
Copper, Zinc, and Selenium Levels During Pregnancy and Their Relationship with Pre-Eclampsia Risk: A Systematic Review
 , ,
, ,  ,
,
Abstract
1. Introduction
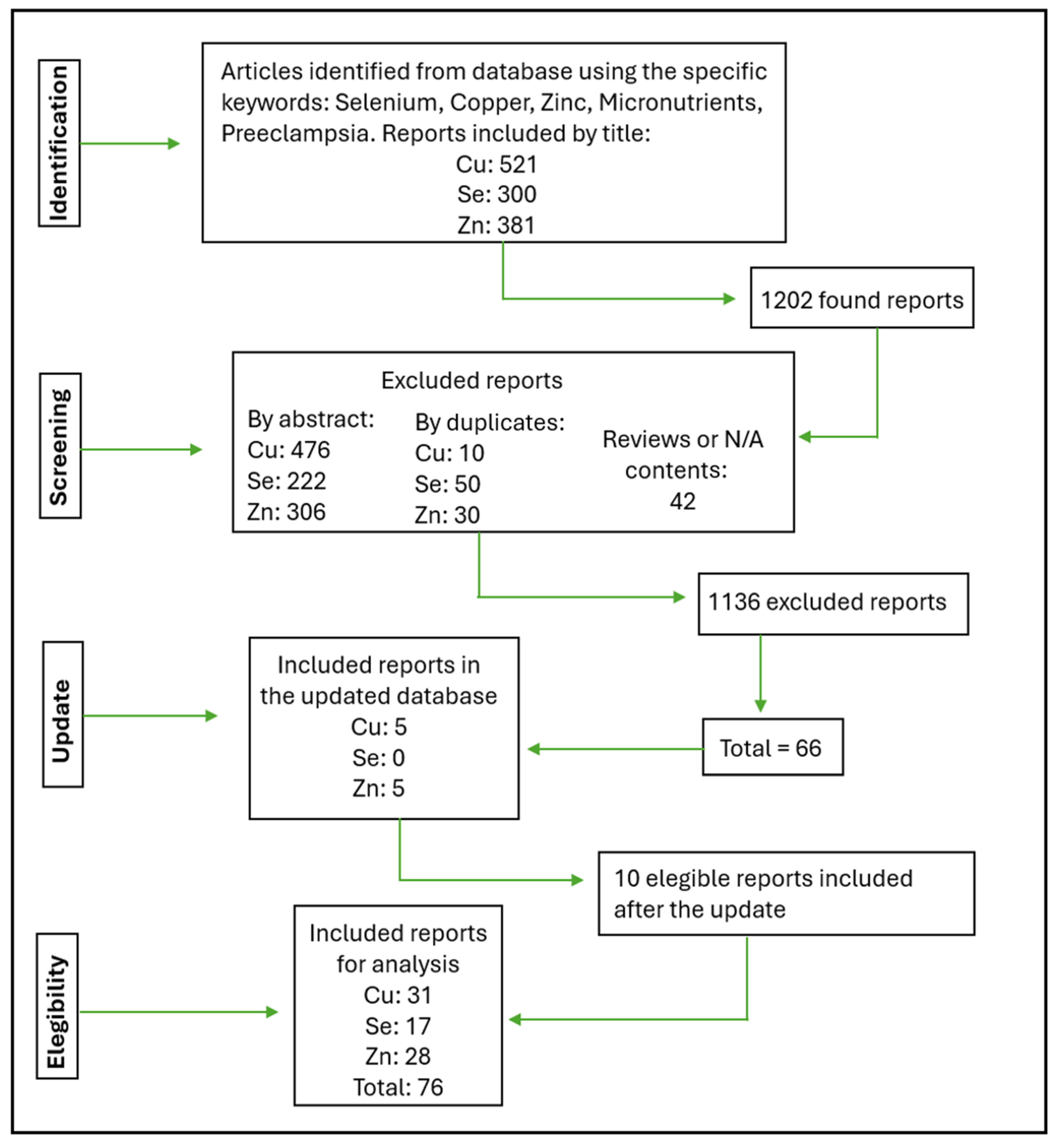
2. Materials and Methods
3. Results and Discussion
4. Conclusions
Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jiang, T.; Christian, P.; Khatry, S.K.; Wu, L.; West, K.P. Micronutrient Deficiencies in Early Pregnancy Are Common, Concurrent, and Vary by Season among Rural Nepali Pregnant Women. J. Nutr. 2005, 135, 1106–1112. [Google Scholar] [CrossRef]
- WHO Antenatal Care Recommendations for a Positive Pregnancy Experience. Nutritional Interventions Update: Multiple Micronutrient Supplements During Pregnancy, 1st ed.; World Health Organization: Geneva, Switzerland, 2020; ISBN 978-92-4-000778-9.
- Salam, R.A.; Zuberi, N.F.; Bhutta, Z.A. Pyridoxine (Vitamin B6) Supplementation during Pregnancy or Labour for Maternal and Neonatal Outcomes. Cochrane Database Syst. Rev. 2015, 6, CD000179. [Google Scholar] [CrossRef] [PubMed]
- Darnton-Hill, I.; Mkparu, U. Micronutrients in Pregnancy in Low- and Middle-Income Countries. Nutrients 2015, 7, 1744–1768. [Google Scholar] [CrossRef]
- Poon, L.C.; Shennan, A.; Hyett, J.A.; Kapur, A.; Hadar, E.; Divakar, H.; McAuliffe, F.; Da Silva Costa, F.; Von Dadelszen, P.; McIntyre, H.D.; et al. The International Federation of Gynecology and Obstetrics (FIGO) Initiative on Pre-eclampsia: A Pragmatic Guide for First-trimester Screening and Prevention. Int. J. Gynecol. Obstet. 2019, 145, 1–33. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.M. Preeclampsia Epidemiology(Ies) and Pathophysiology(Ies). Best Pract. Res. Clin. Obstet. Gynaecol. 2024, 94, 102480. [Google Scholar] [CrossRef] [PubMed]
- Jung, E.; Romero, R.; Yeo, L.; Gomez-Lopez, N.; Chaemsaithong, P.; Jaovisidha, A.; Gotsch, F.; Erez, O. The Etiology of Preeclampsia. Am. J. Obstet. Gynecol. 2022, 226, S844–S866. [Google Scholar] [CrossRef]
- Farhat, G.; Lees, E.; Macdonald-Clarke, C.; Amirabdollahian, F. Inadequacies of Micronutrient Intake in Normal Weight and Overweight Young Adults Aged 18-25 Years: A Cross-Sectional Study. Public Health 2019, 167, 70–77. [Google Scholar] [CrossRef]
- Park-Wyllie, L.; Mazzotta, P.; Pastuszak, A.; Moretti, M.E.; Beique, L.; Hunnisett, L.; Friesen, M.H.; Jacobson, S.; Kasapinovic, S.; Chang, D.; et al. Birth Defects after Maternal Exposure to Corticosteroids: Prospective Cohort Study and Meta-Analysis of Epidemiological Studies. Teratology 2000, 62, 385–392. [Google Scholar] [CrossRef]
- Duan, S.; Jiang, Y.; Mou, K.; Wang, Y.; Zhou, S.; Sun, B. Correlation of Serum Vitamin A and Vitamin E Levels with the Occurrence and Severity of Preeclampsia. Am. J. Transl. Res. 2021, 13, 14203–14210. [Google Scholar]
- Kiondo, P.; Wamuyu-Maina, G.; Wandabwa, J.; Bimenya, G.S.; Tumwesigye, N.M.; Okong, P. The Effects of Vitamin C Supplementation on Pre-Eclampsia in Mulago Hospital, Kampala, Uganda: A Randomized Placebo Controlled Clinical Trial. BMC Pregnancy Childbirth 2014, 14, 283. [Google Scholar] [CrossRef]
- Fogacci, S.; Fogacci, F.; Banach, M.; Michos, E.D.; Hernandez, A.V.; Lip, G.Y.H.; Blaha, M.J.; Toth, P.P.; Borghi, C.; Cicero, A.F.G.; et al. Vitamin D Supplementation and Incident Preeclampsia: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Clin. Nutr. Edinb. Scotl. 2020, 39, 1742–1752. [Google Scholar] [CrossRef] [PubMed]
- Ushida, T.; Tano, S.; Matsuo, S.; Fuma, K.; Imai, K.; Kajiyama, H.; Kotani, T. Dietary Supplements and Prevention of Preeclampsia. Hypertens. Res. 2025, 1–14. [Google Scholar] [CrossRef]
- Khaing, W.; Vallibhakara, S.A.-O.; Tantrakul, V.; Vallibhakara, O.; Rattanasiri, S.; McEvoy, M.; Attia, J.; Thakkinstian, A. Calcium and Vitamin D Supplementation for Prevention of Preeclampsia: A Systematic Review and Network Meta-Analysis. Nutrients 2017, 9, 1141. [Google Scholar] [CrossRef]
- Andreini, C.; Banci, L.; Bertini, I.; Rosato, A. Zinc through the Three Domains of Life. J. Proteome Res. 2006, 5, 3173–3178. [Google Scholar] [CrossRef] [PubMed]
- Kambe, T.; Tsuji, T.; Hashimoto, A.; Itsumura, N. The Physiological, Biochemical, and Molecular Roles of Zinc Transporters in Zinc Homeostasis and Metabolism. Physiol. Rev. 2015, 95, 749–784. [Google Scholar] [CrossRef] [PubMed]
- Portbury, S.; Adlard, P. Zinc Signal in Brain Diseases. Int. J. Mol. Sci. 2017, 18, 2506. [Google Scholar] [CrossRef]
- Younus, H. Therapeutic Potentials of Superoxide Dismutase. Int. J. Health Sci. 2018, 12, 88–93. [Google Scholar]
- Yu, C.; Wang, P.; Li, S.; Wang, X.; Yu, Z.; Wang, Z. The Protective Effect of Cu/Zn-SOD against Oxidative Stress after PTEN Deletion. Cancer Investig. 2011, 29, 253–256. [Google Scholar] [CrossRef]
- Ratn, A.; Prasad, R.; Awasthi, Y.; Kumar, M.; Misra, A.; Trivedi, S.P. Zn2+ Induced Molecular Responses Associated with Oxidative Stress, DNA Damage and Histopathological Lesions in Liver and Kidney of the Fish, Channa Punctatus (Bloch, 1793). Ecotoxicol. Environ. Saf. 2018, 151, 10–20. [Google Scholar] [CrossRef]
- Da Silva, A.C.; Martins-Costa, S.H.; Valério, E.G.; Lopes Ramos, J.G. Comparison of Serum Selenium Levels among Hypertensive and Normotensive Pregnant Women. Hypertens. Pregnancy 2017, 36, 64–69. [Google Scholar] [CrossRef]
- Vanderlelie, J.; Perkins, A.V.A. Selenium and Preeclampsia: A Global Perspective. Pregnancy Hypertens. 2011, 1, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Mistry, H.D.; Williams, P.J. The Importance of Antioxidant Micronutrients in Pregnancy. Oxid. Med. Cell. Longev. 2011, 2011, 841749. [Google Scholar] [CrossRef] [PubMed]
- Lewandowska, M.; Sajdak, S.; Lubiński, J. Serum Selenium Level in Early Healthy Pregnancy as a Risk Marker of Pregnancy Induced Hypertension. Nutrients 2019, 11, 1028. [Google Scholar] [CrossRef] [PubMed]
- Ghaemi, S.Z.; Forouhari, S.; Dabbaghmanesh, M.H.; Sayadi, M.; Bakhshayeshkaram, M.; Vaziri, F.; Tavana, Z. A Prospective Study of Selenium Concentration and Risk of Preeclampsia in Pregnant Iranian Women: A Nested Case–Control Study. Biol. Trace Elem. Res. 2013, 152, 174–179. [Google Scholar] [CrossRef]
- Eze, S.C.; Ododo, N.A.; Ugwu, E.O.; Enebe, J.T.; Onyegbule, O.A.; Eze, I.O.; Ezem, B.U. Serum Selenium Levels of Pre-Eclamptic and Normal Pregnant Women in Nigeria: A Comparative Study. PLoS ONE 2020, 15, e0238263. [Google Scholar] [CrossRef]
- Enebe, J.T.; Dim, C.C.; Ugwu, E.O.; Enebe, N.O.; Meka, I.A.; Obioha, K.C.; Eleje, G.U.; Nwagha, U.I. Serum Antioxidant Micronutrient Levels in Pre-Eclamptic Pregnant Women in Enugu, South-East Nigeria: A Comparative Cross-Sectional Analytical Study. BMC Pregnancy Childbirth 2020, 20, 392. [Google Scholar] [CrossRef]
- Rayman, M.P.; Bode, P.; Redman, C.W.G. Low Selenium Status Is Associated with the Occurrence of the Pregnancy Disease Preeclampsia in Women from the United Kingdom. Am. J. Obstet. Gynecol. 2003, 189, 1343–1349. [Google Scholar] [CrossRef]
- Negi, R.; Pande, D.; Karki, K.; Kumar, A.; Khanna, R.S.; Khanna, H.D. Trace Elements and Antioxidant Enzymes Associated with Oxidative Stress in the Pre-Eclamptic/Eclamptic Mothers during Fetal Circulation. Clin. Nutr. 2012, 31, 946–950. [Google Scholar] [CrossRef]
- Zanette, E.; Parpinelli, M.A.; Surita, F.G.; Costa, M.L.; Haddad, S.M.; Sousa, M.H.; Silva, J.L.P.E.; Souza, J.P.; Cecatti, J.G. Brazilian Network for Surveillance of Severe Maternal Morbidity Group Maternal near Miss and Death among Women with Severe Hypertensive Disorders: A Brazilian Multicenter Surveillance Study. Reprod. Health 2014, 11, 4. [Google Scholar] [CrossRef]
- Schaefer, E. Micronutrient Deficiency in Women Living in Industrialized Countries During the Reproductive Years: Is There a Basis for Supplementation with Multiple Micronutrients? J. Nutr. Disord. Ther. 2016, 6, 199. [Google Scholar] [CrossRef]
- Araùjo Brito, J.; Nascimento Marreiro, D.D.; Machado Moita Neto, J.; Michelle Costa e Silva, D.; Gonçalves de Sousa Almondes, K.; Valadares Neto, J.D.; Nascimento Nogueira, N.D. LA ACTIVIDAD FÍSICA DE LA ENZIMA SUPERÓXIDO DISMUTASA Y ZINCEMIA EN. Nutr. Hosp. 2013, 28, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Wibowo, N.; Kurniawan, R.H.; Irwinda, R.; Prameswari, N. Maternal and Cord Blood Cyclophilin A in Severe Preeclampsia and Normal Pregnancy and Its Correlation with Vitamin D and Zinc. Hypertens. Pregnancy 2017, 36, 283–287. [Google Scholar] [CrossRef]
- Bahadoran, P.; Zendehdel, M.; Movahedian, A.; Zahraee, R.H. The Relationship between Serum Zinc Level and Preeclampsia. Iran. J. Nurs. Midwifery Res. 2010, 15, 120–124. [Google Scholar] [PubMed]
- Yusrawati; Saputra, N.P.K.; Lipoeto, N.I.; Machmud, R. Analyses of Nutrients and Body Mass Index as Risk Factor for Preeclampsia. J. Obstet. Gynaecol. India 2017, 67, 409–413. [Google Scholar] [CrossRef]
- Serdar, Z.; Gür, E.; Develioğlu, O. Serum Iron and Copper Status and Oxidative Stress in Severe and Mild Preeclampsia. Cell Biochem. Funct. 2006, 24, 209–215. [Google Scholar] [CrossRef]
- Al-Jameil, N.; Tabassum, H.; Al-Mayouf, H.; Aljohar, H.I.; Alenzi, N.D.; Hijazy, S.M.; Khan, F.A. Analysis of Serum Trace Elements-Copper, Manganese and Zinc in Preeclamptic Pregnant Women by Inductively Coupled Plasma Optical Emission Spectrometry: A Prospective Case Controlled Study in Riyadh, Saudi Arabia. Int. J. Clin. Exp. Pathol. 2014, 7, 1900–1910. [Google Scholar] [PubMed]
- Polat, M.; Biberoğlu, E.H.; Güler, İ.; Biberoğlu, Ö.K. Coexistence of Preeclampsia and Inherited Thrombophilia in Turkish Pregnant Women. Turk. J. Med. Sci. 2016, 46, 1094–1100. [Google Scholar] [CrossRef]
- Kashanian, M.; Hadizadeh, H.; Faghankhani, M.; Nazemi, M.; Sheikhansari, N. Evaluating the Effects of Copper Supplement during Pregnancy on Premature Rupture of Membranes and Pregnancy Outcome. J. Matern.-Fetal Neonatal Med. Off. J. Eur. Assoc. Perinat. Med. Fed. Asia Ocean. Perinat. Soc. Int. Soc. Perinat. Obstet. 2018, 31, 39–46. [Google Scholar] [CrossRef]
- Sak, S.; Barut, M.; Çelik, H.; Incebiyik, A.; Ağaçayak, E.; Uyanikoglu, H.; Kirmit, A.; Sak, M. Copper and Ceruloplasmin Levels Are Closely Related to the Severity of Preeclampsia. J. Matern. Fetal Neonatal Med. 2020, 33, 96–102. [Google Scholar] [CrossRef]
- Monia, M.-M.; Fethi, B.A.; Wafa, L.-B.A.; Hédi, R. Status of Zinc and Copper in Pregnant Women and Their Changes during Preeclampsia. Ann. Biol. Clin. (Paris) 2012, 70, 423–429. [Google Scholar] [CrossRef]
- Haque, M.d.M.; Moghal, M.d.M.R.; Sarwar, M.d.S.; Anonna, S.N.; Akter, M.; Karmakar, P.; Ahmed, S.; Sattar, M.; Islam, M.S. Low Serum Selenium Concentration Is Associated with Preeclampsia in Pregnant Women from Bangladesh. J. Trace Elem. Med. Biol. 2016, 33, 21–25. [Google Scholar] [CrossRef]
- Harma, M.; Harma, M.; Kocyigit, A. Correlation Between Maternal Plasma Homocysteine and Zinc Levels in Preeclamptic Women. Biol. Trace Elem. Res. 2005, 104, 097–106. [Google Scholar] [CrossRef] [PubMed]
- Açikgoz, S.; Harma, M.; Harma, M.; Mungan, G.; Can, M.; Demirtas, S. Comparison of Angiotensin-Converting Enzyme, Malonaldehyde, Zinc, and Copper Levels in Preeclampsia. Biol. Trace Elem. Res. 2006, 113, 1–8. [Google Scholar] [CrossRef]
- Fenzl, V.; Flegar-Meštrić, Z.; Perkov, S.; Andrišić, L.; Tatzber, F.; Žarković, N.; Duić, Ž. Trace Elements and Oxidative Stress in Hypertensive Disorders of Pregnancy. Arch. Gynecol. Obstet. 2013, 287, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Bakacak, M.; Kılınç, M.; Serin, S.; Ercan, Ö.; Köstü, B.; Avcı, F.; Kıran, H.; Kıran, G. Changes in Copper, Zinc, and Malondialdehyde Levels and Superoxide Dismutase Activities in Pre-Eclamptic Pregnancies. Med. Sci. Monit. 2015, 21, 2414–2420. [Google Scholar] [CrossRef] [PubMed]
- Elmugabil, A.; Hamdan, H.Z.; Elsheikh, A.E.; Rayis, D.A.; Adam, I.; Gasim, G.I. Serum Calcium, Magnesium, Zinc and Copper Levels in Sudanese Women with Preeclampsia. PLoS ONE 2016, 11, e0167495. [Google Scholar] [CrossRef]
- Al-Shalah, H.H.; Al-Hilli, N.M.; Hasan, M.A. The Association of Serum Iron, Zinc, and Copper Levels with Preeclampsia. Med. J. Babylon 2015, 12, 1027–1036. [Google Scholar]
- Ilhan, N.; Ilhan, N.; Simsek, M. The Changes of Trace Elements, Malondialdehyde Levels and Superoxide Dismutase Activities in Pregnancy with or without Preeclampsia. Clin. Biochem. 2002, 35, 393–397. [Google Scholar] [CrossRef]
- Rafeeinia, A.; Tabandeh, A.; Khajeniazi, S.; Marjani, A.J. Serum Copper, Zinc and Lipid Peroxidation in Pregnant Women with Preeclampsia in Gorgan. Open Biochem. J. 2014, 8, 83–88. [Google Scholar] [CrossRef]
- Onyegbule, A.O.; Onah, C.; Iheukwumere, B.; Udo, J.; Atuegbu, C.; Nosakhare, N. Serum Copper and Zinc Levels in Preeclamptic Nigerian Women. Niger. Med. J. 2016, 57, 182. [Google Scholar] [CrossRef]
- Keshavarz, P.; Nobakht, M.; Gh, B.F.; Mirhafez, S.R.; Nematy, M.; Azimi-Nezhad, M.; Afin, S.A.; Esmaily, H.; Pourali, L.; Hakak, A.M.; et al. Alterations in Lipid Profile, Zinc and Copper Levels and Superoxide Dismutase Activities in Normal Pregnancy and Preeclampsia. Am. J. Med. Sci. 2017, 353, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Abo-Elmatty, D.M.; Badawy, E.A.; Hussein, J.S.; Elela, S.A.; Megahed, H.A. Role of Heme Oxygenase, Leptin, Coenzyme Q10 and Trace Elements in Pre-Eclamptic Women. Indian J. Clin. Biochem. 2012, 27, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, M.S.; Ahmed, S.; Ullah, M.S.; Kabir, H.; Rahman, G.K.M.M.; Hasnat, A.; Islam, M.S. Comparative Study of Serum Zinc, Copper, Manganese, and Iron in Preeclamptic Pregnant Women. Biol. Trace Elem. Res. 2013, 154, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Jamal, B. To Determine the Effects of Copper, Zinc and Magnesium in Patients with Pre-Eclampsia. J. Liaquat Univ. Med. Health Sci. 2017, 16, 53–57. [Google Scholar] [CrossRef]
- Gul, A.Z.; Atakul, N.; Selek, S.; Atamer, Y.; Sarıkaya, U.; Yıldız, T.; Demirel, M. Maternal Serum Levels of Zinc, Copper, and Thiols in Preeclampsia Patients: A Case-Control Study. Biol. Trace Elem. Res. 2022, 200, 464–472. [Google Scholar] [CrossRef]
- Kim, J.; Kim, Y.J.; Lee, R.; Moon, J.H.; Jo, I. Serum Levels of Zinc, Calcium, and Iron Are Associated with the Risk of Preeclampsia in Pregnant Women. Nutr. Res. 2012, 32, 764–769. [Google Scholar] [CrossRef]
- Maduray, K.; Moodley, J.; Soobramoney, C.; Moodley, R.; Naicker, T. Elemental Analysis of Serum and Hair from Pre-Eclamptic South African Women. J. Trace Elem. Med. Biol. 2017, 43, 180–186. [Google Scholar] [CrossRef]
- Maleki, A.; Fard, M.K.; Zadeh, D.H.; Mamegani, M.A.; Abasaizadeh, S.; Mazloomzadeh, S. The Relationship between Plasma Level of Se and Preeclampsia. Hypertens. Pregnancy 2011, 30, 180–187. [Google Scholar] [CrossRef]
- Mistry, H.D.; Gill, C.A.; Kurlak, L.O.; Seed, P.T.; Hesketh, J.E.; Méplan, C.; Schomburg, L.; Chappell, L.C.; Morgan, L.; Poston, L. Association between Maternal Micronutrient Status, Oxidative Stress, and Common Genetic Variants in Antioxidant Enzymes at 15 Weeks’ Gestation in Nulliparous Women Who Subsequently Develop Preeclampsia. Free Radic. Biol. Med. 2015, 78, 147–155. [Google Scholar] [CrossRef]
- Basu, A.; Yu, J.Y.; Jenkins, A.J.; Nankervis, A.J.; Hanssen, K.F.; Henriksen, T.; Lorentzen, B.; Garg, S.K.; Menard, M.K.; Hammad, S.M.; et al. Trace Elements as Predictors of Preeclampsia in Type 1 Diabetic Pregnancy. Nutr. Res. 2015, 35, 421–430. [Google Scholar] [CrossRef]
- Choi, R.; Sun, J.; Yoo, H.; Kim, S.; Cho, Y.; Kim, H.; Kim, S.; Chung, J.; Oh, S.; Lee, S.-Y. A Prospective Study of Serum Trace Elements in Healthy Korean Pregnant Women. Nutrients 2016, 8, 749. [Google Scholar] [CrossRef]
- Katz, O.; Paz-Tal, O.; Lazer, T.; Aricha-Tamir, B.; Mazor, M.; Wiznitzer, A.; Sheiner, E. Severe Pre-Eclampsia Is Associated with Abnormal Trace Elements Concentrations in Maternal and Fetal Blood. J. Matern. Fetal Neonatal Med. 2012, 25, 1127–1130. [Google Scholar] [CrossRef] [PubMed]
- Atamer, Y.; Koçyigit, Y.; Yokus, B.; Atamer, A.; Erden, A.C. Lipid Peroxidation, Antioxidant Defense, Status of Trace Metals and Leptin Levels in Preeclampsia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 119, 60–66. [Google Scholar] [CrossRef]
- Farzin, L.; Sajadi, F. Comparison of Serum Trace Element Levels in Patients with or without Pre-Eclampsia. J. Res. Med. Sci. 2012, 17, 938–941. [Google Scholar] [PubMed]
- Kolusari, A.; Kurdoglu, M.; Yildizhan, R.; Adali, E.; Edirne, T.; Cebi, A.; Demir, H.; Yoruk, I. Catalase Activity, Serum Trace Element and Heavy Metal Concentrations, and Vitamin A, D and E Levels in Pre-Eclampsia. J. Int. Med. Res. 2008, 36, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Rezende, V.B.; Barbosa, F.; Palei, A.C.; Cavalli, R.C.; Tanus-Santos, J.E.; Sandrim, V.C. Correlations among Antiangiogenic Factors and Trace Elements in Hypertensive Disorders of Pregnancy. J. Trace Elem. Med. Biol. 2015, 29, 130–135. [Google Scholar] [CrossRef]
- Walker, L.R.; Rattigan, M.; Canterino, J. A Case of Isolated Elevated Copper Levels during Pregnancy. J. Pregnancy 2011, 2011, 385767. [Google Scholar] [CrossRef]
- Abbassi-Ghanavati, M.; Greer, L.G.; Cunningham, F.G. Pregnancy and Laboratory Studies: A Reference Table for Clinicians. Obstet. Gynecol. 2009, 114, 1326–1331. [Google Scholar] [CrossRef]
- Roberts, E.A.; Schilsky, M.L. Diagnosis and Treatment of Wilson Disease: An Update. Hepatology 2008, 47, 2089–2111. [Google Scholar] [CrossRef]
- Lensen, S. When to Pool Data in a Meta-Analysis (and When Not To)? Fertil. Steril. 2023, 119, 902–903. [Google Scholar] [CrossRef]
- Huang, T.; Lu, F. Genetically Predicted Circulating Concentrations of Micronutrients and Risk of Hypertensive Disorders of Pregnancy: A Mendelian Randomization Study. Arch. Gynecol. Obstet. 2024, 310, 1019–1025. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Micronutrient (n Manuscripts) | References |
|---|---|
| Zn (4) | [32,33,34,35] |
| Cu (6) | [36,37,38,39,40,41] |
| Se (6) | [21,24,25,26,28,42] |
| Zn and Cu (15) | [29,43,44,45,46,47,48,49,50,51,52,53,54,55,56] |
| Zn and Se (2) | [57,58] |
| Cu and Se (3) | [59,60,61] |
| Cu, Zn, and Se (6) | [27,29,62,63,64,65] |
| Reference | Study Type | Patients (n) | Age Group | Time of Measurement | Comorbidities | Outcomes | Quality | Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| [49] | Case–control study | 30 PN 21 PE | PN and PE: 19–31 median 25 | 31st to 38th weeks of gestation | No comorbidities described in the study, besides hypertension | Cu (μg/dL) PN: 158.15 ± 27.86 PE: 176.73 ± 25.91 |  | |
| [64] | Cross-sectional prospective study | 28 PN 32 PE | PN: 25.85 ± 3.36 PE: 27.00 ± 3.89 | PN: 36.53 ± 3.15 weeks PE: 35.68 ± 2.94 weeks | No comorbidities described in the study, besides hypertension | Cu (mg/L) PN: 1.458 ± 0.396 PE: 2.612 ± 0.472 that corresponds to Cu (μg/dL) PN: 1–45.8 ± 39.6 PE: 261.2 ± 47.2 |  | |
| [36] | Cohort study | 30 PN 30 Mild PE 30 Severe PE | PN: 27 ± 4.1 Mild PE: 25 ± 2.3 Severe PE: 26 ± 1.9 | 31st to 38th weeks of pregnancy. | No comorbidities described in the study, besides hypertension | Cu (μg/dL) PN: 159 ± 38 Mild PE: 188 ± 48 Severe PE: 192 ± 52 | | |
| [44] | Cohort study | 20 PN 17 PE | PN: 26.4 ± 2.7 PE: 24.9 ± 2.5 | After the 35th week of gestation | No comorbidities were reported, besides hypertension. | Cu (µg/g placental tissue): PN: 281.0 ± 88.4 PE: 269.7 ± 86.7 | | |
| [66] | Case–control study | 48 PN 47 PE | PN: 27.92 ± 4.25 PE: 27.91 ± 5.21 | Venous blood samples collected during weeks 29th to 38th | No comorbidities described in the study, besides hypertension | sample from placenta Cu (μg/dL): PN: 2.08 ± 0.46 PE: 2.65 ± 0.76 | | |
| [65] | Case–control study | 60 PN 60 PE | PN: 26.66 ± 3.72 PE: 27.43 ± 3.91 | 30th–40th week of gestation | No comorbidities described in the study, besides hypertension and obesity | Cu (μg/dL): PN: 116.55 +1 5.23 PE: 118.28 + 16.92 | | |
| [63] | Prospective case–control study | 80 PN 43 PE | PN: 30.28 ± 5.7 PE: 27.23 ± 7.0 | PN: 38.15 ± 2.19 until delivery. PE: 37.72 ± 2.56 weeks until delivery. | No comorbidities described in the study | Cu (μg/dL) (1) cesarean delivery Severe PE Maternal–venous: 229.87 ± 95.59 Cord–artery: 69.46± 61.63 Cord–vein: 71.76 ± 58.26 PN: Maternal–venous: 0.03817 ± 0.06319 Cord–artery: 90.46 ± 77.32 Cord–vein: 62.48± 65.82 (2) vaginal delivery 57.48 Cord–artery: 53.93 ± 22.1 Cord–vein: 52.63 ± 21.06 PN Maternal–venous: 104.97± 87.74 Cord–artery: 99.35 ± 81.15 Cord–vein: 110.92 ± 88.54 (3) maternal and fetal blood. Severe PE Maternal–venous: 226.46 ± 75.17 Cord–artery: 58.16 ± 36.74 PN: Maternal–venous: 104.8 ± 85.11 Cord–artery: 94.9 ± 78.88 Cord–vein: 86.69 ± 81.26 | | |
| [29] | Case–control study | 18 PN 19 PE 14 E | PN: 25 ± 4 PE: 25 ± 4 E: 28 ± 4 | During the partum | No comorbidities described in the study, besides hypertension | umbilical cord Cu (µg/dL) PN: 42.47 ± 8.23 PE: 34.93 ± 9.53 E: 26.09 ± 7.21 | | |
| [41] | Prospective case–control | 56 PE + PN | PE + PN: 31.0 ± 4.9 | 1st, 2nd, 3rd trimesters | No other comorbidities described in the study, besides hypertension 4% had anemia, 4% DM, and smoking condition | Cu (μg/dL): PN: 106 ± 12 (1st) 107 ± 22 (2nd) 112 ± 14.5 (3rd) PE: 102 ± 8 (1st) 88 ± 1 (2nd) 81 ± 1 (3rd) | | |
| [53] | Case–control study | 60 PN 60 PE | Not informed | N/A | No comorbidities described in the study | Cu (mg/L) The study does not show the results, just a graphic PN: 4.5 PE: 3.0 that corresponds to Cu (ug/dL) PN: 0.45 PE: 0.30 | | |
| [45] | Prospective study | 37 PN 30 PH 30 PE | PN: 30.8 PH: 30.8 PE: 31.2 | Gestational age at baseline, in days: PN: 261.92 PH: 261.57 PE: 255.83 | No comorbidities described in the study, besides hypertension and obesity | Cu (μmol/L) PE: 33.91 ± 8.19 PH: 33.32 ± 5.59 PN: 32.04 ± 7.33 that corresponds to: Cu (ug/dL) PN: 203.60 ± 46.6 PH: 211.74 ± 35.5 PE: 215.48 ± 52.0 |  | |
| [54] | Case–control study | 58 PN 50 PE | PN: 25.76 ± 0.73 PE: 25.46 ± 0.85 | 3rd trimester | No comorbidities described in the study, besides hypertension | Cu (mg/L) PN: 2.58 ± 0.06 PE 1.98 ± 0.10 that corresponds to Cu (ug/dL) PN: 258 ± 6 PE 198 ± 10 | | |
| [37] | Case–control study | 40 PN 40 HRPE 40 PE | PN: 31.20 ± 5.84 HRPE: 34.26 ± 6.69 PE: 31.55 ± 6.14 | During the admission after the 24th week of gestation | HRPE Group: BMI ≥ 35, hypertension or PE, gestational diabetes, intrauterine growth restriction or pre-partum. | Cu (mg/L): PN: 2.014 ± 0.43 PE: 1.554 ± 0.53 HRPE: 1.786 + 0.51 that corresponds to Cu (µg/dL) PN: 201.4 ± 0.04 PE: 155.4 ± 0.05 HRPE: 178.6 ± 0.05 | | |
| [60] | Multi- center case–control study | 472 PN 244 PE | PN: 29 (23–32) PE: 28 (23–32) | PN: 15th to 40th week PE: 15th to 38th week | No comorbidities described in the study, besides hypertension and obesity | Cu (µg/L): PN: 1850.0 (1663.5–2051.5) PE: 1957.4 (1787.0–2177.5) that corresponds to Cu(μg/dL) PN: 185.0 (166.35–205.15) PE: 195.74 (178.7–217.75) | | |
| [50] | Prospective cohort study | 50 PN 50 PE: (35 mild 15 severe) | PN: 27.10 ± 4.60 PE: 26.50 ± 3.90 | PN 31.50 ± 3.60 weeks PE: 30.80 ± 3.30 weeks | No comorbidities described in the study | Cu (mg/L) PN: 1.32 ± 0.34 PE: Mild: 2.26 ± 0.48 Severe: 2.70 ± 0.85 that corresponds to Cu (μg/dL) PN: 132 ± 34 Mild: 226 ± 48 Severe: 270 ± 85 | | |
| [61] | Prospective cohort study | 19 PN 24 PDM 23 PEDM | PN:32 ± 5 PDM: 30 ± 4. PEDM: 29 ± 6 | 3 collections: 1st, 2nd, 3rd trimester | Type 1 diabetes mellitus and obesity | Higher Cu levels only at the 3rd trimester in the DM PE group. The authors do not show the levels of micronutrients in the graphics. | | |
| [46] | Prospective cohort study | 40 PN 38 PE | PN: 28.7 ± 3.82 PE: 29.2 ± 3.56 | 32–38 gestational weeks | No comorbidities described in the study | Cu (μg/dL) PN: 152.45 (187.32–104.56) PE: 199.5 (281.86–114.4) | | |
| [67] | Multi-centric case-control study | 51 PN 61 PH 37 PE | PN: 25 ± 5 PH: 27 ± 6 PE: 27 ± 7 | 12th, 21st, and 31st gestational weeks | No comorbidities described in the study, besides hypertension | Cu (µg/dL) PN 192.0 ± 40.0 PH: 196.0 ± 35.0 PE: 199.0 ± 38.0 | | |
| [38] | Case–control study | 60 PN 70 PE | PN: 29.4 ± 3.48 PE: 28.92 ± 4.71 | 28th to 36th weeks of gestation | No comorbidities described in the study, besides hypertension and obesity | Cu (μg/dL) PN: 121.21 ± 25.08 PE: 210.95 ± 56.58 | | |
| [51] | Case–control study | 48 PN 54 PE | PN: 29 ± 5.35 PE: 27 ± 7.02 | after the 20th week of gestation | No comorbidities described in the study | Cu (µmol/L): PN: 8.14 ± 1.80 PE: 16.62 ± 3.17 that corresponds to Cu (μg/dL): PN: 51.47 ± 11.44 PE: 105.49 ± 20.33 | | |
| [62] | Prospective cohort study | 222 PN 5 PE | 32.0 (24.0–43.9) | N/A | BMI was obtained from the self-reported weight and height | In a pooled analysis, pregnancy and neonatal outcomes when trimesters were included in statistical analysis, the prevalence of PE was significantly lower, with high Cu (p = 0.03) median Cu (µg/dL) of all 245 pregnant women was 165.0 (144.0–187.0) Cu measurement of PE was not included | | |
| [47] | Case–control study | 50 PN 50 PE | PN: 28.6 (6.6) PE: 28.6 (6.4) | PN: 36.8 weeks PE: 37.1 weeks | No comorbidities described in the study, besides hypertension and obesity | Cu (μg/dL): PN: 103.6 (86.6–126.7) PE: 111.6 (94.3–135.3) |  | |
| [39] | Triple-blind randomized clinical trial (interventional study) | 107 PN not supplemented 124 PN supplemented (1000 mg Cu oral) | 18 to 35 | After the 16th week up to delivery | No comorbidities described in the study | No measurement of Cu concentrations was reported Overall incidence of PROM (7.6%), the risk of PROM was PN: 6.7% PN supplemented: 9.9% Overall incidence of PROM (1.3%), the risk of PROM was PN: 0.7% PN supplemented: 1.8% Incidence of PE: PN: 0% PN supplemented: 1.6%—2 cases Incidence of placenta abruption: PN: 0% PN supplemented: 0.7%—1 case | | |
| [52] | Case–control study | 100 PN 100 PE | PN: 28.36 ± 3.26 PE: 28.83 ± 5.94 | 2nd and 3rd trimesters Gestational age: PN: 35.57± 2.4 PE: 35.13 ± 3.24 | No comorbidities described in the study, besides hypertension and obesity | Cu (mg/L): PN: 2.76 ± 1.02 PE: 2.01 ± 0.83 that corresponds to Cu (μg/dL): PN: 276 ± 102 PE: 201± 83 | | |
| [40] | Case–control study | 58 PN 121 PH 71 mild PE 26 severe PE 24 HELLP | PN: 36.6 ± 6.6 Mild PE: 35.7 ± 7.28 Severe PE: 36.6 ± 7.72 HELLP: 35.6 ± 7.54 | after the 20th week of gestation | No comorbidities described in the study | PE severity related to Cu and ceruloplasmin concentration. Cu (μg/dL): PN: 62.6 ± 25.63 Mild PE: 81.2 ± 11.4 Severe PE: 160. 2 ± 20.89 HELLP: 209. 9 ± 28.55 Ceruloplasmin (mg/dL) Control: 28.3 ± 10.9 Mild PE: 33.0 ± 4.81 Severe PE: 65.3 ± 9.17 HELLP: 92.7 ± 16.21 | | |
| [27] | Cross-sectional analytical study | 81 PN 81 PE | PN: 29.31 ± 5.22 PE: 29.53 ± 5.38 | Not stated | No comorbidities described in the study, besides hypertension and obesity | Cu (mg/L) PN: 1.670 ± 1.47 PE: 0.844 ± 0.57 that corresponds to PN: 167 ± 147 PE: 84.4 ± 57.0 | | |
| [48] | Case–control study | 60 PN 60 PE | PN: 26.85 ± 0.53 PE: 27.72 ± 0.66 | The time of collection not stated, only third trimester | No comorbidities described in the study, besides hypertension and overweight | Cu (µg/dL) PN: 143.153 ± 3.316 PE: 209.657± 8.679 | | |
| [43] | Cohort study | 44 PN 24 PE | PN: 27 PE: 26 | Prior to or during the latent phase of labor. | No comorbidities described in the study. | Cu (µg/protein (g)) PE: 47.90 ± 19.75 PN: 31.60 ± 11.74 Data without protein reference | | |
| [56] | Case–control study | 45 PN 43 PE | PN: 27.2 ± 5.3 PE: 30.2 ± 6.8 | 28th to 40th weeks of pregnancy | No comorbidities described in the study, besides hypertension | Cu (μg/dL) PN: 195.2 ± 38 PE: 224.5 ± 26.6 | | |
| [55] | Cross-sectional and comparative study | 40 PN 40 PE | PN: 25.46 ± 0.85 PE: 25.76 ± 0.73 | PN: 36.8 ± 0.27 weeks PE: 35.32 ± 0.37 weeks | No comorbidities described in the study, besides hypertension | Cu (mg/dL) PN 0.39 ± 0.02 PE: 0.15 ± 0.07 that corresponds to PN: 390 ± 2.0 PE: 150 ± 7.0 | |  |
| Reference | Study Type | Patients (n) | Age Group | Time of Measurement | Comorbidities | Outcomes | Quality | Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| [43] | Cohort study | 44 PN 24 PE | PN: 27.2 ± 2.7 PE: 26.7 ± 2.6 | Prior to or during the latent phase of labor. | No comorbidities were described in the study. | Zn (µg/g protein) PE: 15.53 ± 4.92 PN: 11.93 ± 3.11 |  | |
| [44] | Prospective cohort study | 20 PN 17 PE | PN: 26.4 ± 2.7 PE: 24.9 ± 2.5 | After the 35th week of gestation | No comorbidities were reported, besides hypertension. | sample: placenta tissue Zn (μg/g tissue): PN: 91.1 ± 36.8 PE: 60.3 ± 27.8 | |  |
| [45] | Prospective study | 30 PN 30 PH 30 PE | PN: 30.8 PH: 30.8 PE: 31.2 | Gestational age at baseline, in days: PE: 255.83 PH: 261.57 PN: 261.92 | No comorbidities were reported, besides hypertension. | Zn (μmol/L) PN: 8.85 ± 1.43 PH: 9.16 ± 1.27 PE: 9.23 ± 1.43 that corresponds to Zn (μg/dL) PN: 57.9 ± 9.4 PH: 59.9 ± 8.3 PE: 60.4 ± 9.4 | | |
| [32] | Case–control study | 50 PN 20 PE 24 severe PE | 17–45 | Two collections, 1st before the delivery, 2nd 30–45 days after partum | No comorbidities were described in the study, besides hypertension | PN: 48.3 ± 8.3 Mild PE: 50.0 ± 9.4 Severe PE: 38.8 ± 8.2 | | |
| [46] | Prospective cohort study | 40 PN 38 PE | PN: 28.7 ± 3.82 PE: 29.2 ± 3.56 | 32–38 gestational weeks | No comorbidities were described in the study, besides hypertension | Zn (μg/dL) PN: 108.45 (138.55–88.12) PE: 81.24 (110.65–62.4) | | |
| [47] | Case–control study | 50 PN 50 PE | PN: 28.6 (6.6) PE: 28.6 (6.4) | PN: 36.8 weeks PE: 37.1 weeks | No comorbidities were described in the study, besides hypertension and obesity | Zn (μg/dL) PN: 108.0 (91.6–131.7) PE: 102.0 (82.8–124.0) |  | |
| [48] | Case–control study | 60 PN 60 PE | PN: 26.85 ± 0.53 PE: 27.72 ± 0.66 | 3rd trimester | No comorbidities were described in the study, besides hypertension and overweight | Zn (µg/dL) PN: 87.535 ± 3.710 PE: 57.283 ± 1.740 | | |
| [33] | Cross-sectional study | 16 PN 23 PE | PN: 28.0 ± 6.9 PE: 31.7 ± 5.8 | PN: 38 (33–41) PE: 34 (21–41) | No comorbidities were reported, besides hypertension. | Zn (no unit reported) PN: 43.3 (26–27) Severe PE: 47 (28–97) | | |
| [27] | Cross-sectional analytical study | 81 PN 81 PE | PN: 29.53 ± 5.38 PE: 29.31 ± 5.22 | N/A | No comorbidities were reported, besides hypertension and obesity | Zn (mg/L) PN: 0.535 ± 0.8 PE: 0.408 ± 0.39 that corresponds to: Zn (µg/dL) PN: 53.5 ± 80.0 PE: 40.8 ± 39.0 | | |
| [49] | Case–control study | 30 PN 21 PE | PN and PE: 19–31 | 31st to 38th weeks of gestation | No comorbidities were reported, besides hypertension | Zn (µg/dL) PN: 125.19 ± 24.23 PE: 82.94 ± 28.93 | | |
| [50] | Prospective cohort study | 50 PE 50 PN | PN: 27.10 ± 4.60 PE: 26.50 ± 3.90 | PN: 31.50 ± 3.60 weeks PE: 30.80 ± 3.30 weeks. | No comorbidities were reported, besides hypertension. | Zn (mg/L): PN: 0.73 ± 0.33 PE: 0.71 ± 0.26 that corresponds to Zn (µg/dL) PN: 73.0 ± 33.0 PE: 71.0 ± 26.0 | | |
| [51] | Case–control study | 48 PN 54 PE | PN: 29 ± 5.35 PE: 27 ± 7.02 | After 20 weeks of gestation | No comorbidities described in the study. | Zn (µmol/L): PN: 8.27 ± 0.6 PE: 12.26 ± 1.83 that corresponds to Zn (µg/dL) PN: 54.1 ± 3.9 PE: 80.2 ± 12.0 | | |
| [52] | Case–control study | 100 PN 100 PE | PN: 28.36 ± 3.26 PE: 28.83 ± 5.94 | PN: 35.57 ± 2.4 PE: 35.13 ± 3.24. | No comorbidities described in the study, besides hypertension and obesity | Zn (mg/L): PN: 0.87 ± 0.30 PE: 0.69 ± 0.21 that corresponds to Zn (µg/dL) PN: 87.0 ± 30.0 PE: 69.0 ± 21.0 | | |
| [53] | Case–control study | 60 PN 60 PE | N/A | After the 20th week of gestation | No comorbidities described in the study. | The results are shown only in a graph | | |
| [57] | Cohort study | 30 PN 29 PE | PN: 32 PE: 32 | During labor | No comorbidities described in the study. | Zn (mg/L) PN: 1.9 ± 0.5 PE: 0.7 ± 0.2 that corresponds to Zn (µg/dL) PN: 190.0 ± 50.0 PE: 70.0 ± 20.0 | | |
| [54] | Case–control study | 58 PN 50 PE | PN: 25.76 ± 0.73 PE: 25.46 ± 0.85 | 3rd trimester | No comorbidities described in the study. | Zn (mg/L): PN: 0.98 ± 0.03 PE: 0.77± 0.05 that corresponds to Zn (µg/dL) PN: 98.0 ± 3.0 PE: 77.0 ± 5.0 | | |
| [62] | Prospective cohort study | 222 PN 5 PE | 32.0 (24.0–43.9) | N/A | BMI was calculated from self-reported weight and height | The relationship between PE and Zn was not stated. | | |
| [63] | Prospective case–control | 80 PN 43 severe PE | PN: 30.28 ± 5.71 Severe PE: 27.23 ± 7.09. | PN: 38.15 ± 2.19 until delivery. Severe PE: 37.72 ± 2.56 weeks until delivery. | No comorbidities described in the study. | Maternal–venous Zn (µg//L) PN: 575.5 ± 215.2 Severe PE: 652.7± 668.6 that corresponds to Zn (µg/dL) PN: 57.55 ± 21.52 PE:65.27 ± 66.86 | | |
| [64] | Cross-sectional prospective study | 28 PN 32 PE | PN: 25.85 ± 3.36 PE: 27.00 ± 3.89 | PN: 36.53± 3.15 PE: 35.68 ± 2.94 | No comorbidities described in the study, besides hypertension. | Zn (mg/L) PN: 1.086 ± 0.199 PE: 0.792 ± 0.180 that corresponds to Zn (µg/dL) PN: 108.6 ± 19.9 PE: 79.2 ± 18.0 | | |
| [65] | Case–control study | 60 PN 60 PE | PN: 26.66 ± 3.72 PE: 27.43 ± 3.91. | 30th–40th weeks | No comorbidities described in the study, besides hypertension and obesity | Zn (µg/dL) PN 100.61 ± 20.12 PE: 76.49 ± 17.62 | | |
| [66] | Case–control study | 48 PN 47 PE | PN: 27.92 ± 4.25 PE: 27.91 ± 5.21 | 29th–38th weeks. | No comorbidities described in the study. | Zn (µg/dL) PE: 1.06 ± 0.44 PN: 1.27 ± 0.41 | | |
| [29] | Case–control study | 18 PN 19 PE 14 E | PN: 25 ± 4 PE: 25 ± 4 E: 28 ± 4 | During the partum | No comorbidities described in the study, besides hypertension | Zn (µg/dL) PN: 83.03 ± 8.85 PE: 74.43 ± 14.99 E: 67.66 ± 11.71 | | |
| [55] | Cross-sectional and comparative study | 40 PN 40 PE | PN: 25.46 ± 0.85 PE: 25.76 ± 0.73 | PN: 36.8 ± 0.27 weeks PE: 35.32 ± 0.37 weeks; | No comorbidities described in the study, besides hypertension | Zn (mg/dL) PN: 5.11 ± 0.21 PE: 2.94 ± 0.45 that corresponds to Zn (µg/dL) PN 5.110 ± 210 PE: 2.940 ± 450 | | |
| [58] | Case–control study | 23 PN 43 PE | PN: 24 ± 5 PE: 25 ± 5 | PN: 37 ± 5 PE: 33 ± 5 | No comorbidities described in the study, besides obesity. | Zn (mg/L): PN: 2.13 ± 3.01 PE: 18.03 ± 30.28 that corresponds to Zn (µg/dL) PN: 213.0 ± 301.0 PE: 1803.0 ± 3028.0 | | |
| [35] | Case–control study | 70 PE 70 PN | N/A | after the 20th week | No comorbidities described in the study. | Results (Zn mg) assessed by Food Frequency Questionnaire PN: 5.5 (2.4–16.5) PE: 4.8 (2.39–12.87) | | |
| [56] | Case–control study | 45 PN 43 PE | PN: 27.2 ± 5.3 PE: 30.2 ± 6.8 | 28th to 40th weeks of pregnancy | No comorbidities described in the study, besides hypertension | Zn (μg/dL) PN: 80.3 PE: 75.1 | | |
| [34] | Case–control study | 48 PN 48 PE | 20–30 years old | Third trimester | No comorbidities described in the study. | Zn (mg/dL) PN: 47.83 ± 12.72 PE: 43.66 ± 11.98 that corresponds to Zn (μg/dL) PN: 47,830.0 ± 12,720.0 PE: 43,660.0 ± 11,980.0 | | |
| Reference | Study Type | Patients (n) | Age Group | Time of Measurement | Comorbidities | Outcomes | Quality | Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| [28] | Case–control study | 53 PN 53 PE | PN: 30 ± 5 PE: 31 ± 5 | Toenail sample collected 3–12 months before | No comorbidities were reported, besides hypertension. | Toenail sample: Se (mg/Kg) PN: 0.62 (0.57–0.69) PE: 0.56 (0.51–0.64) |  | |
| [60] | Cross-sectional cohort study | 27 PN 25 PE | PN: 29 ± 6 PE: 32 ± 5 | PN: 37 ± 5 PE: 33 ± 5 | No comorbidities described in the study, besides hypertension and obesity | Se (μg/L) PN: 58.4 ± 14.9 PE: 39.7 ± 13.8 that corresponds to Se (μg/dL) PN: 5.84 ± 1.49 PE: 3.97 ± 1.38 | | |
| [58] | Case–control study | 23 PN 43 PE | PN: 24 ± 5 PE: 25 ± 5 | N/A | No comorbidities described in the study, besides obesity. | Hair sample Se (μg/g) PN: 23.93 ± 2.62 PE: 24.42 ± 1.78 Se serum (mg/L) PN: 0.14 ± 0.01 PE: 0.06 ± 0.01 that corresponds to Se (μg/dL) PN: 14.0 ± 1.0 PE: 6.0 ± 1.0 | | |
| [59] | Case–control study | 40 PN 40 PE | PN: 26.42 ± 3.73 PE: 27.62 ± 5.25 | 34th to 39th weeks | No comorbidities described in the study. | Se (μg/L) PN: 58.51 ± 11.85 PE: 51.75 ± 11.62 that corresponds to Se (μg/dL) PN: 5.851 ± 1.185 PE: 5.175 ± 1.162 | | |
| [64] | Cross-sectional prospective study | 28 PN 32 PE | PN: 25.85 ± 3.36 PE: 27.00 ± 3.89 | PN: 36.53 ± 3.15 PE: 35.68 ± 2.94 | No comorbidities described in the study, besides hypertension. | Se (mg/L) PN: 87.50 ± 10.96 PE: 60.68 ± 6.42 that corresponds to Se (μg/dL) PN: 8750.0 ± 1096.0 PE: 6068.0 ± 642.0 |  | |
| [29] | Case–control study | 18 PN 19 PE 14 E | PN: 25 ± 4PE: 28 ± 4 E: 28 ± 4 | During the partum | No comorbidities described in the study, besides hypertension | Se (µg/dL) PN: 22.17 ± 4.19 PE: 18.58 ± 5.21 E: 16.34 ± 5.23 | | |
| [63] | Case–control study | 80 PH 43 HRPE | PN: 30.28 ± 5.7 PE: 27.23 ± 7 | Before the partum | No comorbidities described in the study. | Se (µg/L) from the placenta after birth PN: 110.7 ± 19.4 Severe PE: 98.26 ± 24.2 that corresponds to PN: 11.07 ± 1.94 Severe PE: 9.826 ± 2.42 | | |
| [57] | Case–control study | 30 PN 29 PE | PN: 31 ± 3.1 PE: 32.1 ± 4.6 | PN: 39.1± 1.1 PE: 34.1 ± 3.0 | No comorbidities described in the study. | Se (mg/L) PN: 0.09 ± 0.01 PE: 0.09 ± 0.01 that corresponds to Se (µg/L) PN:9.0 ±1.0 PE: 9.0 ± 1.0 | | |
| [65] | Case–control study | 60 PN 60 PE | PN: 26.66 ± 3.72 PE: 7.43 ± 3.91 | 30th–40th weeks of gestation | No comorbidities described in the study, besides hypertension and obesity. | Se (µg/dL) PN: 10.47 ± 2.78 PE: 8.82 ± 2.10 | | |
| [25] | Prospective case–control study | 38 PN 38 PE | PN: 28.2 ± 3.12 PE: 28.4 ± 3.13 | From the 24th–28th weeks of gestation, and followed up 48 h after the partum | No comorbidities described in the study, besides overweight | Se (µg/dL) PN: 82.03 ± 15.54 PE: 70.63 ± 21.41 | | |
| [61] | Prospective cohort study | 19 PN 24 PDM 23 PEDM | PN: 32 ± 5 PDM: 30 ± 4 PEDM: 29 ± 6 | 3 collections: 1st, 2nd, 3rd trimesters | Diabetes mellitus type 1 and obesity | Data was shown only in graphics. The serum levels of Se were not significantly different between the three analyzed groups. | | |
| [42] | Case–control study | 118 PN 74 PE | PN: 24 ± 0.51 PE: 27 ± 0.98 | 6 h apart from patients and 20 gestational weeks | No comorbidities described in the study. | Se (µg/L) rural area: PN: 32.18 ± 1.22 µg/L PE: 23.07 ± 0.96 µg/L that corresponds to Se (µg/dL) PN: 3.218 ± 0.122 PE: 2.307 ± 0.096 Se (µg/L) urban area: PN: 24.67 ± 0.75 PE: 32.29 ± 2.09 that corresponds to Se (µg/dL) PN: 2.467 ± 0.075 PE: 3.229 ± 0.209 | | |
| [21] | Case–control study | 32 PN 20 PH 38 PE | PN: 27.9 ± 6.4 PH ± PE: 28.7 ± 6.828 | During patient admission. | High level of comorbidities, including recurrent urinary tract infection, kidney stones, depression, and heart disease, besides hypertension and obesity | Se (µg/dL) PN: 56.4 ± 15.3 PH: 53.2 ± 15.2 PE: 53.3 ± 16.8 | | |
| [62] | Prospective cohort study | 222 PN 5 PE | median age 32.0 years (24.0–43.9) | N/A | BMI was calculated from self-reported weight and height | The relationship between PE and Se was not stated | | |
| [27] | Cross-sectional analytical study | 81 PN 81 PE | PN: 29.53 ± 5.38 PE: 29.31± 5.22 | N/A | No comorbidities were reported, besides hypertension and obesity | Se (mg/L) PN: 0.842 ± 0.71 mg/L PE: 01.758 ± 3.35 mg/L that corresponds to Se (µg/dL) PN: PN: 84.2 ± 71.0 PE: 175.8 ± 335.0 | | |
| [26] | Comparative case–control study | 56 PN 56 PE | PN: 31.45 ± 4.9 PE: 31.03 ± 4.73 | N/A | No comorbidities described in the study, besides obesity | Se (µmol/L) PN:1.20 ± 0.46 µmol/L PE: 0.67 ± 0.27 µmol/L that corresponds to Se (µg/dL) PN: 94.75 ± 36.38 PE: 52.91 ± 21.32 | | |
| [24] | Cohort study | 363 PN 121 PH 12 PE | 35.1 ± 4 | 1st trimester and 12 weeks post-partum | No comorbidities described in the study, besides hypertension, obesity, and smoking condition | Se (µg/L) PN: 63.58 (48.35–90.14) PH + PE: 57.69 (44.63–70.13) that corresponds to Se (µg/dL) PN: 6.358 (4.835–9.014) PH + PE: 5.769 (4.463–7.013) | | |
| Non-Pregnant | 1st Trimester | 2nd Trimester | 3rd Trimester | |
|---|---|---|---|---|
| Cu | 63–158 µg/dL | 112–199 µg/dL | 165–221 µg/dL | 130–240 µg/dL |
| Zn | 75–120 µg/dL | 57–88 µg/dL | 51–80 µg/dL | 50–70 µg/dL |
| Se | 63–160 µg/L | 116–146 µg/L | 75–145 µg/L | 71–133 µg/L |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goularte, P.d.S.; Imperador, C.H.L.; Piedade, F.H.; Guerin, A.N.; Martins, K.d.T.; Boreski, D.; Gabriel, E.A.; Gabriel, S.A.; Tiezzi, D.G.; Chin, C.M. Copper, Zinc, and Selenium Levels During Pregnancy and Their Relationship with Pre-Eclampsia Risk: A Systematic Review. Nutrients 2025, 17, 1038. https://doi.org/10.3390/nu17061038
Goularte PdS, Imperador CHL, Piedade FH, Guerin AN, Martins KdT, Boreski D, Gabriel EA, Gabriel SA, Tiezzi DG, Chin CM. Copper, Zinc, and Selenium Levels During Pregnancy and Their Relationship with Pre-Eclampsia Risk: A Systematic Review. Nutrients. 2025; 17(6):1038. https://doi.org/10.3390/nu17061038
Chicago/Turabian StyleGoularte, Pietra dos Santos, Carlos Henrique Lima Imperador, Felipe Hassan Piedade, Amanda Nascimento Guerin, Karina de Toledo Martins, Diogo Boreski, Edmo Atique Gabriel, Sthefano Atique Gabriel, Daniel Guimarães Tiezzi, and Chung Man Chin. 2025. "Copper, Zinc, and Selenium Levels During Pregnancy and Their Relationship with Pre-Eclampsia Risk: A Systematic Review" Nutrients 17, no. 6: 1038. https://doi.org/10.3390/nu17061038
APA StyleGoularte, P. d. S., Imperador, C. H. L., Piedade, F. H., Guerin, A. N., Martins, K. d. T., Boreski, D., Gabriel, E. A., Gabriel, S. A., Tiezzi, D. G., & Chin, C. M. (2025). Copper, Zinc, and Selenium Levels During Pregnancy and Their Relationship with Pre-Eclampsia Risk: A Systematic Review. Nutrients, 17(6), 1038. https://doi.org/10.3390/nu17061038