
Sulforaphane Treatment in Children with Autism: A Prospective Randomized Double-Blind Study

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Patients and Methods
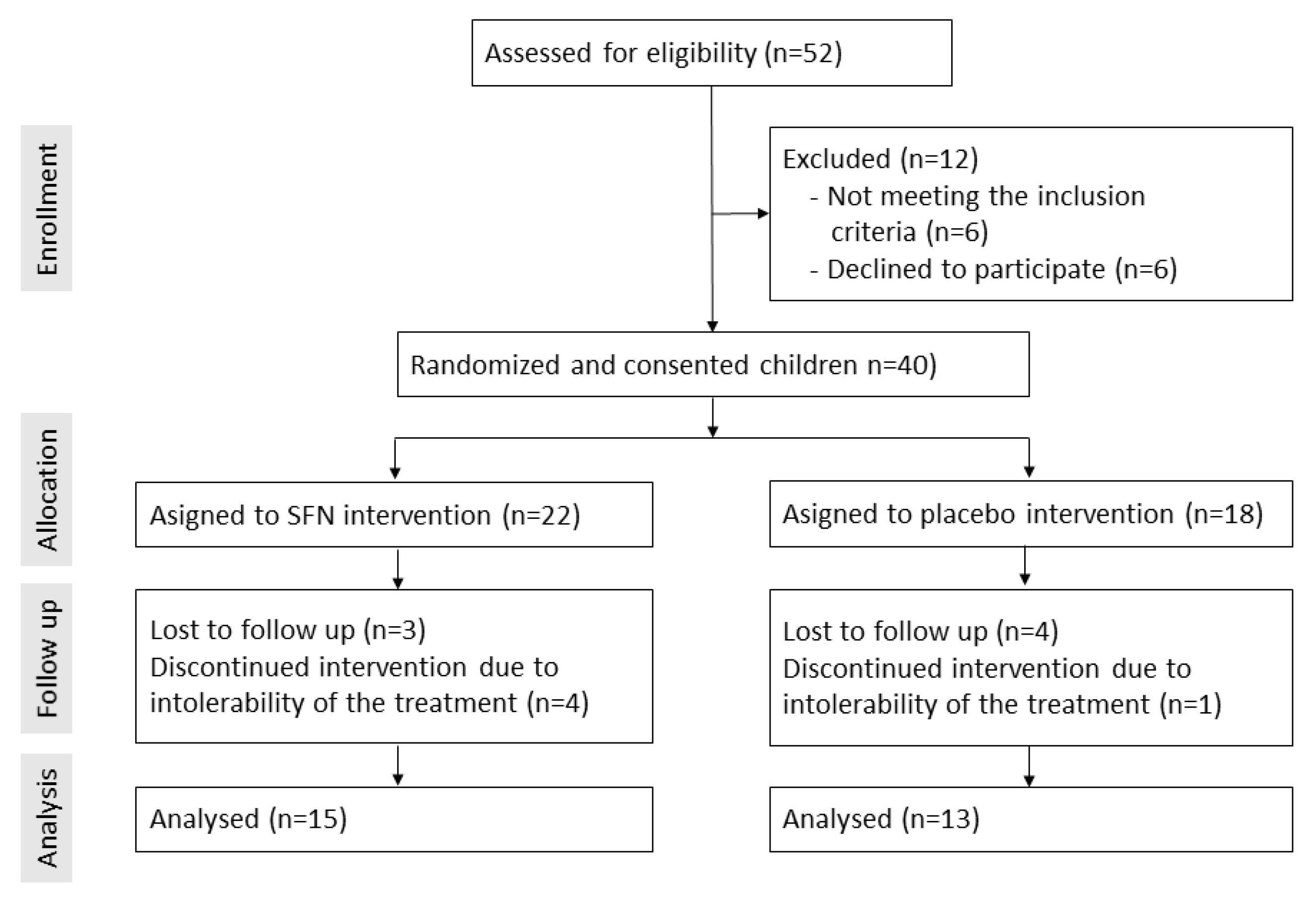
2.1. Patients and Study Design
2.2. Psychological Examination
2.2.1. ADOS-2
2.2.2. SRS-2
2.2.3. ABC
2.3. Preparation of Sulforaphane-Rich Broccoli Sprouts and Placebo Powder
2.4. Statistics
2.5. Ethics
3. Results
3.1. Study Population
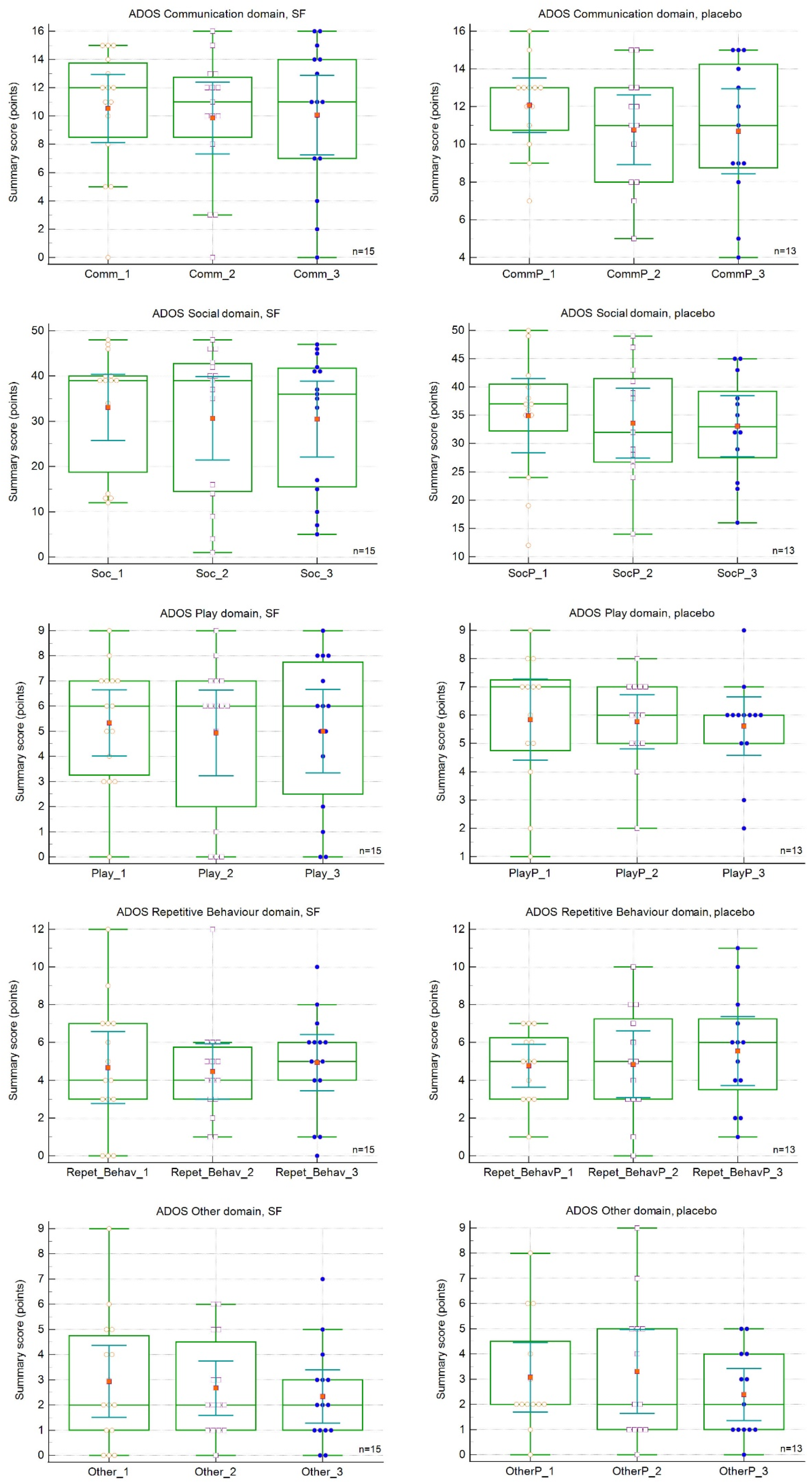
3.2. Changes in Symptoms
3.3. Comparison of Parental and Trained Professional Ratings of Children’s ASD Symptoms or Feature Development
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Cautionary statement for forensic use of DSM-5. In Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Lord, C.; Brugha, T.S.; Charman, T.; Cusack, J.; Dumas, G.; Frazier, T.; Jones, E.J.H.; Jones, R.M.; Pickles, A.; State, M.W.; et al. Autism spectrum disorder. Nat. Rev. Dis. Prim. 2020, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Zhao, Y.; Zhang, H.; Feng, C.; Gao, Y.; Zhao, D.; Yao, F. Advances in biomarker studies in autism spectrum disorders. Adv. Exp. Med. Biol. 2013, 1118, 207–233. [Google Scholar]
- Shen, L.; Liu, X.; Zhang, H.; Lin, J.; Feng, C.; Iqbal, J. Biomarkers in autism spectrum disorders: Current progress. Clin. Chim. Acta 2020, 502, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Farmer, C.; Thurm, A.; Grant, P. Pharmacotherapy for the core symptoms in autistic disorder: Current status of the research. Drugs 2013, 73, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Rossignol, D.A.; Frye, R.E. A review of research trends in physiological abnormalities in autism spectrum disorders: Immune dysregulation, inflammation, oxidative stress, mitochondrial dysfunction and environmental toxicant exposures. Mol. Psychiatry 2012, 17, 389–401. [Google Scholar] [CrossRef]
- Rose, S.; Melnyk, S.; Pavliv, O.; Bai, S.; Nick, T.G.; Frye, R.E.; James, S.J. Evidence of oxidative damage and inflammation associated with low glutathione redox status in the autism brain. Translantional Psychiatry 2012, 2, e134. [Google Scholar] [CrossRef]
- Liu, X.; Lin, J.; Zhang, H.; Khan, N.U.; Zhang, J.; Tang, X.; Cao, X.; Shen, L. Oxidative Stress in Autism Spectrum Disorder-Current Progress of Mechanisms and Biomarkers. Front. Psychiatry 2022, 13, 813304. [Google Scholar] [CrossRef]
- Masi, A.; Quintana, D.S.; Glozier, N.; Lloyd, A.R.; Hickie, I.B.; Guastella, A.J. Cytokine aberrations in autism spectrum disorder: A systematic review and meta-analysis. Mol. Psychiatry 2015, 20, 440–446. [Google Scholar] [CrossRef]
- Liu, H.; Talalay, P.; Fahey, J.W. Biomarker-Guided Strategy for Treatment of Autism Spectrum Disorder (ASD). CNS Neurol. Disord.-Drug Targets 2016, 15, 602–613. [Google Scholar] [CrossRef]
- Rossignol, D.A.; Frye, R.E. Evidence linking oxidative stress, mitochondrial dysfunction, and inflammation in the brain of individuals with autism. Front. Physiol. 2014, 5, 150. [Google Scholar] [CrossRef] [PubMed]
- Klomparens, E.A.; Ding, Y. The neuroprotective mechanisms and effects of sulforaphane. Brain Circ. 2019, 5, 74–83. [Google Scholar]
- Yang, J.; Fu, X.; Liao, X.; Li, Y. Nrf2 Activators as Dietary Phytochemicals Against Oxidative Stress, Inflammation, and Mitochondrial Dysfunction in Autism Spectrum Disorders: A Systematic Review. Front. Psychiatry 2020, 11, 561998. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Connors, S.L.; Macklin, E.A.; Smith, K.D.; Fahey, J.W.; Talalay, P.; Zimmerman, A.W. Sulforaphane treatment of autism spectrum disorder (ASD). Proc. Natl. Acad. Sci. USA 2014, 111, 15550–15555. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.; Fuller, D.J. Initial outcomes from an autism treatment demonstration. Clin. Med. Investig. 2016, 1, 16–19. [Google Scholar] [CrossRef]
- Bent, S.; Lawton, B.; Warren, T.; Widjaja, F.; Dang, K.; Fahey, J.W.; Hendren, R.L. Identification of urinary metabolites that correlate with clinical improvements in children with autism treated with sulforaphane from broccoli. Mol. Autism 2018, 9, 35. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, A.W.; Singh, K.; Connors, S.L.; Liu, H.; Panjwani, A.A.; Lee, L.; Fahey, J.W. Randomized controlled trial of sulforaphane and metabolite discovery in children with Autism Spectrum Disorder. Mol. Autism 2021, 12, 38, Erratum in Mol. Autism 2021, 12, 44. [Google Scholar] [CrossRef]
- Politte, L. Sulforaphane for the Treatment of Young Men with Autism Spectrum Disorder. NCT02909959 2020. Available online: https://www.clinicaltrials.gov/ct2/show/NCT02909959?cond=NCT02909959 (accessed on 1 January 2023).
- Smith, R.; Ou, J.; Jin, H.; Wu, R.; Fahey, J.; Arriaza, J.; Davis, J.M. Sulforaphane as a Treatment for Autism: A Randomized Double-Blind Study. In ACNP 59th Annual Meeting: Poster Session I: Neuropsychopharmacology; Springer: Berlin, Germany, 2020; Volume 45, pp. 68–169. [Google Scholar]
- Gotham, K.; Pickles, A.; Lord, C.J. Standardizing ADOS scores for a measure of severity in autism spectrum disorders. Autism Dev. Disord. 2009, 39, 693–705. [Google Scholar] [CrossRef]
- Frazier, T.W.; Ratliff, K.R.; Gruber, C.; Zhang, Y.; Law, P.A.; Constantino, J.N. Confirmatory factor analytic structure and measurement invariance of quantitative autistic traits measured by the social responsiveness scale-2. Autism 2014, 18, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Egner, P.A.; Chen, J.G.; Wang, J.B.; Wu, Y.; Sun, Y.; Lu, J.H.; Kensler, T.W. Bioavailability of Sulforaphane from two broccoli sprout beverages: Results of a short-term, cross-over clinical trial in Qidong, China. Cancer Prev. Res. (Phila) 2021, 4, 384–395. [Google Scholar] [CrossRef]
- Goin-Kochel, R.P.; Mazefsky, C.A.; Riley, B.P. Level of functioning in autism spectrum disorders: Phenotypic congruence among affected siblings. J. Autism Dev. Disord. 2008, 38, 1019–1027. [Google Scholar] [CrossRef]
- Stewart-Williams, S.; Podd, J. The placebo effect: Dissolving the expectancy versus conditioning debate. Psychol. Bull. 2004, 120, 324–340. [Google Scholar] [CrossRef] [PubMed]
- Yasir, M.; Angelakis, E.; Bibi, F. Comparison of the gut microbiota of people in France and Saudi Arabia. Nutr. Diabetes 2015, 5, e153. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.K.; Paul, S.; Dutta, C. Geography, Ethnicity or Subsistence-Specific Variations in Human Microbiome Composition and Diversity. Front. Microbiol. 2017, 8, 1162. [Google Scholar] [CrossRef] [PubMed]
- Porras, A.M.; Shi, Q.; Zhou, H.; Callahan, R.; Montenegro-Bethancourt, G.; Solomons, N.; Brito, I.L. Geographic differences in gut microbiota composition impact susceptibility to enteric infection. Cell Rep. 2021, 36, 109457. [Google Scholar] [CrossRef]
- Siafis, S.; Çıray, O.; Wu, H.; Schneider-Thoma, J.; Bighelli, I.; Krause, M.; Leucht, S. Pharmacological and dietary-supplement treatments for autism spectrum disorder: A systematic review and network meta-analysis. Mol. Autism 2022, 13, 10. [Google Scholar] [CrossRef]
- Barbaresi, W.J.; Katusic, S.K.; Voigt, R.G. Autism: A review of the state of the science for pediatric primary health care clinicians. Arch. Pediatr. Adolesc. Med. 2006, 160, 1167–1175. [Google Scholar] [CrossRef]
- Coplan, J.; Souders, M.C.; Mulberg, A.E.; Belchic, J.K.; Wray, J.; Jawad, A.F.; Levy, S.E. Children with autistic spectrum disorders. II. Parents are unable to distinguish secretin from placebo under double-blind conditions. Arch. Dis. Child. 2003, 88, 737–739. [Google Scholar] [CrossRef]
- Silva Pereira, A.; Helena, R.; Almeida, L. A Comparison of Parent and Professional Perceptions of Children with Autism Spectrum Disorder in Portugal. Br. J. Spéc. Educ. 2017, 44, 257–272. [Google Scholar]
- McGuinness, G.; Kim, Y. Sulforaphane treatment for autism spectrum disorder: A systematic review. EXCLI J. 2020, 19, 892–903. [Google Scholar]
- Momtazmanesh, S.; Amirimoghaddam-Yazdi, Z.; Moghaddam, H.S.; Mohammadi, M.R.; Akhondzadeh, S. Sulforaphane as an adjunctive treatment for irritability in children with autism spectrum disorder: A randomized, double-blind, placebo-controlled clinical trial. Psychiatry Clin. Neurosci. 2020, 74, 398–405. [Google Scholar] [CrossRef]
- Aishworiya, R.; Valica, T.; Hagerman, R.; Restrepo, B. An Update on Psychopharmacological Treatment of Autism Spectrum Disorder. Neurotherapeutics 2022, 19, 248–262. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics (Mean ± SD) | Placebo Group (n = 13) | SFN Group (n = 15) | p Value |
|---|---|---|---|
| Age | 4.4 ± 1.5 | 4.6 ± 1.0 | 0.7475 |
| Sex (M/F) | 11/2 | 13/2 | 0.8793 |
| Weight (kg) | 19.9 ± 3.9 | 19.1 ± 2.7 | 0.5272 |
| Medication | 4/13 | 2/15 | 0.4865 |
| Dietary supplements | 1/13 | 2/15 | 0.4755 |
| History of autistic developmental regression | 10/13 | 12/15 | 0.8501 |
| Total and Changes in SRS Mean Total Raw Scores | |||
|---|---|---|---|
| Time of observation (weeks) | |||
| Scale and treatment | 0 | 18 | 36 |
| SRS | |||
| Placebo | |||
| Intervention point | 101.5 | 91.8 | 89.5 |
| Change | - | −9.7 ± 6.1 | −2.7 ± 3.2 |
| SFN | |||
| Intervention point | 95.1 | 93.1 | 93.1 |
| Change | - | −2.0 ± 3.1 | −0.1 ± 3.1 |
| p value (between placebo and SFN) | 0.5235 | 0.9176 | 0.7435 |
| Total and Changes in ABC Mean Summary Scores | |||
|---|---|---|---|
| Time of observation (weeks) | |||
| Scale and treatment | 0 | 18 | 36 |
| ABC | |||
| Placebo | |||
| Intervention point | 72.7 | 64.6 | 63.6 |
| Change | - | −8.1 ± 6.2 | −1.0 ± 3.9 |
| SFN | |||
| Intervention point | 60.2 | 55.3 | 56.9 |
| Change | - | −4.9 ± 4.2 | 1.6 ± 3.2 |
| p value (between placebo and SFN) | 0.2742 | 0.4352 | 0.576 |
| Total and Changes in ADOS Mean Summary Scores | |||
|---|---|---|---|
| Time of observation (weeks) | |||
| Scale and treatment | 0 | 18 | 36 |
| ADOS-2 Language and communication | |||
| Placebo | |||
| Intervention point | 12.1 | 10.8 | 10.7 |
| Change | - | −1.3 ± 0.5 | −0.1 ± 0.5 |
| SFN | |||
| Intervention point | 10.5 | 9.9 | 10.1 |
| Change | - | −0.7 ± 0.3 | 0.2 ± 0.4 |
| p value (between placebo and SFN) | 0.2652 | 0.5519 | 0.7165 |
| ADOS-2 Reciprocal social interaction | |||
| Placebo | |||
| Intervention point | 34.9 | 33.6 | 33.1 |
| Change | - | −1.3 ± 2.1 | −0.5 ± 1.4 |
| SFN | |||
| Intervention point | 33.1 | 30.7 | 30.5 |
| Change | - | −2.4 ± 1.6 | −0.2 ± 1.1 |
| p value (between placebo and SFN) | 0.6907 | 0.5850 | 0.5916 |
| ADOS-2 Play and imagination | |||
| Placebo | |||
| Intervention point | 5.8 | 5.8 | 5.6 |
| Change | - | −0.08 ± 0.5 | −0.2 ± 0.3 |
| SFN | |||
| Intervention point | 5.3 | 4.9 | 5.0 |
| Change | - | −0.4 ± 0.5 | 0.07 ± 0.2 |
| p value (between placebo and SFN) | 0.5742 | 0.3867 | 0.5198 |
| ADOS-2 Stereotyped behaviours and restricted interests | |||
| Placebo | |||
| Intervention point | 4.8 | 4.8 | 5.5 |
| Change | - | 0.08 ± 0.6 | 0.7 ± 0.4 |
| SFN | |||
| Intervention point | 4.7 | 4.5 | 4.9 |
| Change | - | −0.2 ± 0.5 | 0.5 ± 0.5 |
| p value (between placebo and SFN) | 0.9244 | 0.7219 | 0.5791 |
| ADOS-2 Other behaviours | |||
| Placebo | |||
| Intervention point | 3.1 | 3.3 | 2.4 |
| Change | - | 0.2 ± 0.7 | −0.9 ± 0.6 |
| SFN | |||
| Intervention point | 2.9 | 2.7 | 2.3 |
| Change | - | −0.3 ± 0.7 | −0.3 ± 0.3 |
| p value (between placebo and SFN) | 0.8782 | 0.4788 | 0.9414 |
| Characteristics (Mean ± SD) | Placebo Group (n = 13) | SFN Group (n = 15) | p Value * | ||||
|---|---|---|---|---|---|---|---|
| −1 | 0 | 1 | −1 | 0 | 1 | ||
| Parents’ impression (18 weeks) | 0/13 | 0/13 | 13/13 | 1/15 | 3/15 | 11/15 | 0.1324 |
| Parents’ impression (36 weeks) | 0/13 | 7/13 | 6/13 | 1/15 | 5/15 | 9/15 | 0.4066 |
| Parents’ impression at 18 weeks vs. 36 weeks | p = 0.0028 * | p = 0.8940 | - | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magner, M.; Thorová, K.; Župová, V.; Houška, M.; Švandová, I.; Novotná, P.; Tříska, J.; Vrchotová, N.; Soural, I.; Jílek, L. Sulforaphane Treatment in Children with Autism: A Prospective Randomized Double-Blind Study. Nutrients 2023, 15, 718. https://doi.org/10.3390/nu15030718
Magner M, Thorová K, Župová V, Houška M, Švandová I, Novotná P, Tříska J, Vrchotová N, Soural I, Jílek L. Sulforaphane Treatment in Children with Autism: A Prospective Randomized Double-Blind Study. Nutrients. 2023; 15(3):718. https://doi.org/10.3390/nu15030718
Chicago/Turabian StyleMagner, Martin, Kateřina Thorová, Veronika Župová, Milan Houška, Ivana Švandová, Pavla Novotná, Jan Tříska, Naděžda Vrchotová, Ivo Soural, and Ladislav Jílek. 2023. "Sulforaphane Treatment in Children with Autism: A Prospective Randomized Double-Blind Study" Nutrients 15, no. 3: 718. https://doi.org/10.3390/nu15030718
APA StyleMagner, M., Thorová, K., Župová, V., Houška, M., Švandová, I., Novotná, P., Tříska, J., Vrchotová, N., Soural, I., & Jílek, L. (2023). Sulforaphane Treatment in Children with Autism: A Prospective Randomized Double-Blind Study. Nutrients, 15(3), 718. https://doi.org/10.3390/nu15030718