Abstract
Background & aims: Iodine is important for thyroid function during pregnancy to support fetal growth, but studies of maternal iodine status and birth outcomes are conflicting. We aimed to quantify the association between iodine status and birth outcomes, including potential threshold effects using nonlinear dose–response curves. Methods: We systematically searched Medline and Embase to 10 October 2022 for relevant cohort studies. We conducted random-effects meta-analyses of urinary iodine concentration (UIC), iodine:creatinine ratio (I:Cr), and iodide intake for associations with birth weight, birth weight centile, small for gestational age (SGA), preterm delivery, and other birth outcomes. Study quality was assessed using the Newcastle-Ottawa scale. Results: Meta-analyses were conducted on 23 cohorts with 42269 participants. Birth weight was similar between UIC ≥ 150 μg/L and <150 μg/L (difference = 30 g, 95% CI −22 to 83, p = 0.3, n = 13, I2 = 89%) with no evidence of linear trend (4 g per 50 μg/L, −3 to 10, p = 0.2, n = 12, I2 = 80%). I:Cr was similar, but with nonlinear trend suggesting I:Cr up to 200 μg/g associated with increasing birthweight (p = 0.02, n = 5). Birthweight was 2.0 centiles (0.3 to 3.7, p = 0.02, n = 4, I2 = 0%) higher with UIC ≥ 150 μg/g, but not for I:Cr. UIC ≥ 150 μg/L was associated with lower risk of SGA (RR = 0.85, 0.75 to 0.96, p = 0.01, n = 13, I2 = 0%), but not with I:Cr. Conclusions: The main risk of bias was adjustment for confounding, with variation in urine sample collection and exposure definition. There were modest-sized associations between some measures of iodine status, birth weight, birth weight centile, and SGA. In pregnancy, we recommend that future studies report standardised measures of birth weight that take account of gestational age, such as birth weight centile and SGA. Whilst associations were modest-sized, we recommend maintaining iodine sufficiency in the population, especially for women of childbearing age on restricted diets low in iodide.
1. Introduction
Iodine has an important role in normal thyroid function, with demands for iodine increasing during pregnancy to support fetal growth as well as compensating for increased renal clearance [1,2]. Severe maternal iodine deficiency is considered an established risk factor for maternal goitre and neurological impairment in the neonate [1,3], with possible associations with subsequently less developed motor skills and intellectual capacity [4]. To avoid these outcomes, pregnant populations are defined by the World Health Organization (WHO) as having insufficient iodine where the median urinary iodine concentration (UIC) is less than 150 μg/L [1,3].
Despite salt iodisation programmes available across many regions, the populations of over 50 countries are still considered to be affected by iodine deficiency [5]. To avoid iodine deficiency, WHO recommend an iodide intake of 150 μg/day in adults, and 250 μg/day during pregnancy [3]. However, two thirds of European countries that monitor iodine in pregnancy have reported inadequate iodine intake [6].
Dairy and seafood are the main dietary sources of dietary iodine, excluding supplements and fortified foods such as iodised salt. With recent increases in diets that restrict intake of these foods, particularly in women of childbearing age, the iodine status of populations previously considered sufficient are moving more towards mild deficiency [7,8]. Whilst the effects of severe deficiency are known, the extent to which adverse outcomes are associated with milder levels of deficiency is less clear.
Two recent systematic reviews of observational studies of iodine and birth outcomes drew differing conclusions [9,10]. Since these reviews were published, results on iodine and birth outcomes from a number of large birth cohorts have become available, including the Norwegian Mother and Child Cohort Study (MoBa) [11], the Screening for Pregnancy Endpoints (SCOPE) cohort [12], the Born in Bradford (BiB) cohort [13], and results from the Shanghai birth registry [14]. There is potential for studies in deficient populations to draw substantially different conclusions from those in less-deficient populations, and for effects to only be seen in individuals with particularly poor intakes. We therefore aimed to systematically review the new and existing literature, additionally investigating potential threshold effects.
2. Material and Methods
2.1. Search Strategy
We conducted a systematic literature review of cohort studies that included relevant information on both maternal iodine status and birth outcomes. We searched MEDLINE and EMBASE databases through OVID, up to 10 October 2022 using a PICO structure, with a cohort study search filter, synonyms relating to pregnancy, iodine status, and specific birth outcomes, with adjacency terms and allowing for alternative spellings where appropriate. The key words included synonyms relating to pregnancy, maternity, and birth (study population); iodide, iodine, and urinary biomarkers of iodine (exposure); and birthweight, fetal growth, head circumference, preterm, and spontaneous abortion (outcomes). The complete search strategies are detailed in Supplementary Table S1).
We included preferred reporting items for systematic reviews and meta-analyses (PRISMA) and followed guidelines for conducting meta-analysis of observational studies in epidemiology (MOOSE) throughout the review. The review protocol was published on PROSPERO (registration number CRD42016043748) prior to starting the study.
2.2. Study Selection
Eligible studies were cohorts, case-control studies nested within cohorts, and case-cohort studies, with exposure measured during pregnancy. Relevant exposures were urinary iodine concentration (UIC), urinary iodine excretion or iodine to creatinine ratio (I:Cr), and iodide intake. Relevant outcomes were pre-specified as those related to fetal loss, preterm birth, and birth size. Low birth weight and macrosomia were taken as birth weight <2.5 kg and >4 kg, respectively.
Birth weight centile was based on standardized birth weight adjusting for at least gestational age, using the study-specific definitions, and transforming z-scores to centiles where necessary. Small for gestational age (SGA) was defined as birth weight <10th centile and large for gestational age (LGA) >90th centile. Spontaneous abortion was defined as fetal loss ≤24 weeks gestation and stillbirth as fetal loss >24 weeks gestation. Preterm delivery was taken as spontaneous preterm birth <37 weeks, or any preterm delivery <37 weeks if this information was not available.
2.3. Data Extraction and Quality Assessment
Titles and abstracts were screened by two independent reviewers (from CK, ET, JW, LJH) using Screenatron and Disputatron [15], with disagreements resolved by a third reviewer (DCG). Full text screening was conducted by two independent reviewers (DCG, LJH) with disagreements resolved by consensus. Data were extracted by DCG and numeric data independently checked by JW. Where two publications reported results from the same cohorts, data were extracted from the most complete report. Information was also extracted from published study protocols or cohort profiles where necessary. For three studies, investigators were contacted for additional data [12,13,16]. Non-English language and unpublished articles and abstracts were excluded.
We assessed methodological quality of studies using the Newcastle–Ottawa scale for cohort studies [17]. Studies were rated for representativeness of the exposed and non-exposed cohorts, ascertainment of exposure, and the outcome not being present before the study. Levels of exposure were considered comparable if length of gestation was controlled for (apart from for preterm deliveries), either through adjustment or by outcome definition, and adjustment for any other relevant confounder. Outcomes were rated on being objective, followed until the end of pregnancy, with >90% of potential participants following up. Quality was assessed independently by two reviewers (CK, ET) with disagreements resolved by a third (DCG) for the first six consecutive studies retrieved, after which all studies were assessed by DCG. All studies were included regardless of perceived quality, but risk of bias was taken into account in the interpretation.
2.4. Data Synthesis and Analysis
Data from each study were synthesised by meta-analysis, comparing dichotomous exposures of UIC < 150 μg/L with ≥150 μg/L based on the WHO criteria [3] and I:Cr < 150 μg/g with ≥150 μg/g, alongside linear and nonlinear dose-response trends.
Linear and nonlinear dose-response trends in relative risks for binary outcomes (low birth weight, macrosomia, SGA, LGA, spontaneous abortion, still birth, and preterm delivery) were derived using Greenland and Longnecker’s method [18,19]. The estimated mean iodine status for each category of exposure was extracted, or the midpoint of each category derived where the mean or median were not provided. For unbounded upper limits, we assumed the category width was 1.5 times the adjacent one. If the reference category was not the lowest, we used the Greenland and Longnecker fitted counts to express adjusted risks relative to the lowest category [18,20]. This method also allowed us to combine categories to estimate relative risks for dichotomised iodine status.
To compare dichotomised exposures, adjusted means were first combined using common (fixed) effect meta-analysis where necessary, then differences pooled using random-effects meta-analysis. Linear trends in continuous outcomes (birth weight, birth weight centile, birth length, and head circumference) were estimated using multivariate random-effects meta-analysis [21,22] and presented per 50 μg/L higher UIC or 50 μg/g higher I:Cr. Nonlinear trends for each study were estimated using restricted cubic splines fitted to each study using knots at the 10th, 50th, and 90th percentiles [23], and then pooled using multivariable random-effects meta-analysis, compared to a reference of 150 μg/L for UIC, 150 μg/g for I:Cr, and 150 μg/d for iodide intake [20]. Meta-analyses were only conducted where more than two studies reported on the same outcome.
Between-study heterogeneity was expressed as the range of study estimates, and as a percentage of total variation (I2) [24,25]. Potential heterogeneity was explored through a limited number of pre-defined subgroup analyses where sufficient data were available as follows: by mean week of gestation when the urine samples were provided, median UIC of study population, high income vs. low-or-middle income country, by any adjustment for potential confounding such as gestational age (other than for preterm delivery), and by Newcastle-Ottawa domain score. Potential small-study effects such as publication bias were explored through contour-enhanced funnel plots and Egger’s test, where more than 10 studies reported on the same outcome. All analyses were conducted in Stata version 17 [26].
3. Results
3.1. Literature Search
Two hundred and forty-seven unique references were identified by the literature search. Of these, 53 were identified as potentially relevant after screening of titles and abstracts (with 89% agreement between reviewers) and 26 were identified as relevant following reading of the full texts (with 80% agreement between reviewers). These publications reported on 24 cohorts containing 42,503 participants (Figure 1, Supplementary Table S2) [11,12,13,14,16,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45].
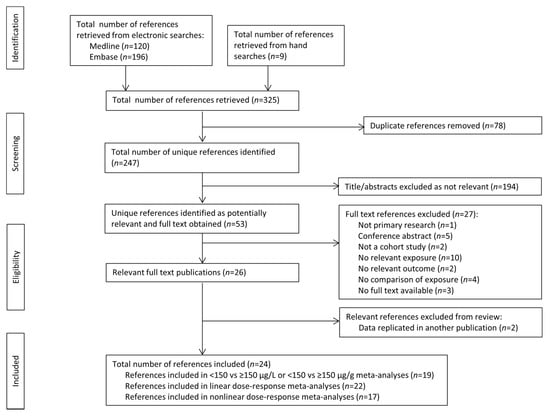
Figure 1.
Article retrieval and screening process flow chart.
Eighteen cohorts reported UIC exposure, seven used I:Cr, three dietary intake and one total intake including dietary and supplemental sources. Eleven (46%) studies were from higher income countries, 14 (58%) were from iodine-deficient populations with median UIC < 150 μg/L, including six (25%) with median UIC < 100 μg/L. Study characteristics are presented in Table 1.

Table 1.
Characteristics of included studies.
Study quality was assessed in duplicate for six papers (25%) with 89% agreement between reviewers across all items, and the remainder extracted by one reviewer. Overall study quality was generally good, with results based on established birth cohorts using objective measures of exposures and outcomes. The main differences in risk of potential bias derived from adjustment for confounding (Supplementary Table S3).
3.2. Birth Weight Outcomes
Fifteen studies reported birth weight in relation to UIC. Comparisons of UIC < 150 μg/L with ≥150 μg/L were derived for 13 studies, linear trends for 12 studies, and nonlinear trends for 11 studies. One study did not quantify the UIC exposure so could not be pooled [45]. There was no evidence that UIC ≥ 150 μg/L was associated with greater birth weight than <150 μg/L (difference = 30 g, 95% CI −22 to 83, p = 0.3, n = 13, I2 = 89%), nor of a linear trend (4 g per 50 μg/L, −3 to 10, p = 0.2, n = 12, I2 = 80%). Between-study heterogeneity was high, but there was no evidence of nonlinearity (p = 0.2, n = 11) (Figure 2a–c).
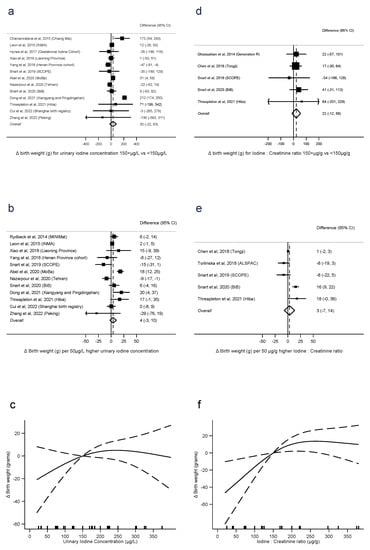
Figure 2.
Urinary iodine concentration (a–c), iodine to creatinine ratio and birth weight (grams) (d–f), dichotomous (a,d), linear (b,e), and nonlinear (c,f) meta-analyses. CI: Confidence interval; Δ: Change in outcome [11,12,13,14,16,28,29,31,33,34,36,37,39,40,41,42,44].
Six studies reported birth weight in relation to I:Cr. There was no evidence that I:Cr ≥ 150 μg/g was associated with greater birth weight than <150 μg/g (difference = 22 g, −12 to 56, p = 0.2, n = 5, I2 = 0%), nor linear trend (3 g per 50 μg/g, −7 to 14, p = 0.5, n = 5, I2 = 88%). However, there was evidence of nonlinearity (p = 0.02, n = 5), with an association between I:Cr and increasing birth weight evident up to around 200 μg/g (Figure 2d–f).
There were too few studies reporting iodide intake with the same category boundaries to conduct meta-analysis on the dichotomous exposure. There was no evidence of a linear association between intake and birth weight (9 g per 50 μg/day, −8 to 26, p = 0.3, n = 3, I2 = 85%), but some evidence of nonlinearity (p < 0.001, n = 3) (Supplementary Figure S1a,b).
For the binary outcomes of low birth weight (<2.5 kg) and macrosomia (>4 kg) there was no evidence of any association with UIC (Supplementary Figures S2 and S3) and too few studies reported this outcome to conduct meta-analysis for I:Cr or iodide intake.
3.3. Standardised Birth Weight Outcomes
For birth weight centile, UIC ≥150 μg/L was associated with 2.0 centiles higher birth weight than UIC < 150 μg/L (difference = 2.0 centiles, 0.3 to 3.7, p = 0.02, n = 4, I2 = 0%), with no evidence of a linear dose-response trend (0.5 centiles per 50 μg/L, −0.5 to 1.4, p = 0.3, n = 4, I2 = 86%), and no evidence of nonlinearity (p = 0.4, n = 4) (Figure 3a–c). There was no evidence that I:Cr ≥ 150 μg/g was associated with higher birth weight centiles than I:Cr < 150 μg/g (difference =0.8, −4.8, 6.5, p = 0.8, n = 3, I2 = 35%), nor evidence of a linear trend (0.5 centiles per 50 μg/g, −0.3 to 1.3, p = 0.2, n = 5, I2 = 70%). There was also no evidence of nonlinearity (p = 0.1, n = 4) (Figure 3e–f).
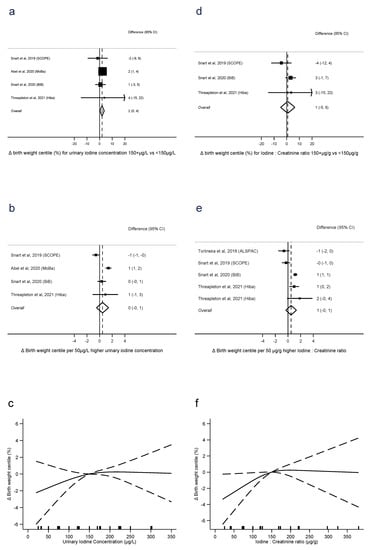
Figure 3.
Urinary iodine concentration (a–c), iodine to creatinine ratio (d–f) and birth weight centile, dichotomous (a,d), linear (b,e), and nonlinear (c,f) meta-analyses. CI: Confidence interval; Δ: Change in outcome [11,12,13,16,40].
UIC was associated with lower risk of SGA, in terms of ≥150 μg/L vs. UIC < 150 μg/L (RR = 0.85, 0.75 to 0.96, p = 0.01, n = 13, I2 = 0%), but with no evidence of a linear trend (RR = 0.96 per 50 μg/L, 0.92 to 1.01, p = 0.1, n = 8, I2 = 52%). There was no evidence of nonlinearity (p = 0.6, n = 7) (Figure 4a–c). There was no evidence of the same association with I:Cr, either for dichotomised exposure (RR = 0.95, 0.70 to 1.28, p = 0.7, n = 5, I2 = 66%) or as a linear trend (RR = 0.98 per 50 μg/g, 0.92 to 1.05, p = 0.6, n = 5, I2 = 70%). However, there was evidence of nonlinearity, with the lowest risk around 150 μg/g and higher risks associated with both lower and higher I:Cr (p = 0.003, n = 4). There were sufficient studies of iodide intake and SGA only to investigate linear trend, where there was no evidence of an association (RR = 0.95 per 50 μg/d, 0.87 to 1.05, p = 0.3, I2 = 35%) (Supplementary Figure S4).
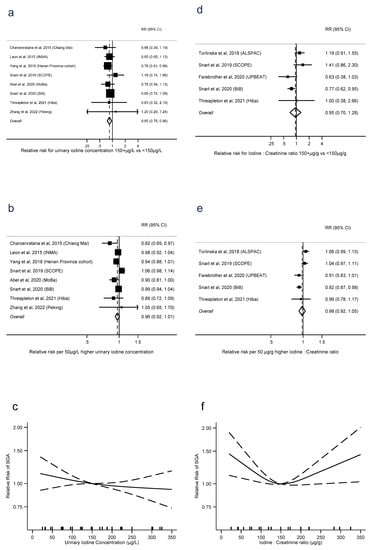
Figure 4.
Urinary iodine concentration (a–c), iodine to creatinine ratio (d–f) and small for gestational age, dichotomous (a,d), linear (b,e) and nonlinear (c,e) meta-analyses. CI: Confidence interval; RR: Relative risk [11,12,13,16,28,32,36,40,42,44].
There were too few studies reporting LGA to conduct any meta-analyses for this outcome.
3.4. Birth Length and Head Circumference
There was no evidence of an association between birth length and UIC as a dichotomous exposure (difference = 0.0 cm, −0.1 to 0.2, p = 0.6, n = 5, I2 = 0%), as a linear trend (0.01 cm per 50 μg/L, 0.00 to 0.02, p = 0.1, n = 4, I2 = 0%), or any evidence of nonlinearity (p = 0.5, n = 5) (Supplementary Figure S5a–c). There were not enough data to conduct meta-analysis for I:Cr or iodide intake.
There was no evidence of an association between head circumference and UIC as a dichotomous exposure (difference = 0.0 cm, −0.2 to 0.2, p = 0.9, n = 5, I2 = 78%), as a linear trend (0.00 cm per 50 μg/L, −0.03 to 0.03, p = 0.8, n = 6, I2 = 16%), or any evidence of nonlinearity (p = 0.4, n = 6) (Supplementary Figure S6a–c). Neither was there evidence of an association between head circumference and I:Cr as a dichotomous exposure (difference = 0.1 cm, −0.1 to 0.3, p = 0.4, n = 3, I2 = 0%), as a linear trend (0.01 cm per 50 μg/g, −0.03 to 0.05, p = 0.6, n = 3, I2 = 49%), or any evidence of nonlinearity (p = 0.6, n = 3) (Supplementary Figure S7a–c). There were insufficient data to conduct meta-analyses for iodide intake.
3.5. Pregnancy Outcomes
Preterm delivery was defined as spontaneous preterm birth in only two studies [11,12], with the remainder using the broader definition of any delivery <37 weeks gestation. There was no evidence of an association between preterm delivery and UIC dichotomised into ≥150 μg/L vs. UIC < 150 μg/L (RR = 0.88, 0.72 to 1.08, p = 0.2, n = 12, I2 = 47%), or as a linear trend (RR = 0.97 per 50 μg/L, 0.92 to 1.02, p = 0.2, n = 12, I2 = 56%). There was also no evidence of nonlinearity in the trend (p = 0.1, n = 10) (Figure 5a–c). Similarly for preterm delivery and I:Cr, there was no evidence of an association with dichotomised I:Cr (RR = 0.97, 0.75 to 1.25, p = 0.8, n = 4, I2 = 14%) or as a linear trend (RR = 1.01 per 50 μg/g, 0.96 to 1.07, p = 0.7, n = 4, I2 = 0%). There was also no evidence of nonlinearity (p = 0.1, n = 4) (Figure 5d–f). There were sufficient studies of iodide intake and preterm delivery only to investigate linear trend, where there was no evidence of an association (RR = 0.99 per 50 μg/d, 0.95 to 1.04, p = 0.8, I2 = 0%) (Supplementary Figure S8).
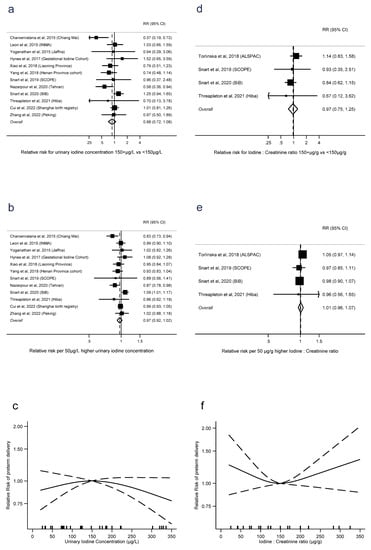
Figure 5.
Urinary iodine concentration (a–c), iodine to creatinine ratio (d–f) and preterm delivery, dichotomous (a,d), linear (b,e), and nonlinear (c,f) meta-analyses. CI: Confidence interval; RR: Relative risk [12,13,14,16,28,34,36,37,40,41,42,43,44].
There were insufficient studies categorising UIC consistently to dichotomise into ≥150 μg/L and UIC < 150 μg/L for meta-analysis of spontaneous abortion ≤24 weeks gestation, however there was no evidence of a linear trend (RR = 0.88, 0.71 to 1.10, p = 0.3, n = 3, I2 = 94%), albeit with large between-study heterogeneity (Supplementary Figure S9). There were insufficient studies to explore potential nonlinearity. There were not enough studies to conduct meta-analysis for I:Cr or iodide intake of this outcome.
There were not enough data to conduct meta-analyses for stillbirth as fetal loss >24 weeks gestation in relation to any outcome.
3.6. Subgroup Analyses and Small-Study Effects
There was no evidence that associations between birth weight and UIC differed by timing of urine collection, median population UIC, income status of country, or any adjustment for potential confounding (Supplementary Table S4, Supplementary Figures S10–S13). Studies with lower scores for selection had higher estimates comparing UIC ≥ 150 μg/L and <150 μg/L, but not with any other domains (Supplementary Figures S14–S16). There was no evidence of associations between SGA and UIC differing by subgroup, other than stronger linear trends seen in studies with lower Newcastle-Ottawa selection scores (Supplementary Table S5, Supplementary Figures S17–S23). For preterm delivery associations between higher UIC and lower risk of preterm delivery were stronger in low and middle-income countries in analyses of dichotomous exposures (p = 0.01) and linear trends (p = 0.02), and some differences between Newcastle-Ottawa comparability scores (Supplementary Table S6, Supplementary Figures S24–S30). There were too few studies reporting I:Cr or iodide intake to conduct subgroup analyses for these outcomes.
There was no evidence of any small-study effects such as publication bias for UIC and birth weight or preterm delivery, where sufficient studies existed to investigate, with no evidence of funnel plot asymmetry (Egger’s tests p = 0.4 and p = 0.9) (Supplementary Figures S31 and S32).
4. Discussion
Our systematic review and series of meta-analyses have included nearly four times as many studies as the most recent reviews, involving analysis of iodine and birth outcomes for more than five times as many participants [9,10]. In addition to UIC, we have also included alternative measures of exposure, such as iodine to creatinine ratio and iodide intake. Moreover, we have investigated continuous dose-response trends over the full range of intakes, including both linear and potential nonlinear trends, to identify potential threshold or plateau effects.
There was evidence of children born to mothers with UIC > 150 μg/L having higher birth weight centile, and lower risk of SGA, but the association between these outcomes and I:Cr was less clear. We also found evidence of an association between higher I:Cr and higher birth weight, up to a threshold of around 200 μg/g, but not for UIC. The potential size of the associations identified was relatively modest compared to other established modifiable risk factors for lower birth weight and SGA, such as smoking [46,47,48], alcohol [49,50] and caffeine [51,52,53], and small enough to be potentially explained by bias in study design, analysis, or selective publication. There was no evidence of an association with preterm delivery, though only two studies reported results for spontaneous preterm delivery.
Results were broadly consistent across studies collecting urine samples earlier in pregnancy and those collecting later, and across different populations defined by median UIC and geographical region, with adjustment for confounding making little difference too.
Our results are consistent with the most recent review, which found insufficient evidence of an association UIC and low birth weight, but adds to this previous work with findings on birth weight centile and SGA. Furthermore, we identified nonlinearity in some of the dose-response curves and differences between subgroups, none of which would have been apparent without the additional information provided by the more recent cohorts. For example, we saw threshold effects in the associations between I:Cr and birth weight and between iodide intake and birth weight, and noted a potential u-shaped association between I:Cr and SGA.
We have included results from studies reporting iodine exposure as both UIC and I:Cr, with the latter identifying stronger associations with birth outcomes. I:Cr may hold some advantage for epidemiological studies in pregnancy, because UIC cannot adequately estimate iodine status of individuals because of day-to-day variation in iodine status and urine dilution. Results from our review support this, with less between-study heterogeneity with I:Cr, and clearer associations despite the smaller number of studies. However, in addition to maternal kidney function, creatinine excretion may also vary with age, physical activity levels, and body mass index, which themselves may be associated with fetal growth [11].
One well-conducted case-control study nested with the Finnish Medical Birth Register using serum iodide as a measure of iodine status was excluded as outside our pre-defined list of exposures in our protocol [54]. The authors found serum iodide was associated with higher odds of preterm birth, but not with SGA. Serum iodide offers an additional measure of iodine status for consideration. In addition, two studies were excluded for using pre-conception measures of iodine status not specified in our pre-defined protocol [55,56]. However, this timeframe is very relevant and may offer a good measure of maternal iodine resources early in pregnancy.
Taking risk of bias into account, we interpret results for preterm delivery cautiously, because of potential reverse causality, with the decision to deliver influenced by fetal growth up to that point. Otherwise, our assessment of study quality mostly differed by choice of covariate adjustment. Standardised measures of birth weight, such as birth weight centile and SGA controlled for important potential confounding, led to broadly reduced between-study heterogeneity in our results, and potentially provide more informative outcomes for obstetricians and paediatricians.
Our review was partly limited by the available data. As with all observational studies, residual confounding within each study is a potential source of bias, with covariate adjustments differing between studies. Self-reported intake is also prone to measurement error, which can bias associations in either direction. In addition, not all studies reported all birth outcomes or all measures of iodine status. Whilst there was no evidence of small study effects such as publication bias for the more widely reported outcomes of birth weight and preterm delivery, there is more opportunity for publication bias in the less frequently reported outcomes, which we could not assess for small study effects using Egger’s test because of insufficient data.
Very few randomised controlled trials of iodine supplementation or fortification have been conducted outside severely iodine-deficient settings [57], so we have focused on meta-analysis of well-conducted cohort studies as the next strongest evidence. However, without random allocation, our ability to infer causality is limited due to potential residual confounding. All but one study of iodide intake reported only dietary sources, so we included both dietary and total iodide intake in the same meta-analyses. However, because of high supplement use in pregnancy, supplemental sources make a large contribution to total iodine intake [16]. Therefore, studies of dietary intake alone that contribute towards our meta-analyses may have underestimated total intake and overestimated any associations.
Most studies reviewed measured iodine status in spot urines for pragmatic reasons. These are prone to greater variability than 24-h urine collections, so subsequent results are inevitably less precise. Furthermore, the timing of the urine collections was averaged within each study for subgroup comparisons, potentially masking some within-study variation.
Our review is strengthened by the large number of well-conducted birth cohorts that have recently published on this topic allowing greater precision in our results and allowing us to identify potential threshold effects and differences between pre-defined subgroups. We have also been able to explore urine dilution-adjusted results using I:Cr, with novel findings, as well as including self-reported iodide intake. We have conducted a comprehensive review, in terms of the range of different measures of iodine status and birth outcomes that give an overall picture of the association between maternal iodine status and birth outcomes.
5. Conclusions
In conclusion, we have found evidence of modest associations between some measures of iodine status, birth weight, birth weight centiles standardised for gestational age. In pregnancy, we recommend reporting iodine status accounting for urine dilution variability using I:Cr as well as the more usual UIC, because of inconsistency in findings between the two measures. Any future studies should also report standardised measures of birth weight for more accurate comparison of outcomes. Whilst the associations are small and not found in all outcomes, they are potentially still important at a population level, and we recommend consideration of methods to maintain iodine sufficiency in the population, especially for women of childbearing age on restricted diets.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu15020387/s1, Supplementary Table S1: Full search strategies; Supplementary Table S2: List of excluded full text articles, with reasons; Supplementary Table S3: Covariate adjustment and Newcastle-Ottawa quality assessment for included studies; Supplementary Table S4: Summary of subgroup analyses for UIC and birth weight; Supplementary Table S5: Summary of subgroup analyses for UIC and SGA; Supplementary Table S6: Summary of subgroup analyses for UIC and preterm delivery; Supplementary Figure S1a: Birth weight and iodide intake forest plot for linear trend, Supplementary Figure S1b: Birth weight and iodide intake nonlinear trend; Supplementary Figure S2a: Low birth weight and UIC forest plot for dichotomous comparison, Supplementary Figure S2b: Low birth weight and UIC forest plot for linear trend, Supplementary Figure S2c: Low birth weight and UIC nonlinear trend; Supplementary Figure S3a: Macrosomia and UIC forest plot for dichotomous comparison, Supplementary Figure S3b: Macrosomia and UIC forest plot for linear trend, Supplementary Figure S3c: Macrosomia and UIC nonlinear trend; Supplementary Figure S4: SGA and iodide intake forest plot for linear trend; Supplementary Figure S5a: Birth length and UIC forest plot for dichotomous comparison, Supplementary Figure S5b: Birth length and UIC forest plot for linear trend, Supplementary Figure S5c: Birth length and UIC nonlinear trend; Supplementary Figure S6a: Head circumference and UIC forest plot for dichotomous comparison, Supplementary Figure S6b: Head circumference and UIC forest plot for linear trend, Supplementary Figure S6c: Head circumference and UIC nonlinear trend; Supplementary Figure S7a: Head circumference and I:Cr forest plot for dichotomous comparison, Supplementary Figure S7b: Head circumference and I:Cr forest plot for linear trend, Supplementary Figure S7c: Head circumference and I:Cr nonlinear trend; Supplementary Figure S8: Preterm delivery and iodide intake forest plot for linear trend; Supplementary Figure S9: Spontaneous abortion and UIC forest plot for linear trend; Supplementary Figure S10: Association between UIC and birth weight by mean gestation when urine sample provided; Supplementary Figure S11: Association between UIC and birth weight by median UIC of study population; Supplementary Figure S12: Association between UIC and birth weight by income status of country; Supplementary Figure S13: Association between UIC and birth weight by adjustment for potential confounding; Supplementary Figure S14: Association between UIC and birth weight by Newcastle-Ottawa quality assessment score for selection; Supplementary Figure S15: Association between UIC and birth weight by Newcastle-Ottawa quality assessment score for comparability; Supplementary Figure S16: Association between UIC and birth weight by Newcastle-Ottawa quality assessment score for outcome; Supplementary Figure S17: Association between UIC and SGA by mean gestation when urine sample provided; Supplementary Figure S18: Association between UIC and SGA by median UIC of study population; Supplementary Figure S19: Association between UIC and SGA by income status of country; Supplementary Figure S20: Association between UIC and SGA by adjustment for potential confounding; Supplementary Figure S21: Association between UIC and SGA by Newcastle-Ottawa quality assessment score for selection; Supplementary Figure S22: Association between UIC and SGA by Newcastle-Ottawa quality assessment score for comparability; Supplementary Figure S23: Association between UIC and SGA by Newcastle-Ottawa quality assessment score for outcome; Supplementary Figure S24: Association between UIC and preterm delivery by mean gestation when urine sample provided; Supplementary Figure S25: Association between UIC and preterm delivery by median UIC of study population; Supplementary Figure S26: Association between UIC and preterm delivery by income status of country; Supplementary Figure S27: Association between UIC and preterm delivery by adjustment for potential confounding; Supplementary Figure S28: Association between UIC and preterm delivery by Newcastle-Ottawa quality assessment score for selection; Supplementary Figure S29: Association between UIC and preterm delivery by Newcastle-Ottawa quality assessment score for comparability; Supplementary Figure S30: Association between UIC and preterm delivery by Newcastle-Ottawa quality assessment score for outcome; Supplementary Figure S31: Contour-enhanced funnel plots for UIC and birth weight; Supplementary Figure S32: Contour-enhanced funnel plots for UIC and preterm delivery.
Author Contributions
Conceptualization, D.C.G.; Methodology, D.C.G.; Validation, D.C.G. and J.W.; Formal analysis, D.C.G.; Investigation, D.C.G., C.K., E.T. and L.J.H.; Writing—Original Draft, D.C.G.; Writing—Review and Editing, D.C.G., J.W., C.K., E.T. and L.J.H.; Visualization, D.C.G.; Supervision, D.C.G. and L.J.H.; Project administration, D.C.G. and L.J.H. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no specific funding for this work. JW is in receipt of a scholarship from the School of Food Science and Nutrition, University of Leeds; and Rank Prize Funds. DCG and LJH were joint principal investigators on previous work funded by the National Institute for Health Research (NIHR) Policy Research Programme (Assessing iodine status and associated health outcomes in British women during pregnancy, PR-R10-0514-11004). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. No funding bodies had any role in study design, data collection, analysis or interpretation, in the writing of the report or in the decision to submit the article for publication.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Example template data collection spreadsheets are available from authors on reasonable request.
Acknowledgments
The authors thank the authors of contributing studies.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
Iodine to creatinine ratio (I:Cr); large for gestational age (LGA); urinary iodine concentration (UIC); small for gestational age (SGA); World Health Organization (WHO).
References
- Scientific Advisory Committee on Nutrition. SACN Statement on Iodine and Health—2014. Available online: https://www.gov.uk/government/publications/sacn-statement-on-iodine-and-health-2014 (accessed on 8 January 2023).
- Zimmermann, M.B. The importance of adequate iodine during pregnancy and infancy. World Rev. Nutr. Diet. 2016, 115, 118–124. [Google Scholar]
- World Health Organization. Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination: A Guide for Programme Managers; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Zimmermann, M.B. Iodine deficiency in pregnancy and the effects of maternal iodine supplementation on the offspring: A review. Am. J. Clin. Nutr. 2009, 89, 668S–672S. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; Takkouche, B.; Egli, I.; Benoist, B.d. The WHO Global Database on iodine deficiency disorders: The importance of monitoring iodine nutrition. Scand. J. Nutr. 2003, 47, 162–166. [Google Scholar] [CrossRef]
- Zimmermann, M.B.; Gizak, M.é.; Abbott, K.; Andersson, M.; Lazarus, J.H. Iodine deficiency in pregnant women in Europe. Lancet Diabetes Endocrinol. 2015, 3, 672–674. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.; Irdam, D.; Bulceag, I.; Barber, T.; Draper, A. The Food and You Survey Wave 5 Secondary Analysis: The Current Food Landscape across England, Wales and Northern Ireland. 2019. Available online: https://www.food.gov.uk/sites/default/files/media/document/food-and-you-wave-5-secondary-analysis-current-food-landscape.pdf (accessed on 8 January 2023).
- Public Health England. NDNS: Results from Years 9 to 11 (2016 to 2017 and 2018 to 2019). Available online: https://www.gov.uk/government/statistics/ndns-results-from-years-9-to-11-2016-to-2017-and-2018-to-2019 (accessed on 24 March 2022).
- Nazarpour, S.; Ramezani Tehrani, F.; Behboudi-Gandevani, S.; Bidhendi Yarandi, R.; Azizi, F. Maternal Urinary Iodine Concentration and Pregnancy Outcomes in Euthyroid Pregnant Women: A Systematic Review and Meta-analysis. Biol. Trace Elem. Res. 2020, 197, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Nazeri, P.; Shab-Bidar, S.; Pearce, E.N.; Shariat, M. Do maternal urinary iodine concentration or thyroid hormones within the normal range during pregnancy affect growth parameters at birth? A systematic review and meta-analysis. Nutr. Rev. 2020, 78, 747–763. [Google Scholar] [CrossRef] [PubMed]
- Abel, M.H.; Caspersen, I.H.; Sengpiel, V.; Jacobsson, B.; Meltzer, H.M.; Magnus, P.; Alexander, J.; Brantsaeter, A.L. Insufficient maternal iodine intake is associated with subfecundity, reduced foetal growth, and adverse pregnancy outcomes in the Norwegian Mother, Father and Child Cohort Study. BMC Med. 2020, 18, 211. [Google Scholar] [CrossRef] [PubMed]
- Snart, C.J.P.; Keeble, C.; Taylor, E.; Cade, J.E.; Stewart, P.M.; Zimmermann, M.; Reid, S.; Threapleton, D.E.; Poston, L.; Myers, J.E.; et al. Maternal iodine status and associations with birth outcomes in three major cities in the United Kingdom. Nutrients 2019, 11, 441. [Google Scholar] [CrossRef]
- Snart, C.J.P.; Threapleton, D.E.; Keeble, C.; Taylor, E.; Waiblinger, D.; Reid, S.; Alwan, N.A.; Mason, D.; Azad, R.; Cade, J.E.; et al. Maternal iodine status, intrauterine growth, birth outcomes and congenital anomalies in a UK birth cohort. BMC Med. 2020, 18, 132. [Google Scholar] [CrossRef]
- Cui, X.; Yu, H.; Wang, Z.; Wang, H.; Shi, Z.; Jin, W.; Song, Q.; Guo, C.; Tang, H.; Zang, J. No Association Was Found Between Mild Iodine Deficiency During Pregnancy and Pregnancy Outcomes: A Follow-up Study Based on a Birth Registry. Biol. Trace Elem. Res. 2022, 200, 4267–4277. [Google Scholar] [CrossRef]
- Clark, J.; Glasziou, P.; Del Mar, C.; Bannach-Brown, A.; Stehlik, P.; Scott, A.M. A full systematic review was completed in 2 weeks using automation tools: A case study. J. Clin. Epidemiol. 2020, 121, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Threapleton, D.E.; Waiblinger, D.; Snart, C.J.P.; Taylor, E.; Keeble, C.; Ashraf, S.; Bi, S.; Ajjan, R.; Azad, R.; Hancock, N.; et al. Prenatal and Postpartum Maternal Iodide Intake from Diet and Supplements, Urinary Iodine and Thyroid Hormone Concentrations in a Region of the United Kingdom with Mild-to-Moderate Iodine Deficiency. Nutrients 2021, 13, 230. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 21 January 2014).
- Greenland, S.; Longnecker, M.P. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am. J. Epidemiol. 1992, 135, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Orsini, N.; Bellocco, R.; Greenland, S. Generalized least squares for trend estimation of summarized dose-response data. Stata J. 2006, 6, 40–57. [Google Scholar] [CrossRef]
- Orsini, N.; Li, R.; Wolk, A.; Khudyakov, P.; Spiegelman, D. Meta-analysis for linear and nonlinear dose-response relations: Examples, an evaluation of approximations, and software. Am. J. Epidemiol. 2012, 175, 66–73. [Google Scholar] [CrossRef]
- White, I.R. Multivariate random-effects meta-analysis. Stata J. 2009, 9, 40–56. [Google Scholar] [CrossRef]
- White, I.R. Multivariate random-effects meta-regression: Updates to mvmeta. Stata J. 2011, 11, 255–270. [Google Scholar] [CrossRef]
- Harrell, F.E., Jr.; Lee, K.L.; Pollock, B.G. Regression models in clinical studies: Determining relationships between predictors and response. J. Natl. Cancer Inst. 1988, 80, 1198–1202. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Borenstein, M.; Higgins, J.P.T.; Hedges, L.V.; Rothstein, H.R. Basics of meta-analysis: I2 is not an absolute measure of heterogeneity. Res. Synth. Methods 2017, 8, 5–18. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 17; StataCorp LLC: College Station, TX, USA, 2021. [Google Scholar]
- Bienertova-Vasku, J.; Grulichova, M.; Mikes, O.; Zlamal, F.; Prusa, T.; Pohorala, A.; Andryskova, L.; Pikhart, H. Estimated dietary iodine intake as a predictor of placental size: Evidence from the ELSPAC study. Nutr. Metab. 2018, 15, 5. [Google Scholar] [CrossRef] [PubMed]
- Charoenratana, C.; Leelapat, P.; Traisrisilp, K.; Tongsong, T. Maternal iodine insufficiency and adverse pregnancy outcomes. Matern. Child Nutr. 2016, 12, 680–687. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Li, Q.; Cui, W.; Wang, X.; Gao, Q.; Zhong, C.; Sun, G.; Chen, X.; Xiong, G.; Yang, X.; et al. Maternal Iodine Insufficiency and Excess Are Associated with Adverse Effects on Fetal Growth: A Prospective Cohort Study in Wuhan, China. J. Nutr. 2018, 148, 1814–1820. [Google Scholar] [CrossRef] [PubMed]
- Dillon, J.C.; Milliez, J. Reproductive failure in women living in iodine deficient areas of West Africa. Br. J. Obstet. Gynaecol. 2000, 107, 631–636. [Google Scholar] [CrossRef]
- Dong, J.; Liu, S.; Wang, L.; Zhou, X.; Zhou, Q.; Liu, C.; Zhu, J.; Yuan, W.; Xu, W.Y.; Deng, J. Iodine monitoring models contribute to avoid adverse birth outcomes related more than adequate iodine intake. BMC Pregnancy Childbirth 2021, 21, 454. [Google Scholar] [CrossRef] [PubMed]
- Farebrother, J.; Dalrymple, K.V.; White, S.L.; Gill, C.; Brockbank, A.; Lazarus, J.H.; Godfrey, K.M.; Poston, L.; Flynn, A.C. Iodine status of pregnant women with obesity from inner city populations in the United Kingdom. Eur. J. Clin. Nutr. 2021, 75, 801–808. [Google Scholar] [CrossRef]
- Ghassabian, A.; Steenweg-de Graaff, J.; Peeters, R.P.; Ross, H.A.; Jaddoe, V.W.; Hofman, A.; Verhulst, F.C.; White, T.; Tiemeier, H. Maternal urinary iodine concentration in pregnancy and children’s cognition: Results from a population-based birth cohort in an iodine-sufficient area. BMJ Open 2014, 4, e005520. [Google Scholar] [CrossRef]
- Hynes, L.K.; Otahal, P.; Burgess, R.J.; Oddy, H.W.; Hay, I. Reduced Educational Outcomes Persist into Adolescence Following Mild Iodine Deficiency in Utero, Despite Adequacy in Childhood: 15-Year Follow-Up of the Gestational Iodine Cohort Investigating Auditory Processing Speed and Working Memory. Nutrients 2017, 9, 1354. [Google Scholar] [CrossRef]
- Kianpour, M.; Aminorroaya, A.; Amini, M.; Feizi, A.; Aminorroaya Yamini, S.; Janghorbani, M. Thyroid-stimulating hormone (TSH) serum levels and risk of spontaneous abortion: A prospective population-based cohort study. Clin. Endocrinol. 2019, 91, 163–169. [Google Scholar] [CrossRef]
- Leon, G.; Murcia, M.; Rebagliato, M.; Alvarez-Pedrerol, M.; Castilla, A.M.; Basterrechea, M.; Iniguez, C.; Fernandez-Somoano, A.; Blarduni, E.; Foradada, C.M.; et al. Maternal thyroid dysfunction during gestation, preterm delivery, and birthweight. The infancia y medio ambiente cohort, Spain. Paediatr. Perinat. Epidemiol. 2015, 29, 113–122. [Google Scholar] [CrossRef]
- Nazarpour, S.; Ramezani Tehrani, F.; Amiri, M.; Simbar, M.; Tohidi, M.; Bidhendi Yarandi, R.; Azizi, F. Maternal Urinary Iodine Concentration and Pregnancy Outcomes: Tehran Thyroid and Pregnancy Study. Biol. Trace Elem. Res. 2020, 194, 348–359. [Google Scholar] [CrossRef] [PubMed]
- Ovadia, Y.S.; Zangen, S.; Rosen, S.R.; Gefel, D.; Almashanu, S.; Benbassat, C.; Fytlovich, S.; Aharoni, D.; Anteby, E.Y.; Shenhav, S. Maternal iodine deficiency: A newborns’ overweight risk factor? A prospective study. Arch. Gynecol. Obstet. 2022, 305, 777–787. [Google Scholar] [CrossRef] [PubMed]
- Rydbeck, F.; Rahman, A.; Grander, M.; Ekstrom, E.C.; Vahter, M.; Kippler, M. Maternal urinary iodine concentration up to 1.0 mg/L is positively associated with birth weight, length, and head circumference of male offspring. J. Nutr. 2014, 144, 1438–1444. [Google Scholar] [CrossRef]
- Torlinska, B.; Bath, S.C.; Janjua, A.; Boelaert, K.; Chan, S.Y. Iodine status during pregnancy in a region of mild-to-moderate iodine deficiency is not associated with adverse obstetric outcomes; Results from the Avon Longitudinal Study of Parents and Children (ALSPAC). Nutrients 2018, 10, 291. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Sun, H.; Li, C.; Li, Y.; Peng, S.; Fan, C.; Teng, W.; Shan, Z. Effect of Iodine Nutrition on Pregnancy Outcomes in an Iodine-Sufficient Area in China. Biol. Trace Elem. Res. 2018, 182, 231–237. [Google Scholar] [CrossRef]
- Yang, J.; Liu, Y.; Liu, H.; Zheng, H.; Li, X.; Zhu, L.; Wang, Z. Associations of maternal iodine status and thyroid function with adverse pregnancy outcomes in Henan Province of China. J. Trace Elem. Med. Biol. 2018, 47, 104–110. [Google Scholar] [CrossRef]
- Yoganathan, T.; Hettiarachchi, M.; Arasaratnam, V.; Liyanage, C. Maternal iodine status and the thyroid function of pregnant mothers and their neonates in Jaffna District of Sri Lanka. Indian J. Endocrinol. Metab. 2015, 19, 817–823. [Google Scholar] [CrossRef]
- Zhang, X.; Yuan, N.; Sun, J.; Zhao, X.; Du, J.; Nan, M.; Zhang, Q.L.; Ji, L. Association Between Iodine Nutritional Status and Adverse Pregnancy Outcomes in Beijing, China: A Single-Center Cohort Study. Biol. Trace Elem. Res. 2022, 200, 2620–2628. [Google Scholar] [CrossRef]
- Lean, M.I.; Lean, M.E.; Yajnik, C.S.; Bhat, D.S.; Joshi, S.M.; Raut, D.A.; Lubree, H.G.; Combet, E. Iodine status during pregnancy in India and related neonatal and infant outcomes. Public Health Nutr. 2014, 17, 1353–1362. [Google Scholar] [CrossRef]
- Di, H.-K.; Gan, Y.; Lu, K.; Wang, C.; Zhu, Y.; Meng, X.; Xia, W.-Q.; Xu, M.-Z.; Feng, J.; Tian, Q.-F.; et al. Maternal smoking status during pregnancy and low birth weight in offspring: Systematic review and meta-analysis of 55 cohort studies published from 1986 to 2020. World J. Pediatr. 2022, 18, 176–185. [Google Scholar] [CrossRef]
- Rumrich, I.; Vähäkangas, K.; Viluksela, M.; Gissler, M.; de Ruyter, H.; Hänninen, O. Effects of maternal smoking on body size and proportions at birth: A register-based cohort study of 1.4 million births. BMJ Open 2020, 10, e033465. [Google Scholar] [CrossRef] [PubMed]
- Wojtyła, C.; Wojtyła-Buciora, P.; Ciebiera, M.; Orzechowski, S.; Wojtyła, A. The effect of active and passive maternal smoking before and during pregnancy on neonatal weight at birth. Arch. Med. Sci. 2021, 17, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Patra, J.; Bakker, R.; Irving, H.; Jaddoe, V.W.V.; Malini, S.; Rehm, J. Dose–response relationship between alcohol consumption before and during pregnancy and the risks of low birthweight, preterm birth and small for gestational age (SGA)—A systematic review and meta-analyses. BJOG Int. J. Obstet. Gynaecol. 2011, 118, 1411–1421. [Google Scholar] [CrossRef] [PubMed]
- Mamluk, L.; Edwards, H.B.; Savović, J.; Leach, V.; Jones, T.; Moore, T.H.M.; Ijaz, S.; Lewis, S.J.; Donovan, J.L.; Lawlor, D.; et al. Low alcohol consumption and pregnancy and childhood outcomes: Time to change guidelines indicating apparently ‘safe’ levels of alcohol during pregnancy? A systematic review and meta-analyses. BMJ Open 2017, 7, e015410. [Google Scholar] [CrossRef] [PubMed]
- Boylan, S.; Cade, J.E.; Dolby, V.A.; Greenwood, D.C.; Hay, A.W.M.; Kirk, S.F.L.; Shires, S.; Simpson, N.; Thomas, J.D.; Walker, J.; et al. Maternal caffeine intake during pregnancy and risk of fetal growth restriction: A large prospective observational study. BMJ 2008, 337, a2332. [Google Scholar] [CrossRef]
- Greenwood, D.C.; Thatcher, N.J.; Ye, J.; Garrard, L.; Keogh, G.; King, L.G.; Cade, J.E. Caffeine intake during pregnancy and adverse birth outcomes: A systematic review and dose–response meta-analysis. Eur. J. Epidemiol. 2014, 29, 725–734. [Google Scholar] [CrossRef]
- Chen, L.-W.; Wu, Y.; Neelakantan, N.; Chong, M.F.-F.; Pan, A.; van Dam, R.M. Maternal caffeine intake during pregnancy is associated with risk of low birth weight: A systematic review and dose-response meta-analysis. BMC Med. 2014, 12, 174. [Google Scholar] [CrossRef]
- Purdue-Smithe, A.C.; Mannisto, T.; Bell, G.A.; Mumford, S.L.; Liu, A.; Kannan, K.; Kim, U.J.; Suvanto, E.; Surcel, H.M.; Gissler, M.; et al. The joint role of thyroid function and iodine status on risk of preterm birth and small for gestational age: A population-based nested case-control study of Finnish women. Nutrients 2019, 11, 2573. [Google Scholar] [CrossRef]
- Melero, V.; Runkle, I.; de la Torre, N.G.; De Miguel, P.; Valerio, J.; Del Valle, L.; Barabash, A.; Sanabria, C.; Moraga, I.; Familiar, C.; et al. The consumption of food-based iodine in the immediate pre-pregnancy period in madrid is insufficient. San carlos and pregnancy cohort study. Nutrients 2021, 13, 4458. [Google Scholar] [CrossRef]
- Mills, J.L.; Mehnaz, A.; Louis, G.M.B.; Kannan, K.; Weck, J.; Wan, Y.; Maisog, J.; Giannakou, A.; Sundaram, R. Pregnancy loss and iodine status: The LIFE prospective cohort study. Nutrients 2019, 11, 534. [Google Scholar] [CrossRef]
- Nazeri, P.; Shariat, M.; Azizi, F. Effects of iodine supplementation during pregnancy on pregnant women and their offspring: A systematic review and meta-analysis of trials over the past 3 decades. Eur. J. Endocrinol. 2021, 184, 91–106. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).