
Mediterranean Diet on Development and Progression of Age-Related Macular Degeneration: Systematic Review and Meta-Analysis of Observational Studies


 , and
, and
Abstract

1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search Strategy
2.3. Study Selection and Data Extraction
2.4. Risk-of-Bias (Quality) Assessment
2.5. Quantitative Synthesis
3. Results
3.1. Search Results
3.2. Description of Studies
3.3. Main Findings and Meta-Analysis
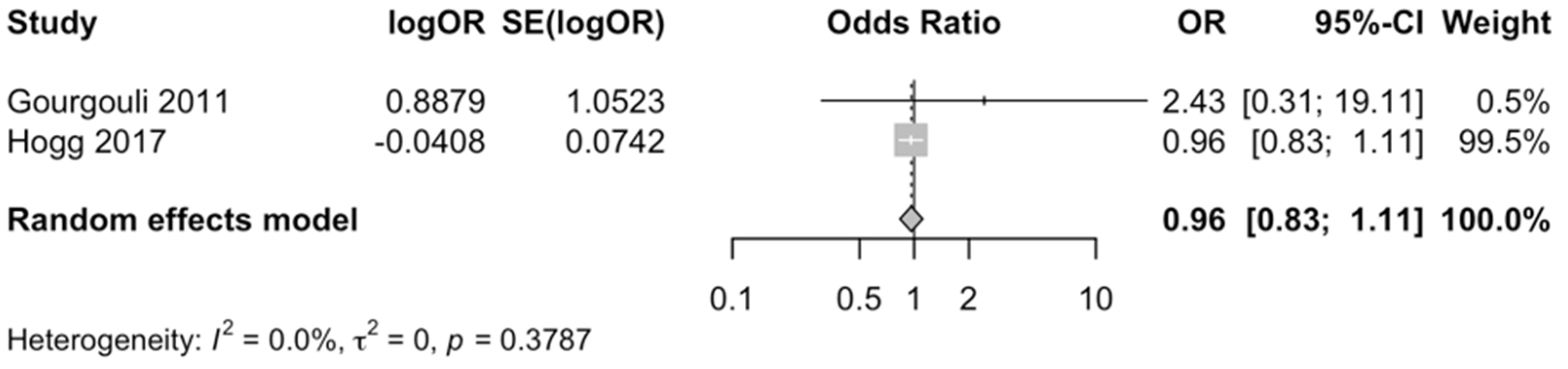
3.3.1. Cross-Sectional Studies
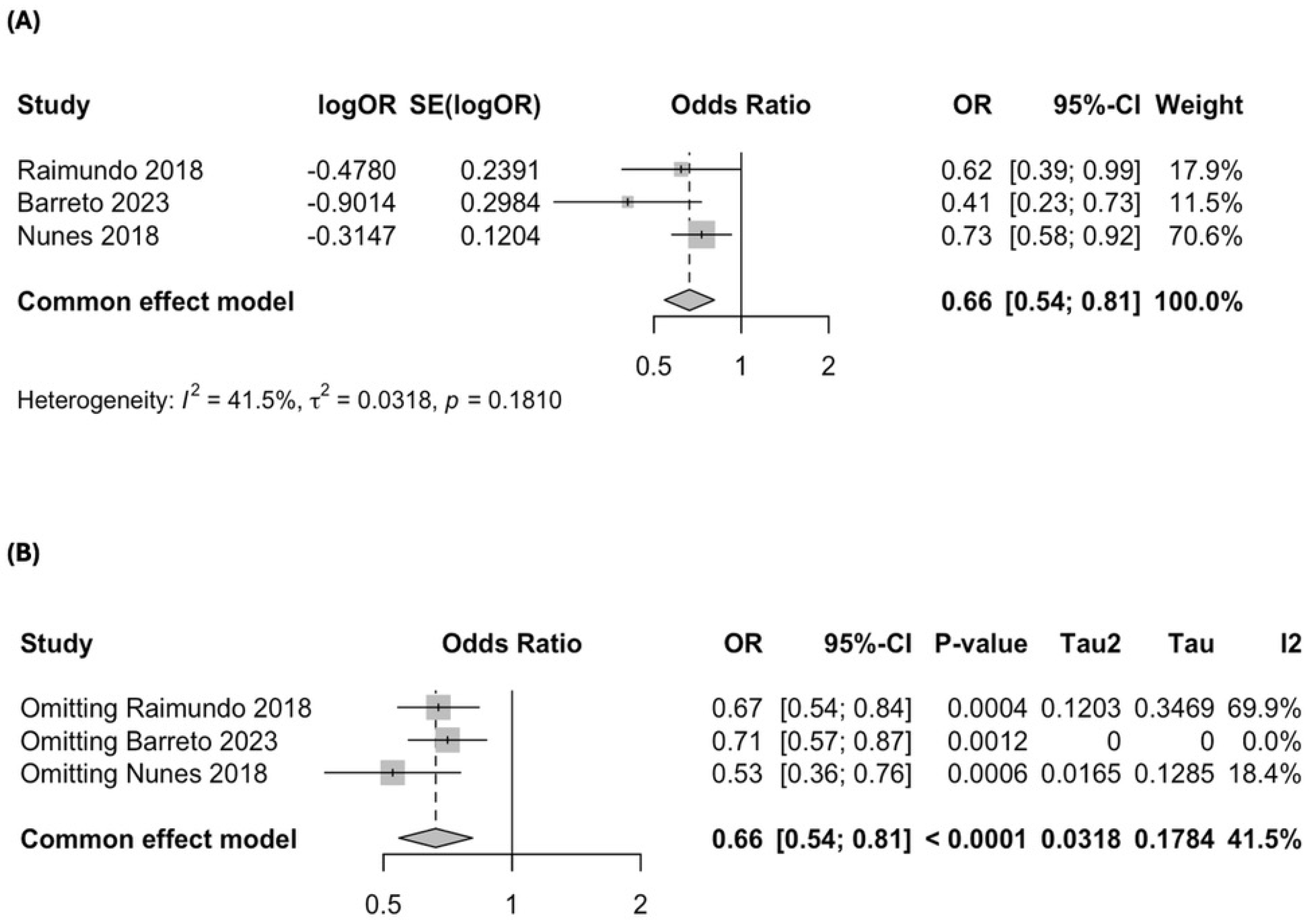
3.3.2. Case–Control Studies
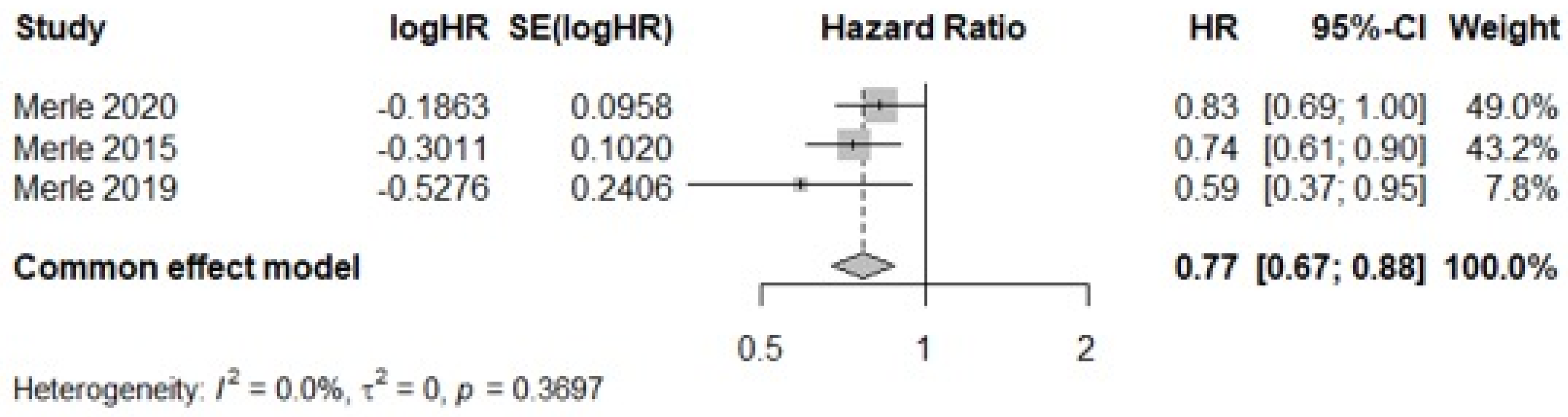
3.3.3. Prospective Cohort Studies
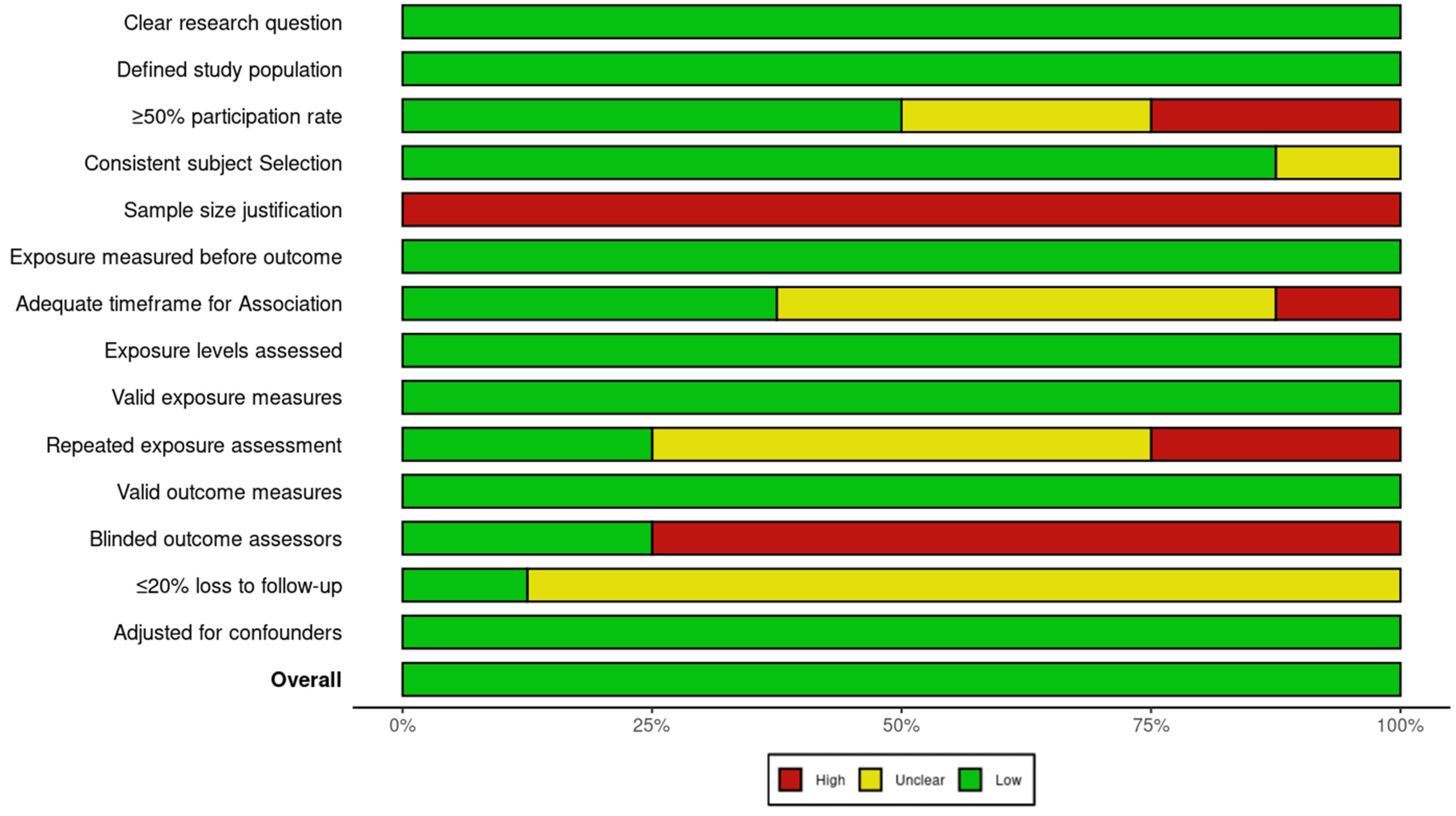
3.4. Studies Quality and Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fleckenstein, M.; Schmitz-Valckenberg, S.; Chakravarthy, U. Age-Related Macular Degeneration: A Review. JAMA 2024, 331, 147. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.Y.; Ferreira, A.; Hughes, R.; Carter, G.; Mitchell, P. Epidemiology and Disease Burden of Pathologic Myopia and Myopic Choroidal Neovascularization: An Evidence-Based Systematic Review. Am. J. Ophthalmol. 2014, 157, 9–25.e12. [Google Scholar] [CrossRef] [PubMed]
- Flores, R.; Carneiro, Â.; Vieira, M.; Tenreiro, S.; Seabra, M.C. Age-Related Macular Degeneration: Pathophysiology, Management, and Future Perspectives. Ophthalmologica 2021, 244, 495–511. [Google Scholar] [CrossRef] [PubMed]
- Lambert, N.G.; ElShelmani, H.; Singh, M.K.; Mansergh, F.C.; Wride, M.A.; Padilla, M.; Keegan, D.; Hogg, R.E.; Ambati, B.K. Risk factors and biomarkers of age-related macular degeneration. Prog. Retin. Eye Res. 2016, 54, 64–102. [Google Scholar] [CrossRef]
- Hyman, L.; Neborsky, R. Risk factors for age-related macular degeneration: An update. Curr. Opin. Ophthalmol. 2002, 13, 171–175. [Google Scholar] [CrossRef]
- Agrón, E.; Mares, J.; Clemons, T.E.; Swaroop, A.; Chew, E.Y.; Keenan, T.D.L. Dietary Nutrient Intake and Progression to Late Age-Related Macular Degeneration in the Age-Related Eye Disease Studies 1 and 2. Ophthalmology 2021, 128, 425–442. [Google Scholar] [CrossRef]
- Zampatti, S.; Ricci, F.; Cusumano, A.; Marsella, L.T.; Novelli, G.; Giardina, E. Review of nutrient actions on age-related macular degeneration. Nutr. Res. 2014, 34, 95–105. [Google Scholar] [CrossRef]
- Carneiro, Â.; Andrade, J.P. Nutritional and Lifestyle Interventions for Age-Related Macular Degeneration: A Review. Oxidative Med. Cell. Longev. 2017, 2017, 6469138. [Google Scholar] [CrossRef]
- Kiani, A.K.; Medori, M.C.; Bonetti, G.; Aquilanti, B.; Velluti, V.; Matera, G.; Iaconelli, A.; Stuppia, L.; Connelly, S.T.; Herbst, K.L.; et al. Modern vision of the Mediterranean diet. J. Prev. Med. Hyg. 2022, 63, E36–E43. [Google Scholar] [CrossRef]
- Datta, S.; Cano, M.; Ebrahimi, K.; Wang, L.; Handa, J.T. The impact of oxidative stress and inflammation on RPE degeneration in non-neovascular AMD. Prog. Retin. Eye Res. 2017, 60, 201–218. [Google Scholar] [CrossRef]
- Age-Related Eye Disease Study 2 Research Group. Lutein + Zeaxanthin and Omega-3 Fatty Acids for Age-Related Macular Degeneration: The Age-Related Eye Disease Study 2 (AREDS2) Randomized Clinical Trial. JAMA 2013, 309, 2005. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.; Zou, J.; Yoshida, S.; Jiang, B.; Zhou, Y. The Role of Inflammation in Age-Related Macular Degeneration. Int. J. Biol. Sci. 2020, 16, 2989–3001. [Google Scholar] [CrossRef] [PubMed]
- Gourgouli, D.-M.; Gourgouli, I.; Spai, S.; Gourgouli, K.; Tzorovili, E.; Skouroliakou, M.; Papakonstantinou, D.; Moschos, M.M. Effect of the Mediterranean Diet on Progression of Dry Form of Age-related Macular Degeneration. In Vivo 2023, 37, 1809–1815. [Google Scholar] [CrossRef]
- Merle, B.M.; E Silver, R.; Rosner, B.; Seddon, J.M. Adherence to a Mediterranean diet, genetic susceptibility, and progression to advanced macular degeneration: A prospective cohort study. Am. J. Clin. Nutr. 2015, 102, 1196–1206. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.5 (Updated August 2024); Cochrane: London, UK, 2024; Available online: www.training.cochrane.org/handbook (accessed on 20 January 2025).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- The Age-Related Eye Disease Study Research Group. The Age-Related Eye Disease Study (AREDS). Control. Clin. Trials 1999, 20, 573–600. [Google Scholar] [CrossRef]
- National Heart, Lung and Blood Institute (NIH). Study Quality Assessment Tools. July 2021. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 20 January 2025).
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Keenan, T.D.L. Geographic Atrophy in Age-Related Macular Degeneration. Ophthalmol. Sci. 2023, 3, 100306. [Google Scholar] [CrossRef]
- Sondel, S.A.; Voland, R.; Millen, A.E.; Tinker, L.; Mares, J.A. Relationship of Healthy Lifestyles to the Prevalence of Intermediate Age-Related Macular Degeneration (AMD) in the Carotenoids in Age-Related Eye Diseases Study (CAREDS), an Ancillary Study of the Women’s Health Initiative Observational Study (WHIOS). Investig. Ophthalmol. Vis. Sci. 2010, 51, 4529. [Google Scholar]
- Merle, B.M.J.; Silver, R.E.; Rosner, B.; Seddon, J.M. Mediterranean diet, genetic susceptibility and progression to advanced macular degeneration. Investig. Ophthalmol. Vis. Sci. 2015, 56, 2573. [Google Scholar]
- Altersabhängige Makuladegeneration. Ophthalmologe 2019, 116, 106–107. [CrossRef] [PubMed]
- Broadhead, G.K.; Agrón, E.; Peprah, D.; Keenan, T.D.L.; Lawler, T.P.; Mares, J.; Chew, E.Y.; AREDS/AREDS2 Investigators. Association of Dietary Nitrate and a Mediterranean Diet with Age-Related Macular Degeneration Among US Adults: The Age-Related Eye Disease Study (AREDS) and AREDS2. JAMA Ophthalmol. 2023, 141, 130. [Google Scholar] [CrossRef] [PubMed]
- Bernat, N.S.O.; i Izquierdo, J.Q.; Trescastro-López, E.M. Health Determinants Associated with the Mediterranean Diet: A Cross-Sectional Study. Nutrients 2022, 14, 4110. [Google Scholar] [CrossRef] [PubMed]
- Dighe, S.; Zhao, J.; Steffen, L.; Mares, J.A.; Meuer, S.M.; Klein, B.E.K.; Klein, R.; Millen, A.E. Diet patterns and the incidence of age-related macular degeneration in the Atherosclerosis Risk in Communities (ARIC) study. Br. J. Ophthalmol. 2020, 104, 1070–1076. [Google Scholar] [CrossRef]
- Lin, Y.; Peng, T.; Li, Y.; Liu, Y. The frequency of early age-related macular degeneration and its relationship with dietary pattern in Hunan, China: A cross-sectional study. BMC Ophthalmol. 2022, 22, 324. [Google Scholar] [CrossRef]
- Piermarocchi, S.; Tognetto, D.; Piermarocchi, R.; Masetto, M.; Monterosso, G.; Segato, T.; Cavarzeran, F.; Turrini, A.; Peto, T.; for the PAMDI Study Group. Risk Factors and Age-Related Macular Degeneration in a Mediterranean-Basin Population: The PAMDI (Prevalence of Age-Related Macular Degeneration in Italy) Study—Report 2. Ophthalmic Res. 2016, 55, 111–118. [Google Scholar] [CrossRef]
- Montgomery, M.P.; Kamel, F.; Pericak-Vance, M.A.; Haines, J.L.; Postel, E.A.; Agarwal, A.; Richards, M.; Scott, W.K.; Schmidt, S. Overall Diet Quality and Age-Related Macular Degeneration. Ophthalmic Epidemiol. 2010, 17, 58–65. [Google Scholar] [CrossRef]
- Kang, K.T.; Kim, Y.C. Dietary Patterns and Age-Related Macular Degeneration in Korea: The Korea National Health and Nutrition Examination Survey 2010–2011. Sci. Rep. 2019, 9, 8200. [Google Scholar] [CrossRef]
- Keenan, T.D.; Agrón, E.; Mares, J.A.; Clemons, T.E.; van Asten, F.; Swaroop, A.; Chew, E.Y.; AREDS 1 and 2 Research Groups. Adherence to the Mediterranean Diet and Progression to Late Age-Related Macular Degeneration in the Age-Related Eye Disease Studies 1 and 2. Ophthalmology 2020, 127, 1515–1528. [Google Scholar] [CrossRef]
- Ajana, S.; Cougnard-Grégoire, A.; Colijn, J.M.; Merle, B.M.J.; Verzijden, T.; de Jong, P.T.V.M.; Hofman, A.; Vingerling, J.R.; Hejblum, B.P.; Korobelnik, J.-F.; et al. Predicting Progression to Advanced Age-Related Macular Degeneration from Clinical, Genetic, and Lifestyle Factors Using Machine Learning. Ophthalmology 2021, 128, 587–597. [Google Scholar] [CrossRef]
- Merle, B.M.J.; Colijn, J.M.; Cougnard-Grégoire, A.; de Koning-Backus, A.P.M.; Delyfer, M.-N.; Kiefte-de Jong, J.C.; Meester-Smoor, M.; Féart, C.; Verzijden, T.; Samieri, C.; et al. Mediterranean Diet and Incidence of Advanced Age-Related Macular Degeneration: The EYE-RISK Consortium. Ophthalmology 2019, 126, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Hogg, R.E.; Woodside, J.V.; McGrath, A.; Young, I.S.; Vioque, J.L.; Chakravarthy, U.; de Jong, P.T.; Rahu, M.; Seland, J.; Soubrane, G.; et al. Mediterranean Diet Score and Its Association with Age-Related Macular Degeneration. Ophthalmology 2017, 124, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Nunes, S.; Alves, D.; Barreto, P.; Raimundo, M.; da Luz Cachulo, M.; Farinha, C.; Laíns, I.; Rodrigues, J.; Almeida, C.; Ribeiro, L.; et al. Adherence to a Mediterranean diet and its association with age-related macular degeneration. The Coimbra Eye Study–Report 4. Nutrition 2018, 51–52, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Raimundo, M.; Mira, F.; Cachulo, M.d.L.; Barreto, P.; Ribeiro, L.; Farinha, C.; Laíns, I.; Nunes, S.; Alves, D.; Figueira, J.; et al. Adherence to a Mediterranean diet, lifestyle and age-related macular degeneration: The Coimbra Eye Study—Report 3. Acta Ophthalmol. 2018, 96. [Google Scholar] [CrossRef]
- Barreto, P.; Farinha, C.; Coimbra, R.; Cachulo, M.L.; Melo, J.B.; Lechanteur, Y.; Hoyng, C.B.; Cunha-Vaz, J.; Silva, R. Interaction between genetics and the adherence to the Mediterranean diet: The risk for age-related macular degeneration. Coimbra Eye Study Report 8. Eye Vis. 2023, 10, 38. [Google Scholar] [CrossRef]
- Merle, B.M.J.; Rosner, B.; Seddon, J.M. Genetic Susceptibility, Diet Quality, and Two-Step Progression in Drusen Size. Invest. Ophthalmol. Vis. Sci. 2020, 61, 17. [Google Scholar] [CrossRef]
- Kumar, D.M.; Talwar, P. Retinal degenerative diseases: Role of dietary supplements in retinal health. Discov. Food 2024, 4, 174. [Google Scholar] [CrossRef]
- SanGiovanni, J.P.; Chew, E.Y. The role of omega-3 long-chain polyunsaturated fatty acids in health and disease of the retina. Prog. Retin. Eye Res. 2005, 24, 87–138. [Google Scholar] [CrossRef]
- Wei, W.; Li, L.; Zhang, Y.; Geriletu; Yang, J.; Zhang, Y.; Xing, Y. Vitamin C Protected Human Retinal Pigmented Epithelium from Oxidant Injury Depending on Regulating SIRT1. Sci. World J. 2014, 2014, 750634. [Google Scholar] [CrossRef]
- Edwards, G.; Olson, C.G.; Euritt, C.P.; Koulen, P. Molecular Mechanisms Underlying the Therapeutic Role of Vitamin E in Age-Related Macular Degeneration. Front. Neurosci. 2022, 16, 890021. [Google Scholar] [CrossRef]
- Li, L.H.; Lee, J.C.-Y.; Leung, H.H.; Lam, W.C.; Fu, Z.; Lo, A.C.Y. Lutein Supplementation for Eye Diseases. Nutrients 2020, 12, 1721. [Google Scholar] [CrossRef] [PubMed]
- Thomson, L.R.; Toyoda, Y.; Delori, F.C.; Garnett, K.M.; Wong, Z.-Y.; Nichols, C.R.; Cheng, K.M.; Craft, N.E.; Dorey, C.K. Long Term Dietary Supplementation with Zeaxanthin Reduces Photoreceptor Death in Light-damaged Japanese Quail. Exp. Eye Res. 2002, 75, 529–542. [Google Scholar] [CrossRef] [PubMed]
- Age-Related Eye Disease Study Research Group. A Randomized, Placebo-Controlled, Clinical Trial of High-Dose Supplementation with Vitamins C and E, Beta Carotene, and Zinc for Age-Related Macular Degeneration and Vision Loss: AREDS Report No. 8. Arch. Ophthalmol. 2001, 119, 1417. [Google Scholar] [CrossRef]
- Jeong, Y.; Woo, S.J. Compliance with the Recommended Age-related Eye Disease Study 2 Supplementation among Korean Age-related Macular Degeneration Patients. J. Retin. 2022, 7, 121–126. [Google Scholar] [CrossRef]
- Yong, J.J.; Scott, I.U.; Greenberg, P.B. Ocular Nutritional Supplements. Ophthalmology 2015, 122, 595–599. [Google Scholar] [CrossRef]
- Hochstetler, B.S.; Scott, I.U.; Kunselman, A.R.; Thompson, K.; Zerfoss, E. Adherence to Recommendations of The Age-Related Eye Disease Study in Patients with Age-Related Macular Degeneration. Retina 2010, 30, 1166–1170. [Google Scholar] [CrossRef]
- Hogg, R.E.; Woodside, J.V. Mediterranean Diet and Age-Related Macular Degeneration: Is It Time to Attempt Dietary Modification? Ophthalmology 2019, 126, 391–392. [Google Scholar] [CrossRef]
- Beatty, S.; Koh, H.-H.; Phil, M.; Henson, D.; Boulton, M. The Role of Oxidative Stress in the Pathogenesis of Age-Related Macular Degeneration. Surv. Ophthalmol. 2000, 45, 115–134. [Google Scholar] [CrossRef]
- Barbouti, A.; Goulas, V. Dietary Antioxidants in the Mediterranean Diet. Antioxidants 2021, 10, 1213. [Google Scholar] [CrossRef]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef]
- Shim, J.-S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health. 2014, 36, e2014009. [Google Scholar] [CrossRef] [PubMed]
- Tuo, J.; Bojanowski, C.M.; Chan, C.-C. Genetic factors of age-related macular degeneration. Prog. Retin. Eye Res. 2004, 23, 229–249. [Google Scholar] [CrossRef]
- Gastaldello, A.; Giampieri, F.; Quiles, J.L.; Navarro-Hortal, M.D.; Aparicio, S.; Villena, E.G.; Pifarre, K.T.; De Giuseppe, R.; Grosso, G.; Cianciosi, D.; et al. Adherence to the Mediterranean-Style Eating Pattern and Macular Degeneration: A Systematic Review of Observational Studies. Nutrients 2022, 14, 2028. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.C.; Thurlby, D.A.; Shahid, H.; Clayton, D.G.; Yates, J.R.W.; Bradley, M.; Moore, A.T.; Bird, A.C. Smoking and age related macular degeneration: The number of pack years of cigarette smoking is a major determinant of risk for both geographic atrophy and choroidal neovascularisation. Br. J. Ophthalmol. 2006, 90, 75–80. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, M.B.; Le, J.; Mitchell, P.; Gopinath, B.; Cerin, E.; Saksens, N.T.M.; Schick, T.; Hoyng, C.B.; Guymer, R.H.; Finger, R.P. Physical Activity and Age-related Macular Degeneration: A Systematic Literature Review and Meta-analysis. Am. J. Ophthalmol. 2017, 180, 29–38. [Google Scholar] [CrossRef]
- Hassell, J.B. Impact of age related macular degeneration on quality of life. Br. J. Ophthalmol. 2006, 90, 593–596. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Author; Year) | Study Characteristics | Patient Characteristics | ||||||
|---|---|---|---|---|---|---|---|---|
| Location | Study Design | Inclusion Period; Follow-Up Period | Eligible Population Age; Sex a | Patient Disease Stage b (Classification) | Sample Size | Age Range in Years [Mean (SD) or Median (IQR) *] | Male (n, %) | |
| Cross-sectional studies | ||||||||
| Gourgouli, et al. (2011) [13] | Greece | Cross-sectional | 2 years; NA | >55 years; both | Early or intermediate AMD (AREDS2 classification) | 164 | 73 (7.4) * | 52 (31.7%) |
| Hogg et al. (2017) [34] | Norway, Estonia, United Kingdom, France, Italy, Greece, Spain | Cross-sectional, within the EUREYE study (cross-sectional study with retrospective and current exposure measurements) | 2001–2002; NA | >65 years; both | Any stage AMD (International Classification System for Age-Related Maculopathy) | 4753 | 73.2 (5.6) | 45% |
| Case–control studies | ||||||||
| Nunes et al. (2018) [35] | Portugal | Nested case–control study within the “Epidemiologic Study of the Prevalence of Age-Related Macular Degeneration in Portugal: The Coimbra Eye Study” (cross-sectional) | 12 months; NA | >55 years; both | Cases: stage 1–4 AMD Controls: stage 0 AMD (Rotterdam Classification) | 1992 (768 cases; 1224 controls) | Cases: 71.6 (7.7) Controls: 70.6 (7.0) | Cases: 323 (42.1%) Controls: 556 (45.4%) |
| Raimundo et al. (2018) [36] | Portugal | Nested case–control study within the “Epidemiologic Study of the Prevalence of Age-Related Macular Degeneration in Portugal: The Coimbra Eye Study” (cross-sectional) | NR; NA | ≥55 years; both | Cases: stage 1–4 AMD Controls: stage 0 AMD (Rotterdam Classification) | 883 (434 cases; 449 controls) | Cases: 69.7 (7.9) Controls: 69.0 (7.5) | Cases: 187 (43.1%) Controls: 198 (44.1%) |
| Barreto et al. (2023) [37] | Portugal | Nested case–control study within the “AMD Incidence Study” and the “Lifestyle and Food Habits Questionnaire in the Portuguese Population Aged 55 or More” (both cross-sectional) | 2016–2017; NA | ≥55 years; both | Cases: stage 2–4 AMD Controls: stage 0 AMD and >60 years or stage 1 AMD and >70 years (Rotterdam Classification) | 612 (161 cases; 451 controls) | Cases: 74.8 (6.8) Controls: 71.8 (6.4) | Cases: 60 (37.3%) Controls: 200 (44.3%) |
| Prospective cohort studies | ||||||||
| Merle et al. (2015) [14] | United States | Prospective cohort within AREDS (RCT) | 1992–1998; 13 years | 55–80; both | Stage 0–3 AMD (CARMS system) | 2525 (4663 eyes) | NR | NR |
| Merle et al. (2019) [33] | Europe | Prospective cohort study of the Rotterdam Study I (RS-I) and Antioxydants, Lipides Essentiels, Nutrition et maladies Oculaires (Alienor) study populations, part of the EYE-RISK project | RS-I: NR; 1990–2011; Alienor: NR; 2006–2012 | RS-I: ≥55 years; both Alienor: ≥73 year; both | No AMD or early AMD (modificated Wiconsin Age-Related System for RS-I; Internation Classification for Alienor) | 4996 (4446 from RS-I and 550 from Alienor) | NR | NR |
| Merle et al. (2020) [38] | United States | Prospective cohort within AREDS (RCT) | 1992–1998; 13 years | 55–80; both | Eyes without drusen or with drusen but without advanced AMD or drusen ≥ 125 µm | 1838 (3023 eyes) | NR | 1328 (43.9%) |
| Study (Author; Year) | Exposure Assessment | Outcome Assessment | Comparator Group and Statistical Approach | Effect Measure (OR or HR, 95%CI); p-Value |
|---|---|---|---|---|
| Cross-sectional studies | ||||
| Gourgouli, et al. (2011) [13] | FFQ about the 12 previous months was assessed by a semi-quantitative FFQ MDScore was calculated | AMD progression considered when patients had deterioration in visual acuity and/or anatomical changes | Comparator group: patients without supplement intake and low MD adherence Patients were divided into 4 groups: (1) high adherence/supplement intake, (2) high adherence/no supplement intake, (3) low adherence/supplement intake, (4) low adherence/no supplement intake Logistic regression (unadjusted and adjusted for age, sex, BMI, and smoking) | Unadjusted OR = 2.17 (0.30–15.71); 0.444 Adjusted OR = 2.43 (0.31–19.18); 0.397 |
| Hogg et al. (2017) [34] | Semiquantitative FFQ (130 foods) tailored to each country MDScore was calculated | AMD graded according to the ICS for Age-Related Maculopathy | Patients were divided into 4 MDScore groups: Q1 ≤ 4, Q2 = 5, Q3 = 6, and Q4 ≥ 6 Association with all early AMD, large Drusen and nvAMD was assessed (unadjusted and adjusted for age, sex, country, education, smoking habits, drinking habits, self-reported history of cardiovascular disease, aspirin consumption, diabetes, and BMI—OR) Q1 was defined as reference | ALL EARLY AMD Unadjusted OR Q2: OR = 0.99 (0.92–1.07); Q3: OR = 0.98 (0.89–1.08); Q4: OR = 0.94 (0.85–1.03); p trend = 0.4 Adjusted OR Q2: OR = 1.01 (0.91–1.12); Q3: OR = 1.01 (0.90–1.14); Q4: OR = 0.96 (0.83–1.11); p trend = 0.9 LARGE DRUSEN Unadjusted OR Q2: OR = 0.96 (0.83–1.11); Q3: OR = 0.89 (0.70–1.12): Q4: OR = 0.79 (0.65–0.97); p trend = 0.05 Adjusted OR Q2: OR = 0.99 (0.80–1.21); Q3: OR = 0.90 (0.69–1.17); Q4: OR = 0.80 (0.65–0.98); p trend = 0.1 nvAMD Unadjusted OR Q2: OR = 0.88 (0.55–1.39); Q3: OR = 0.62 (0.33–1.16); Q4: OR = 0.52 (0.29–0.93); p trend = 0.03 Adjusted OR Q2: OR = 0.83 (0.55–1.26); Q3: OR = 0.62 (0.39–1.00); Q4: OR = 0.53 (0.27–1.04); p trend = 0.01 |
| Case–control studies | ||||
| Nunes et al. (2018) [35] | Validated FFQ (86 items) mediSCORE (0–9); high adherence = ≥6 | AMD graded according to the Rotterdam Classification for AMD | High mediSCORE vs. prevalence of AMD | Prevalence of AMD OR = 0.73 (0.58–0.93, p = 0.009)) |
| Raimundo et al. (2018) [36] | Validated FFQ (86 items) mediSCORE (0–9); high adherence = ≥6 | AMD graded according to the Rotterdam Classification for AMD | High mediSCORE (≥6) vs. prevalence of AMD (unadjusted and adjusted for age, gender and calories consumption) | Prevalence of AMD Unadjusted: 38.4% vs. 50.5%, p = 0.041, OR: 0.62 (0.38–0.97) Adjusted: OR: 0.63 (0.41–0.98), p = 0.043 |
| Barreto, et al. (2023) [37] | Validated FFQ (86 items) mediSCORE (0–9); high adherence = ≥6 Two groups: low MD adherence (0–3) or medium-high MD adherence (4–9) | AMD graded according to the Rotterdam Classification for AMD | High mediSCORE (≥6) vs. low mediSCORE (<6) (adjusted for age, sex, physical exercise, and smoking) | Prevalence of AMD OR = 0.406 (0.226–0.728, p = 0.002) |
| Prospective cohort studies | ||||
| Merle et al. (2015) [14] | Validated, self-administered, 90-item, semiquantitative FFQ at baseline mediSCORE (0–9) - Low MD adherence was defined as mediSCORE ≤3 - Medium MD adherence was defined as mediSCORE = 4–5 - High MD adherence was defined as mediSCORE ≥6 | CARMS Progression was defined as either eye progressing from no, early, or intermediate AMD at baseline to advanced disease (either GA or nvAMD) | Low MD adherence was defined as reference Two models 1. Adjusted for age, sex, AREDS treatment, AMD grade at baseline for both eyes, and total energy intake 2. Adjusted for age, sex, AREDS treatment, AMD grade at baseline for both eyes, and total energy intake, educational level, smoking, BMI, supplement use, and 10 genetic variants [CFH rs1061170 (Y402H), CFH rs1410996, CFHrs121913059 (R1210C), ARMS2/HTRA1 rs10490924, C2 rs9332739 (E318D), CFB rs641153 (R32Q), C3 rs2230199 (R102G), C3 rs147859257 (K155Q), COL8A1 rs13095226, and RAD51B rs8017304] | High mediSCORE (≥6) vs. low mediSCORE (≤3) Model 1: HR = 0.91 (0.77–1.07) Model 2: HR = 0.92 (0.78–1.07) Intermediate mediSCORE (4–5) vs. low mediSCORE score (≤3) Model 1: 0.74 (0.61–0.90) Model 2: 0.74 (0.61–0.91) |
| Merle et al. (2019) [33] | RS-I: 170-item validated semiquantitative FFQ at baseline Alienor: 40-item validated FFQ at baseline and a 24 h dietary recall mediSCORE (0–9) - Low MD adherence was defined as ≤3 - Medium MD adherence was defined as (4–5) - High MD adherence was defined as (≥6) | AMD graded based on the Wisconsin Age-Related System (RS-I) and the ICS (Alienor) Incidence of advanced AMD was defined as the participant progressing from no or early AMD at baseline to advanced AMD (either neovascular or atrophic) | Low MD adherence was defined as reference Two models 1. Unadjusted 2. Adjusted for gender, total energy intake, age-related macular degeneration grade at baseline, education, body mass index, smoking, supplement use of multivitamins or minerals, and presence of diabetes and hypercholesterolemia. | MODEL 1 RS-1: 1. Medium vs. low MD adherence: HR= 0.69 (0.46–1.03) 2. High vs. low MD adherence: HR = 0.56 (0.33–0.96) Alienor: 1. Medium vs. low MD adherence: HR = 0.80 (0.39–1.63) 2. High vs. low MD adherence: HR = 0.48 (0.18–1.26) Overall: 1. Medium vs. low MD adherence: HR = 0.71 (0.50–1.00) 2. High vs. low MD adherence: HR = 0.53 (0.33–0.84) MODEL 2 RS-1: 1. Medium vs. low MD adherence: HR = 0.70 (0.46–1.06) 2. High vs. low MD adherence: HR = 0.69 (0.40–1.20) Alienor: 1. Medium vs. low MD adherence: HR = 0.83 (0.38–1.80) 2. High vs. low MD adherence: HR = 0.52 (0.19–1.40) Overall: 1. Medium vs. low MD adherence: HR = 0.70 (0.49–1.01) 2.High vs. low MD adherence: HR = 0.59 (0.37–0.95) |
| Merle et al. (2020) [38] | Validated, self-administered, semiquantitative FFQ (90 items) at AREDS baseline aMED score (0–9) - Low MD adherence was defined as ≤3 - Medium MD adherence was defined as (4–5) - High MD adherence was defined as (≥6) | Eye-specific progression of maximum drusen size was defined as one eye advancing at least two grades during the study period | Medium-high MD adherence (≥4) versus low MD adherence (≤3) | HR = 0.83 (0.68–0.99), p = 0.049 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marques-Couto, P.; Coelho-Costa, I.; Ferreira-da-Silva, R.; Andrade, J.P.; Carneiro, Â. Mediterranean Diet on Development and Progression of Age-Related Macular Degeneration: Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2025, 17, 1037. https://doi.org/10.3390/nu17061037
Marques-Couto P, Coelho-Costa I, Ferreira-da-Silva R, Andrade JP, Carneiro Â. Mediterranean Diet on Development and Progression of Age-Related Macular Degeneration: Systematic Review and Meta-Analysis of Observational Studies. Nutrients. 2025; 17(6):1037. https://doi.org/10.3390/nu17061037
Chicago/Turabian StyleMarques-Couto, Pedro, Inês Coelho-Costa, Renato Ferreira-da-Silva, José Paulo Andrade, and Ângela Carneiro. 2025. "Mediterranean Diet on Development and Progression of Age-Related Macular Degeneration: Systematic Review and Meta-Analysis of Observational Studies" Nutrients 17, no. 6: 1037. https://doi.org/10.3390/nu17061037
APA StyleMarques-Couto, P., Coelho-Costa, I., Ferreira-da-Silva, R., Andrade, J. P., & Carneiro, Â. (2025). Mediterranean Diet on Development and Progression of Age-Related Macular Degeneration: Systematic Review and Meta-Analysis of Observational Studies. Nutrients, 17(6), 1037. https://doi.org/10.3390/nu17061037