
Food Neophobia in Brazilian Children: A Nationwide Cross-Sectional Study Comparing Neurodivergent and Neurotypical Children with and Without Dietary Restrictions

 ,
, 
 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
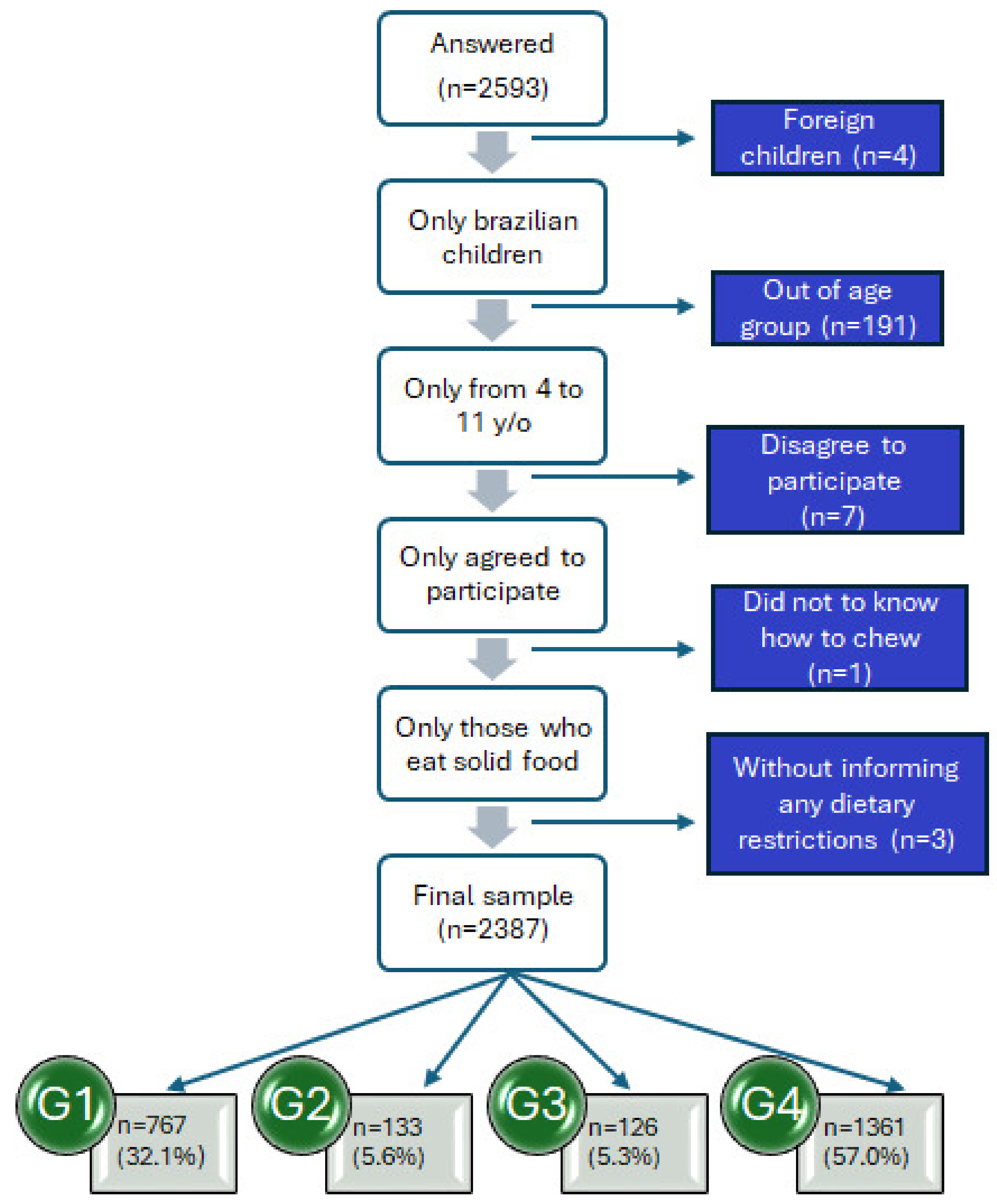
2.1. Participants
2.2. Instruments and Application
2.3. Statistical Analysis
3. Results

{kind=link}
| Categories | Sample | ||
|---|---|---|---|
| n | % | ||
| Gender | Female | 1009 | 42.3 |
| Male | 1378 | 57.7 | |
| Age | 4 years old | 460 | 19.3 |
| 5 years old | 406 | 17.0 | |
| 6 years old | 321 | 13.4 | |
| 7 years old | 243 | 10.2 | |
| 8 years old | 272 | 11.4 | |
| 9 years old | 276 | 11.6 | |
| 10 years old | 221 | 9.3 | |
| 11 years old | 188 | 7.9 | |
| Diagnose a | Down’s syndrome | 266 | 11.1 |
| Autism spectrum disorder | 604 | 25.3 | |
| Sensory processing disorder | 13 | 0.5 | |
| Attention deficit hyperactivity disorder (ADHD) | 37 | 1.5 | |
| Giftedness/high-ability | 4 | 0.1 | |
| Epilepsy | 8 | 0.3 | |
| Intellectual disability | 3 | 0.1 | |
| Heart disease | 6 | 0.2 | |
| Thyroid diseases b | 6 | 0.2 | |
| Eating disorders c | 20 | 0.8 | |
| Food intolerance d | 158 | 6.6 | |
| Food allergies e | 136 | 5.7 | |
| Celiac disease | 4 | 0.1 | |
| G6PD enzyme deficiency | 2 | 0.1 | |
| Diabetes | 1 | 0.1 | |
| Inflammatory bowel disease | 1 | 0.1 | |
| Colitis | 1 | 0.1 | |
| Gluten sensitivity | 2 | 0.1 | |
| Fructosemia | 1 | 0.1 | |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Volkmar, F.R. Encyclopedia of Autism Spectrum Disorders. Encycl. Autism Spectr. Disord. Second Ed. 2021, 2, 5329. [Google Scholar]
- Mcgee, M. Neurodiversity. SAGE J. 2012, 11, 12–13. [Google Scholar] [CrossRef]
- Cleveland Clinic Neurodivergent. Available online: https://my.clevelandclinic.org/health/symptoms/23154-neurodivergent (accessed on 15 December 2024).
- Swanepoel, A. Evolutionary Perspective Basic Points. Clin. Neuropsychiatry 2024, 21, 451–454. [Google Scholar] [CrossRef]
- Parliamentary Office of Science and Technology (POST). Support for Children and Young People; Parliamentary Office of Science and Technology (POST): London, UK, 2024. [Google Scholar]
- Uchoa, B.K.P.; Araújo, A.E.; Menescala, J.V.; Leite, Á.J.M. “This Boy Doesn’t Eat”—Mothers’ Narratives about Food Selectivity and Autism. Cad. Bras. Ter. Ocupacional 2024, 32, e3848. [Google Scholar] [CrossRef]
- Williams, K.E.; Seiverling, L.J. Neophobia in Children with Special Needs: Selective Eating and Its Treatment. In Food Neophobia Behavioral and Biological Influences; Woodhead Publishing: London, UK, 2018; pp. 351–371. [Google Scholar] [CrossRef]
- Almeida, P.C.D.; Rosane, B.P.; Nakano, E.Y.; Vasconcelos, I.A.L.; Zandonadi, R.P.; Botelho, R.B.A. Instrument to Identify Food Neophobia in Brazilian Children by Their Caregivers. Nutrients 2020, 12, 1943. [Google Scholar] [CrossRef]
- Pliner, P.; Hobden, K. Development of a Scale to Measure the Trait of Food Neophobia in Humans. Appetite 1992, 19, 105–120. [Google Scholar] [CrossRef]
- Pliner, P. Development of Measures of Food Neophobia in Children. Appetite 1994, 23, 147–163. [Google Scholar] [CrossRef]
- De Almeida, P.C.; Vasconcelos, I.A.L.; Zandonadi, R.P.; Nakano, E.Y.; Raposo, A.; Han, H.; Araya-Castillo, L.; Ariza-Montes, A.; Botelho, R.B.A. Food Neophobia among Brazilian Children: Prevalence and Questionnaire Score Development. Sustainability 2022, 14, 975. [Google Scholar] [CrossRef]
- Herle, M.; Carter Leno, V.; Mandy, W. Recommendations for Advancing Understanding of Eating Disorders in Neurodivergent People: A Commentary on Inal-Kaleli et al. 2024 and Nimbley et al. 2024. Int. J. Eat. Disord. 2025, 58, 677–679. [Google Scholar] [CrossRef]
- Cobbaert, L.; Millichamp, A.R.; Elwyn, R.; Silverstein, S.; Schweizer, K.; Thomas, E.; Miskovic-Wheatley, J. Neurodivergence, Intersectionality, and Eating Disorders: A Lived Experience-Led Narrative Review. J. Eat. Disord. 2024, 12, 187. [Google Scholar] [CrossRef]
- Harris, H.A.; Mou, Y.; DIeleman, G.C.; Voortman, T.; Jansen, P.W. Child Autistic Traits, Food Selectivity, and Diet Quality: A Population-Based Study. J. Nutr. 2022, 152, 856–862. [Google Scholar] [CrossRef]
- Byrska, A.; Błażejczyk, I.; Faruga, A.; Potaczek, M.; Wilczyński, K.M.; Janas-Kozik, M. Patterns of Food Selectivity among Children with Autism Spectrum Disorder. J. Clin. Med. 2023, 12, 5469. [Google Scholar] [CrossRef] [PubMed]
- Molina-López, J.; Leiva-García, B.; Planells, E.; Planells, P. Food Selectivity, Nutritional Inadequacies, and Mealtime Behavioral Problems in Children with Autism Spectrum Disorder Compared to Neurotypical Children. Int. J. Eat. Disord. 2021, 54, 2155–2166. [Google Scholar] [CrossRef] [PubMed]
- Tahech, M.S.; Odahowski, C.L.; Garcia, J.M. Differences in Mealtime Behaviors, Food Security, and Weight Concerns Between Neurotypical Youth and Youth with Autism Spectrum Disorder. Adv. Neurodev. Disord. 2024, 8, 262–270. [Google Scholar] [CrossRef]
- Sitar, M. Coming to the Table: A Literature Review of Child Eating Behavior in Children with Autism Spectrum Disorder (ASD); 2023. Available online: https://openresearch.okstate.edu/server/api/core/bitstreams/28072b1c-d0a8-4f8e-8346-8bda0854be2f/content (accessed on 31 March 2025).
- De Almeida, P.C.; Zandonadi, R.P.; Nakano, E.Y.; Vasconcelos, I.A.L.; Botelho, R.B.A. Food Neophobia in Children with Autistic Spectrum Disorder (ASD): A Nationwide Study in Brazil. Children 2022, 9, 1907. [Google Scholar] [CrossRef]
- Pérez-Cabral, I.D.; Bernal-Mercado, A.T.; Islas-Rubio, A.R.; Suárez-Jiménez, G.M.; Robles-García, M.Á.; Puebla-Duarte, A.L.; Del-Toro-Sánchez, C.L. Exploring Dietary Interventions in Autism Spectrum Disorder. Foods 2024, 13, 3010. [Google Scholar] [CrossRef]
- De Almeida, P.C.; Vasconcelos, I.A.L.; Nakano, E.Y.; Zandonadi, R.P.; Botelho, R.B.A. Food Neophobia: A Common Challenge Among Brazilian Children with Down Syndrome. Nutrients 2025, 17, 1199. [Google Scholar] [CrossRef]
- Smith, B.L.; Ludlow, A.K. An Exploration of Eating Behaviours and Caregiver Mealtime Actions of Children with Tourette Syndrome. Front. Pediatr. 2022, 10, 933154. [Google Scholar] [CrossRef]
- National Down Syndrome Society Gastrointestinal System and Down Syndrome. Available online: https://ndss.org/resources/gastrointestinal-tract-syndrome (accessed on 15 December 2024).
- Wang, L.; Shen, W.; Yao, H.; Zheng, R.; Chen, W.; Zhang, W. Association between Autism Spectrum Disorder and Food Allergy: A Systematic Review and Meta-Analysis. Autism Res. 2021, 14, 220–230. [Google Scholar] [CrossRef]
- Taylor, S.L.; Baumert, J.L. Food Allergies, Sensitivities, and Intolerances; Elsevier Inc.: Amsterdam, The Netherlands, 2020; Volume 2, ISBN 9780128184608. [Google Scholar]
- Muthukumar, J.; Selvasekaran, P.; Lokanadham, M.; Chidambaram, R. Food and Food Products Associated with Food Allergy and Food Intolerance—An Overview. Food Res. Int. 2020, 138, 109780. [Google Scholar] [CrossRef]
- Tuck, C.J.; Biesiekierski, J.R.; Schmid-Grendelmeier, P.; Pohl, D. Food Intolerances. Nutrients 2024, 54, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Elghoudi, A.; Narchi, H. Food Allergy in Children-the Current Status and the Way Forward. World J. Clin. Pediatr. 2022, 11, 253–269. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; Food and Agriculture Organization of the United Nations; UNICEF. Guidance for Monitoring Healthy Diets Globally; WHO: Geneva, Switzerland, 2024; ISBN 9789240094383. [Google Scholar]
- Brasil Guia Alimentar Para a População Brasileira Ministério Da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Guia Alimentar Para a População Brasileira/Ministério Da Saúde, Secretaria de Atenção à Saúde de Atenção Básica.—2. Ed., 1.; Brasília. 2014. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/guia_alimentar_populacao_brasileira_2ed.pdf (accessed on 31 March 2025).
- Del Campo, C.; Bouzas, C.; Tur, J.A. Risk Factors and Consequences of Food Neophobia and Pickiness in Children and Adolescents: A Systematic Review. Foods 2025, 14, 69. [Google Scholar] [CrossRef]
- The World Medical Association. Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects; The World Medical Association: Fortaleza, Brazil, 2013. [Google Scholar]
- Brasil Resolução No 466, de 12 de Dezembro de 2012. 2012. Available online: https://www.gov.br/conselho-nacional-de-saude/pt-br/acesso-a-informacao/atos-normativos/resolucoes/2012/resolucao-no-466.pdf/view (accessed on 1 March 2025).
- Etikan, I.; Alkassim, R.; Abubakar, S. Comparision of Snowball Sampling and Sequential Sampling Technique. Biom. Biostat. Int. J. 2016, 3, 55. [Google Scholar] [CrossRef]
- Diotaiuti, P.; Girelli, L.; Mancone, S.; Valente, G.; Bellizzi, F.; Misiti, F.; Cavicchiolo, E. Psychometric Properties and Measurement Invariance across Gender of the Italian Version of the Tempest Self-Regulation Questionnaire for Eating Adapted for Young Adults. Front. Psychol. 2022, 13, 941784. [Google Scholar] [CrossRef]
- Damsbo-Svendsen, M.; Frøst, M.B.; Olsen, A. Development of Novel Tools to Measure Food Neophobia in Children. Appetite 2017, 113, 255–263. [Google Scholar] [CrossRef]
- Hollar, D.; Paxton-Aiken, A.; Fleming, P. Exploratory Validation of the Fruit and Vegetable Neophobia Instrument among Third- to Fifth-Grade Students. Appetite 2013, 60, 226–230. [Google Scholar] [CrossRef]
- Allirot, X.; da Quinta, N.; Chokupermal, K.; Urdaneta, E. Involving Children in Cooking Activities: A Potential Strategy for Directing Food Choices toward Novel Foods Containing Vegetables. Appetite 2016, 103, 275–285. [Google Scholar] [CrossRef]
- Almeida, P.C. De Construção e Validação de Um Instrumento Para Avaliar a Neofobia Alimentar de Crianças Brasileiras. Master’s Thesis, Universidade de Brasília, Brasília, Brazil, 2020. [Google Scholar]
- Neofobia Alimentar @neofobiaalimentar. Available online: https://www.instagram.com/neofobiaalimentar/ (accessed on 15 November 2022).
- @Neofobiaalimentar Pesquisa Sobre Neofobia Alimentar. Available online: https://www.facebook.com/neofobia.alimentar (accessed on 15 November 2022).
- De Almeida, P.C.; Nakano, E.Y.; Vasconcelos, I.A.L.; Zandonadi, R.P.; Raposo, A.; Saraiva, A.; Alturki, H.A.; Botelho, R.B.A. Food Neophobia in Children: A Case Study in Federal District/Brazil. Nutrients 2024, 16, 2962. [Google Scholar] [CrossRef]
- Firme, J.N.; De Almeida, P.C.; Batistela, E.; Zandonadi, R.P.; Raposo, A.; Botelho, R.B.A. Instruments to Evaluate Food Neophobia in Children: An Integrative Review with a Systematic Approach. Nutrients 2023, 15, 4769. [Google Scholar] [CrossRef]
- Nocerino, R.; Mercuri, C.; Bosco, V.; Giordano, V.; Simeone, S.; Guillari, A.; Rea, T. Development and Management of Avoidant/Restrictive Food Intake Disorder and Food Neophobia in Pediatric Patients with Food Allergy: A Comprehensive Review. Nutrients 2024, 16, 3034. [Google Scholar] [CrossRef] [PubMed]
- Kotchetkoff, E.C.d.A.; de Oliveira, L.C.L.; Sarni, R.O.S. Elimination Diet in Food Allergy: Friend or Foe? J. Pediatr. 2024, 100, S65–S73. [Google Scholar] [CrossRef] [PubMed]
- Firme, J.N.; dos Santos, E.B.; Zandonadi, R.P.; Nakano, E.Y.; Botelho, R.B.A. Dietary Challenges in Children with Gluten-Related Disorders: A Study on Food Neophobia. Nutrients 2024, 16, 3924. [Google Scholar] [CrossRef]
- D’Auria, E.; Cattaneo, C.; Panelli, S.; Pozzi, C.; Acunzo, M.; Papaleo, S.; Comandatore, F.; Mameli, C.; Bandi, C.; Zuccotti, G.; et al. Alteration of Taste Perception, Food Neophobia and Oral Microbiota Composition in Children with Food Allergy. Sci. Rep. 2023, 13, 7010. [Google Scholar] [CrossRef]
- Rodrigues, J.V.S.; Poli, M.C.F.; Petrilli, P.H.; Dornelles, R.C.M.; Turcio, K.H.; Theodoro, L.H. Food Selectivity and Neophobia in Children with Autism Spectrum Disorder and Neurotypical Development: A Systematic Review. Nutr. Rev. 2023, 81, 1034–1050. [Google Scholar] [CrossRef]
- Xie, Q.; Yong, C.; Xiang, C.; Xi, Y.; Huo, J.; Liang, J.; Zou, H.; Pan, Y.; Wu, M.; Lin, Q. The Impact of Caregiver Pressure to Eat on Food Neophobia in Children with Autism Spectrum Disorder: A Cross-Sectional Study. Children 2024, 11, 528. [Google Scholar] [CrossRef]
- Smith, B.; Rogers, S.L.; Blissett, J.; Ludlow, A.K. The Relationship between Sensory Sensitivity, Food Fussiness and Food Preferences in Children with Neurodevelopmental Disorders. Appetite 2020, 150, 104643. [Google Scholar] [CrossRef]
- Hazley, D.; Stack, M.; Walton, J.; McNulty, B.A.; Kearney, J.M. Food Neophobia across the Life Course: Pooling Data from Five National Cross-Sectional Surveys in Ireland. Appetite 2022, 171, 105941. [Google Scholar] [CrossRef]
- Alley, T.R. Conceptualization and Measurement of Human Food Neophobia. In Food neophobia; Elsevier: Amsterdam, The Netherlands, 2018; pp. 169–192. [Google Scholar]
| Food Neophobia | |||
|---|---|---|---|
| Low n (%) | Moderate n (%) | High n (%) | |
| Domain of neophobia in general * (FNgen) | 516 (21.6%) | 672 (28.2%) | 1199 (50.2%) |
| Domain of neophobia for fruits * (FNfru) | 760 (31.8%) | 698 (29.2%) | 929 (38.9%) |
| Domain of neophobia for vegetables * (FNveg) | 535 (22.4%) | 655 (27.4%) | 1197 (50.1%) |
| TOTAL INSTRUMENT SCORE ** (BCFNeoTot) | 575 (24.1%) | 756 (31.7%) | 1056 (44.2%) |
| Gender | Age | |||||
|---|---|---|---|---|---|---|
| Girls (n = 1009) | Boys (n = 1378) | p | 4–7 y (n = 1430) | 8–11 y (n = 957) | p | |
| General neophobia (FNgen) | ||||||
| Score; Mean ± SD | 19.22 ± 8.69 | 21.93 ± 8.68 | <0.001 * | 20.67 ± 8.67 | 20.95 ± 8.95 | 0.452 * |
| Distribution; n (%) | ||||||
| Low (up to 13) | 262 (26.0%) | 254 (18.4%) | 307 (21.5%) | 209 (21.8%) | ||
| Moderate (14 to 21) | 324 (32.1%) | 348 (25.3%) | <0.001 ** | 416 (29.1%) | 256 (26.8%) | 0.539 ** |
| High (22 or more) | 423 (41.9%) | 776 (56.3%) | 707 (49.4%) | 492 (51.4%) | ||
| Fruit neophobia (FNfru) | ||||||
| Score; Mean ± SD | 16.28 ± 8.45 | 19.10 ± 8.68 | <0.001 * | 17.85 ±8.67 | 18.00 ± 8.74 | 0.675 * |
| Distribution; n (%) | ||||||
| Low (up to 13) | 386 (38.3%) | 374 (27.1%) | 459 (32.1%) | 301 (31.5%) | ||
| Moderate (14 to 21) | 321 (31.8%) | 377 (27.4%) | <0.001 ** | 419 (29.3%) | 279 (29.2%) | 0.680 ** |
| High (22 or more) | 302 (29.9%) | 627 (45.5%) | 552 (38.6%) | 377 (39.4%) | ||
| Vegetable Neophobia (FNveg) | ||||||
| Score; Mean ± SD | 18.95 ± 8.27 | 21.32 ± 8.30 | <0.001 * | 20.30 ±8.38 | 20.35 ± 8.36 | 0.877 * |
| Distribution; n (%) | ||||||
| Low (up to 13) | 273 (27.1%) | 262 (19.0%) | 317 (22.2%) | 218 (22.8%) | ||
| Moderate (14 to 21) | 302 (29.9%) | 353 (25.6%) | <0.001 ** | 399 (27.9%) | 256 (26.8%) | 0.959 ** |
| High (22 or more) | 434 (43.0%) | 763 (55.4%) | 714 (49.9%) | 483 (50.5%) | ||
| TOTAL (BCFNeoTot) | ||||||
| Score; Mean ± SD | 54.45 ± 23.77 | 62.35 ± 24.11 | <0.001 * | 58.82 ±24.2 | 59.30 ± 24.39 | 0.634 * |
| Distribution; n (%) | ||||||
| Low (up to 40) | 281 (27.8%) | 294 (21.3%) | 353 (24.7%) | 222 (23.2%) | ||
| Moderate (41 to 65) | 371 (36.8%) | 385 (27.9%) | <0.001 ** | 454 (31.7%) | 302 (31.6%) | 0.349 ** |
| High (66 or more) | 357 (35.4%) | 699 (50.7%) | 623 (43.6%) | 433 (45.2%) | ||
| G1 (n = 767) | G2 (n = 133) | G3 (n = 126) | G4 (n = 1361) | p | |
|---|---|---|---|---|---|
| General neophobia (FNgen) | |||||
| Score; Mean ± SD | 23.86 ± 8.21 b | 23.38 ± 8.38 b | 18.16 ± 9.37 a | 19.03 ± 8.53 a | <0.001 * |
| Distribution; n (%) | |||||
| Low (up to 13) | 100 (13.0%) | 15 (11.3%) | 42 (33.3%) | 359 (26.4%) | |
| Moderate (14 to 21) | 149 (19.4%) b | 36 (27.1%) b | 31 (24.6%) a | 456 (33.5%) a | <0.001 ** |
| High (22 or more) | 518 (67.5%) | 82 (61.7%) | 53 (42.1%) | 546 (40.1%) | |
| Fruit neophobia (FNfru) | |||||
| Score; Mean ± SD | 21.32 ± 8.15 b | 21.37 ± 8.24 a | 15.03 ± 8.40 a | 15.92 ± 8.35 a | <0.001 * |
| Distribution; n (%) | |||||
| Low (up to 13) | 138 (18.0%) | 21 (15.8%) | 55 (43.7%) | 546 (40.1%) | |
| Moderate (14 to 21) | 199 (25.9%) b | 43 (32.3%) b | 40 (31.7%) a | 416 (30.6%) a | <0.001 ** |
| High (22 or more) | 430 (56.1%) | 69 (51.9%) | 31 (24.6%) | 399 (29.3%) | |
| Vegetable Neophobia (FNveg) | |||||
| Score; Mean ± SD | 22.89 ± 8.17 b | 22.39 ± 8.75 b | 17.75 ± 8.33 a | 18.91 ± 8.04 a | <0.001 * |
| Distribution; n (%) | |||||
| Low (up to 13) | 108 (14.1%) | 24 (18.0%) | 45 (35.7%) | 358 (26.3%) | |
| Moderate (14 to 21) | 168 (21.9%) b | 25 (18.8%) b | 35 (27.8%) a | 427 (31.4%) a | <0.001 ** |
| High (22 or more) | 491 (64.0%) | 84 (63.2%) | 46 (36.5%) | 576 (42.3%) | |
| TOTAL (BCFNeoTot) | |||||
| Score; Mean ± SD | 68.07 ± 22.90 b | 67.14 ± 23.47 b | 50.94 ± 24.98 a | 53.86 ± 23.28 a | <0.001 * |
| Distribution; n (%) | |||||
| Low (up to 40) | 107 (14.0%) | 17 (12.8%) | 50 (39.7%) | 401 (29.5%) | |
| Moderate (41 to 65) | 178 (23.2%) b | 33 (24.8%) b | 39 (31.0%) a | 506 (37.2%) a | <0.001 ** |
| High (66 or more) | 482 (62.8%) | 83 (62.4%) | 37 (29.4%) | 454 (33.4%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Almeida, P.C.; Freire, N.F.; Oliveira, L.L.d.; Nakano, E.Y.; Vasconcelos, I.A.L.; Zandonadi, R.P.; Botelho, R.B.A. Food Neophobia in Brazilian Children: A Nationwide Cross-Sectional Study Comparing Neurodivergent and Neurotypical Children with and Without Dietary Restrictions. Nutrients 2025, 17, 1327. https://doi.org/10.3390/nu17081327
De Almeida PC, Freire NF, Oliveira LLd, Nakano EY, Vasconcelos IAL, Zandonadi RP, Botelho RBA. Food Neophobia in Brazilian Children: A Nationwide Cross-Sectional Study Comparing Neurodivergent and Neurotypical Children with and Without Dietary Restrictions. Nutrients. 2025; 17(8):1327. https://doi.org/10.3390/nu17081327
Chicago/Turabian StyleDe Almeida, Priscila Claudino, Nathália França Freire, Letícia Leal de Oliveira, Eduardo Yoshio Nakano, Ivana Aragão Lira Vasconcelos, Renata Puppin Zandonadi, and Raquel Braz Assunção Botelho. 2025. "Food Neophobia in Brazilian Children: A Nationwide Cross-Sectional Study Comparing Neurodivergent and Neurotypical Children with and Without Dietary Restrictions" Nutrients 17, no. 8: 1327. https://doi.org/10.3390/nu17081327
APA StyleDe Almeida, P. C., Freire, N. F., Oliveira, L. L. d., Nakano, E. Y., Vasconcelos, I. A. L., Zandonadi, R. P., & Botelho, R. B. A. (2025). Food Neophobia in Brazilian Children: A Nationwide Cross-Sectional Study Comparing Neurodivergent and Neurotypical Children with and Without Dietary Restrictions. Nutrients, 17(8), 1327. https://doi.org/10.3390/nu17081327