
Trends in Nutrition-Related Risk Factors Identified Post-Operatively in Patients Treated for a Lower-Extremity Injury

 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Participants
2.2. Procedures
2.3. Statistical Analysis
3. Results
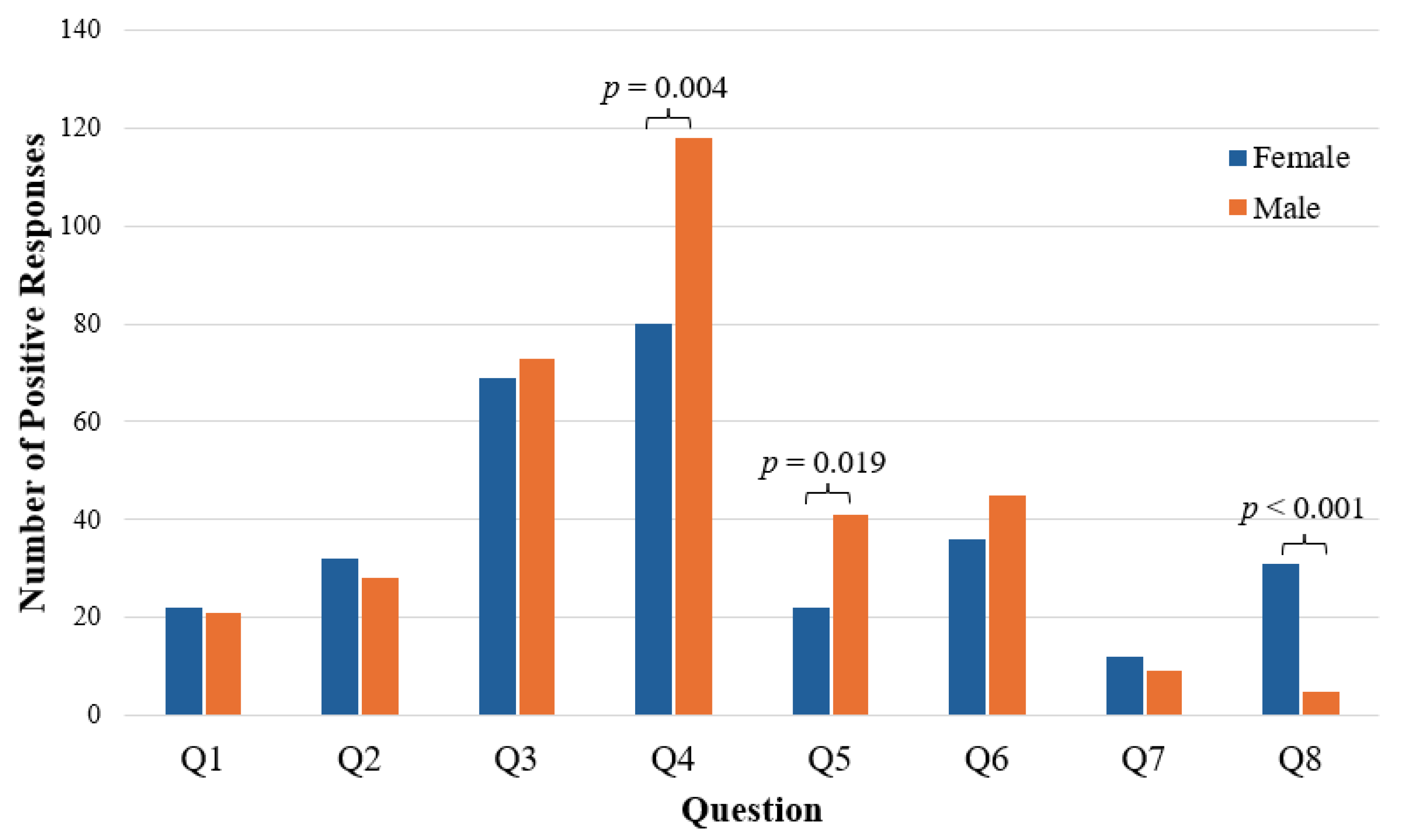
3.1. Sex Comparison
3.2. Age Comparison
4. Discussion
4.1. Weight Concerns
4.2. Appetite and Under Fueling
4.3. Sex- and Age-Related Differences
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Child and Adolescent Health Measurement Initiative. 2019 National Survey of Children’s Health (NSCH) Data Query; Resource Center for Child and Adolescent Health Supported by the U.S. Department of Health and Human Services, Maternal and Child Health Bureau (MCHB): Washington, DC, USA, 2019. [Google Scholar]
- Fabricant, P.D.; Robles, A.; Downey-Zayas, T.; Do, H.T.; Marx, R.G.; Widmann, R.F.; Green, D.W. Development and validation of a pediatric sports activity rating scale: The Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS). Am. J. Sports Med. 2013, 41, 2421–2429. [Google Scholar] [CrossRef] [PubMed]
- Jayanthi, N.A.; LaBella, C.R.; Fischer, D.; Pasulka, J.; Dugas, L.R. Sports-specialized intensive training and the risk of injury in young athletes: A clinical case-control study. Am. J. Sports Med. 2015, 43, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Desbrow, B. Youth Athlete Development and Nutrition. Sports Med. 2021, 51 (Suppl. S1), 3–12. [Google Scholar] [CrossRef] [PubMed]
- Huhmann, K. Menses Requires Energy: A Review of How Disordered Eating, Excessive Exercise, and High Stress Lead to Menstrual Irregularities. Clin. Ther. 2020, 42, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Kontele, I.; Vassilakou, T. Nutritional Risks among Adolescent Athletes with Disordered Eating. Children 2021, 8, 715. [Google Scholar] [CrossRef] [PubMed]
- Hannon, M.P.; Flueck, J.L.; Gremeaux, V.; Place, N.; Kayser, B.; Donnelly, C. Key Nutritional Considerations for Youth Winter Sports Athletes to Optimize Growth, Maturation and Sporting Development. Front. Sports Act. Living 2021, 3, 599118. [Google Scholar] [CrossRef] [PubMed]
- Wahl, R. Nutrition in the adolescent. Pediatr. Ann. 1999, 28, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou, S.K.; Mantzorou, M.; Kondyli-Sarika, F.; Alexandropoulou, I.; Papathanasiou, J.; Voulgaridou, G.; Nikolaidis, P.T. The Key Role of Nutritional Elements on Sport Rehabilitation and the Effects of Nutrients Intake. Sports 2022, 10, 84. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou, S.K. Rehabilitation Nutrition for Injury Recovery of Athletes: The Role of Macronutrient Intake. Nutrients 2020, 12, 2449. [Google Scholar] [CrossRef]
- Hirsch, K.R.; Wolfe, R.R.; Ferrando, A.A. Pre- and Post-Surgical Nutrition for Preservation of Muscle Mass, Strength, and Functionality Following Orthopedic Surgery. Nutrients 2021, 13, 1675. [Google Scholar] [CrossRef]
- Hoelscher, D.M.; Kirk, S.; Ritchie, L.; Cunningham-Sabo, L. Position of the Academy of Nutrition and Dietetics: Interventions for the prevention and treatment of pediatric overweight and obesity. J. Acad. Nutr. Diet. 2013, 113, 1375–1394. [Google Scholar] [CrossRef] [PubMed]
- Smith-Ryan, A.E.; Hirsch, K.R.; Saylor, H.E.; Gould, L.M.; Blue, M.N.M. Nutritional Considerations and Strategies to Facilitate Injury Recovery and Rehabilitation. J. Athl. Train. 2020, 55, 918–930. [Google Scholar] [CrossRef] [PubMed]
- Mackie, A.T.; Pascual-Leone, N.; Coxe, F.R.; Fabricant, P.D.; Doyle, S.M. No Postoperative Change in Body Mass Index Was Observed Among Adolescent Female Patients After Sports or Trauma Surgery. J. Pediatr. Orthop. Soc. N. Am. 2022, 4, 417. [Google Scholar] [CrossRef]
- Olson, T.; Devana, S.; Papanos, L.; Hame, S. Postoperative Body Composition in NCAA Division I Collegiate Athletes. J. Women’s Sports Med. 2023, 3, 22–29. [Google Scholar] [CrossRef]
- Belarde, C.; Barrack, M.; Gray, V.; Blaine, R. Evaluating the Concurrent Validity of a Web-Based Nutrition Screening Survey among Preadolescent Student Athletes; Department of Family and Consumer Sciences, California State University Long Beach: Long Beach, CA, USA, 2020. [Google Scholar]
- Sánchez-Díaz, S.; Yanci, J.; Raya-González, J.; Scanlan, A.T.; Castillo, D. A Comparison in Physical Fitness Attributes, Physical Activity Behaviors, Nutritional Habits, and Nutritional Knowledge Between Elite Male and Female Youth Basketball Players. Front. Psychol. 2021, 12, 685203. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Espino, K.; Fernández-Tena, C.; Lizarraga-Dallo, M.A.; Farran-Codina, A. Development and Validation of a Short Sport Nutrition Knowledge Questionnaire for Athletes. Nutrients 2020, 12, 3561. [Google Scholar] [CrossRef] [PubMed]
- Manore, M.M.; Patton-Lopez, M.M.; Meng, Y.; Wong, S.S. Sport Nutrition Knowledge, Behaviors and Beliefs of High School Soccer Players. Nutrients 2017, 9, 350. [Google Scholar] [CrossRef] [PubMed]
- Dvorak, T.E.; Jordan, K.C.; Dolan, S.H.; Wing-Gaia, S.L.; Manore, M.M.; Meyer, N.L. The Adolescent Sport Nutrition (SN) Knowledge Questionnaire: Validity and Reliability: 1459: Board #6 May 28 2:00 PM–3:30 PM. Med. Sci. Sports Exerc. 2008, 40, S218. [Google Scholar] [CrossRef]
- Rosi, A.; Ferraris, C.; Guglielmetti, M.; Meroni, E.; Charron, M.; Menta, R.; Manini, F.; Di Gioia, V.; Martini, D.; Erba, D. Validation of a General and Sports Nutrition Knowledge Questionnaire in Italian Early Adolescents. Nutrients 2020, 12, 3121. [Google Scholar] [CrossRef]
- Keller, H.H.; Goy, R.; Kane, S.L. Validity and reliability of SCREEN II (Seniors in the community: Risk evaluation for eating and nutrition, Version II). Eur. J. Clin. Nutr. 2005, 59, 1149–1157. [Google Scholar] [CrossRef]
- Bird, S.P.; Rushton, B.D. Nutritional knowledge of youth academy athletes. BMC Nutr. 2020, 6, 35. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.; Seabrook, J.A.; Stranges, S.; Clark, A.F.; Haines, J.; O’Connor, C.; Doherty, S.; Gilliland, J.A. Examining the Correlates of Adolescent Food and Nutrition Knowledge. Nutrients 2021, 13, 2044. [Google Scholar] [CrossRef] [PubMed]
- Dignard, N.A.L.; Jarry, J.L. The “Little Red Riding Hood effect”: Fitspiration is just as bad as thinspiration for women’s body satisfaction. Body Image 2021, 36, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Prichard, I.; Kavanagh, E.; Mulgrew, K.E.; Lim, M.S.C.; Tiggemann, M. The effect of Instagram #fitspiration images on young women’s mood, body image, and exercise behaviour. Body Image 2020, 33, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Betz, D.E.; Sabik, N.J.; Ramsey, L.R. Ideal comparisons: Body ideals harm women’s body image through social comparison. Body Image 2019, 29, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Rothwell, C.J.; Desmond, D. The effect of viewing fitness imagery on body dissatisfaction: Sex and physical activity differences. Psychol. Health Med. 2018, 23, 980–986. [Google Scholar] [CrossRef]
- Sundar, T.K.B.; Londal, K.; Lagerlov, P.; Glavin, K.; Helseth, S. Overweight adolescents’ views on physical activity—Experiences of participants in an internet-based intervention: A qualitative study. BMC Public Health 2018, 18, 448. [Google Scholar] [CrossRef]
- Corr, M.; McSharry, J.; Murtagh, E.M. Adolescent Girls’ Perceptions of Physical Activity: A Systematic Review of Qualitative Studies. Am. J. Health Promot. 2019, 33, 806–819. [Google Scholar] [CrossRef]
- Damiano, S.R.; McLean, S.A.; Nguyen, L.; Yager, Z.; Paxton, S.J. Do we cause harm? Understanding the impact of research with young children about their body image. Body Image 2020, 34, 59–66. [Google Scholar] [CrossRef]
- Mendo-Lazaro, S.; Polo-Del-Rio, M.I.; Amado-Alonso, D.; Iglesias-Gallego, D.; Leon-Del-Barco, B. Self-Concept in Childhood: The Role of Body Image and Sport Practice. Front. Psychol. 2017, 8, 853. [Google Scholar] [CrossRef]
- Neves, C.M.; Cipriani, F.M.; Meireles, J.F.F.; Morgado, F.; Ferreira, M.E.C. Body Image in Childhood: An Integrative Literature Review. Rev. Paul. Pediatr. 2017, 35, 331–339. [Google Scholar] [CrossRef]
- Melin, A.K.; Heikura, I.A.; Tenforde, A.; Mountjoy, M. Energy Availability in Athletics: Health, Performance, and Physique. Int. J. Sport. Nutr. Exerc. Metab. 2019, 29, 152–164. [Google Scholar] [CrossRef]
- Meyer, F.; O’Connor, H.; Shirreffs, S.M.; International Association of Athletics, F. Nutrition for the young athlete. J. Sports Sci. 2007, 25 (Suppl. S1), S73–S82. [Google Scholar] [CrossRef]
- Smith, J.W.; Holmes, M.E.; McAllister, M.J. Nutritional Considerations for Performance in Young Athletes. J. Sports Med. 2015, 2015, 734649. [Google Scholar] [CrossRef]
- Spronk, I.; Heaney, S.E.; Prvan, T.; O’Connor, H.T. Relationship Between General Nutrition Knowledge and Dietary Quality in Elite Athletes. Int. J. Sport. Nutr. Exerc. Metab. 2015, 25, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Foo, W.L.; Faghy, M.A.; Sparks, A.; Newbury, J.W.; Gough, L.A. The Effects of a Nutrition Education Intervention on Sports Nutrition Knowledge during a Competitive Season in Highly Trained Adolescent Swimmers. Nutrients 2021, 13, 2713. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, K.E.; Holtzman, B.; Cooper, K.M.; Flynn, E.F.; Bruinvels, G.; Tenforde, A.S.; Popp, K.L.; Simpkin, A.J.; Parziale, A.L. Low energy availability surrogates correlate with health and performance consequences of Relative Energy Deficiency in Sport. Br. J. Sports Med. 2019, 53, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Holtzman, B.; Ackerman, K.E. Recommendations and Nutritional Considerations for Female Athletes: Health and Performance. Sports Med. 2021, 51 (Suppl. S1), 43–57. [Google Scholar] [CrossRef]
- Voelker, D.K.; Reel, J.J.; Greenleaf, C. Weight status and body image perceptions in adolescents: Current perspectives. Adolesc. Health Med. Ther. 2015, 6, 149–158. [Google Scholar] [CrossRef]
- Davison, K.K.; Markey, C.N.; Birch, L.L. A longitudinal examination of patterns in girls’ weight concerns and body dissatisfaction from ages 5 to 9 years. Int. J. Eat. Disord. 2003, 33, 320–332. [Google Scholar] [CrossRef]
- Lytle, L.; Himes, J.; Feldman, H.; Zive, M.; Dwyer, J.; Hoelscher, D.; Webber, L.; Yang, M. Nutrient intake over time in a multi-ethnic sample of youth. Public Health Nutr. 2002, 5, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D.; Croll, J.; Story, M.; Hannan, P.J.; French, S.A.; Perry, C. Ethnic/racial differences in weight-related concerns and behaviors among adolescent girls and boys: Findings from Project EAT. J. Psychosom. Res. 2002, 53, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Klein, D.J.; Eck, K.M.; Walker, A.J.; Pellegrino, J.K.; Freidenreich, D.J. Assessment of Sport Nutrition Knowledge, Dietary Practices, and Sources of Nutrition Information in NCAA Division III Collegiate Athletes. Nutrients 2021, 13, 2962. [Google Scholar] [CrossRef] [PubMed]
- North, M.; Kelly, A.; Ranchordas, M.; Cole, M. Nutritional Considerations in High Performance Youth Soccer: A Systematic Review. J. Sci. Sport Exerc. 2022, 4, 195–212. [Google Scholar] [CrossRef]
- Jakše, B.; Jakše, B.; Mis, N.F.; Jug, B.; Šajber, D.; Godnov, U.; Čuk, I. Nutritional Status and Cardiovascular Health in Female Adolescent Elite-Level Artistic Gymnasts and Swimmers: A Cross-Sectional Study of 31 Athletes. J. Nutr. Metab. 2021, 2021, 8810548. [Google Scholar] [CrossRef] [PubMed]
- Petrie, H.J.; Stover, E.A.; Horswill, C.A. Nutritional concerns for the child and adolescent competitor. Nutrition 2004, 20, 620–631. [Google Scholar] [CrossRef] [PubMed]
- Matt, S.A.; Barrack, M.T.; Gray, V.B.; Cotter, J.A.; Van Loan, M.D.; Rauh, M.J.; McGowan, R.; Nichols, J.F. Adolescent Endurance Runners Exhibit Suboptimal Energy Availability and Intakes of Key Nutrients. J. Am. Nutr. Assoc. 2022, 41, 551–558. [Google Scholar] [CrossRef]
- Nieves, J.W.; Melsop, K.; Curtis, M.; Kelsey, J.L.; Bachrach, L.K.; Greendale, G.; Sowers, M.F.; Sainani, K.L. Nutritional Factors That Influence Change in Bone Density and Stress Fracture Risk Among Young Female Cross-Country Runners. PM&R 2010, 2, 740–750. [Google Scholar] [CrossRef]

{kind=link}
| Question | All | Female | Male |
|---|---|---|---|
| 1. Do you have any food allergies/intolerances or avoid any food groups? | |||
| Yes | 43 (9.0) | 22 (9.6) | 21 (8.4) |
| No | 434 (91.0) | 206 (90.4) | 228 (91.6) |
| 2. Have you experienced any recent changes in appetite? | |||
| Yes | 60 (12.6) | 32 (14.0) | 28 (11.2) |
| No | 417 (87.4) | 196 (86.0) | 221 (88.8) |
| 3. Do you regularly skip at least one a meal a day? | |||
| Yes | 142 (29.8) | 69 (30.3) | 73 (29.3) |
| No | 335 (70.2) | 159 (69.7) | 176 (70.7) |
| 4. Do you wish you better understood nutrition for your recovery? | |||
| Yes | 198 (41.5) | 80 (35.1) | 118 (47.4) |
| No | 279 (58.5) | 148 (64.9) | 131 (52.6) |
| 5. Have you experienced any recent intentional or unintentional changes in your weight? | |||
| Yes | 63 (13.2) | 22 (9.6) | 41 (16.5) |
| No | 414 (86.8) | 206 (90.4) | 208 (83.5) |
| 6. Are you trying or has someone recommended that you change your body composition or weight? | |||
| Yes | 81 (17.0) | 36 (15.8) | 45 (18.1) |
| No | 396 (83.0) | 192 (84.2) | 204 (81.9) |
| 7. Do you have a history of stress fractures? | |||
| Yes | 21 (4.4) | 12 (5.3) | 9 (3.6) |
| No | 456 (95.6) | 216 (94.7) | 240 (96.4) |
| 8. Do you struggle with dizziness or fatigue during games, practices or with exercise? | |||
| Yes | 36 (7.5) | 31 (13.6) | 5 (2.0) |
| No | 441 (92.5) | 197 (86.4) | 244 (98.0) |
| Question | All | Female | Male |
|---|---|---|---|
| To optimize your return to sport rehabilitation, would you like to meet with our sports dietitian? (% of prompted) | |||
| Yes | 103 (32.3) | 45 (30.2) | 58 (34.1) |
| No | 216 (67.7) | 104 (69.8) | 112 (65.9) |
| Please list the reason(s) for choosing not to have a sports dietitian consult. (% of declined) | |||
| I don’t feel like this applies to me | 124 (57.4) | 63 (60.6) | 61 (54.4) |
| Time | 31 (14.3) | 13 (12.5) | 18 (16.1) |
| No Response | 28 (13.0) | 12 (11.5) | 16 (14.3) |
| Other | 19 (8.8) | 11 (10.6) | 8 (7.1) |
| Financial Concern | 11 (5.1) | 4 (3.8) | 7 (6.3) |
| Transportation | 3 (1.4) | 1 (1.0) | 2 (1.8) |
| Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Consult? | |
|---|---|---|---|---|---|---|---|---|
| Q1: Food allergies/intolerances | 1.40 | 0.60 | 1.70 | 2.18 | 1.13 | 2.52 | 1.29 | 1.22 |
| 95% CI [lower, upper] | [0.59, 3.30] | [0.28, 1.28] | [0.71, 3.19] | [1.02, 4.68] | [0.50, 2.54] | [0.81, 7.85] | [0.43, 3.83] | [0.63, 2.37] |
| p-value | 0.287 | 0.123 | 0.066 | 0.042 | 0.451 | 0.110 | 0.411 | 0.338 |
| Q2: Changes in appetite | 2.15 | 2.36 | 3.93 | 2.41 | 1.68 | 3.52 | 1.31 | |
| 95% CI [lower, upper] | [1.24, 3.73] | [1.36, 4.10] | [2.10, 7.36] | [1.30, 4.45] | [0.55, 5.17] | [1.63, 7.59] | [0.73, 2.34] | |
| p-value | 0.005 | 0.002 | <0.001 | 0.005 | 0.265 | 0.002 | 0.223 | |
| Q3: Skip meals | 2.28 | 2.27 | 1.81 | 1.48 | 2.89 | 0.98 | ||
| 95% CI [lower, upper] | [1.53, 3.39] | [1.32, 3.90] | [1.10, 2.97] | [0.60, 3.65] | [1.45, 5.74] | [0.62, 1.56] | ||
| p-value | <0.001 | 0.003 | 0.014 | 0.265 | 0.002 | 0.516 | ||
| Q4: Desire better understanding | 5.63 | 4.30 | 2.96 | 1.85 | 5.00 | |||
| 95% CI [lower, upper] | [3.05, 10.40] | [2.56, 7.22] | [1.17, 7.47] | [0.93, 3.66] | [2.82, 8.86] | |||
| p-value | <0.001 | <0.001 | 0.016 | 0.055 | <0.001 | |||
| Q5: Experienced weight changes | 13.11 | 2.80 | 2.01 | 2.96 | ||||
| 95% CI [lower, upper] | [7.23, 23.79] | [1.04, 7.51] | [0.87, 4.62] | [1.69, 5.21] | ||||
| p-value | <0.001 | 0.045 | 0.086 | <0.001 | ||||
| Q6: Goal/Rec. to change weight | 1.56 | 3.10 | 1.65 | |||||
| 95% CI [lower, upper] | [0.56, 4.39] | [1.50, 6.42] | [0.98, 2.78] | |||||
| p-value | 0.276 | 0.003 | 0.040 | |||||
| Q7: History of stress fractures | 1.31 | 0.61 | ||||||
| 95% CI [lower, upper] | [0.29, 5.85] | [0.22, 1.70] | ||||||
| p-value | 0.482 | 0.240 | ||||||
| Q8: Struggle with dizziness/fatigue | 0.75 | |||||||
| 95% CI [lower, upper] | [0.35, 1.61] | |||||||
| p-value | 0.291 |
| Variable | Yes | No | p-Value |
|---|---|---|---|
| Food allergies/intolerances | 15.1 ± 2.1 | 15.0 ± 2.0 | 0.982 |
| Changes in appetite | 15.6 ± 1.8 | 15.0 ± 2.0 | 0.022 |
| Skip meals | 15.4 ± 1.7 | 14.9 ± 2.1 | 0.002 |
| Desire for better understanding | 15.5 ± 1.8 | 14.8 ± 2.1 | <0.001 |
| Experienced changes in weight | 15.8 ± 1.6 | 14.9 ± 2.1 | <0.001 |
| Goal/Recommendation to change weight | 15.6 ± 1.8 | 14.9 ± 2.0 | 0.005 |
| History of stress fractures | 15.7 ± 1.6 | 15.0 ± 2.0 | 0.066 |
| Struggle with dizziness or fatigue | 15.1 ± 1.5 | 15.0 ± 2.1 | 0.684 |
| Positive Response for a consult | 15.5 ± 1.7 | 15.2 ± 1.9 | 0.183 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Podvin, C.; Morrison, T.; Dabis, J.; McGinley, J.J.; Ellis, H.B.; Wilson, P.L.; Ulman, S. Trends in Nutrition-Related Risk Factors Identified Post-Operatively in Patients Treated for a Lower-Extremity Injury. Nutrients 2024, 16, 1847. https://doi.org/10.3390/nu16121847
Podvin C, Morrison T, Dabis J, McGinley JJ, Ellis HB, Wilson PL, Ulman S. Trends in Nutrition-Related Risk Factors Identified Post-Operatively in Patients Treated for a Lower-Extremity Injury. Nutrients. 2024; 16(12):1847. https://doi.org/10.3390/nu16121847
Chicago/Turabian StylePodvin, Caroline, Taylor Morrison, Jessica Dabis, James J. McGinley, Henry B. Ellis, Philip L. Wilson, and Sophia Ulman. 2024. "Trends in Nutrition-Related Risk Factors Identified Post-Operatively in Patients Treated for a Lower-Extremity Injury" Nutrients 16, no. 12: 1847. https://doi.org/10.3390/nu16121847
APA StylePodvin, C., Morrison, T., Dabis, J., McGinley, J. J., Ellis, H. B., Wilson, P. L., & Ulman, S. (2024). Trends in Nutrition-Related Risk Factors Identified Post-Operatively in Patients Treated for a Lower-Extremity Injury. Nutrients, 16(12), 1847. https://doi.org/10.3390/nu16121847