
A Study on the Establishment of a Variable Stiffness Physical Model of Abdominal Soft Tissue and an Interactive Massage Force Prediction Algorithm


Abstract
1. Introduction
2. Analysis of Abdominal Anatomical Structure
2.1. Anatomical Characteristics of the Abdomen
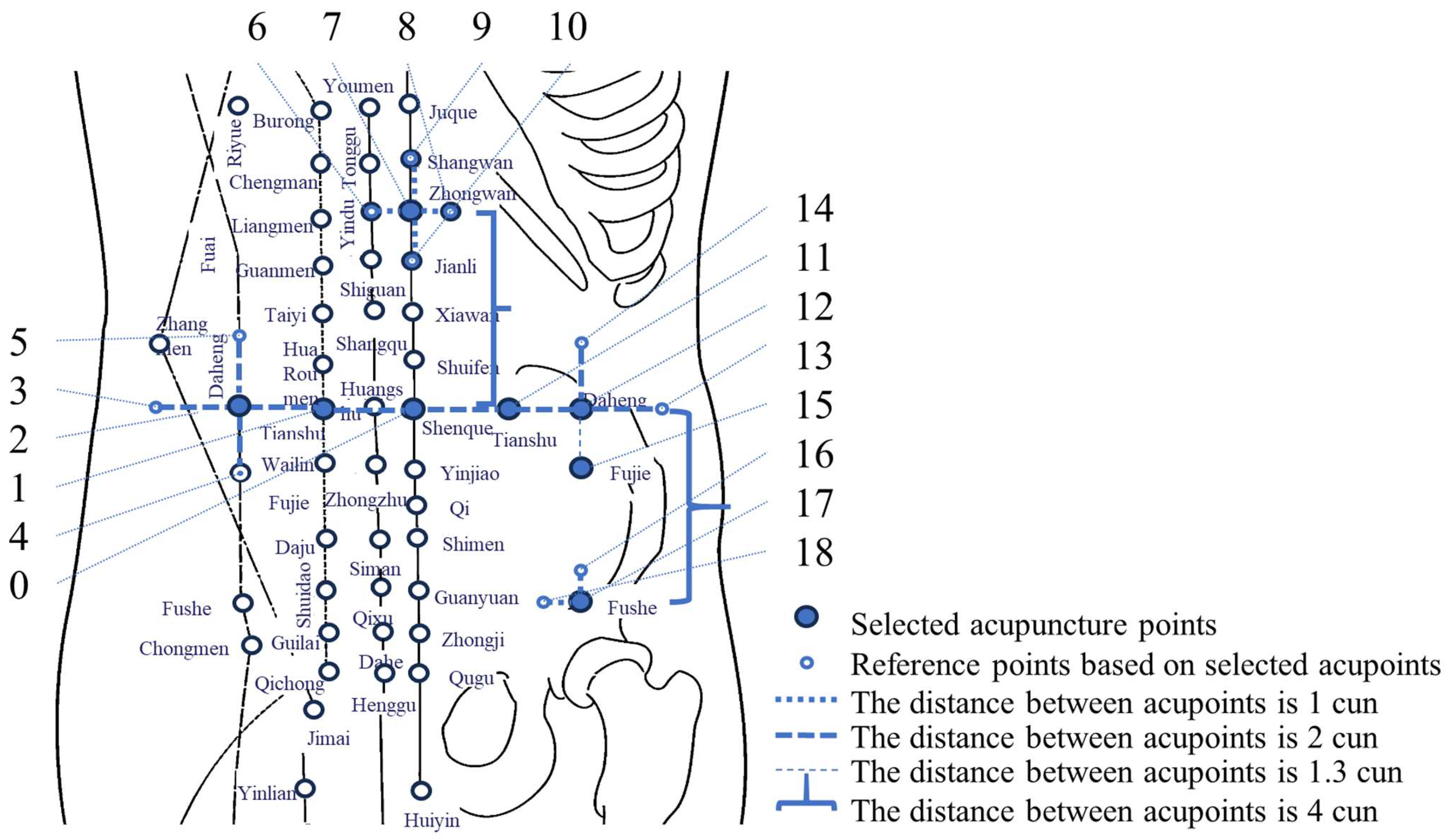
2.2. Key-Point Model for Abdominal Massage Action
3. Abdominal Human Data Collection
3.1. Experimental Subjects
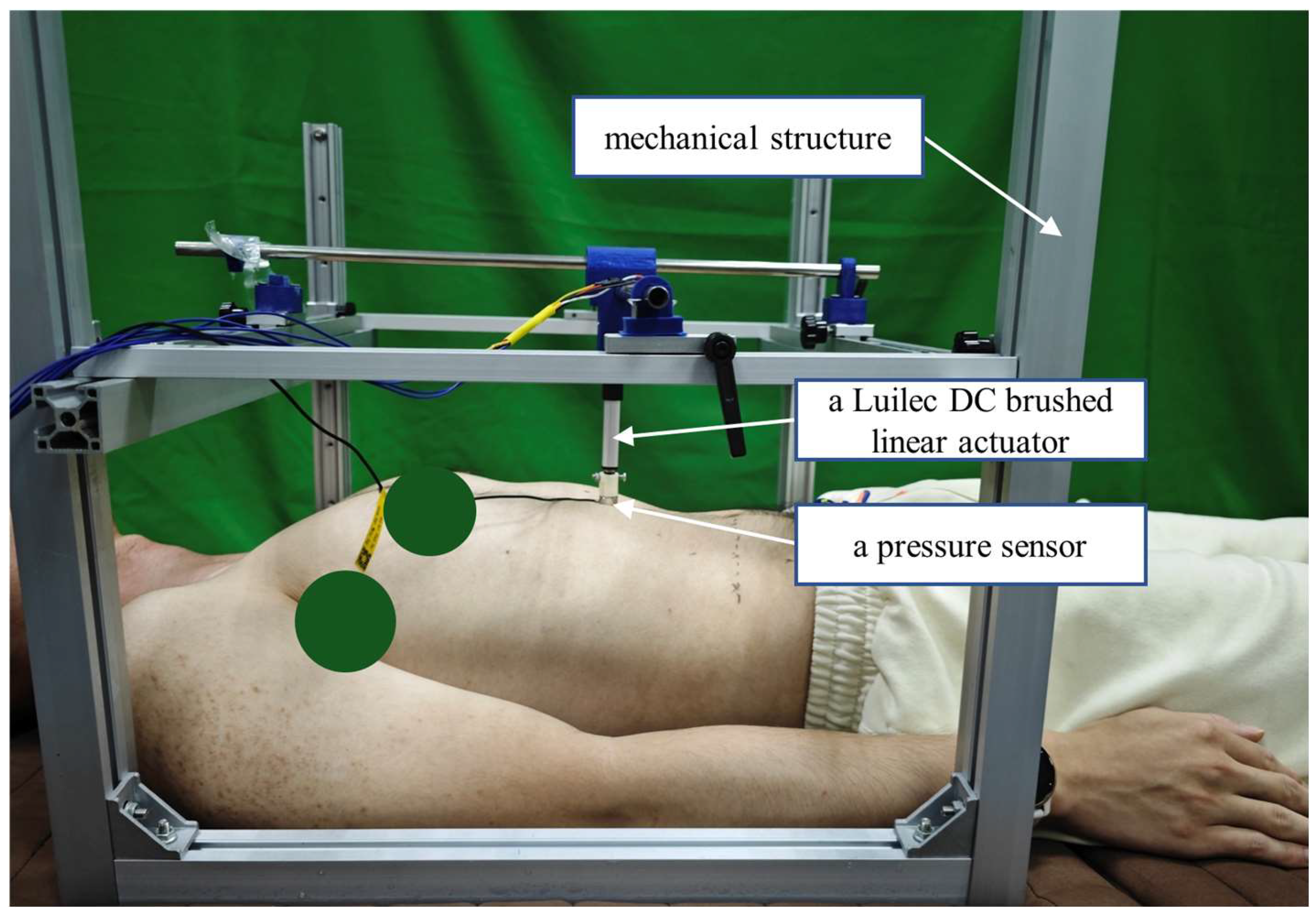
3.2. Experimental Equipment
3.3. Experimental Protocol
- Conduct a questionnaire survey for each subject, recording details such as the time of their last bowel movement within the past 24 h, as well as basic physical metrics including height, weight, body fat percentage, waist width at the navel, abdominal thickness at the navel, and age.
- Have the subject lie flat on a bed with their arms naturally resting at their sides.
- Identify and mark all anatomical landmarks on the subject’s body. Measure the corresponding distances between these landmarks. Note: For female subjects, the distance between the nipples is not recorded.
- Based on GB/T 23237-2009 “Human Measurement Methods for Acupoint Location,” [39] precisely calculate the positions of the action points and mark all identified points.
- The operator uses a muscle tension tester to locate the acupoints on the subject’s body.
- Press perpendicularly to the body surface at a slow and steady pace.
- Immediately stop pressing when the subject reports discomfort. Simultaneously, the ultrasonic distance sensor records the initial and final displacement data during the pressing process.
- Before conducting Experiment 2, administer a supplementary questionnaire to inquire whether the subject has had a bowel movement between Experiments 1 and 2.
- Have the subject lie flat on the bed again, with their arms naturally resting at their sides.
- Identify and mark all key action points.
- The operator controls the action head of the self-developed mechanical testing platform, aligning it with the abdominal action points on the subject’s body.
- The single reciprocating compression method is adopted. During a single reciprocating compression cycle, the actuator (a Luilec DC brushed linear actuator) of the mechanical experiment platform moves from a position where it does not touch the subject’s abdomen, presses into the abdomen to a target depth, and then retracts to a position where it no longer makes contact. The maximum pressing speed of the push rod motor is set to 5 mm/s, perpendicular to the surface of the abdomen. After each single reciprocating compression, data are recorded, and the target pressing depth of the push rod motor is increased by 5 mm for the next compression. This process continues until the pain threshold determined in Experiment 1 is reached. During the experiment, the pressing frequency of the push rod motor is up to 0.25 Hz, slowly acting on the human abdomen.
- Throughout the experiment, monitor and record displacement and force sensor data in real-time. Output the data uniformly after the experiment concludes.
- If the subject experiences discomfort during the experiment, stop immediately and record the data at that point. These data will provide critical support for subsequent safe force-displacement control.
4. Derivation Method and Results of the Variable Stiffness Physical Model for the Abdomen
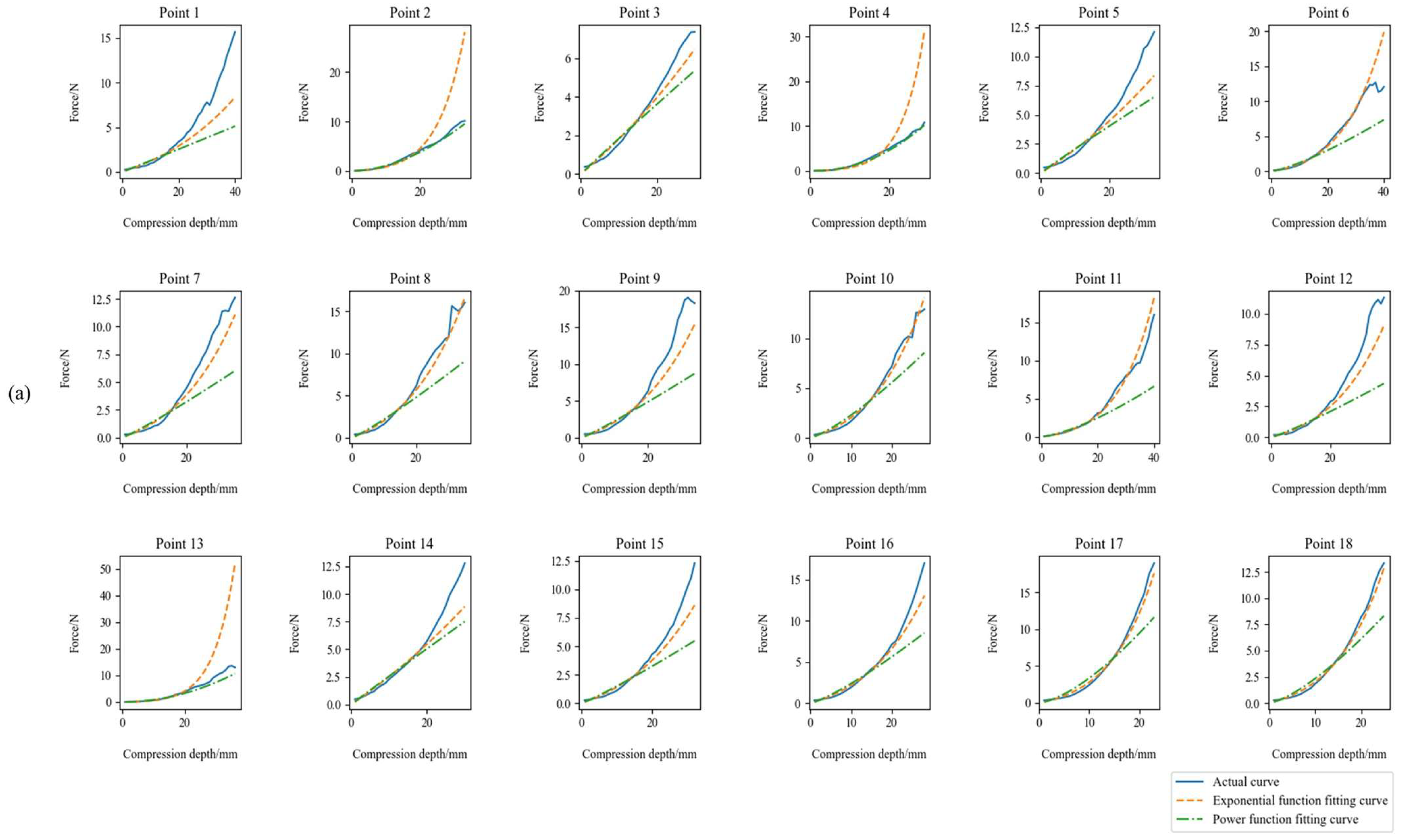
4.1. Variable Stiffness Physical Model Based on Exponential Function
4.2. Variable Stiffness Physical Model Based on Power Function Representation
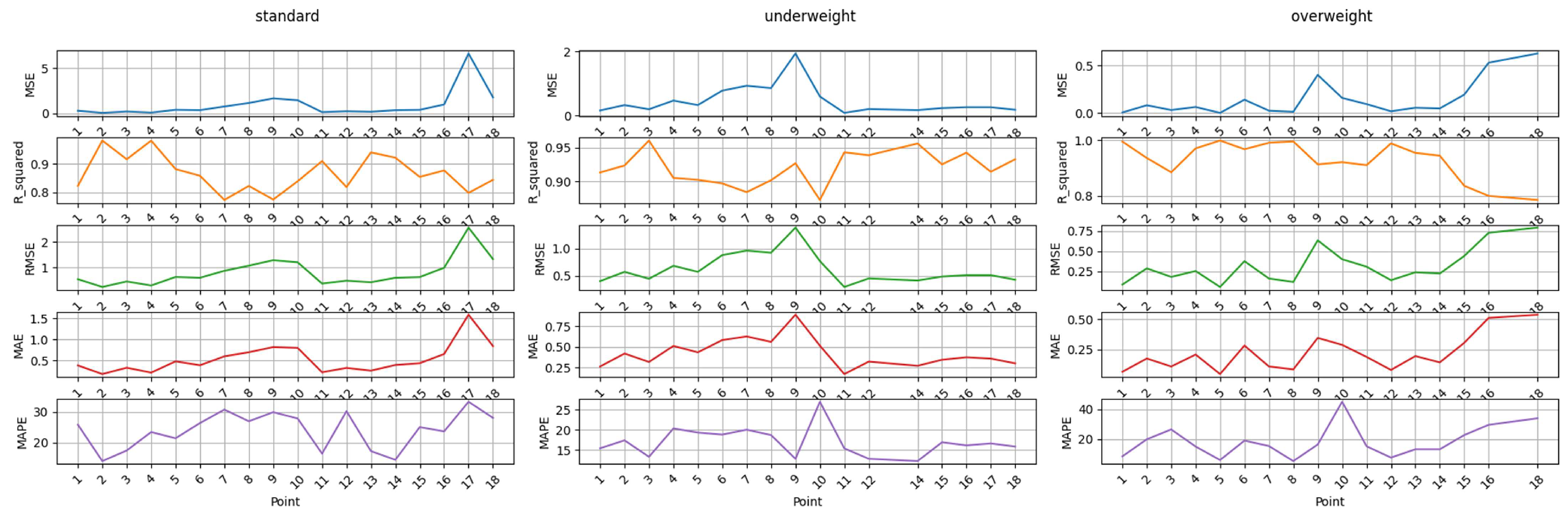
4.3. Comparison of Two Fitting Models
5. Abdominal Massage Force Prediction Algorithm Based on Machine Learning
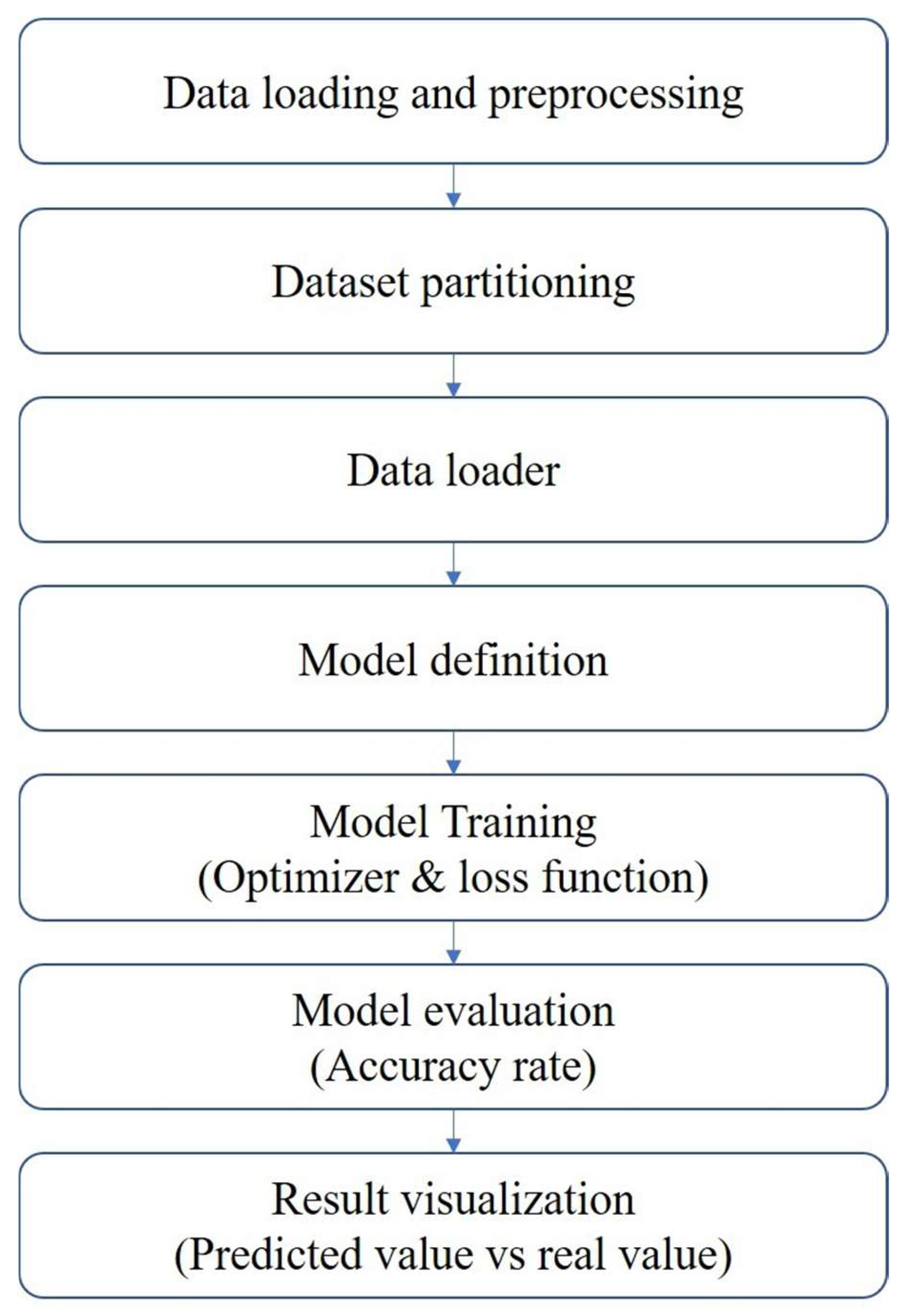
5.1. Algorithm Execution Process
- Data loading and preprocessing
- 2.
- Dataset partitioning
- 3.
- Data loader
- 4.
- Model definition
- 5.
- Model training
- 6.
- Visualization of results
5.2. Algorithm Complexity Analysis
- Time complexity
- 2.
- Space complexity
5.3. Experiments and Results
6. Discussion
- (A)
- Enriching the Database: On the one hand, the impacts of factors such as different ages, regions, genders, and constipation durations on the abdominal interaction force and pressing depth should be considered. On the other hand, the impacts of massage tips of different sizes and shapes on the abdominal force and the subjective feelings of the subjects should be taken into account. We could expand the sample set to optimize the variable-stiffness physical model. We could introduce the quantitative modeling of subjective feelings, incorporate the subjective evaluations of subjects into the data, establish a database of the mapping relationship between “mechanical parameters–subjective feelings”, and extract personalized force control grading standards for light, medium, and heavy massage, to achieve the dynamic matching between voice instructions such as “increase the force” and “decrease the force” and force control parameters for the subsequent robots.
- (B)
- Enhancing the Generalization Ability of the Model: In view of the fitting limitations of the existing exponential/power functions, we could introduce polynomial functions, fractional-order differential equations, or neural network models (such as Long Short-term Memory (LSTM) time-series networks) to construct a hybrid model framework and improve the generalization ability of the physical model.
- (C)
- Complementing Dynamic Interaction Scenarios: We could develop a respiratory motion compensation algorithm and utilize visual technology to reduce the interference problem of abdominal displacement caused by breathing, thereby improving the accuracy of the prediction model.
- (A)
- Integration with the Intelligent Adaptive Control System. a. Model-driven control strategy: Embed the established variable-stiffness physical models (exponential/power functions) into the robot control system. Through the dynamic comparison between real-time force-displacement data and model prediction values, develop an adaptive algorithm based on model predictive control or impedance control to achieve the autonomous adjustment of massage force according to the change in tissue stiffness; b. Real-time force-feedback closed-loop: Establish a real-time communication interface between the robot’s end-effector and the database. Continuously update the prediction model parameters using the massage force prediction algorithm. Combine the feedback from the force sensor to achieve a “perception–decision–execution” closed-loop control, thereby enhancing the dynamic response ability to complex abdominal deformations.
- (B)
- Integration with the Digital Twin Model: Combine finite-element simulation (such as the Abaqus soft-tissue model) with medical imaging data to construct a “mechanics-tissue state” coupling model, use the finite element model simulation of the abdomen to construct a strain rate-dependent viscoelastic constitutive equation, to better describe the stress–strain effect generated when the abdomen is subjected to external force, and to enhance the prediction ability of abdominal mechanical response characteristics during the massage process.
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brenner, D.M.; Corsetti, M.; Drossman, D.; Tack, J.; Wald, A. Perceptions, Definitions, and Therapeutic Interventions for Occasional Constipation: A Rome Working Group Consensus Document. Clin. Gastroenterol. Hepatol. 2024, 22, 397–412. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Rao, S. Constipation: Pathophysiology and Current Therapeutic Approaches. In Gastrointestinal Pharmacology. Handbook of Experimental Pharmacology; Greenwood-Van Meerveld, B., Ed.; Springer: Cham, Switzerland, 2016; Volume 239. [Google Scholar] [CrossRef]
- Imran, A.; Whitehead, W.E.; Palsson, O.S.; Trnblom, H.; Magnus Simrén. An approach to the diagnosis and management of rome iv functional disorders of chronic constipation. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 39–46. [Google Scholar]
- Zhang, X.; Li, Y.; Jiang, X.; Liu, J.; Fang, Y.; He, Z.; Cui, Q. The 99mTc-DTPA labeled solid meal was used to measure the gastric and small intestinal transit in constipation patients and evaluate its value in evaluating colonic transit in constipation patients. Chin. J. Gastroenterol. Hepatol. 2025, 34, 224–227. [Google Scholar]
- Yang, Z.; Wu, C.; Gao, J.; Bai, D.; Zhu, L.; Liu, R.; Liang, Y.; Wu, Q. Prevalence of Chronic Constipation in Chinese Adults:a Meta-analysis. Chin. Gen. Pract. 2021, 24, 2092–2097. [Google Scholar]
- Leng, Y.; Wei, W.; Tang, X. Expert Consensus on Diagnosis and Treatment of Constipation by Traditional Chinese Medicine (2024). J. Tradit. Chin. Med. 2025, 66, 321–328. [Google Scholar] [CrossRef]
- Jones, K.C.; Du, W. Development of a massage robot for medical therapy. In Proceedings of the 2003 IEEE/ASME International Conference on Advanced Intelligent Mechatronics (AIM), Kobe, Japan, 20–24 July 2003. [Google Scholar]
- Aitreat-About Emma. Available online: https://www.aitreat.com/about-emma (accessed on 6 March 2025).
- Kuka-Solutions Database. Available online: https://www.kuka.cn/zh-cn (accessed on 6 March 2025).
- Hou, P.; Han, L. Development of a home—Use back—Scrubbing and massage robot. Mach. Des. Res. 2009, 25, 101–105. [Google Scholar] [CrossRef]
- Jiao, C.B. Structural Analysis and Optimization of the LLR—1 Traditional Chinese Medicine Massage and Physical Therapy Robot. Master’s Thesis, Shandong Jianzhu University, Jinan, China, 2012. [Google Scholar]
- Kong, Y.X. Design and Research of a Hybrid Robot Based on Traditional Chinese Massage Techniques. Master’s Thesis, North University of China, Taiyuan, China, 2021. [Google Scholar] [CrossRef]
- Aubo-Robotic. Available online: https://www.aubo-robotics.cn/cases_m (accessed on 6 March 2025).
- Universal Robots. Available online: http://www.universal-robots.com/ (accessed on 6 March 2025).
- Mimidis, K.; Galinsky, D.; Rimon, E.; Papadopoulos, V.; Zicherman, Y.; Oreopoulos, D. Use of a device that applies external kneading—Like force on the abdomen for treatment of constipation. World J. Gastroenterol. 2005, 11, 5. [Google Scholar] [CrossRef]
- Mowoot. Available online: https://www.mowoot.com/en/product/mowoot-2/#moreinfo (accessed on 6 March 2025).
- Mcclurg, D.; Booth, L.; Herrero—Fresneda, I. Safety and efficacy of intermittent colonic exoperistalsis device to treat chronic constipation: A prospective multicentric clinical trial. Clin. Transl. Gastroenterol. 2020, 11, e00267. [Google Scholar] [CrossRef]
- Choi, Y.I.; Kim, K.O.; Chung, J.W.; Kim, Y.J.; Park, D.K. Effects of automatic abdominal massage device in treatment of chronic constipation patients: A prospective study. Dig. Dis. Sci. 2020, 66, 3105–3112. [Google Scholar] [CrossRef]
- Li, H.Y.; Zhao, H.; Gong, Z.K. Application of a novel intestinal massage device in stroke patients with constipation. Nurs. Res. 2018, 32, 636–638. [Google Scholar]
- Ning, P.F. A Nursing Massage Robot for Promoting Digestion. CN109498397A, 22 March 2019. [Google Scholar]
- Zhu, H.L. A Novel Abdominal Massage Device. CN202020731814, 7 May 2020. [Google Scholar]
- Gou, Y.Q.; Yang, L.X. An Abdominal Massage Device for Gastroenterology. CN211750916U, 27 October 2020. [Google Scholar]
- Tang, X.; Ping, S.; Luo, Z.; Yu, H. A Novel 6-DOF Multi-Technique Abdominal Massage Robot System: A New Solution for Relieving Constipation and an Exploration of Standardization. Electronics 2025, 14, 1123. [Google Scholar] [CrossRef]
- Cardoso, M.H.S. Experimental Study of the Human Anterolateral Abdominal Wall: Biomechanical Properties of Fascia and Muscles. Ph.D. Thesis, Universidade do Porto, Porto, Portugal, 2012. [Google Scholar]
- Assoul, N.; Flaud, P.; Chaouat, M.; Letourneur, D.; Bataille, I. Mechanical properties of rat thoracic and abdominal aortas. J. Biomech. 2008, 41, 2227–2236. [Google Scholar] [CrossRef] [PubMed]
- Wang, H. Research on the Mechanical Properties of Adipose Tissue and Its Influence on the Simulation of Thoraco—Abdominal Impact Injury. Master’s Thesis, Tianjin University of Science and Technology, Tianjin, China, 2021. [Google Scholar] [CrossRef]
- Tayebi, S.; Gutierrez, A.; Mohout, I.; Smets, E.; Wise, R.; Stiens, J.; Malbrain, M.L. A concise overview of non-invasive intra-abdominal pressure measurement techniques: From bench to bedside. J. Clin. Monit. Comput. 2021, 35, 51–70. [Google Scholar] [CrossRef]
- Leclerc, G.E.; Debernard, L.; Foucart, F.; Robert, L.; Pelletier, K.M.; Charleux, F.; Ehman, R.; Tho, M.-C.H.B.; Bensamoun, S.F. Characterization of a hyper—Viscoelastic phantom mimicking biological soft tissue using an abdominal pneumatic driver with magnetic resonance elastography (MRE). J. Biomech. 2012, 45, 952–957. [Google Scholar] [CrossRef] [PubMed]
- Li, F.T.; Sun, L.F.; Tao, Y.P.; Yang, P.; Ji, M.Q.; Sang, J.B. Inversion of constitutive parameters of plantar soft tissue using random forest and neural networks algorithms. Med. Biomech. 2024, 39, 476–481. [Google Scholar]
- Remus, R.; Sure, C.; Selkmann, S.; Uttich, E.; Bender, B. Soft tissue material properties based on human abdominal in vivo macroindenter measurements. Front. Bioeng. Biotechnol. 2024, 12, 1384062. [Google Scholar] [CrossRef]
- Zheng, Y.; Ning, H.; Rangarajan, E.; Merali, A.; Geale, A.; Lindenroth, L.; Xu, Z.; Wang, W.; Kruse, P.; Morris, S.; et al. Design of a Cost-Effective Ultrasound Force Sensor and Force Control System for Robotic Extra-Body Ultrasound Imaging. Sensors 2025, 25, 468. [Google Scholar] [CrossRef]
- Kim, J.; Ahn, B.; De, S.; Srinivasan, M.A. An efficient soft tissue characterization algorithm from in vivo indentation experiments for medical simulation. Int. J. Med. Robot. Comput. Assist. Surg. 2010, 4, 277–285. [Google Scholar] [CrossRef]
- Robinson, D.G. The Dynamic Response of the Seated Human to Mechanical Shock. Ph.D. Thesis, Simon Fraser University, Burnaby, BC, Canada, 1999. [Google Scholar]
- Lim, Y.J.; Deo, D.; Singh, T.P.; Jones, D.B.; De, S. In situ measurement and modeling of biomechanical response of human cadaveric soft tissues for physics—Based surgical simulation. Surg. Endosc. 2009, 23, 1298–1307. [Google Scholar] [CrossRef]
- Shao, Y.; Zou, D.; Li, Z.; Wan, L.; Qin, Z.; Liu, N.; Zhang, J.; Zhong, L.; Chen, Y. Blunt liver injury with intact ribs under impacts on the abdomen: A biomechanical investigation. PLoS ONE 2013, 8, e52366. [Google Scholar] [CrossRef]
- Lan, F.C.; Cai, Z.H.; Chen, J.Q.; Ma, Z.W. Biomechanical Responses and Injury Evaluation of Human Thorax and Abdomen During Vehicle Collision. J. South China Univ. Technol. (Nat. Sci. Ed.) 2012, 40, 70–78. [Google Scholar]
- Du, T. Research on the Impact Biomechanics Response and Injury Evaluation of the Thorax of Automobile Occupants Covering the Liver. South China University of Technology. Ph.D. Thesis, Guangzhou, China, 2018. [Google Scholar]
- Hu, H.; Li, X.; Ding, L.; Zhao, C. Establishment of a Finite Element Model of the Thorax and Abdomen and Analysis of Collision Biomechanics. Stand. Sci. 2015, 7, 15–18+44. [Google Scholar] [CrossRef]
- GB/T 23237-2009; Methods of Anthropometry for Locating Acupuncture Points. China Standards Press: Beijing, China, 2009.
- Maurel, W.; Wu, Y.; Thalmann, N.M.; Thalmann, D. Biomechanical Models for Soft Tissue Simulation; Springer: Berlin/Heidelberg, Germany, 1998; pp. 23–25. [Google Scholar]
- Xu, S.P.; Liu, X.P.; Zhang, H.; Luo, J. Research progress on real—Time deformation models of soft tissues in virtual surgery. J. Biomed. Eng. 2010, 27, 435–439. [Google Scholar]
- Zhang, Q.K.; Luo, L.M.; Yang, W. Nonlinear model for real—Time simulation of soft tissue deformation. J. Appl. Sci. 2007, 25, 276–282. [Google Scholar]
- Jiang, C.T. Research on the Elastic Model of Human Soft Tissues. Master’s Thesis, Southeast University, Dhaka, Bangladesh, 2004. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject ID | Body Type | BMI | Age Group | Gender |
|---|---|---|---|---|
| 1 | Underweight | 17.6 | 30–40 | Female |
| 2 | Underweight | 16.7 | 20–30 | Female |
| 3 | Underweight | 17.5 | 20–30 | Female |
| 4 | Underweight | 18.4 | 20–30 | Male |
| 5 | Overweight | 25.5 | 20–30 | Male |
| 6 | Overweight | 24.4 | <20 | Male |
| 7 | Overweight | 24.9 | 30–40 | Male |
| 8 | Standard | 21.2 | 30–40 | Female |
| 9 | Standard | 21 | 20–30 | Female |
| 10 | Standard | 23.6 | 20–30 | Female |
| 11 | Standard | 23.9 | 30–40 | Male |
| 12 | Standard | 22.6 | <20 | Male |
| Point | a | b | MSE | R_Square | RMSE | MAE | MAPE | |
|---|---|---|---|---|---|---|---|---|
| standard | 1 | 0.1004 | 0.0183 | 0.1054 | 0.9347 | 0.3246 | 0.2604 | 20.9452 |
| 2 | 0.0302 | 0.1011 | 0.2988 | 0.8963 | 0.5466 | 0.3162 | 14.7593 | |
| 3 | 0.1659 | 0.0087 | 0.0660 | 0.9721 | 0.2569 | 0.2097 | 13.5855 | |
| 4 | 0.0175 | 0.1418 | 1.2439 | 0.7224 | 1.1153 | 0.6087 | 30.1429 | |
| 5 | 0.1864 | 0.0093 | 0.1430 | 0.9565 | 0.3781 | 0.3215 | 16.9908 | |
| 6 | 0.0650 | 0.0508 | 0.0346 | 0.9860 | 0.1860 | 0.1411 | 13.7449 | |
| 7 | 0.0997 | 0.0330 | 0.2318 | 0.9298 | 0.4815 | 0.3619 | 21.8757 | |
| 8 | 0.1433 | 0.0343 | 0.2687 | 0.9582 | 0.5184 | 0.3492 | 17.4046 | |
| 9 | 0.1539 | 0.0318 | 0.5055 | 0.9308 | 0.7110 | 0.4662 | 20.6267 | |
| 10 | 0.1209 | 0.0509 | 0.1835 | 0.9795 | 0.4284 | 0.3207 | 15.5394 | |
| 11 | 0.0452 | 0.0579 | 0.0081 | 0.9944 | 0.0902 | 0.0570 | 4.8663 | |
| 12 | 0.0611 | 0.0358 | 0.0474 | 0.9618 | 0.2176 | 0.1648 | 19.4340 | |
| 13 | 0.0179 | 0.1220 | 0.1209 | 0.9579 | 0.3477 | 0.1915 | 14.9959 | |
| 14 | 0.2327 | 0.0080 | 0.1368 | 0.9693 | 0.3698 | 0.2576 | 11.0203 | |
| 15 | 0.1039 | 0.0297 | 0.0864 | 0.9671 | 0.2940 | 0.2309 | 16.5623 | |
| 16 | 0.1410 | 0.0427 | 0.1090 | 0.9862 | 0.3302 | 0.2413 | 12.7977 | |
| 17 | 0.1282 | 0.0778 | 0.4326 | 0.9868 | 0.6577 | 0.4582 | 14.7612 | |
| 18 | 0.1082 | 0.0624 | 0.1181 | 0.9895 | 0.3437 | 0.2525 | 13.2991 | |
| underweight | 1 | 0.0589 | 0.0341 | 0.0164 | 0.9910 | 0.1280 | 0.0939 | 6.7222 |
| 2 | 0.1732 | 0.0097 | 0.0834 | 0.9803 | 0.2888 | 0.2231 | 12.2858 | |
| 3 | 0.1579 | 0.0177 | 0.0163 | 0.9967 | 0.1278 | 0.1078 | 7.4928 | |
| 4 | 0.1618 | 0.0144 | 0.1159 | 0.9764 | 0.3404 | 0.2771 | 13.6856 | |
| 5 | 0.1634 | 0.0064 | 0.1098 | 0.9670 | 0.3313 | 0.2697 | 14.8614 | |
| 6 | 0.1018 | 0.0398 | 0.0733 | 0.9903 | 0.2708 | 0.2104 | 8.8662 | |
| 7 | 0.0959 | 0.0431 | 0.0716 | 0.9910 | 0.2676 | 0.2005 | 8.5638 | |
| 8 | 0.1154 | 0.0382 | 0.0789 | 0.9909 | 0.2808 | 0.1882 | 9.5939 | |
| 9 | 0.3083 | 0.0225 | 0.3865 | 0.9853 | 0.6217 | 0.4201 | 7.0918 | |
| 10 | 0.0627 | 0.0492 | 0.0435 | 0.9906 | 0.2086 | 0.1786 | 15.6618 | |
| 11 | 0.0233 | 0.0693 | 0.0168 | 0.9885 | 0.1295 | 0.0802 | 10.9623 | |
| 12 | 0.2055 | −0.0012 | 0.1001 | 0.9694 | 0.3164 | 0.2447 | 11.4228 | |
| 14 | 0.0839 | 0.0370 | 0.0098 | 0.9974 | 0.0991 | 0.0756 | 6.1102 | |
| 15 | 0.1442 | 0.0107 | 0.0561 | 0.9819 | 0.2368 | 0.1808 | 11.7923 | |
| 16 | 0.1570 | 0.0154 | 0.0355 | 0.9921 | 0.1883 | 0.1546 | 9.8284 | |
| 17 | 0.1272 | 0.0142 | 0.0669 | 0.9778 | 0.2586 | 0.1989 | 11.6283 | |
| 18 | 0.1043 | 0.0205 | 0.0231 | 0.9913 | 0.1521 | 0.1196 | 8.7519 | |
| overweight | 1 | 0.0219 | 0.1113 | 0.2893 | 0.8053 | 0.5378 | 0.3175 | 22.2520 |
| 2 | 0.0143 | 0.1216 | 0.0603 | 0.9532 | 0.2455 | 0.1378 | 11.0655 | |
| 3 | 0.0197 | 0.0633 | 0.0013 | 0.9953 | 0.0364 | 0.0304 | 15.3565 | |
| 4 | 0.0752 | 0.0524 | 0.0462 | 0.9789 | 0.2150 | 0.1423 | 8.6169 | |
| 5 | 0.0320 | 0.1010 | 0.2505 | 0.8911 | 0.5005 | 0.2917 | 21.2097 | |
| 6 | 0.0345 | 0.1111 | 0.5196 | 0.8808 | 0.7209 | 0.4042 | 13.9233 | |
| 7 | 0.0125 | 0.1561 | 0.8696 | 0.6874 | 0.9325 | 0.4799 | 30.5411 | |
| 8 | 0.0294 | 0.1147 | 0.6115 | 0.8014 | 0.7820 | 0.4543 | 24.0232 | |
| 9 | 0.0309 | 0.1290 | 2.3355 | 0.4953 | 1.5283 | 0.8559 | 49.3368 | |
| 10 | 0.0058 | 0.1846 | 0.7322 | 0.6379 | 0.8557 | 0.4323 | 32.1401 | |
| 11 | 0.0316 | 0.0723 | 0.0032 | 0.9970 | 0.0566 | 0.0465 | 6.8349 | |
| 12 | 0.0203 | 0.1200 | 0.4308 | 0.7512 | 0.6564 | 0.3661 | 31.9549 | |
| 13 | 0.1418 | 0.0056 | 0.0218 | 0.9825 | 0.1476 | 0.1269 | 10.9313 | |
| 14 | 0.0387 | 0.0601 | 0.0005 | 0.9995 | 0.0219 | 0.0181 | 4.2279 | |
| 15 | 0.0771 | 0.0268 | 0.0652 | 0.9450 | 0.2554 | 0.1932 | 16.9639 | |
| 16 | 0.0994 | 0.0329 | 0.1472 | 0.9444 | 0.3836 | 0.2931 | 20.0819 | |
| 18 | 0.0702 | 0.0521 | 0.1122 | 0.9616 | 0.3350 | 0.2569 | 20.3195 |
| Point | c | d | MSE | R_Squared | RMSE | MAE | MAPE | |
|---|---|---|---|---|---|---|---|---|
| standard | 1 | 0.1210 | 1.0147 | 0.2865 | 0.8223 | 0.5353 | 0.3870 | 25.8445 |
| 2 | 0.0156 | 1.8341 | 0.0518 | 0.9820 | 0.2275 | 0.1834 | 13.8429 | |
| 3 | 0.1956 | 0.9733 | 0.1987 | 0.9161 | 0.4457 | 0.3324 | 17.3393 | |
| 4 | 0.0072 | 2.1564 | 0.0816 | 0.9818 | 0.2856 | 0.2176 | 23.4146 | |
| 5 | 0.2287 | 0.9584 | 0.3891 | 0.8815 | 0.6238 | 0.4819 | 21.3691 | |
| 6 | 0.0615 | 1.2968 | 0.3506 | 0.8579 | 0.5921 | 0.3910 | 26.3764 | |
| 7 | 0.1143 | 1.1155 | 0.7508 | 0.7727 | 0.8665 | 0.6009 | 30.7987 | |
| 8 | 0.1576 | 1.1406 | 1.1429 | 0.8220 | 1.0691 | 0.6975 | 26.9581 | |
| 9 | 0.1797 | 1.1006 | 1.6511 | 0.7741 | 1.2850 | 0.8193 | 29.9418 | |
| 10 | 0.1165 | 1.2890 | 1.4466 | 0.8385 | 1.2027 | 0.8003 | 27.8771 | |
| 11 | 0.0354 | 1.4185 | 0.1319 | 0.9094 | 0.3632 | 0.2256 | 16.3205 | |
| 12 | 0.0682 | 1.1421 | 0.2259 | 0.8181 | 0.4752 | 0.3284 | 30.2806 | |
| 13 | 0.0082 | 2.0031 | 0.1716 | 0.9402 | 0.4143 | 0.2635 | 17.1454 | |
| 14 | 0.2678 | 0.9801 | 0.3489 | 0.9217 | 0.5907 | 0.3965 | 14.2547 | |
| 15 | 0.1142 | 1.1165 | 0.3837 | 0.8538 | 0.6194 | 0.4384 | 25.0321 | |
| 16 | 0.1383 | 1.2367 | 0.9736 | 0.8768 | 0.9867 | 0.6561 | 23.6336 | |
| 17 | 0.1077 | 1.4937 | 6.6155 | 0.7977 | 2.5721 | 1.5820 | 33.3749 | |
| 18 | 0.0965 | 1.3848 | 1.7658 | 0.8435 | 1.3288 | 0.8422 | 28.0752 | |
| underweight | 1 | 0.0504 | 1.2684 | 0.1591 | 0.9130 | 0.3989 | 0.2621 | 15.4010 |
| 2 | 0.2011 | 0.9960 | 0.3253 | 0.9233 | 0.5703 | 0.4196 | 17.3723 | |
| 3 | 0.1578 | 1.1062 | 0.1951 | 0.9601 | 0.4417 | 0.3171 | 13.2735 | |
| 4 | 0.1830 | 1.0353 | 0.4667 | 0.9049 | 0.6832 | 0.5122 | 20.3224 | |
| 5 | 0.2017 | 0.9512 | 0.3256 | 0.9022 | 0.5706 | 0.4342 | 19.3071 | |
| 6 | 0.0848 | 1.3139 | 0.7768 | 0.8968 | 0.8814 | 0.5835 | 18.8015 | |
| 7 | 0.0800 | 1.3324 | 0.9284 | 0.8839 | 0.9635 | 0.6276 | 20.0087 | |
| 8 | 0.0978 | 1.2968 | 0.8562 | 0.9015 | 0.9253 | 0.5617 | 18.6840 | |
| 9 | 0.2933 | 1.1550 | 1.9354 | 0.9266 | 1.3912 | 0.8928 | 12.7703 | |
| 10 | 0.0512 | 1.3777 | 0.5932 | 0.8724 | 0.7702 | 0.5153 | 26.9514 | |
| 11 | 0.0134 | 1.6425 | 0.0838 | 0.9427 | 0.2896 | 0.1697 | 15.3725 | |
| 12 | 0.2540 | 0.9057 | 0.2013 | 0.9384 | 0.4487 | 0.3212 | 12.7762 | |
| 14 | 0.0640 | 1.3327 | 0.1686 | 0.9558 | 0.4106 | 0.2703 | 12.2073 | |
| 15 | 0.1649 | 1.0088 | 0.2327 | 0.9249 | 0.4824 | 0.3437 | 16.8887 | |
| 16 | 0.1678 | 1.0646 | 0.2593 | 0.9422 | 0.5092 | 0.3743 | 16.1239 | |
| 17 | 0.1385 | 1.0496 | 0.2586 | 0.9141 | 0.5085 | 0.3582 | 16.5999 | |
| 18 | 0.1052 | 1.1187 | 0.1799 | 0.9325 | 0.4242 | 0.2999 | 15.8232 | |
| overweight | 1 | 0.0103 | 1.9213 | 0.0075 | 0.9950 | 0.0864 | 0.0657 | 8.4288 |
| 2 | 0.0077 | 1.9173 | 0.0823 | 0.9362 | 0.2868 | 0.1752 | 19.8938 | |
| 3 | 0.0174 | 1.3865 | 0.0326 | 0.8853 | 0.1806 | 0.1092 | 26.5079 | |
| 4 | 0.0612 | 1.3669 | 0.0643 | 0.9706 | 0.2536 | 0.2081 | 15.0075 | |
| 5 | 0.0158 | 1.8478 | 0.0032 | 0.9986 | 0.0564 | 0.0467 | 5.9198 | |
| 6 | 0.0189 | 1.8538 | 0.1410 | 0.9677 | 0.3754 | 0.2825 | 19.0025 | |
| 7 | 0.0047 | 2.2608 | 0.0260 | 0.9907 | 0.1612 | 0.1097 | 15.3694 | |
| 8 | 0.0131 | 1.9668 | 0.0141 | 0.9954 | 0.1185 | 0.0851 | 5.2082 | |
| 9 | 0.0103 | 2.1706 | 0.4004 | 0.9135 | 0.6327 | 0.3455 | 16.3824 | |
| 10 | 0.0023 | 2.3890 | 0.1594 | 0.9212 | 0.3992 | 0.2882 | 45.1130 | |
| 11 | 0.0223 | 1.5366 | 0.0946 | 0.9105 | 0.3076 | 0.1885 | 15.1905 | |
| 12 | 0.0081 | 2.0405 | 0.0197 | 0.9886 | 0.1404 | 0.0808 | 7.5740 | |
| 13 | 0.1600 | 0.9742 | 0.0567 | 0.9544 | 0.2381 | 0.1954 | 13.1718 | |
| 14 | 0.0290 | 1.4443 | 0.0496 | 0.9446 | 0.2226 | 0.1433 | 13.1665 | |
| 15 | 0.0845 | 1.0988 | 0.1934 | 0.8369 | 0.4398 | 0.3049 | 22.7294 | |
| 16 | 0.1138 | 1.1101 | 0.5278 | 0.8007 | 0.7265 | 0.5110 | 29.6168 | |
| 18 | 0.0738 | 1.2495 | 0.6245 | 0.7863 | 0.7903 | 0.5376 | 33.9833 |
| Type | Calculation Range | Model 1 | Model 2 |
|---|---|---|---|
| standard | 0–15 | 94.44% | 82.96% |
| 0–20 | 90.56% | 72.22% | |
| full data | 46.03% | 35.85% | |
| underweight | 0–15 | 92.59% | 82.22% |
| 0–20 | 92.22% | 84.17% | |
| full data | 55.43% | 40.25% | |
| overweight | 0–15 | 88.52% | 92.96% |
| 0–20 | 83.33% | 84.44% | |
| full data | 42.99% | 45.90% |
| Feature | |
|---|---|
| Input | Gender |
| Subjective Perception: Fear of Pain or Not | |
| Subjective Perception: Sensitivity to Tickling or Not | |
| Action Point | |
| Body Fat Percentage. | |
| Average Distance of “one cun” | |
| Abdominal Thickness (over the navel) | |
| Waist Width (over the navel) | |
| Weight | |
| BMI | |
| Pressing Depth | |
| Output | The predicted value of the massage force |
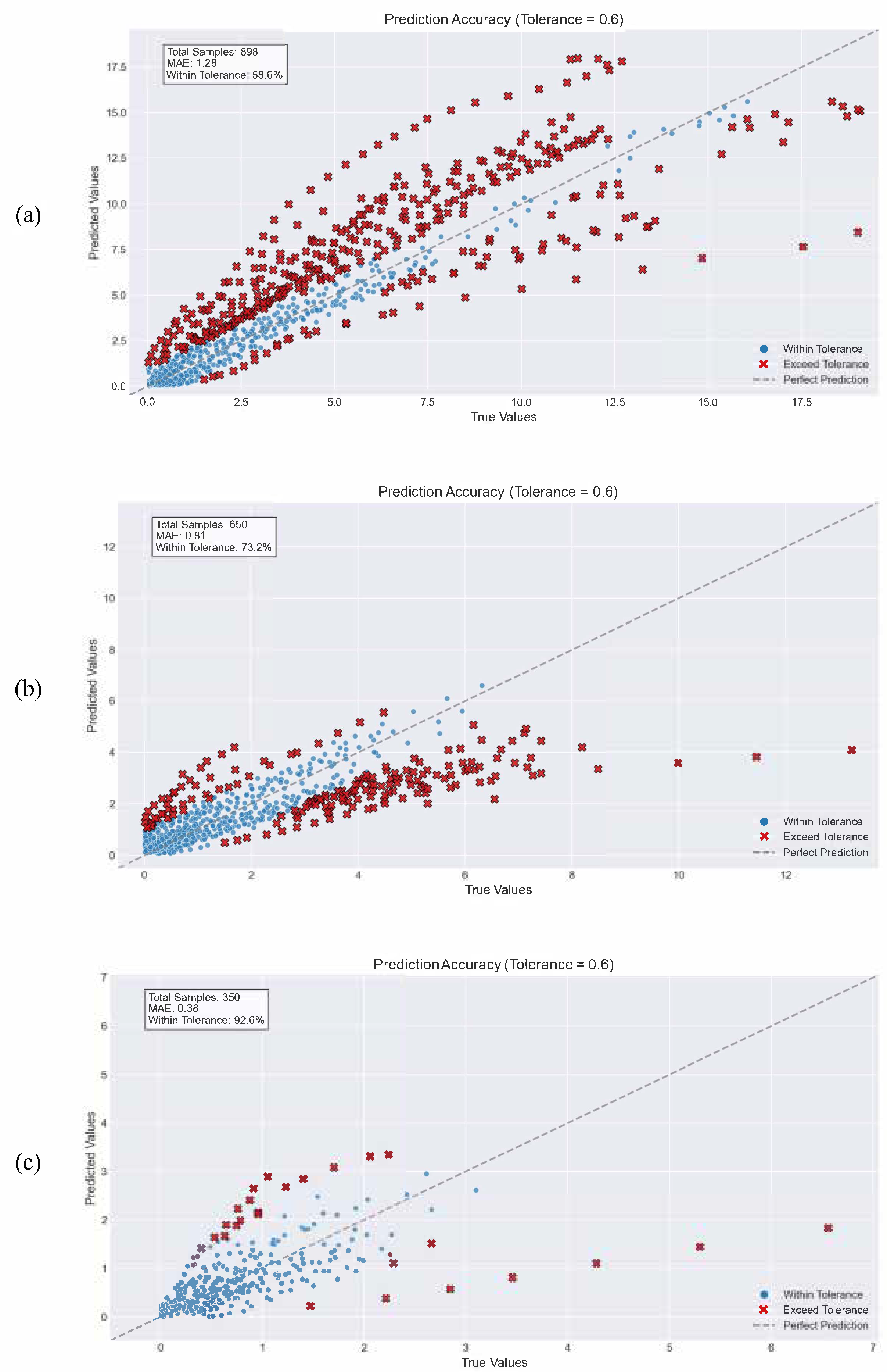
| Calculation Range | Accuracy |
|---|---|
| 0–15 | 92.60% |
| 0–20 | 73.20% |
| full data | 58.60% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, X.; Shi, P.; Luo, Z.; Li, S.; Yu, H. A Study on the Establishment of a Variable Stiffness Physical Model of Abdominal Soft Tissue and an Interactive Massage Force Prediction Algorithm. Machines 2025, 13, 441. https://doi.org/10.3390/machines13060441
Tang X, Shi P, Luo Z, Li S, Yu H. A Study on the Establishment of a Variable Stiffness Physical Model of Abdominal Soft Tissue and an Interactive Massage Force Prediction Algorithm. Machines. 2025; 13(6):441. https://doi.org/10.3390/machines13060441
Chicago/Turabian StyleTang, Xinyi, Ping Shi, Zhenjie Luo, Sujiao Li, and Hongliu Yu. 2025. "A Study on the Establishment of a Variable Stiffness Physical Model of Abdominal Soft Tissue and an Interactive Massage Force Prediction Algorithm" Machines 13, no. 6: 441. https://doi.org/10.3390/machines13060441
APA StyleTang, X., Shi, P., Luo, Z., Li, S., & Yu, H. (2025). A Study on the Establishment of a Variable Stiffness Physical Model of Abdominal Soft Tissue and an Interactive Massage Force Prediction Algorithm. Machines, 13(6), 441. https://doi.org/10.3390/machines13060441