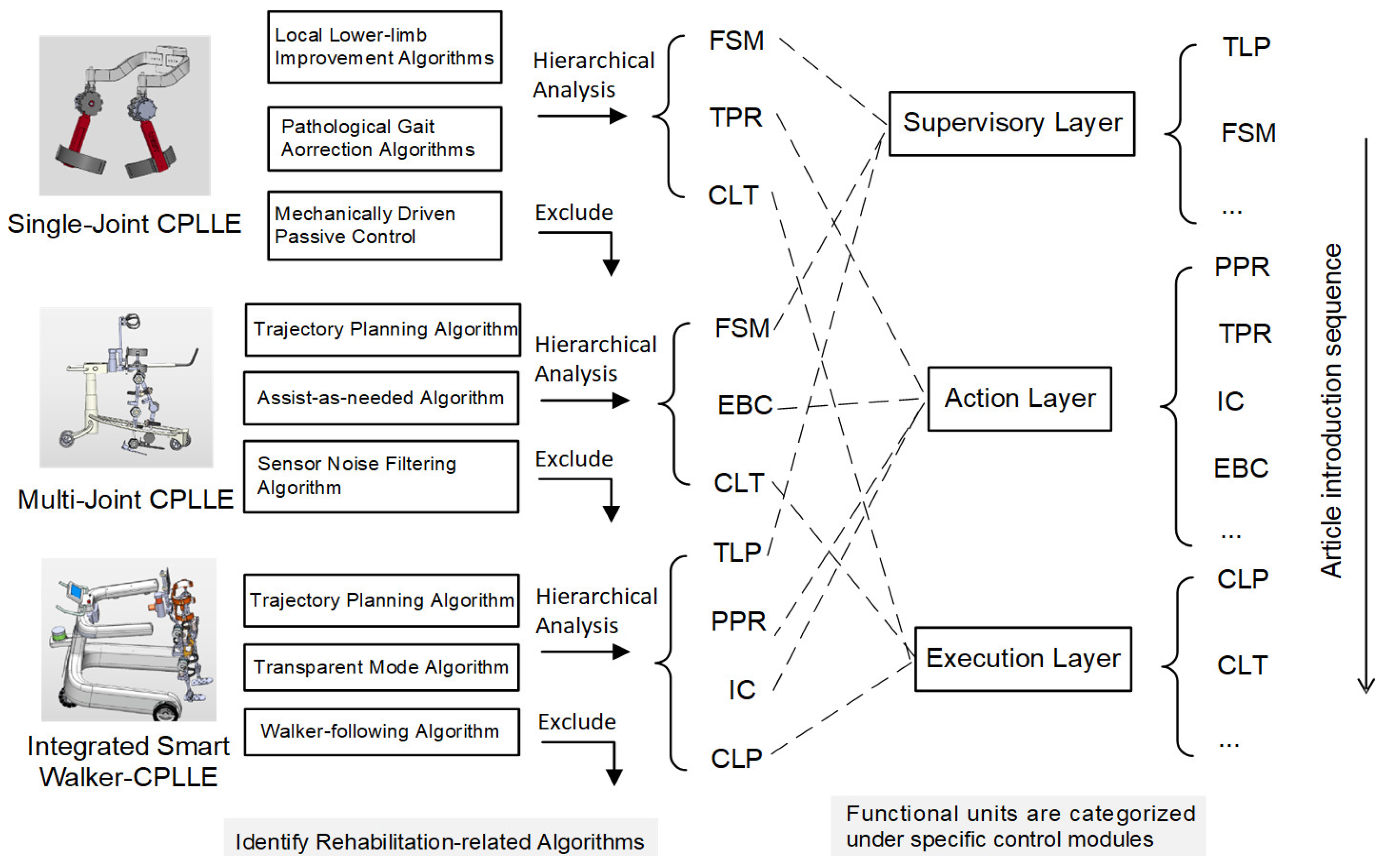
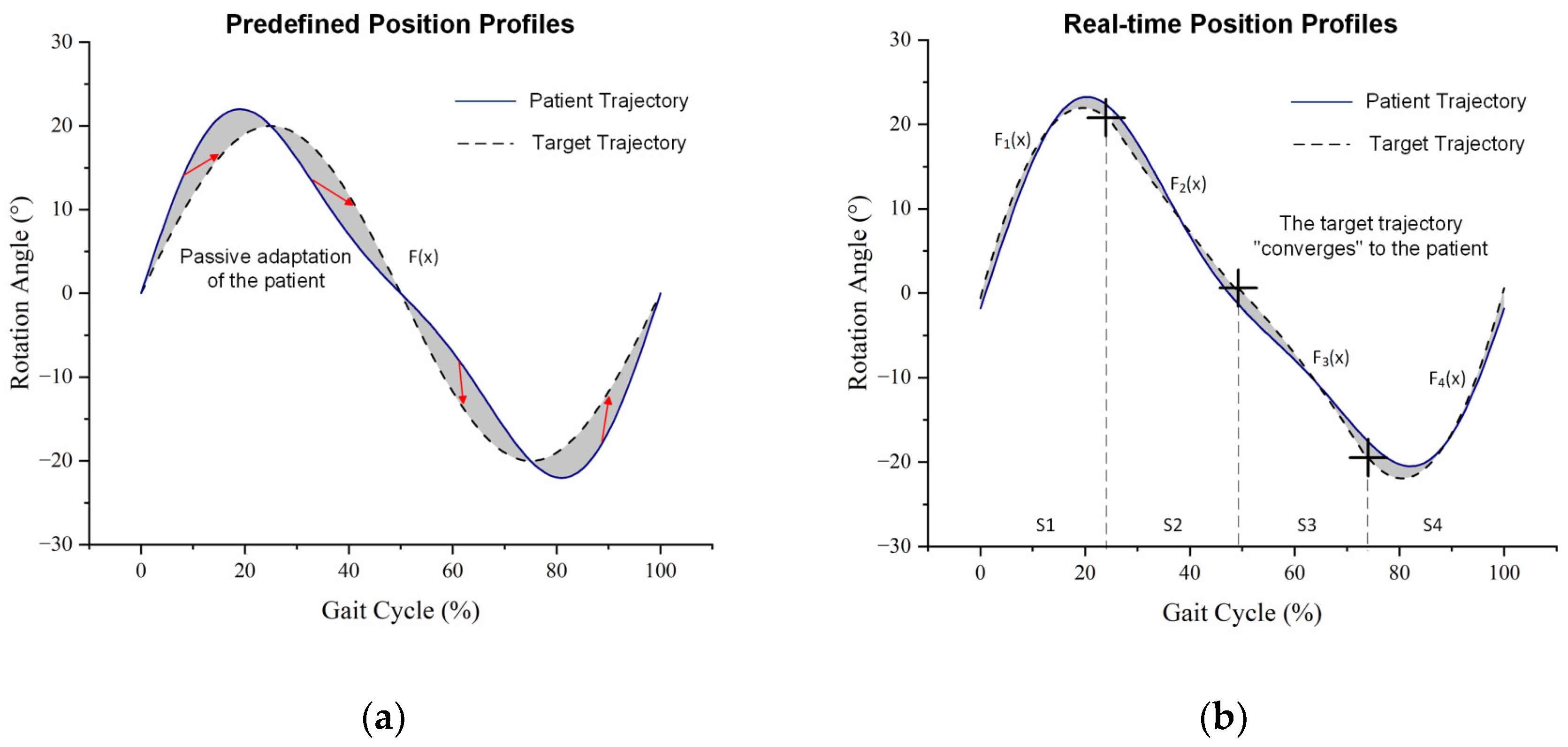
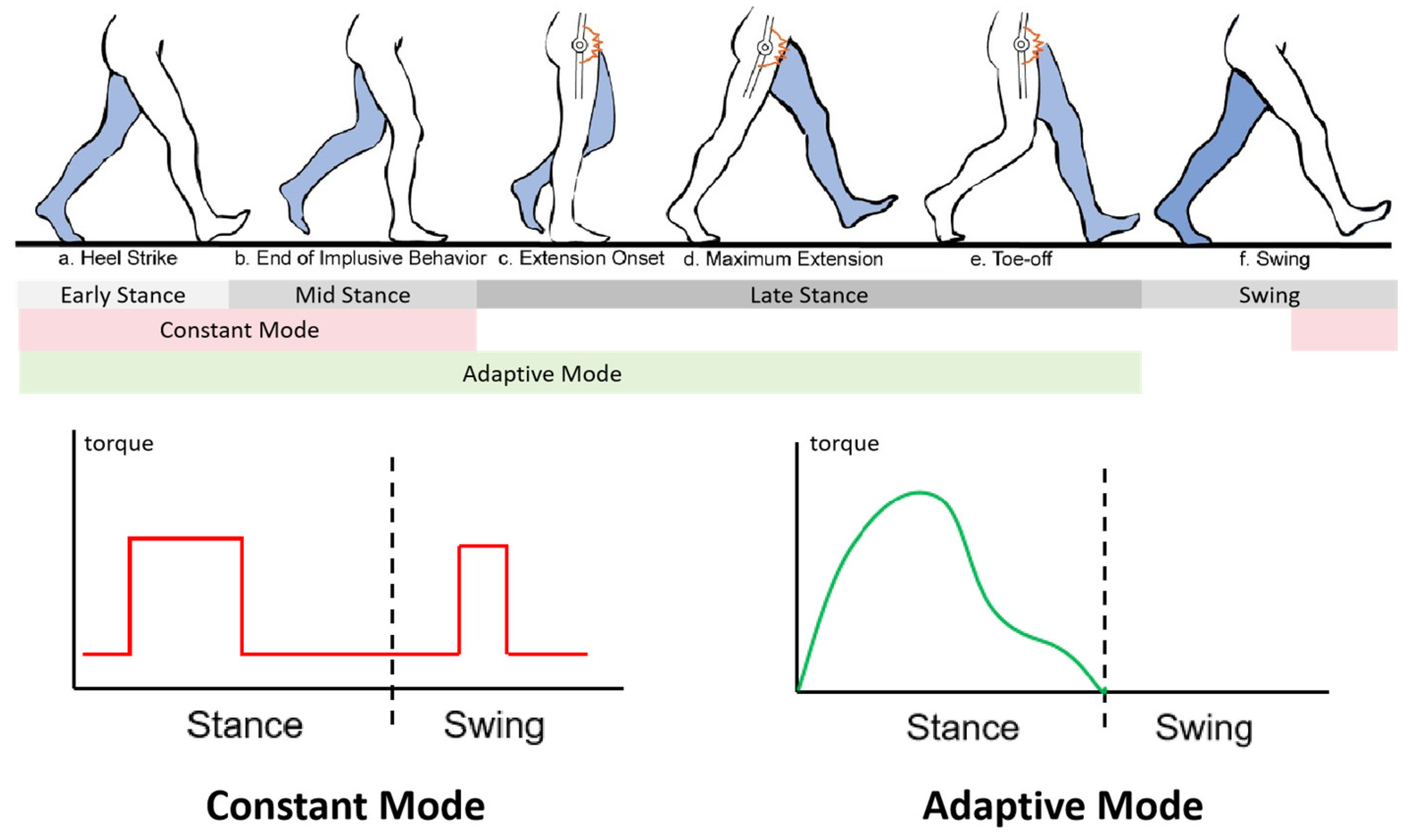
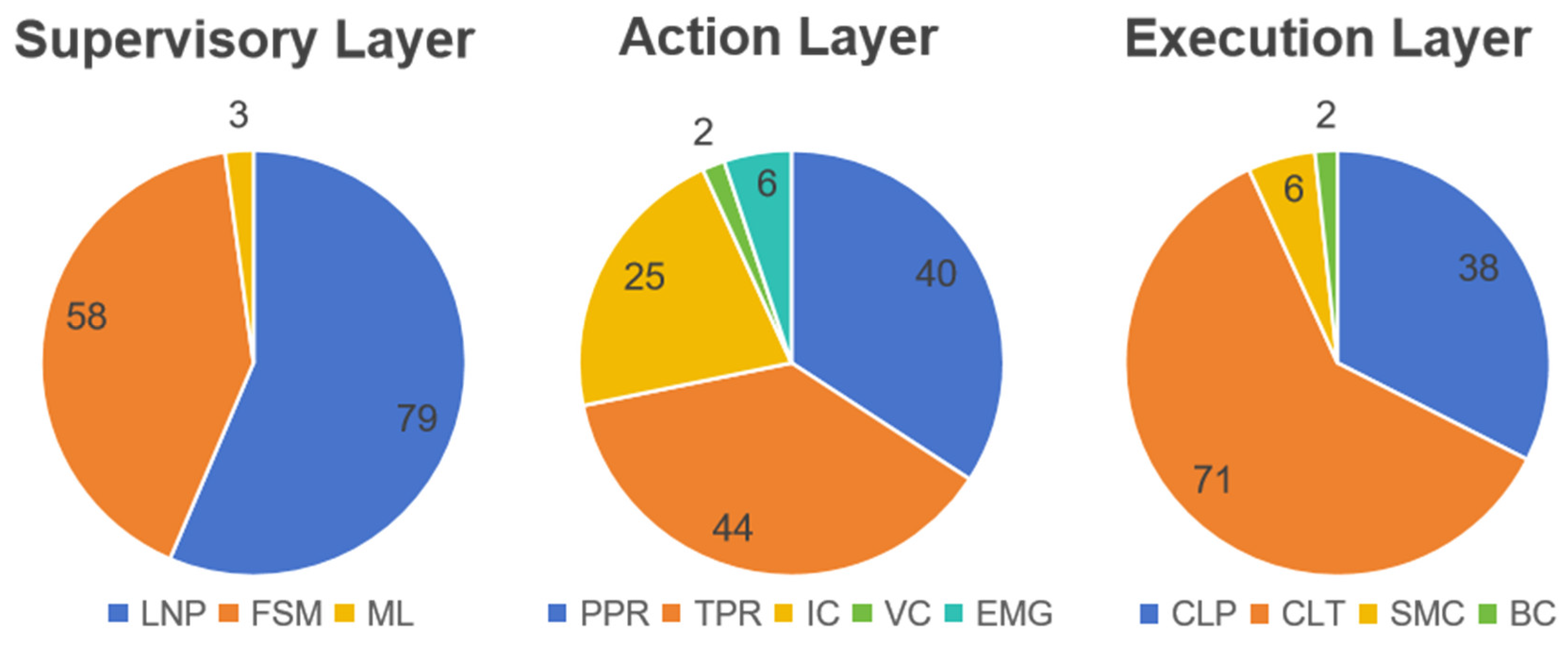
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).